Contents
What is a pulmonary embolism
A pulmonary embolism is a sudden blockage in a lung artery that is usually caused a blood clot in the leg called a deep vein thrombosis (DVT) that breaks loose and travels through the bloodstream to the lung. A clot that forms in one part of the body and travels in the bloodstream to another part of the body is called an embolus. Pulmonary embolism most often is a complication of a condition called deep vein thrombosis. In deep vein thrombosis (DVT), blood clots form in the deep veins of the body—most often in your legs. These clots can break free, travel through the bloodstream to the lungs, and block an artery. However, pulmonary embolism rarely also originate in the pelvic, renal, upper extremity veins, or the right heart chambers.
Other embolic sources include:
- air embolism
- carbon dioxide embolism
- other gas embolism (e.g. nitrogen, helium)
- fat embolism
- tumor embolism: comprised of tumor thrombus
- hydatid embolism
- talc embolism
- iodinated oil embolism
- metallic embolism
- mercury embolism
- barium embolism
- amniotic fluid embolism
- cement embolism: comprised of polymethyl methacrylate
- catheter embolism
- septic embolism
Pulmonary embolism is not a disease in and of itself. Rather, it is a complication of underlying vein thrombosis. Under normal conditions, microthrombi (tiny aggregates of red cells, platelets, and fibrin) are formed and dissolve continually within the venous circulatory system.
