
Shaving pubic hair
Pubic hair grooming is a growing phenomenon and is associated with body image and sexual activity. Hair is a distinguishing feature of mammals, though the persistence of visible head, armpit, and pubic hair remains anthropologically unclear. Humans throughout the ages have modified their head and body hair, but aesthetic removal of pubic hair has become the “the ultimate barometer of how fashionable you really are” in the 21st century. Pubic hair was rarely depicted in artistic representations of the nude until the late 19th century 1. Since the latter half of the 20th century, pubic hair removal also called depilation or epilation, has become an increasingly common grooming practice in the United States and other developed nations 2. Pubic hair grooming is increasingly prevalent among men and women in the United States 3.
It is postulated that the current trend of pubic hair removal may be related to the increased accessibility of Internet-based pornography 1. Vannier et al. 4 analyzed pornographic movies and found men are likely to be groomed and most women were likely to have no pubic hair at all, mirroring some pubic hair grooming trends. Anecdotally, pubic hair removal may carry benefits regarding increased sexual sensation and satisfaction though there is no quantative research in this field 1. Pubic hair removal appears to be an important aspect of expressing one’s sexuality and participation in sexual activity. This practice has an interesting psychosexual basis which, to date, has not yet been fully explored in sexual medicine. Changing beauty ideals are reflected in media sources, such as sexually explicit media or pornographic images 5 and have likely contributed to the expansion of this cultural trend. Pubic hair removal has also been associated with various sexual behaviors in women, such as receiving vaginal and clitoral stimulation with fingers 6. The role of sexual behavior and pubic hair removal in men is less clear. Several studies have looked at psychological factors contributing to pubic hair removal in men and have found the drive for muscularity, gender role conflicts, and physical appearance social comparisons have been correlated with increasing degrees of body hair removal 7. It has been shown that men who have sex with men remove their pubic hair more frequently 8.
There are numerous reasons to remove pubic hair; the most commonly reported are focused on sexual activity and sexual expression 9. Increasing access to sexually explicit material may also influence grooming motivation and trends 4. In a recent study, pubic hair grooming was strongly associated with sexual activity and practices 3. Pubic hair grooming may lead to higher genital satisfaction and sexual function in women 10 and to greater positive body image in men 8. Interestingly, pubic hair–related grooming injuries have increased over the past 10 years, and it has been suggested that anogenital grooming may put one at risk for a sexually transmitted infection (STI) 3. The association between pubic hair grooming, sexual activity, and genital injuries/infections indicate that this is a potentially important but overlooked public health issue.
From a public health perspective, pubic hair removal has been implicated in the spread of certain sexually transmitted infections; however, the evidence has largely been anecdotal or limited to case reports 11, 5, 12. Pubic hair removal has also been associated with a decreased incidence of pubic lice 13.
Pubic hair removal can be accomplished by shaving, waxing, trimming with scissors or clippers, and/or tweezing. Herbenick et al. 11 in a cross-sectional Internet-based survey of women aged 18–68 years, found that of those who had removed pubic hair ≥1 time in the previous month, ≤67% used razors, 6% waxed, and 1%–2% had undergone electrolysis or laser hair removal. These rates varied by age group as did the frequency and extent of pubic hair removal. Other studies have reported similar distributions of products used.6 Although the safety of certain personal use depilatory products such as hot wax have been questioned 14, genital injury from grooming products is largely unstudied. Minor complications, such as painful irritation, erythema, or folliculitis are not uncommon 15; however, severe complications after pubic hair removal, such as bacterial sepsis 16, have been reported.
From survey data, partial or complete pubic hair removal has been reported by upward of 70%–88% of young women in the United States 17. Similar findings have been reported from both Australia 18, New Zealand 19 and the United Kingdom 20. The data demonstrated that substantial proportions of both women and men remove body hair from many sites. However, gendered differences remain, and a key dimension of gendered difference appears in the concept of flexible choice around body hair removal or retention. This was seen in the difference between perceived acceptability of having body hair (81% for men, 11% for women). These findings suggest that although men, like women, are now coming under some pressure to remove body hair, there is still a great difference in men and women’s capacity to choose whether to follow it. Investigators have also assessed the prevalence of pubic hair depilation practices in gay and heterosexual men, and 58%–78% reported regular partial or complete pubic hair removal 21. Until the 1980s, it was considered normal for women to shave only the bikini zone and armpits, while the latest trend, especially among younger women, is total pubic hair removal 22. Although women’s total removal of their pubic hair has been described as a “new norm,” this study involving 2,451 women ages 18 to 68 years 22 reported a diverse range of pubic hair-grooming practices. Women’s total removal of their pubic hair was associated with younger age, sexual orientation, sexual relationship status, having received cunnilingus in the past 4 weeks, and higher scores on the Female Genital Self-Image Scale and Female Sexual Function Index (with the exception of the orgasm subscale). Findings from that study 22. Although women’s total removal of their pubic hair has been described as a “new norm,” this study involving 2,451 women ages 18 to 68 years 22 suggest that pubic hair styles are diverse and that it is more common than not for women to have at least some pubic hair on their genitals. In addition, total pubic hair removal was associated with younger age, being partnered (rather than single or married), having looked closely at one’s own genitals in the previous month, cunnilingus in the past month, and more positive genital self-image and sexual function. This trend can be observed in magazines like Playboy, which demonstrate a transition from completely hairy pubic areas to different degrees of shaving and, finally, to total pubic hair removal 23.
