
Contents
- What is tenesmus
- Tenesmus causes
- Tenesmus symptoms
- Tenesmus diagnosis
- Tenesmus treatment
- Rectal tenesmus
- Tenesmus IBS
- Vesical tenesmus
What is tenesmus
Tenesmus is the feeling that you need to pass stools, even though your bowels are already empty. Tenesmus may involve straining, pain, and cramping. Tenesmus most often occurs with inflammatory diseases of the bowels. These diseases may be caused by an infection or other conditions.
Tenesmus can also occur with diseases that affect the normal movements of the intestines. These diseases are known as motility disorders.
People with tenesmus may push very hard (strain) to try to empty their bowels. However, they will only pass a small amount of stool.
Tenesmus treatment home remedy
Increasing the amount of fiber and fluid in your diet can help ease constipation.
See your health care provider if you continue to have symptoms of tenesmus that are constant or come and go.
Also see your doctor if you have:
- Abdominal pain
- Blood in the stool
- Chills
- Fever
- Nausea
- Vomiting
These symptoms could be a sign of a disease that might be causing the problem.
Tenesmus causes
Tenesmus may be caused by:
- Anorectal abscess
- Proctitis
- Colorectal cancer or tumors
- Crohn disease
- Infection of the colon (infectious colitis)
- Inflammation of the colon or rectum from radiation (radiation proctitis or colitis)
- Inflammatory bowel disease (IBD)
- Movement (motility) disorder of the intestines
- Ulcerative colitis
- Rectal prolapse
Tenesmus symptoms
Tenesmus is the feeling that you need to pass stools, even though your bowels are already empty. Tenesmus may involve straining, pain, and cramping.
Tenesmus diagnosis
Your doctor will examine you and ask questions such as:
- When did this problem occur? Have you had it before?
- What symptoms are you having?
- Have you eaten any raw, new, or unfamiliar foods? Have you eaten at a picnic or large gathering?
- Do any others in your household have similar problems?
- What other health problems do you have or have had in the past?
The physical exam may include a detailed abdominal exam. A rectal exam is performed in most cases.
Tests that may be done include:
- Colonoscopy to look at the colon and rectum
- Complete blood count (CBC)
- CT scan of the abdomen (in rare cases)
- Proctosigmoidoscopy (an examination of the lower bowel)
- Stool cultures
- X-rays of the abdomen
Tenesmus treatment
Overall, management should be focused on the primary cause of tenesmus and not on tenesmus itself.
Rectal tenesmus
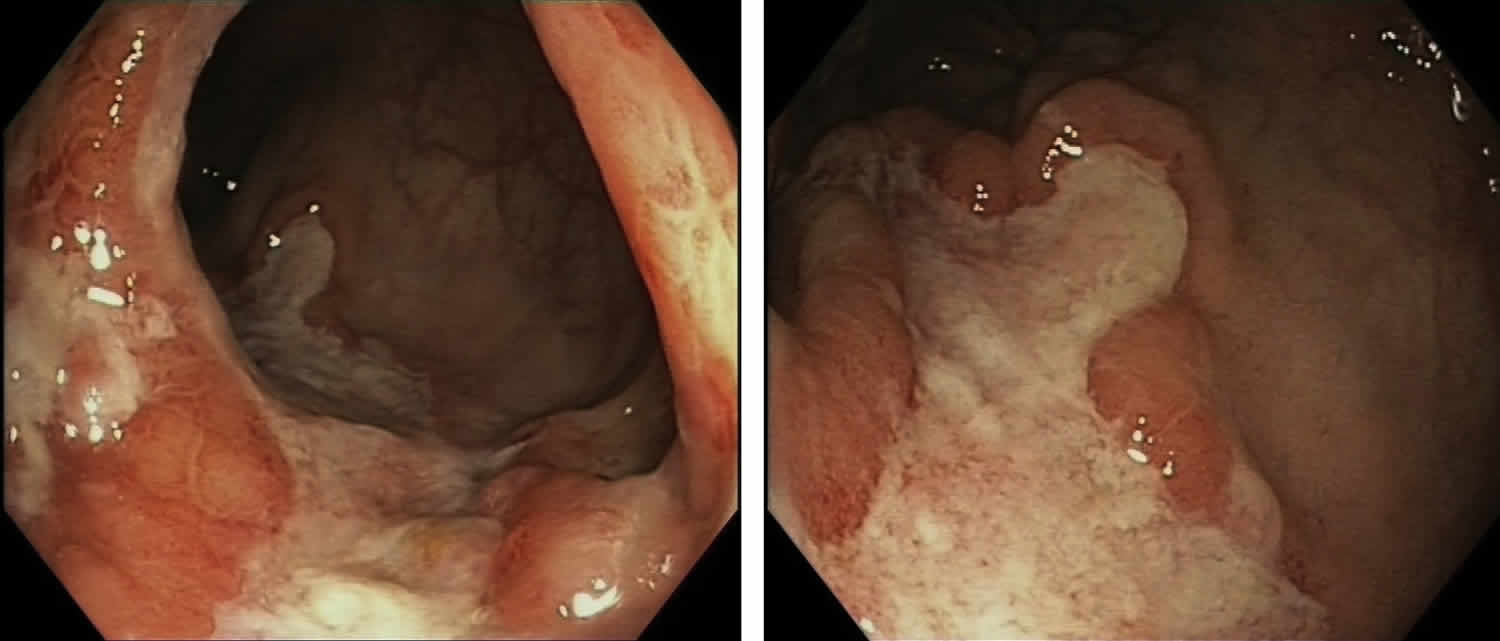
Proctitis is inflammation of the lining of the rectum. The rectum is a muscular tube that’s connected to the end of your colon. Stool passes through the rectum on its way out of the body. Proctitis can cause rectal pain, diarrhea, bleeding and mucus discharge, as well as the continuous feeling that you need to have a bowel movement (tenesmus). Proctitis symptoms can be short-lived, or they can become chronic.
Proctitis is common in people who have inflammatory bowel disease (Crohn’s disease or ulcerative colitis). Sexually transmitted infections or sexually transmitted diseases (STDs) are another frequent cause. Sexually transmitted diseases (STDs) are the most common cause of proctitis in men who have sex with men. Neisseria gonorrhoeae and Chlamydia trachomatis, followed by Treponema pallidum and herpes simplex virus, are most frequently found 1. Symptoms are usually nonspecific and include rectal discharge, bleeding and tenesmus. Ulcers are found in approximately 50% of symptomatic patients, most of them internal and external 2.
Proctitis also can also be a side effect of radiation therapy for certain cancers.
Make an appointment with your doctor if you have any signs or symptoms of proctitis.
Figure 1. Proctitis
Proctitis causes
Several diseases and conditions can cause inflammation of the rectal lining. They include:
- Inflammatory bowel disease. About 30 percent of people with inflammatory bowel disease (Crohn’s disease or ulcerative colitis) have inflammation of the rectum.
- Autoimmune disease
- Harmful substances
- Non-sexually transmitted infection. Infections associated with foodborne illness, such as salmonella, shigella and campylobacter infections, also can cause proctitis.
- Sexually transmitted disease (STD). Sexually transmitted infections, spread particularly by people who engage in anal intercourse, can result in proctitis. Sexually transmitted infections that can cause proctitis include gonorrhea, genital herpes and chlamydia.
- Radiation therapy for cancer. Radiation therapy directed at your rectum or nearby areas, such as the prostate, can cause rectal inflammation. Radiation proctitis can begin during radiation treatment and last for a few months after treatment. Or it can occur years after treatment.
- Antibiotics. Sometimes antibiotics used to treat an infection can kill helpful bacteria in the bowels, allowing the harmful Clostridium difficile bacteria to grow in the rectum.
- Diversion proctitis. Proctitis can occur in people following some types of colon surgery in which the passage of stool is diverted from the rectum to a surgically created opening (stoma).
- Food protein-induced proctitis. This can occur in infants who drink either cow’s milk- or soy-based formula. Infants breast-fed by mothers who eat dairy products also may develop proctitis.
- Eosinophilic proctitis. This condition occurs when a type of white blood cell (eosinophil) builds up in the lining of the rectum. Eosinophilic proctitis affects only children younger than 2.
