Contents
Ruptured spleen
Ruptured spleen is a serious medical emergency that leads to life-threatening internal bleeding that requires swift diagnosis and intervention, and sometimes surgery 1. Severe internal bleeding can cause death within hours if it isn’t treated right away. The mortality rate from simple splenic rupture is 1% 2. Delayed diagnosis of a ruptured spleen increases the rate to 10% 2. Your spleen is an organ that sits just below your left rib cage adjacent to ribs nine through 12, just beneath the left diaphragm (see Figure 4 below). Your spleen lies behind and to the left side of your stomach. The normal sized spleen abuts the stomach, colon, and left kidney.
Ruptured spleen causes may include 3, 4:
- Trauma: The most common cause of ruptured spleen is blunt force trauma to the abdomen or the left lower chest, such as from a car accident, a fall, fistfights, a sports injury (like from football or hockey), or a blow to the left side of the body. An injured spleen can rupture soon after the stomach trauma or, in some cases, days or weeks after the injury.
- Four types of splenic injuries are recognized: intraparenchymal laceration, subcapsular hematoma, and splenic rupture and delayed rupture 5.
- An enlarged spleen. Your spleen can become enlarged when blood cells accumulate in the spleen. An enlarged spleen can be caused by various underlying problems, such as mononucleosis and other infections, liver disease, and blood cancers:
- Viral infections, such as mononucleosis
- Bacterial infections, such as syphilis or an infection of your heart’s inner lining (endocarditis)
- Parasitic infections, such as malaria
- Cirrhosis and other diseases affecting the liver
- Various types of hemolytic anemia — a condition characterized by early destruction of red blood cells
- Blood cancers, such as leukemia and myeloproliferative neoplasms, and lymphomas, such as Hodgkin’s disease
- Metabolic disorders, such as Gaucher disease and Niemann-Pick disease
- Pressure on the veins in the spleen or liver or a blood clot in these veins
- Autoimmune conditions, such as lupus or sarcoidosi
- Spontaneous rupture: In rare cases, spleen rupture can occur spontaneously without a known injury 6, 7. Malaria is a known risk factor for spontaneous splenic rupture, particularly in individuals staying in endemic areas or returning travelers presenting with splenomegaly 8, 9. Atraumatic splenic rupture may also result from pancreatitis.
Splenic injuries are classified according to the American Association for the Surgery of Trauma (AAST) Organ Injury Scale, which standardizes grading based on the extent of hematoma, laceration, and vascular involvement 10. Accurate injury grading guides appropriate decision-making for nonoperative versus operative management.
- Grade 1: Subcapsular hematoma involving less than 10% of surface area, or capsular laceration less than 1 cm in depth
- Grade 2: Subcapsular hematoma involving 10% to 50% of surface area, intraparenchymal hematoma less than 5 cm, or laceration 1 cm to 3 cm in depth without involvement of trabecular vessels
- Grade 3: Subcapsular hematoma involving more than 50% of surface area or expanding, intraparenchymal hematoma greater than 5 cm or expanding, or laceration greater than 3 cm in depth or involving trabecular vessels
- Grade 4: Laceration involving segmental or hilar vessels with devascularization of more than 25% of the spleen
- Grade 5: Shattered spleen or hilar vascular injury resulting in complete splenic devascularization
- *Advance one grade for multiple injuries up to grade 3. Higher-grade injuries often require surgical management, while lower grades may be managed conservatively in stable patients.
Your spleen is located in the upper left quadrant of your abdomen, under your left ribcage and diaphragm (see Figure 4 below). Symptoms of injured spleen or ruptured spleen include pain in your upper left abdomen that can radiate to your left shoulder, abdomen may feel rigid and tender to the touch, lightheadedness, dizziness, confusion, and a rapid heart rate. Furthermore, the types of injuries that can cause a ruptured spleen are likely to cause other trauma too, for example, a fractured rib. You may not be able to distinguish the feeling of a ruptured spleen from these other injuries.
After the moment of rupture, pain from your ruptured spleen may seem to move to the left side of your chest or your left shoulder. This is called Kehr’s sign 11, 12. It happens because bleeding from your ruptured spleen can irritate a nerve (your left phrenic nerve) that runs from your neck down through the left side of your chest. You may notice the pain is worse when you breathe in.
You may have symptoms related to blood loss and a rapid drop in blood pressure. These can include:
- Dizziness or lightheadedness.
- Mental confusion or disorientation.
- Blurred vision.
- Paleness and faintness.
- Restlessness or anxiety.
- Nausea.
- A rapid heart rate.
A ruptured spleen is a medical emergency. Seek immediate emergency care if you suspect you have one, especially after an injury to your abdomen. If you have severe upper left abdominal pain or Kehr’s sign (referred pain to your left shoulder), even if it occurs sometime after your original injury, you should go straight to the emergency room. Call an ambulance if necessary. Tell the ER doctors about your symptoms and any recent injuries, infections or chronic diseases you’ve had. Injured spleen treatment depends on severity and ranges from a hospital stay with observation to surgery to repair or remove the spleen.
Most injuries to the spleen manifest at the moment of injury with symptoms of acute intraperitoneal hemorrhage (bleeding into the peritoneal cavity, the space surrounding abdominal and pelvic organs) and hemorrhagic shock (a life-threatening condition caused by significant blood loss that leads to a drop in blood volume, causing inadequate oxygen delivery to the body’s tissues) 13. At this point the patient falls into one of two categories:
- Hemodynamically Stable or
- Hemodynamically Unstable based on their vital signs (blood pressure and heart rate).
If the patient has a low blood pressure and/or a high heart rate (hemodynamically unstable), the trauma surgeon must identify the cause, which is often due to bleeding. Next the trauma surgeon determines the location of the bleeding. If it appears that the abdomen is the source, the patient may need to be taken to the operating room emergently for exploratory abdominal surgery. If a splenic injury with bleeding is found, removal of the entire spleen (splenectomy) or removing only part of it (partial splenectomy) may be required.
For minor injuries, a hospital stay for observation, bed rest, and possibly blood transfusions may be sufficient. Follow-up CT scans are used to monitor healing.
In simple terms, unstable patients suspected of splenic injury and intra-abdominal hemorrhage should undergo exploratory laparotomy and splenic repair or removal. A blunt trauma patient with evidence of hemodynamic instability unresponsive to fluid challenge with no other signs of external hemorrhage should be considered to have a life-threatening solid organ (splenic) injury until proven otherwise. Transient responders, those patients who respond to an initial fluid bolus only to deteriorate again with a drop in blood pressure and increasing heart rate (tachycardia), are also likely to have solid organ injury with ongoing hemorrhage. Patients with compensated shock may be managed by angioembolization but only if these services can be performed in a timely manner equivalent to that of operative intervention.
For many years it was accepted that splenic injury was best managed by splenectomy (removal of the entire spleen). However, it has more recently been realized that patients whose spleen has been removed are more liable to life-threatening infections 14. This is of particular consequence if splenectomy is performed in childhood, with a long life expectancy. The spleen has many functions including filtering or removing old poorly functioning red blood cells, catching bacteria, and producing antibodies (see Spleen Function below). After removal of the spleen, these functions are lost and the patient could be susceptible to an overwhelming post-splenectomy infections from bacteria such as streptococcus pneumoniae, neisseria meningitidis, and hemophilus influenza 3. To reduce this risk, patients who undergo surgery to remove their spleen receive vaccines against these bacteria.With greater understanding of the splenic anatomy and function, and natural course of splenic injuries, the management has evolved into a more conservative approach though a splenectomy may still be required in some situations.
Treatment for splenic injury:
- Approximately 70% to 90% of children with isolated blunt splenic injury receive Non-Operative Management (NOM) 15, 16. The success rate of Non-Operative Management (NOM) in children with isolated blunt splenic injury has been reported at 90% to 100% 17, 18, 19. However, delayed complications have been reported, including pseudocysts, abscess, pseudoaneurysms, and delayed rupture 20, 21. Among these complications, delayed splenic bleeding is the most severe. Delayed splenic bleeding is an extremely rare complication in children, with incidence rates of only 0 to 0.33% 17, 18, 19, 22. Various theories concerning the cause of delayed splenic bleeding include tears in a subcapsular hematoma, clot disruption, rupture of pseudoaneurysm, and internal splenic pseudocyst bleeding 23, 22.
- Approximately 40% to 50% of adult patients with splenic injury receive Non-Operative Management (NOM). A retrospective analysis by Scarborough et al 24 compared the effectiveness of Non-Operative Management (NOM) with immediate splenectomy for adult patients with grade 4 or 5 blunt splenic injury. The study found that both approaches had similar rates of in-hospital mortality (11.5% in the splenectomy group vs 10.0%); however, there was a higher incidence of infectious complications in the immediate splenectomy group 24. The rate of failure in the Non-Operative Management (NOM) was 20.1% and symptoms of a bleeding disorder, the need for an early blood transfusion, and grade 5 injury were all early predictors of nonoperative management failure 24.
- 85% patient receive Non-Operative Management (NOM) in some centers. Splenic artery embolization is increasingly being used in both stable patients and transient responders for fluid resuscitation under constant supervision by a surgeon with an operating room on standby. Femoral artery access with embolization of the splenic artery or its branches can be accomplished with gel foam or metal coils. Splenic artery embolization requires intimate cooperation between the trauma surgeon and the interventional radiologist. Not all hospitals will have the proper facilities for such treatment, and any surgeon contemplating splenic artery embolization for a patient should first make sure the hospital interventional radiology suite and personnel are set up for rapid response at any hour of the day.
- Higher splenectomy rates have been reported in smaller hospitals, often due to limited access to interventional radiology or intensive care monitoring.
In the stable trauma patient (hemodynamically stable), commonly defined as a patient with systolic blood pressure greater than 90 mm Hg with a heart rate less than 120 beats per minute (bpm), CT scan of the abdomen/pelvis provides the most ideal noninvasive means for evaluating the spleen. Helical or spiral scanners may provide even more information and may clarify the degree of injury. At this point if the patient is found to have a splenic laceration it is graded according to the American Association for the Surgery of Trauma splenic injury scale (see Table 1 below). Other factors such as intravenous contrast extravasation or “blush” can also be identified via the CT scan, which indicates that there may be active bleeding in progress in which case a hemodynamically stable patient may be sent to interventional radiology so that an angiogram can be performed and a potential active bleeding vessel can be embolized or coiled to stop any further bleeding. The patient then may be observed in the ICU/floor depending on severity and other trauma to the patient. Close monitoring of the patient’s condition, vital signs, blood tests and serial abdominal exams are required in order to assess the stability of the bleeding from the injury. The trauma surgeon must be prepared to operate 24/7 in case recurrent bleeding develops after a period of stability. Thus, these patients are best managed at a trauma center, which has the necessary resources to intervene quickly. If the patient remains stable the patient’s diet and activity can slowly be started after 24 hrs or depending on the individual institution’s protocols.
In the cases of CT scan–documented splenic injury, the decision for operative intervention is determined by the grade of the injury, the patient’s current and preexisting medical conditions, and the facilities available at the hospital, including the intensive care unit and the availability of operating and anesthesia services.