Figure 1. Pulmonary embolism
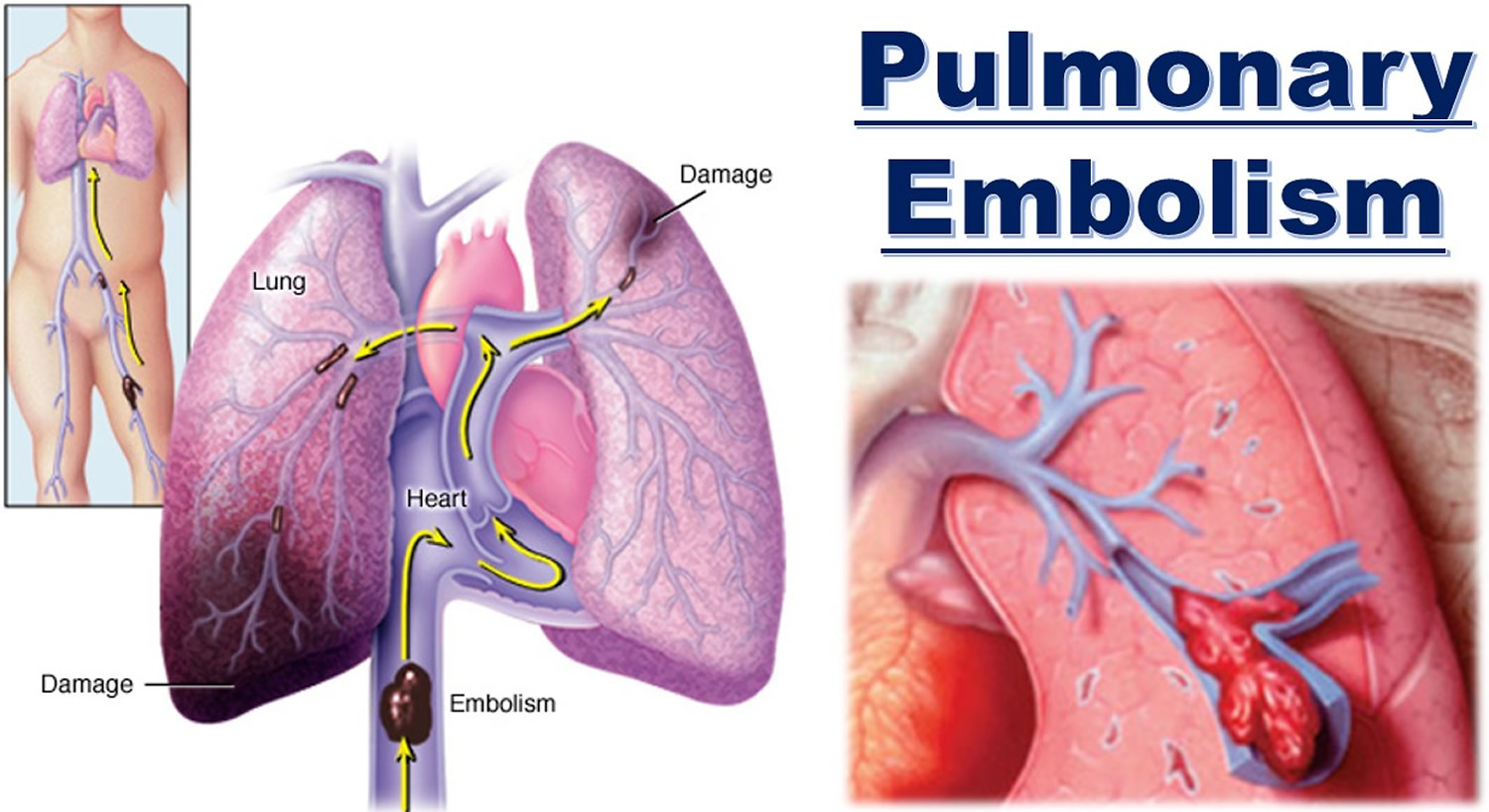 Figure 2. Pulmonary artery
Figure 2. Pulmonary artery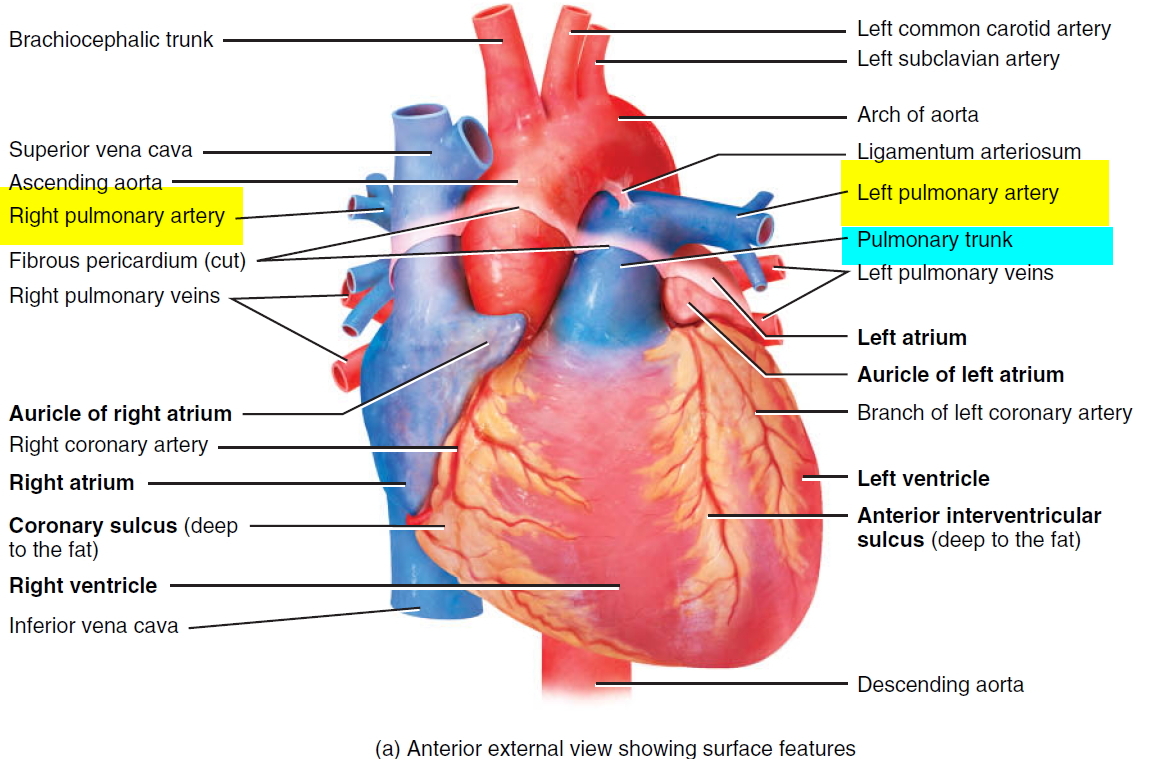
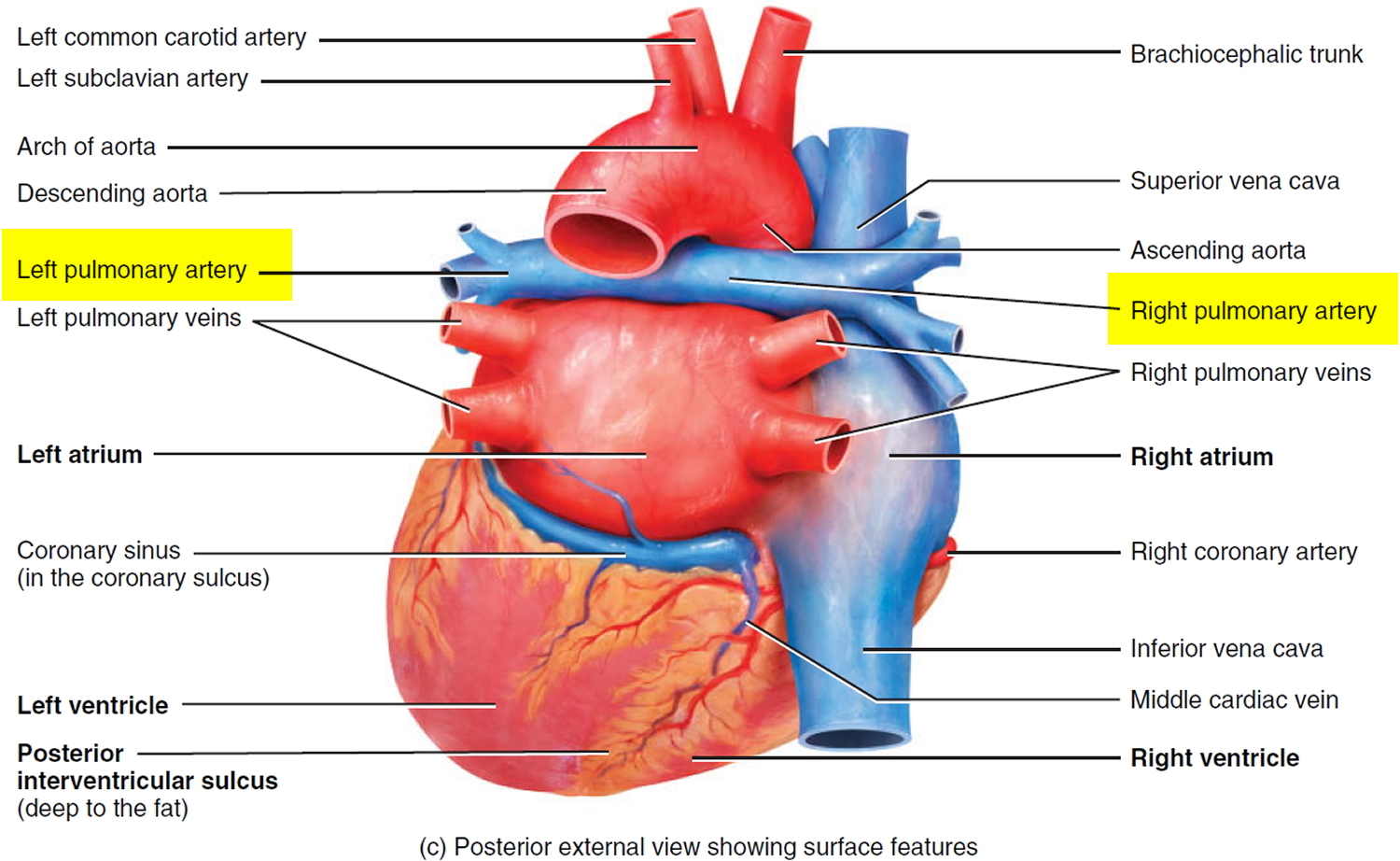
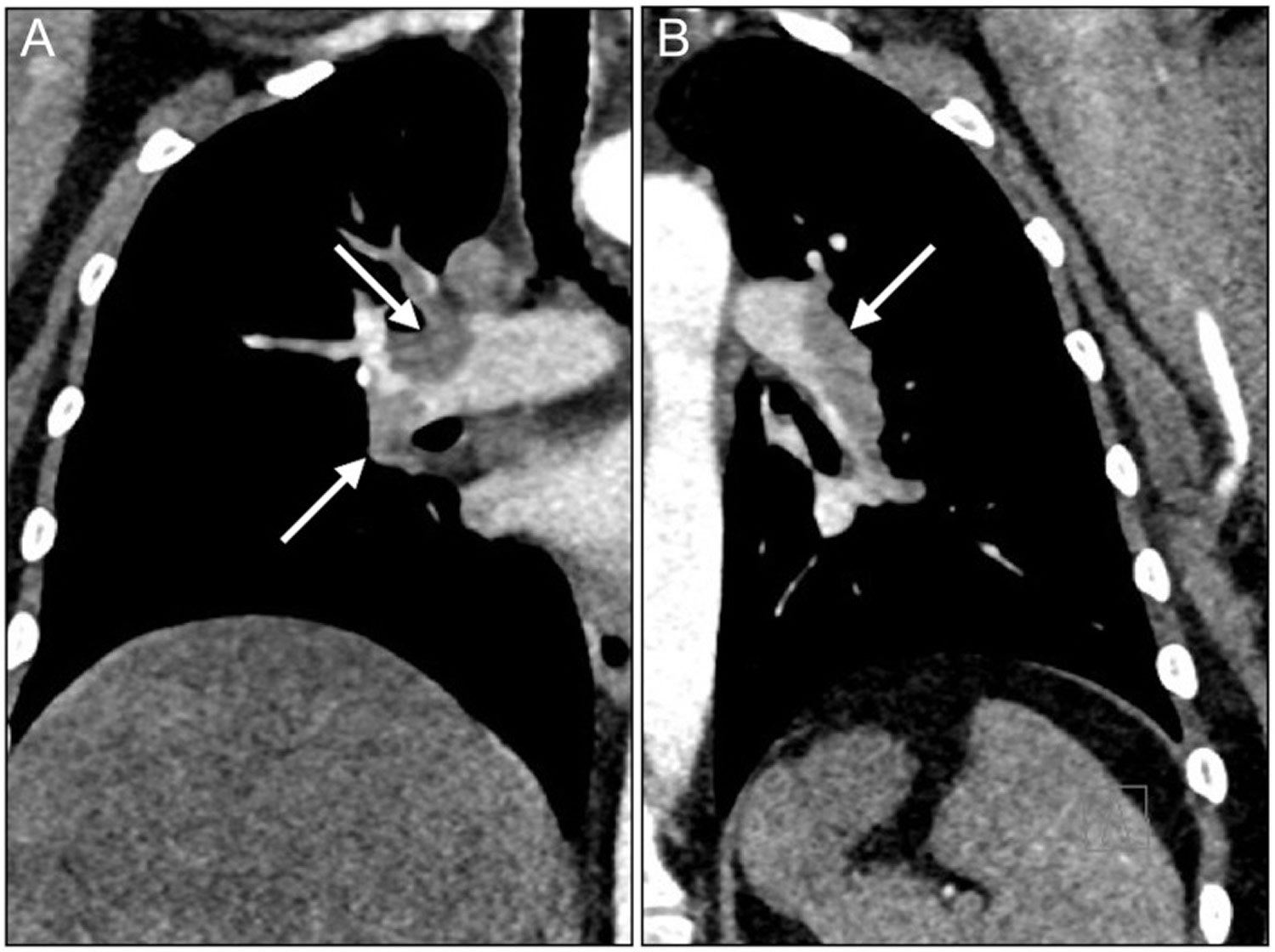
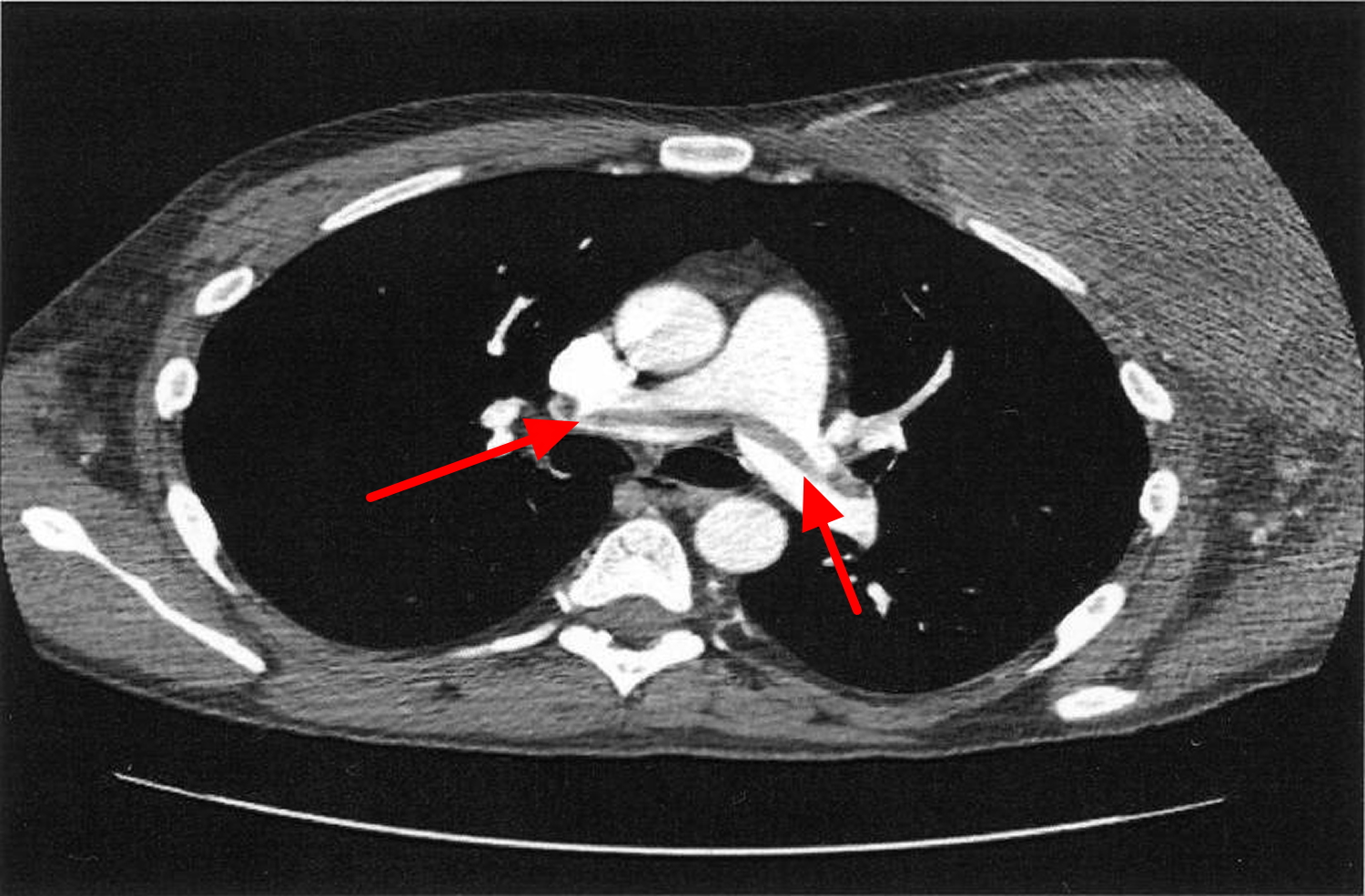
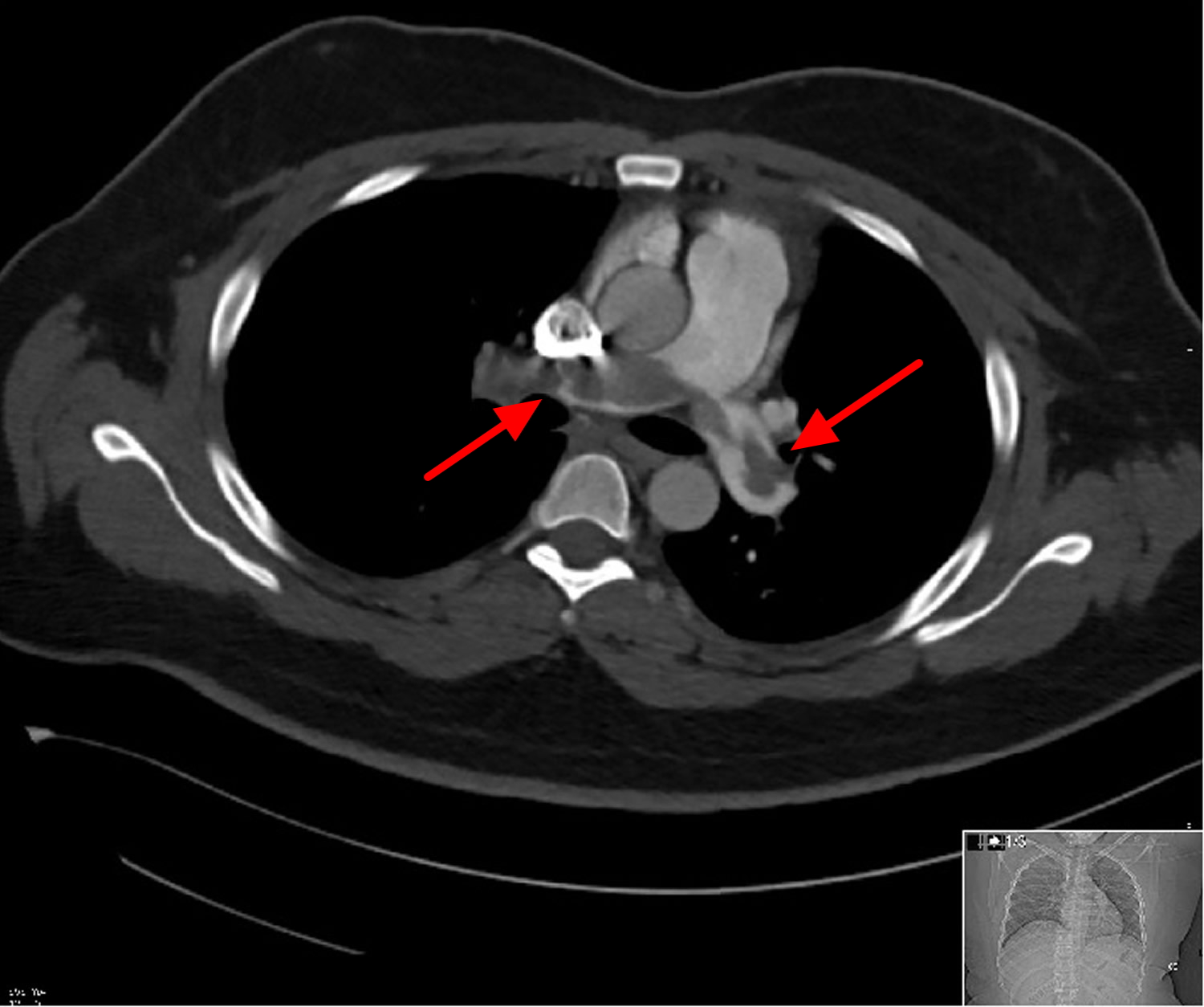
Figure 3. Bilateral pulmonary embolism – the emboli in the right (A) and left (B) lungs are indicated by arrows (CT angiogram).
Deep vein clots are not like clots in veins close to the skin’s surface. Those clots remain in place and do not cause pulmonary embolism.
Pulmonary embolism is a serious condition that can cause:
- Damage part of your lung because of a lack of blood flow to your lung tissue. This damage may lead to pulmonary hypertension (increased pressure in the pulmonary arteries).
- Cause low oxygen levels in your blood.
- Permanent damage to the affected lung
- Damage to other organs in your body from not getting enough oxygen
If a clot is large, or if there are many clots, pulmonary embolism can cause death.
Half the people who have pulmonary embolism have no symptoms. If you do have symptoms, they can include shortness of breath, chest pain or coughing up blood. Symptoms of a blood clot include warmth, swelling, pain, tenderness and redness of the leg. The goal of treatment is to break up clots and help keep other clots from forming.