Proctitis caused by STD is common in people who have anal intercourse. Sexually transmitted diseases (STDs) that can cause proctitis include gonorrhea, herpes, chlamydia, and lymphogranuloma venereum.
Infections that are not sexually transmitted are less common than STD proctitis. One type of proctitis not from an STD is an infection in children that is caused by the same bacteria as strep throat.
Autoimmune proctitis is linked to diseases such as ulcerative colitis or Crohn disease. If the inflammation is in the rectum only, it may come and go or move upward into the large intestine.
Proctitis may also be caused by some medicines, radiotherapy or inserting harmful substances into the rectum.
Risk factors for proctitis
Risk factors for proctitis include:
- Unsafe sex and high-risk sexual practices, such as anal sex. Practices that increase your risk of a sexually transmitted infection (STI) can increase your risk of proctitis. Your risk of contracting an STI increases if you have multiple sex partners, don’t use condoms and have sex with a partner who has an STI.
- Inflammatory bowel diseases. Having an inflammatory bowel disease (Crohn’s disease or ulcerative colitis ) increases your risk of proctitis.
- Radiation therapy for cancer. Radiation therapy directed at or near your rectum (such as for rectal, ovarian or prostate cancer) increases your risk of proctitis.
Proctitis prevention
To reduce your risk of proctitis, take steps to protect yourself from sexually transmitted infections (STIs). The surest way to prevent an STI is to abstain from sex, especially anal sex. If you choose to have sex, reduce your risk of an sexually transmitted infection (STI) by:
- Limiting your number of sex partners
- Using a latex condom during each sexual contact
- Not having sex with anyone who has any unusual sores or discharge in the genital area
If you’re diagnosed with a sexually transmitted infection, stop having sex until after you’ve completed treatment. Ask your doctor when it’s safe to have sex again.
Proctitis symptoms
Proctitis signs and symptoms may include:
- A frequent or continuous feeling that you need to have a bowel movement (tenesmus)
- Rectal bleeding
- Passing mucus through your rectum
- Rectal pain
- Pain on the left side of your abdomen
- A feeling of fullness in your rectum
- Diarrhea
- Pain with bowel movements
Proctitis complications
Proctitis that isn’t treated or that doesn’t respond to treatment may lead to complications, including:
- Anemia. Chronic bleeding from your rectum can cause anemia. With anemia, you don’t have enough red blood cells to carry adequate oxygen to your tissues. Anemia causes you to feel tired, and you may also experience dizziness, shortness of breath, headache, pale skin and irritability.
- Ulcers. Chronic inflammation in the rectum can lead to open sores (ulcers) on the inside lining of the rectum.
- Severe bleeding.
- Rectal abscess.
- Anal Fistulas. Sometimes ulcers extend completely through the intestinal wall, creating a fistula, an abnormal connection that can occur between different parts of your intestine, between your intestine and skin, or between your intestine and other organs, such as the bladder and vagina.
- Recto-vaginal fistula (women)
Proctitis diagnosis
Tests and procedures used to diagnose proctitis include:
- Blood tests. These can detect blood loss or infections.
- Stool test. You may be asked to collect a stool sample for testing. A stool test may help determine if your proctitis is caused by a bacterial infection.
- Scope exam of the last portion of your colon. During this test (flexible sigmoidoscopy), your doctor uses a slender, flexible, lighted tube to examine the last part of your colon (sigmoid), as well as the rectum. During the procedure, your doctor can also take small samples of tissue (biopsy) for laboratory analysis.
- Scope exam of your entire colon. This test (colonoscopy) allows your doctor to view your entire colon using a thin, flexible, lighted tube with an attached camera. Your doctor can also take a biopsy during this test.
- Tests for sexually transmitted infections. These tests involve obtaining a sample of discharge from your rectum or from the tube that drains urine from your bladder (urethra).
- In case a STD is suspected, Gram stains of rectal exudates and microbiological tests for the previously mentioned infections should be taken 3. Rectal swabs are the optimum specimens, although rectal biopsies might also be used. Samples should be placed into closed containers or viral transport medium. Samples deemed for NAAT should be managed according to the manufacturer’s recommendation 4.
Proctitis treatment
Treatment for proctitis depends on the underlying cause of the inflammation.
Treatment for proctitis caused by an infection
Your doctor may recommend medications to treat your infection. Options may include:
- Antibiotics. For proctitis caused by bacterial infections, your doctor may recommend an antibiotic, such as doxycycline (Doxteric, Vibramycin).
- Antivirals. For proctitis caused by viral infections, such as the sexually transmitted virus herpes, your doctor may prescribe an antiviral medication, such as acyclovir (Sitavig, Zovirax, others).
Treatment for proctitis caused by radiation therapy
Mild cases of radiation proctitis may not require treatment. In other cases, radiation proctitis can cause severe pain and bleeding that requires treatment. Your doctor may recommend treatments such as:
- Medications. Medications are given in pill, suppository or enema form. They include sucralfate (Carafate), mesalamine (Asacol HD, Canasa, others), sulfasalazine (Azulfidine) and metronidazole (Flagyl). These medications can help control inflammation and reduce bleeding.
- Stool softeners and dilation. These can help open up obstructions in the bowel.
- Treatment to destroy damaged tissue. These techniques improve proctitis symptoms by destroying abnormal tissue (ablation) that is bleeding. Ablation procedures used to treat proctitis include argon plasma coagulation (APC), electrocoagulation and other therapies.
Proctitis caused by inflammatory bowel disease
Treatment of proctitis related to Crohn’s disease or ulcerative colitis is aimed at reducing the inflammation in your rectum. Treatment may include:
- Medications to control rectal inflammation. Your doctor may prescribe anti-inflammatory medications, either by mouth or as a suppository or enema, such as mesalamine (Asacol HD, Canasa, others) — or corticosteroids — such as prednisone (Rayos) or budesonide (Entocort EC, Uceris). Inflammation in people with Crohn’s disease often requires treatment with a medication that suppresses the immune system, such as azathioprine (Azasan, Imuran) or infliximab (Remicade).
- Surgery. If drug therapy doesn’t relieve your signs and symptoms, your doctor may recommend surgery to remove a damaged portion of your digestive tract.
Tenesmus IBS
Irritable bowel syndrome (IBS) is a common disorder that affects the large intestine. Signs and symptoms of IBS include cramping, abdominal pain, bloating, gas, and diarrhea or constipation, or both. Some people with irritable bowel syndrome (IBS) have constipation. Some have diarrhea. Others go back and forth between the two. Although IBS can cause a great deal of discomfort, it does not harm the intestines. IBS is a chronic condition that you’ll need to manage long term.
Only a small number of people with IBS have severe signs and symptoms. Some people can control their symptoms by managing diet, lifestyle and stress. More-severe symptoms can be treated with medication and counseling.
IBS (irritable bowel syndrome) doesn’t cause changes in bowel tissue or increase your risk of colorectal cancer.
Studies suggest that about 12 percent of people in the United States have IBS 5. IBS (irritable bowel syndrome) affects about twice as many women as men and is most often found in people younger than 45 years. No one knows the exact cause of IBS. There is no specific test for it. Your doctor may run tests to be sure you don’t have other diseases. These tests may include stool sampling tests, blood tests, and x-rays. Your doctor may also do a test called a sigmoidoscopy or colonoscopy. Most people diagnosed with IBS can control their symptoms with diet, stress management, probiotics, and medicine.
Other health problems do people with IBS may have
People with IBS often have other health problems, including1
- certain conditions that involve chronic pain, such as fibromyalgia , chronic fatigue syndrome and chronic pelvic pain
- certain digestive diseases, such as dyspepsia and gastroesophageal reflux disease
- certain mental disorders, such as anxiety , depression , and somatic symptom disorder
See your doctor if you have a persistent change in bowel habits or other signs or symptoms of IBS. They may indicate a more serious condition, such as colon cancer. More-serious signs and symptoms include:
- Weight loss
- Diarrhea at night
- Rectal bleeding
- Iron deficiency anemia
- Unexplained vomiting
- Difficulty swallowing
- Persistent pain that isn’t relieved by passing gas or a bowel movement
Who is more likely to develop IBS?
