Contents
- What is sigmoid colon
- Sigmoid colon anatomy
- How long is the sigmoid colon?
- Where is the sigmoid colon located?
- Sigmoid colon function
- Sigmoid volvulus
- Diverticulosis in the sigmoid colon
- Sigmoid colon cancer
- Sigmoid colon resection
- Sigmoid colon polyp
What is sigmoid colon
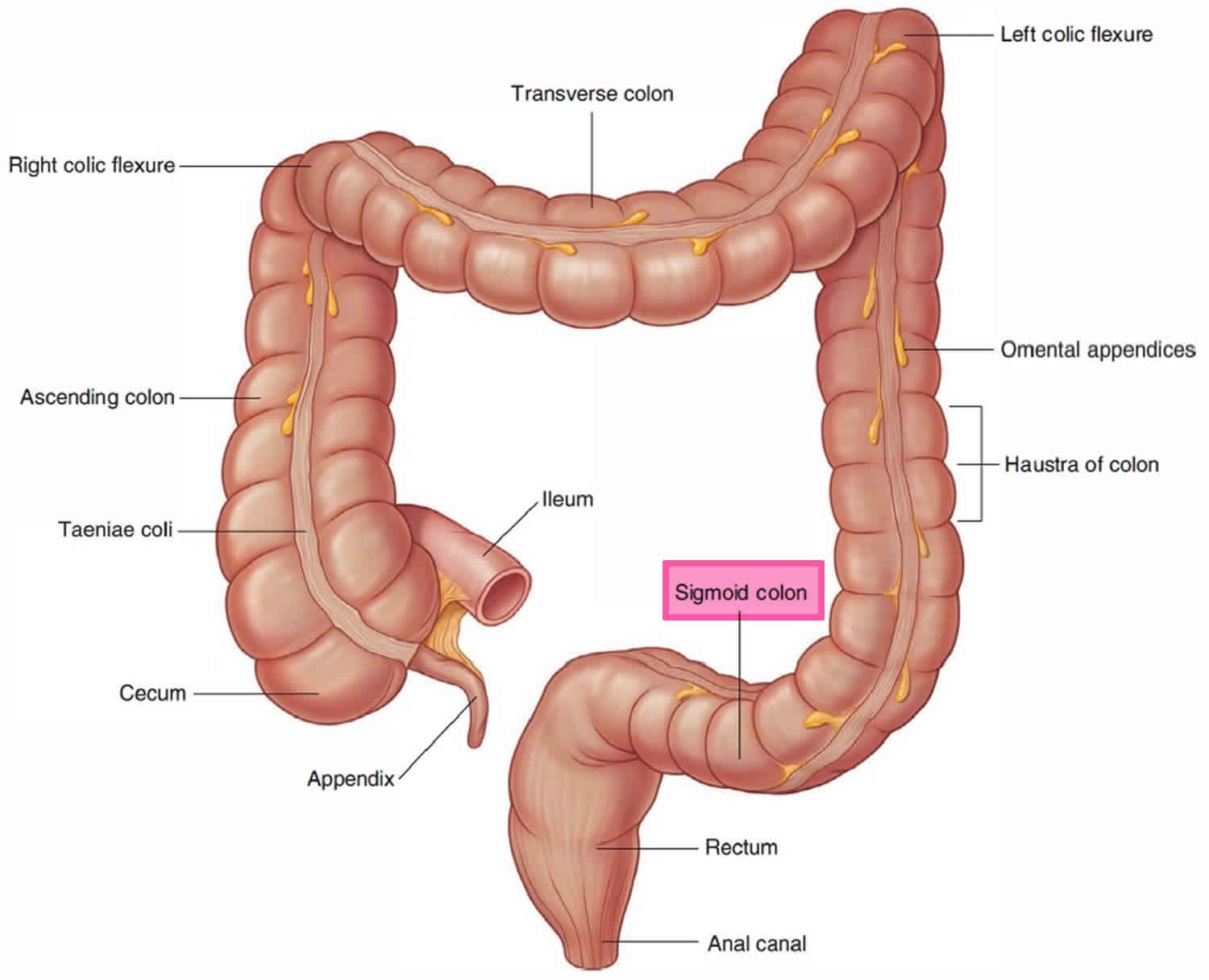
The sigmoid colon is an S-shaped loop of the final segment of the colon (the fifth part of the large intestine). The sigmoid colon is the continuation of the descending colon linking the descending colon to the rectum. The sigmoid colon begins above the pelvic inlet near the left iliac crest, projects medially to the midline, and terminates as the rectum at about the level of the third sacral vertebra (S3). The sigmoid colon is quite mobile except at its beginning, where it continues from the descending colon, and at its end, where it continues as the rectum. Between these points, it is suspended by the sigmoid mesocolon.
Sigmoid colon anatomy
Relations
- Anteriorly
- male: bladder
- female: bladder and uterus
- Superiorly: loops of small intestine
- Posteriorly: left internal iliac artery and vein, left ureter, piriformis muscle, sacrum, sacral plexus
- Laterally
- male: pelvic side wall, ductus deferens
- female: pelvic side wall, ovary
Blood supply
- Arterial: two-to-four sigmoid arteries (branch of inferior mesenteric artery)
- Venous: similarly named veins drain into the inferior mesenteric vein
Nerve supply
- Sympathetic: inferior mesenteric plexus
- Parasympathetic: via pelvic splanchnic nerves (from S2-S4)
Lymphatic drainage
- Lymphatics travel with vessels to the inferior mesenteric group.
Figure 1. Sigmoid colon anatomy
How long is the sigmoid colon?
Sigmoid colon averages about 35–40 cm (13.78-15.75 in) in length.
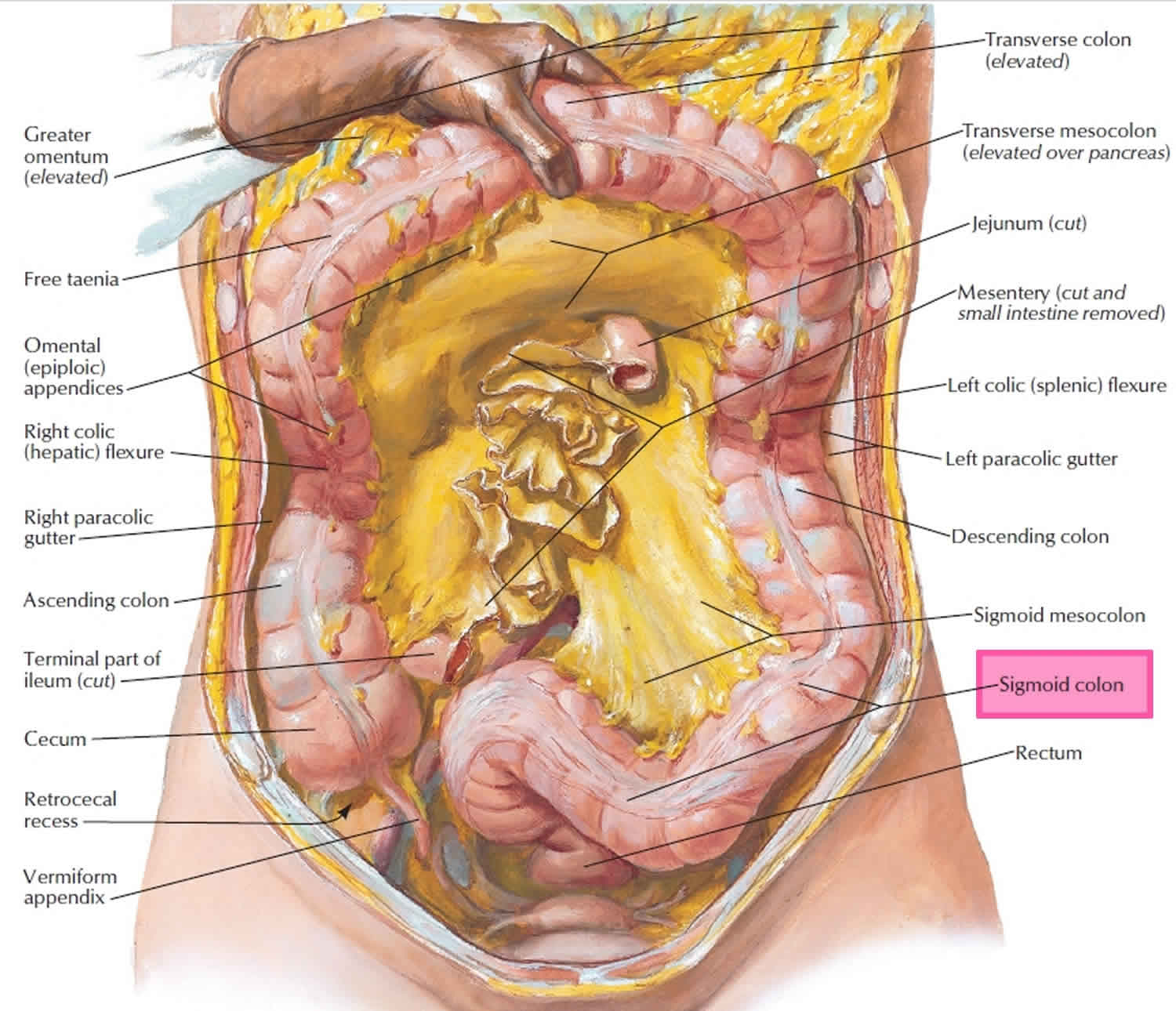
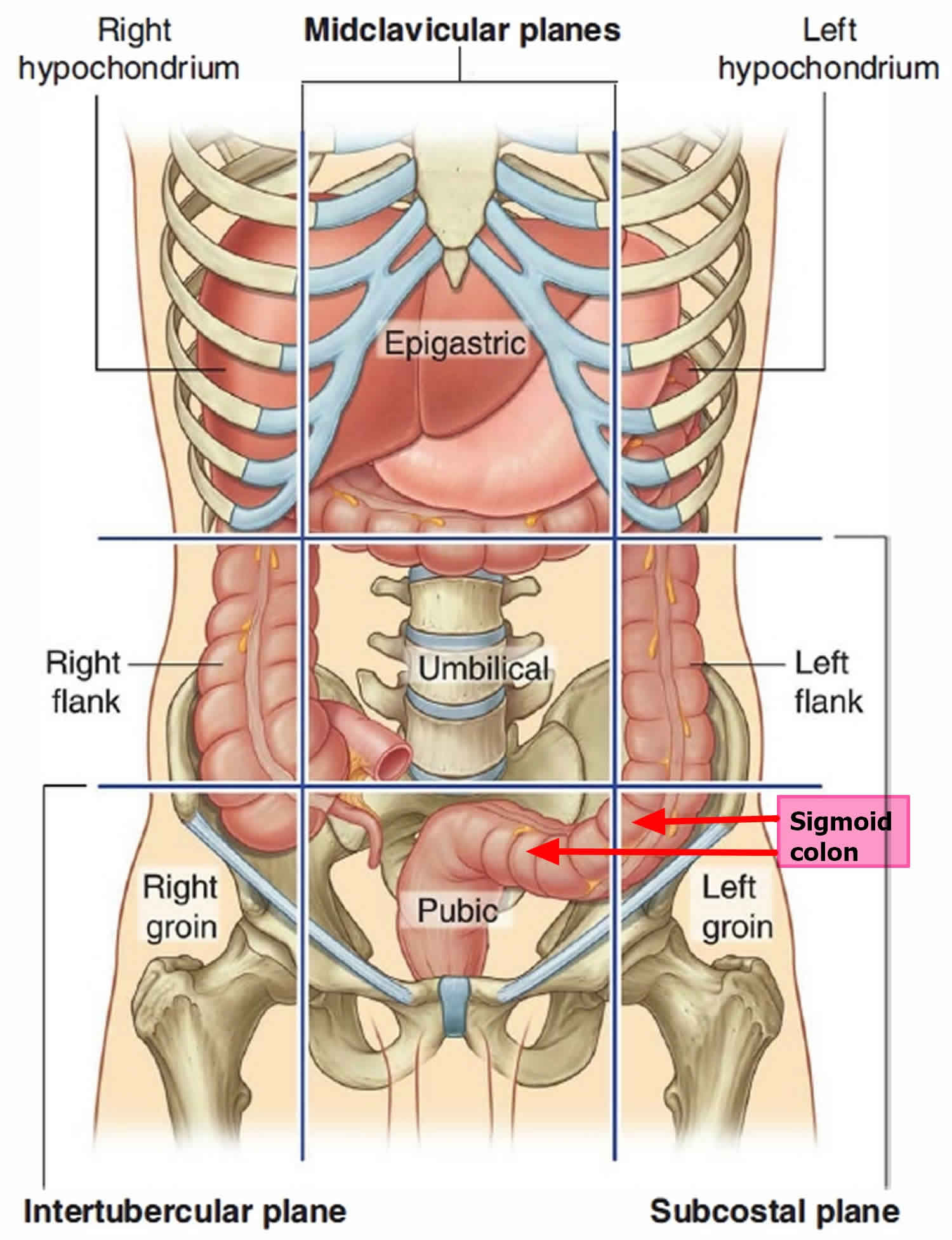
Where is the sigmoid colon located?