Whether the patient undergoes surgery or is managed non-operatively there are risks and complications associated with either strategy. After surgery there is always a small risk of infection and additionally bleeding from the procedure. If the spleen has been removed, the patient is at risk for certain bacterial infections, as discussed earlier and will require vaccinations. There is also a risk during the procedure of injuring the pancreas or other organs necessitating additional procedures. With the non-operative strategy there is a risk of delayed bleeding which may require an operation to remove the spleen. Also if the patient is selected for nonoperative management there is a chance of a missed associated injury in the abdomen such as a bowel injury.
As a result of understanding the function of the spleen, natural evolution of the splenic injury, improving technology and adjuncts such as angiogram the trauma surgeons are better able to manage blunt spleen injuries nonoperatively more successfully than before. Managing a hemodynamically unstable patient suspected of having an intra-abdominal injury often requires an immediate surgery for abdominal exploration. However, out of the patients managed nonoperatively there still is a set of patients that fail this type of management who will require surgical intervention and it is in those patients that the trauma surgeon must be vigilant. Blunt splenic trauma management has evolved significantly over the last few decades and as our understanding of the injury and its evolution improves so does our ability to manage the splenic injury whether it’s nonoperatively or surgically.
Figure 1. Ruptured spleen
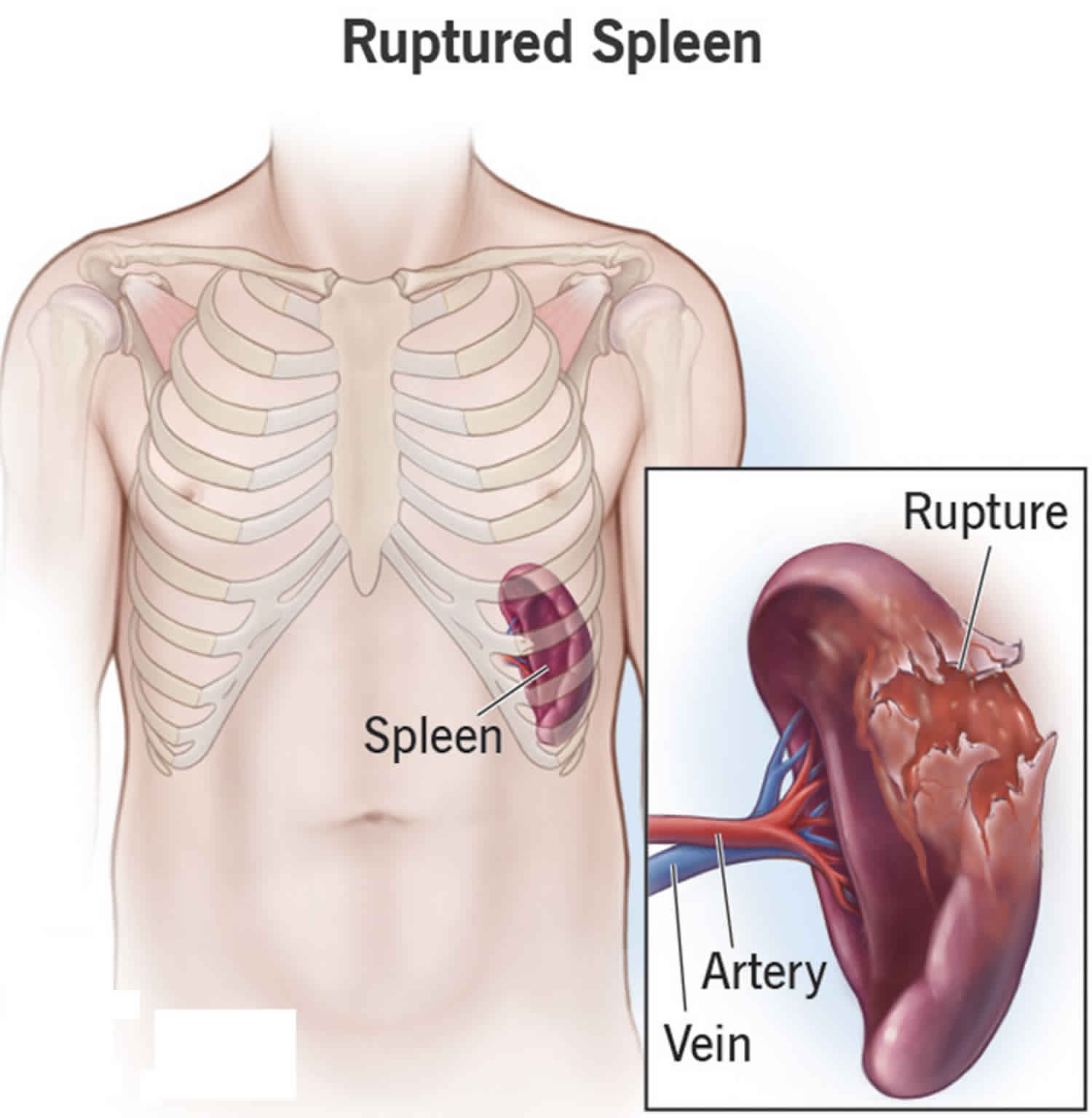
Figure 2. Ruptured spleen CT scan
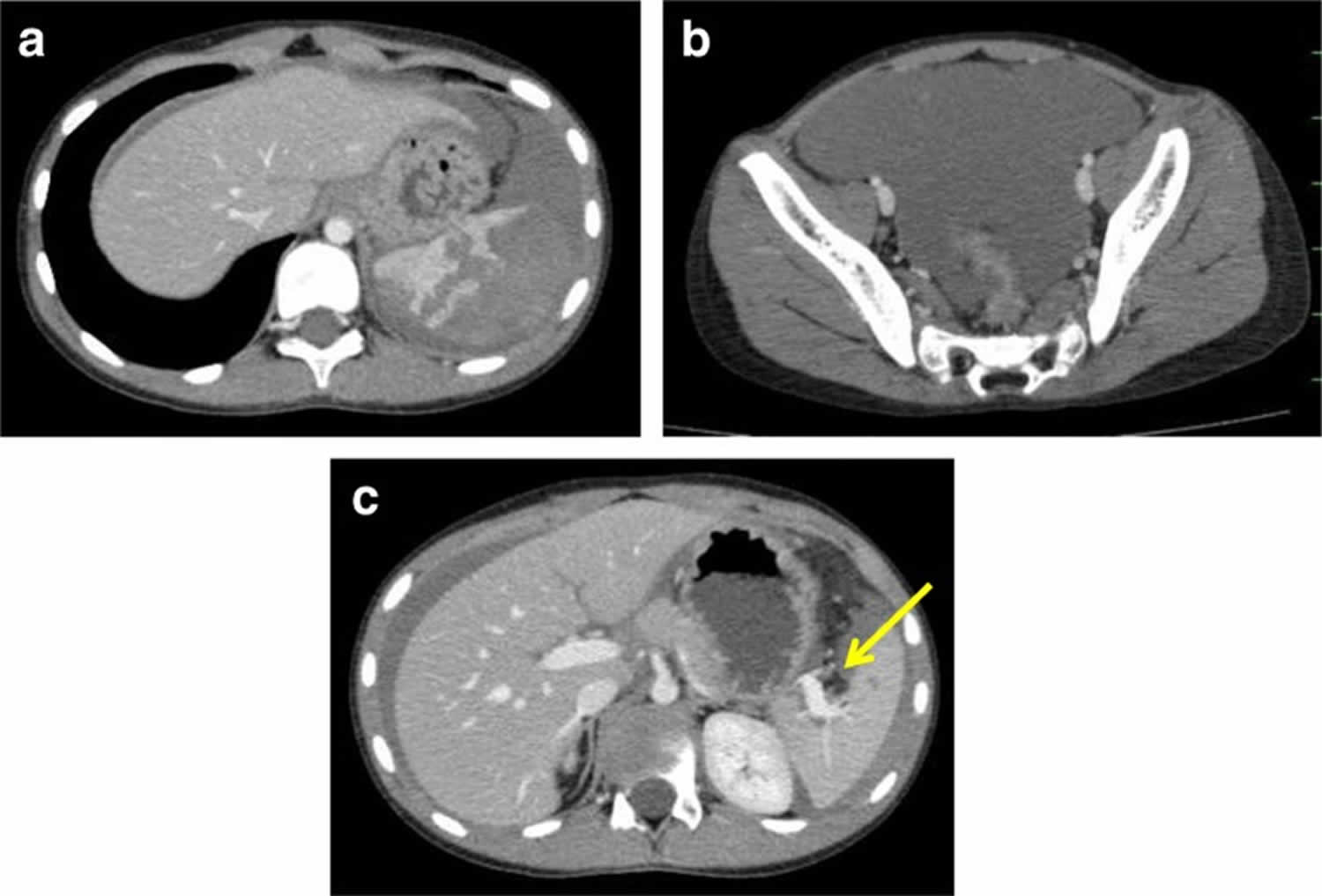
Footnotes: A 9-year-old boy (height: 133 cm, weight: 25.8 kg) with severe abdominal pain was transferred to a hospital. Twenty-one hours before admission, he had been kicked in the region of his left lateral abdomen. On admission, his face was pale, and his Glasgow coma scale was recorded at 13/15 (E: 3, V: 4, M: 6). A physical examination revealed severe tenderness on the left lateral abdomen with moderate abdominal distension. His vital signs were as follows: blood pressure 80/50 mmHg, heart rate 110 bpm, and a respiratory rate of 30/min, respectively. Contrast-enhanced abdominal computed tomography (21 hours after injury) revealed (a) a severe intraparenchymal hematoma with multiple lacerations of the spleen and (b) a large amount of hemoperitoneum was detected in the pelvic cavity. (c) The hilar vessels of the spleen were not injured, and no active bleeding was seen in the spleen (yellow arrow). His injury was diagnosed as grade 3 on the American Association for the Surgery of Trauma (AAST) splenic injury scale. The patient’s laboratory data showed his red blood cell count 251 × 104/ml, hemoglobin (Hb) 9.1 g/dl, hematocrit (Ht) 27.1%, and platelets 33.6 × 104/μl. All of his other laboratory data were within normal limits. After fluid resuscitation, his blood Hb and Ht levels fell to 7.6 g/dl and 22.3%, respectively. He required a transfusion of 1000 ml red blood cells in order to maintain his blood pressure. His vital signs became stable, and he regained clear consciousness.