Women are up to two times more likely than men to develop IBS 5. People younger than age 50 are more likely to develop IBS than people older than age 50 6.
Factors that can increase your chance of having IBS include:
- having a family member with IBS
- a history of stressful or difficult life events, such as abuse, in childhood
- having a severe infection in your digestive tract
Types of IBS
Three types of IBS are based on different patterns of changes in your bowel movements or abnormal bowel movements. Sometimes, it is important for your doctor to know which type of IBS you have. Some medicines work only for some types of IBS or make other types worse. Your doctor might diagnose IBS even if your bowel movement pattern does not fit one particular type.
Many people with IBS have normal bowel movements on some days and abnormal bowel movements on other days.
IBS with constipation (IBS-C)
With IBS-C, on days when you have at least one abnormal bowel movement
- more than a quarter of your stools are hard or lumpy and
- less than a quarter of your stools are loose or watery
IBS with diarrhea (IBS-D)
In IBS-D, on days when you have at least one abnormal bowel movement
- more than a quarter of your stools are loose or watery and
- less than a quarter of your stools are hard or lumpy
IBS with mixed bowel habits (IBS-M)
In IBS-M, on days when you have at least one abnormal bowel movement
- more than a quarter of your stools are hard or lumpy and
- more than a quarter of your stools are loose or watery
Causes of IBS
The precise cause of IBS isn’t known. IBS is a functional gastrointestinal (GI) disorder. Functional gastrointestinal disorders, which doctors now call disorders of gut-brain interactions, are related to problems with how your brain and your gut work together. These problems can cause your gut to be more sensitive and change how the muscles in your bowel contract. If your gut is more sensitive, you may feel more abdominal pain and bloating. Changes in how the muscles in your bowel contract lead to diarrhea, constipation, or both.
Factors that appear to play a role include:
- Stressful or difficult early life events, such as physical or sexual abuse
- Certain mental disorders, such as depression, anxiety , and somatic symptom disorder
- Muscle contractions in the intestine. The walls of the intestines are lined with layers of muscle that contract as they move food through your digestive tract. Contractions that are stronger and last longer than normal can cause gas, bloating and diarrhea. Weak intestinal contractions can slow food passage and lead to hard, dry stools.
- Nervous system. Abnormalities in the nerves in your digestive system may cause you to experience greater than normal discomfort when your abdomen stretches from gas or stool. Poorly coordinated signals between the brain and the intestines can cause your body to overreact to changes that normally occur in the digestive process, resulting in pain, diarrhea or constipation.
- Inflammation in the intestines. Some people with IBS have an increased number of immune-system cells in their intestines. This immune-system response is associated with pain and diarrhea.
- Severe infection. IBS can develop after a severe bout of diarrhea (gastroenteritis) caused by bacteria or a virus. IBS might also be associated with a surplus of bacteria in the intestines (bacterial overgrowth). Small intestinal bacterial overgrowth, an increase in the number or a change in the type of bacteria in your small intestine
- Changes in bacteria in the gut (microflora). Microflora are the “good” bacteria that reside in the intestines and play a key role in health. Research indicates that microflora in people with IBS might differ from microflora in healthy people.
- Food intolerances or sensitivities, in which certain foods cause digestive symptoms.
Research suggests that genes may make some people more likely to develop IBS.
Triggers of IBS
Symptoms of IBS can be triggered by:
- Food. The role of food allergy or intolerance in IBS isn’t fully understood. A true food allergy rarely causes IBS. But many people have worse IBS symptoms when they eat or drink certain foods or beverages, including wheat, dairy products, citrus fruits, beans, cabbage, milk and carbonated drinks.
- Stress. Most people with IBS experience worse or more frequent signs and symptoms during periods of increased stress. But while stress may aggravate symptoms, it doesn’t cause them.
- Hormones. Women are twice as likely to have IBS, which might indicate that hormonal changes play a role. Many women find that signs and symptoms are worse during or around their menstrual periods.
Risk factors for IBS
Many people have occasional signs and symptoms of IBS. But you’re more likely to have the syndrome if you:
- Are young. IBS occurs more frequently in people under age 50.
- Are female. In the United States, IBS is more common among women. Estrogen therapy before or after menopause also is a risk factor for IBS.
- Have a family history of IBS. Genes may play a role, as may shared factors in a family’s environment or a combination of genes and environment.
- Have a mental health problem. Anxiety, depression and other mental health issues are associated with IBS. A history of sexual, physical or emotional abuse also might be a risk factor.
IBS prevention
Finding ways to deal with stress may help prevent or ease symptoms of IBS. Consider trying:
- Counseling. A counselor can help you learn to modify or change your responses to stress. Studies have shown that psychotherapy can provide significant and long-lasting reduction of symptoms.
- Biofeedback. Electrical sensors help you receive information (feedback) on your body’s functions. The feedback helps you focus on making subtle changes, such as relaxing certain muscles, to ease symptoms.
- Progressive relaxation exercises. These exercises help you relax muscles in your body, one by one. Start by tightening the muscles in your feet, then concentrate on slowly letting all of the tension go. Next, tighten and relax your calves. Continue until the muscles in your body, including those in your eyes and scalp, are relaxed.
- Mindfulness training. This stress-reduction technique helps you focus on being in the moment and letting go of worries and distractions.
IBS symptoms
The signs and symptoms of IBS vary. The most common include:
- Abdominal pain, cramping or bloating that is typically relieved or partially relieved by passing a bowel movement
- Excess gas
- Diarrhea or constipation — sometimes alternating bouts of diarrhea and constipation
- Mucus in the stool
Most people with IBS experience times when the signs and symptoms are worse and times when they improve or even disappear completely.
IBS complications
Chronic constipation or diarrhea can cause hemorrhoids.
In addition, IBS is associated with:
- Poor quality of life. Many people with moderate to severe IBS report poor quality of life. Research indicates that people with IBS miss three times as many days from work as do those without bowel symptoms.
- Mood disorders. Experiencing the signs and symptoms of IBS can lead to depression or anxiety. Depression and anxiety also can make IBS worse.
How is IBS diagnosed
There’s no test to definitively diagnose IBS. Your doctor is likely to start with a complete medical history, physical exam and tests to rule out other conditions. If you have IBS with diarrhea, you likely will be tested for gluten intolerance (celiac disease).
After other conditions have been ruled out, your doctor is likely to use one of these sets of diagnostic criteria for IBS:
- Rome criteria. These criteria include abdominal pain and discomfort lasting on average at least one day a week in the last three months, associated with at least two of these factors: Pain and discomfort are related to defecation, the frequency of defecation is altered, or stool consistency is altered.
- Manning criteria. These criteria focus on pain relieved by passing stool and on having incomplete bowel movements, mucus in the stool and changes in stool consistency. The more symptoms you have, the greater the likelihood of IBS.
- Type of IBS. For the purpose of treatment, IBS can be divided into three types, based on your symptoms: constipation-predominant, diarrhea-predominant or mixed.
Your doctor will also likely assess whether you have other signs or symptoms that might suggest another, more serious, condition. These signs and symptoms include:
- Onset of signs and symptoms after age 50
- Weight loss
- Rectal bleeding
- Fever
- Nausea or recurrent vomiting
- Abdominal pain, especially if it’s not completely relieved by a bowel movement, or occurs at night
- Diarrhea that is persistent or awakens you from sleep
- Anemia related to low iron
If you have these signs or symptoms, or if an initial treatment for IBS doesn’t work, you’ll likely need additional tests.
Additional tests
Your doctor may recommend several tests, including stool studies to check for infection or problems with your intestine’s ability to take in the nutrients from food (malabsorption). You may also have a number of other tests to rule out other causes for your symptoms.
Imaging tests can include:
- Flexible sigmoidoscopy. Your doctor examines the lower part of the colon (sigmoid) with a flexible, lighted tube (sigmoidoscope).
- Colonoscopy. Your doctor uses a small, flexible tube to examine the entire length of the colon.
- X-ray or CT scan. These tests produce images of your abdomen and pelvis that might allow your doctor to rule out other causes of your symptoms, especially if you have abdominal pain. Your doctor might fill your large intestine with a liquid (barium) to make any problems more visible on X-ray. This barium test is sometimes called a lower GI series.