Figure 2. Sigmoid colon location
Sigmoid colon function
The key functions of the colon include the following 1:
- Water and nutrient absorption
- Vitamin absorption
- Feces compaction
- Potassium and chloride secretion
- Moving waste material toward the rectum
Sigmoid volvulus
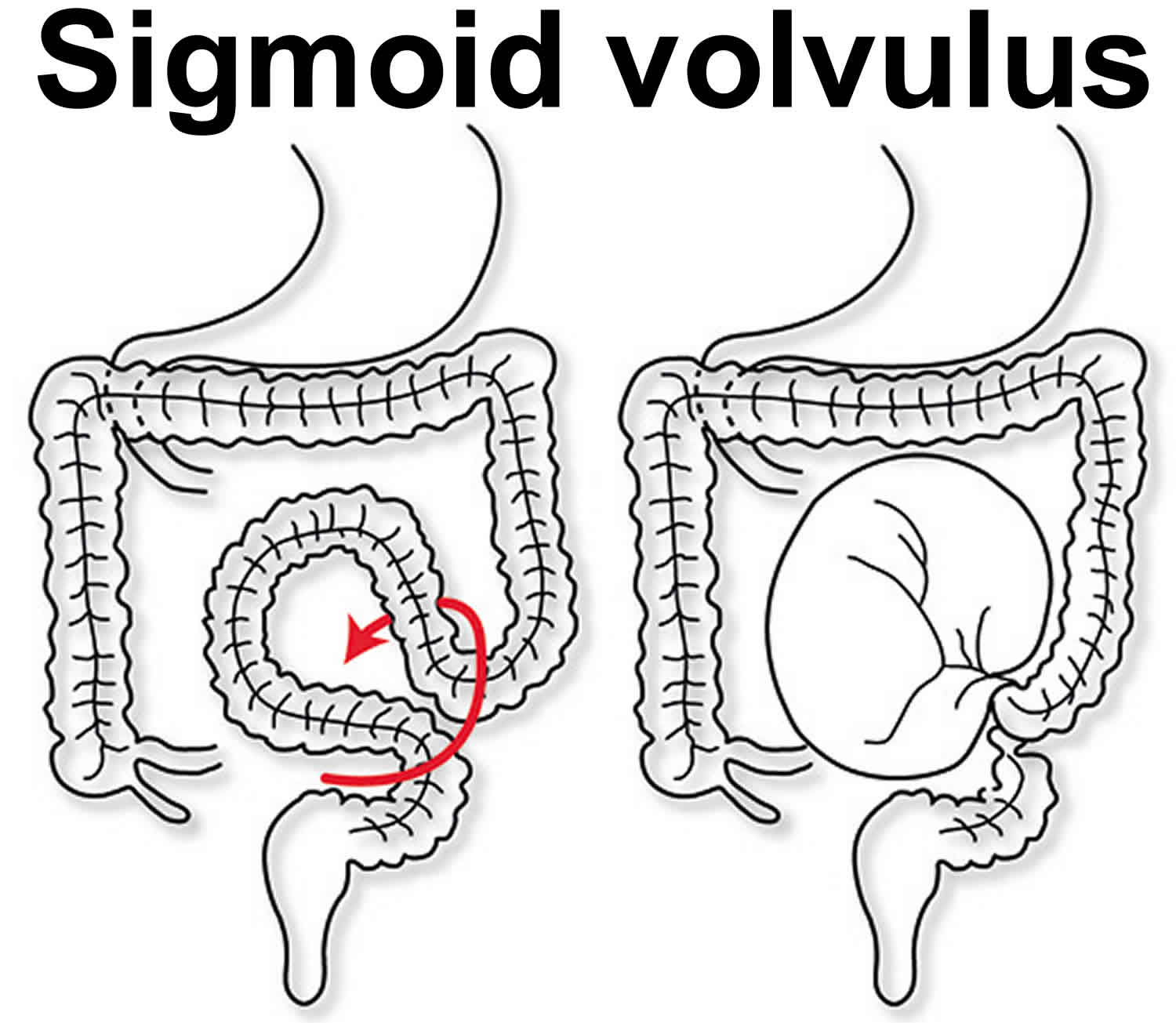
A volvulus is a twist of the intestine around the axis of its blood supply. In the case of a sigmoid volvulus, the twist occurs in the sigmoid mesentery at its base. Sigmoid volvulus is the most common type of volvulus of the colon 2. Less common are caecal volvulus and volvulus of the transverse colon. Large bowel volvulus accounts for ~5% of all large bowel obstructions, with ~60% of intestinal volvulus involving the sigmoid colon 3. Sigmoid volvulus is a cause of large bowel obstruction and occurs when the sigmoid colon twists on its mesentery, the sigmoid mesocolon. Sigmoid volvulus presents most commonly in patients who are less mobile, bed bound and institutionalized, usually with a background of chronic constipation. Sigmoid volvulus is more common in the elderly 4.
In order for a volvulus to occur, the bowel needs to be able to twist around a narrow-based mesentery. This occurs mostly in less mobile patients with a history of chronic constipation, where the sigmoid colon becomes chronically distended and redundant.
Sigmoid volvulus is more common in Africa, as the food intake is of high fiber and the base of the sigmoid mesentery in the African population is narrow compared with other ethnic groups, leading to an anatomical situation that makes the population more susceptible to developing a sigmoid volvulus 2.
Figure 3. Sigmoid volvulus
Sigmoid volvulus causes
There is a wide range of sigmoid volvulus causes; some are geographically-specific 5:
- Chronic constipation and/or laxative abuse
- Fiber-rich diet (especially in Africa)
- Chagas disease (especially in South America)
Sigmoid volvulus associations:
- Chronic neurological conditions (e.g. Parkinson disease, multiple sclerosis, pseudobulbar palsy)
- Medications from chronic psychiatric conditions (e.g. chronic schizophrenia)
Volvulus is a classical example of a large bowel closed loop obstruction. If inflow and outflow of the colon are both obstructed, the obstructed bowel will continue to distend, due to a large amount of gas forming bacteria trapped inside. This will eventually lead to a perforation of the obstructed segment.
While the colon is obstructed and distending, there is impaired blood supply, leading to ischemia, as well as bacterial translocation of the gut flora. Usually, the venous outflow is compromised first, increasing congestion even further, until arterial supply stops. The colonic mucosa is most susceptible to ischaemic insult, leading to an impaired barrier and translocation of bacteria, until the ischemia affects muscular and serosa, leading to necrosis and perforation.
Sigmoid volvulus can become a recurrent situation, and in those patients treated conservatively, the base of mesentery will eventually become fibrotic and the bowel chronically distended.
Sigmoid volvulus diagnosis
Patients presenting with volvulus are usually of an older age group with potential other comorbidities, often have reduced mobility or are bed bound and commonly get referred from residential and nursing homes. A history of chronic constipation is common. The symptoms usually leading to acute hospital admission are a loss of appetite and reduced oral intake, increasing abdominal distension, and cessation of bowel output. Patients complain of discomfort due to the significant distension, but are rarely in pain, unless ischemia and/or a perforation have occurred. They can, however, have respiratory compromise due to the splinting of the diaphragm that is a result of the colonic distension.
Patients may present with sigmoid volvulus as a recurrent problem if they have been treated with conservative measures in the past. A recurrent episode of volvulus needs to be taken a seriously as a first presentation and requires the same attention to history and physical examination as a patient presenting with volvulus for the first time.
Examination of the abdomen reveals significant distension, a generalized tympanitic percussion note and potentially guarding and rebound over areas of ischemia or impending perforation. If a perforation has already occurred, the patient will be grossly peritonitic. Digital rectal examination reveals an empty and often capacious rectum.
Sigmoid volvulus tests
The patient should have the standard blood work (full blood count and renal function tests), to aid in resuscitation and assess the kidney function for a potential CT scan with contrast. Plain abdominal radiographs will show the classical coffee bean or kidney bean sign, and often dilatation of the proximal colon. Depending on the duration of symptoms, the proximal colon can decompress into the distal small bowel, as long as the ileocaecal valve is incompetent. CT scan shows the characteristic “whirl” appearance of the twisted mesentery, as well as the distended loop of sigmoid colon with an air-fluid level. Free air on either the abdominal radiograph or the CT scan indicates a more serious bowel perforation and requires immediate action.
A CT scan is recommended to establish the diagnosis and distinguish the etiology from other causes of large bowel obstruction, such as a malignant tumor. This is especially the case if the patients present with symptoms for the first time and have not had any previous colonic investigations such as a colonoscopy.
Sigmoid volvulus treatment
Before any surgical intervention, the patient needs to be adequately resuscitated with intravenous fluids, and electrolyte imbalances should be corrected. A nasogastric tube can aid proximal decompression. Decompression of the sigmoid volvulus should be attempted with a soft rectal flatus tube by the bedside, ideally feeding the tube under direct vision through a rigid sigmoidoscope. Flexible Sigmoidoscopy with gentle insufflation is indicated if the bedside decompression fails or if there are concerns about the viability of the bowel wall, as the mucosa can be inspected during the sigmoidoscopy and areas of mucosal ischemia will become obvious.
Rectal tube insertion is successful in treating 90% of cases 5. The mortality rate is 20-25% 4. The most serious complication is bowel ischemia.
Bedside decompression with a flatus tube should only be carried out by experienced physicians, and under no circumstance against resistance, as there is a risk of inadvertent iatrogenic perforation. The safest method to decompress the sigmoid colon is under direct vision with rigid or flexible sigmoidoscopy.