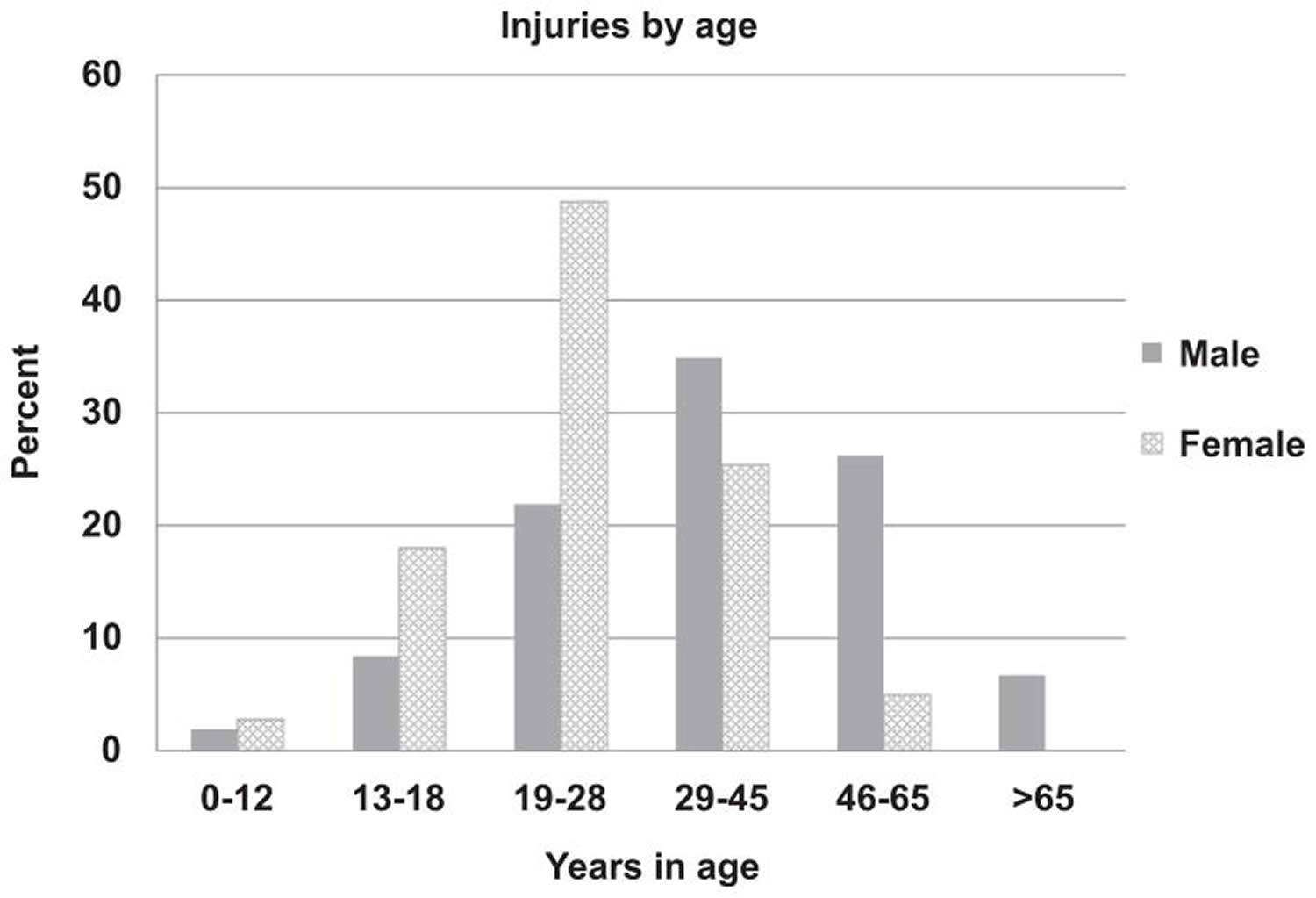
Body hair removal practices are potentially influenced by a variety of factors, including sex, age, partner and sexual activity status, sexual orientation, and body image 17. Not surprisingly, the demographic group largely purported to remove pubic hair—young women—had the greatest injury prevalence. Studies have found that more than one-half of all genitourinary injuries due to pubic hair removal were in women, who also had a younger age distribution, because about one-half were 19–28 years and 21% were ≤18 years old. One report, which surveyed women in a gynecologic clinic, found that >70% of adolescent girls aged 12–20 years routinely shaved or waxed their pubic hair 17. In an Internet-based survey completed by 2451 women aged 18–68 years, total pubic hair (vs partial) removal was associated with younger age 11. Pubic hair growth in both men and women peaks in the mid-20s and later declines 24. Increased hair growth at these earlier ages may in part explain a greater prevalence of grooming in younger ages.
At-home pubic hair removal is typically accomplished by shaving, waxing, trimming with scissors or clippers, or tweezing. Although minor adverse events, such as rash, folliculitis, pain, or irritation, have been reported after at-home hair removal techniques,10 case reports of subacute complications after pubic hair removal, such as methicillin-resistant Staphylococcus aureus infection 25 or follicular keratosis requiring excision 26, have been reported. Abscess was the primary diagnosis identified in 15.6% of that cohort, with patients typically presenting a various number of days after grooming. Systemic or life-threatening injuries associated with grooming products have been reported in published studies. Dendle et al 15 described a 20-year-old Australian woman with poorly controlled type 1 diabetes who developed life-threatening sepsis with Streptococcus pyogenes and Herpes simplex after undergoing complete pubic hair removal with hot wax.
Although few published reports have described the effect of grooming practices on external genital injury, the U.S. Consumer Products Safety Commission issued a Hazards Screening Report in 2005 27, describing injuries related to “personal use” products from 1997 to 2003. Individual product categories included electric grooming devices, unpowered grooming devices, and grooming devices nonspecified, in addition to other categories such as clothing, eye glasses, and shopping carts. An estimated 506,650 injuries due to personal items occurred in 2003, with 5.0% requiring hospitalization and 370 deaths (none related to hair removal devices). Although the hazards report estimated 285.5 million electric grooming products were in use in U.S. households in 2003, it is unknown what portion were hair removal devices. Thus, because genital hair removal is a relatively common practice, the overall injury rate has been very low. Nevertheless, emergency department doctors have found a sharp increase in the number of both men and women who presented to U.S. emergency departments with genitourinary injury in recent years 2. In a national stratified probability sample of consumer product-related injuries presenting to U.S. emergency departments, doctors found a modest rate of genitourinary injuries related to grooming product usage (3% of all genitourinary injuries documented). Injuries occurred slightly more often in women (56.7%). When stratified by sex, differences in product type and injury diagnosis were observed. For both sexes, the number of incident cases increased approximately linearly during the study period but was most dramatic among women.
Depilatory practices account for a small portion of genitourinary injuries presenting to U.S. hospital emergency departments. Most injuries are related to nonelectric razors, are minor, and are managed with outpatient treatment. The demographics of patients with genitourinary injuries from grooming products largely parallel observations about cultural changes and grooming practices in the United States. Although hair removal products account for a small proportion of genitourinary injuries, the increasing number of incidents in both men and women is an important concern for healthcare practitioners.
Figure 1. Percentage of grooming injuries stratified by age category
The proportion of products involved in the injuries is presented in Table 1. Nonelectric razors were involved in 9,600 or 81.9% of the injuries. Electric razors were implicated in 0.7% of the injuries overall and were associated with laceration, rash, or unspecified injury diagnoses. Hot wax was involved in 1.4% of injuries, and a small proportion of these involved the use of both hot wax and a nonelectric razor, which resulted in nonspecific pubic or external genital injury. The proportion of scissors-related injury was greater for men than for women (21.6% vs 6.7%). Furthermore, injury resulting from hair clippers was only reported for men, and injury from shaving cream and hot wax-related injuries was only reported for women. In a small study of depilatory wax burns from the Royal Adelaide Hospital, Australia 14 found patients with burn injury as a result of using microwave-heated hair removal wax products in a domestic setting. The pilot study revealed an increase in wax temperature with the number of times the wax was heated. During definitive wax temperature testing, the maximum wax temperature recorded was 227.3 °F (108.5 °C). Seventeen of 60 wax surface temperatures recorded exceeded 194 °F (90 °C), 9 exceeded 212 °F (100°C). Ninety-three percent of the stirred wax temperatures showed an increase in wax temperature with an increase in microwave power output. The results of that study 14 show that when heating hair removal wax in the microwave according to manufacturer’s instructions, wax temperatures regularly reach unsafe working temperatures. As microwave output power increased, wax temperature also increased. Of the 9 wax temperature measurements that reached over 212 °F (100°C), 8 of them were heated in the 1200-Watts microwave. The results from that study show that the wax heats unevenly, as different areas of the wax surface heated to different temperatures, once mixed the temperature dropped significantly. It was observed that areas of wax at a higher temperature were less viscous with a greater tendency to spill. Given that the majority of burns resulted from wax spillage during removal from the microwave, the packaging of all microwave-heated hair removal wax products should warn that, following heating, the surface wax will become hotter and less viscous than the wax below, and the container may become less rigid and too hot to hold. This should be accompanied by a recommendation that wax is heated on a microwave-safe plate to reduce spillage, and the wax be stirred before use. Heating instructions should include appropriate microwave wattage for heating, an indicator when the wax is too hot for use—for example, a thermometer or color indicator—and detailed instructions for heating and reheating when the container is of varying fullness. Before the most common injury involved the hands (76%), additional safety instructions suggesting that the hot product is removed from the microwave using “oven gloves” might prevent most injuries. Also included should be a warning of the risk of burn injury and simple but appropriate first aid instructions. Most burn injury caused by hair removal wax is preventable, but requires user awareness as well as appropriate warnings and first aid instruction to be provided.
