Contents
- What are the types of fat?
- What are Healthy fats?
- What are Unhealthy fats?
- How much fat do I need?
- The Truth About Fats and Oils: the good, the bad, and the in-between
- Are unsaturated fats bad?
- 2) Saturated Fats
- Is Saturated Fat Bad for you?
- Is Saturated Fat Healthy?
- There’s a lot of conflicting information about saturated fats. Should you eat them or not?
- Foods high in saturated fat
- Are there “good” saturated fats?
- I’ve heard that grass-fed beef contains healthy fat, is this true?
- What about coconut oil, isn’t that the healthy type of saturated fat?
- Aren’t nuts and olives healthy, do I have to worry about the saturated fat in those?
- Do I have to completely remove saturated fat from my diet?
- What’s my daily limit for foods with saturated fats?
- 3) Bad Fats (Trans Fat or Hydrogenated Oils)
- How to Make Healthy Lifestyle and Eating Choices
- What is the best way to lose weight?
What are the types of fat?
There are 4 main types of fats:
- Unsaturated fats are those that are liquid at room temperature. The two kinds of unsaturated fats are monounsaturated fat and polyunsaturated fat. Both of these unsaturated fats are typically liquid at room temperature. Unsaturated fats are in fish, such as salmon, trout and herring, and plant-based foods such as avocados, olives and walnuts. Liquid vegetable oils, such as soybean oil, corn oil, safflower oil, canola oil, olive oil, peanut oil, canola oil and sunflower oil, also contain unsaturated fats. Eaten in moderation, both kinds of unsaturated fats may help improve your blood cholesterol when used in place of saturated and trans fats. You want to include as many unsaturated fats in your diet because they can decrease bad cholesterol, contain high amounts of antioxidants such as Vitamin E, and contain essential omega-3 and omega-6 fatty acids. Unsaturated fats are typically classified by how many hydrogen bonds they have in their structure: either 1 (mono) or two or more (poly).
- Monounsaturated fats. Monounsaturated fat is a type of unsaturated fat. Monounsaturated fats are liquid at room temperature but start to harden when chilled. Monounsaturated fats is one of the healthy fats, along with polyunsaturated fat. Monounsaturated fats are good for your health in several ways:
- Monounsaturated fats can help lower your LDL (bad) cholesterol level. Cholesterol is a soft, waxy substance that can cause clogged, or blocked, arteries (blood vessels). Keeping your LDL level low reduces your risk for heart disease and stroke.
- Eating plant foods high in monounsaturated fats, particularly extra virgin olive oil and tree nuts, may benefit heart health and blood sugar regulation. Monounsaturated fats from plants may lower bad cholesterol and raise good cholesterol. They also may improve the control of blood sugar levels. Replacing saturated fats with monounsaturated fats in your diet may lower the level of bad cholesterol and triglycerides in your blood. Triglycerides are fat cells that circulate in the bloodstream and are stored in the body’s fat cells. A high level of triglycerides in the blood increases the risk of diseases of the heart and blood vessels.
- Monounsaturated fats help develop and maintain your cells.
- Monounsaturated fats are found in plant foods, such as nuts, avocados, and vegetable oils. Monounsaturated fats are found in red meats and dairy products. About half the fats in these foods are saturated and half monounsaturated. Many plants and plant oils are high in monounsaturated fats but low in saturated fats. These include:
- Oils from olives, peanuts, canola seeds, safflower seeds, and sunflower seeds.
- Avocadoes.
- Pumpkin seeds.
- Sesame seeds.
- Almonds.
- Cashews.
- Peanuts and peanut butter.
- Pecans.
- Polyunsaturated fats. Polyunsaturated fat is a type of unsaturated fat. Polyunsaturated fats are liquid at room temperature but start to harden when chilled. Polyunsaturated fats include omega-3 and omega-6 fats. These are essential fatty acids that your body needs for brain function and cell growth. Your body does not make essential fatty acids, so you must get them from food. Polyunsaturated fats can help lower your LDL (bad) cholesterol. Cholesterol is a soft, waxy substance that can cause clogged or blocked arteries (blood vessels). Having low LDL cholesterol reduces your risk for heart disease. Polyunsaturated fats is one of the healthy fats, along with monunsaturated fat. Polyunsaturated fat is found in plant and animal foods, such as salmon, vegetable oils, and some nuts and seeds.