Laboratory tests can include:
- Lactose intolerance tests. Lactase is an enzyme you need to digest the sugar found in dairy products. If you don’t produce lactase, you may have problems similar to those caused by IBS, including abdominal pain, gas and diarrhea. Your doctor may order a breath test or ask you to remove milk and milk products from your diet for several weeks.
- Breath test for bacterial overgrowth. A breath test also can determine if you have bacterial overgrowth in your small intestine. Bacterial overgrowth is more common among people who have had bowel surgery or who have diabetes or some other disease that slows down digestion.
- Upper endoscopy. A long, flexible tube is inserted down your throat and into the tube connecting your mouth and stomach (esophagus). A camera on the end of the tube allows the doctor to inspect your upper digestive tract and obtain a tissue sample (biopsy) from your small intestine and fluid to look for overgrowth of bacteria. Your doctor might recommend endoscopy if celiac disease is suspected.
- Stool tests. Your stool might be examined for bacteria or parasites, or a digestive liquid produced in your liver (bile acid), if you have chronic diarrhea.
IBS treatment
Treatment of IBS focuses on relieving symptoms so that you can live as normally as possible.
Diet and lifestyle
Mild signs and symptoms can often be controlled by managing stress and by making changes in your diet and lifestyle. Try to:
- Avoid foods that trigger your symptoms
- Eat high-fiber foods
- Drink plenty of fluids
- Exercise regularly
- Get enough sleep
Fiber may improve constipation in IBS because it makes stool soft and easier to pass.
Two types of fiber are:
- Soluble fiber, which is found in beans, fruit, and oat products
- Insoluble fiber, which is found in whole-grain products and vegetables
Research suggests that soluble fiber is more helpful in relieving IBS symptoms. To help your body get used to more fiber, add foods with fiber to your diet a little at a time. Too much fiber at once can cause gas, which can trigger IBS symptoms. Adding fiber to your diet slowly, by 2 to 3 grams a day, may help prevent gas and bloating.
Your doctor might suggest that you eliminate from your diet:
- High-gas foods. If you experience bloating or gas, you might avoid items such as carbonated and alcoholic beverages, caffeine, raw fruit, and certain vegetables, such as cabbage, broccoli and cauliflower.
- Gluten. Research shows that some people with IBS report improvement in diarrhea symptoms if they stop eating gluten (wheat, barley and rye) even if they don’t have celiac disease.
- FODMAPs. Some people are sensitive to certain carbohydrates such as fructose, fructans, lactose and others, known as FODMAPs — fermentable oligo-, di-, and monosaccharides and polyols. FODMAPs are found in certain grains, vegetables, fruits and dairy products. Your IBS symptoms might ease if you follow a strict low-FODMAP diet and then reintroduce foods one at a time. Examples of foods that contain FODMAPs include:
- fruits such as apples, apricots, blackberries, cherries, mango, nectarines, pears, plums, and watermelon, or juice containing any of these fruits
- canned fruit in natural fruit juice, or large amounts of fruit juice or dried fruit
- vegetables such as artichokes, asparagus, beans, cabbage, cauliflower, garlic and garlic salts, lentils, mushrooms, onions, and sugar snap or snow peas
- dairy products such as milk, milk products, soft cheeses, yogurt, custard, and ice cream
- wheat and rye products
- honey and foods with high-fructose corn syrup
- products, including candy and gum, with sweeteners ending in “–ol,” such as sorbitol, mannitol, xylitol, and maltitol
Your doctor may suggest that you try the low FODMAP diet for a few weeks to see if it helps with your symptoms. If your symptoms improve, your doctor may recommend slowly adding foods that contain FODMAPs back into your diet. You may be able to eat some foods with FODMAPs without having IBS symptoms.
A dietitian can help you with these diet changes.
If your problems are moderate or severe, your doctor might suggest counseling — especially if you have depression or if stress tends to worsen your symptoms.
Medications
In addition, based on your symptoms your doctor might suggest medications such as:
- Fiber supplements. Taking a supplement such as psyllium (Metamucil) with fluids may help control constipation.
- Laxatives. If fiber doesn’t help symptoms, your doctor may prescribe magnesium hydroxide oral (Phillips’ Milk of Magnesia) or polyethylene glycol (Miralax).
- Anti-diarrheal medications. Over-the-counter medications, such as loperamide (Imodium), can help control diarrhea. Your doctor might also prescribe a bile acid binder, such as cholestyramine (Prevalite), colestipol (Colestid) or colesevelam (Welchol). Bile acid binders can cause bloating.
- Anticholinergic medications. Medications such as dicyclomine (Bentyl) can help relieve painful bowel spasms. They are sometimes prescribed for people who have bouts of diarrhea. These medications are generally safe but can cause constipation, dry mouth and blurred vision.
- Tricyclic antidepressants. This type of medication can help relieve depression as well as inhibit the activity of neurons that control the intestines to help reduce pain. If you have diarrhea and abdominal pain without depression, your doctor may suggest a lower than normal dose of imipramine (Tofranil), desipramine (Norpramine) or nortriptyline (Pamelor). Side effects — which might be reduced if you take the medication at bedtime — can include drowsiness, blurred vision, dizziness and dry mouth.
- Selective serotonin reuptake inhibitor (SSRI) antidepressants. Selective serotonin reuptake inhibitor (SSRI) antidepressants, such as fluoxetine (Prozac, Sarafem) or paroxetine (Paxil), may help if you’re depressed and have pain and constipation.
- Pain medications. Pregabalin (Lyrica) or gabapentin (Neurontin) might ease severe pain or bloating.
Other medicines may help treat pain in your abdomen, including:
- antispasmodics
- antidepressants , such as low doses of tricyclic antidepressants and selective serotonin reuptake inhibitors
- coated peppermint oil capsules
Follow your doctor’s instructions when you use medicine to treat IBS. Talk with your doctor about possible side effects and what to do if you have them.
Probiotics
Your doctor may also recommend probiotics. Probiotics are live microorganisms , most often bacteria, that are similar to microorganisms you normally have in your digestive tract. Researchers are still studying the use of probiotics to treat IBS.
To be safe, talk with your doctor before using probiotics or any other complementary or alternative medicines or practices. If your doctor recommends probiotics, talk with him or her about how much probiotics you should take and for how long.
Medications specifically for IBS
Medications approved for certain people with IBS include:
- Alosetron (Lotronex). Alosetron is designed to relax the colon and slow the movement of waste through the lower bowel. Alosetron can be prescribed only by doctors enrolled in a special program, is intended for severe cases of diarrhea-predominant IBS in women who haven’t responded to other treatments, and isn’t approved for use by men. It has been linked to rare but important side effects, so it should only be considered when other treatments aren’t successful.
- Eluxadoline (Viberzi). Eluxadoline can ease diarrhea by reducing muscle contractions and fluid secretion in the intestine, and increasing muscle tone in the rectum. Side effects can include nausea, abdominal pain and mild constipation. Eluxadoline has also been associated with pancreatitis, which can be serious and more common in certain individuals.
- Rifaximin (Xifaxan). This antibiotic can decrease bacterial overgrowth and diarrhea.
- Lubiprostone (Amitiza). Lubiprostone can increase fluid secretion in your small intestine to help with the passage of stool. It’s approved for women who have IBS with constipation, and is generally prescribed only for women with severe symptoms that haven’t responded to other treatments.
- Linaclotide (Linzess). Linaclotide also can increase fluid secretion in your small intestine to help you pass stool. Linaclotide can cause diarrhea, but taking the medication 30 to 60 minutes before eating might help.
Mental health therapies
Your doctor may recommend mental health therapies to help improve your IBS symptoms. Therapies used to treat IBS include
- Cognitive behavioral therapy (CBT), which focuses on helping you change thought and behavior patterns to improve IBS symptoms
- Gut-directed hypnotherapy, in which a therapist uses hypnosis—a trance-like state in which you are relaxed or focused—to help improve your IBS symptoms
- Relaxation training, which can help you relax your muscles or reduce stress
Potential future treatments
Researchers are investigating new treatments for IBS. Serum-derived bovine immunoglobulin/protein isolate (SBI), a nutritional therapy, has shown some promise as a treatment for IBS with diarrhea.