Table 1. Number of product-associated injuries with pubic hair shaving
| Men | Women | ||||
| Actual | Estimate (%) | Actual | Estimate (%) | ||
| Razors (nonelectric) | 100 | 3668 (72.3) | 178 | 5914 (89.2) | |
| Razors (electric) | 3 | 47 (0.9) | 2 | 30 (0.5) | |
| Wax (with razor) | 0 | 0 (0) | 2 | 31 (0.5) | |
| Wax (without razor) | 0 | 0 (0) | 2 | 141 (2.1) | |
| Scissors | 25 | 1097 (21.6) | 13 | 443 (6.7) | |
| Hair clippers | 9 | 262 (5.2) | 0 | 0 (0) | |
| Shaving cream | 0 | 0 (0) | 1 | 71 (1.1) | |
The most common site of injury was the external female genitalia ~36.0% (Table 2). Perineal/perianal injury was noted in 7 of the 132 (5%) actual cases of external female genital injury according to a review of narrative reports. External male genitalia constituted 34.5% of all genitourinary injuries, reflecting a scrotal, penile, and genital not otherwise specified injury rate of 21.8%, 11.8%, and 2.0%, respectively. No documentation of urethral or internal genitourinary organ injury was found.
Table 2. Pubic hair removal and shaving injury incidents stratified by genitourinary site
| Location | Actual | Estimate (%) |
| External female genitalia | 132 | 4208 (36.0) |
| Female pubic not otherwise specified | 65 | 2347 (20.0) |
| Scrotum | 64 | 2557 (21.8) |
| Penis | 37 | 1385 (11.8) |
| Male genitalia not otherwise specified | 5 | 236 (2.0) |
| Male pubic not otherwise specified | 32 | 972 (8.3) |
Tips for shaving pubic hair
If you are considering shaving or grooming your pubic hair, you should use electric hair clippers instead of nonelectric razor to prevent injury and reduce the risk of microscopic lacerations or abrasions to the skin.
Shaving pubic hair women
Pubic hair removal in women is associated with younger ages, receiving cunnilingus, and a positive genital self-image 10. Grooming was associated with modestly higher genital satisfaction but this relationship did not persist after multivariable analysis. While female body hair removal is generally practiced according to psychosocial reasons regardless of the body part the hair being removed from, genital hair removal does have health risks because pubic hair has a definite biological purpose as a safety net to protect the vulva from bacterial infections 28. A study based on data from the “National Electronic Injury Surveillance System” showed that the number of emergency room consultations due to genital injuries after shaving increased 5-fold from 2002 to 2010 29. The authors stated that 81.9% of the injuries were caused by nonelectric shaving methods. The long-term consequences of these injuries are not yet clear 29. Another study gathered data from 1110 college students in the United States, who reported on the complications they experience during genital shaving, namely, pain, rash, cuts, and itching with genital itching as the most common complication of genital hair removal being reported by 80.2% of the participants in this study 30. The Federal Center of Health Education in Germany, with the University of Hamburg, interviewed 160 teenagers aged 16–19 years and found that 94% of the female and 81% of the male participants shaved their pubic hair 31. A study at the University of Leipzig in 2009 investigated the shaving patterns of 2,512 young participants aged 18–25. In this study, 88% of female and 67% of male participants admitted to practicing partial or total pubic hair shaving. This trend strongly declined at the beginning of the 31st year of age 32.
Pubic hair removal may be a risk factor for vulvar intraepithelial neoplasia (VIN) or correlated with the increasing incidence of vulvar intraepithelial neoplasia (VIN) 33. Researchers noticed that the women with vulvar dysplasia or vulvar cancer reported that they completely or partially shave their pubic hair more often and experienced recurrent inflammation. These results are in accordance with those of a previous study 32, which showed that shaving the pubic hair leads to a 4-fold increase in the risk of vulvar dysplasia or cancer.
Complete shaving and shaving only the labia majora were correlated to the occurrence of dysplasia and cancer more frequently than those who did not perform this extent of shaving. The correlation between age and the degree of shaving in our study was similar to that reported by a previous study 32.
Women who completely shave their pubic hair or shave the labia majora show more correlation with developing vulvar dysplasia and cancer. A possible explanation for this may be that shaving the genitals leads to an increased risk of inflammation. This would also account for the higher rates of vulvar intraepithelial neoplasia and cancer in the anterior commissure 34. Other means of removing pubic hair, such as waxing, were not accessible to the participants in the rural area in northwestern Germany where the study was conducted. Therefore, this study could only analyze the impact of shaving and not other forms of hair removal 35.
Vulvar intraepithelial neoplasia was classified by the international society for the study of vulvovaginal disease in 2004 into the following categories 36:
- Classical vulvar intraepithelial neoplasia: including lesions formerly known as vulvar intraepithelial neoplasia II and vulvar intraepithelial neoplasia III, bowenoid, condylomatous, and mixed form
- Differentiated vulvar intraepithelial neoplasia: previously known as vulvar intraepithelial neoplasia of simple type.
Vulvar intraepithelial neoplasia presents clinically as elevated or flat vulvar lesions with a color that varies from white to grey or red to brown or black 37. Vulvar cancer appears as a vulvar lump or mass that might also be ulcerated 38.
Classical vulvar intraepithelial neoplasia is the most common form of vulvar dysplasia with an incidence of 5/100,000 women 39. The common age of patients at presentation is between 30 and 40 years. The progression rate of classical vulvar intraepithelial neoplasia to invasive cancer is 3.3–5.7% within 2.4 to 13.8 years 40. Differentiated vulvar intraepithelial neoplasia constitutes only 5–10% of all vulvar preinvasive lesions and is often found associated with lichen sclerosis 39. In 33% of cases, it progresses to vulvar carcinoma 39.