The exact number of people affected by deep vein thrombosis (DVT) and pulmonary embolism isn’t known. Estimates suggest these conditions affect 300,000 to 600,000 people in the United States each year. Post-mortem studies show that pulmonary embolism in fact occurs very commonly, but is not diagnosed this often in life, partly because very small emboli often don’t cause any problems. Symptomatic pulmonary embolism occurs in 20 to 25 per 100 000 hospitalized patients, and much less often in non-hospitalized patients. If left untreated, about 30 percent of patients who have pulmonary embolism will die. Most of those who die do so within the first few hours of the event. The good news is that a prompt diagnosis and proper treatment can save lives and help prevent the complications of pulmonary embolism.
The course of events depends on the size of the clot causing pulmonary embolism.
- Small to medium pulmonary embolism: cut off the circulation to a part of the lung, and cause shortness of breath due to hypoxia. In 10% of cases, the region of lung supplied by the blocked artery dies due to inadequate blood flow. This will eventually heal with a fibrous scar.
- Massive pulmonary embolism: If a very large clot forms, usually in one of the pelvic or large abdominal veins, it may embolise in the main pulmonary artery, blocking off almost all blood flow to the lungs. This causes back-pressure on the right side of the heart, causing a reduction in the amount of blood pumped from the heart into the lungs, and right heart failure. These changes to the heart may happen suddenly (massive pulmonary embolism), or gradually, due to recurrent pulmonary emboli.
Saddle pulmonary embolism
Saddle pulmonary embolism commonly refers to a large pulmonary embolism that straddles the bifurcation of the pulmonary trunk, extending into the left and right pulmonary arteries.
If large enough, it can completely obstruct both left and right pulmonary arteries resulting in right heart failure and, unless treatment is prompt, death.
With such extensive embolic burden, signs of right heart strain are usually present and include:
- dilatation of the right ventricle (RV) (i.e. RV width > LV width)
- straightening or leftward bulging of the interventricular septum
- enlargement of the pulmonary trunk
Contrast reflux into the azygos vein, via the superior vena cava, and hepatic veins, via the inferior vena cava, is a controversial sign of RV strain, as it often occurs in the absence of raised right-sided heart pressures.
Figure 4. Saddle pulmonary embolism (CT angiogram)
Pulmonary embolism prognosis
Around 10% of clinical pulmonary emboli are fatal. Importantly, 30% of patients with pulmonary embolism will suffer a second, thus, secondary prevention is important. In the long term pulmonary embolism may cause decompensated right heart failure which also has significant morbidity and mortality.