Studies also show that, in people who have IBS with diarrhea, a specially coated tablet that slowly releases peppermint oil in the small intestine (enteric-coated peppermint oil) eases bloating, urgency, abdominal pain and pain while passing stool. It isn’t clear how enteric-coated peppermint oil might affect IBS, so ask your doctor before using it.
Vesical tenesmus
Vesical tenesmus is more commonly known as an overactive bladder syndrome, which is a condition in which your urinary bladder squeezes urine out at the wrong time. Vesical tenesmus is characterized by a sudden urge to urinate, urinary frequency and nocturia (excessive urination at night time disrupting sleep), with or without urge urinary incontinence 7. The urge may be difficult to stop, and overactive bladder may lead to the involuntary loss of urine (urge incontinence) 8.
You may have vesical tenesmus (overactive bladder) if you have two or more of these symptoms:
- You urinate eight or more times a day or two or more times at night
- You have the sudden, strong need to urinate immediately
- You leak urine after a sudden, strong urge to urinate
You also may have urinary incontinence, a loss of bladder control. Nerve problems, too much fluid, or too much caffeine can cause it. Often the cause is unknown.
Vesical tenesmus (overactive bladder) can have a significant effect on your quality of life, you may feel embarrassed, isolate yourself, or limit your work and social life. The good news is that a brief evaluation can determine whether there’s a specific cause for your overactive bladder symptoms.
Overactive bladder syndrome affects 12–17% of the population. Prevalence increases with age. The management of overactive bladder syndrome involves exclusion of underlying pathology. First line treatment includes lifestyle interventions, pelvic floor exercises, bladder training and antimuscarinic agents. Failure of conservative management necessitates second line therapies, which are more invasive and include botulinum toxin, neuromodulation or surgical interventions such as augmentation cystoplasty or urinary diversion.
Management of overactive bladder often begins with behavioral strategies, such as fluid schedules, timed voiding and bladder-holding techniques using your pelvic floor. If these initial efforts don’t help enough with your overactive bladder symptoms, medications are available.
Your doctor may prescribe a medicine that can calm muscles and nerves. The medicine may come as a pill, a liquid, or a patch. The medicines can cause your eyes to become dry. They can also cause dry mouth and constipation. To deal with these effects, use eye drops to keep your eyes moist, chew sugarless gum or suck on sugarless hard candy if dry mouth bothers you, and take small sips of water throughout the day.
What causes vesical tenesmus
Normal bladder function
The urinary bladder is a hollow, collapsible muscular sac that stores and expels urine situated in the pelvic cavity posterior to the pubic symphysis. When slightly distended due to the accumulation of urine, the urinary bladder is spherical. When it is empty, it collapses. As urine volume increases, it becomes pear shaped and rises into the abdominal cavity.
Urinary bladder capacity averages 700–800 mL. It is smaller in females because the uterus occupies the space just superior to the urinary bladder.
For the urinary system to do its job, muscles and nerves must work together to hold urine in the bladder and then release it at the right time. Nerves carry messages from the bladder to the brain to let it know when the bladder is full. They also carry messages from the brain to the bladder, telling muscles either to tighten or release. A nerve problem might affect your bladder control if the nerves that are supposed to carry messages between the brain and the bladder do not work properly.
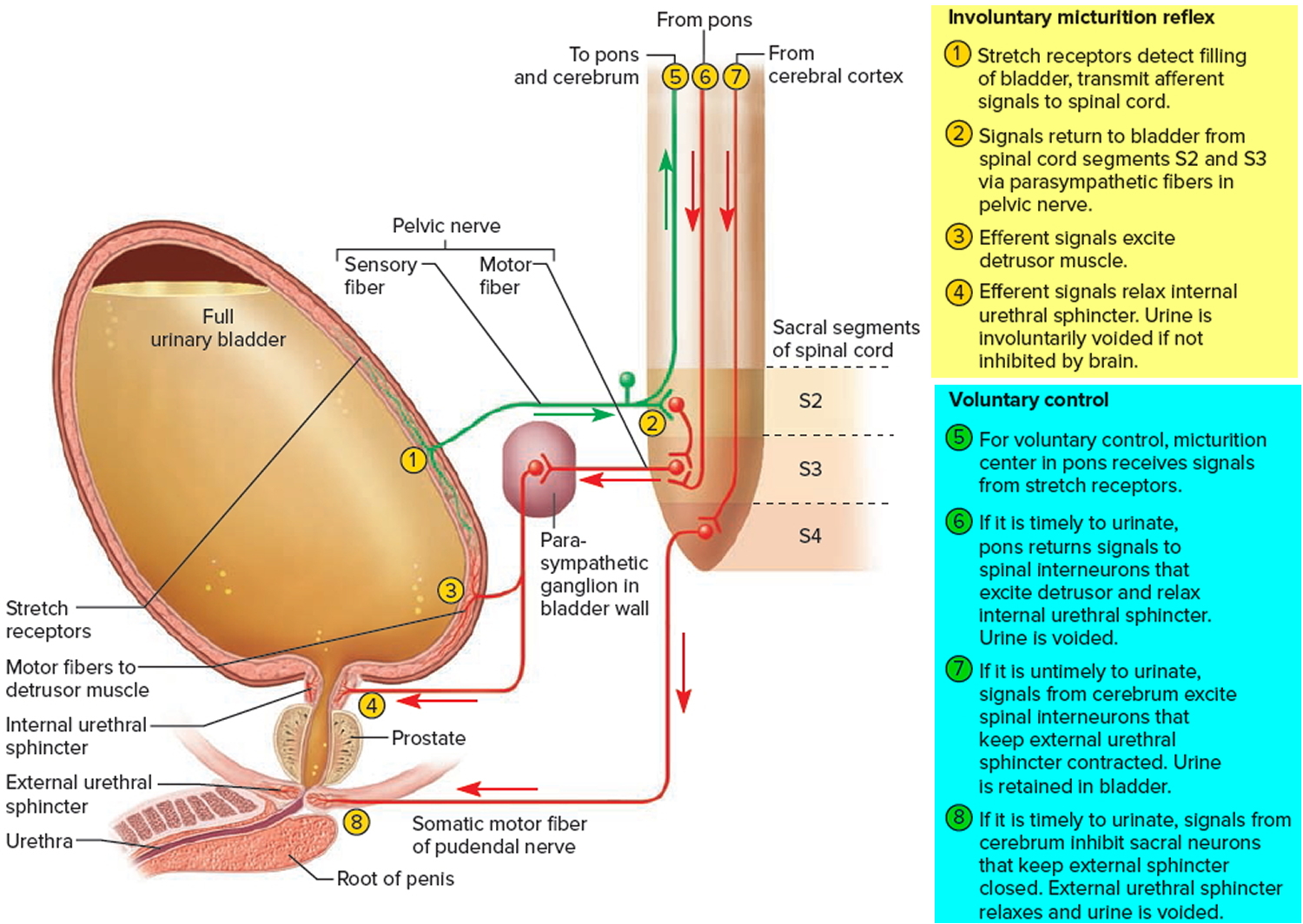
Discharge of urine from the urinary bladder, called micturition, is also known as urination or voiding. Micturition occurs via a combination of involuntary and voluntary muscle contractions. When the volume of urine in the urinary bladder exceeds 200–400 mL, pressure within the bladder increases considerably, and stretch receptors in its wall transmit nerve impulses into the spinal cord. These impulses propagate to the micturition center in sacral spinal cord segments S2 and S3 and trigger a spinal reflex called the micturition reflex. In this reflex arc, parasympathetic impulses from the micturition center propagate to the urinary bladder wall and internal urethral sphincter.
The nerve impulses cause contraction of the detrusor muscle and relaxation of the internal urethral sphincter muscle. Simultaneously, the micturition center inhibits somatic motor neurons that innervate skeletal muscle in the external urethral sphincter. On contraction of the urinary bladder wall and relaxation of the sphincters, urination takes place. Urinary bladder filling causes a sensation of fullness that initiates a conscious desire to urinate before the micturition reflex actually occurs. Although emptying of the urinary bladder is a reflex, in early childhood we learn to initiate it and stop it voluntarily.