A successful decompression will immediately result in the evacuation of liquid and gas per rectum with subsequent resolution of the abdominal distension, resulting in a soft abdomen. This resolution can be documented on a repeat abdominal radiograph.
It is important to assess the patient for sustained resolution once the flatus tube has been removed and the patient is started on oral intake, to avoid the volvulus recur before the patient is even discharged.
Those patients who cannot be decompressed or who have progressed to compromised viability of the colon will need surgical intervention. The surgery of choice is a sigmoid colectomy with either a primary anastomosis or an end colostomy, depending on findings during the surgery and the individual patients’ physiological reserves.
A patient presenting with bowel perforation will require aggressive resuscitation and an immediate laparotomy to control the fecal contamination and remove the perforated segment of bowel.
Patients presenting with recurrent episodes of sigmoid volvulus that can be decompressed should have an informed discussion about the benefits and risks of an elective resection of the sigmoid to prevent further episodes of volvulus leading to emergency admission to hospital. In the elective situation, a sigmoid colectomy can usually be performed with a primary anastomosis instead of an end colostomy, unless the patient has significant comorbidities.
Diverticulosis in the sigmoid colon
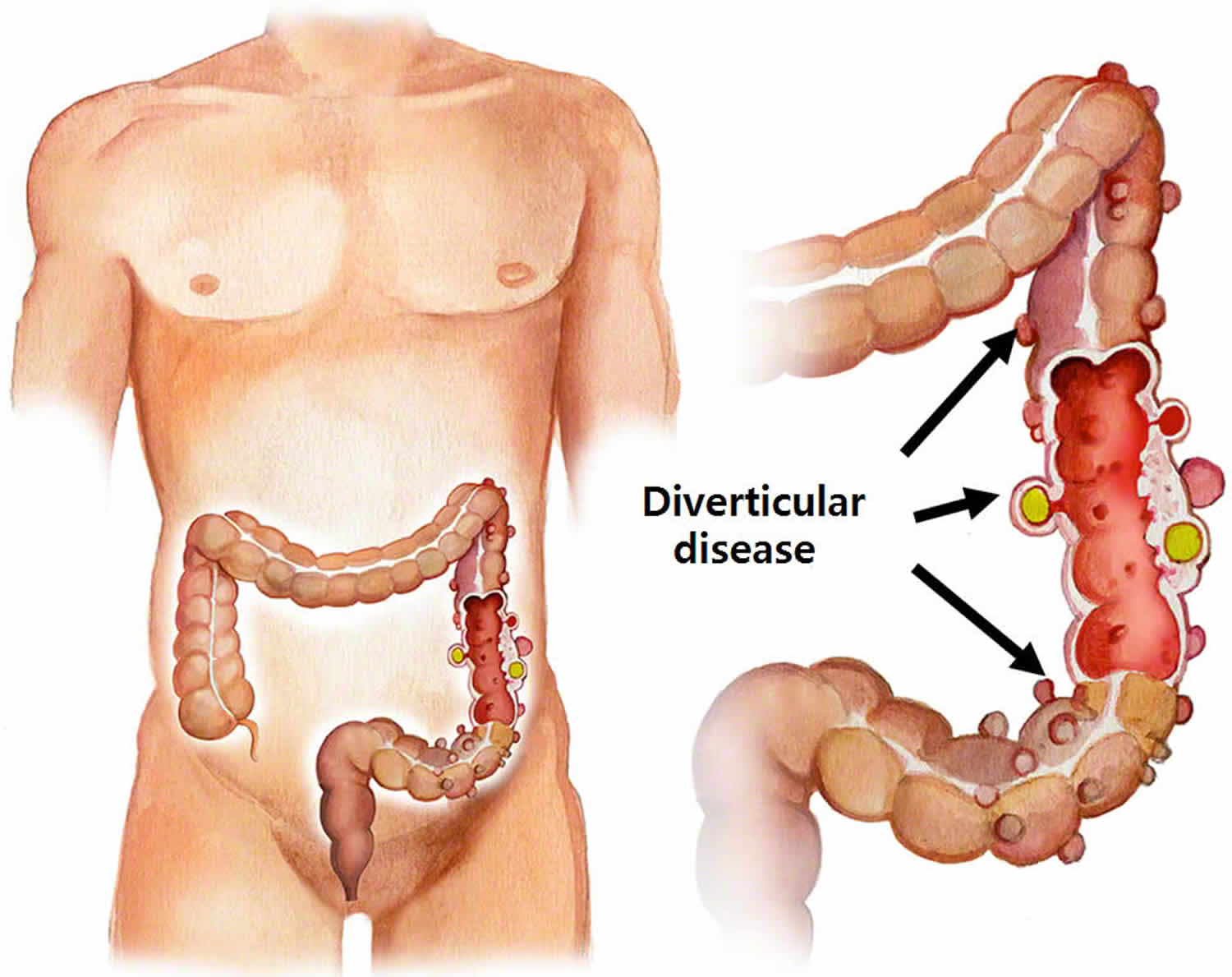
Diverticulosis is a clinical condition in which multiple sac-like protrusions (diverticula) develop along the gastrointestinal tract 6. Though diverticula may form at weak points in the walls of either the small or large intestines, in 95% of affected individuals the sigmoid colon is involved, usually exclusively 7. Colonic diverticulosis is quite distinct from diverticulitis which describes inflammation and infection of one or multiple diverticula 7.
The majority of individuals with diverticulosis are asymptomatic. Diverticular disease occurs when there is symptomatic diverticulosis (e.g., diverticular bleeding); diverticulitis (e.g., acute or chronic inflammation that may or may not is complicated by abscess formation, fistula formation, bowel obstruction or perforation); or associated segmental colitis (e.g., inflammation in segments of the mucosal segments of colon in between diverticula) 8.
The prevalence of diverticulosis is highest in the Western world and in countries that follow a more Western lifestyle 6. Diverticulosis affects 5% to 45% of individuals in the Western world, depending on both the method of diagnosis and age of the individual. In general, the prevalence of diverticulosis increases with age from under 20% of individuals affected at the age of 40, to 60% of individuals affected by the age of 60 6. Approximately 95% of patients in the Western world with diverticulosis have diverticula in the sigmoid colon 6. Of all of the patients with diverticulosis, 24% have diverticula involving mainly the sigmoid colon, 7% have diverticula spread evenly throughout the colon, and 4% have diverticula located only proximally to the sigmoid colon 9.
In Asia, diverticulosis has a prevalence of approximately 13% to 25% 6. Individuals with diverticulosis in this region also tend to have predominantly right-sided colonic diverticula (unlike the Western world where left-sided diverticula are much more common).
Approximately 5% to 15% of patients with diverticulosis experience bleeding. A third of which experience massive bleeding. In 50% to 60% of patients experiencing diverticular bleeding, the source is right-sided diverticula, possibly due to the thinner wall of the right-sided colon or the wider neck and domes of right-sided diverticula (e.g., an increased surface area of exposure of the vasa recta to potential injury).
Diverticulitis occurs in approximately 4% to 15% of patients with diverticula, and the incidence increases with age. On average, patients admitted for diverticulitis are about 63 years old. The overall incidence of diverticulitis continues to rise, with a 26% jump from 1998 to 2005, and the largest increases were seen in patients between the ages of 18 to 44 years.
Under the age of 50, diverticulosis is more common in males, whereas between the ages of 50 to 70, the disease is seen slightly more often in females. Over the age of 70, there is a significantly greater incidence of diverticulosis in females.
The prevalence of diverticulosis is very high and while the disorder is asymptomatic, it can present with painless bleeding or progress into an inflammatory state. The key to managing diverticulosis is to prevent it in the first place. Patients need to be educated about their dietary habits and start to include more fiber. In addition, the patient must be told to exercise, lose weight and drink ample fluids. These simple recommendations can help avoid complications like bleeding and diverticulitis. Finally, it is important to inform the patient that when surgery is undertaken for a complication of diverticulosis, there is always a risk of a stoma which can seriously impair the quality of life 10.
Figure 4. Sigmoid colon diverticulosis
Sigmoid colon diverticulosis causes
Age and constipation are the leading causes of diverticular disease. Diverticulosis is thought to occur as a result of peristalsis abnormalities (e.g., intestinal spasms), intestinal dyskinesia, or high segmental intraluminal pressures. Although the exact cause of these abnormalities is unknown, some environmental and lifestyle risk factors have been linked to this condition 11.
Several studies have suggested that a diet low in fiber and high in red meat may be associated with an increased risk of diverticulosis, although a diet high in fiber will not reduce the symptoms of an uncomplicated diverticular disease. In patients with symptomatic complicated diverticular disease (e.g., inflammation or bleeding) there may be a benefit from a diet high in fiber by decreasing overall inflammation and favorably changing the intestinal microbiota.
The risk of diverticulitis and bleeding is significantly higher in patients with obesity or a larger waist circumference.
Smokers have been noted to have an increased incidence of diverticular abscess formation or perforation.
Medications associated with an increased risk of diverticular bleeding or diverticulitis include nonsteroidal anti-inflammatory drugs, opiates, and steroids.
Sigmoid colon diverticulosis pathophysiology
Diverticula occur in weaker portions of the colonic wall where the vasa recta infiltrate the circular muscular layer. The vast majority of colonic diverticula are typically “false” diverticula which are mucosa and submucosa herniating through a defect or weakness in the muscularis layer, covered externally only by serosa. True diverticula are much more uncommon (e.g., Meckel’s diverticulum) and involve outpouching of all layers of the intestinal wall (e.g., mucosa, muscularis, and serosa) 12.
A major predisposing factor for the formation of colonic diverticula is abnormal colonic motility (e.g., intestinal spasms or dyskinesis) resulting in exaggerated segmental muscle contractions, elevated intraluminal pressures, and separation of the colonic lumen into chambers. The increased incidence of diverticula in the sigmoid colon is explained by Laplace’s law, such that pressure is proportional to wall tension and inversely proportional to bowel radius. As the sigmoid colon is the segment of colon with the smallest diameter, it is also the segment with highest intraluminal pressures.
Connective tissue disorders such as Marfan syndrome, Ehlers-Danlos syndrome, or autosomal dominant polycystic kidney disease may additionally predispose an individual to the formation of colonic diverticula as these diseases often involve structural changes (e.g., weakness) in the intestinal wall.
Diverticula are prone to bleeding due to the proximity of the vasa recta to the intestinal lumen as a result of herniation of the mucosa and submucosa through the muscularis layer. With diverticula formation, the vasa recta become separated from the intestinal lumen by a layer of mucosa alone and are therefore exposed to a greater amount of injury. This results in eccentric intimal thickening, thinning of the media, and ultimately segmental weaknesses along these arteries which predispose the vasa recta to rupture and bleeding into the intestinal lumen. Diverticular bleeding typically occurs in the absence of diverticular inflammation or infection (i.e., diverticulitis).
Diverticulitis typically results from micro- or macroscopic perforation of a diverticulum, and this may or may not result from obstruction (e.g., by a fecalith). Increased intraluminal pressures or inspissated (thickened and condensed) food matter, with resultant inflammation and focal necrosis, are what ultimately result in diverticular perforation. Associated inflammation is usually mild, and pericolic fat and mesentery tend to wall off the perforations of diverticula. This may or may not result in abscess or fistula formation, or intestinal obstruction. In rare cases, perforations may be large and uncontained and lead to peritonitis.
