Contents
- What is tetracycline
- Tetracycline mechanism of action
- What is tetracycline used for?
- Tetracycline special precautions
- Tetracycline and pregnancy
- I took tetracycline during the first trimester of my pregnancy. Is there a risk for birth defects?
- Is there a risk for other problems if I take tetracycline at any time during pregnancy?
- I have heard that tetracycline also affects the bones of developing babies. Is this true?
- What if I am taking one of the other medications in this group such as minocycline, oxytetracycline, or doxycycline instead of tetracycline? Does that still put my baby at risk?
- Can I breastfeed my baby if I am taking tetracycline?
- Tetracycline interactions
- Tetracycline and pregnancy
- Tetracycline dosage
- Adult dose for acne
- Adult dose for bronchitis
- Adult dose for brucellosis
- Adult dose for chlamydia infection
- Adult dose for Helicobacter pylori infection
- Adult dose for Lyme disease – arthritis
- Adult dose for Lyme disease – carditis
- Adult dose for Lyme disease – erythema chronicum migrans
- Adult dose for Lyme disease – neurologic
- Adult dose for pneumonia
- Adult dose for Rickettsial infection
- Adult dose for Upper Respiratory Tract Infection
- Adult dose for Psittacosis
- Adult dose for Ornithosis
- Adult dose for Syphilis – Early
- Adult dose for Syphilis – Latent
- Adult dose for Tertiary Syphilis
- Adult dose for nongonococcal urethritis
- Adult dose for gonococcal infection – uncomplicated
- Adult dose for cystitis
- Adult dose for epididymitis – sexually transmitted
- Adult dose for lymphogranuloma venereum
- Adult dose for Pelvic Inflammatory Disease
- Pediatric Dose for Bacterial Infection
- Renal Dose Adjustments
- Liver Dose Adjustments
- What should I do if I forget a dose?
- Tetracycline side effects
What is tetracycline
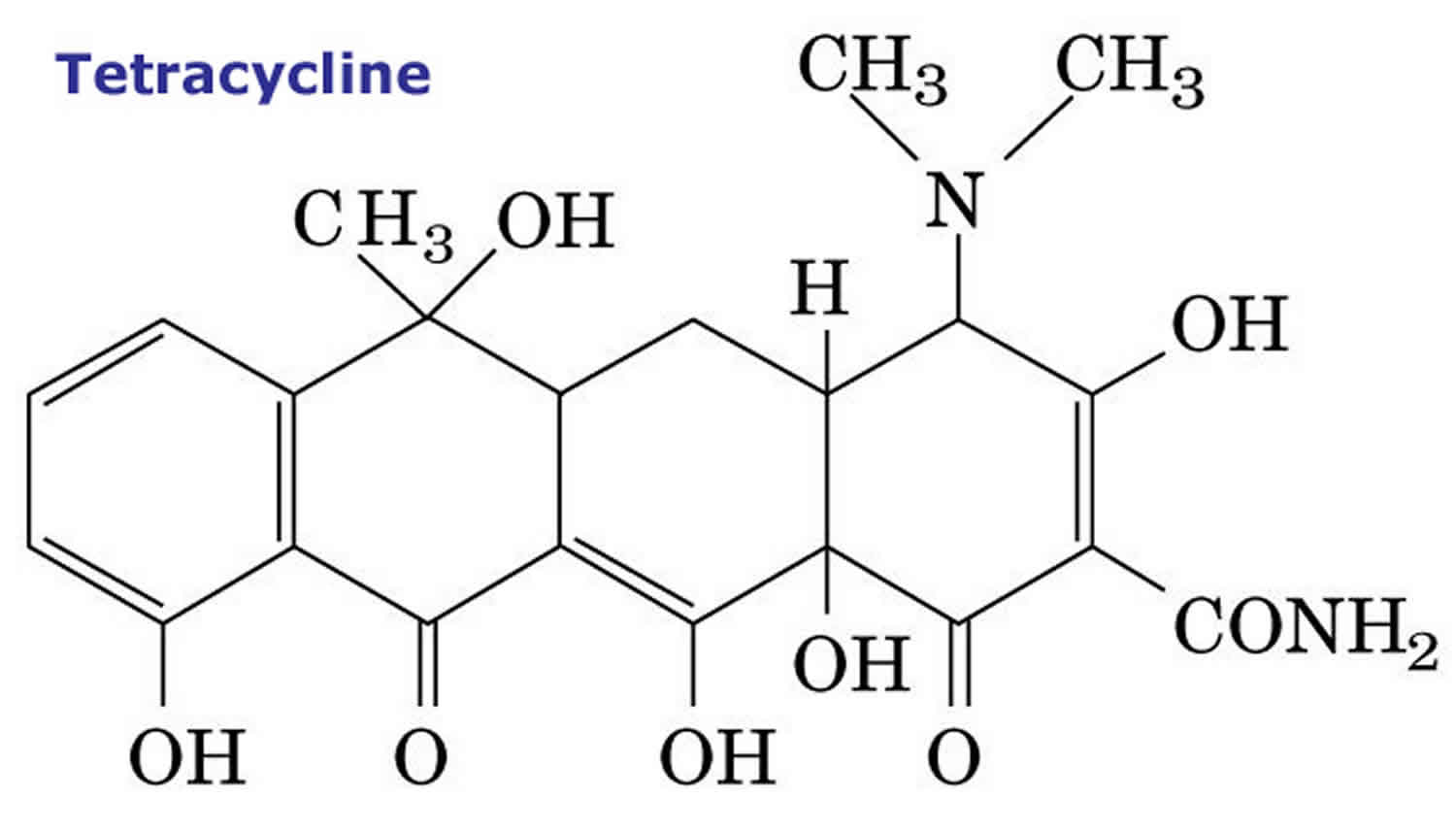
Tetracyclines are oral broad-spectrum, bacteriostatic antibiotics that are active against many pathogens including gram positive and gram negative bacteria, spirochetes, chlamydia, leptospira, mycoplasma and rickettsia. Currently, tetracycline is most frequently used for upper respiratory and skin and soft tissue infection and more than 2 million prescriptions are filled yearly. Chronic therapy with tetracycline is effective in improving acne, but because of their better absorption and tissue penetration, minocycline and doxycycline have largely replaced tetracycline for this indication. Tetracycline is also active against infections