Human bladder contraction is mediated mainly through stimulation of muscarinic receptors in the detrusor muscle by acetylcholine 9. Antimuscarinic agents act during the filling/storage phase of the micturition cycle by inhibiting afferent (sensory) input from the bladder, and directly inhibiting smooth muscle contractility 10. They are competitive antagonists, so with massive release of acetylcholine during micturition the drug effect is decreased and the muscle can contract 11.
Through learned control of the external urethral sphincter muscle and certain muscles of the pelvic floor, the cerebral cortex can initiate micturition or delay its occurrence for a limited period.
Figure 2. Bladder control
Involuntary bladder contractions
Overactive bladder occurs because the muscles of the bladder start to contract involuntarily even when the volume of urine in your bladder is low. This involuntary contraction creates the urgent need to urinate.
Overactive bladder symptoms are usually associated with involuntary contractions of the detrusor (bladder) muscle, which can result in urge incontinence, depending on the response of the sphincter 12. The most common cause of overactive bladder symptoms is detrusor overactivity 9; 64% of all patients with overactive bladder symptoms have detrusor overactivity on cystometry, and 69% of men and 44% of women with urgency have detrusor overactivity 13. Detrusor overactivity is thought to result not only from efferent (motor) hyper function/dysfunction but also most likely by afferent (sensory) noise. Patients with overactive bladder symptoms seem to respond to antimuscarinic treatment irrespective of the presence of detrusor overactivity 14.
Several conditions may contribute to signs and symptoms of vesical tenesmus, including:
- Neurological disorders, such as stroke and multiple sclerosis
- Diabetes
- Medications that cause a rapid increase in urine production or require that you take them with lots of fluids
- Acute urinary tract infections that can cause symptoms similar to an overactive bladder
- Abnormalities in the bladder, such as tumors or bladder stones
- Factors that obstruct bladder outflow — enlarged prostate, constipation or previous operations to treat other forms of incontinence
- Excess consumption of caffeine or alcohol
- Declining cognitive function due to aging, which may make it more difficult for your bladder to understand the signals it receives from your brain
- Difficulty walking, which can lead to bladder urgency if you’re unable to get to the bathroom quickly
- Incomplete bladder emptying, which may lead to symptoms of overactive bladder, as you have little urine storage space left
The specific cause of an overactive bladder may be unknown.
Risk factors for vesical tenesmus
As you age, you’re at increased risk of developing overactive bladder. You’re also at higher risk of diseases and disorders, such as enlarged prostate and diabetes, which can contribute to other problems with bladder function.
Many people with cognitive decline — for instance, after a stroke or with Alzheimer’s disease — develop an overactive bladder. Incontinence that results from situations like this can be managed with fluid schedules, timed and prompted voiding, absorbent garments, and bowel programs.
Other risk factors include: vaginal birth delivery 15, with 40% of parous women experiencing urge urinary incontinence, older age, obesity and chronic constipation 16. Childhood urinary symptoms in women have been found to be independently associated with adult lower urinary tract symptoms, specifically urgency, frequency and nocturia 17.
Some people with an overactive bladder also have bowel control problems; tell your doctor if this is a problem for you.
Complications of vesical tenesmus
Any type of incontinence can affect your overall quality of life. If your overactive bladder symptoms cause a major disruption to your life, you might also have:
- Emotional distress or depression
- Anxiety
- Sleep disturbances and interrupted sleep cycles
- Issues with sexuality
Your doctor might recommend treatment of associated conditions, to see if effective treatment of an associated condition will help with your urinary symptoms.
Some women also may have a disorder called mixed incontinence, when both urge and stress incontinence occur. Stress incontinence is the loss of urine when you exert physical stress or pressure on your bladder, such as during activities that include running or jumping. Treatment of the stress incontinence is not likely to help the overactive bladder symptoms.
Older people may have a common combination of bladder storage problems and bladder-emptying issues. The bladder may cause a lot of urgency and even incontinence, but it doesn’t empty well. A specialist may be able to help you with this combination of bladder problems.
Prevention of vesical tenesmus
These healthy lifestyle choices may reduce your risk of overactive bladder:
- Maintain a healthy weight.
- Get regular, daily physical activity and exercise.
- Limit consumption of caffeine and alcohol.
- Quit smoking.
- Manage chronic conditions, such as diabetes, that might contribute to overactive bladder symptoms.
- Learn where your pelvic floor muscles are and then strengthen them by doing Kegel exercises — tighten (contract) muscles, hold the contraction for two seconds and relax muscles for three seconds. Work up to holding the contraction for five seconds and then 10 seconds at a time. Do three sets of 10 repetitions each day.
Diagnosis of vesical tenesmus
If you have an abnormal urge to urinate, your doctor will check to make sure that you don’t have an infection or blood in your urine. Your doctor may also want to make sure that you’re emptying your bladder completely when you urinate.
Your doctor will look for clues that might also indicate contributing factors. The work-up will likely include a:
- Medical history
- Physical exam, focusing on your abdomen and genitals
- Urine sample to test for infection, traces of blood or other abnormalities
- Focused neurological exam that may identify sensory problems or abnormal reflexes
Special tests
Your doctor may order a simple urodynamic test to assess the function of your bladder and its ability to empty steadily and completely. These tests usually require a referral to a specialist, and may not be necessary to make a diagnosis or begin treatment. Tests include:
- Measuring urine left in the bladder. This test is important if your bladder doesn’t empty completely when you urinate or experience urinary incontinence. Remaining urine (postvoid residual urine) may cause symptoms identical to an overactive bladder. To measure residual urine after you have voided, your doctor may request an ultrasound scan of your bladder or pass a thin tube (catheter) through the urethra and into your bladder to drain and measure the remaining urine.
- Measuring urine flow rate. To measure the volume and speed of your voiding, you may be asked to urinate into a uroflowmeter. This device translates the data into a graph of changes in your flow rate.
- Testing bladder pressures. Cystometry measures pressure in your bladder and in the surrounding region during bladder filling. During this test, your doctor uses a thin tube (catheter) to fill your bladder slowly with warm water. Another catheter with a pressure-measuring sensor is placed in your rectum or, if you’re a woman, in your vagina.This procedure can identify whether you have involuntary muscle contractions or a stiff bladder that’s not able to store urine under low pressure.
Your doctor will review the results of any tests with you and suggest a treatment strategy.
Treatment of vesical tenesmus
A combination of treatment strategies may be the best approach to relieve overactive bladder symptoms.
Behavioral interventions
Behavioral interventions are the first choice in helping manage an overactive bladder. They’re often effective, and they carry no side effects.
Behavioral treatments have been shown to be effective in older adults, reducing leakage by 50–80% 18. Behavioral training requires a highly motivated patient, and 20–30% will become dry. As behavioral treatments work gradually at first and rely on patient self management.
Behavioral interventions may include:
Pelvic floor muscle exercises
Kegel exercises strengthen your pelvic floor muscles and urinary sphincter. These strengthened muscles can help you stop the bladder’s involuntary contractions.
Your doctor or a physical therapist can help you learn how to do Kegel exercises correctly. It may take as long as six to eight weeks before you notice a difference in your symptoms.
What are Kegel exercises ?
To do Kegel exercises, you just squeeze your pelvic floor muscles. The part of your body including your hip bones is the pelvic area. At the bottom of the pelvis, several layers of muscle stretch between your legs. The muscles attach to the front, back, and sides of the pelvic bone.
Kegel exercises are designed to make your pelvic floor muscles stronger. These are the muscles that hold up your bladder and help keep it from leaking.
Building up your pelvic muscles with Kegel exercises can help with your bladder control.
How do you exercise your pelvic muscles ?
Find the right muscles. Try one of the following ways to find the right muscles to squeeze.
- Imagine that you are trying to stop passing gas. Squeeze the muscles you would use. If you sense a “pulling” feeling, you are squeezing the right muscles for pelvic exercises.
- Imagine that you are sitting on a marble and want to pick up the marble with your vagina. Imagine “sucking” the marble into your vagina.
- For Women: If you still are not sure you are tightening the right muscles – lie down and put your finger inside your vagina. Squeeze as if you were trying to stop urine from coming out. If you feel tightness on your finger, you are squeezing the right pelvic muscles.
