Contents
Status asthmaticus
Status asthmaticus is a severe asthma attack or the most severe form of asthma exacerbation which is a medical emergency that is poorly responsive to standard therapeutic measures, characterized by hypoxemia (a low level of oxygen in the blood), hypercarbia (an increase in carbon dioxide in the blood), and secondary respiratory failure 1, 2, 3. Status asthmaticus is a life-threatening condition and all patients with bronchial asthma are at risk of developing status asthmaticus. Two distinctive features are usually used to identify status asthmaticus, they are: severity and lack of response to bronchodilators. However, the latter condition is not always observed and thus the term status asthmaticus basically implies severity. “Severe acute asthma” is a new term which has replaced “status asthmaticus”. Nevertheless, a severe attack of asthma may occur suddenly or can take place after days or weeks of a progressive deterioration. A status asthmaticus can be “acute” or “subacute” according to the rate of deterioration; therefore the term “severe acute asthma” is misleading. Since the term status asthmaticus essentially implies severity, severe attacks would be better described as “severe exacerbation of asthma”. Classification of the severe exacerbation of asthma into two types (acute and subacute), could help to reveal the etiology of the attack and might also be relevant to the management of the patient. For instance an acute severe exacerbation of asthma can be seen in brittle asthma and in patients with aspirin intolerance. On the other hand, patients with the subacute form are refractory to bronchodilators and must be treated with corticosteroids.
An estimated 3% to 16% of hospitalized adult asthmatic patients progress to respiratory failure requiring ventilatory support, although the statistics might be lower in children. Multiple observational studies have reported a higher incidence of status asthmaticus in women, among African Americans and in subjects with adult-onset asthma, which developed after an age of 17 years 4.
If not recognized and managed appropriately, status asthmaticus portends risk of acute ventilatory failure and even, death. The mortality rate in status asthmaticus ranges from 3.5% to 8.3% 5. Afessa et al. 6 have reported mortality of around 10% in intensive care unit (ICU) patients admitted with status asthmaticus. Therapeutic approach in acute severe asthma is based on oxygen supply, high doses of nebulized beta2-agonists and systemic corticosteroids administered intravenously or orally. Second line therapy is comprised of methyloxantines, nebulized cholinolitics and management of electrolytes and water balance. Status asthmaticus resulting in acute respiratory failure will often require invasive or non-invasive mechanical ventilation. Mortality in patients with asthma who require mechanical ventilation might exceed 20%. International guidelines for management of status asthmaticus have been published recently, but those recommendations often remain unknown. Thus there is an urgent need for elaboration of national standards on managing acute severe asthma and putting it into clinical practice. Status asthmaticus, especially a severe one, should be treated in a respiratory intermediate intensive care unit.
Increasing standardization of low tidal volume ventilation strategies, avoidance of prolonged neuromuscular blockade, and assist control mode ventilation hopefully helped reduce this trend even further over the past decade. In a retrospective review of 280 hospitalizations over a period of 30 years in the University of Texas, Health Science Center, San Antonio, 61.2 % patients required intubation and mechanical ventilation. Mortality rate was about 0.35% 7.
In spite of advances in pharmacotherapy and access to early diagnosis and treatment of asthma itself, status asthmaticus remains one of the most common causes of visits to the emergency department. No single clinical or diagnostic index has been known to predict clinical outcome in status asthmaticus. Hence, a multi-pronged and time-sensitive approach combining symptoms and signs, assessment of airflow and blood gas, and a rapid escalation of treatment based on initial treatment response are favored to diagnose and manage status asthmaticus.
Status asthmaticus pathophysiology
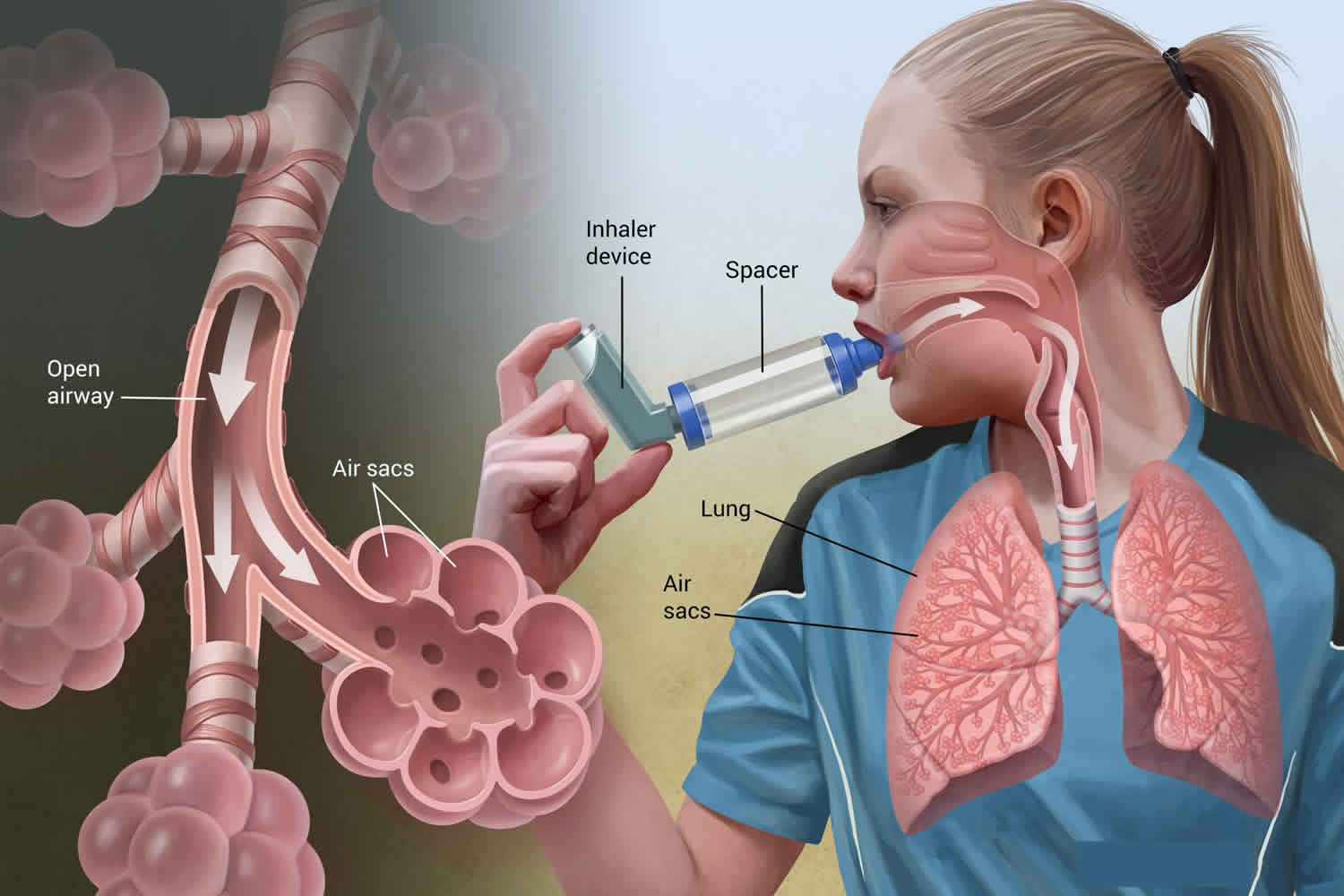
At a physiological level, premature airway closure during exhalation causes an increase in functional residual capacity and air trapping. Heterogeneous distribution of air trapping results in ventilation-perfusion mismatch and hypoxemia- triggering anaerobic metabolism and lactic acidosis. It is offset initially by respiratory alkalosis and is compounded once respiratory fatigue and respiratory acidosis ensue.