- Omega-3 fatty acids are good for your heart in several ways. They help:
- Reduce triglycerides, a type of fat in your blood
- Reduce the risk of developing an irregular heartbeat (arrhythmia)
- Slow the buildup of plaque, a substance comprising fat, cholesterol, and calcium, which can harden and clog your arteries
- Slightly lower your blood pressure
- Sources of omega-3 fatty acids include:
- Fish such as salmon, anchovies, mackerel, herring, sardines and tuna.
- Oils from canola seeds, soybeans, walnuts and flaxseed.
- Soybeans.
- Chia seeds.
- Flaxseed.
- Walnuts.
- Omega-6 fatty acids may help:
- Control your blood sugar
- Reduce your risk for diabetes
- Lower your blood pressure
- Sources of omega-6 fatty acids include:
- Corn oil.
- Cottonseed oil.
- Peanut oil.
- Soybean oil.
- Sunflower oil.
- Omega-3 fatty acids are good for your heart in several ways. They help:
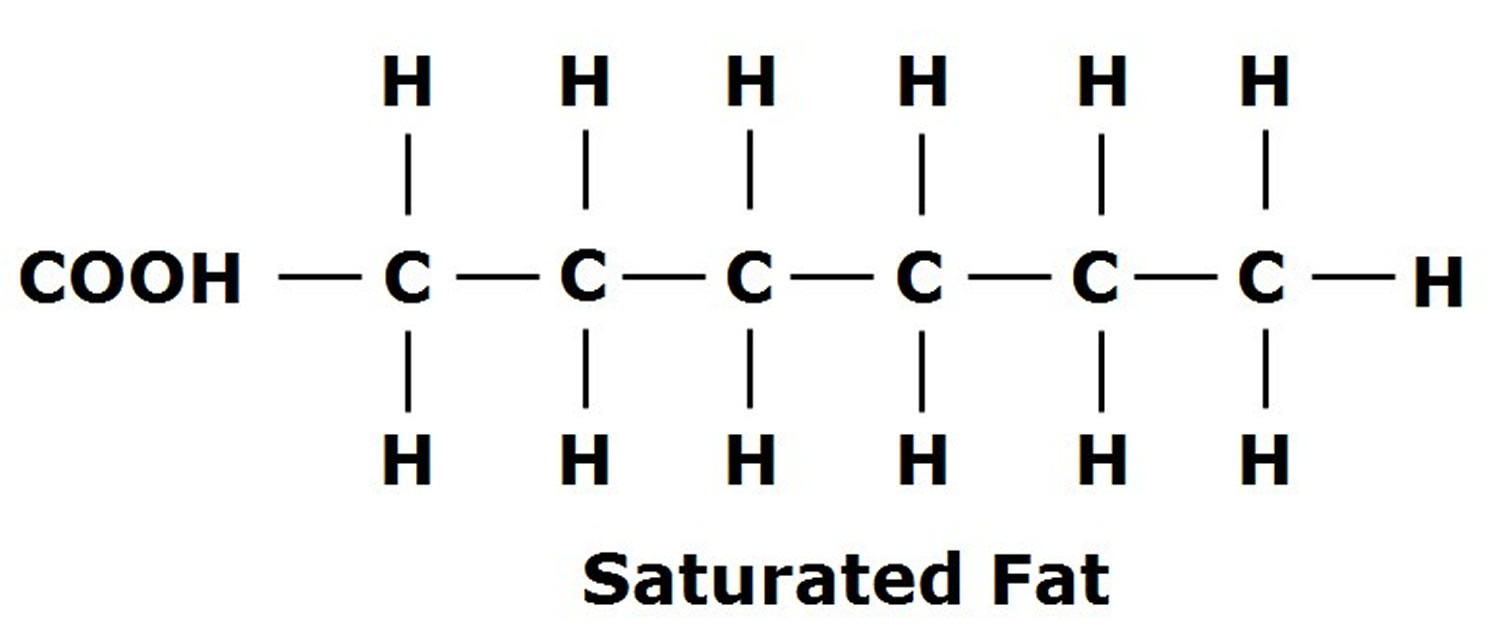
- Saturated fats. Saturated fats are those that are solid at room temperature. Examples include margarine, butter, whole fat dairy products, the fat marbling in meats, and coconut oil. Saturated fats don’t need to be avoided entirely, but diets high in saturated fats can increase bad cholesterol and triglycerides, increasing the risk for heart disease. The Dietary Guidelines for Americans suggest that less than 10% of calories a day should be from saturated fats. The American Heart Association recommends that saturated fats only make up 5 to 6% of your daily calories. For a 2,000 calorie diet, that is a total of 100 calories, or 11 grams a day. Foods high in saturated fats include:
- Foods baked or fried using saturated fats.