Pulmonary embolism complications
Pulmonary embolism can be life-threatening. About one-third of people with undiagnosed and untreated pulmonary embolism don’t survive. When the condition is diagnosed and treated promptly, however, that number drops dramatically.
Pulmonary embolism can also lead to pulmonary hypertension, a condition in which the blood pressure in your lungs and in the right side of the heart is too high. When you have obstructions in the arteries inside your lungs, your heart must work harder to push blood through those vessels. This increases the blood pressure within these vessels and the right side of the heart, which can weaken your heart.
In rare cases, small emboli occur frequently and develop over time, resulting in chronic pulmonary hypertension, also known as chronic thromboembolic pulmonary hypertension.
Pulmonary embolism causes
What causes pulmonary embolism
Pulmonary embolism usually begins as a blood clot in a deep vein of your leg. This condition is called deep vein thrombosis (DVT). The clot can break free, travel through the bloodstream to the lungs, and block an artery.
In most cases, multiple clots are involved but not necessarily all at once. The portions of lung served by each blocked artery are robbed of blood and may die. This is known as pulmonary infarction. This makes it more difficult for your lungs to provide oxygen to the rest of your body.
Blood clots can form in the deep veins of the legs if blood flow is restricted and slows down. This can happen if you don’t move around for long periods, such as:
- After some types of surgery
- During a long trip in a car or airplane
- If you must stay in bed for an extended time
Blood clots are more likely to develop in veins damaged from surgery or injured in other ways.
Other causes of pulmonary embolism
Occasionally, blockages in the blood vessels are caused by substances other than blood clots, such as an air bubble, part of a tumor, or other tissue travels to the lungs and causes pulmonary embolism. Also, if a large bone in the body (such as the thigh bone) breaks, fat from the bone marrow can travel through the blood. If the fat reaches the lungs, it can cause pulmonary embolism.
Pulmonary embolism risk factors
Pulmonary embolism occurs equally in men and women. The risk increases with age. For every 10 years after age 60, the risk of having pulmonary embolism doubles.
Certain inherited conditions, such as factor V Leiden, increase the risk of blood clotting and pulmonary embolism.
Major Risk Factors
Your risk for pulmonary embolism is high if you have deep vein thrombosis (DVT) or a history of DVT. In DVT, blood clots form in the deep veins of the body—most often in the legs. These clots can break free, travel through the bloodstream to the lungs, and block an artery.
Your risk for pulmonary embolism also is high if you’ve had the condition before.
The most important risk factors are:
- Recent surgery, especially pelvic and abdominal surgery,
- Prolonged bed rest, pelvic and leg fractures.
- Pregnancy and childbirth,
- Advanced age,
- Smoking,
- Inherited clotting diseases,
- Any severe, debilitating illness (for example heart disease, cancer).
- Increased estrogen in the body can increase the likelihood of clot formation, and thus of pulmonary embolism. The commonest cause of increased estrogen is the oral contraceptive pill. Studies have shown, however, that only women over the age of 40, who smoke, and take the pill, have an increased risk of clot formation.
Other Risk Factors
Other factors also can increase the risk for pulmonary embolism, such as:
- Being bedridden or unable to move around much. Being confined to bed for an extended period after surgery, a heart attack, leg fracture, trauma or any serious illness makes you more vulnerable to blood clots. When the lower extremities are horizontal for long periods, the flow of venous blood slows and blood can pool in the legs.
- Heart disease. Cardiovascular disease, specifically heart failure, makes clot formation more likely.
- Cancer. Certain cancers — especially pancreatic, ovarian and lung cancers, and many cancers with metastasis — can increase levels of substances that help blood clot, and chemotherapy further increases the risk. Women with a personal or family history of breast cancer who are taking tamoxifen or raloxifene also are at higher risk of blood clots.
- Having surgery or breaking a bone (the risk goes up in the weeks following the surgery or injury). Surgery is one of the leading causes of problem blood clots. For this reason, medication to prevent clots may be given before and after major surgery such as joint replacement.
- Having certain diseases or conditions, such as a stroke, paralysis (an inability to move), chronic heart disease, or high blood pressure
- Smoking. For reasons that aren’t well-understood, tobacco use predisposes some people to blood clot formation, especially when combined with other risk factors.
- Long trips. Sitting in a cramped position during lengthy plane or car trips slows blood flow in the legs, which contributes to the formation of clots.
- Being overweight. Excess weight increases the risk of blood clots — particularly in women who smoke or have high blood pressure.
- Supplemental estrogen. The estrogen in birth control pills and in hormone replacement therapy can increase clotting factors in your blood, especially if you smoke or are overweight.
- Pregnancy. The weight of the baby pressing on veins in the pelvis can slow blood return from the legs. Clots are more likely to form when blood slows or pools.
- Primary hypercoagulable states:
- protein C deficiency
- protein S deficiency
- antithrombin III deficiency
- lupus anticoagulant
People who have recently been treated for cancer or who have a central venous catheter are more likely to develop DVT, which increases their risk for pulmonary embolism. A central venous catheter is a tube placed in a vein to allow easy access to the bloodstream for medical treatment.
Other risk factors for DVT include sitting for long periods (such as during long car or airplane rides), pregnancy and the 6-week period after pregnancy, and being overweight or obese. Women who take hormone therapy pills or birth control pills also are at increased risk for DVT.
The risk of developing blood clots increases as your number of risk factors increases.
The link between air travel and pulmonary embolism is a weak one. Research suggests so far that long-haul air travel causes a very slight increase in risk of deep vein thrombosis, or leg clots. This increase is mainly in those with pre-existing illness or other predisposing factors. If the increased risk of DVT on long flights is slight, then the risk of pulmonary embolism arising from such DVTs is even lower. One French study found the incidence of pulmonary embolism to be 0.5 per million passengers landing in Paris per year; it is debatable how many of these were due to the air travel.
Pulmonary embolism prevention
Preventing pulmonary embolism begins with preventing deep vein thrombosis (DVT). Knowing whether you’re at risk for DVT and taking steps to lower your risk are important.
- Exercise your lower leg muscles if you’re sitting for a long time while traveling.
- Get out of bed and move around as soon as you’re able after having surgery or being ill. The sooner you move around, the better your chance is of avoiding a blood clot. This is one of the main reasons your nurse may push you to get up, even on your day of surgery, and walk despite pain at the site of your surgical incision.
- Take medicines to prevent clots after some types of surgery (as your doctor prescribes).
- Blood thinners (anticoagulants). These medications are often given to people at risk of clots before and after an operation — as well as to people admitted to the hospital with a heart attack, stroke or complications of cancer.
- Follow up with your doctor.