Exposure to an allergen or trigger causes a characteristic form of airway inflammation in susceptible individuals, exemplified by mast cell degranulation, release of inflammatory mediators, infiltration by eosinophils, and activated T lymphocytes. Multiple inflammatory mediators may be involved, including interleukin (IL)–3, IL-4, IL-5, IL-6, IL-8, IL-10, and IL-13, leukotrienes, and granulocyte-macrophage colony-stimulating factors (GM-CSFs). These, in turn, incite involvement of mast cells, neutrophils, and eosinophils.
Physiologically, acute asthma has two components: an early, acute bronchospastic aspect marked by smooth muscle bronchoconstriction and a later inflammatory component resulting in airway swelling and edema.
Early bronchospastic response
Within minutes of exposure to an allergen, mast cell degranulation is observed along with the release of inflammatory mediators, including histamine, prostaglandin D2, and leukotriene C4. These substances cause airway smooth muscle contraction, increased capillary permeability, mucus secretion, and activation of neuronal reflexes. The early asthmatic response is characterized by bronchoconstriction that is generally responsive to bronchodilators, such as beta2-agonist agents.
Later inflammatory response
The release of inflammatory mediators primes adhesion molecules in the airway epithelium and capillary endothelium, which then allows inflammatory cells, such as eosinophils, neutrophils, and basophils, to attach to the epithelium and endothelium and subsequently migrate into the tissues of the airway. Eosinophils release eosinophilic cationic protein (ECP) and major basic protein (MBP). Both ECP and MBP induce desquamation of the airway epithelium and expose nerve endings. This interaction promotes further airway hyperresponsiveness in asthma. This inflammatory component may even occur in individuals with mild asthma exacerbation.
Bronchospasm, mucus plugging, and edema in the peripheral airways result in increased airway resistance and obstruction. Air trapping results in lung hyperinflation, ventilation/perfusion (V/Q) mismatch, and increased dead space ventilation. The lung becomes inflated near the end-inspiratory end of the pulmonary compliance curve, with decreased compliance and increased work of breathing.
The increased pleural and intra-alveolar pressures that result from obstruction and hyperinflation, together with the mechanical forces of the distended alveoli, eventually lead to a decrease in alveolar perfusion. The combination of atelectasis and decreased perfusion leads to V/Q mismatch within lung units. The V/Q mismatch and resultant hypoxemia trigger an increase in minute ventilation.
Complications
In the early stages of acute asthma, hyperventilation may result in respiratory alkalosis. This is because obstructed lung units (slow compartment) are relatively less numerous than unobstructed lung units (fast compartment). Hyperventilation allows carbon dioxide removal via the fast compartment. However, as the disease progresses and more lung units become obstructed, an increase in the slow compartments occurs, resulting in decreased ability for carbon dioxide removal and eventually causing hypercarbia.
Status asthmaticus cause
The time course of progression, as well as the severity of airway obstruction, follows 2 distinct patterns 8.
- One subgroup if appropriately documented, shows a slow subacute worsening of peak expiratory flow rate (PEFR) over days, known as “slow onset asthma exacerbation.” This patient subgroup usually has intrinsic patient induced factors of predisposition- including inadequate inhaler regimen, suboptimal compliance, psychological stressor, among others.
- The other phenotype, known as “sudden onset asthma exacerbation” presents with severe deterioration within hours. They often correlate with sudden massive exposure to external triggers like predisposed allergens, food articles, sulfites, among others.
Eighty percent to 85% of asthma fatalities are in the subgroup of slow onset asthma exacerbation, perhaps reflecting an inadequate disease control over time. In contrast to the sudden onset exacerbation phenotype, which presents mostly with clear airways, slow onset exacerbation patients have extensive airway inflammation and mucus plugging 9.
Physiologically, acute asthma is divided into two phases. An early bronchospastic phase is observed within minutes after exposure to the allergen with mast cell degranulation and release of inflammatory mediators like histamine, prostaglandin D2, and leukotriene C4 3. A later inflammatory phase causing airway swelling and edema due to eosinophils released eosinophilic cationic proteins (ECP) and major basic protein (MBP) 3.
Increasing understanding of the pathophysiology of asthma at the histological level over the last two decades has emphasized airway inflammation as the primary player, over and above smooth muscle contraction, and airway hyperresponsiveness 3. An interplay of mast cells, T lymphocytes, and epithelial cells results in a circulatory surge of inflammatory cells and cytokines. Histamines, leukotrienes, and platelet-activating factors are found in increased concentrations locally and systemically. Lymphocytic and eosinophilic submucosal infiltrates in tracheal and bronchial biopsy specimens are reportedly associated with poorer outcomes in adult patients with asthma 10.
Destruction of cilia and epithelial denudation render nerve endings irritable, resulting in hyperreactivity. Inflammation also causes hypertrophy and hyperfunctioning of goblet cells and mucous glands resulting in mucus plugging.
The scheming of the catastrophe at the cellular level is orchestrated by a dysregulated parasympathetic overdrive, mediated through pulmonary vagus innervation in the parasympathetic ganglia of small bronchi. The release of postganglionic acetylcholine causes bronchoconstriction and hypersecretion through muscarinic receptors, while the inhibitory M2 receptors are often dysfunctional in individuals with atopy, sustained exposure to allergens, viral infection, and chronic inflammation.
Risk factors for status asthmaticus
Asthma results from a number of factors, including genetic predisposition and environmental factors. Patients often have a history of atopy. The severity of asthma has been correlated with the number of positive skin test results.
Gastroesophageal reflux disease is another risk factor for asthma, with studies indicating that the reflux of gastric contents with or without aspiration can trigger asthma in susceptible children and adults. Animal studies have shown that the instillation of even minute amounts of acid into the distal esophagus can result in marked increases in intrathoracic pressure and airway resistance. This response is thought to be due to vagal and sympathetic neural responses.
Risk factors for developing severe or persistent status asthmaticus include the following 11 12:
- History of previous intensive care unit (ICU) admissions, with or without intubation and mechanical ventilatory support.