- Meats, including beef, lamb, pork as well as poultry, especially with skin.
- Lard.
- Dairy products like butter and cream.
- Whole or 2% milk.
- Whole-milk cheese or yogurt.
- Oils from coconuts, palm fruits, or palm kernels.
- Trans fats. Trans fatty acids are unhealthy fats that form when vegetable oil goes through a process called hydrogenation. This leads the fat to harden and become solid at room temperature. Hydrogenated fats, partially hydrogenated oils (PHOs) or “trans fats,” are often used to keep some foods fresh for a long time. Trans fats are unsaturated fats that are artificially turned into saturated fats and increase heart disease and stroke risk by raising bad LDL cholesterol and decreasing good HDL cholesterol levels. High LDL (bad) cholesterol along with low HDL (good) cholesterol levels can cause cholesterol to build up in your arteries (blood vessels). This increases your risk for heart disease and stroke. Trans fats have also been known to increase the risk of developing type 2 diabetes. Trans fats are most commonly found in fried foods, frozen baked products such as pizza, non-dairy coffee creamers, vegetable shortenings, some margarines, crackers, cookies, snack foods, and other foods made with or fried in partially hydrogenated oils (PHOs). Because of the health risks from trans fats, the United States Food and Drug Administration (FDA) has banned food manufacturers from adding partially hydrogenated oils (PHOs) to foods. Although the food industry has greatly reduced the use of trans fat in recent years, trans fat may still be found in many fried, packaged, or processed foods. There are very small amounts of naturally occurring trans fat in meats and dairy from grazing animals, such as cows, sheep and goats. You should avoid foods made with hydrogenated and partially hydrogenated oils (such as hard butter and margarine). They may contain high levels of trans fatty acids. It is important to read nutrition labels on foods. This will help you know what kinds of fats, and how much, your food contains.
Cutting down on foods and drinks that are high in saturated and trans fats will help to keep your heart healthy and maintain your weight. You can replace some of them with unsaturated fats.
Recommendations for fat intake
Because some dietary fats are potentially helpful and others potentially harmful to your health, it pays to know which ones you’re eating and whether you’re meeting recommendations.
The Dietary Guidelines for Americans offers the following recommendations about dietary fat intake 1:
- Avoid trans fat.
- Limit saturated fat to less than 10 percent of calories a day.
- Replace saturated fat with healthier monounsaturated and polyunsaturated fats.
Be aware that many foods contain different kinds of fat and varying levels of each type. For example, butter contains unsaturated fats, but a large percentage of the total fat is saturated fat. And canola oil has a high percentage of monounsaturated fat but also contains smaller amounts of polyunsaturated and saturated fat.
Your body needs some fat — the healthy fats — to function normally. If you try to avoid all fat, you risk getting insufficient amounts of fat-soluble vitamins and essential fatty acids.
The most common monounsaturated fats (monounsaturated fatty acids or MUFA) in daily nutrition is oleic acid, followed by palmitoleic acid, and vaccenic acid 2. Moreover, oleic acid represents the topmost monounsaturated fats (monounsaturated fatty acids or MUFA) provided in the diet (~90% of all MUFA) 2. No dietary recommendations for monounsaturated fats are given by the National Institute of Medicine, the United States Department of Agriculture, the European Food and Safety Authority and the American Diabetes Association. In contrast, the Academy of Nutrition and Dietetics as well as the Canadian Dietetic Association both promote <20% monounsaturated fats of daily total energy consumption, while the American Heart Association sets a limit of 20% monounsaturated fats in their respective guidelines 3, 4.