[Source 25 ]Figure 3. Delayed rupture of the spleen with traumatic pseudoaneurysms and A-V fistula
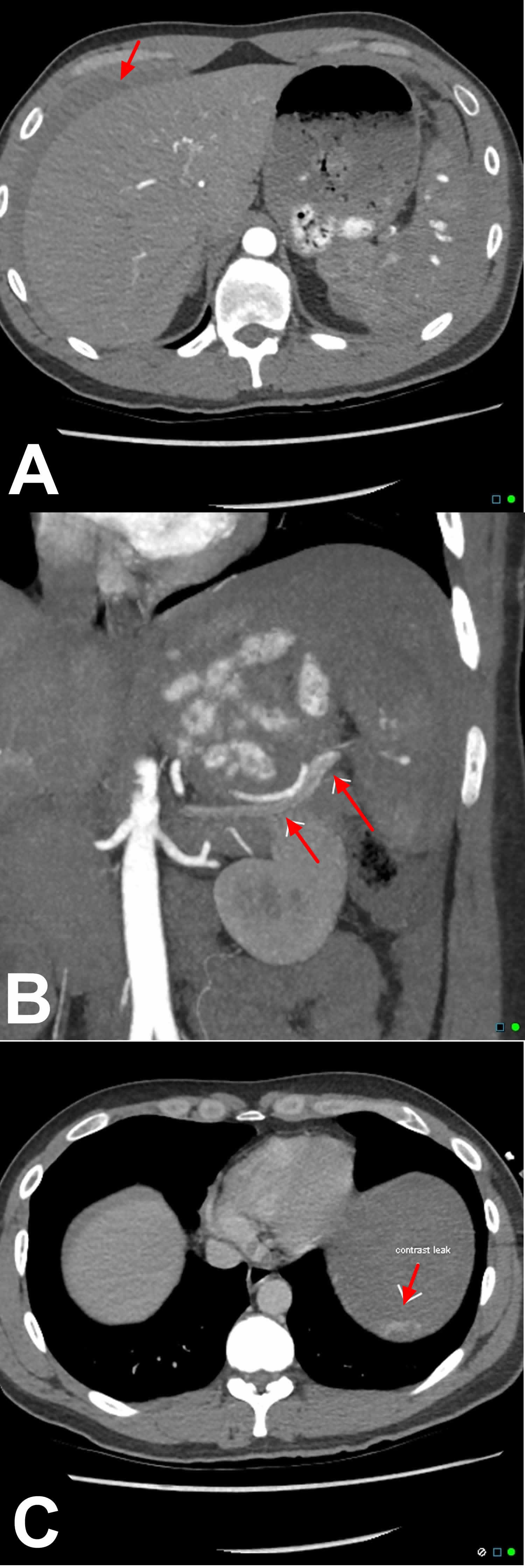
Footnotes: A 30 year old male who was assaulted 1 week prior to presentation. Managed conservatively, now sudden onset of severe left upper quardrant pain. Prominent perisplenic hematoma (sentinel clot) with marked liquid blood around the liver. Initial CT at the time of trauma shows a minor splenic laceration/contusion with minor sentinel clot and free blood around the liver. No contrast extravasation. Delayed splenic rupture typically occurs 7-10 days following the original injury due to lysis of clot on traumatised blood vessels. Note the multiple small punctate contrast pools on arterial phase CT due to multiple splenic pseudoaneurysms. This is the CT equivalent of the angiographic appearance termed ‘Seurat spleen’ because of a likeness to the pointillistic artwork of French impressionist Georges Seurat. There is also an associated traumatic A-V fistula characterized by early filling of the splenic vein on the arterial phase of the study. Note leak of contrast into the left subphrenic space indicating that there is active bleeding requiring urgent treatment (in this case splenectomy).
[Source 26 ]What is a spleen?
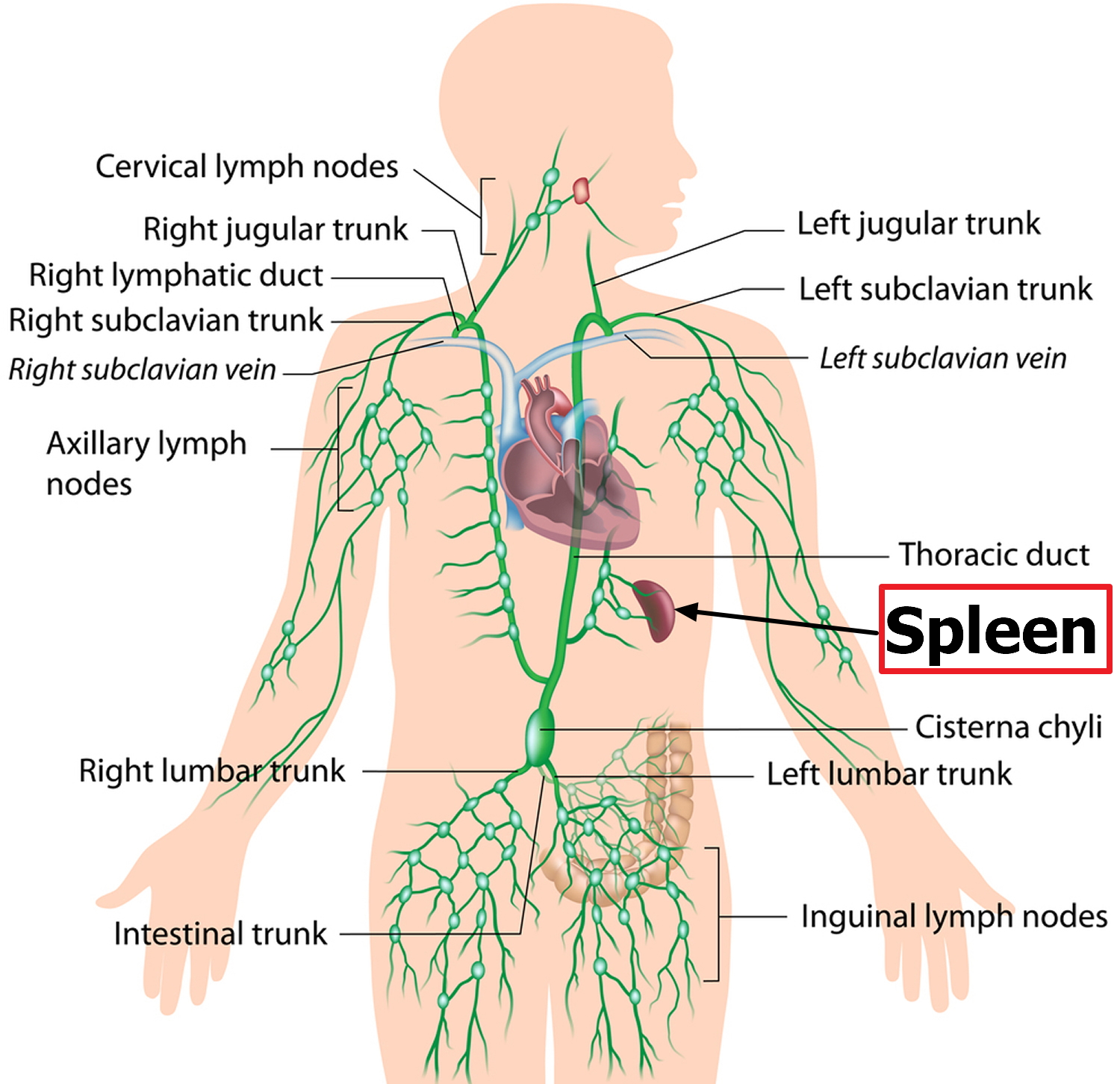
The spleen is the largest lymphoid organ and has a crucial function in the immune system. The spleen is responsible for the production and maturation of IgM, B lymphocytes, and opsonins 27. The spleen most importantly protects against infections from polysaccharide-encapsulated bacteria including Streptococcus pneumoniae, Haemophilus influenzae type B, Neisseria meningitidis, Escherichia coli, Salmonella, Klebsiella, and group B Streptococci (SHiNE SKiS) 27. The spleen also acts as the primary reservoir for platelets and as a filter for red blood cells (RBCs), removing damaged or malformed red blood cells from the circulation. In addition, the spleen performs extramedullary hematopoiesis.
The normal position of the spleen is within the peritoneal cavity in the left upper quadrant of the abdominal cavity adjacent to ribs nine through 12, just beneath the left diaphragm. The spleen lies behind and to the left side of your stomach (see Figure 4). The normal sized spleen abuts the stomach, colon, and left kidney. The spleen resembles a large lymph node and is subdivided into lobules (see Figure 6). However, unlike the lymphatic sinuses of a lymph node, the spaces in the spleen, called venous sinuses, are filled with blood instead of lymph.
A normal spleen ranges in length from 6 to 13 cm and in weight from 75 to 200 g 28. The spleen is not normally palpable except in slender young adults 28. When the spleen can be felt below the left costal (rib) margin, at rest or on inspiration, spleen enlargement should be assumed and the explanation sought. Although the normal-size or even the abnormally small, spleen can be involved in pathologic processes, with the exception of rubs associated with splenic infarcts, physical examination is generally not helpful in identifying the problem. Nevertheless, the enlarged and palpable spleen is an important clue to the presence of a variety of illnesses 28.
Figure 4. Spleen location
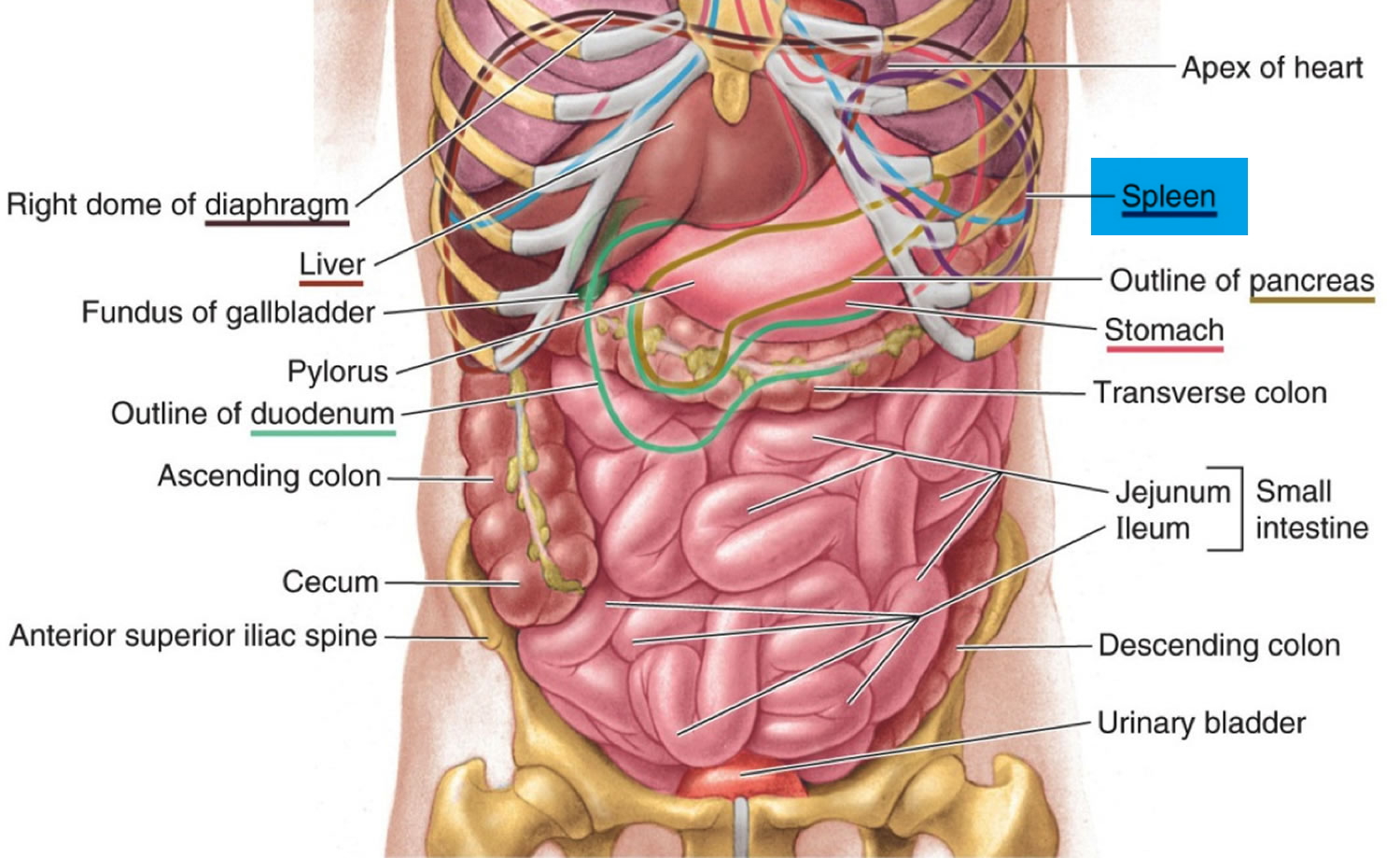
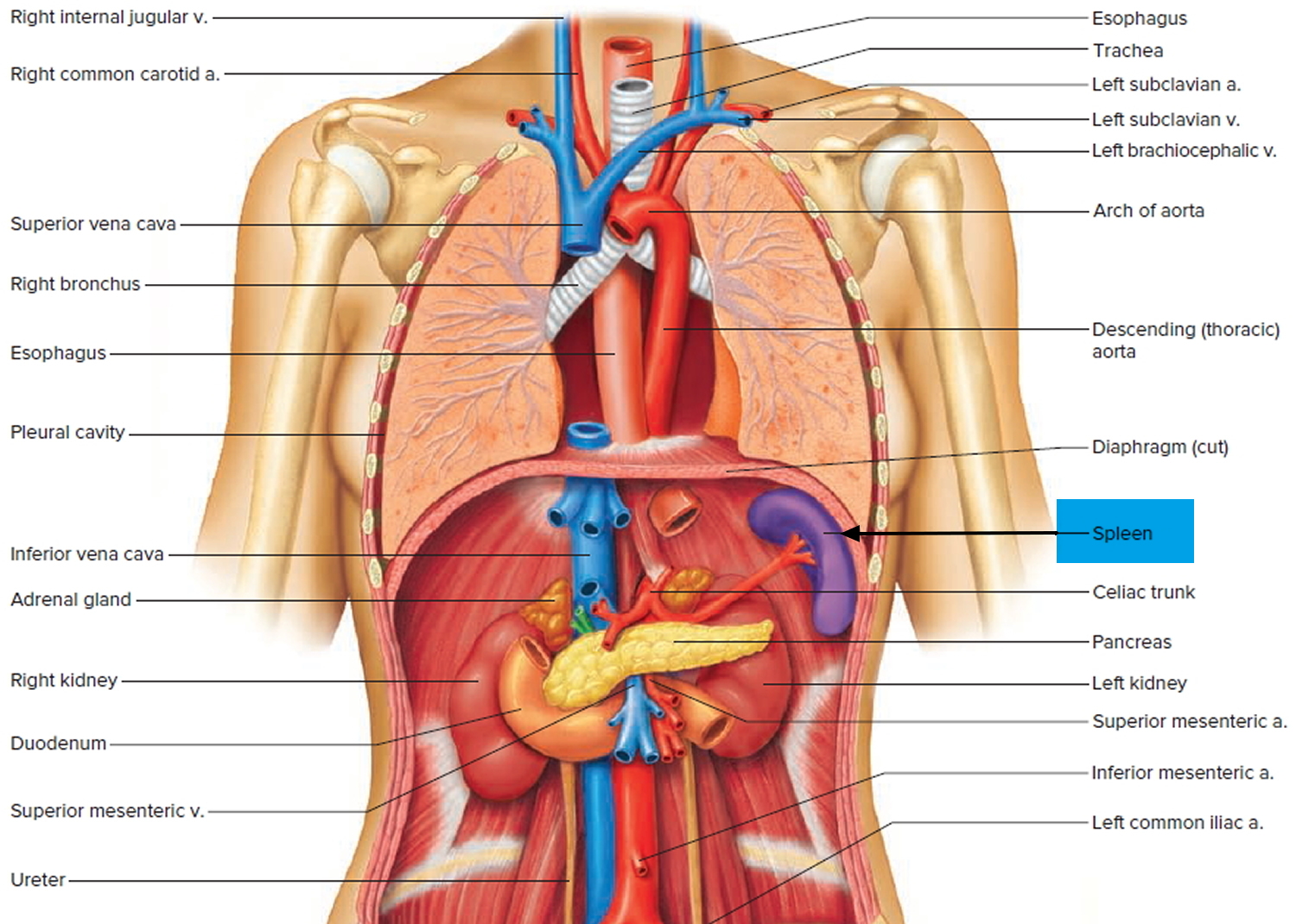
Figure 5. Spleen and the lymphatic system
What does the spleen do?