- Compression stockings. Compression stockings steadily squeeze your legs, helping your veins and leg muscles move blood more efficiently. They offer a safe, simple and inexpensive way to keep blood from stagnating during and after general surgery.
- Leg elevation. Elevating your legs when possible and during the night also can be very effective. Raise the bottom of your bed 4 to 6 inches with blocks or books.
- Pneumatic compression. This treatment uses thigh-high or calf-high cuffs that automatically inflate with air and deflate every few minutes to massage and squeeze the veins in your legs and improve blood flow.
If you’ve already had DVT or pulmonary embolism, you can take more steps to prevent new blood clots from forming. Visit your doctor for regular checkups. Also, use compression stockings to prevent chronic (ongoing) swelling in your legs from DVT (as your doctor advises).
See your doctor right away if you have any signs or symptoms of DVT or pulmonary embolism.
Prevention while traveling
The risk of blood clots developing while traveling is low, but increases as travel increases. If you have risk factors for blood clots and you’re concerned about traveling, talk with your doctor.
Your doctor might suggest the following to help prevent blood clots during travel:
- Drink plenty of fluids. Water is the best liquid for preventing dehydration, which can contribute to the development of blood clots. Avoid alcohol, which contributes to fluid loss.
- Take a break from sitting. Move around the airplane cabin once an hour or so. If you’re driving, stop every hour and walk around the car a couple of times.
- Do a few deep knee bends.
- Fidget in your seat. Flex your ankles every 15 to 30 minutes.
- Wear support stockings. Your doctor may recommend these to help promote circulation and fluid movement in your legs. Compression stockings are available in a range of stylish colors and textures. There are even devices, called stocking butlers, to help you put on the stockings.
Pulmonary embolism signs and symptoms
Pulmonary embolism symptoms can vary greatly, depending on how much of your lung is involved, the size of the clots, and whether you have underlying lung or heart disease. It’s also possible to have pulmonary embolism and not have any signs or symptoms.
Signs and symptoms of pulmonary embolism include unexplained shortness of breath, problems breathing, chest pain, coughing, or coughing up blood. An arrhythmia (irregular heartbeat) also may suggest that you have pulmonary embolism.
Sometimes the only signs and symptoms are related to deep vein thrombosis (DVT). These include swelling of the leg or along a vein in the leg, pain or tenderness in the leg, a feeling of increased warmth in the area of the leg that’s swollen or tender, and red or discolored skin on the affected leg.
The classic presentation of pulmonary embolism is the abrupt onset of pleuritic chest pain, shortness of breath, and hypoxia. However, most patients with pulmonary embolism have no obvious symptoms at presentation. Rather, symptoms may vary from sudden catastrophic hemodynamic collapse to gradually progressive dyspnea. The diagnosis of pulmonary embolism should be suspected in patients with respiratory symptoms unexplained by an alternative diagnosis.
Common signs and symptoms of pulmonary embolism include:
- Shortness of breath. This symptom typically appears suddenly and always gets worse with exertion.
- Chest pain. You may feel like you’re having a heart attack. The pain may become worse when you breathe deeply (pleurisy), cough, eat, bend or stoop. The pain will get worse with exertion but won’t go away when you rest.
- Cough. The cough may produce bloody or blood-streaked sputum.
Other signs and symptoms that can occur with pulmonary embolism include:
- Leg pain or swelling, or both, usually in the calf
- Clammy or discolored skin (cyanosis)
- Fever
- Excessive sweating
- Rapid or irregular heartbeat
- Lightheadedness or dizziness
Patients with pulmonary embolism may present with atypical symptoms, such as the following:
- Seizures
- Syncope
- Abdominal pain
- Fever
- Productive cough
- Wheezing
- Decreasing level of consciousness
- New onset of atrial fibrillation
- Hemoptysis (coughing up blood)
- Flank pain
- Delirium (in elderly patients)
Other signs and symptoms of pulmonary embolism
Some people who have pulmonary embolism have feelings of anxiety or dread, light-headedness or fainting, rapid breathing, sweating, or an increased heart rate.
Symptoms of DVT
In some cases, there may be no symptoms of DVT. If symptoms do occur they can include:
- pain, swelling and tenderness in one of your legs (usually your calf)
- a heavy ache in the affected area
- warm skin in the area of the clot
- red skin, particularly at the back of your leg below the knee
DVT usually (although not always) affects one leg. The pain may be worse when you bend your foot upward towards your knee.
If left untreated, about 1 in 10 people with a DVT will develop a pulmonary embolism.
Pulmonary embolism can be life-threatening. See your doctor right away if you have any signs or symptoms of pulmonary embolism or DVT.
Pulmonary embolism diagnosis
Pulmonary embolism is diagnosed based on your medical history, a physical exam, and test results.
Doctors who treat patients in the emergency room often are the ones to diagnose pulmonary embolism with the help of a radiologist. A radiologist is a doctor who deals with x rays and other similar tests.
Medical History and Physical Exam
To diagnose pulmonary embolism, the doctor will ask about your medical history. He or she will want to:
- Find out your deep vein thrombosis (DVT) and pulmonary embolism risk factors
- See how likely it is that you could have pulmonary embolism
- Rule out other possible causes for your symptoms
Your doctor also will do a physical exam. During the exam, he or she will check your legs for signs of DVT. He or she also will check your blood pressure and your heart and lungs.
Diagnostic Tests
Many tests can help diagnose pulmonary embolism. Which tests you have will depend on how you feel when you get to the hospital, your risk factors, available testing options, and other conditions you could possibly have. You may have one or more of the following tests.
Ultrasound
Doctors can use ultrasound to look for blood clots in your legs. Ultrasound uses sound waves to check blood flow in your veins.
For this test, gel is put on the skin of your legs. A hand-held device called a transducer is moved back and forth over the affected areas. The transducer gives off ultrasound waves and detects their echoes as they bounce off the vein walls and blood cells.
A computer turns the echoes into a picture on a computer screen, allowing the doctor to see blood flow in your legs. If the doctor finds blood clots in the deep veins of your legs, he or she will recommend treatment.
DVT and pulmonary embolism both are treated with the same medicines.
Computed Tomography Scans
Doctors can use computed tomography scans, or CT scans, to look for blood clots in the lungs and legs.
For this test, dye is injected into a vein in your arm. The dye makes the blood vessels in your lungs and legs show up on x-ray images. You’ll lie on a table, and an x-ray tube will rotate around you. The tube will take pictures from many angles.
This test allows doctors to detect most cases of pulmonary embolism. The test only takes a few minutes. Results are available shortly after the scan is done.
Lung Ventilation/Perfusion Scan
A lung ventilation/perfusion scan, or VQ scan, uses a radioactive substance to show how well oxygen and blood are flowing to all areas of your lungs. This test can help detect pulmonary embolism.
Pulmonary Angiography
Pulmonary angiography is another test used to diagnose pulmonary embolism. This test isn’t available at all hospitals, and a trained specialist must do the test.