- History of near fatal asthma in the past requiring endotracheal intubation is the greatest single predictor of death from bronchial asthma 13.
- Similarly, poor patient perception of dyspnea and hypercapnia due to a blunted hypoxic ventilatory response rendered by the chronicity of severe disease, or even psychiatric illness is also an ominous risk factor 14.
- Recurrent hospitalizations or asthma exacerbation in spite of chronic oral steroid use, late presentation since the onset of symptoms, altered mental status and sleep deprivation during an ongoing presentation can also be bad prognostic markers of a favorable outcome to initial treatment.
- History of coronary artery disease poses a risk of cardiological adverse events with therapy itself. All these in medical history should alert the evaluating clinical team for a level of preparedness towards risk of imminent status asthmaticus.
- History of increased use of home bronchodilator treatment without improvement or effect.
- Frequent emergency department visits and/or hospitalization (implies poor control)
- Less than 10% improvement in peak expiratory flow rate (PEFR) from baseline despite treatment.
- History of syncope or seizures during acute exacerbation.
- Oxygen saturation below 92% despite supplemental oxygen.
- Subgroup of asthma patients who are poor perceivers of dyspnea are a greater risk of intubation and death 15.
Status asthmaticus signs and symptoms
Status asthmaticus is considered a medical emergency. Status asthmaticus is the extreme form of an asthma exacerbation that can result in hypoxemia, hypercarbia, and secondary respiratory failure.
Patients with status asthmaticus have severe dyspnea that has developed over hours to days. In most cases, there is a lead time of several days 16. Frequently, these individuals have a previous history of endotracheal intubation and mechanical ventilation, frequent emergency department visits, and previous use of systemic corticosteroids.
Status asthmaticus stages
The 4 stages of status asthmaticus are based on arterial blood gas (ABG) progressions in status asthma. Patients in stage 1 or 2 may be admitted to the hospital, depending on the severity of their dyspnea, their ability to use accessory muscles, and their PEF values or FEV1 after treatment (>50% but < 70% of predicted values).
Patients with arterial blood gas (ABG) determinations characteristic of stages 3 and 4 require admission to an ICU. The PEF value or FEV1 is less than 50% of the predicted value after treatment.
Stage 1
Patients are not hypoxemic, but they are hyperventilating and have a normal PO2. Data suggest that to possibly facilitate hospital discharge, these patients may benefit from ipratropium treatment via a handheld nebulizer in the emergency setting as an adjunct to beta-agonists.
Stage 2
This stage is similar to stage 1, but patients are hyperventilating and hypoxemic. Such patients may still be discharged from the emergency department, depending on their response to bronchodilator treatment, but will require systemic corticosteroids.
Stage 3
These patients are generally ill and have a normal PCO2 due to respiratory muscle fatigue. Their PCO2 is considered a false-normal value and is a very serious sign of fatigue that signals a need for expanded care. This is generally an indication for elective intubation and mechanical ventilation, and these patients require admission to an ICU. Parenteral corticosteroids are indicated, as is the continued aggressive use of an inhaled beta2-adrenergic bronchodilator. These patients may benefit from theophylline.
Stage 4
This is a very serious stage in which the PO2 is low and the PCO2 is high, signifying respiratory failure. These patients have less than 20% of predicted lung function or FEV1 and require intubation and mechanical ventilation.
Patients in stage 4 should be admitted to an ICU. Switching from inhaled beta2-agonists and anticholinergics to metered-dose inhalers (MDIs) via mechanical ventilator tubing is indicated. Parenteral corticosteroids are essential, and theophylline may be added, as with patients in stage 3.
Status asthmaticus complications
Acute Hypotension on Mechanical Ventilation
Acute hypotension beyond the initial period of sedation and paralytic effect post-intubation needs immediate bedside intervention in status asthmaticus patients 17. The first and most time-sensitive pathology to be ruled out is tension pneumothorax. If bedside clinical examination, ultrasound or chest x-ray support so, it needs to be managed immediately with tube thoracostomy. Apart from sedation and hypovolemia as other potential causes, a common etiology of hypotension in mechanically ventilated asthma patients is dynamic hyperinflation causing air trapping and auto-PEEP generation. It can be detected by observing flow pattern in ventilator graphics and inability to return airflow to baseline. It is confirmed by measuring total PEEP with expiratory breath hold and then managed by increasing exhalation time, either by reducing the tidal volume or respiratory rate. Sometimes deeper sedation or paralysis may also be necessary.
Ventilator applied PEEP should be kept in moderation in status asthmaticus patients because of the risk of barotrauma and hypotension as well.
In patients without raised intracranial pressure or severely depressed myocardial function, purposeful hypoventilation and permissive hypercapnia is, therefore, an often practiced strategy for above reasons. More importance is paid to a ph target than a target PCO2, and ph greater than 7.25 is generally well tolerated.
High peak pressure with stable plateau pressure on the ventilator should also prompt effort at clearance of airway and endotracheal tube from secretion as it tends to be thick and tenacious in this subgroup of patients. Larger lumen endotracheal tube (7.5 or 8 Fr) is preferred due to higher airway resistance and the need for airway clearance.
Other Complications
Apart from complications related to neuromuscular blockade and those that are outcome of the pathophysiology of asthma itself, other commonly reported complications are electrolyte abnormalities, hypotension, and dysrhythmias 18.
Severe hypotension and respiratory acidosis in refractory cases have resulted in myocardial infarction, hypoxic and anoxic encephalopathy and death.
Status asthmaticus diagnosis
Physical examination
Patients are usually tachypneic upon examination and, in the early stages of status asthmaticus, may have significant wheezing. Initially, wheezing is heard only during expiration, but wheezing later occurs during expiration and inspiration.
The chest is hyperexpanded, and accessory muscles, particularly the sternocleidomastoid, scalene, and intercostal muscles, are used. Later, as bronchoconstriction worsens, the wheezing may disappear, which may indicate severe airflow obstruction.
Normally, the difference in systolic blood pressure between inspiration and expiration does not exceed 15 mm Hg. In patients with severe asthma, a difference of greater than 25 mm Hg usually indicates severe airway obstruction.
An inability to speak more than one or two words at a time may also be observed in the later stages of an acute asthma episode. Ventilation/perfusion mismatch results in decreased oxygen saturation and hypoxia. Vital signs may show tachycardia and hypertension. The peak flow rate should be included in the vital signs in patients who are able to cooperate and who are able to tolerate the peak flow maneuver without significant distress.
The patient’s level of consciousness may progress from lethargy to agitation, air hunger, and even syncope and seizures. If untreated, prolonged airway obstruction and marked increase in the work of breathing may eventually lead to bradycardia, hypoventilation, and even cardiorespiratory arrest.