Sigmoid colon diverticulosis symptoms
Most individuals with diverticulosis do not have any symptoms, and the condition itself is not dangerous. Some patients, however, may experience unexplained abdominal pain or cramping, alterations in bowel habits, or notice blood in the stool. Any bleeding associated with diverticulosis is painless.
A diagnosis of diverticulosis is suspected when a patient presents with a history of painless rectal bleeding or unexplained abdominal pain or cramping, or alterations in bowel function.
Acute diverticulitis (e.g., inflammation, infection, or perforation) is typically suspected when a patient presents with lower abdominal pain (particularly on the left side). Patients may additionally present with abdominal tenderness to palpation and an elevated white blood cell count (leukocytosis). An abdominal CT will help differentiate between complicated versus uncomplicated disease in this case.
Sigmoid colon diverticulosis diagnosis
A diagnosis of diverticulosis is suspected based on clinical presentation (e.g., a history of painless rectal bleeding or unexplained abdominal pain and cramping, or altered bowel movements) and may be confirmed by colonoscopy or an x-ray following a barium enema. If the patient presents with extreme abdominal pain, however, the test of choice is typically a CT of the abdomen to avoid the risk of intestinal rupture in the setting of intestinal infection or inflammation 13.
A colonoscopy remains the best test to identify the source of bleeding if blood is present in the stool. If a colonoscopy is inconclusive, however, angiography or radionuclide scanning may be considered to locate the source.
Patients presenting with acute diverticulitis may require additional treatment. Uncomplicated diverticulitis is treated non-operatively, with either intravenous (IV) or oral (PO) antibiotics. Complicated diverticulitis (e.g., with an associated fistula, abscess, obstruction, or perforation) may, in addition to antibiotic therapy, require hospitalization and/or surgery, to treat the associated complication. Similarly, patients presenting with sepsis, immunosuppression, advanced age, significant comorbidities, high fever (greater than 102.5 °F [39.2°C]), significant leukocytosis, inability to tolerate oral intake, non-compliance, or failed outpatient treatment, may require hospitalization for proper treatment.
Sigmoid colon diverticulosis treatment
Treatment is typically aimed at reducing intestinal spasms which may be achieved by increasing fiber and fluids in the diet. Greater intestinal bulk reduces the number of spasms, and as a result decreases intestinal pressures. Most bleeding associated with diverticulosis is self-limiting and does not require intervention. In some cases, however, endoscopic, radiologic, or surgical intervention may be required to stop persistent bleeding 14. In the case of recurrent bleeding, or if a source cannot be determined, surgery may be considered to remove portions of affected intestine (e.g., colectomy). Similarly, in the case of a giant diverticulum, with an increased risk of infection and rupture, surgery is more likely to be considered 15.
Sigmoid colon cancer
Colorectal cancer is a cancer that starts in the colon or the rectum. These cancers can also be named colon cancer or rectal cancer, depending on where they start. Colon cancer and rectal cancer are often grouped together because they have many features in common.
Colorectal carcinoma is the most common cancer of the gastrointestinal tract and the third most frequently diagnosed malignancy in adults and second deadliest malignancy for both sexes combined 16. CT and MRI are the modalities most frequently used for staging. Surgical resection may be curative although five-year survival rate is 40-50%.
The American Cancer Society’s estimates for the number of colorectal cancer cases in the United States for 2018 are 17:
- 97,220 new cases of colon cancer
- 43,030 new cases of rectal cancer
Lifetime risk of colorectal cancer
Overall, the lifetime risk of developing colorectal cancer is: about 1 in 22 (4.49%) for men and 1 in 24 (4.15%) for women. This risk is slightly lower in women than in men. A number of other factors (described in Colorectal cancer risk factors) can also affect your risk for developing colorectal cancer.
Deaths from colorectal cancer
Colorectal cancer is the third leading cause of cancer-related deaths in men and women in the United States. It’s expected to cause about 50,630 deaths during 2018.
The death rate (the number of deaths per 100,000 people per year) from colorectal cancer has been dropping in both men and women for several decades. There are a number of likely reasons for this. One is that colorectal polyps are now being found more often by screening and removed before they can develop into cancers or are being found earlier when the disease is easier to treat. In addition, treatment for colorectal cancer has improved over the last few decades. As a result, there are now more than 1 million survivors of colorectal cancer in the United States.
Types of colorectal cancer
Adenocarcinomas make up about 96% of colorectal cancers. These cancers start in cells that make mucus to lubricate the inside of the colon and rectum. When doctors talk about colorectal cancer, they’re almost always talking about this type. Some sub-types of adenocarcinoma, such as signet ring and mucinous, may have a worse prognosis (outlook).
Other, much less common types of tumors can start in the colon and rectum, too. These include:
- Carcinoid tumors. These start from special hormone-making cells in the intestine.
- Gastrointestinal stromal tumors (GISTs) start from special cells in the wall of the colon called the interstitial cells of Cajal. Some are not cancer (benign). These tumors can be found anywhere in the digestive tract, but are not common in the colon.
- Lymphomas are cancers of immune system cells. They mostly start in lymph nodes, but they can also start in the colon, rectum, or other organs.
- Sarcomas can start in blood vessels, muscle layers, or other connective tissues in the wall of the colon and rectum. Sarcomas of the colon or rectum are rare.
Sigmoid colon cancer causes
Researchers have found several factors that can increase a person’s risk of colorectal cancer, but it’s not yet clear exactly how all of these factors might cause this cancer.
Cancer is caused by changes in the DNA inside our cells. DNA is the chemical in our cells that makes up our genes, which control how our cells function. We usually look like our parents because they are the source of our DNA. But DNA affects more than just how we look.
Some genes help control when our cells grow, divide into new cells, and die:
- Certain genes that help cells grow, divide, and stay alive are called oncogenes.
- Genes that help keep cell division under control or cause cells to die at the right time are called tumor suppressor genes.
Cancers can be caused by DNA mutations (changes) that turn on oncogenes or turn off tumor suppressor genes. This leads to cells growing out of control. Changes in many different genes are usually needed to cause colorectal cancer.
Inherited gene mutations
Some DNA mutations can be passed on in families and are found in all of a person’s cells. These are called inherited muations. . A very small portion of colorectal cancers are caused by inherited gene mutations. Many of these DNA changes and their effects on the growth of cells are now known. For example:
- Familial adenomatous polyposis (FAP), attenuated FAP (AFAP), and Gardner syndrome are caused by inherited changes in the APC gene. The APC gene is a tumor suppressor gene; it normally helps keep cell growth in check. In people with inherited changes in the APC gene, this “brake” on cell growth is turned off, causing hundreds of polyps to form in the colon. Over time, cancer will nearly always develop in one or more of these polyps.
- Lynch syndrome (hereditary non-polyposis colon cancer, or HNPCC) is caused by changes in genes that normally help a cell repair damaged DNA. A mutation in one of the DNA repair enzyme genes like MLH1, MSH2, MLH3, MSH6, PMS1, and PMS2, can allow DNA errors to go unfixed. These errors will sometimes affect growth-regulating genes, which may lead to the development of cancer.
- Peutz-Jeghers syndrome is caused by inherited changes in the STK11 (LKB1) gene, a tumor suppressor gene.
- MYH-associated polyposis (MAP) is caused by mutations in the MYH gene, which is involved in how the cell “proofreads” or checks the DNA and fixes errors when cells divide.
Special genetic tests can find gene mutations linked to these inherited syndromes. If you have a family history of colorectal polyps or cancer or other symptoms linked to these syndromes, you may want to ask your doctor about genetic counseling and genetic testing. The American Cancer Society recommends discussing genetic testing with a qualified cancer genetics professional before any genetic testing is done.
Acquired gene mutations
Most gene mutations that lead to cancer are acquired mutations. They happen during a person’s lifetime and are not passed on to their children. these DNA changes affect only cells that come from the original mutated cell.
In most cases of colorectal cancer, the DNA mutations that lead to cancer are acquired during a person’s life rather than having been inherited. Certain risk factors probably play a role in causing these acquired mutations, but so far it’s not known what causes most of them.
There doesn’t seem to be a single genetic pathway to colorectal cancer that’s the same in all cases. In many cases, the first mutation occurs in the APC gene. This leads to an increased growth of colorectal cells because of the loss of this “brake” on cell growth. Further mutations may then occur in other genes, which can lead the cells to grow and spread uncontrollably. Other genes that aren’t known yet are probably involved as well.
Colorectal cancer risk factors
A risk factor is anything that affects your chance of getting a disease such as cancer. Different cancers have different risk factors. Some risk factors, like smoking, can be changed. Others, like a person’s age or family history, can’t be changed.
But having a risk factor, or even many, does not mean that you will get the disease. And some people who get the disease may not have any known risk factors.
Researchers have found several risk factors that might increase a person’s chance of developing colorectal polyps or colorectal cancer.
Colorectal cancer risk factors you can change
Many lifestyle-related factors have been linked to colorectal cancer. In fact, the links between diet, weight, and exercise and colorectal cancer risk are some of the strongest for any type of cancer.
Being overweight or obese
If you are overweight or obese (very overweight), your risk of developing and dying from colorectal cancer is higher. Being overweight (especially having a larger waistline) raises the risk of colon and rectal cancer in both men and women, but the link seems to be stronger in men.
Physical inactivity
If you’re not physically active, you have a greater chance of developing colon cancer. Being more active can help lower your risk.
Certain types of diets
A diet that’s high in red meats (such as beef, pork, lamb, or liver) and processed meats (like hot dogs and some luncheon meats) raises your colorectal cancer risk.
Cooking meats at very high temperatures (frying, broiling, or grilling) creates chemicals that might raise your cancer risk. It’s not clear how much this might increase your colorectal cancer risk.
It’s not clear if other dietary components (for example, certain types of fats) affect colorectal cancer risk.
Smoking
People who have smoked tobacco for a long time are more likely than non-smokers to develop and die from colorectal cancer. Smoking is a well-known cause of lung cancer, but it’s linked to a lot of other cancers, too.
Heavy alcohol use
Colorectal cancer has been linked to moderate to heavy alcohol use. Limiting alcohol use to no more than 2 drinks a day for men and 1 drink a day for women could have many health benefits, including a lower risk of many kinds of cancer.
Colorectal cancer risk factors you cannot change
Being older
Your risk of colorectal cancer goes up as you age. Younger adults can get it, but it’s much more common after age 50.
A personal history of colorectal polyps or colorectal cancer
If you have a history of adenomatous polyps (adenomas), you are at increased risk of developing colorectal cancer. This is especially true if the polyps are large, if there are many of them, or if any of them show dysplasia.
If you’ve had colorectal cancer, even though it was completely removed, you are more likely to develop new cancers in other parts of the colon and rectum. The chances of this happening are greater if you had your first colorectal cancer when you were younger.
A personal history of inflammatory bowel disease
If you have inflammatory bowel disease (IBD), including either ulcerative colitis or Crohn’s disease, your risk of colorectal cancer is increased.
Inflammatory bowel disease is a condition in which the colon is inflamed over a long period of time. People who have had inflammatory bowel disease for many years, especially if untreated, often develop dysplasia. Dysplasia is a term used to describe cells in the lining of the colon or rectum that look abnormal, but are not true cancer cells. They can change into cancer over time.
If you have inflammatory bowel disease, you may need to start getting screened for colorectal cancer when you are younger and be screened more often.
Inflammatory bowel disease is different from irritable bowel syndrome (IBS), which does not increase your risk for colorectal cancer.