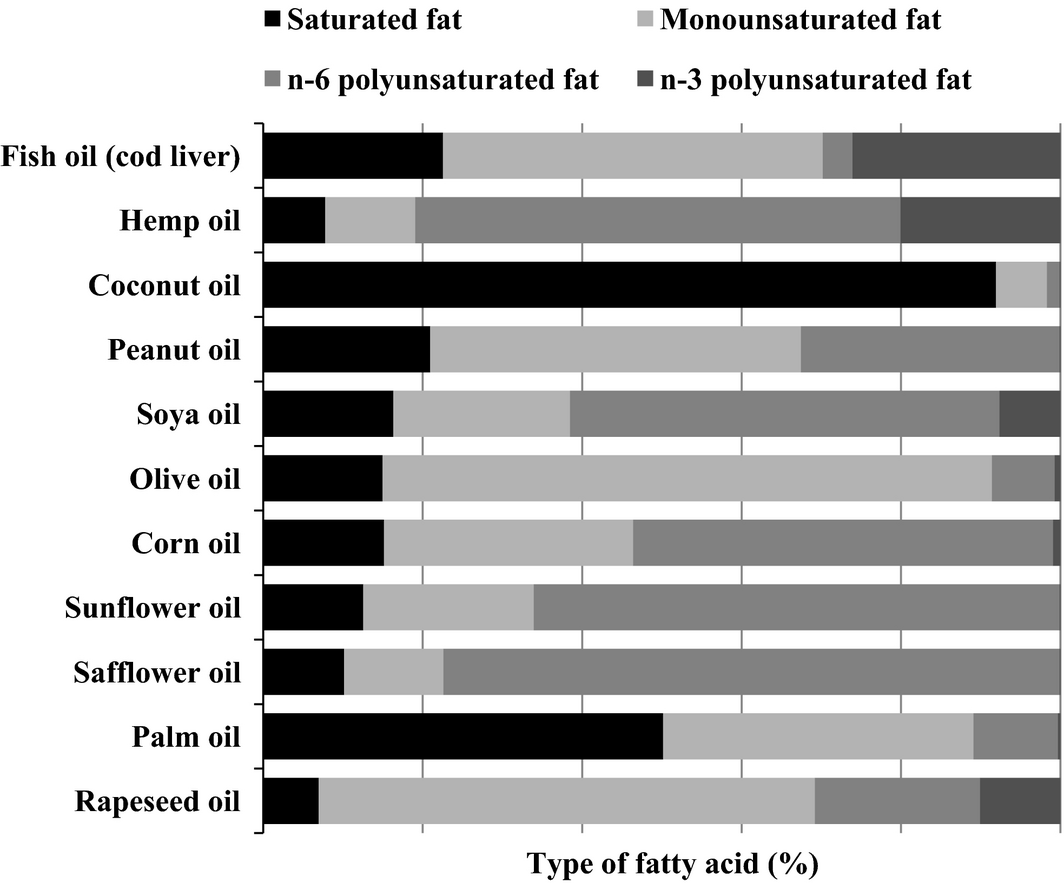
Table 1. Fatty acid content of different oils, nuts, fruits, seeds and animal products
| Oils | Monounsaturated fatty acid (MUFA) % | Polyunsaturated fatty acid (PUFA) % | Saturated fatty acid (SFA) % |
|---|---|---|---|
| Olive oil | 73 | 10.5 | 14 |
| Coconut oil | 6 | 2 | 86 |
| Soybean oil | 23 | 58 | 16 |
| Peanut oil | 46 | 32 | 17 |
| Sesame oil | 40 | 42 | 14 |
| Sunflower oil (linoleic acid <60%) | 45 | 40 | 10 |
| High-oleic safflower oil | 72 | 13 | 7.5 |
| Sunflower oils (linoleic acid >70%) | 14 | 75 | 6 |
| Walnut oil | 23 | 63 | 9 |
| Almond oil | 70 | 17 | 8 |
| Hazelnut oil | 78 | 10 | 7 |
| Avocado oil | 71 | 13 | 12 |
| Canola oil | 63 | 28 | 7 |
| Mustard oil | 59 | 21 | 12 |
| High oleic sunflower | 84 | 4 | 10 |
| Hering oil | 57 | 16 | 21 |
| Fish oil, cold liver | 47 | 23 | 23 |
| Flaxseed oil, cold press | 18 | 68 | 9 |
| Corn and canola oil | 58 | 29 | 8 |
| High oleic sunflower | 84 | 4 | 10 |