Brenner and colleagues 19 demonstrated certain hemodynamic traits in patients who assumed an upright position than supine. They tend to have a significantly higher heart and respiratory rate along with pulsus paradoxes, a significantly lower PaO2 and lower peak expiratory flow rate (PEFR). However, the progressive decline in clinical and mental status in late presentation of status asthmaticus may also counter-intuitively lead patients to assume a supine position. That alone should not be a decision maker. After initial treatment, a diaphoretic patient, preferring to sit upright, unable to speak complete sentences or using accessory muscles of respiration all point toward status asthmaticus.
One of the circulatory consequences of status asthmaticus apart from tachycardia and tachypnea is also a large respiratory phase variation in pleural pressure. The increased inspiratory effort against obstructed airway results in augmented negative intrathoracic pressure. This results in reduced left ventricular filling and outflow due to a combination of (1) septal deviation to the left due to an enlarged RV, (2) increased LV afterload, and (3) increased RV afterload due to increase in pulmonary arterial pressure. Systolic blood pressure, therefore, tends to fall at the height of inspiration. Pulsus paradoxus is the difference between end-expiratory and end-inspiratory systolic blood pressure. It is augmented to more than 12 mm Hg in status asthmaticus, although may paradoxically decline in late-stage with increasing fatigability and loss of respiratory drive 20.
Tachycardia greater than 120 can be an indicator of disease severity as well as treatment response to beta agonists. Grossman et al. demonstrated that successful treatment results in a 24-hour drop in heart rate from 120 per minute to 105 per minute. Sinus tachycardia is the predominant rhythm, although supraventricular and ventricular arrhythmias have also been reported 21.
Classic wheezing, as an indicator of bronchospasm, is poorly reliable, as the extent of alveolar airflow is so significantly impaired in these subsets of patients that it cannot generate a wheeze before bronchodilation.
General examination
The peak flow rate is a standard measure of airflow obstruction and is relatively simple to perform. Most patients with more than a mild exacerbation of asthma have hypoxia and decreased oxygen saturation due to V/Q mismatch. Oxygen saturation may increase following the use of bronchodilators secondary to an increase in V/Q mismatch. Some patients prefer to remain seated and leaning forward, rather than assuming a supine position.
Retractions (ie, intercostal and subcostal) and the use of abdominal muscles may be observed in patients with status asthmaticus. The use of accessory muscles has been shown to correlate with the severity of airflow obstruction. An abnormally prolonged expiratory phase with audible wheezing can be observed. Patients with moderate to severe asthma are often unable to speak in full sentences.
Dehydration can occur in adults, but is observed less frequently than in children.
Cardiovascular symptoms may include tachycardia or hypertension in mild to moderate asthma. With worsening hypoxemia, hypercarbia, marked air trapping, and hyperinflation, the ventricular stroke volume is compromised and hypotension and bradycardia may be observed.
CNS status ranges from wide awake to lethargic and from agitated to comatose. As hypoxemia progresses, lethargy progresses to agitation caused by air hunger. As more lung units become obstructed, hypoxemia worsens and hypercarbia develops. Both hypoxemia and hypercarbia can lead to seizures and coma and are late signs of respiratory compromise.
Examination of the respiratory system
Wheezing occurs from air moving through narrowed, obstructed airways. Thus exhalation results in turbulent airflow and produces wheezes. Although asthma is the most common cause of wheezing, anything that causes airway obstruction and narrowing that results in turbulent airflow may generate wheezes. Therefore, not all wheezing is asthma.
Auscultation often reveals bilateral expiratory and possibly inspiratory wheezes and crackles. Air entry may or may not be diminished or absent, depending on severity. Remember, the silent chest may herald impending respiratory failure in a patient too obstructed or fatigued to generate wheezing.
If tension pneumothorax develops, signs of tracheal deviation to the opposite side, decreased or absent air entry on the affected side, shift of the location of heart sounds, and hypotension may be evident. Air leaks may also result in pneumomediastinum and subcutaneous emphysema.
In moderate to severe status asthmaticus, abdominal muscle use can cause symptoms of abdominal pain.
Pulsus paradoxus (a decrease in the systolic blood pressure during inspiration) results from a decrease in cardiac stroke volume with inspiration due to greatly increased left-ventricular afterload. This increase is generated by the dramatic increase in negative intrapleural and transmural pressure in a patient struggling to breathe against significant airways obstruction. Pulsus paradoxus of greater than 20 mm Hg correlates well with the presence of severe airways obstruction (ie, forced expiratory volume in 1 second [FEV1] < 60% predicted).
Measurement of airflow obstruction can be challenging to perform but is best achieved at the bedside with an assessment of PEFR than FEV1 22. Reduction of both values by 50% from personal best of the patient is an indicator of status. The absolute value of PEFR less than 120 L per minute and FEV1 less than 1 L corresponds with the proportional reduction. These absolute numbers should prompt an assessment of arterial blood gas (ABG) immediately 23. Initial blood gas results indicate respiratory alkalosis with hypoxemia. Therefore, developing respiratory acidosis or elevated PCO2 is indicators of status asthmaticus that is indicative of the need for ventilatory support 24. However, it should not be the lone decision maker and should be coupled with a serial physical examination, evidence of worsening mentation, and fatigability or hemodynamic alterations.
Mountain and colleagues 14, in their study of 229 hospitalized patients with acute asthma, detected a 28% incidence of anion gap metabolic acidosis, caused by rising lactate.
ECG may also show transient and reversible signs of right heart strain including peaked P wave or right axis deviation.
Chest radiography has little role to play in predicting the course of status asthmaticus, other than ruling out alternate etiologies or associated complicating diagnoses.
Laboratory and imaging studies
The selection of laboratory studies depends on historical data and patient condition. Tests that should be performed in patients with status asthmaticus include the following:
- Complete blood cell (CBC) count
- Arterial blood gas (ABG) analysis
- Serum electrolyte levels
- Serum glucose levels
- Peak expiratory flow measurement
- Chest radiography
- Electrocardiogram (in older patients)
- Blood theophylline levels (if indicated)
- IgE level in selected patients
Arterial Blood Gas
An arterial blood gas (ABG) value can be obtained to assess the severity of the asthma attack and to substantiate the need for more intensive care. However, the use of blood gas determination is controversial. The information generated by this measurement may be helpful in determining whether or not to intubate a patient with asthma. However, such decisions are usually made on the basis of clinical grounds in a patient who is either in respiratory arrest or impending respiratory arrest.
If a patient with acute asthma has adequate peripheral oxygen saturation, is receiving further therapy, and does not warrant immediate intubation, then the usefulness of blood gas data should be weighed against the potential pain and agitation that running this test may cause in a child. Improvement or deterioration in acute asthma can generally be followed clinically. Indwelling arterial catheters reduce the pain issue and generate highly reliable and reproducible information.
Arterial blood gas (ABG) determinations are indicated when the peak expiratory flow (PEF) rate or the forced expiratory volume in 1 second (FEV1) is less than or equal to 30% of the predicted value or when the patient shows evidence of fatigue or progressive airway obstruction despite treatment.