Shaving pubic hair men
Men’s hair removal practices are becoming mainstream, seen as a consequence of changing masculine norms and men’s relationships to their bodies. This is often presented as a straightforward ‘shift’ from men’s ideal bodies as naturally hairy, to increased hairlessness, and the consequence on men’s body concerns as inevitable. Although hairlessness is rapidly becoming a component of the ideal male body, little research has examined men’s concerns about their body hair or their hair removal practices 41. It is well documented that pubic hair grooming is associated with sexual activity and behavior in women 42. This study 43 identifies that the number one motivation for grooming among men of all ages was sex. Certain sexual behaviors, especially receiving and giving oral sex, are associated with grooming. The top three motivations for grooming include sex, hygiene, and routine care. Most men who remove their pubic hair groom the hair above the penis, the scrotum, and the penile shaft. Interestingly, in the multivariate model, higher frequency of sexual activity was not associated with greater odds of grooming. This suggests that, although men might groom for sex, other aspects of sexual behavior beyond frequency might influence grooming. In particular, oral sex seems to be associated with grooming in the current study as well as another study in women 10. Overall, pubic hair grooming in men is common and grooming is more common in younger men. The prevalence of pubic hair grooming (50.5%) in men reported in a Gaither et al. 43 study is similar to 63.6% men that was reported by Boroughs et al. 44.
Grooming may play a role in male body image, as many college males report grooming for a drive of muscularity and physical appearance 45. Perceived increase in physical appearance might be a reason that so many men groom for sex. Also, from Figure 2 below, about one in five men report grooming because it makes their penis look longer, which may be another reason that so many men groom for sex. A common reason for grooming in women is concerns about perspiration and odor 46. The focus on hygiene as a reason to groom may be a male equivalent of this concern. Whether grooming actually decreases perspiration and odor has not been studied. Pubic hair grooming may also be a reflection of a religious hygienic teaching 47.
No difference of self-reported baseline hairiness was found between men who have sex with men (gay men) and men who have sex with women 48. Compared with men who have sex with women, men who have sex with men were more likely to groom more than five times per year (42.5% vs. 29.0%), daily (2.4% vs. 1.3%), and to have completely removed all pubic hair more than five times (24.6% vs. 20.7%). Men who have sex with men reported grooming more for sex (76.5% vs. 67.9%) and for vacation (31.9% vs. 20.5%). Men who have sex with men were less likely to prefer their partner to be groomed (42.8% vs. 63.3%). Hair on penile shaft, from penis to navel, scrotum, between scrotum and anus, around anus, and buttocks were areas groomed more often by men who have sex with men 48.
Figure 2. Reasons for male grooming by age in a nationally representative sample of U.S. men
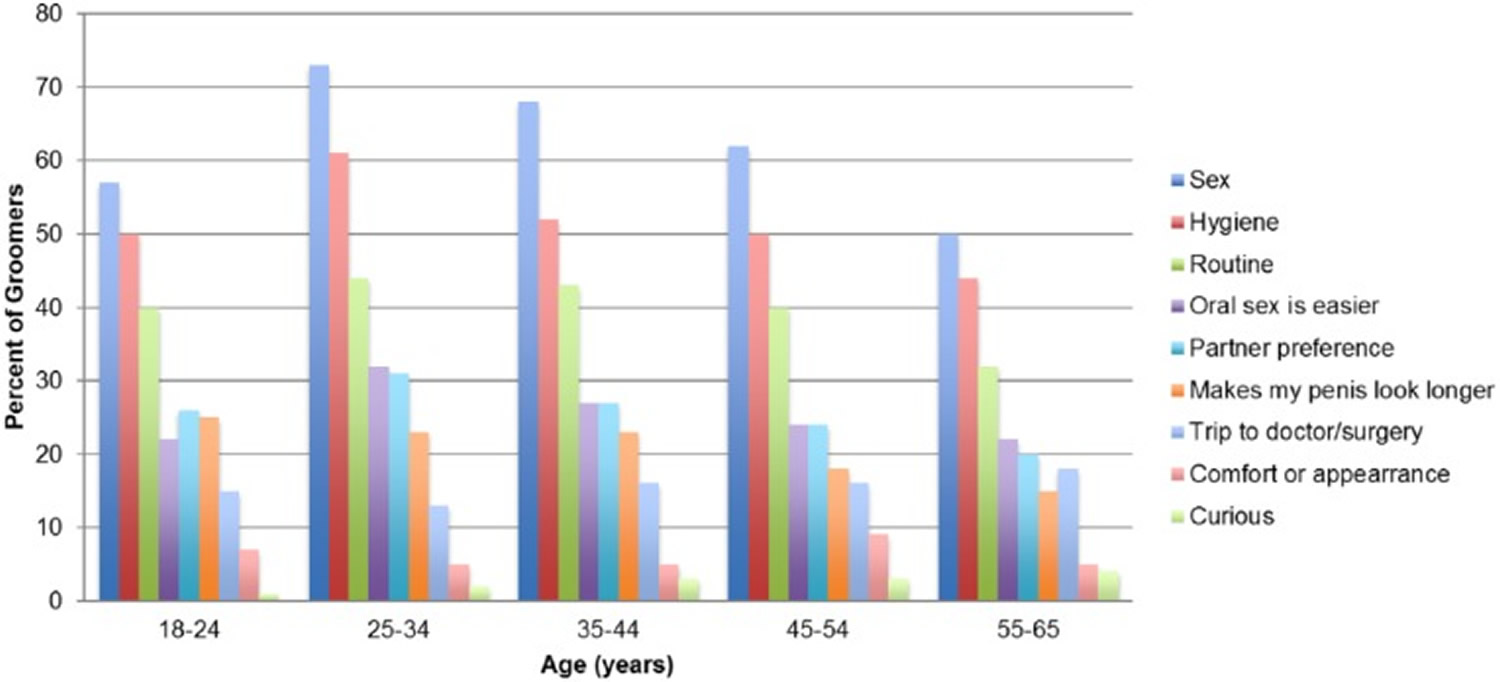
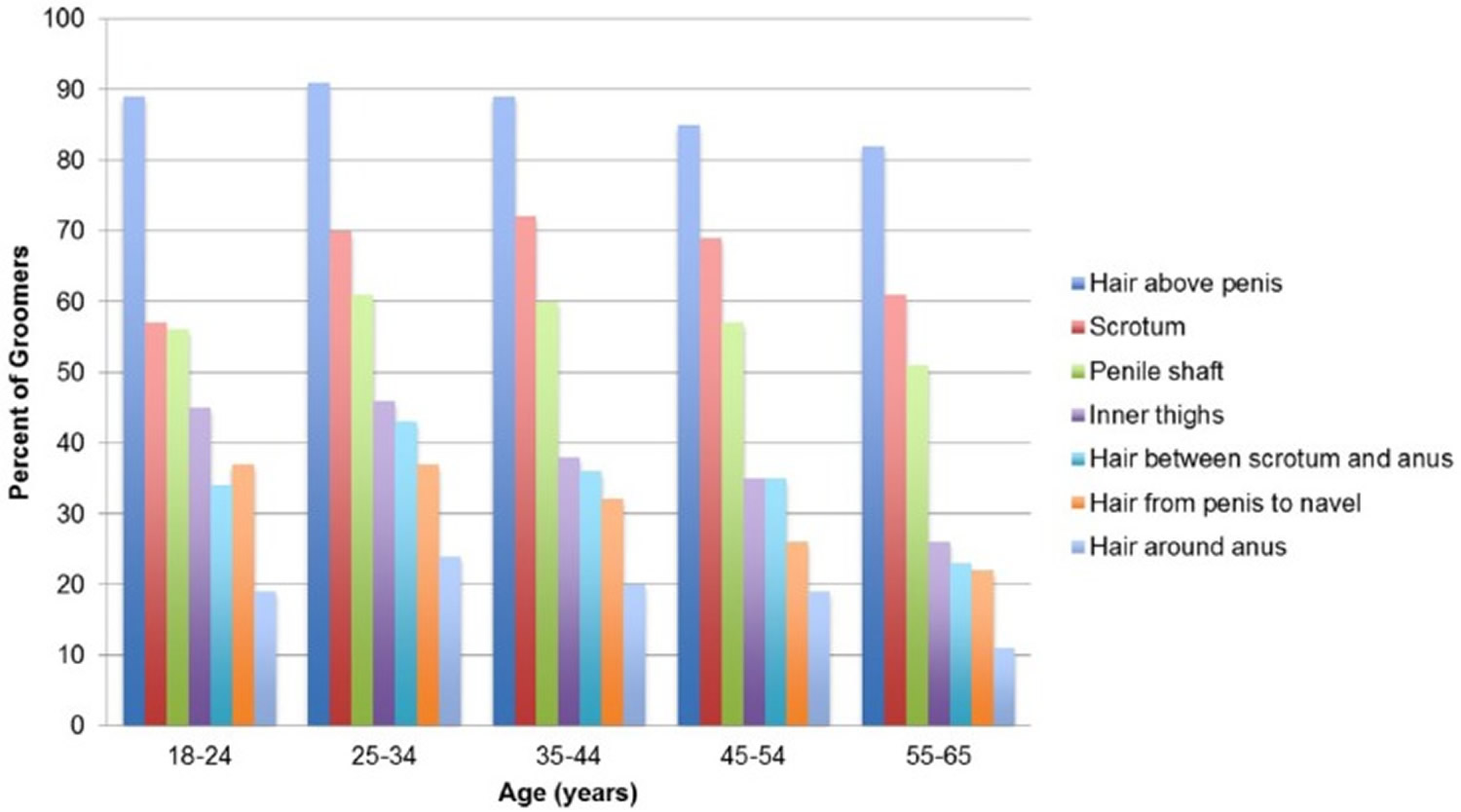
Figure 3. Areas men groom by age in a nationally representative sample of U.S. men