The spleen plays a significant role in hematopoiesis and immunosurveillance. The major functions of the spleen include clearance of abnormal erythrocytes, removal of microorganisms and antigens as well as the synthesis of immunoglobulin G (IgG). The spleen also synthesizes the immune system peptides properdin and tuftsin 29. Also, approximately one-third of circulating platelets are stored in the spleen.
The tissues within splenic lobules are of two types (see Figure 6). The white pulp is distributed throughout the spleen in tiny islands. This tissue is composed of splenic nodules, which are similar to the lymphatic nodules in lymph nodes and are packed with lymphocytes (T lymphocyte cells and B lymphocyte cells). The red pulp, which fills the remaining spaces of the lobules, surrounds the venous sinuses. This pulp contains numerous red blood cells, which impart its color, plus many lymphocytes and macrophages.
Without an immune system, a human being would be just as exposed to the harmful influences of pathogens or other substances from the outside environment as to changes harmful to health happening inside of the body. The main tasks of the body’s immune system are:
- Neutralizing pathogens like bacteria, viruses, parasites or fungi that have entered the body, and removing them from the body
- Recognizing and neutralizing harmful substances from the environment
- Fighting against the body’s own cells that have changed due to an illness, for example cancerous cells.
The normal adult spleen contributes to the homeostasis of the body by removing from the blood useless or potentially injurious materials (e.g., abnormal or “wornout” red blood cells and microorganisms) and by synthesizing immunoglobulins and properdin 28.
Figure 6. Spleen anatomy
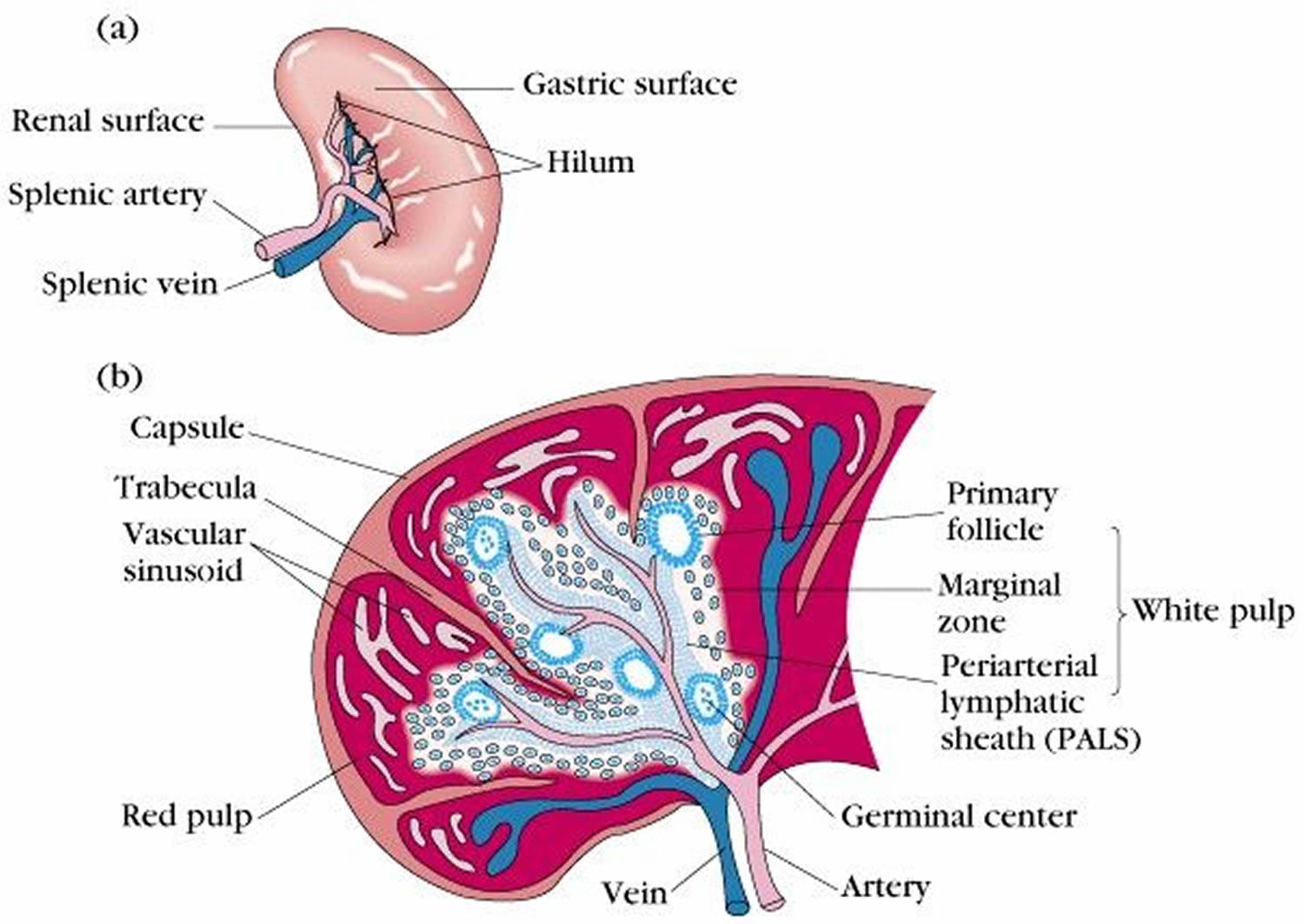
Blood capillaries in the red pulp are quite permeable. Red blood cells can squeeze through the pores in these capillary walls and enter the venous sinuses. The older, more fragile red blood cells may rupture during this passage, and the resulting cellular debris is removed by phagocytic macrophages in the venous sinuses. These macrophages also engulf and destroy foreign particles, such as bacteria, that may be carried in the blood as it flows through the venous sinuses. Thus, the spleen filters blood much as the lymph nodes filter lymph.
Phagocytosis removes foreign particles from the lymph as it moves from the interstitial spaces to the bloodstream. Phagocytes in the blood vessels and in the tissues of the spleen (and the liver and bone marrow) remove particles that reach the blood. Monocytes that leave the bloodstream by diapedesis become macrophages. These large cells may be free, or fixed in various tissues. The fixed macrophages can divide and produce new macrophages. Neutrophils, monocytes, and macrophages constitute the mononuclear phagocytic system (reticuloendothelial system).
Fever is body temperature elevated above an individual’s normal temperature due to an elevated setpoint. It is part of the innate defense because as a result of the fever the body becomes inhospitable to certain pathogens. Higher body temperature causes the spleen (and the liver) to sequester iron, which reduces the level of iron in the blood. Because bacteria and fungi require iron for normal metabolism, their growth and reproduction in a fever-ridden body slows and may cease. Also, phagocytic cells attack more vigorously when the temperature rises. For these reasons, low-grade fever of short duration may be a natural response to infection, not a treated symptom.