| Hazelnut oil | 78 | 10 | 7 |
| Olive oil | 73 | 10.5 | 14 |
| High-oleic safflower oil | 72 | 13 | 7.5 |
| Avocado oil | 71 | 13 | 12 |
| Almond oil | 70 | 17 | 8 |
| Canola oil | 63 | 28 | 7 |
| Mustard oil | 59 | 21 | 12 |
| Corn and canola oil | 58 | 29 | 8 |
| Hering oil | 57 | 16 | 21 |
| Fish oil, cold liver | 47 | 23 | 23 |
| Peanut Oil | 46 | 32 | 17 |
| Sunflower Oil (linoleic acid <60%) | 45 | 40 | 10 |
| Sesame Oil | 40 | 42 | 14 |
| Soybean oil | 23 | 58 | 16 |
| Walnut oil | 23 | 63 | 9 |
| Flaxseed oil, cold press | 18 | 68 | 9 |
| Sunflower oils (linoleic acid >70%) | 14 | 75 | 6 |
| Coconut oil | 6 | 2 | 86 |
| Nuts and Seeds | Monounsaturated fatty acid (MUFA) % | Polyunsaturated fatty acid (PUFA) % | Saturated fatty acid (SFA) % |
| Macademia | 59 | 12 | 2 |
| Hazelnut | 46 | 8 | 4 |
| Pecanut | 41 | 22 | 6 |
| Almonds | 31 | 11 | 4 |
| cashew nuts, dry roasted | 27 | 7 | 9 |
| Pistacchio nuts | 24 | 14 | 5 |
| Sunflower seed kernels, dried | 19 | 23 | 4 |