A nationally representative survey of non-institutionalized adults aged 18 to 65 years residing in the United States was conducted. Four thousand one hundred and ninety-eight men completed the survey. Of these men, 2,120 (50.5%) reported regular pubic hair grooming 43. Samples of gay and heterosexual men completed questionnaires that assessed whether they had ever removed their back, buttock or pubic hair, the frequency with which they did so, the methods used and their self-reported reasons for removing this hair, as well as their level of appearance investment. Results indicated that many gay and heterosexual men remove their back, buttock and pubic hair regularly and that their primary reason for doing so is to maintain or improve their appearance 41. Of the 4,062 men who completed the survey, 3,176 (78.2%) report having sex with only women, 198 (4.9%) report sex with men, and 688 (16.9%) report not being sexually active. Men who have sex with men are more likely to groom (42.5% vs. 29.0%) and groom more around the anus, scrotum, and penile shaft compared with men who have sex with only women. Men who have sex with men receptive partners groom more often (50.9% vs. 26.9%) and groom more for sex (85.3% vs. 51.9%) compared with men who have sex with men insertive partners.
The prevalence of grooming decreases with age. Adjusting for sexual frequency and sexual orientation, grooming is associated with performing and receiving oral sex. The majority of men report grooming in preparation for sexual activity with a peak prevalence of 73% among men aged 25 to 34 years, followed by hygiene (61%) and routine care (44%) 43. The majority of men who remove their pubic hair groom the hair above the penis (87%), followed by the scrotum (66%) and the penile shaft (57%) 43. Overall, pubic hair grooming is common among men aged 18 to 65 years in the United States 43. Younger ages are associated with greater rates of pubic hair grooming. Many men groom for sex, in particular oral sex, as well as for routine care and hygiene 43.
Table 3. Comparison of demographic characteristics between men groomers and nongroomers
| Groomers, n = 2,120 | Nongroomers, n = 2,034 | |
| Age | 41.1 (40.6-41.6) | 48.0 (47.5-48.6) |
| Race/ethnicity | ||
| White | 1,416 (66.8) | 1,407 (69.2) |
| Black | 215 (10.1) | 288 (14.2) |
| Other, non-Hispanic | 84 (4.0) | 63 (3.1) |
| Hispanic | 330 (15.6) | 214 (10.5) |
| Mixed races | 75 (3.6) | 62 (3.1) |
| Education | ||
| Less than high school | 110 (5.2) | 141 (6.9) |
| High school graduate | 557 (26.3) | 648 (31.9) |
| Some college | 610 (28.8) | 530 (26.1) |
| Bachelor’s degree or higher | 843 (39.8) | 715 (25.2) |
| Income ($) | ||
| <50,000 | 740 (34.9) | 814 (40.0) |
| 50,000-74,999 | 452 (21.2) | 399 (19.6) |
| 75,000-99,999 | 363 (17.1) | 310 (15.2) |
| >100,000 | 565 (26.7) | 511 (25.1) |
| Marital status | ||
| Married/living with partner | 1,391 (65.6) | 1,328 (65.3) |
| Widowed | 15 (0.7) | 25 (1.2) |
| Divorced/separated | 197 (9.3) | 194 (9.5) |
| Never married | 517 (24.4) | 487 (23.9) |
| Location | ||
| Northeast | 356 (16.8) | 354 (17.4) |
| Midwest | 543 (25.6) | 517 (25.4) |
| South | 740 (34.9) | 711 (35.0) |
| West | 481 (22.7) | 452 (22.2) |
| Other | ||
| Baseline hairinessa | 3.99 (3.94-4.05) | 3.84 (3.78-3.90) |
| Partner hairinessa | 2.26 (2.18-2.33) | 2.19 (2.11-2.27) |
| Genital satisfaction a | 4.92 (4.88-4.97) | 4.78 (4.74-4.83) |
Note: aMeasured via Likert-type scales (1-7), genital satisfaction measured using the Index of Male Genital Image.
[Source 43]Men who have sex with men report more injuries to the anus (7.0% vs. 1.0%), more grooming-related infections (7.0% vs. 1.0%) and abscesses (8.8% vs. 2.5%), as well as lifetime sexually transmitted infections (STIs) 48 compared with men who have sex with only women. More receptive partners report grooming at the time of their sexually transmitted infection (52.2% vs. 14.3%) compared with insertive partners. Sexual orientation, and in particular sexual role, may influence male grooming behavior and impact grooming-related injuries and infections. Anogenital grooming may put one at risk for an sexually transmitted infection.