with several rickettsial, spirochetal, chlamydial and mycoplasmas infections and are often used for therapy of nonspecific urethritis and several Rickettsia diseases, such as Rocky Mountain spotted fever and Lyme disease. Tetracycline is a semisynthetic derivative of Streptomyces actinobacteria. Tetracycline acts by inhibition of protein synthesis by binding to the 30S subunit of microbial ribosomes. Human cells are less susceptible to this inhibition.
Tetracycline was first approved for use in the United States in 1957 and was one of several oral tetracyclines used at that time (oxytetracycline, chlortetracycline), many of which are no longer available or are used in veterinary medicine only. More modern forms of tetracycline include doxycycline and minocycline which are much more commonly used and have similar indications.
At least eight different tetracyclines are currently available in the United States: tetracycline, doxycycline, minocycline, tigecycline, sarecycline, omadacycline, eravacycline and demeclocycline. Several others tetracyclines have been used in the past in the United States or Europe, but have been withdrawn (chlortetracycline, aureomycin, triacetyloleandomycin, rolitetracycline, oxytetracycline). While all tetracyclines are capable of causing a distinctive form of acute fatty liver disease when given intravenously in high doses, liver injury from oral forms tetracyclines vary greatly in frequency and clinical features. Minocycline is the most commonly implicated tetracycline in causing liver injury and generally ranks within the 10 most common causes of drug induced liver injury in developed nations. Minocycline hepatotoxicity generally presents with a long latency, hepatocellular enzyme elevations, prominent autoimmune features, apparent response to corticosteroid therapy and relatively bengn course. Doxycycline, in contrast, usually presents with a short latency (within 60 days), a cholestatic course, mild immunoallergic or autoimmune features and sometimes prolonged, but ultimately benign course.
- Demeclocycline
- Doxycycline
- Eravacycline
- Minocycline
- Omadacycline
- Sarecycline
- Tetracycline
- Tigecycline
Tetracycline is available in multiple generic forms as capsules or tablets of 250 and 500 mg and generally recommended in doses of 250 to 500 mg three to four times daily for 7 to 30 days. Chronic therapy is typical for therapy of acne. Pediatric formulations as oral suspension are also available. Parenteral tetracycline is no longer used.