| Sesame, whole, roasted and toasted | 18 | 21 | 7 |
| Walnuts | 15 | 35 | 3 |
| Flaxseed | 8 | 29 | 4 |
| Safflower kernels, dried | 5 | 28 | 4 |
| Products of Animal Origin | Monounsaturated fatty acid (MUFA) % | Polyunsaturated fatty acid (PUFA) % | Saturated fatty acid (SFA) % |
| Butter, salted | 21 | 3 | 51 |
| Cheese, cheddar | 9 | 1 | 21 |
| Pork, ham | 8.3 | 2 | 6.5 |
| Mackerl | 5.4 | 3.3 | 3.2 |
| Beef, steak | 4.5 | 0.4 | 4.3 |
| Egg | 3.6 | 2 | 3 |
| Salmon | 2.1 | 2.5 | 0.9 |
| Milk, 3.7% fat | 1 | 0.1 | 2.2 |
| Chicken | 0.9 | 0.75 | 0.8 |
Footnote: MUFA = monounsaturated fatty acid; PUFA = polyunsaturated fatty acid; SFA = saturated fatty acid
[Source 3 ]Figure 1. Monounsaturated Fat Structure
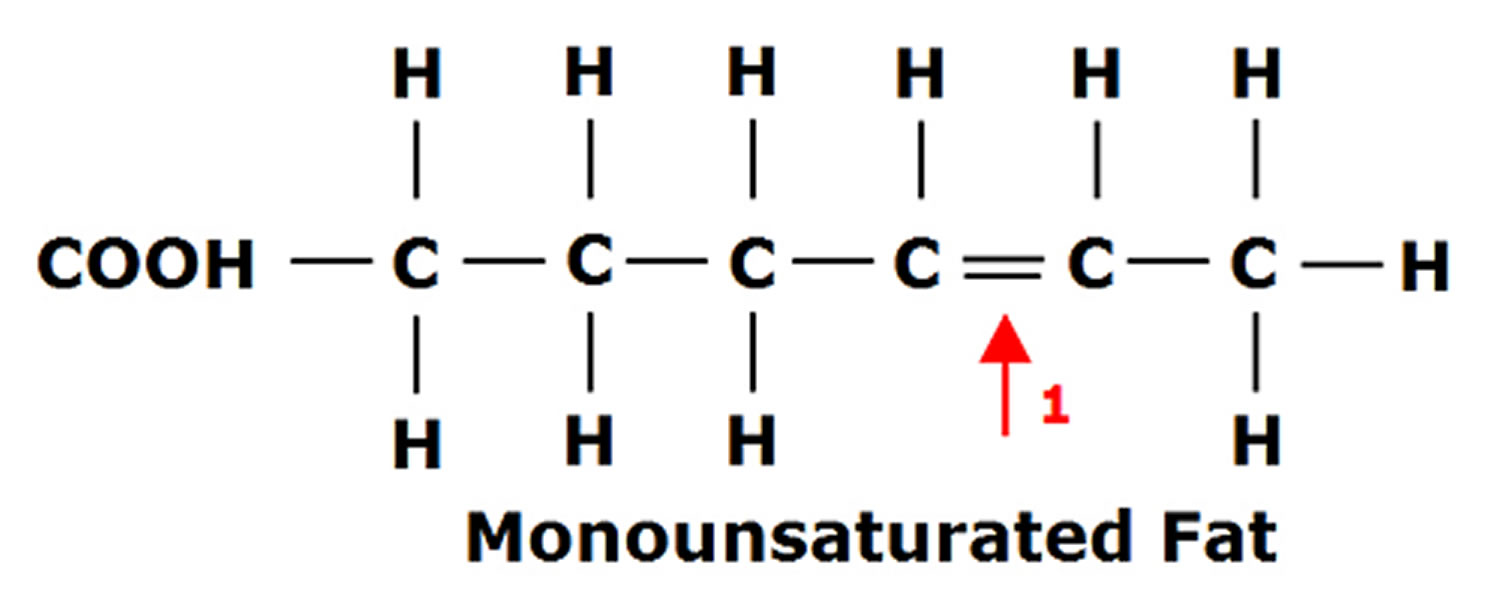
Figure 2. Polyunsaturated Fatty Acids Structure
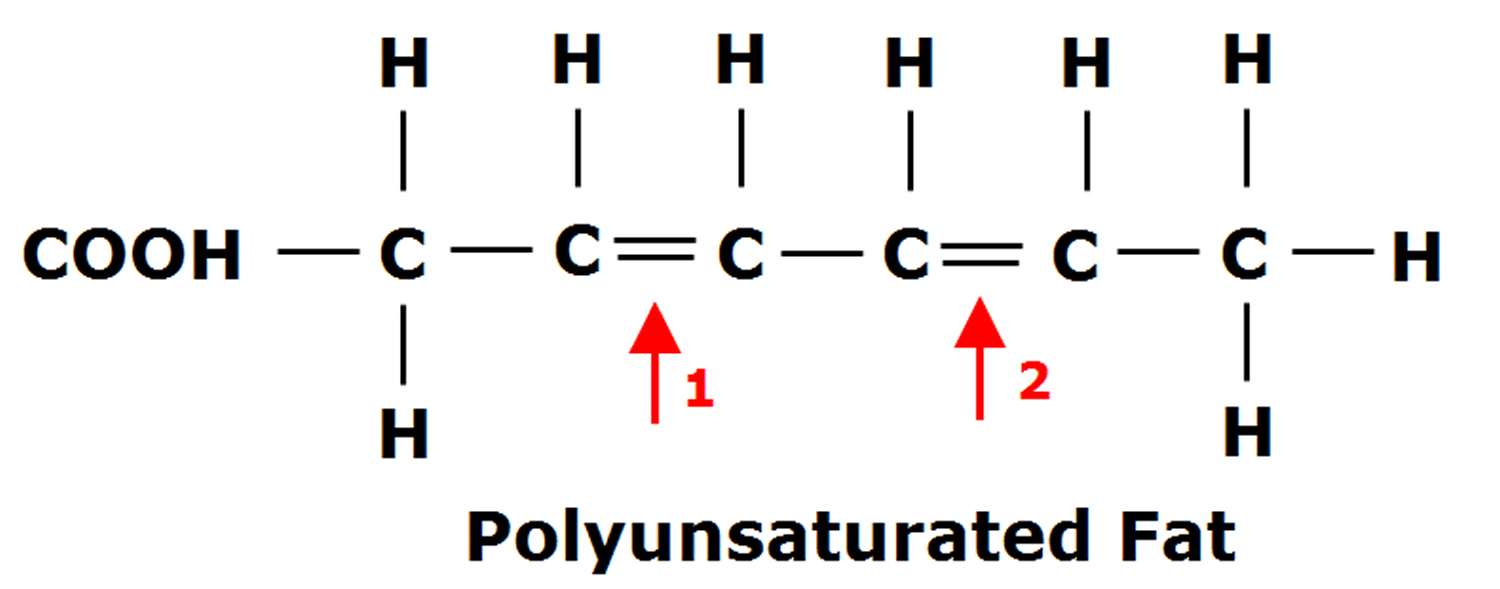
Figure 3. Saturated Fat Structure
What are Healthy fats?
Healthy fats include:
- Monounsaturated fats
- Polyunsaturated fats (omega-3 and omega-6).