A family history of colorectal cancer or adenomatous polyps
Most colorectal cancers are found in people without a family history of colorectal cancer. Still, nearly 1 in 3 people who develop colorectal cancer have other family members who have had it.
People with a history of colorectal cancer in a first-degree relative (parent, sibling, or child) are at increased risk. The risk is even higher if that relative was diagnosed with cancer when they were younger than 45, or if more than one first-degree relative is affected.
The reasons for the increased risk are not clear in all cases. Cancers can “run in the family” because of inherited genes, shared environmental factors, or some combination of these.
Having family members who have had adenomatous polyps is also linked to a higher risk of colon cancer. Adenomatous polyps are the kind of polyps that can become cancer.
If you have a family history of adenomatous polyps or colorectal cancer, talk with your doctor about the possible need to start screening before age 45. If you’ve had adenomatous polyps or colorectal cancer, it’s important to tell your close relatives so that they can pass along that information to their doctors and start screening at the right age.
Having an inherited syndrome
About 5% of people who develop colorectal cancer have inherited gene changes (mutations) that cause family cancer syndromes and can lead to them getting the disease.
The most common inherited syndromes linked with colorectal cancers are Lynch syndrome (hereditary non-polyposis colorectal cancer, or HNPCC) and familial adenomatous polyposis (FAP), but other rarer syndromes can increase colorectal cancer risk, too.
Lynch syndrome (hereditary non-polyposis colon cancer or HNPCC)
Lynch syndrome is the most common hereditary colorectal cancer syndrome. It accounts for about 2% to 4% of all colorectal cancers. In most cases, this disorder is caused by an inherited defect in either the MLH1 or MSH2 gene, but changes in other genes can also cause Lynch syndrome. These genes normally help repair DNA that has been damaged.
The cancers linked to this syndrome tend to develop when people are relatively young. People with Lynch syndrome can have polyps, but they tend to only have a few. The lifetime risk of colorectal cancer in people with this condition may be as high as 80%, but this depends on which gene is affected.
Women with this condition also have a very high risk of developing cancer of the endometrium (lining of the uterus). Other cancers linked with Lynch syndrome include cancer of the ovary, stomach, small intestine, pancreas, kidney, prostate, breast, brain, ureters (tubes that carry urine from the kidneys to the bladder), and bile duct.
Familial adenomatous polyposis (FAP)
FAP is caused by changes (mutations) in the APC gene that a person inherits from his or her parents. About 1% of all colorectal cancers are caused by FAP.
In the most common type of FAP, hundreds or thousands of polyps develop in a person’s colon and rectum, often starting at ages 10 to 12 years. Cancer usually develops in 1 or more of these polyps as early as age 20. By age 40, almost all people with FAP will have colon cancer if their colon hasn’t been removed to prevent it. People with FAP also have an increased risk for cancers of the stomach, small intestines, pancreas, liver, and some other organs.
There are 3 sub-types of FAP:
- In attenuated FAP or AFAP, patients have fewer polyps (less than 100), and colorectal cancer tends to occur at a later age.
- Gardner syndrome is a type of FAP that also causes non-cancer tumors of the skin, soft tissue, and bones.
- Turcot syndrome is a very rare inherited condition in which people have a higher risk of many adenomatous polyps and colorectal cancer, as well as brain cancer. There are actually 2 types of Turcot syndrome:
Rare inherited syndromes linked to colorectal cancer
- Peutz-Jeghers syndrome (PJS): People with this inherited condition tend to have freckles around the mouth (and sometimes on their hands and feet) and a special type of polyp called hamartomas in their digestive tracts. These people are at a much higher risk for colorectal cancer, as well as other cancers, and they usually are diagnosed at a younger than usual age. This syndrome is caused by mutations in the STK11 (LKB1) gene.
- MYH-associated polyposis (MAP): People with this syndrome develop many colon polyps. These will almost always become cancer if not watched closely with regular colonoscopies. These people also have an increased risk of other cancers of the GI (gastrointestinal) tract and thyroid. This syndrome is caused by mutations in the MYH gene (which is involved in “proofreading” the DNA and fixing any mistakes) and often leads to cancer at a younger age.
Since many of these syndromes are linked to colorectal cancer at a young age and also linked to other types of cancer, identifying families with these inherited syndromes is important. It lets doctors recommend specific steps such as screening and other preventive measures when the person is younger.
Your racial and ethnic background
African Americans have the highest colorectal cancer incidence and mortality rates of all racial groups in the US. The reasons for this are not fully understood.
Jews of Eastern European descent (Ashkenazi Jews) have one of the highest colorectal cancer risks of any ethnic group in the world.
Having type 2 diabetes
People with type 2 (usually non-insulin dependent) diabetes have an increased risk of colorectal cancer. Both type 2 diabetes and colorectal cancer share some of the same risk factors (such as being overweight and physical inactivity). But even after taking these factors into account, people with type 2 diabetes still have an increased risk. They also tend to have a less favorable prognosis (outlook) after diagnosis.
Colorectal cancer prevention
There’s no sure way to prevent colorectal cancer. But there are things you can do that might help lower your risk, such as changing the risk factors that you can control.
Colorectal cancer screening
Screening is the process of looking for cancer or pre-cancer in people who have no symptoms of the disease. Regular colorectal cancer screening is one of the most powerful weapons for preventing colorectal cancer.
From the time the first abnormal cells start to grow into polyps, it usually takes about 10 to 15 years for them to develop into colorectal cancer. With regular screening, most polyps can be found and removed before they have the chance to turn into cancer. Screening can also find colorectal cancer early, when it’s small and easier to treat.
If you’re age 45 or older, you should start getting screened for colorectal cancer. Several types of tests can be used. Talk to your health care provider about which ones might be good options for you. No matter which test you choose, the most important thing is to get tested.
If you have a strong family history of colorectal polyps or cancer, talk with your doctor about your risk. You might benefit from genetic counseling to review your family medical tree to see how likely it is that you have a family cancer syndrome.
Body weight, physical activity, and diet
You might be able to lower your risk of colorectal cancer by managing some of the risk factors that you can control, like diet and physical activity.
Weight: Being overweight or obese increases the risk of colorectal cancer in both men and women, but the link seems to be stronger in men. Having more belly fat (that is, a larger waistline) has also been linked to colorectal cancer. Staying at a healthy weight and avoiding weight gain around the midsection may help lower your risk.
Physical activity: Increasing your level of activity lowers your risk of colorectal cancer and polyps. Regular moderate activity (doing things that make you breathe as hard as you would during a brisk walk) lowers the risk, but vigorous activity might have an even greater benefit. Increasing the intensity and amount of your physical activity may help reduce your risk.
Diet: Overall, diets that are high in vegetables, fruits, and whole grains (and low in red and processed meats) have been linked with lower colorectal cancer risk, although it’s not exactly clear which factors are important. Many studies have found a link between red meats (beef, pork, and lamb) or processed meats (such as hot dogs, sausage, and lunch meats) and increased colorectal cancer risk. Limiting red and processed meats and eating more vegetables and fruits may help lower your risk.
In recent years, some large studies have suggested that fiber in the diet, especially from whole grains, may lower colorectal cancer risk. Research in this area is still under way.
Alcohol: Several studies have found a higher risk of colorectal cancer with increased alcohol intake, especially among men. Avoiding excess alcohol may help reduce your risk.
Not smoking
Long-term smoking is linked to an increased risk of colorectal cancer, as well as many other cancers and health problems. Quitting smoking may help lower you risk of colorectal cancer and many other types of cancer, too.
Vitamins, calcium, and magnesium
Some studies suggest that taking a daily multi-vitamin containing folic acid, or folate, may lower colorectal cancer risk, but not all studies have found this. In fact, some studies have hinted that folic acid might help existing tumors grow. More research is needed in this area.
Some studies have suggested that vitamin D, which you can get from sun exposure, in certain foods, or in a vitamin pill, might lower colorectal cancer risk. Because of concerns that excess sun exposure can cause skin cancer, most experts do not recommend this as a way to lower colorectal cancer risk at this time. More studies are needed to determine if vitamin D can help prevent colorectal cancer.
Low levels of dietary calcium have been linked with an increased risk of colorectal cancer in some studies. Other studies suggest that increasing calcium intake may lower colorectal cancer risk. Calcium is important for a number of health reasons aside from possible effects on cancer risk. But because of the possible increased risk of prostate cancer in men with high calcium intake, the American Cancer Society does not recommend increasing calcium intake specifically to try to lower colorectal cancer risk.
Calcium and vitamin D might work together to reduce colorectal cancer risk, as vitamin D aids in the body’s absorption of calcium. Still, not all studies have found that supplements of these nutrients reduce risk.
A few studies have found a possible link between a diet that’s high in magnesium and reduced colorectal cancer risk, especially among women. More research is needed to determine if this link exists.
Non-steroidal anti-inflammatory drugs (NSAIDs)
Many studies have found that people who regularly take aspirin or other non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen (Motrin, Advil) and naproxen (Aleve), have a lower risk of colorectal cancer and polyps.
But aspirin and other NSAIDs can cause serious or even life-threatening side effects, such as bleeding from stomach irritation or stomach ulcers, which may outweigh the benefits of these medicines for the general public. For this reason, most experts don’t recommend taking NSAIDs just to lower colorectal cancer risk if you are someone at average risk.
Still, for some people in their 50s who have a high risk of heart disease, where low-dose aspirin is found to be beneficial, the aspirin may also have the added benefit of reducing the risk of colorectal cancer.
Because aspirin or other NSAIDs can have serious side effects, check with your doctor before starting any of them on a regular basis.
Hormone replacement therapy for women
Taking estrogen and progesterone after menopause (sometimes called menopausal hormone therapy or combined hormone replacement therapy) may reduce a woman’s risk of developing colorectal cancer, but cancers found in women taking these hormones after menopause may be at a more advanced stage.
Because taking estrogen and progesterone after menopause can also increase a woman’s risk of heart disease, blood clots, and cancers of the breast and lung, it’s not commonly recommended just to lower colorectal cancer risk.
If you’re considering using menopausal hormone therapy, be sure to discuss the pros and cons with your doctor.
Colorectal cancer symptoms
Colorectal cancer might not cause symptoms right away, but if it does, it may cause one or more of these symptoms:
- A change in bowel habits, such as diarrhea, constipation, or narrowing of the stool, that lasts for more than a few days
- A feeling that you need to have a bowel movement that’s not relieved by having one
- Rectal bleeding with bright red blood
- Blood in the stool, which may make the stool look dark
- Cramping or abdominal (belly) pain
- Weakness and fatigue
- Unintended weight loss
Colorectal cancers can often bleed into the digestive tract. Sometimes the blood can be seen in the stool or make it look darker, but often the stool looks normal. But over time, the blood loss can build up and can lead to low red blood cell counts (anemia). Sometimes the first sign of colorectal cancer is a blood test showing a low red blood cell count.
Many of these symptoms can be caused by conditions other than colorectal cancer, such as infection, hemorrhoids, or irritable bowel syndrome. Still, if you have any of these problems, it’s important to see your doctor right away so the cause can be found and treated, if needed.
Sigmoid colon cancer diagnosis
If you have symptoms that might be from colorectal cancer, or if a screening test shows something abnormal, your doctor will recommend one or more of the exams and tests below to find the cause.