Male injuries constituted a substantial portion of the cohort and were found to increase at a rate that paralleled female grooming injuries. This finding is congruent with contemporary studies that report relatively high pubic hair removal among men 21. More men who have sex with men reported never sustaining a grooming injury compared with men who have sex with women (65.9% vs. 79.0%); however, no differences were observed for total lifetime grooming injuries between the two groups. men who have sex with men had more grooming injuries involving scissors (28.6% vs. 12.8%) and reported more injuries to the anus (7.0% vs. 1.0%). men who have sex with men sought more medical treatment for injuries than men who have sex with women (8.8% vs. 1.3%). Infections (7.0% vs. 1.0%) and abscesses (8.8% vs. 2.5%) were more common injury types in men who have sex with men (Table 4).
Table 4. Grooming injuries in men
| Men who have sex with men and women* (n = 198, 4.9%) | Men who have sex with women (n = 3,176, 78.2%) | |
| Experienced grooming injury | ||
| Yes | 110 (65.9%) | 1,652 (79.0%) |
| Number of grooming injuries | 7.24 ± 9.49 | 6.03 ± 8.73 |
| Instrument used | ||
| Nonelectric blade | 30 (57.7%) | 168 (52.0%) |
| Electric razor | 29 (56.2%) | 209 (40.5%) |
| Scissors | 12 (28.6%) | 41 (12.8%) |
| Wax/electrolysis/laser removal | 0 (0.0%) | 3 (1.0%) |
| Injury location | ||
| Scrotum | 29 (50.9%) | 296 (56.8%) |
| Penis | 13 (22.8%) | 141 (27.1%) |
| Anus | 4 (7.0%) | 5 (1.0%) |
| Perineum | 5 (8.8%) | 28 (5.4%) |
| Inner thigh | 10 (17.5%) | 57 (10.9%) |
| Pubis | 16 (28.1%) | 154 (29.6%) |
| Other | 0 (0.0%) | 13 (2.5%) |
| Sought medical treatment | ||
| Yes | 5 (8.8%) | 7 (1.3%) |
| Injury type | ||
| Burn | 13 (22.8%) | 84 (16.1%) |
| Rash | 20 (35.1%) | 155 (29.8%) |
| Laceration with blood | 37 (64.9%) | 355 (68.3%) |
| Injury requiring medical care | 0 (0.0%) | 4 (0.8%) |
| Infection | 4 (7.0%) | 5 (1.0%) |
| Abscess | 5 (8.8%) | 13 (2.5%) |
| Other | 7 (12.3%) | 43 (8.3%) |
Baseline skin infections and abscesses were reported more by men who have sex with men (12.7% vs. 4.7%). More men who have sex with men self-reported being diagnosed with MRSA (4.8%) than men who have sex with women (2.5%). men who have sex with men reported fewer regular sexual partners (64.5% vs. 87.3%), more sexual partners in a year and more sexual partners in a lifetime. The number of lifetime sexually transmitted infections (STIs) was higher in men who have sex with men than men who have sex with women (1.65 vs. 1.45). Compared with men who have sex with women, men who have sex with men report higher prevalence of HIV (20.8% vs. 0.4%), syphilis (23.7% vs. 6.8%), anal warts (9.7% vs. 1.1%) and less prevalence of genital herpes (herpes simplex virus [HSV]) (4.2% vs. 15.5%). No statistical differences were found between groups for chlamydia, human papillomavirus (HPV), gonorrhea or pubic lice. Grooming at the time of an sexually transmitted infection (STI) was more prevalent in men who have sex with men (45.2% vs. 11.5%). men who have sex with men were using more nonelectric blades to groom during the time of an STI (88.2% vs. 54.5%) (Table 5).
Table 5. Infections, number of sexual partners, and sexually transmitted infection (STI)
| Men who have sex with men and women* (n = 198, 4.9%) | Men who have sex with women (n = 3,176, 78.2%) | |
| Previous infections | ||
| Skin infections/abscesses | 21 (12.7%) | 102 (4.7%) |
| Diagnosed with MRSA | 8 (4.8%) | 51 (2.4%) |
| Regular sexual partner | ||
| Yes | 107 (64.5%) | 1,907 (87.3%) |
| Annual sexual partner (median, IQR)† | 2.81, 5.00 | 1.00, 0.00 |
| Lifetime sexual partners (median, IQR)† | 25.00, 65.00 | 6.00, 12.00 |
| Lifetime # of STI | 1.65 ± 0.67 | 1.45 ± 0.65 |
| Type of STI | ||
| HIV | 15 (20.8%) | 1 (0.4%) |
| Syphilis | 17 (23.7%) | 19 (6.8%) |
| Gonorrhea | 31 (43.7%) | 124 (44.8%) |
| Genital herpes (HSV) | 3 (4.2%) | 43 (15.5%) |
| Anal warts | 7 (9.7%) | 3 (1.1%) |
| Grooming at the time of STI | ||
| Yes | 28 (45.2%) | 22 (11.5%) |
| Grooming instrument at time of STI | ||
| Nonelectric blade | 23 (88.2%) | 12 (54.5%) |
| Electric razor | 17 (62.1%) | 12 (54.5%) |
| Scissors | 7 (25.0%) | 4 (18.2%) |
| Wax/electrolysis/laser removal | 0 (0.0%) | 0 (0.0%) |
Notes: HSV = herpes simplex virus; IQR = interquartile range; MSM = men who have sex with men; MSW = men who have sex with women; STI = sexually transmitted infection; MRSA = Methicillin-resistant Staphylococcus aureus
[Source 48]As seen in Table 5, the majority of injuries for both men who have sex with men and men who have sex with women were to the scrotum, pubis, or penis, which mirrors the results from our previous study, which showed these sites as the most common male genitourinary injury presenting to the emergency department from 2002 to 2010 49. These sites have thin, delicate skin with folds and surfaces that may be hard to visualize and makes these areas more prone to injury. Reserachers found that men who have sex with men had more injuries to the anus as well as more infections and abscesses due to their personal grooming (Table 5). This correlates with the finding that more than double the percentage of men who have sex with men groom the anal region compared with men who have sex with women, suggesting a potential connection between increased grooming frequency and injuries. Further research is required to understand if frequency, grooming instrument, or other mechanism lead to more injury.
Increased frequency of grooming, in particular removing all pubic hair among men who have sex with men, is associated with increased prevalence of infections and abscesses. Removing pubic hair may lead to microscopic lacerations and abrasions, which could predispose an individual to infection. Although the number of grooming injuries between men who have sex with men and men who have sex with women did not differ, men who have sex with men did seek more medical attention for their injuries. Increased reported infections and abscesses due to pubic hair grooming in men who have sex with men might be a reason for seeking medical advice.