Tetracycline should be taken on an empty stomach, at least 1 hour before or 2 hours after meals or snacks. Tetracyclines should be taken with a full glass (8 ounces) of water to prevent irritation of the esophagus (tube between the throat and stomach) or stomach. Do not take tetracycline with food, especially dairy products such as milk, milk formulas, yogurt, cheese, and ice cream. They may keep tetracycline from working properly. However, if this medicine upsets your stomach, your doctor may want you to take it with food. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take tetracycline exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
Tetracycline common side effects include gastrointestinal upset, nausea, poor appetitle, diarrhea, glossitis, rash and hypersensitivity reactions. Tetracycline can cause staining of developing teeth (in children or when taken by a pregnant mother).
Tetracycline mechanism of action
Tetracyclines act by binding to bacterial ribosomes (30S subunit) inhibiting protein synthesis. Bacterial resistance is common and is usually caused by plasmids that decrease the bacterial cell wall permeability.
What is tetracycline used for?
Tetracycline is used to treat infections caused by bacteria including pneumonia and other respiratory tract infections; certain infections of skin, eye, lymphatic, intestinal, genital and urinary systems; and certain other infections that are spread by ticks, lice, mites, and infected animals. Tetracycline is also used along with other medications to treat acne. Tetracycline is also used to treat plague and tuleramia. Tetracycline can also be used in patients who cannot be treated with penicillin to treat certain types of food poisoning, and anthrax.
Tetracycline is also sometimes used to treat Lyme disease and malaria, and to prevent plague and tularemia in people who have been exposed to plague or tularemia germs.
Antibiotics such as tetracycline will not work for colds, flu, or other viral infections. Using antibiotics when they are not needed increases your risk of getting an infection later that resists antibiotic treatment.
Tetracycline special precautions
Before taking tetracycline:
- tell your doctor and pharmacist if you are allergic to tetracycline, minocycline, doxycycline, demeclocycline, any other medications, or any of the ingredients in the tetracycline capsule. Ask your pharmacist for a list of the ingredients.
- tell your doctor and pharmacist what prescription and nonprescription medicines, vitamins, nutritional supplements, and herbal products you are taking or plan to take. Be sure to mention any of the following: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven), and penicillin.
be aware that antacids containing magnesium, aluminum, calcium, or sodium bicarbonate, calcium supplements, zinc products, iron products, and laxatives containing magnesium interfere with tetracycline, making it less effective. Take tetracycline 2 hours before or 6 hours after antacids, calcium supplements, zinc products, and laxatives containing magnesium. Take tetracycline 2 hours before or 4 hours after iron preparations and vitamin products that contain iron. Take tetracycline 2 hours before or after zinc containing products. - tell your doctor if you have or have ever had lupus (condition in which the immune system attacks many tissues and organs including the skin, joints, blood, and kidneys), or kidney disease.
- tell your doctor if you are pregnant, plan to become pregnant, or are breastfeeding. If you become pregnant while taking tetracycline, call your doctor immediately. Tetracycline can harm the fetus.
- plan to avoid unnecessary or prolonged exposure to sunlight and to wear protective clothing, sunglasses, and sunscreen. Tetracycline may make your skin sensitive to sunlight. Tell your doctor right away if you get a sunburn.
- you should know that when tetracycline is used during pregnancy or in babies or children up to age 8, it can cause the teeth to become permanently stained. Tetracycline should not be used in children under age 8 unless your doctor decides it is needed.
Tetracycline and pregnancy
One small study, involving 111 women who filled a prescription for tetracycline at the beginning of their pregnancy, found a slightly higher chance of miscarriage. However, this study did not identify what illness the women were being treated for, or, if the women actually took their medication. It is difficult to know if the medical condition for which the tetracycline was prescribed could have also been a cause for the higher chance of miscarriage.
I took tetracycline during the first trimester of my pregnancy. Is there a risk for birth defects?
Unlikely. The studies are not extensive on tetracycline but have been reassuring. Researchers have studied the outcome of pregnancies when women took tetracycline during the first trimester (the first 14 weeks). This is the time when the organs are forming in the baby. These studies have not shown an increased chance for major birth defects in children exposed to tetracycline in the first trimester of pregnancy.