Medical history and physical exam
Your doctor will ask about your medical history to learn about possible risk factors, including your family history. You will also be asked if you’re having any symptoms and, if so, when they started and how long you’ve had them.
As part of a physical exam, your doctor will feel your abdomen for masses or enlarged organs, and also examine the rest of your body. You may also have a digital rectal exam (DRE). During this test, the doctor inserts a lubricated, gloved finger into your rectum to feel for any abnormal areas.
Tests to look for blood in your stool
If you are seeing the doctor because of symptoms you are having (other than bleeding from your rectum or blood in your stools), he or she may recommend a test to check your stool for blood that isn’t visible to the naked eye (occult blood), which might be a sign of cancer. These types of tests – a fecal occult blood test (FOBT) or fecal immunochemical test (FIT) – are done at home, and require you to collect 1 to 3 samples of stool from a bowel movement.
A stool blood test should not be the next test done if you’ve already had an abnormal screening test, in which case you should have a diagnostic colonoscopy, which is described below.
Blood tests
Your doctor might also order certain blood tests to help determine if you have colorectal cancer. These tests also can be used to help monitor your disease if you’ve been diagnosed with cancer.
Complete blood count (CBC): This test measures the different types of cells in your blood. It can show if you have anemia (too few red blood cells). Some people with colorectal cancer become anemic because the tumor has been bleeding for a long time.
Liver enzymes: You may also have a blood test to check your liver function, because colorectal cancer can spread to the liver.
Tumor markers: Colorectal cancer cells sometimes make substances called tumor markers that can be found in the blood. The most common tumor markers for colorectal cancer are carcinoembryonic antigen (CEA) and CA 19-9.
Blood tests for these tumor markers can sometimes suggest someone might have colorectal cancer, but they can’t be used alone to screen for or diagnose cancer. This is because tumor marker levels can sometimes be normal in someone who has cancer and can be abnormal for reasons other than cancer.
Tumor markers are used most often along with other tests to monitor patients who already have been diagnosed with colorectal cancer. They may help show how well treatment is working or provide an early warning that a cancer has returned.
If symptoms or the results of the physical exam or blood tests suggest that you might have colorectal cancer, your doctor could recommend more tests. This most often is colonoscopy, but sometimes other tests may be done first.
Sigmoidoscopy
A procedure to look inside the rectum and sigmoid (lower) colon for polyps (small areas of bulging tissue), other abnormal areas, or cancer. A sigmoidoscope is inserted through the rectum into the sigmoid colon. A sigmoidoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove polyps or tissue samples, which are checked under a microscope for signs of cancer.
Diagnostic colonoscopy
A diagnostic colonoscopy is just like a screening colonoscopy, but it’s done because a person is having symptoms, or because something abnormal was found on another type of screening test.
For this test, the doctor looks at the entire length of the colon and rectum with a colonoscope, a thin, flexible, lighted tube with a small video camera on the end. It is inserted through the anus and into the rectum and the colon. Special instruments can be passed through the colonoscope to biopsy or remove any suspicious-looking areas such as polyps, if needed.
Colonoscopy may be done in a hospital outpatient department, in a clinic, or in a doctor’s office.
Proctoscopy
This test may be done if rectal cancer is suspected. For this test, the doctor looks inside the rectum with a proctoscope, a thin, rigid, lighted tube with a small video camera on the end. It’s put in through the anus. The doctor can look closely at the inside lining of the rectum through the scope. The tumor can be seen, measured, and its exact location can be determined. For instance, the doctor can see how close the tumor is to the sphincter muscles that control the passing of stool.
Biopsy
Usually if a suspected colorectal cancer is found by any screening or diagnostic test, it is biopsied during a colonoscopy. In a biopsy, the doctor removes a small piece of tissue with a special instrument passed through the scope. Less often, part of the colon may need to be surgically removed to make the diagnosis.
Lab tests of biopsy samples
Biopsy samples (from colonoscopy or surgery) are sent to the lab where they are looked at closely. Other tests may suggest that colorectal cancer is present, but the only way to be sure is to look at the biopsy samples under a microscope.
If cancer is found, other lab tests may also be done on the biopsy specimens to help better classify the cancer.
Gene tests: Doctors may look for specific gene changes in the cancer cells that might affect how the cancer is best treated especially if the cancer has spread (metastasized). For example, doctors now typically test the cells for changes in the KRAS and NRAS and BRAF genes. Some doctors may also test for changes in the BRAF gene. Patients whose cancers have mutations in these genes typically do not benefit from treatment with certain targeted anti-cancer drugs.
MSI and MMR testing: Colorectal cancer cells are typically tested to see if they show high levels of gene changes called microsatellite instability (MSI). Testing might also be done to see if the cancer cells have changes in any of the mismatch repair (MMR) genes (MLH1, MSH2, MSH6, and PMS2).
Changes in MSI or in MMR genes (or both) are often seen in people with Lynch syndrome (HNPCC). Most colorectal cancers do not have high levels of MSI or changes in MMR genes. But most colorectal cancers that are linked to Lynch syndrome do.
There are 2 possible reasons to test colorectal cancers for MSI or for MMR gene changes:
- To identify patients who should be tested for Lynch syndrome. A diagnosis of Lynch syndrome can help plan other cancer screenings for the patient (for example, women with Lynch syndrome may need to be screened for uterine cancer). Also, if a patient has Lynch syndrome, their relatives could also have it, and may want to be tested for it.
- To determine treatment options for colorectal cancer, where MSI or MMR results could change the way it is treated.
Imaging tests to look for colorectal cancer
Imaging tests use sound waves, x-rays, magnetic fields, or radioactive substances to create pictures of the inside of your body. Imaging tests may be done for a number of reasons, such as:
- To look at suspicious areas that might be cancer
- To learn how far cancer has spread
- To help determine if treatment is working
Computed tomography (CT or CAT) scan
A CT scan uses x-rays to make detailed cross-sectional images of your body. This test can help tell if colon cancer has spread into your liver or other organs.
Ultrasound
Ultrasound uses sound waves and their echoes to create images of the inside of the body. A small microphone-like instrument called a transducer gives off sound waves and picks up the echoes as they bounce off organs. The echoes are converted by a computer into an image on a screen.
Abdominal ultrasound: For this exam, a technician moves the transducer along the skin over your abdomen. This test can be used to look for tumors in your liver, gallbladder, pancreas, or elsewhere in your abdomen, but it can’t look for tumors of the colon.
Endorectal ultrasound: This test uses a special transducer that is inserted into the rectum. It is used to see how far through the rectal wall a cancer has grown and whether it has reached nearby organs or tissues such as lymph nodes.
Intraoperative ultrasound: This exam is done during surgery. The transducer is placed directly against the surface of the liver, making this test very useful for detecting the spread of colorectal cancer to the liver. This allows the surgeon to biopsy the tumor, if one is found, while the patient is asleep.
Magnetic resonance imaging (MRI) scan
Like CT scans, MRI scans show detailed images of soft tissues in the body. But MRI scans use radio waves and strong magnets instead of x-rays. A contrast material called gadolinium may be injected into a vein before the scan to see details better.
MRI can be used to look at abnormal areas in the liver or the brain and spinal cord that could be cancer spread.
Chest x-ray
An x-ray may be done after colorectal cancer has been diagnosed to see if cancer has spread to the lungs.
Positron emission tomography (PET) scan
PET scans usually use a form of radioactive sugar that is put into the blood. Body cells take in different amounts of the sugar, depending on how fast they are growing. Cancer cells, which grow quickly, are more likely to take up larger amounts of the sugar than normal cells. A special camera is used to create a picture of areas of radioactivity in the body.
The picture from a PET scan is not as detailed as a CT or MRI scan, but it provides helpful information about whether abnormal areas seen on these other tests are likely to be cancer or not.
If you have already been diagnosed with cancer, your doctor may use this test to see if the cancer has spread to lymph nodes or other parts of the body. A PET scan can also be useful if your doctor thinks the cancer may have spread but doesn’t know where.
PET/CT scan: Some machines can do both a PET and CT scan at the same time. This lets the doctor compare areas of higher radioactivity on the PET scan with the more detailed picture of that area on the CT scan.
Angiography
Angiography is an x-ray test for looking at blood vessels. A contrast dye is injected into an artery, and then x-rays are taken. The dye outlines the blood vessels on x-rays.
If your cancer has spread to the liver, this test can show the arteries that supply blood to those tumors. This can help surgeons decide if the liver tumors can be removed and if so, it can help plan the operation. Angiography can also help in planning other treatments for cancer spread to the liver, like embolization.
Most all colorectal cancer will present by diagnostic colonoscopy for suspicious signs and symptoms (80%), asymptomatic, routine screening (11%), or incidental finding at an acute abdomen emergent admission (7%) 16. Patients diagnosed with routine cancer screening are frequently earlier stage compared to advanced disease of incidental surgical findings. Diagnostic colonoscopy’s triggers are blood per rectum (37%), abdominal pain (34%) and anemia (23%). Most common indications of emergency surgery are an obstruction (57%), peritonitis (25%) and perforation (18%). Tumor location on clinical presentation can be separated on left-sided with more changes in bowel habits and hematochezia, and right-sided with obscured anemia impacting on late stage at diagnosis. Late presentation with metastatic disease at diagnosis will depend on the symptoms at the organ-affected by the route of spread; to the liver via the portal system, to lungs via the inferior vena cava, to supraclavicular adenopathy via lymphatic or to neighbor structures by contiguous invasion. The provider should perform a thorough physical examination for signs of ascites, hepatomegaly, and lymphadenopathy. A comprehensive family history is of great relevance to identify familial clusters and inherent patterns that would alter surveillance and therapy on the high-risk patient.
Colorectal cancer treatment
Different types of treatment are available for patients with colon cancer. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer.
Six types of standard treatment are used 18:
Surgery
Surgery (removing the cancer in an operation) is the most common treatment for all stages of colon cancer. A doctor may remove the cancer using one of the following types of surgery:
- Local excision: If the cancer is found at a very early stage, the doctor may remove it without cutting through the abdominal wall. Instead, the doctor may put a tube with a cutting tool through the rectum into the colon and cut the cancer out. This is called a local excision. If the cancer is found in a polyp (a small bulging area of tissue), the operation is called a polypectomy.
- Resection of the colon with anastomosis: If the cancer is larger, the doctor will perform a partial colectomy (removing the cancer and a small amount of healthy tissue around it). The doctor may then perform an anastomosis (sewing the healthy parts of the colon together). The doctor will also usually remove lymph nodes near the colon and examine them under a microscope to see whether they contain cancer.
- Resection of the colon with colostomy: If the doctor is not able to sew the 2 ends of the colon back together, a stoma (an opening) is made on the outside of the body for waste to pass through. This procedure is called a colostomy. A bag is placed around the stoma to collect the waste. Sometimes the colostomy is needed only until the lower colon has healed, and then it can be reversed. If the doctor needs to remove the entire lower colon, however, the colostomy may be permanent.
After the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given chemotherapy or radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Radiofrequency ablation
Radiofrequency ablation is the use of a special probe with tiny electrodes that kill cancer cells. Sometimes the probe is inserted directly through the skin and only local anesthesia is needed. In other cases, the probe is inserted through an incision in the abdomen. This is done in the hospital with general anesthesia.
Cryosurgery
Cryosurgery is a treatment that uses an instrument to freeze and destroy abnormal tissue. This type of treatment is also called cryotherapy.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy).