Increased infections and number of sexually transmitted infection in men who have sex with men, particularly HIV, are well documented in the literature 50 and study results confirm this. Men who have sex with men had higher rates of HIV, syphilis, and anal warts (Table 5). Receptive partners had higher rates of HIV and syphilis (Table 5). HIV has a high probability of transmission via receptive anal intercourse 50 and although higher rates among receptive partners were of borderline significance, it supports this idea. Interestingly, more than four times as many men who have sex with men were grooming at the time of sexually transmitted infection and using nonelectric blades to groom. This could result from the baseline increase in grooming in men who have sex with men that grooming might predicate riskier sexual behavior or that grooming actually increases the likelihood of an sexually transmitted infection. Still, the use of nonelectric blades to groom in men who have sex with men may not be advisable. Going further, three times as many receptive partners reported grooming at the time of sexually transmitted infection. As such, sexual role and grooming together may harbor an environment for an sexually transmitted infection infection; however, given the small sample size, the results are inconclusive. The role of grooming and the risk of acquiring an sexually transmitted infection are still uncertain and require further study with more robust controls with assessment of safe sex behavior. However, electric razors may be safer for anogenital grooming.
- Pubic Hair and Sexuality: A Review. The Journal of Sexual Medicine Volume 6, Issue 8, August 2009, Pages 2102-2110. https://www.sciencedirect.com/science/article/pii/S1743609515326242[↩][↩][↩]
- Glass AS, Bagga HS, Tasian GE, et al. Pubic Hair Grooming Injuries Presenting to U.S. Emergency Departments. Urology. 2012;80(6):1187-1191. doi:10.1016/j.urology.2012.08.025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3559025/[↩][↩][↩][↩][↩]
- The influence of sexual orientation and sexual role on male grooming-related injuries and infections. Gaither TW, Truesdale M, Harris CR, Alwaal A, Shindel AW, Allen IE, Breyer BN. J Sex Med. 2015 Mar; 12(3):631-40. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4599875/[↩][↩][↩]
- Schoolgirls and soccer moms: a content analysis of free “teen” and “MILF” online pornography. Vannier SA, Currie AB, O’Sullivan LF. J Sex Res. 2014; 51(3):253-64. https://www.ncbi.nlm.nih.gov/pubmed/24228745/[↩][↩]
- Schick VR, Rima BN, Calabrese SK. Evulvalution: the portrayal of women’s external genitalia and physique across time and the current Barbie doll ideals. J Sex Res. 2011;48:74–81 https://www.ncbi.nlm.nih.gov/pubmed/19916105[↩][↩]
- Herbenick D, Hensel D, Smith NK, Schick V, Reece M, Sanders SA, Fortenberry JD. Pubic hair removal and sexual behavior: Findings from a perspective daily diary study of sexually active women in the United States. J Sex Med. 2013;10:678–685 https://www.ncbi.nlm.nih.gov/pubmed/23237246[↩]
- Boroughs MS, Thompson JK. Correlates of body depilation: An exploratory study into the health implications of body hair reduction and removal among college-aged men. Am J Mens Health. 2013;8:217–225 https://www.ncbi.nlm.nih.gov/pubmed/24128670[↩]
- Hair today, gone tomorrow: a comparison of body hair removal practices in gay and heterosexual men. Martins Y, Tiggemann M, Churchett L. Body Image. 2008 Sep; 5(3):312-6. https://www.ncbi.nlm.nih.gov/pubmed/18586585/[↩][↩]
- Pubic hair and sexuality: a review. Ramsey S, Sweeney C, Fraser M, Oades G. J Sex Med. 2009 Aug; 6(8):2102-10. https://www.ncbi.nlm.nih.gov/pubmed/19453886/[↩]
- Pubic hair removal among women in the United States: prevalence, methods, and characteristics. Herbenick D, Schick V, Reece M, Sanders S, Fortenberry JD. J Sex Med. 2010 Oct; 7(10):3322-30. https://www.ncbi.nlm.nih.gov/pubmed/20646183/[↩][↩][↩]
- Herbenick D, Schick V, Reece M, et al. Pubic hair removal among women in the United States: prevalence, methods, and characteristics. J Sex Med. 2010;7:3322–3330 https://www.ncbi.nlm.nih.gov/pubmed/20646183[↩][↩][↩]
- Trager JD. Pubic hair removal—pearls and pitfalls. J Pediatr Adolesc Gynecol. 2006;19:117–123. https://www.ncbi.nlm.nih.gov/pubmed/16624702[↩]
- Armstrong NR, Wilson JD. Did the “Brazilian” kill the pubic louse? Sex Transm Infect. 2006;82:265–266 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2564756/[↩]
- Chang AC, Watson KM, Aston TL, Wagstaff MJ, Greenwood JE. Depilatory Wax Burns: Experience and Investigation. Eplasty. 2011;11:e25. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3098007/[↩][↩][↩]
- Dendle C, Mulvey S, Pyrlis F, et al. Severe complications of a “Brazilian” bikini wax. Clin Infect Dis. 2007;45:e29–e31 https://www.ncbi.nlm.nih.gov/pubmed/17599301[↩][↩]
- U.S. Consumer Product Safety Commission. NEISS: National Electronic Injury Surveillance System, A Tool for Researchers. https://www.cpsc.gov/[↩]
- Bercaw-Pratt JL, Santos XM, Sanchez J, et al. The incidence, attitudes and practices of the removal of pubic hair as a body modification. J Pediatr Adolesc Gynecol. 2011;25:12–14 https://www.ncbi.nlm.nih.gov/pubmed/22088314[↩][↩][↩]
- Tiggemann M, Hodgson S. The hairlessness norm extended: reasons for and predictors of women’s body hair removal at different body sites. Sex Roles. 2008;59:889–897[↩]
- To let hair be, or to not let hair be? Gender and body hair removal practices in Aotearoa/New Zealand. Body Image Volume 10, Issue 4, September 2013, Pages 599-606. https://www.sciencedirect.com/science/article/abs/pii/S174014451300079X[↩]
- Toerin K, Wilkinson S, Choi PYL. Body hair removal: the “mundane” production of normative femininity. Sex Roles. 2005;52:399–406[↩]
- Martins Y, Tiggemann M, Churchett L. Hair today, gone tomorrow: a comparison of body hair removal practices in gay and heterosexual men. Body Image. 2008;5:312–316 https://www.ncbi.nlm.nih.gov/pubmed/18586585[↩][↩]
- Pubic hair removal among women in the United States: prevalence, methods, and characteristics. Herbenick D, Schick V, Reece M, Sanders S, Fortenberry JD. J Sex Med. 2010 Oct; 7(10):3322-30. https://www.jsm.jsexmed.org/article/S1743-6095(15)32732-6/fulltext[↩][↩][↩][↩]
- Evulvalution: the portrayal of women’s external genitalia and physique across time and the current barbie doll ideals. Schick VR, Rima BN, Calabrese SK. J Sex Res. 2011 Jan; 48(1):74-81. https://www.ncbi.nlm.nih.gov/pubmed/19916105/[↩]