The 4 stages of blood gas progression in persons with status asthmaticus are as follows:
- Stage 1 – Characterized by hyperventilation with a normal partial pressure of oxygen (PO2)
- Stage 2 – Characterized by hyperventilation accompanied by hypoxemia (ie, a low partial pressure of carbon dioxide [PCO2] and low PO2)
- Stage 3 – Characterized by the presence of a false-normal PCO2; ventilation has decreased from the hyperventilation present in the second stage; this is an extremely serious sign of respiratory muscle fatigue that signals the need for more intensive medical care, such as admission to an ICU and, probably, intubation with mechanical ventilation.
- Stage 4 – Characterized by a low PO2 and a high PCO2, which occurs with respiratory muscle insufficiency; this is an even more serious sign that mandates intubation and ventilatory support.
Chest Radiography
Obtain a chest radiograph to evaluate for pneumonia, pneumothorax, pneumomediastinum, congestive heart failure (CHF), and signs of chronic obstructive pulmonary disease, which would complicate the patient’s response to treatment or reduce the patient’s baseline spirometry values.
Chest radiography is indicated in patients who have an atypical presentation or in those who do not respond to therapy.
Status asthmaticus treatment
The initial therapy of status asthmaticus includes oxygen, repetitive administration of inhaled beta2-agonists and ipratropium, and systemic corticosteroids. The aim of these treatments is to improve airflow obstruction and hypoxemia as quickly as possible. For patients who do not respond to initial therapy, magnesium sulphate, aminophylline and intravenous salbutamol are suggested 25, 26. Depending on local or national guidelines, intravenous salbutamol is used as second- or third-line treatment. Intensive care admission is often needed for continuous monitoring 27. Intravenous salbutamol may be more effective in severe asthma as delivery of inhaled drugs to airways may be attenuated and unpredictable as a result of severe airflow obstruction 28.
Salbutamol (albuterol) is a selective beta2-adrenoreceptor agonist with potent smooth muscle relaxant properties, and is a chiral compound with (R)- and (S)-enantiomers. The pharmacologic activity of salbutamol resides predominantly in the (R)-enantiomer, with little or no activity attributed to the (S)-enantiomer 29. Moreover, there are concerns that particularly high exposure to S-salbutamol may have negative effects. The primary route of elimination of salbutamol is by sulfate conjugation (SULT1A3), followed by renal excretion. Up to 50% of salbutamol is excreted unchanged in urine 30. The elimination of (R)-salbutamol is much more rapid than that of (S)-salbutamol, which leads to relatively higher plasma concentrations of (S)-salbutamol with the same continuous infusion 31.
Status asthmaticus guidelines
There are no specific guidelines for managing status asthmaticus 32. The use of beta-agonists (via inhalation nebulizer or intravenous treatment), intravenous corticosteroids, and, in extreme cases, mechanical ventilation have been alluded to in previous sections.
The most important guideline is prevention. Adherence to the guidelines of the National Heart-Lung and Blood Institute in the management of asthma in an outpatient setting results in future prevention of recurrent attacks of status asthmaticus. This has been studied by Miller at al 33 adherence to an asthma protocol resulted in less usage of rescue bronchodilator and systemic corticosteroid therapy.
Indication for Hospitalization and ICU
Serial measurement of PEFR is a practical and reliable predictor of severity and need for hospitalization. Stein and Cole found that a significant improvement in PEFR, 2 hours after treatment predicted the need for hospitalization, even though initial PEFR on presentation did not (improvement noted from a median of 250 L per minute to 330 L per minute). Rodrigo and Rodrigo demonstrated a similar pattern with treatment response in FEV1, although it may not be the most practical approach at the bedside 34.
A favorable response to initial treatment of status asthmaticus should be a visible improvement in symptoms which sustains 30 minutes or beyond the last bronchodilator dose, and a PEFR greater than 70% of predicted.
On the other hand, patients with evidence of continuing clinical decline or less than 10% improvement in PEFR or less than 40% of predicted, should be considered for admission to the intensive care unit. Anyone with worsening evidence of respiratory failure, alteration of mental status, arrhythmia, cardiac or respiratory arrest, or complications like pneumothorax or pneumomediastinum naturally requires ICU admission along with aggressive resuscitation measures if consistent with their goals of care.
FEV1 or PEFR between 40% to 70% of predicted after initial treatment in the emergency room is considered as “inadequate response.” Duration of management in the hospital does play a role in these subsets of patients. Kelsen and colleagues showed a 50% relapse rate in patients treated for 2 hours or less in a facility as opposed to 4% in those treated and observed for an additional 2 to 4 hours. The consensus, therefore, varies anywhere between 4 to 6 hours of treatment in a facility in this group of patients before deciding on admission versus discharge. A poor psychosocial makeup or a hostile home environment with obvious exposure to triggers may tilt the decision in favor of hospitalization.
Status asthmaticus medication
Beta Agonists
Short-acting inhaled beta-agonists are the drug of first choice in acute asthma 35. Albuterol is preferred over metaproterenol in that class because of its higher beta 2 selectivities and longer duration of action. The dose-response curve and duration of action of these medications are adversely affected by a combination of patient factors including preexisting bronchoconstriction, airway inflammation, mucus plugging, poor patient effort, and coordination. Therefore, larger and more frequent dosing than conventional therapy is necessary. Initial treatment consists of 2.5 mg of albuterol (0.5 mL of a 0.5% solution in 2.5 mL normal saline) by nebulization every 20 minutes for 60 minutes (three doses) followed by treatments hourly during the first several hours of therapy. Interestingly, Idris and colleagues demonstrated that even in patients with severe disease, 4 puffs of albuterol (0.36 mg) delivered with a metered dose inhaler (MDI) and spacer was as effective as a 2.5-mg dose by nebulization. In an ER setting, a nebulizer is still preferred because of less need for supervision, coordination and continued instructions.
An area that needs clarity is the appropriate mode of delivery of these inhaled medications in a ventilated patient. So far consensus prevails over a higher dosage required to achieve physiologic benefits compared to non-intubated patients. However, there is an ongoing debate about the use of MDI versus nebulizers, the appropriate mode of ventilation, the exact site of the connection of the delivery device on the ventilator circuit among others. The optimal delivery device has been a point of polarizing opinion. Mcintyre and colleagues demonstrated that only 2.9% of a radioactive aerosol was deposited in the lungs when delivered by a small volume nebulizer. They, therefore, advocated use of MDI via an adapter attached to the inspiratory limb of the ventilator circuit. However, their findings were refuted by a subsequent study by Manthous and colleagues demonstrating a poor effect on inspiratory flow-resistive pressure by MDI as opposed to nebulized albuterol 36. Assessment of airway peak to pause pressure gradient can be a rational indicator to use when either one of the delivery modes is used. A 15% or greater decline in the gradient is considered to be a favorable response to be aimed for, with repetitive doses, monitoring for toxicity 37.