Is there a risk for other problems if I take tetracycline at any time during pregnancy?
Yes. Studies suggest that if tetracycline is taken after the fourth month of pregnancy, there is a chance for discoloration (gray or yellowish brown) of the “baby” teeth. The discoloration of the baby teeth is due to calcification (hardening) of the teeth. Although this changes the look of the teeth, it does not seem to change the development of the outer covering, the enamel, or, the chance of getting cavities. It is not clear how many babies who are exposed in pregnancy will go on to have toot staining. It is suggested that the use of tetracycline be avoided after four months of pregnancy unless there is a special reason for your healthcare provider to prescribe the medication.
I have heard that tetracycline also affects the bones of developing babies. Is this true?
Tetracycline appears to affect the calcification (hardening) of the bones and teeth, and it also appears to cause reduced growth of some bones while the baby is being exposed to the medication. Even though the tooth discoloration is permanent, the bone growth seems to return to normal after the exposure to tetracycline ends.
What if I am taking one of the other medications in this group such as minocycline, oxytetracycline, or doxycycline instead of tetracycline? Does that still put my baby at risk?
Studies have not looked at minocycline or oxytetracycline use during pregnancy. Since these antibiotics are like tetracycline, it is possible that they could also affect a baby’s teeth and bones in the same way if taken in the second and third trimesters of pregnancy. There are some reports of babies with tooth discoloration after similar exposures. For this reason, it is best to use the same caution with these medications.
Can I breastfeed my baby if I am taking tetracycline?
Yes if it is short-term. The bones and teeth in the baby continue to harden until one year of age. Theoretically, if a baby is exposed to tetracycline in breast milk, it could cause tooth discoloration and delayed bone growth. However, only very low levels of tetracycline pass into breast milk. At this time, there have been no problems reported in babies exposed to tetracycline through breast milk.
The World Health Organization (WHO) Working Group on Human Lactation states that when tetracycline is used for 7-10 days while nursing, the risk to the infant appears to be low. However, other types of antibiotics may be suggested for use while breastfeeding. Be sure to talk to your health care provider about all of your breastfeeding questions.
Tetracycline interactions
Although certain medicines should not be used together at all, in other cases two different medicines may be used together even if an interaction might occur. In these cases, your doctor may want to change the dose, or other precautions may be necessary. When you are taking any of these medicines, it is especially important that your healthcare professional know if you are taking any of the medicines listed below. The following interactions have been selected on the basis of their potential significance and are not necessarily all-inclusive.
Using tetracycline antibiotics with any of the following medicines is not recommended. Your doctor may decide not to treat you with a medication in this class or change some of the other medicines you take.
- Acitretin
- Methoxyflurane
Using tetracycline antibiotics with any of the following medicines is usually not recommended, but may be required in some cases. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Acenocoumarol
- Amoxicillin
- Ampicillin
- Apixaban
- Ardeparin
- Argatroban
- Ascorbic Acid
- Atazanavir
- Bacampicillin
- Betrixaban
- Bexarotene
- Bivalirudin
- Carbamazepine
- Certoparin
- Cholera Vaccine, Live
- Cloxacillin
- Dabigatran Etexilate
- Dalteparin
- Danaparoid
- Desirudin
- Dicloxacillin
- Digoxin
- Edoxaban
- Enoxaparin
- Enzalutamide
- Etretinate
- Fondaparinux
- Fosphenytoin
- Heparin
- Isotretinoin
- Lepirudin
- Lumacaftor
- Methicillin
- Methotrexate
- Methoxyflurane
- Mitotane
- Nafcillin
- Oxacillin
- Parnaparin
- Penicillin G
- Penicillin G Benzathine
- Penicillin G Procaine
- Penicillin V
- Phenindione
- Phenprocoumon
- Phenytoin
- Piperacillin
- Pivampicillin
- Protein C
- Reviparin
- Rifampin
- Rivaroxaban
- St John’s Wort
- Sultamicillin
- Temocillin
- Tinzaparin
- Tretinoin
- Warfarin
Other Interactions
Certain medicines should not be used at or around the time of eating food or eating certain types of food since interactions may occur. Using alcohol or tobacco with certain medicines may also cause interactions to occur. Discuss with your healthcare professional the use of your medicine with food, alcohol, or tobacco.