T Cells and the Cellular Immune Response
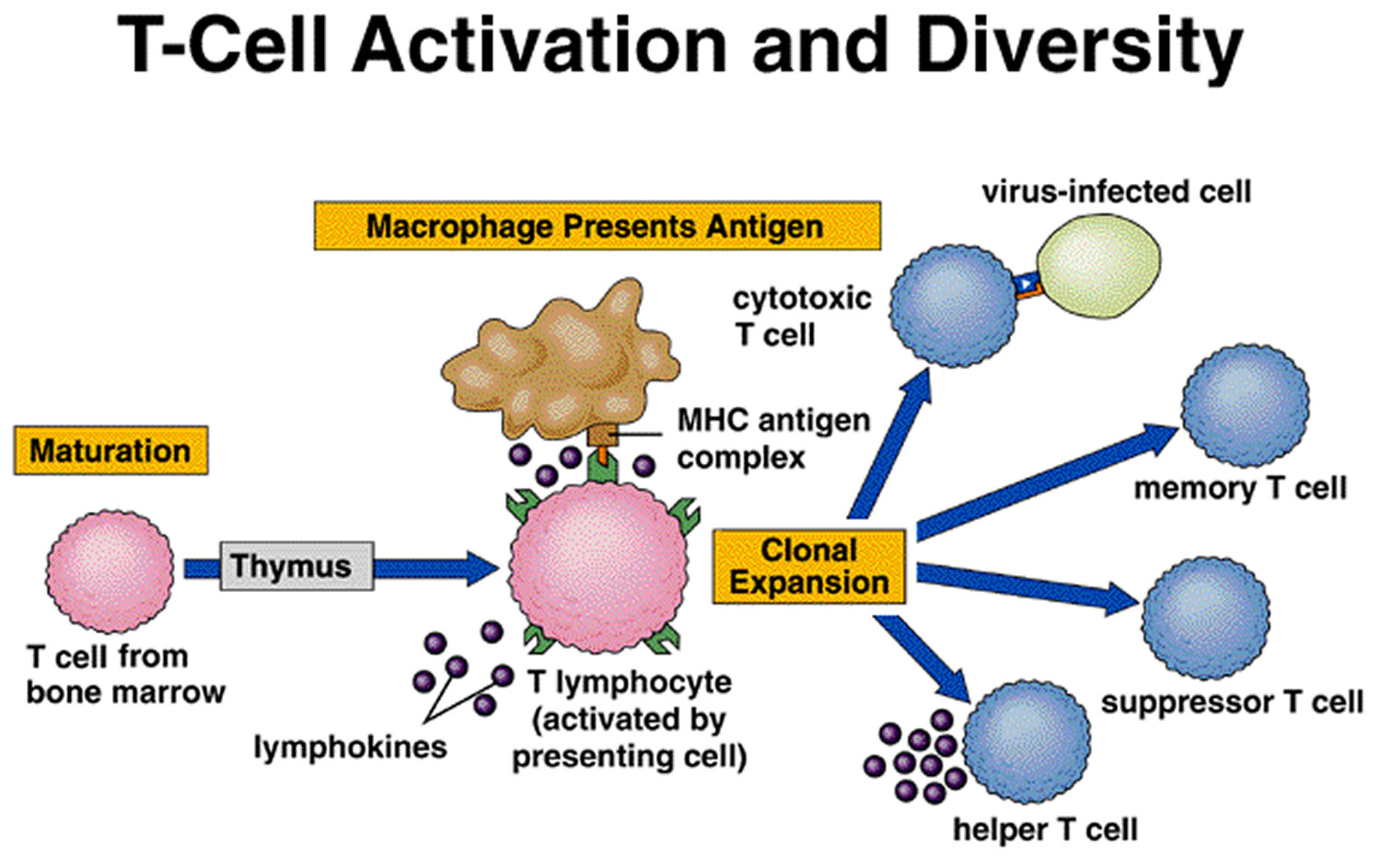
A lymphocyte must be activated before it can respond to an antigen. T cell activation requires that processed fragments of the antigen be attached to the surface of another type of cell, called an antigen-presenting cell (accessory cell). Macrophages, B cells, and several other cell types can be antigen-presenting cells.
T cell activation may occur when a macrophage phagocytizes a bacterium and digests it within a phagolysosome formed by the fusion of the vesicle containing the bacterium (phagosome) and a lysosome. Some of the resulting bacterial antigens are then displayed on the macrophage’s cell membrane near certain protein molecules that are part of a group of proteins called the major histocompatibility complex (MHC). MHC antigens help T cells recognize that a newly displayed antigen is foreign (nonself).
Activated T cells interact directly with antigen-bearing cells. Such cell-to-cell contact is called the cellular immune response, or cell-mediated immunity. T cells (and some macrophages) also synthesize and secrete polypeptides called cytokines that enhance certain cellular responses to antigens. For example, interleukin-1 and interleukin-2 stimulate the synthesis of several other cytokines from other T cells. Additionally, interleukin-1 helps activate T cells, whereas interleukin-2 causes T cells to proliferate. This proliferation increases the number of T cells in a clone, which is a group of genetically identical cells that descend from a single, original cell. Other cytokines, called colony stimulating factors (CSFs), stimulate leukocyte production in red bone marrow and activate macrophages. T cells may also secrete toxins that kill their antigen-bearing target cells, growth-inhibiting factors that prevent target cell growth, or interferon that inhibits the proliferation of viruses and tumor cells. Several types of T cells have distinct functions.
A specialized type of T cell, called a helper T cell, is activated when its antigen receptor combines with a displayed foreign antigen. Once activated, the helper T cell proliferates and the resulting cells stimulate B cells to produce antibodies that are specific for the displayed antigen.
Another type of T cell is a cytotoxic T cell, which recognizes and combines with nonself antigens that cancerous cells or virally infected cells display on their surfaces near certain MHC proteins. Cytokines from helper T cells activate the cytotoxic T cell. Next, the cytotoxic T cell proliferates. Cytotoxic T cells then bind to the surfaces of antigen-bearing cells, where they release perforin protein that cuts pore like openings in the cell membrane, destroying these cells. In this way, cytotoxic T cells continually monitor the body’s cells, recognizing and eliminating tumor cells and cells infected with viruses. Cytotoxic T cells provide much of the body’s defense against HIV infection.
Some cytotoxic T cells do not respond to a nonself antigen on first exposure, but remain as memory T cells that provide for future immune protection. Upon subsequent exposure to the same antigen, these memory cells immediately divide to yield more cytotoxic T cells and helper T cells, often before symptoms arise.
Figure 7. T-cell (T lymphocyte) activation
Steps in Antibody Production
T Cell (T Lymphocyte) Activities
- Antigen-bearing agents enter tissues.
- An accessory cell, such as a macrophage, phagocytizes the antigen-bearing agent, and the macrophage’s lysosomes digest the agent.
- Antigens from the digested antigen-bearing agents are displayed on the membrane of the accessory cell.
- Helper T cell becomes activated when it encounters a displayed antigen that fits its antigen receptors.
- Activated helper T cell releases cytokines when it encounters a B cell that has previously combined with an identical antigen-bearing agent.
- Cytokines stimulate the B cell to proliferate, enlarging its clone.
- Some of the newly formed B cells give rise to cells that differentiate into antibody-secreting plasma cells.
Figure 8. B (lymphocyte)-cell activation
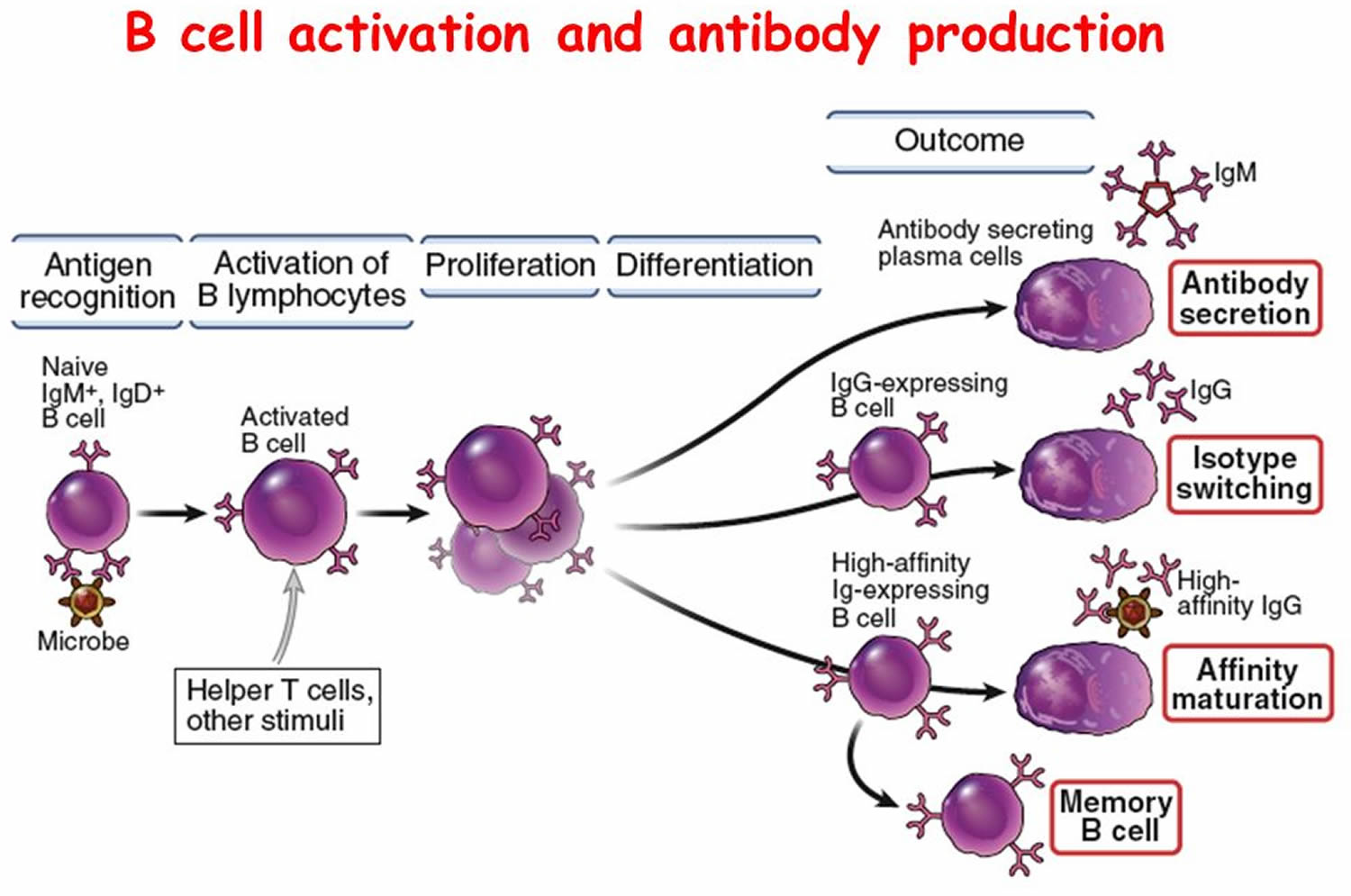
B Cell (B Lymphocyte) Activities
- Antigen-bearing agents enter tissues.
- B cell encounters an antigen that fits its antigen receptors.
- Either alone or more often in conjunction with helper T cells, the B cell is activated. The B cell proliferates, enlarging its clone.
- Some of the newly formed B cells differentiate further to become plasma cells.
- Plasma cells synthesize and secrete antibodies whose molecular structure is similar to the activated B cell’s antigen receptors.
Antibody Actions
In general, antibodies react to antigens in three ways. Antibodies directly attack antigens, activate complement, or stimulate localized changes (inflammation) that help prevent the spread of pathogens or cells bearing foreign antigens.