Chemoembolization of the hepatic artery may be used to treat cancer that has spread to the liver. This involves blocking the hepatic artery (the main artery that supplies blood to the liver) and injecting anticancer drugs between the blockage and the liver. The liver’s arteries then deliver the drugs throughout the liver. Only a small amount of the drug reaches other parts of the body. The blockage may be temporary or permanent, depending on what is used to block the artery. The liver continues to receive some blood from the hepatic portal vein, which carries blood from the stomach and intestine.
The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
- External radiation therapy uses a machine outside the body to send radiation toward the cancer.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
The way the radiation therapy is given depends on the type and stage of the cancer being treated. External radiation therapy is used as palliative therapy to relieve symptoms and improve quality of life.
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells without harming normal cells.
Types of targeted therapies used in the treatment of colon cancer include the following:
- Monoclonal antibodies: Monoclonal antibodies are made in the laboratory from a single type of immune system cell. These antibodies can identify substances on cancer cells or normal substances that may help cancer cells grow. The antibodies attach to the substances and kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells.
- There are different types of monoclonal antibody therapy:
- Vascular endothelial growth factor (VEGF) inhibitor therapy: Cancer cells make a substance called VEGF, which causes new blood vessels to form (angiogenesis) and helps the cancer grow. VEGF inhibitors block VEGF and stop new blood vessels from forming. This may kill cancer cells because they need new blood vessels to grow. Bevacizumab and ramucirumab are VEGF inhibitors and angiogenesis inhibitors.
- Epidermal growth factor receptor (EGFR) inhibitor therapy: EGFRs are proteins found on the surface of certain cells, including cancer cells. Epidermal growth factor attaches to the EGFR on the surface of the cell and causes the cells to grow and divide. EGFR inhibitors block the receptor and stop the epidermal growth factor from attaching to the cancer cell. This stops the cancer cell from growing and dividing. Cetuximab and panitumumab are EGFR inhibitors.
- Immune checkpoint inhibitor therapy: PD-1 is a protein on the surface of T cells that helps keep the body’s immune responses in check. When PD-1 attaches to another protein called PDL-1 on a cancer cell, it stops the T cell from killing the cancer cell. PD-1 inhibitors attach to PDL-1 and allow the T cells to kill cancer cells. Pembrolizumab is a type of immune checkpoint inhibitor.
- There are different types of monoclonal antibody therapy:
- Angiogenesis inhibitors: Angiogenesis inhibitors stop the growth of new blood vessels that tumors need to grow.
- Ziv-aflibercept is a vascular endothelial growth factor trap that blocks an enzyme needed for the growth of new blood vessels in tumors.
- Regorafenib is used to treat colorectal cancer that has spread to other parts of the body and has not gotten better with other treatment. It blocks the action of certain proteins, including vascular endothelial growth factor. This may help keep cancer cells from growing and may kill them. It may also prevent the growth of new blood vessels that tumors need to grow.
Sigmoid colon resection
Removing the sigmoid colon is also called a sigmoid colectomy. The commonest indication for surgical resection of the sigmoid colon is a colorectal malignancy, and the resection should be carried out according to oncological principles 19:
- Resection margin 5 cm proximal and distal to tumor for colonic malignancies
- Circumferential resection margin for rectum, distal margin of 2 cm adequate
- Remove vasculature and lymphatic drainage at level of origin of primary feeding vessel
- Thus allowing resection of locoregional lymph node-bearing mesentery for cure and staging
- The fashioning of a well vascularized and tension-free anastomosis
Sigmoid colon resection can be carried out via open (laparotomy) or minimal access (laparoscopic, robotic) approaches.
- The open approach requires a sterile operating theater, an operating table that allows removal of the end segment and sidebars for mounting the attachments to place the patient’s legs in a Lloyd Davies position. All instruments can be found in a major laparotomy set, including bowel clamps.
- The laparoscopic approach in addition to the above set up requires a gas insufflator, display screens, laparoscopic camera, and instruments.
- For the robotic approach, the robot is required.
- Equipment for bowel anastomosis would be suture material for a handsewn anastomosis (absorbable braided or monofilament, strength 3/0).
Stapled anastomosis would require linear staplers for a side-to-side anastomosis (75 or 100mm in length), or a circular stapling device for an end-to-end anastomosis (diameter 28 mm to 33 mm, depending on patient size).
Sigmoid colon resection can be carried out as an open or laparoscopic procedure; the surgical principles remain the same 20.
The key to adequate resection is the blood supply to the colon. Resection for benign disease does not need to be as extensive, but resection for malignancy should aim to resect the named colonic vessels supplying the cancer-bearing portion of the colon as close to their origin as possible to yield an adequate number of lymph nodes in the colonic mesentery (> 12).
The bowel proximal and distal to the resection has to be mobilized to allow a tension-free anastomosis, and the anastomosis should have a good blood supply. Depending on expertise and equipment available, a bowel anastomosis can be performed hand-sewn or stapled.
For example, a formal right hemicolectomy entails ligation of the ileocolic, right colic (if present) and right branch of the middle colic artery. Proximal bowel division is carried out at the terminal ileum, and distal bowel division at the transverse colon. The anastomosis is conventionally formed as a side-to-side between the terminal ileum and the transverse colon.
Resection of a sigmoid colon tumor entails ligation of the inferior mesenteric artery and inferior mesenteric vein. Proximal bowel division is carried out at the distal descending colon, and distal bowel division at the upper rectum, above the peritoneal reflection. The anastomosis is conventionally formed as an end-to-end between the descending colon and the upper rectum with the help of a circular stapling device inserted via the anal canal.
Sigmoid colon resection contraindications
Colonic resection is classified as major surgery and should not be undertaken if the patient is physically not fit to sustain a major procedure. Reversible and modifiable risk factors should be addressed before surgery, and postoperatively, a patient may require intensive or high dependency facilities.
Sigmoid colon resection complications
Procedure-related complications can be divided into complications encountered during the surgery and post-operative complications 21.
Procedural complications include bleeding, most often venous in nature due to the handling of the mesocolon or during dissection of the greater omentum, and rarely from any of the named vessels.
However, an arterial bleed from the named vessels of the colon can be torrential and requires swift action, especially in laparoscopic procedures, where the bleeding can potentially obscure the view if it hits the camera.
Direct pressure where possible to temporarily arrest the bleeding buys time to strategise, reposition, request additional instruments, site further ports, if necessary, and definitively stop the bleed.
Another intra-operative complication is damage to surrounding structures. The structure most at risk is the left ureter. For left-sided surgery, it should always be identified. If an intra-operative injury (diathermy burn, transection) occurs and is recognised immediately, it can be repaired, and a ureteric stent should be placed to reduce the risk of stricture. If the injury is only diagnosed in the post-operative period, management depends on the extent and location of the injury, the general state of the patient and expertise available. A urological specialist should be consulted if available.
Post-operative complications include infections (wound, chest, urinary tract). Early mobilization, physiotherapy, incentive spirometry and removal of urinary catheters can prevent infections. Wound infection risk in clean-contaminated surgery is greatly reduced by giving prophylactic antibiotics within one hour of skin incision.
Anastomotic leak is a dreaded complication for all surgeons performing colonic resection and primary anastomosis. A high index of suspicion is indicated if postoperatively, a patient does not progress as expected, as signs and symptoms can be subtle to start with, especially if the leak is in the pelvis and the patient has a defunctioning stoma. Patients may have pyrexia, tachycardia, cardiac arrhythmias (new onset atrial fibrillation), complain of abdominal pain and bloating, and have a distended, tender, and potentially peritonitic abdomen. Inflammatory markers will be raised more markedly than expected in the post-operative period. Free air under the diaphragm may not be visible on an erect chest x-ray, but CT will show pneumoperitoneum and fluid around the anastomosis. In patients who have undergone anterior resection, it is advised to perform the scan with rectal contrast.
Depending on the severity of the leak and the patient’s general state, the management can include all or parts of the following:
- antimicrobial therapy,
- drainage of pus collections (percutaneously if patient stable and expertise available), and
- consideration for a re-look surgical procedure to wash and drain the abdominal cavity, inspect the anastomosis, and either defunction the patient or take the anastomosis apart and bring out the proximal bowel as an end stoma (akin to a Hartmann’s procedure).
Sigmoid colon resection recovery
Today elective colon resections have excellent outcomes. Most patients have a short stay in hospital of about four days. By paying attention to detail, the risk of wound infection is also minimized. Current data indicate that laparoscopic colectomy is as effective as open colectomy in preventing recurrence of cancer. Further, several clinical trials have shown that the risk of seeding is not increased at the port sites 22.
Sigmoid colon polyp
A sigmoid colon polyp is a small clump of cells that forms on the lining of the sigmoid colon. Most colon polyps are harmless. But over time, some colon polyps can develop into colon cancer, which is often fatal when found in its later stages. To be safe, doctors remove polyps and test them. Polyps can be removed when a doctor examines the inside of the large intestine during a colonoscopy.
There are two main categories of polyps, non-neoplastic and neoplastic.
- Non-neoplastic polyps include hyperplastic polyps, inflammatory polyps and hamartomatous polyps. These types of polyps typically do not become cancerous.
- Neoplastic polyps include adenomas and serrated types. In general, the larger a polyp, the greater the risk of cancer, especially with neoplastic polyps.
Anyone can develop colon polyps. You’re at higher risk if you’re 50 or older, are overweight or a smoker, or have a personal or family history of colon polyps or colon cancer.
Anyone can get polyps, but certain people are more likely than others. You may have a greater chance of getting polyps if you:
- Are over age 50
- Have had polyps before
- Have a family member with polyps
- Have a family history of colon cancer
Most colon polyps do not cause symptoms. If you have symptoms, they may include blood on your underwear or on toilet paper after a bowel movement, blood in your stool, or constipation or diarrhea lasting more than a week.
It’s important to have regular screening tests, such as a colonoscopy, because colon polyps found in the early stages can usually be removed safely and completely. The best prevention for colon cancer is regular screening for polyps.
See your doctor if you experience:
- Abdominal pain
- Blood in your stool
- A change in your bowel habits that lasts longer than a week
You should be screened regularly for polyps if:
- You’re age 50 or older.
- You have risk factors, such as a family history of colon cancer. Some high-risk individuals should begin regular screening much earlier than age 50.
Sigmoid colon polyp causes
Healthy cells grow and divide in an orderly way. Mutations in certain genes can cause cells to continue dividing even when new cells aren’t needed. In the colon and rectum, this unregulated growth can cause polyps to form. Polyps can develop anywhere in your large intestine.
There are two main categories of polyps, non-neoplastic and neoplastic. Non-neoplastic polyps include hyperplastic polyps, inflammatory polyps and hamartomatous polyps. Non-neoplastic polyps typically do not become cancerous.
Inflammatory polyps may be seen with ulcerative colitis or Crohn’s disease of the colon. Although the polyps themselves are not a significant threat, having ulcerative colitis or Crohn’s disease of the colon increases your overall risk of colon cancer.
Neoplastic polyps include adenomas and serrated types. Most colon polyps are adenomas. Serrated polyps may become cancerous, depending on their size and location in the colon. In general, the larger a polyp, the greater the risk of cancer, especially with neoplastic polyps.
Sigmoid colon polyp risk factors
Factors that may contribute to the formation of colon polyps or cancer include:
- Age. Most people with colon polyps are 50 or older.