- Androgens, hair loss and eugenics: a tale of discovery and American social history. Ayob SM, Messenger AG. Exp Dermatol. 2015 Jun; 24(6):412-3 https://www.ncbi.nlm.nih.gov/pubmed/25808933/[↩]
- Begier EM, Frenette K, Barrett NL, et al. A high-morbidity outbreak of methicillin-resistant Staphylococcus aureus among players on a college football team, facilitated by cosmetic body shaving and turf burns. Clin Infect Dis. 2004;39:1446–1453 https://www.ncbi.nlm.nih.gov/pubmed/15546080[↩]
- Roth LM, Look KY. Inverted follicular keratosis of the vulvar skin: a lesion that can be confused with squamous cell carcinoma. Int J Gynecol Pathol. 2000;19:369–373 https://www.ncbi.nlm.nih.gov/pubmed/11109167[↩]
- Marcy N, Rutherford G. Hazards Screening Report: Personal Use Items. U.S. Consumer Product Safety Commission; 2005 https://www.cpsc.gov [↩]
- Tiggemann M., Hodgson S. The hairlessness norm extended: reasons for and predictors of women’s body hair removal at different body sites. Sex Roles. 2008;59(11-12):889–897. doi: 10.1007/s11199-008-9494-3[↩]
- Glass A. S., Bagga H. S., Tasian G. E., et al. Pubic hair grooming injuries presenting to U.S. emergency departments. Urology. 2012;80(6):1187–1191. doi: 10.1016/j.urology.2012.08.025 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3559025/[↩][↩]
- Butler S. M., Smith N. K., Collazo E., Caltabiano L., Herbenick D. Pubic hair preferences, reasons for removal, and associated genital symptoms: comparisons between men and women. Journal of Sexual Medicine. 2015;12(1):48–58. doi: 10.1111/jsm.12763 https://www.ncbi.nlm.nih.gov/pubmed/25394526[↩]
- Matthiesen S., Mainka J. Bundeszentrale für gesundheitliche Aufklärung—Forum Sexualaufklärung und Familienplanung. 2011. Intimrasur als neue Köpernorm bei Jugendlichen; pp. 25–29.[↩]
- Universität Leipzig: Körperhaarentfernung bei immer mehr jungen Erwachsenen im Trend, 2008.[↩][↩][↩]
- Schild-Suhren M, Soliman AA, Malik E. Pubic Hair Shaving Is Correlated to Vulvar Dysplasia and Inflammation: A Case-Control Study. Infectious Diseases in Obstetrics and Gynecology. 2017;2017:9350307. doi:10.1155/2017/9350307. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5591962/[↩]
- Hampl M. Invasives Vulvakarzinom und Präkanzerosen. Der Gynäkologe. 2015;48(6):440–450. doi: 10.1007/s00129-015-3708-x[↩]
- Schild-Suhren M, Soliman AA, Malik E. Pubic Hair Shaving Is Correlated to Vulvar Dysplasia and Inflammation: A Case-Control Study. Infectious Diseases in Obstetrics and Gynecology. 2017;2017:9350307. doi:10.1155/2017/9350307 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5591962[↩]
- Sideri M., Jones R. W., Wilkinson E. J., et al. Squamous vulvar intraepithelial neoplasia: 2004 modified terminology, ISSVD vulvar oncology subcommittee. Obstetrical & Gynecological Survey. 2006;61(3):174–175. doi: 10.1097/01.ogx.0000201921.69949.10 https://www.ncbi.nlm.nih.gov/pubmed/16419625[↩]
- American College of Obstetrics and Gynecology. Committee opinion No. 675 summary: management of vulvar intraepithelial neoplasia. Obstetrics & Gynecology. 2016;128(4):937–938. doi: 10.1097/AOG.0000000000001704 https://www.ncbi.nlm.nih.gov/pubmed/27661648[↩]
- Alkatout I., Schubert M., Garbrecht N., et al. Vulvar cancer: epidemiology, clinical presentation, and management options. International Journal of Women’s Health. 2015;7:305–313. doi: 10.2147/IJWH.S68979 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4374790/[↩]
- van de Nieuwenhof H. P., van der Avoort I. A. M., de Hullu J. A. Review of squamous premalignant vulvar lesions. Critical Reviews in Oncology/Hematology. 2008;68(2):131–156. doi: 10.1016/j.critrevonc.2008.02.012 https://www.ncbi.nlm.nih.gov/pubmed/18406622[↩][↩][↩]
- van de Nieuwenhof H. P., Massuger L. F. A. G., van der Avoort I. A. M., et al. Vulvar squamous cell carcinoma development after diagnosis of VIN increases with age. European Journal of Cancer. 2009;45(5):851–856. doi: 10.1016/j.ejca.2008.11.037 https://www.ncbi.nlm.nih.gov/pubmed/19117749[↩]
- Martins Y, Tiggemann M, Churchett L. Hair today, gone tomorrow: a comparison of body hair removal practices in gay and heterosexual men. Body Image. 2008;5:312–316 https://www.sciencedirect.com/science/article/abs/pii/S1740144508000508[↩][↩]
- Prevalence and correlates of pubic hair grooming among low-income Hispanic, Black, and White women. DeMaria AL, Berenson AB. Body Image. 2013 Mar; 10(2):226-31. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3643298/[↩]
- Gaither TW, Awad MA, Osterberg EC, Rowen TS, Shindel AW, Breyer BN. Prevalence and Motivation: Pubic Hair Grooming Among Men in the United States. American Journal of Men’s Health. 2017;11(3):620-640. doi:10.1177/1557988316661315. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5675231/[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Boroughs M., Cafri G., Thompson J. (2005). Male body depilation: Prevalence and associated features of body hair removal. Sex Roles, 52, 637-644[↩]
- Correlates of body depilation: an exploratory study into the health implications of body hair reduction and removal among college-aged men. Boroughs MS, Thompson JK. Am J Mens Health. 2014 May; 8(3):217-25. https://www.ncbi.nlm.nih.gov/pubmed/24128670/[↩]
- Riddell L., Varto H., Hodgson Z. (2010). Smooth talking: The phenomenon of pubic hair removal in women. Canadian Journal of Human Sexuality, 19, 121-130[↩]
- Pfluger-Schindlbeck I. (2006). On the symbolism of hair in Islamic societies: An analysis of approaches. Anthropology of the Middle East, 1(2), 72-88.[↩]
- Gaither TW, Truesdale M, Harris CR, et al. The Influence of Sexual Orientation and Sexual Role on Male Grooming-Related Injuries and Infections. The journal of sexual medicine. 2015;12(3):631-640. doi:10.1111/jsm.12780. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4599875/[↩][↩][↩][↩][↩]
- Glass AS, Bagga HS, Tasian GE, Fisher PB, McCulloch CE, Blaschko SD, McAninch JW, Breyer BN. Pubic hair grooming injuries presenting to U.S. emergency departments. Urology. 2012;6:1187–1191. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3559025/[↩]
- Beyrer C, Baral SD, van Griensven F, Goodreau SM, Chariyalertsak S, Wirtz AL, Brookmeyer R. Global epidemiology of HIV infection in men who have sex with men. Lancet. 2012;380:367–377. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3805037/[↩][↩]


{kind=link}