In a direct attack, antibodies combine with antigens, causing them to clump (agglutination) or to form insoluble substances (precipitation). Such actions make it easier for phagocytic cells to recognize and engulf the antigen-bearing agents and eliminate them. In other instances, antibodies cover the toxic portions of antigen molecules and neutralize their effects (neutralization). However, under normal conditions, direct antibody attack is not as important as complement activation in protecting against infection.
When certain IgG or IgM antibodies combine with antigens, they expose reactive sites on antibody molecules. This triggers a series of reactions, leading to activation of the complement proteins, which in turn produce a variety of effects. These include:
- coating the antigen-antibody complexes (opsonization), making the complexes more susceptible to phagocytosis;
- attracting macrophages and neutrophils into the region (chemotaxis);
- rupturing membranes of foreign cells (lysis); agglutination of antigen-bearing cells; and
- neutralization of viruses by altering their molecular structure, making them harmless.
Other proteins promote inflammation, which helps prevent the spread of infectious agents.
Immune Responses
Activation of B cells or T cells after they first encounter the antigens for which they are specialized to react constitutes a primary immune response. During such a response, plasma cells release antibodies (IgM, followed by IgG) into the lymph. The antibodies are transported to the blood and then throughout the body, where they help destroy antigen bearing agents. Production and release of antibodies continues for several weeks.
Following a primary immune response, some of the B cells produced during proliferation of the clone remain dormant as memory cells. If the same antigen is encountered again, the clones of these memory cells enlarge, and they can respond rapidly by producing IgG to the antigen to which they were previously sensitized. These memory B cells, along with the memory cytotoxic T cells, produce a secondary immune response.
As a result of a primary immune response, detectable concentrations of antibodies usually appear in the blood plasma five to ten days after exposure to antigens. If the same type of antigen is encountered later, a secondary immune response may produce the same antibodies within a day or two. Although newly formed antibodies may persist in the body for only a few months or years, memory cells live much longer.
Naturally acquired active immunity occurs when a person exposed to a pathogen develops a disease. Resistance to that pathogen is the result of a primary immune response.
A vaccine is a preparation that produces artificially acquired active immunity. A vaccine might consist of bacteria or viruses that have been killed or weakened so that they cannot cause a serious infection, or only molecules unique to the pathogens. A vaccine might also be a toxoid, which is a toxin from an infectious organism that has been chemically altered to destroy its dangerous effects. Whatever its composition, a vaccine includes the antigens that stimulate a primary immune response, but does not produce symptoms of disease and the associated infections.
Specific vaccines stimulate active immunity against a variety of diseases, including typhoid fever, cholera, whooping cough, diphtheria, tetanus, polio, chickenpox, measles (rubeola), German measles (rubella), mumps, influenza, hepatitis A, hepatitis B, and bacterial pneumonia. A vaccine has eliminated naturally acquired smallpox from the world.
Ruptured spleen causes
A spleen can rupture due to:
- Trauma: The most common cause of ruptured spleen is blunt force trauma to the abdomen or the left lower chest, such as from a car accident, a fall, fistfights, a sports injury (like from football or hockey), or a blow to the left side of the body. An injured spleen can rupture soon after the stomach trauma or, in some cases, days or weeks after the injury.
- Four types of splenic injuries are recognized: intraparenchymal laceration, subcapsular hematoma, and splenic rupture and delayed rupture 5.
- An enlarged spleen. Your spleen can become enlarged when blood cells accumulate in the spleen. An enlarged spleen can be caused by various underlying problems, such as mononucleosis and other infections, liver disease, and blood cancers:
- Viral infections, such as mononucleosis
- Bacterial infections, such as syphilis or an infection of your heart’s inner lining (endocarditis)
- Parasitic infections, such as malaria
- Cirrhosis and other diseases affecting the liver
- Various types of hemolytic anemia — a condition characterized by early destruction of red blood cells
- Blood cancers, such as leukemia and myeloproliferative neoplasms, and lymphomas, such as Hodgkin’s disease
- Metabolic disorders, such as Gaucher disease and Niemann-Pick disease
- Pressure on the veins in the spleen or liver or a blood clot in these veins
- Autoimmune conditions, such as lupus or sarcoidosi
- Spontaneous rupture: In rare cases, spleen rupture can occur spontaneously without a known injury 6, 7. Malaria is a known risk factor for spontaneous splenic rupture, particularly in individuals staying in endemic areas or returning travelers presenting with splenomegaly 8, 9. Atraumatic splenic rupture may also result from pancreatitis.
Splenic rupture predominantly affects male individuals, with a 2:1 ratio, most commonly between the ages of 18 and 34. Blunt abdominal trauma, particularly from motor vehicle collisions, is the leading cause comprising 50% to 75% of cases. Contact sports such as football, hockey, cycling, and equestrian activities increase the risk of splenic injury. Military training and occupational accidents have also been identified as contributing factors.
Nontraumatic rupture is rare but may occur in individuals with underlying disease or following minor trauma, especially in the presence of enlarged spleen (splenomegaly) 30, 31. Nontraumatic rupture most commonly results from cancers, tumors or infections, each accounting for 30% of cases. Infectious mononucleosis is a well-recognized example, leading to rupture in approximately 0.1% of cases 32. In regions where malaria and typhoid fever are endemic, chronic infection may lead to splenomegaly (enlarged spleen) and elevate the risk of spontaneous rupture. Immunocompromised individuals, including those with hematologic malignancies or solid organ transplants, may be predisposed to splenic rupture either spontaneously or following minimal trauma. Nontraumatic rupture is rare but carries a mortality rate of approximately 12% and is frequently associated with underlying pathology.
Inflammatory diseases contribute to 15% of splenic rupture cases, while medications or medical treatments account for 10%. Mechanical factors and idiopathic cases each represent about 7% 33. Medications implicated in nontraumatic splenic rupture include anticoagulants, thrombolytics, and agents used to treat blood cancers. Inflammatory or infectious processes increase splenic friability, rendering the organ susceptible to rupture from mild physiologic strain such as coughing, vomiting, or defecation.
Table 1. Spleen injury scale
| Grade* | Injury type | Description of injury |
|---|---|---|
| 1 | Hematoma | Subcapsular, <10% surface area |
| Laceration | Capsular tear, <1cm | |
| Parenchymal depth | ||
| 2 | Hematoma | Subcapsular, 10%-50% surface area |
| Intraparenchymal, <5 cm in diameter | ||
| Laceration | Capsular tear, 1-3cm parenchymal depth that does not involve a trabecular vessel | |
| 3 | Hematoma | Subcapsular, >50% surface area or expanding; ruptured subcapsular or parecymal hematoma; intraparenchymal hematoma > 5 cm or expanding |
| Laceration | >3 cm parenchymal depth or involving trabecular vessels | |
| 4 | Laceration | Laceration involving segmental or hilar vessels producing major devascularization (>25% of spleen) |
| 5 | Laceration | Completely shattered spleen |
| Vascular | Hilar vascular injury with devascularizes spleen |
Footnotes: Spleen injury scale (1994 revision). *Advance one grade for multiple injuries up to grade 3.
[Source 10 ]Risk factors for ruptured spleen
If your spleen is already enlarged due to infection or another cause such as liver disease or blood cancers, there is increased risk that your spleen might rupture. If you have an enlarged spleen, a less forceful trauma might cause rupture. Contact sports that involve blows to your chest also increase your risk of a ruptured spleen.
If you’ve been diagnosed with an enlarged spleen, ask your doctor whether you need to avoid physical activities for several weeks that could cause it to rupture. These might include contact sports, heavy lifting and other activities that might increase your risk of stomach trauma.
Ruptured spleen signs and symptoms
Signs and symptoms of a ruptured spleen may include:
- Pain in the upper left stomach.
- Tenderness when you touch the upper left stomach.
- Left shoulder pain.
- Dizziness or lightheadedness.
- Mental confusion or disorientation.
- Blurred vision.
- Paleness and faintness.
- Restlessness or anxiety.
- Nausea.
- Rapid heart rate (tachycardia).
- Rapid breathing (tachypnea).
A ruptured spleen is a medical emergency. Seek emergency care after an injury if your signs and symptoms indicate that you may have a ruptured spleen.
The signs and symptoms of splenic injury is highly variable. Most patients with minor focal injury to the spleen complain of left upper quadrant abdominal tenderness 34. Left shoulder tenderness or Kehr sign may also be present as a result of subdiaphragmatic nerve root irritation with referred pain.
With free intraperitoneal blood, diffuse abdominal pain, peritoneal irritation, and rebound tenderness are more likely. If the intra-abdominal bleeding exceeds 5-10% of blood volume, clinical signs of early shock may manifest. Signs include rapid heart rate (tachycardia), rapid breathing (tachypnea), restlessness, and anxiety. Patients may have a mild pallor noted only by friends and family. Clinical signs include decreased capillary refill and decreased pulse pressure. With increasing blood loss into the abdominal cavity, abdominal distension, peritoneal signs, and overt shock may be observed.
Low blood pressure (hypotension) in a patient with a suspected splenic injury, especially if young and previously healthy, is a grave sign and a surgical emergency. This should prompt immediate evaluation and intervention either in the operating room or interventional radiology if a state of compensated shock can be maintained. Unstable patients have nearly exsanguinated in CT scanners while in the process of documenting splenic injury, when they would have been better served by exploration in the operating room or embolization in the interventional radiology suite.
Ruptured spleen complications
Splenic rupture carries the risk of both immediate and delayed complications, particularly when diagnosis or intervention is delayed. Hemorrhagic shock (a life-threatening condition caused by significant blood loss that leads to a drop in blood volume, causing inadequate oxygen delivery to the body’s tissues) from uncontrolled intra-abdominal bleeding is the most serious acute complication 1. Delayed splenic rupture and rebleeding may occur even in initially stable patients, most often within 7 to 10 days following injury 1. Delayed splenic rupture or bleeding is very serious due to its high mortality rate, reported at 15% in adult cases 23. This risk increases with higher-grade injuries and highlights the importance of close monitoring throughout the observation period.
Splenic rupture typically occurs 48 to 72 hours after injuries in cases diagnosed as delayed splenic rupture 35. However, Jen et al 17 described four cases of delayed splenic rupture that occurred 4 to 20 days post-injury. Davis et al 22 reviewed cases of delayed splenic bleeding and found that they occurred 2 to 28 days post-injury. Some cases occur after discharge from the hospital. It is very important to know the warning signs of delayed splenic rupture or bleeding following a splenic injury 36, 22. Patients with symptoms of increased pain, pallor, dizziness, vomiting, and worsening shoulder pain must return to the hospital 36.
In patients managed nonoperatively, potential complications include expanding hematomas, persistent abdominal pain, and formation of vascular lesions such as pseudoaneurysms (blood-filled sacs that forms outside an artery due to injury to the vessel wall) or arteriovenous fistulae (abnormal connections between arteries and veins) 1. Pseudoaneurysms may develop several days after the initial injury and pose a risk for delayed rupture. Repeat imaging may be indicated if clinical status changes or initial imaging demonstrates high-grade injury or active contrast extravasation.
Additional complications of splenic rupture include left-sided pleural effusion, subphrenic abscess, pancreatitis due to adjacent inflammation or ischemia, and iatrogenic injury during diagnostic or therapeutic interventions. Optimal outcomes depend on close coordination among trauma surgeons, radiologists, critical care specialists, and primary care providers to minimize preventable complications and ensure appropriate long-term follow-up.