Other Medical Problems
The presence of other medical problems may affect the use of tetracycline antibiotics. Make sure you tell your doctor if you have any other medical problems, especially:
- Diabetes insipidus (water diabetes)—Demeclocycline may make the condition worse.
- Kidney disease (does not apply to doxycycline or minocycline)—Patients with kidney disease may have an increased chance of side effects.
- Liver disease—Patients with liver disease may have an increased chance of side effects if they use doxycycline or minocycline.
Tetracycline dosage
The dose tetracycline antibiotics will be different for different patients. Follow your doctor’s orders or the directions on the label. The following information includes only the average doses of tetracycline antibiotics. If your dose is different, do not change it unless your doctor tells you to do so.
The amount of tetracycline antibiotic that you take depends on the strength of the tetracycline antibiotic. Also, the number of doses you take each day, the time allowed between doses, and the length of time you take the tetracycline antibiotic depend on the medical problem for which you are using tetracycline antibiotic.
For oral tetracycline dosage forms (capsules and suspension):
- For bacterial or protozoal infections:
- Adults and teenagers: 250 to 500 milligrams (mg) every six hours; or 500 mg to 1 gram every twelve hours. Gonorrhea is treated with 1.5 grams as the first dose, then 500 mg every six hours for four days.
- Children older than 8 years of age: Dose is based on body weight. The usual dose is 6.25 to 12.5 mg per kilogram (kg) (2.8 to 5.7 mg per pound) of body weight every six hours; or 12.5 to 25 mg per kg (5.7 to 11.4 mg per pound) of body weight every twelve hours.
- Infants and children 8 years of age and younger—Tetracyclines are usually not used in young children because tetracyclines can permanently stain teeth.
Adult dose for acne
- 500 mg orally twice a day for 2 weeks or more, depending on the nature and severity of the infection
Adult dose for bronchitis
- 500 mg orally every 6 hours for 7 to 10 days, depending on the nature and severity of the infection; may be given for 4 to 5 days a week during winter months as prophylaxis against chronic infectious bronchitis
Adult dose for brucellosis
- 500 mg orally 4 times a day for 3 weeks given with streptomycin 1 g IM twice a day the first week and once a day the second week
Adult dose for chlamydia infection
- Uncomplicated urethral, endocervical, or rectal infection: 500 mg orally 4 times a day for at least 7 days
The patient’s sexual partner(s) should also be evaluated/treated.
Oral doxycycline therapy is preferred by the Centers for Disease Control and Prevention (CDC) for the treatment of chlamydial infections in nonpregnant patients.
Adult dose for Helicobacter pylori infection
- 500 mg orally every 6 hours for 14 days given in conjunction with bismuth, metronidazole, and an H2 blocker
Adult dose for Lyme disease – arthritis
- 500 mg orally every 6 hours for 14 to 30 days, depending on the nature and severity of the infection
Adult dose for Lyme disease – carditis
- 500 mg orally every 6 hours for 14 to 30 days, depending on the nature and severity of the infection
Adult dose for Lyme disease – erythema chronicum migrans
- 500 mg orally every 6 hours for 10 to 30 days, depending on the nature and severity of the infection
Adult dose for Lyme disease – neurologic
- 500 mg orally every 6 hours for 21 to 30 days, depending on the nature and severity of the infection
Adult dose for pneumonia
- 500 mg orally every 6 hours for 10 to 21 days, depending on the nature and severity of the infection
Adult dose for Rickettsial infection
- 500 mg orally every 6 hours for 7 days
Adult dose for Upper Respiratory Tract Infection
500 mg orally every 6 hours for 7 to 10 days, depending on the nature and severity of the infection
Adult dose for Psittacosis
- 500 mg orally 4 times a day; initial treatment with IV doxycycline may be necessary for seriously ill patients
- Duration: Treatment should continue at least 10 to 14 days after fever subsides to prevent relapse
Adult dose for Ornithosis
- 500 mg orally 4 times a day; initial treatment with IV doxycycline may be necessary for seriously ill patients
- Duration: Treatment should continue at least 10 to 14 days after fever subsides to prevent relapse
Adult dose for Syphilis – Early
- 500 mg orally every 6 hours for 14 days; alternatively, 30 to 40 g in divided doses over a period of 10 to 15 days has been recommended
Tetracycline should be used only if penicillins are contraindicated.