Subcutaneous epinephrine or terbutaline, used in the past, have fallen out of favor due to their toxicity profile, as has direct endotracheal instillation of epinephrine due to lack of demonstrated efficacy and evidence-based studies.
Intravenous beta agonists are not routinely recommended although there are reports of center-specific use in younger patients with status asthmaticus, nonresponsive to inhaled therapy demonstrating persistent severe hyperinflation of airways.
There have been more recent concerns with several studies showing a correlation between asthma mortality and use of inhaled beta-agonists. Suissa and colleagues demonstrated that risk of asthma mortality increases drastically with use of 1.4 canisters per month or more of inhaled beta-agonists.
The Executive Committee of the American Academy of Allergy and Immunology published a position statement on the use of inhaled beta-agonists in asthma 38.
Conclusions
- More than 1 canister per month use of beta-agonists is a marker for severe asthma.
- Heavy or increased use of beta-agonists warrants additional therapy such as the use of corticosteroids.
- Beta-agonists may make asthma worse, but the available data do not allow for a definitive conclusion regarding this controversy.
- Patients currently using beta-agonists should slowly withdraw nonessential doses and use them only for rescue purposes.
However significant the concerns are regarding their long-term use, the use of short-acting inhaled beta agonists should not be withheld or underdosed during acute attacks, and they remain the drug of first choice under those circumstances.
Corticosteroids
Most available data support a distinct benefit of corticosteroids in status asthmaticus in an emergency setting 39. Rowe et al 40. in their meta-analysis of 30 randomized controlled trials concluded that use of steroids in emergency department significantly reduces rates of admission and number of future relapses in subsequent 7 to 10 days. Route of administration did not make a difference, and McFadden based on analysis of available data came up with a recommended dose of 150 to 225 mg per day of prednisone or its equivalent to reach maximum therapeutic benefit. Littenberg and Gluck also demonstrated a significant reduction in hospitalization with a methylprednisolone dose of 125 mg intravenously on presentation in the emergency room. Currently available data, therefore, support the approach of 60 to 125 mg methylprednisolone intravenously every 6 hours for the initial 24 hours of treatment of status asthmaticus. Oral steroids are usually required for the next 10 to 14 days.
In a physiologic level, steroids not only reduce airway inflammation and mucus production but also potentiates beta-agonist activity in smooth muscles and reduces beta agonists tachyphylaxis in patients with severe asthma.
Anticholinergics
Anticholinergics have a variable response in acute exacerbation with a somewhat underwhelming bronchodilatory role. However, they can be useful in patients with bronchospasm induced by beta-blockade or severe underlying obstructive disease with FEV1 less than 25% of predicted.
Bryant and Rogers demonstrated that 0.25 mg of ipratropium bromide with 5 mg of albuterol by nebulizer resulted in greater improvement in FEV1 than albuterol alone. The response time was also much faster than corticosteroids with a detectable change in FEV1 within 19 minutes. Nebulized glycopyrrolate can also be an alternative although it is not as much in vogue in the United States. Available data and practice still recommend anticholinergics as second-line agents in status asthmaticus patients with inadequate response to beta agonists or steroids. A 0.5-mg dose of Ipratropium by nebulization in conjunction with albuterol is the consensus choice.
Magnesium Sulfate
Magnesium inhibits calcium-mediated smooth muscle constriction, decreases acetylcholine release in the neuromuscular junction, and affects respiratory muscle force generation.
Intravenous Magnesium sulfate has therefore been a useful adjunct in patients with acute status asthmaticus refractory to beta agonists 41. The benefit does not seem to isolate patients with low serum magnesium levels although 50% of patients with acute asthma tend to present with hypomagnesemia. In spite of its widespread use in Emergency department setting, 2 large prospective studies failed to demonstrate any statistically significant improvement in lung function in severe asthma exacerbation. However, it is relatively cheap and harmless and has been proposed to have a trend towards female responsiveness, as estrogen potentiates bronchodilator effects of magnesium. At the commonly used dose of 2 gm intravenously (IV) in 2 separate doses over 20 minutes, side effects of hypotension or hyporeflexia are fairly uncommon.
Heliox and Oxygen
True shunt in acute asthma averages only 1.5% of pulmonary blood flow. Therefore, oxygen supplementation need in status asthmaticus is infrequent and low dose. Refractory hypoxemia in status asthmaticus should trigger a search for complications like pneumonia, atelectasis or barotrauma. Heliox as a mixture of 70:30 or 60:40 helium:oxygen decreases airway resistance and turbulence, and therefore reduces work of breathing and inspiratory muscle fatigue. There is a demonstrated reduction in pulsus paradoxus and enhancement in peak flow. However, its routine use is hindered by the prohibitive cost, infrequent indication and need for recalibration of gas blenders and flow meters when used with mechanical ventilation 42.
Antibiotics
Graham et al. conducted a randomized double-blinded trial and demonstrated no difference in improvement in symptom score, spirometry or length of hospitalization with routine use of antibiotics in status asthmaticus. That does not mean that patients with clinical signs of infection should not be treated with antimicrobials or due diligence should not be pursued in obtaining respiratory culture specimens early on 43.
Mechanical Ventilation and Sedation
The decision to intubate a patient presenting with status asthmaticus is a clinical one and does not unequivocally require a blood gas assessment 44.
Immediate indications for intubation include:
- Acute cardiopulmonary arrest
- Severe obtundation or coma
- Frank evidence of respiratory fatigue with gasping or inability to speak at all
If a patient continues to deteriorate in spite of initial pharmacologic treatment, a bedside assessment around the time window of response needs to be made.
Clinical findings that tilt a decision in favor include:
- Increasing lethargy
- Increasing use of accessory muscles
- Change in posture or speech
- Decreasing rate and depth of respiration
In patients who are not significantly encephalopathic, and has no excessive secretions, noninvasive ventilation with CPAP or BIPAP can be a useful modality to support ventilation, and avoid the need for anesthesia and sedation, as well as the risk of nosocomial infection with endotracheal intubation. It is increasingly being used in the first 24 hours, at pressure support titrated to reduce respiratory rate below 25 per minute and generate tidal volume above 7 ml/kg body weight. Beyond that, there might be an increased risk of aspiration, facial pressure necrosis and suboptimal ventilation to reconsider invasive mechanical ventilation 45.
Once a decision to intubate is made, choice of sedation agent is of paramount importance.
Ketamine
Ketamine has sedative, analgesic, anesthetic and bronchodilatory properties and has been increasingly recommended for emergency intubation in status asthmaticus along with succinylcholine. The usual dose is 1 to 2 mg/kg given intravenously at a rate of 0.5 mg/kg per minute to provide 10 to 15 minutes of general anesthesia without significant respiratory depression (as opposed to bolus doses).
Potential risks to consider before deciding in favor of ketamine include:
- Ability to cause hypertension and tachycardia with sympathetic stimulation. Thus it is to be avoided in patients with uncontrolled hypertension, preeclampsia, raised intracranial pressure.