Ruptured spleen diagnosis
Tests and procedures used to diagnose a ruptured spleen include:
- Physical exam. Your doctor will press on your abdomen to determine the size of your spleen and whether it’s tender.
- Blood tests. Blood tests will evaluate factors such as platelet count and how well your blood clots.
- Checking for blood in your abdominal cavity. In emergency situations, your doctor might either use a special bedside ultrasound called Focused Assessment with Sonography for Trauma (FAST) ultrasound or draw a sample of fluid from your stomach with a needle. If the sample reveals blood in your stomach, you might be referred for emergency surgery. Focused Assessment with Sonography for Trauma (FAST) ultrasound cannot reliably identify pseudoaneurysms or early parenchymal injury.
- Imaging tests of your stomach. Computed tomography (CT) with intravenous contrast remains the gold standard for evaluating hemodynamically stable patients, offering detailed visualization of the splenic parenchyma, vascular integrity, and associated intra-abdominal injuries 37, 38. If your diagnosis isn’t clear, your doctor might recommend a CT scan of the stomach, possibly with contrast dye, or another imaging test to look for other possible causes of your symptoms.
Ruptured spleen differential diagnosis
Splenic rupture may mimic or overlap with various intra-abdominal and thoracic pathologies, necessitating careful diagnostic evaluation.
- Genitourinary trauma: Injuries to the bladder, ureters, or kidneys may present with hematuria, flank pain, or lower abdominal tenderness. CT urogram may be necessary for evaluation.
- Hollow viscus injury: Perforation of the stomach, small intestine, or colon may present with peritonitis, free intraperitoneal air, or sepsis. CT with oral contrast can assist in diagnosis.
- Mesenteric injury: Often subtle initially, these injuries may lead to delayed bleeding, bowel ischemia, or mesenteric hematoma. CT imaging may show mesenteric stranding or active extravasation.
- Gastric or duodenal ulcer perforation: May present with acute abdominal pain, free fluid, or subdiaphragmatic free air. History of nonsteroidal anti-inflammatory drug use or known peptic ulcer disease provides diagnostic context.
- Acute coronary syndrome: In older adults, this condition may mimic intra-abdominal pathology, presenting with epigastric discomfort, hypotension, or referred shoulder pain.
- Musculoskeletal injury: Rib fractures, abdominal wall hematomas, and costochondritis can produce localized pain that resembles splenic injury, particularly after trauma.
- Retroperitoneal hemorrhage: Often due to vascular injury or anticoagulation, this condition may present with flank ecchymosis (Grey Turner sign), hypotension, and abdominal distension.
- Diaphragmatic rupture: Typically results from blunt trauma and may lead to bowel herniation into the thoracic cavity. Chest radiography or CT may show an elevated hemidiaphragm or intrathoracic bowel loops.
- Pancreatic injury: Often related to high-velocity trauma, this injury may present with midabdominal pain, elevated pancreatic enzymes, or retroperitoneal fluid.
- Splenic infarction: Usually presents with left upper quadrant pain in patients with sickle cell disease, hypercoagulable states, or embolic conditions. CT typically reveals wedge-shaped hypodense regions.
Accurate distinction among potential mimics of splenic injury is critical for initiating condition-specific management. Imaging, clinical context, and hemodynamic status guide diagnostic clarity.
Ruptured spleen treatment
Your treatment for a ruptured spleen will depend on the seriousness of your condition. Severe injuries usually require immediate surgery. However, a severe spleen injury might not be immediately obvious.
If your condition is stable (your blood pressure and heart rate are close to normal) your emergency doctor will examine you in a stepwise fashion, beginning with a physical exam and then progressing to imaging tests. If you’re in the emergency room with a traumatic injury, your doctor will begin with a special bedside ultrasound (Focused Assessment with Sonography for Trauma (FAST) ultrasound) that looks for internal bleeding in your abdomen.
If your Focused Assessment with Sonography for Trauma (FAST) ultrasound is positive and your vital signs remain unstable, your doctor will know that you have a ruptured spleen and need immediate treatment. If your condition is stable but your doctor suspects a splenic injury, they will often proceed with a CT scan to get a better look at your spleen and the extent of the injury. They will grade the injury on a scale of 1 (I) to 5 (V) (see Table 1). Some minor tears to the spleen might stop bleeding on their own, while others may require various types of emergency repairs. Only the most severe (grade 5) ruptures require spleen removal (splenectomy). Surgical management should be pursued in the setting of hemodynamic instability, transfusion requirements exceeding 40 mL/kg within 24 to 48 hours, or clinical signs of peritonitis.
Many small or moderate-sized injuries to the spleen can heal without surgery. You’re likely to stay in the hospital while your doctor observe your condition and provide nonsurgical care, such as blood transfusions, if necessary. Sometimes, a stable patient becomes unstable several hours later as the bleeding progresses. Delayed splenic rupture may occur 24 to 48 hours after initial trauma. Ongoing monitoring is warranted even in stable patients 25. You might have periodic follow-up CT scans to check whether your spleen has healed or to determine whether you need surgery. Patients with symptoms of increased pain, pallor, dizziness, vomiting, and worsening shoulder pain must return to the hospital 36.
Splenic artery embolization
For grade 3 and 4 spleen injuries, splenic artery embolization can help manage the bleeding prior to or instead of surgery. Splenic artery embolization is a non-surgical procedure that’s performed by an interventional radiologist. Splenic artery embolization uses radiology imaging techniques to guide a catheter into your blood vessel and inject tiny, sponge-like beads into it to stop the blood flow the entire organ or distally to occlude specific bleeding vessels. Indications for splenic artery embolization include active contrast extravasation (contrast blush) on CT, pseudoaneurysm, arteriovenous fistula, and high-grade injury with hemoperitoneum. Splenic artery embolization is particularly valuable in hemodynamically stable patients at increased risk for delayed bleeding or failure of nonoperative management. Proximal embolization offers shorter procedural times and reduced contrast use, whereas distal embolization allows for greater tissue preservation. Access for embolization may be obtained via the femoral or radial artery 39.
Patients who undergo splenic artery embolization may experience complications such as splenic infarction, abscess formation, coil migration, and rebleeding. Distal embolization, or the combination of proximal and distal techniques, increases the risk of infarction. Most infarcts are clinically silent. However, extensive devascularization may lead to secondary infection or necessitate surgical intervention.
Surgery
Surgical management is indicated in cases of persistent hemodynamic instability, signs of peritonitis, expanding intra-abdominal hematoma, or failure of nonoperative treatment 1. Exploratory laparotomy remains the standard surgical approach 1. When appropriate, splenic preservation techniques such as splenorrhaphy, partial splenectomy, or topical hemostatic agents may be employed 1. In cases involving extensive splenic parenchymal disruption or uncontrolled hemorrhage, splenectomy is frequently required and may be life-saving 1.
Intraoperatively, careful dissection is required to control hilar vessels while avoiding injury to adjacent structures such as the tail of the pancreas. Patients undergoing splenectomy should receive appropriate vaccinations prior to discharge or within 14 days postoperatively to reduce the risk of overwhelming post-splenectomy infection (OPSI). Postsplenectomy complications include early postoperative infections, wound-related issues, and long-term susceptibility to overwhelming post-splenectomy infection (OPSI), a serious disease that can progress from a mild flu-like illness to fulminant sepsis in a short time period, particularly from encapsulated organisms 40, 41, 42, 43. Recommended immunizations include vaccines against Streptococcus pneumoniae (PCV13 or PCV20), Haemophilus influenzae type b, and Neisseria meningitidis. Annual influenza vaccination is also advised. In children and select high-risk adults, antibiotic prophylaxis with penicillin or amoxicillin may be continued for up to 5 years or longer, depending on immune function and clinical judgment 44.
An increased incidence of thromboembolic events, including deep vein thrombosis (DVT) and pulmonary embolism (PE), has also been documented. In children and immunocompromised individuals, lifelong infection prophylaxis may be appropriate based on clinical judgment.
Surgery for a ruptured spleen can include:
- Repairing the spleen (splenorrhaphy). Your surgeon might be able to use stitches to repair the rupture or electrocautery to close the wound or applying topical agents to the wound to stop the bleeding.
- Removing the spleen called a splenectomy. When severe bleeding can’t be controlled and your spleen can’t be preserved by any other means, it may be necessary to remove part or all of your spleen. Only about 20% of spleen ruptures end this way. Since this is an emergency operation, it’s likely to be an open abdominal surgery. This gives your surgeon the best access to manage your urgent condition.
- You can live without your spleen, but it increases your risk of serious bacterial infections such as sepsis. Since your spleen plays an important role in protecting against infections, you may be more prone to getting sick after a splenectomy. Your doctor may recommend vaccinations against meningitis, pneumonia and haemophilus influenza, type b (Hib). Occasionally, you may be prescribed daily oral antibiotics to prevent infections. Your doctor will also advise you to treat infections immediately with antibiotics if you do get sick.
- Removing part of the spleen called partial splenectomy. It might be possible to remove only part of your spleen, depending on the rupture. Partial splenectomy reduces the risk of infection that results from removing your entire spleen.
Spleen surgery is generally safe, but any surgery has risks, such as bleeding, blood clots, infection and pneumonia.
Ruptured spleen prognosis
Your prognosis or outcome depends depends on several factors that include how severe your injury is, your hemodynamic status at presentation, the presence of other injuries, and availability of advanced trauma care and how quickly your ruptured spleen gets diagnosed and treated 1. A minor splenic rupture may only cause a small, slow bleed. This gives you more time, but it also makes it easier to overlook. A more severe bleed will usually be obvious in terms of your symptoms, but it’s more dangerous. Severe internal bleeding can cause death within hours if it isn’t treated right away. The mortality (death) rate from simple splenic rupture is 1% 2. Delayed diagnosis of a ruptured spleen increases the rate to 10% 2. Splenic rupture mortality (death) is most strongly associated with severe loss of blood from uncontrolled hemorrhage and the presence of accompanying injuries, particularly traumatic brain injury or multiple trauma. The overall mortality rate for isolated splenic injury remains low when modern trauma protocols are applied. Prognosis for splenic rupture has improved substantially due to advancements in imaging, resuscitation, and interprofessional trauma care. Optimal outcomes are achieved when management is individualized based on clinical presentation, imaging findings, and institutional resources.
Hemodynamically stable patients with low-grade spleen injuries (American Association for the Surgery of Trauma grades 1 and 2) managed nonoperatively typically experience excellent outcomes, with high rates of splenic preservation and minimal long-term complications 1. Favorable outcomes can also be achieved in select patients with high-grade injuries (American Association for the Surgery of Trauma grades 3 to 5) when treated at centers equipped with interventional radiology and intensive monitoring 1.
Timely diagnosis and appropriate triage are essential to reduce morbidity and mortality 1. Delays in recognizing splenic rupture or failure to stabilize unstable patients increase the risk of poor outcomes.
Patients who undergo splenectomy face an increased long-term risk of serious bacterial infections from encapsulated organisms and may require lifelong preventive measures. Adherence to vaccination protocols and education regarding infection risk reduces this vulnerability. Some studies have also reported elevated risks of thromboembolism (obstruction of a blood vessel by a blood clot that has become dislodged from another site in the circulation) and certain cancers after splenectomy, although the causal relationship remains uncertain. Splenic artery embolization offers partial preservation of immune function and is associated with fewer infectious complications compared to splenectomy.