- For Men: Insert a finger into your rectum. Tighten the muscles as if you are holding in your urine, then let go. You should feel the muscles tighten and move up and down.
Once you know what the movement feels like, do Kegel exercises three times a day:
- Make sure your bladder is empty, then sit or lie down.
- Tighten the pelvic floor muscles. Hold tight and count to 6 to 8.
- Relax the muscles and count to 10.
- Repeat 10 times, three times a day (morning, afternoon, and night).
At first, find a quiet spot to practice—your bathroom or bedroom—so you can concentrate. Lie on the floor. Pull in the pelvic muscles and hold for a count of 6 to 8. Then relax for a count of 10. Work up to 10 to 15 repeats each time you exercise.
Do your pelvic exercises at least three times a day. Every day, use three positions: lying down, sitting, and standing. You can exercise while lying on the floor, sitting at a desk, or standing in the kitchen. Using all three positions makes the muscles strongest.
Breathe deeply, and relax your body when you are doing these exercises. Make sure you are not tightening your stomach, thigh, buttock, or chest muscles.
After 4 to 6 weeks, you should feel better and have fewer symptoms. Keep doing the exercises, but do not increase how many you do. Overdoing it can lead to straining when you urinate or move your bowels.
Some notes of caution:
- Once you learn how to do them, do not practice Kegel exercises at the same time you are urinating more than twice a month. Doing the exercises while you are urinating can weaken your pelvic floor muscles over time.
- In women, doing Kegel exercises incorrectly or with too much force may cause vaginal muscles to tighten too much. This can cause pain during sexual intercourse.
- Incontinence will return if you stop doing these exercises. Once you start doing them, you may need to do them for the rest of your life.
It may take several months for your incontinence to lessen once you start doing these exercises.
Let your doctor, nurse, or therapist help you. Many people have trouble finding the right muscles. Your doctor, nurse, or therapist can check to make sure you are doing the exercises correctly. You can also exercise by using special weights or biofeedback. Ask your health care team about these exercise aids.
Don’t squeeze other muscles at the same time. Be careful not to tighten your stomach, legs, or other muscles. Squeezing the wrong muscles can put more pressure on your bladder control muscles. Just squeeze the pelvic muscle. Don’t hold your breath.
Be patient. Don’t give up. It’s just 5 minutes, three times a day. You may not feel your bladder control improve until after 3 to 6 weeks. Still, most women do notice an improvement after a few weeks.
Method
Pelvic floor muscle training with or without biofeedback. Mastering a voluntary contraction of the pelvic floor muscles will help to increase pressure within the urethra, inhibit detrusor contractions and control leakage of urine. Coaching and verbal feedback during vaginal examination can be as effective as biofeedback and electrical stimulation
- An initial approach is by verbal explanation of the technique reinforced with written materials
- An effective verbal explanation of proper contraction of the pelvic floor muscles is to tell the patient to tighten up the muscles that they use to hold in flatus.
- These muscles can also be identified during a pelvic or digital rectal examination
- An effective exercise prescription for older adults is to contract and relax their pelvic floor muscles for 2 seconds with 15 repetitions, three times per day. Patients should gradually increase the duration of squeeze/relaxations by about 1 second per week, until they achieve 10 second contractions and relaxations. At this point they can begin a maintenance prescription of 10 second contractions and relaxations with 10 repetitions once a day
- Freeze and squeeze:
- when a sense of urgency occurs, instead of rushing to the bathroom, stay still and repeatedly tighten the pelvic floor muscles without relaxing them until the urgency is gone. Walk to the bathroom at a normal pace
- Repeat as needed.
+ A maintenance program is essential to maintain strength and effectiveness
+ At least 3 months of supervised pelvic floor muscle training is required to see benefits
+ Continence management is often best guided by a continence trained professional (eg. nurse or physiotherapist).
Bladder training
| Goal To modify bladder function, reduce voiding frequency, increase bladder capacity and eliminate detrusor overactivity by using scheduled voiding rather than voiding in response to urgency |
Method
|
| A minimum of 6 weeks training is required to see benefits |
Altering fluid intake – decreasing to reduce incontinence and frequency, increasing to improve urine concentration
Smoking cessation
Dietary modification to eliminate possible bladder irritants (eg. reducing caffeine, alcohol and carbonated beverages). Caffeine is a mild diuretic and bladder irritant, and reducing intake can reduce both urge and stress incontinence
Regulating bowel function to avoid constipation and straining during bowel movements
Healthy weight. If you’re overweight, losing weight may ease symptoms central obesity places pressure on the bladder and may worsen urge incontinence 18. Weight loss may help if you also have stress urinary incontinence.
Scheduled toilet trips. Setting a schedule for toileting — for example, every two to four hours — gets you on track to urinate at the same times every day rather than waiting until you feel the urge to urinate.
Intermittent catheterization. Using a catheter periodically to empty your bladder completely helps your bladder do what it can’t do by itself. Ask your doctor if this approach is right for you.
Absorbent pads. Wearing absorbent pads or undergarments can protect your clothing and help you avoid embarrassing incidents, which means that you won’t have to limit your activities. Absorbent garments come in a variety of sizes and absorbency levels.
Bladder training. Bladder training involves training yourself to delay voiding when you feel an urge to urinate. You begin with small delays, such as 30 minutes, and gradually work your way up to urinating every three to four hours. Bladder training is possible only if you’re able to tighten (contract) your pelvic floor muscles successfully.
Medications
Medications that relax the bladder can be helpful for relieving symptoms of overactive bladder and reducing episodes of urge incontinence. These drugs include:
- Tolterodine (Detrol, Detrol LA)
- Oxybutynin (Ditropan XL)
- Oxybutynin as a skin patch (Oxytrol)
- Oxybutynin gel (Gelnique, Gelnique 3%)
- Trospium (Sanctura)
- Solifenacin (Vesicare)
- Darifenacin (Enablex)
- Mirabegron (Myrbetriq)
- Fesoterodine (Toviaz)
Common side effects of most of these drugs include dry eyes and dry mouth, but drinking water to quench thirst can aggravate symptoms of overactive bladder. Constipation — another potential side effect — can aggravate your bladder symptoms. Extended-release forms of these medications, including the skin patch or gel, may cause fewer side effects.
Side Effects in the elderly
Cognitive dysfunction including memory loss and attention deficits are particular side effects in the elderly 19.
Antimuscarinic medications differ in their propensity to cause central nervous system adverse events due to differences in lipophilicity and crossing of the blood-brain barrier. Oxybutinin may be the most likely to cross the blood-brain barrier 14.
The use of anticholinergics should be carefully weighed against the potential cognitive risks in the older adult population 10, as long term exposure to anticholinergics may be associated with increased Alzheimer type pathology 20.
The newer antimuscarinics for overactive bladder – darifenacin, solifenacin and tolterodine – have a significantly reduced impact on cognitition compared with traditional agents. Similarly, oxybutinin transdermal gel does not seem to adversely affect cognition 21. Despite this, their use in the elderly may still contribute to cognitive impairment and appropriate monitoring is recommended.
Prescribing in the elderly
Oxybutinin can be started at 2.5 mg twice per day. The morning dose can be increased or a lunchtime dose added depending on severity and timing of symptoms. The maximum dose is 5 mg three times per day 22. High doses are often not well tolerated due to dry mouth, gritty eyes, exacerbation of gastrointestinal reflux and constipation.
Nonantimuscarinic medications
Duloxetine (a serotonin noradrenaline reuptake inhibitor) can be effective in both stress and mixed stress and urge incontinence 23. In clinical practice, most women discontinue duloxetine within 4 weeks due to adverse effects (Table 1).
Failure of conservative and medical treatments warrants urology referral for further investigation with urodynamics, and more invasive therapies may be considered.
Your doctor may recommend that you suck on a piece of sugar-free candy or chew sugar-free gum to relieve dry mouth, and use eyedrops to keep your eyes moist. Over-the-counter preparations, such as Biotene products, can be helpful for long-term dry mouth. To avoid constipation, your doctor might recommend a fiber-rich diet or use of stool softeners.