- Lowering of seizure threshold
- Increase in laryngeal secretion
- Metabolism through liver thus causing some accumulation with the continuous infusion in liver failure
Propofol
Propofol is an equally preferred initial agent due to its rapid onset of action and east titratability, ability to achieve deep sedation without paralytics and mild bronchodilatory effects. However prolonged propofol administration in this subset of patients raises the risk of increased carbon dioxide (CO2) production, as it is constituted in a fat-based diluent.
Thus for ongoing sedation needs, lorazepam is preferred with caution to minimize sedation to a level to maintain ventilator synchrony and allow response to stimulation.
Paralytics
For patients who continue to remain desynchronized with the ventilator in spite of sedation, and has a risk of generating auto-PEEP or barotrauma, paralytics may need to be considered. Atracurium is the agent of choice because of the lower risk of myopathy although it can cause bronchoconstriction due to histamine release. Vecuronium is an alternative in such circumstances 46.
Status asthmaticus prognosis
Poor prognostic factors:
- Leatherman et al. 47 found an incidence of muscle weakness in asthmatic patients treated with neuromuscular blockers and steroids of 29%.
- Adnet et al. 14 evaluated complications and morbidities associated with a prolonged neuromuscular blockade in status asthmaticus patients. The incidence of post-intubation myopathy, ventilator-associated pneumonia, and duration of ICU stay was higher in the neuromuscular blockade group in the population involving 5 centers.
- A study by Afessa et al. 6 also reported a higher incidence of acidemia and carbon dioxide retention in nonsurvivors compared to survivors with acute asthmaticus.
- Need for mechanical ventilation has also been reported as a poor prognostic factor 48.
Preventing Future Attacks
Beyond the period of recovery from an acute episode of status asthmaticus, the management goal should shift to an interprofessional team approach to help prevent future severe attacks. It should start with extensive patient education from nurses, respiratory therapists, nurse practitioners, physician assistants, and physicians about the pathophysiology of asthma, warning signs and symptoms, elimination and avoidance of triggers, and early identification and treatment of attacks. Inpatient education by respiratory therapists or nursing team about asthma action plan, tools of self-assessment of severity with peak flowmetry, the appropriate technique of inhaler use, and relevant numbers to call for specialist help. Maintenance inhaler therapy should be appropriately addressed along with assessment for the need for advanced immunotherapy based on asthma phenotype and allergy profile 49.
Patients should be well-versed in detecting early warning signs at home and be well equipped to detect and address, based on the asthma action plan.
A 20% drop in PEFR below predicted, or personal best is a good objective indicator.
Finally, patients with a history of anaphylaxis or sudden asphyxic asthma presentation should also be equipped with Epipen for immediate subcutaneous use if needed.
- Korang SK, Feinberg J, Wetterslev J, Jakobsen JC. Non-invasive positive pressure ventilation for acute asthma in children. Cochrane Database Syst Rev. 2016 Sep 30;9(9):CD012067. doi: 10.1002/14651858.CD012067.pub2[↩]
- Basnet S, Mander G, Andoh J, Klaska H, Verhulst S, Koirala J. Safety, efficacy, and tolerability of early initiation of noninvasive positive pressure ventilation in pediatric patients admitted with status asthmaticus: a pilot study. Pediatr Crit Care Med. 2012 Jul;13(4):393-8. doi: 10.1097/PCC.0b013e318238b07a[↩]
- Chakraborty RK, Basnet S. Status Asthmaticus. [Updated 2022 Oct 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526070[↩][↩][↩][↩]
- Braman SS, Kaemmerlen JT. Intensive care of status asthmaticus. A 10-year experience. JAMA. 1990 Jul 18;264(3):366-8.[↩]
- [Status asthmaticus]. Pol Merkur Lekarski. 2005 May;18(107):599-603. https://www.ncbi.nlm.nih.gov/pubmed/16161965[↩]
- Afessa B, Morales I, Cury JD. Clinical course and outcome of patients admitted to an ICU for status asthmaticus. Chest. 2001 Nov;120(5):1616-21[↩][↩]
- Peters JI, Stupka JE, Singh H, Rossrucker J, Angel LF, Melo J, Levine SM. Status asthmaticus in the medical intensive care unit: a 30-year experience. Respir Med. 2012 Mar;106(3):344-8[↩]
- Papiris S, Kotanidou A, Malagari K, Roussos C. Clinical review: severe asthma. Crit Care. 2002 Feb;6(1):30-44[↩]
- Lamblin C, Gosset P, Tillie-Leblond I, Saulnier F, Marquette CH, Wallaert B, Tonnel AB. Bronchial neutrophilia in patients with noninfectious status asthmaticus. Am. J. Respir. Crit. Care Med. 1998 Feb;157(2):394-402[↩]
- Sur S, Crotty TB, Kephart GM, Hyma BA, Colby TV, Reed CE, Hunt LW, Gleich GJ. Sudden-onset fatal asthma. A distinct entity with few eosinophils and relatively more neutrophils in the airway submucosa? Am Rev Respir Dis. 1993 Sep;148(3):713-9. doi: 10.1164/ajrccm/148.3.713[↩]
- McFadden ER Jr. Acute severe asthma. Am J Respir Crit Care Med. 2003 Oct 1;168(7):740-59. doi: 10.1164/rccm.200208-902SO[↩]
- Brenner BE, Abraham E, Simon RR. Position and diaphoresis in acute asthma. Am J Med. 1983 Jun;74(6):1005-9. doi: 10.1016/0002-9343(83)90802-1[↩]
- McFadden ER. Acute severe asthma. Am. J. Respir. Crit. Care Med. 2003 Oct 01;168(7):740-59[↩]
- Mountain RD, Sahn SA. Clinical features and outcome in patients with acute asthma presenting with hypercapnia. Am. Rev. Respir. Dis. 1988 Sep;138(3):535-9[↩][↩][↩]
- Magadle R, Berar-Yanay N, Weiner P. The risk of hospitalization and near-fatal and fatal asthma in relation to the perception of dyspnea. Chest. 2002 Feb. 121 (2):329-33.[↩]
- [Guideline] Dinakar C, Oppenheimer J, Portnoy J, et al. Management of acute loss of asthma control in the yellow zone: a practice parameter. Ann Allergy Asthma Immunol. 2014 Aug. 113 (2):143-59.[↩]