How long does it take to recover from a ruptured spleen?
Depending on the extent of your injury and treatment, it may take anywhere from 3 to 12 weeks to recover. If you have surgery, you’ll probably remain in the hospital for a few days afterward. Open abdominal surgery leaves you with a long incision wound to heal from. You may have a prescription for pain medication to take home. On the other hand, minor spleen injuries heal relatively quickly.
- Wang CF, Launico MV. Splenic Rupture. [Updated 2025 Aug 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK525951[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- “Delayed rupture of the spleen” or delayed diagnosis of the splenic injury ? Isr J Med Sci. 1980 Sep-Oct;16(9-10):659-64. https://www.ncbi.nlm.nih.gov/pubmed/7429801[↩][↩][↩][↩]
- Blunt Splenic Trauma. American Association for the Surgery of Trauma. http://www.aast.org/GeneralInformation/BluntSplenicTrauma.aspx[↩][↩]
- Olsen WR, Polley TZ Jr. A Second Look at Delayed Splenic Rupture. Arch Surg. 1977;112(4):422–425. doi: 10.1001/archsurg.1977.01370040074012. https://www.ncbi.nlm.nih.gov/pubmed/849149[↩]
- Horgan GI. The paediatric Liver and Spleen. In: Rumack CR, Wilson SR, Charboneau J William, editors. Diagnostic ultrasound. Volume 2. Vol. 59. Mosby year Book; 1991. pp. 1175–1176.[↩][↩]
- Systematic review of atraumatic splenic rupture. Renzulli P, Hostettler A, Schoepfer AM, Gloor B, Candinas D. Br J Surg. 2009 Oct; 96(10):1114-21. https://www.ncbi.nlm.nih.gov/pubmed/19787754/[↩][↩]
- Debnath D, Valerio D. Atraumatic rupture of the spleen in adults. J R Coll Surg Edinb. 2002;47:437–445. https://www.ncbi.nlm.nih.gov/pubmed/11874265[↩][↩]
- Moya Sánchez E, Medina Benítez A. Atraumatic splenic rupture as a complication of acute exacerbation of chronic pancreatitis, an unusual disease. Rev Esp Enferm Dig. 2017 Jun;109(6):477-478. doi: 10.17235/reed.2017.4597/2016[↩][↩]
- Zidouh S, Jidane S, Belkouch A, Bekkali H, Belyamani L. Spontaneous splenic rupture from Plasmodium ovalae malaria. Am J Emerg Med. 2017 Feb;35(2):347-349. doi: 10.1016/j.ajem.2016.10.024[↩][↩]
- Spleen injury scale (1994 revision). American Association for the Surgery of Trauma. https://www.aast.org/trauma-acs-resources/trauma-tools/injury-scoring-scale.html[↩][↩]
- Söyüncü S, Bektaş F, Cete Y. Traditional Kehr’s sign: Left shoulder pain related to splenic abscess. Ulus Travma Acil Cerrahi Derg. 2012 Jan;18(1):87-8. doi: 10.5505/tjtes.2011.04874[↩]
- Oh JS, Mentzer CJ, Abuzeid AM, Holsten SB. Delayed Splenic Rupture with Normal Admission CT Scan after Blunt Trauma. Am Surg. 2016 Aug;82(8):e223-4.[↩]
- Delayed splenic rupture: understanding the threat. J Trauma Nurs. 2002 Apr-Jun;9(2):34-40. https://www.ncbi.nlm.nih.gov/pubmed/15997614[↩]
- Conservative management of ruptured spleen. S Afr Med J. 1980 Apr 19;57(16):655-8. https://www.ncbi.nlm.nih.gov/pubmed/7376031[↩]
- Stylianos S. Evidence-based guidelines for resource utilization in children with isolated spleen or liver injury. The APSA Trauma Committee. J Pediatr Surg. 2000 Feb;35(2):164-7; discussion 167-9. doi: 10.1016/s0022-3468(00)90003-4[↩]
- Daodu O, Brindle M, Alvarez-Allende CR, Lockyer L, Weber B, Lopushinsky SR. Outcomes of an accelerated care pathway for pediatric blunt solid organ injuries in a public healthcare system. J Pediatr Surg. 2017 May;52(5):826-831. doi: 10.1016/j.jpedsurg.2017.01.037[↩]
- Jen HC, Tillou A, Cryer HG 3rd, Shew SB. Disparity in management and long-term outcomes of pediatric splenic injury in California. Ann Surg. 2010 Jun;251(6):1162-6. doi: 10.1097/SLA.0b013e3181c98271[↩][↩][↩]
- Martin K, Vanhouwelingen L, Bütter A. The significance of pseudoaneurysms in the nonoperative management of pediatric blunt splenic trauma. J Pediatr Surg. 2011 May;46(5):933-7. doi: 10.1016/j.jpedsurg.2011.02.031[↩][↩]
- Notrica DM, Sayrs LW, Bhatia A, Letton RW, Alder A, St Peter S, Ponsky TA, Eubanks JW 3rd, Lawson KA, Ostlie DJ, Tuggle DW, Garcia NM, Maxson RT, Leys C, Greenwell C. The incidence of delayed splenic bleeding in pediatric blunt trauma. J Pediatr Surg. 2018 Feb;53(2):339-343. doi: 10.1016/j.jpedsurg.2017.10.005[↩][↩]
- Maurer SV, Denys A, Lutz N. Successful embolization of delayed splenic rupture following trauma in a child. J Pediatr Surg. 2009;44:E1–E4. doi: 10.1016/j.jpedsurg.2009.02.070[↩]
- Lynn KN, Werder GM, Callaghan RM, et al. Pediatric blunt splenic trauma: a comprehensive review. Pediatr Radiol. 2009;39:904–916. doi: 10.1007/s00247-009-1336-0[↩]
- Davis DA, Fecteau A, Himidan S, et al. What’s the incidence of delayed splenic bleeding in children after blunt trauma? An institutional experience and review of the literature. J Trauma. 2009;67:573–577. doi: 10.1097/TA.0b013e318190392b[↩][↩][↩][↩]
- Jahromi AH, Migliaro M, Romano M, et al. Delayed splenic rupture; normal appearing spleen on the initial multidetector computed tomography (MDCT) can sometimes be misleading. Trauma Mon. 2016;21:e24465. doi: 10.5812/traumamon.24465[↩][↩]
- Scarborough JE, Ingraham AM, Liepert AE, Jung HS, O’Rourke AP, Agarwal SK. Nonoperative Management Is as Effective as Immediate Splenectomy for Adult Patients with High-Grade Blunt Splenic Injury. J Am Coll Surg. 2016 Aug;223(2):249-58. doi: 10.1016/j.jamcollsurg.2016.03.043[↩][↩][↩]
- Shinkai T, Ono K, Masumoto K, Urita Y, Gotoh C. A rare mechanism of delayed splenic rupture following the nonoperative management of blunt splenic injury in a child. Surg Case Rep. 2018 Jul 11;4(1):75. doi: 10.1186/s40792-018-0477-5[↩][↩]
- Delayed rupture of the spleen – traumatic pseudoaneurysms and A-V fistula. https://radiopaedia.org/cases/delayed-rupture-of-the-spleen-traumatic-pseudoaneurysms-and-a-v-fistula-1?lang=us [↩]
- Hijazi LS, Mead T. Functional Asplenism. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499949[↩][↩]
- Armitage JO. Spleen. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Chapter 150. Available from: https://www.ncbi.nlm.nih.gov/books/NBK258/[↩][↩][↩][↩]
- Chapman J, Bhimji SS. Splenomegaly. [Updated 2017 May 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2017 Jun-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430907/[↩]
- Khan RN, Jindal V. Systematic review of atraumatic splenic rupture (Br J Surg 2009; 96: 1114-1121). Br J Surg. 2010 Apr;97(4):616; author reply 616-7. doi: 10.1002/bjs.7052[↩]
- Debnath D, Valerio D. Atraumatic rupture of the spleen in adults. J R Coll Surg Edinb. 2002 Feb;47(1):437-45.[↩]
- Kocael PC, Simsek O, Bilgin IA, Tutar O, Saribeyoglu K, Pekmezci S, Goksoy E. Characteristics of patients with spontaneous splenic rupture. Int Surg. 2014 Nov-Dec;99(6):714-8. doi: 10.9738/INTSURG-D-14-00143.1[↩]
- Clancy AA, Tiruta C, Ashman D, Ball CG, Kirkpatrick AW. The song remains the same although the instruments are changing: complications following selective non-operative management of blunt spleen trauma: a retrospective review of patients at a level I trauma centre from 1996 to 2007. J Trauma Manag Outcomes. 2012 Mar 13;6(1):4. doi: 10.1186/1752-2897-6-4[↩]
- Splenic Rupture. https://emedicine.medscape.com/article/432823-overview#a10[↩]
- Resteghini N, Nielsen J, Hoimes ML, et al. Delayed splenic rupture presenting 70 days following blunt abdominal trauma. Clin Imag. 2014;38:73–74. doi: 10.1016/j.clinimag.2013.09.003[↩]
- Daodu O, Brindle M, Alvarez-Allende CR, Lockyer L, et al. Outcomes of an accelerated care pathway for pediatric blunt solid organ injuries in a public healthcare system. J Pediatr Surg. 2017;52:826–831. doi: 10.1016/j.jpedsurg.2017.01.037[↩][↩][↩]
- Ma OJ, Mateer JR, Ogata M, Kefer MP, Wittmann D, Aprahamian C. Prospective analysis of a rapid trauma ultrasound examination performed by emergency physicians. J Trauma. 1995 Jun;38(6):879-85. doi: 10.1097/00005373-199506000-00009[↩]
- Gamblin TC, Wall CE Jr, Royer GM, Dalton ML, Ashley DW. Delayed splenic rupture: case reports and review of the literature. J Trauma. 2005 Nov;59(5):1231-4. doi: 10.1097/01.ta.0000197270.25280.7c[↩]
- Livingston MH, Moffat B, Leeper WR, Parry NG, Gray DK. Angiography and embolization for blunt splenic injuries. J Am Coll Surg. 2014 Dec;219(6):1193-4. doi: 10.1016/j.jamcollsurg.2014.08.008[↩]
- Morgan TL, Tomich EB. Overwhelming post-splenectomy infection (OPSI): a case report and review of the literature. J Emerg Med. 2012 Oct;43(4):758-63. doi: 10.1016/j.jemermed.2011.10.029[↩]
- Styrt B. Infection associated with asplenia: risks, mechanisms, and prevention. Am J Med. 1990 May;88(5N):33N-42N.[↩]
- Lortan JE. Management of asplenic patients. Br J Haematol. 1993 Aug;84(4):566-9. doi: 10.1111/j.1365-2141.1993.tb03128.x[↩]
- Cullingford GL, Watkins DN, Watts AD, Mallon DF. Severe late postsplenectomy infection. Br J Surg. 1991 Jun;78(6):716-21. doi: 10.1002/bjs.1800780626[↩]
- Ammann AJ, Addiego J, Wara DW, Lubin B, Smith WB, Mentzer WC. Polyvalent pneumococcal-polysaccharide immunization of patients with sickle-cell anemia and patients with splenectomy. N Engl J Med. 1977 Oct 27;297(17):897-900. doi: 10.1056/NEJM197710272971701[↩]





{kind=link}