Adult dose for Syphilis – Latent
- 500 mg orally every 6 hours for 28 days; alternatively, 30 to 40 g in divided doses over a period of 10 to 15 days has been recommended
Tetracycline should be used only if penicillins are contraindicated.
Adult dose for Tertiary Syphilis
- 500 mg orally every 6 hours for 28 days
Tetracycline should be used only if penicillins are contraindicated.
Adult dose for nongonococcal urethritis
- 500 mg orally every 6 hours for 7 days
- The patient’s sexual partner(s) should also be evaluated/treated.
Adult dose for gonococcal infection – uncomplicated
- 500 mg orally 4 times a day for 7 days
- The patient’s sexual partner(s) should also be evaluated/treated.
Neisseria gonorrhoeae is insufficiently susceptible to tetracycline; therefore, tetracycline is not recommended by the CDC for the treatment of gonorrhea. Oral doxycycline therapy is the preferred treatment for possible concurrent chlamydial infection in nonpregnant patients.
Adult dose for cystitis
500 mg orally every 6 hours for 3 to 7 days, depending on the nature and severity of the infection; recommended if no alternatives exist
Adult dose for epididymitis – sexually transmitted
- 500 mg orally every 6 hours for 10 days
- The patient’s sexual partner(s) should also be evaluated/treated.
Doxycycline for 10 days, in conjunction with a single dose of a parenteral third-generation cephalosporin like ceftriaxone, has been specifically recommended by the CDC as primary treatment for sexually transmitted epididymitis. Tetracycline may be a reasonable substitute for doxycycline in this regimen.
Adult dose for lymphogranuloma venereum
Although tetracyclines in general may be useful for the treatment of lymphogranuloma venereum, doxycycline is much more commonly used and is specifically recommended by the CDC as primary therapy for this disease. Therefore, the use of tetracycline for the treatment of this patient with lymphogranuloma venereum is not recommended. Doxycycline may be an effective alternative.
Adult dose for Pelvic Inflammatory Disease
Although tetracyclines in general may be useful in combination with other agents for the treatment of pelvic inflammatory disease, doxycycline is much more commonly used and is specifically recommended by the CDC as a therapy for this disease. Therefore, the use of tetracycline for the treatment of this patient with pelvic inflammatory disease is not recommended. Doxycycline may be an effective alternative.
Pediatric Dose for Bacterial Infection
- Above 8 years of age: 25 to 50 mg/kg orally per day divided in 4 equal doses
Renal Dose Adjustments
Total dosage should be decreased by reduction of recommended individual doses and/or by extending time intervals between doses.
Some experts recommend:
- CrCl 50 to 80 mL/min: dose every 8 to 12 hours
- CrCl 10 to 50 mL/min: dose 12 to 24 hours
- CrCl less than 10 mL/min: dose every 24 hours
Liver Dose Adjustments
- Data not available
What should I do if I forget a dose?
Take the missed dose as soon as you remember it. However, if it is almost time for the next dose, skip the missed dose and continue your regular dosing schedule. Do not take a double dose to make up for a missed one.
Tetracycline side effects
Tetracycline may cause side effects. Tell your doctor if any of these symptoms are severe or do not go away:
- nausea
- vomiting
- diarrhea
- itching of the rectum or vagina
- swollen tongue
- black or hairy tongue
- sore or irritated throat
Some side effects can be serious. If you experience any of these symptoms, call your doctor immediately:
- headache
- blurred vision, seeing double, or loss of vision
- skin rash
- hives
- swelling of the face, throat, tongue, lips, and eyes
- difficulty breathing or swallowing
- joint stiffness or swelling
- unusual bleeding or bruising
- chest pain
- a return of fever, sore throat, chills, or other signs of infection
- watery or bloody stools , stomach cramps, or fever during treatment or for up to two or more months after stopping treatment
Tetracycline may cause other side effects. Call your doctor if you have any unusual problems while taking tetracycline.





{kind=link}