Unsaturated fats are those that are liquid at room temperature and can have beneficial effect on your heart. The two kinds of unsaturated fats are monounsaturated fat and polyunsaturated fat. Both of these unsaturated fats are typically liquid at room temperature. Unsaturated fats are in fish, such as salmon, trout and herring, and plant-based foods such as avocados, olives and walnuts. Liquid vegetable oils, such as soybean oil, corn oil, safflower oil, canola oil, olive oil, peanut oil, canola oil and sunflower oil, also contain unsaturated fats. Eaten in moderation, both kinds of unsaturated fats may help improve your blood cholesterol when used in place of saturated and trans fats. You want to include as many unsaturated fats in your diet because they can decrease bad cholesterol, contain high amounts of antioxidants such as Vitamin E, and contain essential omega-3 and omega-6 fatty acids. Unsaturated fats are typically classified by how many hydrogen bonds they have in their structure: either 1 (mono) or two or more (poly). Polyunsaturated fats are distinguished from saturated and monounsaturated fatty acids by the presence of two or more double bonds between carbons within the fatty acid chain. Polyunsaturated fatty acids (PUFAs) are frequently designated by their number of carbon atoms and double bonds. Alpha-linolenic acid (ALA), for example, is known as C18:3n-3 because it has 18 carbons and 3 double bonds and is an omega-3 (n-3) fatty acid. Similarly, eicosapentaenoic acid (EPA) is known as C20:5n-3 and docosahexaenoic acid (DHA) as C22:6n-3 5. Omega-6 fatty acids (omega-6s) have a carbon–carbon double bond that is six carbons away from the methyl end of the fatty acid chain. Linoleic acid (C18:2n-6) and arachidonic acid (C20:4n-6) are two of the major omega-6s 5.
Vegetable oils are the healthy choice for frying and baking, and plant-based spreads, avocados or nut butters for sandwiches, toast and potatoes. These are healthier choices than butter or lard. Check food labels and compare the fat content in different products to help you choose ones that are lower in saturated fats. But remember, while this will help to lower your cholesterol level, you need to look at your whole diet to reduce overall risk. Many factors affect heart disease risk, not one food or nutrient alone. The Mediterranean diet is associated with reducing your risk of heart and circulatory disease. It includes plenty of fruit and vegetables, pulses, fish, nuts and seeds, and less butter, meat, full-fat dairy products and high-fat snacks, so it’s naturally higher in unsaturated fats and lower in saturated fats.
Foods that contain healthy monounsaturated fats include:
- Avocados and their oils/spreads
- Unsalted nuts such as almonds, cashews and peanuts and their butters/spreads
- Olives and their oils/spreads
- Cooking oils made from plants or seeds, including: olive, canola, peanut, sunflower, soybean, sesame and safflower.
Foods that contain healthy polyunsaturated fats (omega-3 and omega-6) include:
- Oily fish like salmon, mackerel and sardines
- Tahini (sesame seed spread)
- Linseed (flaxseed) and chia seeds
- Soybean, sunflower, safflower, canola oil and margarine spreads made from these oils
- Pine nuts, walnuts and brazil nuts.
It is important to choose foods with the healthiest type of fat such as avocados, olives, nuts and seeds, and use healthy oils for cooking, for example, olive, canola, sunflower, peanut and soybean oil.
Reduce the amount of highly processed food you eat such as baked goods including cakes, biscuits and pastries, along with processed meat, and fried and takeaway foods. These foods are high in saturated and trans fats, added sugar and salt, and are not part of a heart-healthy eating pattern. Try to have these foods only sometimes and in small amounts.
Many Americans eat more fat than they need, which can lead to weight gain and heart disease.
Polyunsaturated fats
Polyunsaturated fats also called polyunsaturated fatty acids (PUFAs) can help reduce bad cholesterol levels in your blood, which can lower your risk of heart disease and stroke 6. Polyunsaturated fats also provide nutrients to help develop and maintain your body’s cells. Oils rich in polyunsaturated fats also provide vitamin E, an important antioxidant vitamin. Oils rich in polyunsaturated fats also provide essential fats that your body needs but can’t produce itself, including omega-3 and omega-6 fatty acids. You must get essential fats through food. Omega-6 and omega-3 fatty acids are important for many functions in your body.
Omega-3 fatty acids (omega-3s) have a carbon–carbon double bond located three carbons from the methyl end of the chain. Omega-3s, sometimes referred to as n-3s, are present in certain foods such as flaxseed and fish as well as dietary supplements such as fish oil. Several different omega-3 fatty acids exist, but the majority of scientific research focuses on three: alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) 5. Alpha-linolenic acid (ALA) contains 18 carbon atoms, whereas eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) are considered long-chain omega-3s because eicosapentaenoic acid (EPA) contains 20 carbons and docosahexaenoic acid (DHA) contains 22 5.
The human body can only form carbon–carbon double bonds after the ninth carbon from the methyl end of a fatty acid 7. Therefore, alpha-linolenic acid (ALA) and linoleic acid are considered essential fatty acids, meaning that they must be obtained from your diet 8. Alpha-linolenic acid (ALA) can be converted into eicosapentaenoic acid (EPA) and then to docosahexaenoic acid (DHA), but the conversion which occurs primarily in your liver is very limited, with reported rates of less than 15% 9. Therefore, consuming eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) directly from foods and/or dietary supplements is the only practical way to increase levels of these fatty acids in your body 5.