For this test, a flexible tube called a catheter is threaded through the groin (upper thigh) or arm to the blood vessels in the lungs. Dye is injected into the blood vessels through the catheter.
X-ray pictures are taken to show blood flowing through the blood vessels in the lungs. If a blood clot is found, your doctor may use the catheter to remove it or deliver medicine to dissolve it.
Blood Tests
Certain blood tests may help your doctor find out whether you’re likely to have pulmonary embolism.
A D-dimer test measures a substance in the blood that’s released when a blood clot breaks down. High levels of the substance may mean a clot is present. If your test is normal and you have few risk factors, pulmonary embolism isn’t likely.
D-dimer (ELISA) is commonly used as a screening test in patients with a low and moderate probability clinical assessment, on these patients:
- normal D-dimer has almost 100% negative predictive value (virtually excludes pulmonary embolism): no further testing is required
- raised D-dimer is seen with pulmonary embolism but has many other causes and is, therefore, non-specific: it indicates the need for further testing if pulmonary embolism is suspected 1
On patients with a high probability clinical assessment, a D-dimer test is not helpful because a negative D-dimer result does not exclude pulmonary embolism in more than 15%. Patients are treated with anticoagulants while awaiting the outcome of diagnostic tests 1.
Other blood tests check for inherited disorders that cause blood clots. Blood tests also can measure the amount of oxygen and carbon dioxide in your blood. A clot in a blood vessel in your lungs may lower the level of oxygen in your blood.
Other Tests
To rule out other possible causes of your symptoms, your doctor may use one or more of the following tests.
- Echocardiography (echo). This test uses sound waves to create a moving picture of your heart. Doctors use echo to check heart function and detect blood clots inside the heart.
- ECG (electrocardiogram). An ECG is a simple, painless test that detects and records the heart’s electrical activity.
- Chest x ray. This test creates pictures of your lungs, heart, large arteries, ribs, and diaphragm (the muscle below your lungs).
- Chest MRI (magnetic resonance imaging). This test uses radio waves and magnetic fields to create pictures of organs and structures inside the body. MRI often can provide more information than an x ray.
Pulmonary embolism ECG
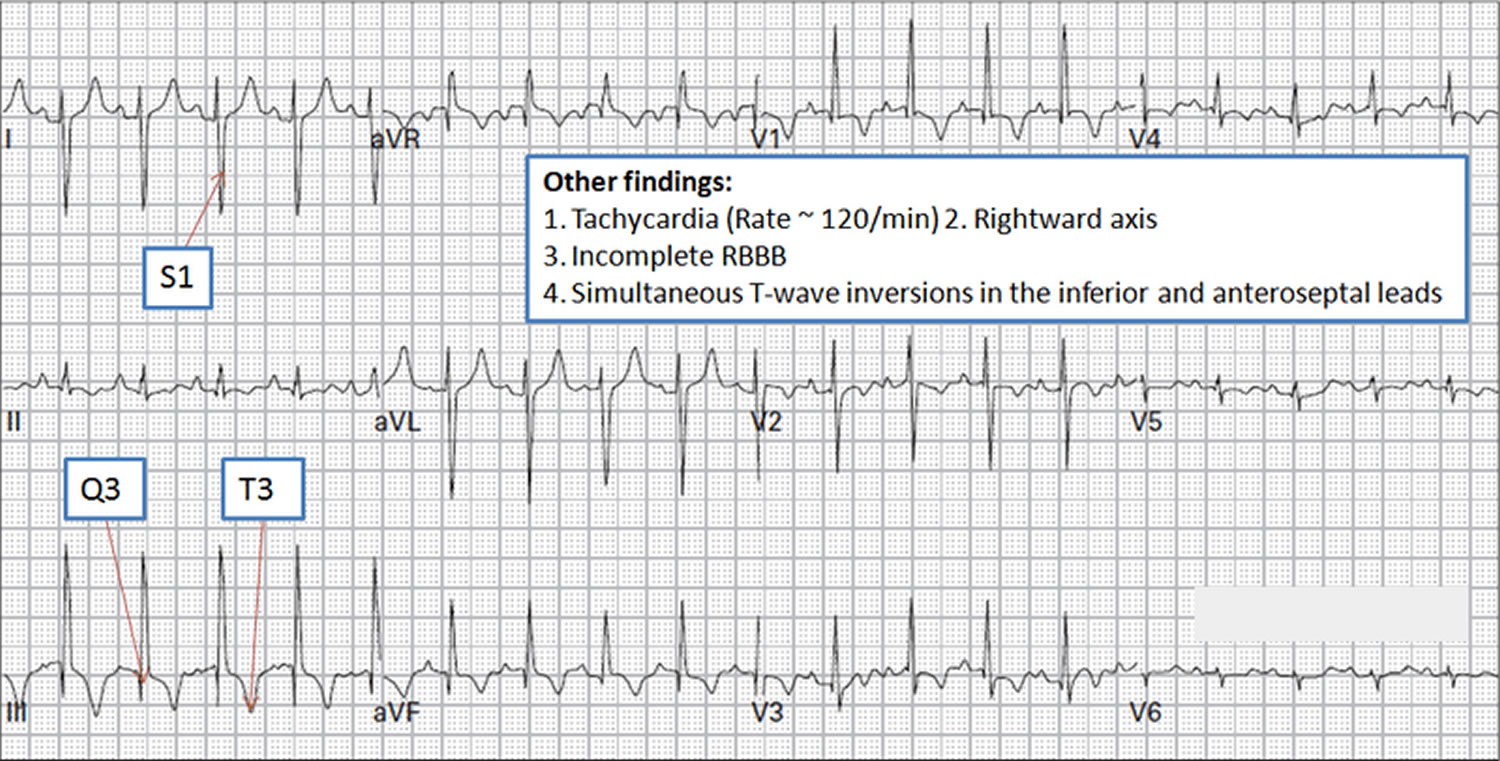
The most common ECG abnormalities in the setting of pulmonary embolism are tachycardia and nonspecific ST-T wave abnormalities. The finding of S1 Q3 T3 (S-waves in lead I, Q-waves in lead III and inverted T-waves in lead III) is nonspecific and insensitive in the absence of clinical suspicion for pulmonary embolism. The classic findings of right heart strain and acute cor pulmonale are tall, peaked P waves in lead II (P pulmonale); right axis deviation; right bundle-branch block; an S1 Q3 T3 pattern; or atrial fibrillation. Unfortunately, only 20% of patients with proven pulmonary embolism have any of these classic ECG abnormalities. If ECG abnormalities are present, they may be suggestive of pulmonary embolism, but the absence of such abnormalities has no significant predictive value.