- Inflammatory intestinal conditions, such as ulcerative colitis and Crohn’s disease.
- Family history. You’re more likely to develop colon polyps or cancer if you have a parent, sibling or child with them. If many family members have them, your risk is even greater. In some people, this connection isn’t hereditary.
- Tobacco and alcohol use.
- Obesity and lack of exercise.
- Race. African-Americans are at higher risk of developing colon cancer.
- Type 2 diabetes that isn’t well-controlled.
Hereditary polyp disorders
Rarely, people inherit genetic mutations that cause colon polyps to form. If you have one of these genetic mutations, you are at much higher risk of developing colorectal cancer. Screening and early detection can help prevent the development or spread of these cancers.
Hereditary disorders that cause colon polyps include:
- Lynch syndrome, also called hereditary nonpolyposis colorectal cancer. People with Lynch syndrome tend to develop relatively few colon polyps, but those polyps can quickly become malignant. Lynch syndrome is the most common form of inherited colon cancer and is also associated with tumors in the breast, stomach, small intestine, urinary tract and ovaries.
- Familial adenomatous polyposis (FAP), a rare disorder that causes hundreds or even thousands of polyps to develop in the lining of your colon beginning during your teenage years. If the polyps aren’t treated, your risk of developing colon cancer is nearly 100 percent, usually before age 40. Genetic testing can help determine your risk of FAP.
- Gardner’s syndrome, a variant of FAP that causes polyps to develop throughout your colon and small intestine. You may also develop noncancerous tumors in other parts of your body, including your skin, bones and abdomen.
- MYH-associated polyposis (MAP), a condition similar to FAP that is caused by mutations in the MYH gene. People with MAP often develop multiple adenomatous polyps and colon cancer at a young age. Genetic testing can help determine your risk of MAP.
- Peutz-Jeghers syndrome, a condition that usually begins with freckles developing all over the body, including the lips, gums and feet. Then noncancerous polyps develop throughout the intestines. These polyps may become malignant, so people with this condition have an increased risk of colon cancer.
- Serrated polyposis syndrome, a condition that leads to multiple serrated adenomatous polyps in the upper part of the colon. These polyps may become malignant.
Sigmoid colon polyp prevention
You can greatly reduce your risk of colon polyps and colorectal cancer by having regular screenings. Certain lifestyle changes also can help:
- Adopt healthy habits. Include plenty of fruits, vegetables and whole grains in your diet and reduce your fat intake. Limit alcohol consumption and quit tobacco. Stay physically active and maintain a healthy body weight.
- Talk to your doctor about calcium and vitamin D. Studies have shown that increasing your consumption of calcium may help prevent recurrence of colon adenomas. But it isn’t clear whether calcium has any protective benefits against colon cancer. Other studies have shown that vitamin D may have a protective effect against colorectal cancer.
- Consider your options if you’re at high risk. If you have a family history of colon polyps, consider having genetic counseling. If you’ve been diagnosed with a hereditary disorder that causes colon polyps, you’ll need regular colonoscopies starting in young adulthood.
Sigmoid colon polyp symptoms
Colon polyps often cause no symptoms. You might not know you have a polyp until your doctor finds it during an examination of your bowel.
But some people with colon polyps experience:
- Rectal bleeding. This can be a sign of colon polyps or cancer or other conditions, such as hemorrhoids or minor tears in your anus.
- Change in stool color. Blood can show up as red streaks in your stool or make stool appear black. A change in color may also be caused by foods, medications and supplements.
- Change in bowel habits. Constipation or diarrhea that lasts longer than a week may indicate the presence of a large colon polyp. But a number of other conditions can also cause changes in bowel habits.
- Pain. A large colon polyp can partially obstruct your bowel, leading to crampy abdominal pain.
- Iron deficiency anemia. Bleeding from polyps can occur slowly over time, without visible blood in your stool. Chronic bleeding robs your body of the iron needed to produce the substance that allows red blood cells to carry oxygen to your body (hemoglobin). The result is iron deficiency anemia, which can make you feel tired and short of breath.
Sigmoid colon polyp diagnosis
Screening tests play a key role in detecting polyps before they become cancerous. These tests can also help find colorectal cancer in its early stages, when you have a good chance of recovery.
Screening methods include:
- Colonoscopy, the most sensitive test for colorectal polyps and cancer. If polyps are found, your doctor may remove them immediately or take tissue samples (biopsies) for analysis.
- Virtual colonoscopy (CT colonography), a minimally invasive test that uses a CT scan to view your colon. Virtual colonoscopy requires the same bowel preparation as a colonoscopy. If a polyp is found, you’ll need a colonoscopy to have it removed.
- Flexible sigmoidoscopy, in which a slender, lighted tube is inserted in your rectum to examine it and the last third of your colon (sigmoid) and rectum. If a polyp is found, you’ll need a colonoscopy to have it removed.
- Stool-based tests. This type of test works by checking for the presence of blood in the stool or assessing your stool DNA. If your stool test is positive you will need a colonoscopy.
Sigmoid colon polyp treatment
Your doctor is likely to remove all polyps discovered during a bowel examination. The options for removal include:
- Removal with forceps or a wire loop (polypectomy). If a polyp is larger than 0.4 inches (about 1 centimeter), a liquid may be injected under it to lift and isolate the polyp from surrounding tissue so that it can be removed.
- Minimally invasive surgery. Polyps that are too large or that can’t be removed safely during screening are usually removed laparoscopically, which is performed by inserting an instrument called a laparoscope into the bowel.
- Colon and rectum removal. If you have a rare inherited syndrome, such as FAP, you may need surgery to remove your colon and rectum (total proctocolectomy).
Some types of colon polyp are far likelier to become malignant than are others. But a doctor who specializes in analyzing tissue samples (pathologist) usually must examine polyp tissue under a microscope to determine whether it’s potentially cancerous.
Follow-up care
If you have had an adenomatous polyp or a serrated polyp, you are at increased risk of colon cancer. The level of risk depends on the size, number and characteristics of the adenomatous polyps that were removed.
You’ll need follow-up screenings for polyps. Your doctor is likely to recommend a colonoscopy:
- In five to 10 years if you had only one or two small adenomas
- In three years if you had more than two adenomas, adenomas measuring 0.4 inches (about 1 centimeter) or larger, or certain adenomas
- Within three years if you had more than 10 adenomas
- Within six months if you had a very large adenoma or an adenoma that had to be removed in pieces
It’s important to fully prepare your colon before a colonoscopy. If stool remains in the colon and obstructs your doctor’s view of the colon wall, you will likely need a follow-up colonoscopy sooner than the guidelines specify.
Sigmoid colon polyp prognosis after treatment
Once a colorectal polyp is completely removed, it rarely comes back. However, at least 30% of patients will develop new polyps after removal. For this reason, your physician will advise follow-up testing to look for new polyps. This is usually done 3 to 5 years after polyp removal. Taking a daily aspirin or other non-steroidal anti-inflammatory drugs (NSAIDs) may reduce the risk of new polyps forming. If you had polyps removed, ask your physician if you should take this medication to help prevent them from coming back.
- Kahai P, Bhimji SS. Anatomy, Abdomen and Pelvis, Large Intestine. [Updated 2018 Dec 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470577[↩]
- Lieske B, Antunes C. Sigmoid Volvulus. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441925[↩][↩]
- Vandendries C, Jullès MC, Boulay-Coletta I et-al. Diagnosis of colonic volvulus: findings on multidetector CT with three-dimensional reconstructions. Br J Radiol. 2010;83 (995): 983-90. doi:10.1259/bjr/35714052[↩]
- Brant WE, Helms CA. Fundamentals of Diagnostic Radiology. Lippincott Williams & Wilkins. (2007) ISBN:0781761352[↩][↩]
- Salati U, Mcneill G, Torreggiani WC. The coffee bean sign in sigmoid volvulus. Radiology. 2011;258 (2): 651-2. doi:10.1148/radiol.101882[↩][↩]
- Foris LA, Patel K. Diverticulosis. [Updated 2018 Dec 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430771[↩][↩][↩][↩][↩]
- Schein M, Paladugn R. Diverticulitis. In: Holzheimer RG, Mannick JA, editors. Surgical Treatment: Evidence-Based and Problem-Oriented. Munich: Zuckschwerdt; 2001. Available from: https://www.ncbi.nlm.nih.gov/books/NBK6986[↩][↩]
- Kosmadakis G, Albaret J, da Costa Correia E, Somda F, Aguilera D. Gastrointestinal Disorders in Peritoneal Dialysis Patients. Am. J. Nephrol. 2018;48(5):319-325.[↩]
- Freckelton J, Holt D, Borsaru A, Gwini S, Croagh D, Moore G. The role of body composition in diverticular disease. Int J Colorectal Dis. 2018 Sep;33(9):1299-1302.[↩]
- Gao JY, Chen JF, Su H, Fang HY, Wu LP, Han YJ, Wang XM. Acute Massive Gastrointestinal Bleeding in the Elderly. J Coll Physicians Surg Pak. 2018 Jun;28(6):S78-S80.[↩]
- Tursi A. A critical appraisal of advances in the diagnosis of diverticular disease. Expert Rev Gastroenterol Hepatol. 2018 Aug;12(8):791-796.[↩]
- Schieffer KM, Kline BP, Yochum GS, Koltun WA. Pathophysiology of diverticular disease. Expert Rev Gastroenterol Hepatol. 2018 Jul;12(7):683-692.[↩]
- Špičák J, Kučera M, Suchánková G. Diverticular disease: diagnosis and treatment. Vnitr Lek. 2018 Summer;64(6):621-634.[↩]
- e.g., injection, coagulation (cautery, argon plasma coagulator), or mechanical devices (clips, bands, loops[↩]
- Almadi MA, Barkun AN. Patient Presentation, Risk Stratification, and Initial Management in Acute Lower Gastrointestinal Bleeding. Gastrointest. Endosc. Clin. N. Am. 2018 Jul;28(3):363-377.[↩]
- Recio-Boiles A, Cagir B. Cancer, Colon. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470380[↩][↩]
- Key Statistics for Colorectal Cancer. https://www.cancer.org/cancer/colon-rectal-cancer/about/key-statistics.html[↩]
- PDQ Adult Treatment Editorial Board. Colon Cancer Treatment (PDQ®): Patient Version. 2018 Aug 17. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK65880[↩]
- Lieske B, Bhimji SS. Colon Resection. [Updated 2018 Nov 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431079[↩]
- Zattoni D, Popeskou GS, Christoforidis D. Left colon resection with transrectal specimen extraction: current status. Tech Coloproctol. 2018 Jun;22(6):411-423.[↩]
- Alhassan N, Yang M, Wong-Chong N, Liberman AS, Charlebois P, Stein B, Fried GM, Lee L. Comparison between conventional colectomy and complete mesocolic excision for colon cancer: a systematic review and pooled analysis : A review of CME versus conventional colectomies. Surg Endosc. 2018 Sep 12[↩]
- McCombie AM, Frizelle F, Bagshaw PF, Frampton CM, Hewett PJ, McMurrick PJ, Rieger N, Solomon MJ, Stevenson AR., ALCCaS Trial group. The ALCCaS Trial: A Randomized Controlled Trial Comparing Quality of Life Following Laparoscopic Versus Open Colectomy for Colon Cancer. Dis. Colon Rectum. 2018 Oct;61(10):1156-1162.[↩]





{kind=link}