- Tuxen DV. Detrimental effects of positive end-expiratory pressure during controlled mechanical ventilation of patients with severe airflow obstruction. Am. Rev. Respir. Dis. 1989 Jul;140(1):5-9[↩]
- Grossman J. The occurrence of arrhythmias in hospitalized asthmatic patients. J. Allergy Clin. Immunol. 1976 Apr;57(4):310-7[↩]
- Corbridge TC, Hall JB. The assessment and management of adults with status asthmaticus. Am. J. Respir. Crit. Care Med. 1995 May;151(5):1296-316[↩]
- Knowles GK, Clark TJ. Pulsus paradoxus as a valuable sign indicating severity of asthma. Lancet. 1973 Dec 15;2(7842):1356-9[↩]
- Paniagua N, Elosegi A, Duo I, Fernandez A, Mojica E, Martinez-Indart L, Mintegi S, Benito J. Initial Asthma Severity Assessment Tools as Predictors of Hospitalization. J Emerg Med. 2017 Jul;53(1):10-17[↩]
- Rebuck AS, Read J. Assessment and management of severe asthma. Am. J. Med. 1971 Dec;51(6):788-98[↩]
- Gunen H, Hacievliyagil SS, Kosar F, Gulbas G, Kizkin O, Sahin I. The role of arterial blood gases, exercise testing, and cardiac examination in asthma. Allergy Asthma Proc. 2006 Jan-Feb;27(1):45-52[↩]
- Rodriguez-Roisin R. Acute severe asthma: pathophysiology and pathobiology of gas exchange abnormalities. Eur. Respir. J. 1997 Jun;10(6):1359-71[↩]
- Asthma: diagnosis, monitoring and chronic asthma management. https://www.nice.org.uk/guidance/indevelopment/gid-ng10186/documents[↩]
- Asthma: diagnosis, monitoring and chronic asthma management. https://www.nice.org.uk/guidance/ng80[↩]
- Rehder KJ. Adjunct therapies for refractory status asthmaticus in children. Respir Care. 2017;62:849–865. doi: 10.4187/respcare.05174[↩]
- Travers AH, Milan SJ, Jones AP, Camargo CA Jr, Rowe BH. Addition of intravenous beta(2)-agonists to inhaled beta(2)-agonists for acute asthma. Cochrane Database Syst Rev. 2012 Dec 12;12:CD010179. doi: 10.1002/14651858.CD010179[↩]
- Boulton DW, Fawcett JP. Enantioselective disposition of salbutamol in man following oral and intravenous administration. Br J Clin Pharmacol. 1996;41:35–40. doi: 10.1111/j.1365-2125.1996.tb00156.x[↩]
- Maier G, Rubino C, Hsu R, Grasela T, Baumgartner RA. Population pharmacokinetics of (R)-albuterol and (S)-albuterol in pediatric patients aged 4-11 years with asthma. Pulm Pharmacol Ther. 2007;20:534–542. doi: 10.1016/j.pupt.2006.05.003[↩]
- Boulton DW, Fawcett JP. The pharmacokinetics of levosalbutamol: what are the clinical implications? Clin Pharmacokinet. 2001;40:23–40. doi: 10.2165/00003088-200140010-00003[↩]
- Status Asthmaticus Guidelines. https://emedicine.medscape.com/article/2129484-guidelines[↩]
- Miller AG, Breslin ME, Pineda LC, Fox JW. An Asthma Protocol Improved Adherence to Evidence-Based Guidelines for Pediatric Subjects With Status Asthmaticus in the Emergency Department. Respir Care. 2015 Dec. 60 (12):1759-64[↩]
- Serrano-Pariente J, Rodrigo G, Fiz JA, Crespo A, Plaza V., High Risk Asthma Research Group. Identification and characterization of near-fatal asthma phenotypes by cluster analysis. Allergy. 2015 Sep;70(9):1139-47[↩]
- National Asthma Education and Prevention Program. Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma-Summary Report 2007. J. Allergy Clin. Immunol. 2007 Nov;120(5 Suppl):S94-138[↩]
- Frei SP. Cost comparison of bronchodilator delivery methods in Emergency Department treatment of asthma. J Emerg Med. 2000 Nov;19(4):323-6.[↩]
- Papiris S, Kotanidou A, Malagari K, Roussos C. Clinical review: severe asthma. Crit Care. 2002 Feb;6(1):30-44.[↩]
- Inhaled beta 2-adrenergic agonists in asthma. The Executive Committee of the American Academy of Allergy and Immunology. J. Allergy Clin. Immunol. 1993 Jun;91(6):1234-7.[↩]
- Edmonds ML, Milan SJ, Camargo CA, Pollack CV, Rowe BH. Early use of inhaled corticosteroids in the emergency department treatment of acute asthma. Cochrane Database Syst Rev. 2012 Dec 12;12:CD002308[↩]
- Edmonds ML, Milan SJ, Camargo CA, Pollack CV, Rowe BH. Early use of inhaled corticosteroids in the emergency department treatment of acute asthma. Cochrane Database Syst Rev. 2012 Dec 12;12:CD002308 [↩]
- Griffiths B, Kew KM, Normansell R. Intravenous magnesium sulfate for treating children with acute asthma in the emergency department. Paediatr Respir Rev. 2016 Sep;20:45-47[↩]
- Tobias JD, Garrett JS. Therapeutic options for severe, refractory status asthmaticus: inhalational anaesthetic agents, extracorporeal membrane oxygenation and helium/oxygen ventilation. Paediatr Anaesth. 1997;7(1):47-57[↩]
- Johnston SL, Szigeti M, Cross M, Brightling C, Chaudhuri R, Harrison T, Mansur A, Robison L, Sattar Z, Jackson D, Mallia P, Wong E, Corrigan C, Higgins B, Ind P, Singh D, Thomson NC, Ashby D, Chauhan A., AZALEA Trial Team. Azithromycin for Acute Exacerbations of Asthma : The AZALEA Randomized Clinical Trial. JAMA Intern Med. 2016 Nov 01;176(11):1630-1637[↩]
- Siddiqui S, Gonem S, Wardlaw AJ. Advances in the management of severe asthma. Semin Respir Crit Care Med. 2012 Dec;33(6):666-84[↩]
- Hess DR. Noninvasive ventilation for acute respiratory failure. Respir Care. 2013 Jun;58(6):950-72[↩]
- Goh AY, Chan PW. Acute myopathy after status asthmaticus: steroids, myorelaxants or carbon dioxide? Respirology. 1999 Mar;4(1):97-9[↩]
- Leatherman JW, Fluegel WL, David WS, Davies SF, Iber C. Muscle weakness in mechanically ventilated patients with severe asthma. Am J Respir Crit Care Med. 1996 May;153(5):1686-90. doi: 10.1164/ajrccm.153.5.8630621[↩]
- Williams TJ, Tuxen DV, Scheinkestel CD, Czarny D, Bowes G. Risk factors for morbidity in mechanically ventilated patients with acute severe asthma. Am. Rev. Respir. Dis. 1992 Sep;146(3):607-15[↩]
- Al-Muhsen S, Horanieh N, Dulgom S, Aseri ZA, Vazquez-Tello A, Halwani R, Al-Jahdali H. Poor asthma education and medication compliance are associated with increased emergency department visits by asthmatic children. Ann Thorac Med. 2015 Apr-Jun;10(2):123-31.[↩]





{kind=link}