Figure 5. Pulmonary embolism ECG
Pulmonary embolism treatment
Pulmonary embolism is treated with medicines, procedures, and other therapies. The main goals of treating pulmonary embolism are to stop the blood clot from getting bigger and keep new clots from forming.
Treatment may include medicines to thin the blood and slow its ability to clot. If your symptoms are life threatening, your doctor may give you medicine to quickly dissolve the clot. Rarely, your doctor may use surgery or another procedure to remove the clot.
Medicines
- Blood thinners (anticoagulants). These drugs prevent new clots from forming while your body works to break up the clots. Heparin is a frequently used anticoagulant that can be given through the vein or injected under the skin. It acts quickly and is often overlapped for several days with an oral anticoagulant, such as warfarin, until it becomes effective, which can take days. A newer class of anticoagulants, referred to as novel oral anticoagulants, has been tested and approved for treatment of venous thromboembolism, including pulmonary embolism. These medications work quickly and have fewer interactions with other medications. Some novel oral anticoagulants have the advantage of being given by mouth, without the need for overlap with heparin. However, all anticoagulants have side effects, with bleeding being the most common.
- Clot dissolvers (thrombolytics). While clots usually dissolve on their own, there are medications given through the vein that can dissolve clots quickly. Because these clot-busting drugs can cause sudden and severe bleeding, they usually are reserved for life-threatening situations.
Anticoagulants or blood thinners, decrease your blood’s ability to clot. They’re used to stop blood clots from getting larger and prevent clots from forming. Blood thinners don’t break up blood clots that have already formed. (The body dissolves most clots with time.)
You can take blood thinners as either a pill, an injection, or through a needle or tube inserted into a vein (called intravenous, or IV, injection). Warfarin is given as a pill. (Coumadin® is a common brand name for warfarin.) Heparin is given as an injection or through an IV tube.
Your doctor may treat you with both heparin and warfarin at the same time. Heparin acts quickly. Warfarin takes 2 to 3 days before it starts to work. Once warfarin starts to work, heparin usually is stopped.
Pregnant women usually are treated with heparin only, because warfarin is dangerous for the pregnancy.
If you have deep vein thrombosis, treatment with blood thinners usually lasts for 3 to 6 months. If you’ve had blood clots before, you may need a longer period of treatment. If you’re being treated for another illness, such as cancer, you may need to take blood thinners as long as pulmonary embolism risk factors are present.
The most common side effect of blood thinners is bleeding. This can happen if the medicine thins your blood too much. This side effect can be life threatening.
Sometimes the bleeding is internal, which is why people treated with blood thinners usually have routine blood tests. These tests, called PT and PTT tests, measure the blood’s ability to clot. These tests also help your doctor make sure you’re taking the right amount of medicine. Call your doctor right away if you’re bruising or bleeding easily.
Thrombin inhibitors are a newer type of blood-thinning medicine. They’re used to treat some types of blood clots in people who can’t take heparin.
Emergency Treatment
When pulmonary embolism is life threatening, a doctor may use treatments that remove or break up the blood clot. These treatments are given in an emergency room or hospital.
Thrombolytics are medicines that can quickly dissolve a blood clot. They’re used to treat large clots that cause severe symptoms. Because thrombolytics can cause sudden bleeding, they’re used only in life-threatening situations.
Sometimes a doctor may use a catheter (a flexible tube) to reach the blood clot. The catheter is inserted into a vein in the groin (upper thigh) or arm and threaded to the clot in the lung. The doctor may use the catheter to remove the clot or deliver medicine to dissolve it.
Rarely, surgery may be needed to remove the blood clot.
Other Types of Treatment
- Clot removal. If you have a very large, life-threatening clot in your lung, your doctor may suggest removing it via a thin, flexible tube (catheter) threaded through your blood vessels.
- Vein filter. A catheter can also be used to position a filter in the body’s main vein — called the inferior vena cava — that leads from your legs to the right side of your heart. This filter can help keep clots from being carried into your lungs. This procedure is typically reserved for people who can’t take anticoagulant drugs or when anticoagulant drugs don’t work well enough or fast enough. Some filters can be removed when they are no longer needed.
If you can’t take medicines to thin your blood, or if the medicines don’t work, your doctor may suggest a vena cava filter. This device keeps blood clots from traveling to your lungs.
The filter is inserted inside a large vein called the inferior vena cava. (This vein carries blood from the body back to the heart). The filter catches clots before they travel to the lungs. This type of treatment can prevent pulmonary embolism, but it won’t stop other blood clots from forming.
Graduated compression stockings can reduce the chronic (ongoing) swelling that a blood clot in the leg may cause.
Graduated compression stockings are worn on the legs from the arch of the foot to just above or below the knee. These stockings are tight at the ankle and become looser as they go up the leg. This causes gentle compression (pressure) up the leg. The pressure keeps blood from pooling and clotting.
Living with pulmonary embolism
Pulmonary embolism (pulmonary embolism) usually is treated in a hospital. After leaving the hospital, you may need to take medicine at home for 6 months or longer. It’s important to:
- Take all medicines as prescribed, and have blood tests done as your doctor advises.
- Talk with your doctor before taking blood-thinning medicines with any other medicines, including over-the-counter products. Over-the-counter aspirin, for example, can thin your blood. Taking two medicines that thin your blood may increase your risk of bleeding.
- Ask your doctor about your diet. Foods that contain vitamin K can affect how well warfarin (Coumadin®) works. Vitamin K is found in green leafy vegetables and some oils, such as canola and soybean oils. It’s best to eat a well-balanced, healthy diet.
- Discuss with your doctor what amount of alcohol is safe for you to drink if you’re taking medicine.
Medicines used to treat pulmonary embolism can thin your blood too much. This can cause bleeding in the digestive system or the brain. If you have signs or symptoms of bleeding in the digestive system or the brain, get treatment at once.
Signs and symptoms of bleeding in the digestive system include:
- Bright red vomit or vomit that looks like coffee grounds
- Bright red blood in your stool or black, tarry stools
- Pain in your abdomen
Signs and symptoms of bleeding in the brain include:
- Severe pain in your head
- Sudden changes in your vision
- Sudden loss of movement in your legs or arms
- Memory loss or confusion
Excessive bleeding from a fall or injury also may mean that your pulmonary embolism medicines have thinned your blood too much. Excessive bleeding is bleeding that won’t stop after you apply pressure to a wound for 10 minutes. If you have excessive bleeding from a fall or injury, get treatment at once.
Once you’ve had pulmonary embolism (with or without deep vein thrombosis (DVT)), you’re at higher risk of having the condition again. During treatment and after, continue to take steps to prevent DVT.
Check your legs for any signs or symptoms of DVT, such as swollen areas, pain or tenderness, increased warmth in swollen or painful areas, or red or discolored skin.
If you think that you have DVT or are having symptoms of pulmonary embolism, contact your doctor right away.





{kind=link}