Table 1. Medications proven to be effective for overactive bladder syndrome
| Drug | Adverse effects | Notes |
|---|---|---|
| Oxybutynin CR 5–15 mg/day |
| Dose response observed Take 1 hour before food |
| Oxybutynin transdermal 3.9 mg twice weekly |
| Transdermal delivery reduces the typical anticholinergic side effects of dry mouth and constipation |
| Tolterodine 2 mg twice per day |
| Dose dependent effect with immediate release Safe in men with bladder outlet obstruction Expensive, not subsidised on the PBS3,2 |
| Solifenacin 5–10 mg/day |
| Steady state at 10 days due to long half-life |
| Darifenacin 7.5–15 mg/day |
| Steady state 4–5 hours Dose response Safety, efficacy and tolerability maintained with long term use Not subsidised on the PBS |
| Vaginal oestrogen (topical) 0.5 g cream nightly for 2 weeks then twice per week |
| For postmenopausal women with vaginal atrophy Contraindications: past history of breast cancer |
| Duloxetine 40 mg twice per day increasing to 60 mg twice per day after 4 weeks (for stress urinary incontinence) |
| Efficacy for stress and mixed stress and urge incontinence Can be used if anticholinergics are contraindicated for overactive bladder syndrome33 TGA indicated and PBS subsidised in Australia for major depressive disorder |
Bladder injections (Second line therapy)
OnabotulinumtoxinA, also called Botox, is a protein from the bacteria that cause botulism illness. The technique is to place multiple injections under cystoscopic guidance directly into the detrusor. Used in small doses directly injected into bladder tissues, prevents acetylcholine release at the neuromuscular junction, resulting in temporary chemo-denervation and muscle relaxation (protein partially paralyzes muscles) for up to 6 months 24.
Complete continence can be achieved in 40–80% of patients and bladder capacity improved by 56% for up to 6 months 25. Maximal benefit is between 2 and 6 weeks, maintained over 6 months. The injections can be repeated 26.
About half of people had side effects from these injections, including 9 percent who had urinary retention. So, if you’re considering Botox treatments, you should be willing and able to catheterize yourself if urinary retention occurs.
Nerve stimulation (Third line therapy)
Regulating the nerve impulses to your bladder can improve overactive bladder symptoms.
One procedure uses a thin wire placed close to the sacral nerves — which carry signals to your bladder — where they pass near your tailbone.
This surgical procedure is often done with a trial of a temporary wire or as an advanced procedure in which the permanent electrode is implanted and a longer trial is performed prior to a surgical placement of the battery-powered pulse generator. Your doctor then uses a device connected to the wire to deliver electrical impulses to your bladder, similar to what a pacemaker does for the heart.
If this successfully reduces your symptoms, the wire is eventually connected to a small battery device that’s placed under your skin.
Surgery
Surgery to treat overactive bladder is reserved for people with severe symptoms who don’t respond to other treatments. The goal is to improve the bladder’s ability to store urine and reduce pressure in the bladder. However, these procedures won’t help relieve bladder pain. Interventions include:
- Surgery to increase bladder capacity. This procedure uses pieces of your bowel to replace a portion of your bladder. This surgery is used only in cases of severe urge incontinence that doesn’t respond to any other, more-conservative treatment measures. If you have this surgery, you may need to use a catheter intermittently for the rest of your life to empty your bladder.
- Bladder removal. This procedure is used as a last resort and involves removing the bladder and surgically constructing a replacement bladder (neobladder) or an opening in the body (stoma) to attach a bag on the skin to collect urine.
- Ask Before Shooting. García-Alonso, Francisco Javier et al. Gastroenterology , Volume 149 , Issue 7 , e7 – e8. https://www.gastrojournal.org/article/S0016-5085(15)00636-8/fulltext[↩]
- Davis, T.W. and Goldstone, S.E. Sexually transmitted infections as a cause of proctitis in men who have sex with men. Dis Colon Rectum. 2009; 52: 507–512[↩]
- de Vries, H.J., Zingoni, A., White, J.A. et al. 2013 European Guideline on the management of proctitis, proctocolitis and enteritis caused by sexually transmissible pathogens. Int J STD AIDS. 2013; 25: 465–474[↩]
- Baron, E.J., Miller, J.M., Weinstein, M.P. et al. A guide to utilization of the microbiology laboratory for diagnosis of infectious diseases: 2013 recommendations by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM)(a). Clin Infect Dis. 2013; 57: e22–e121[↩]
- Chey WD, Kurlander J, Eswaran S. Irritable bowel syndrome: a clinical review. Journal of the American Medical Association. 2015;313(9):949–958.[↩][↩]
- Lacy BE, Mearin F, Chang L, et al. Bowel disorders. Gastroenterology. 2016;150(6):1393–1407.[↩]
- Overactive bladder syndrome. Royal Australian College of General Practitioners. https://www.racgp.org.au/afp/2012/november/overactive-bladder-syndrome/[↩]
- Overactive bladder. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/overactive-bladder/symptoms-causes/syc-20355715[↩]
- Ballert K, Biggs G, Nitti V. Antimuscarinic agents. AUA update series 2008;27:137–47.[↩][↩]
- Saks EK, Arya LA. Pharmacologic management of urinary incontinence, voiding dysfunction, and overactive bladder. Obstet Gynecol Clin North Am 2009;36:493–507.[↩][↩]
- Andersson K-E. Antimuscarinics for treatment of overactive bladder. Lancet Neurol 2004;3:46–53.[↩]
- Chapple C, Gormley EA. Developments in pharmacological therapy for the overactive bladder. BJU Int 2006;98(1 Suppl):78–87.[↩]
- Abrams P, Andersson KE. Muscarinic receptor antagonists for overactive bladder. BJU Int 2007;100:987–1006.[↩]
- Chapple CR, Khullar V, Gabriel Z, Muston D, Bitoun CE, Weinstein D. The effects of antimuscarinic treatments in overactive bladder: an update of a systematic review and meta-analysis. Eur Urol 2008;54:543–62.[↩][↩]
- Lukacz ES, Lawrence JM, Contreras R, Nager CW, Luber KM. Parity, mode of delivery, and pelvic floor disorders. Obstet Gynaecol 2006;107:1253–60.[↩]
- Gamble TL, Du H, Sand PK, Botros SM, Rurak M, Goldberg RP. Urge incontinence: estimating environmental and obstetric risk factors using an identical twin study. Int Urogynecol J 2010;21:939–46.[↩]
- Fitzgerald MP, Thom DH, Wassel-Fyr C, et al. Childhood urinary symptoms predict adult overactive bladder symptoms. J Urol 2006;175:989–93.[↩]
- Markland AD, Vaughan CP, Johnson TM 2nd, Burgio KL, Goode PS. Incontinence. Med Clin North Am 2011;95:539–54.[↩][↩]
- Botlero R, Davis SR, Urquhart DM, Bell RJ. Incidence and resolution rates of different types of urinary incontinence in women: findings from a cohort study. J Urol 2011;185:1331–7.[↩]
- Boustani MA, Campbell NL, Munger S, Maidment I, Fox GC. Impact of anticholinergics on the ageing brain: a review and practical application. Aging Health 2008;4:311–20.[↩]
- Wagg A. Treating overactive bladder in the elderly. Can Urol Assoc J 2011;5(5 Suppl 2):S149–51.[↩]
- Kuteesa W, Moore K. Anticholinergic drugs for overactive bladder. Australian Prescriber 2006;29:22–4.[↩]
- Cartwright R, Srikrishna S, Cardozo L. New pharmacological interventions for overactive bladder. Expert Rev Obstet Gynaecol 2008;3:129–36.[↩]
- Anger JT, Weinberg A, Suttorp MJ, Litwin MS, Shekelle PG. Outcomes of intravesical botulinum toxin for idiopathic overactive bladder symptoms: a systematic review of the literature. J Urol 2010;183:2258–64.[↩]
- Smith C, Chancellor M. Botulinum toxin: clinical uses in urology. AUA update series 2008;27(15).[↩]
- Karsenty G, Denys P, Amarenco G, et al. Botulinum toxin A (Botox) intradetrusor injections in adults with neurogenic detrusor overactivity/neurogenic overactive bladder: a systematic literature review. Eur Urol 2008;53:275–87.[↩]





{kind=link}