Alpha-linolenic acid (ALA) is present in plant oils, such as flaxseed, soybean, and canola oils 9. Eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) are present in fish, fish oils, and krill oils, but they are originally synthesized by microalgae at the base of the marine food chain, not by the fish. As microalgae move up the food chain, fish acquire the omega-3s and accumulate them in their tissues 9.
After ingestion, dietary fats are brokendown in your intestines 7. The hydrolysis products—monoglycerides and free fatty acids—are then incorporated into bile-salt– containing micelles and absorbed into enterocytes, largely by passive diffusion. The process is efficient, with an absorption rate of about 95%, which is similar to that of other ingested fats 7. Within intestinal cells, free fatty acids are primarily incorporated into chylomicrons and enter the circulation via the lymphatic system 7, 10. Once in your bloodstream, lipoprotein particles circulate within your body, delivering lipids to various organs for subsequent oxidation, metabolism, or storage in fat tissue 10, 11.
Omega-3 fatty acids play important roles in your body as components of the phospholipids that form the structures of cell membranes 11. Docosahexaenoic acid (DHA), in particular, is especially high in the retina, brain, and sperm 11, 9, 12. In addition to their structural role in cell membranes, omega-3 fatty acids along with omega-6 fatty acids provide energy for your body and are used to form eicosanoids. Eicosanoids are signaling molecules that have similar chemical structures to the fatty acids from which they are derived; they have wide-ranging functions in the body’s cardiovascular, pulmonary, immune, and endocrine systems 13, 8.
The eicosanoids made from omega-6 fatty acids are generally more potent mediators of inflammation, vasoconstriction, and platelet aggregation than those made from omega-3 fatty acids, although there are some exceptions 9, 14. Because both classes of omega-6 and omega-3 fatty acids compete for the same desaturation enzymes, alpha-linolenic acid (ALA) is a competitive inhibitor of linoleic acid metabolism and vice versa 15. Similarly, eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) can compete with arachidonic acid for the synthesis of eicosanoids. Therefore, higher concentrations of eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) than arachidonic acid tip the eicosanoid balance toward less inflammatory activity 16.
Some researchers propose that the relative intakes of omega-6s and omega-3s, the omega-6/omega-3 ratio, may have important implications for the cause of many chronic diseases, such as cardiovascular disease (heart and blood vessel disease) and cancer 16, but the optimal omega-6/omega-3 ratio—if any—has not been defined 17. Others have concluded that such ratios are too nonspecific and are insensitive to individual fatty acid levels 18, 19, 20. Most agree that raising eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) blood levels is far more important than lowering linoleic acid or arachidonic acid levels.
Nontropical vegetable oils high in polyunsaturated fat include:
- Canola oil
- Corn oil
- Soybean oil
- Sunflower oil.
Foods high in polyunsaturated fats include:
- Fatty, or oily fish, including anchovies, herring, mackerel, black cod, salmon, sardines, bluefin tuna, whitefish, striped bass and cobia. These fish are high in omega-3 fatty acids.
- Some nuts and seeds, including walnuts, flaxseeds and sunflower seeds.
- Tofu/soybeans.
Figure 4. Polyunsaturated Fatty Acids Structure
Figure 5. Polyunsaturated fat foods

Monounsaturated fats
Monounsaturated fats also called monounsaturated fatty acids (MUFAs) can also help reduce bad cholesterol levels in your blood, which can lower your risk of heart disease and stroke 21, 22. Monounsaturated fats also provide nutrients to help develop and maintain your body’s cells. Oils rich in monounsaturated fats also provide vitamin E, an important antioxidant vitamin. Olive oil is a type of oil that contains monounsaturated fats. For good health, consume foods that contain monounsaturated fats in place of those that contain saturated fats and/or trans fats. Oils that contain monounsaturated fats are typically liquid at room temperature but start to turn solid when chilled.
Nontropical vegetable oils high in monounsaturated fats include:
- Olive oil
- Canola oil
- Peanut oil
- Safflower oil
- Sesame oil
Foods high in monounsaturated fats include:
- Avocados.
- Peanut butter.
- Some nuts and seeds, including almonds, hazelnuts, pecans, pumpkin seeds and sesame seeds.
Figure 6. Monounsaturated Fat Structure
Figure 7. Monounsaturated fat foods

What are Unhealthy fats?
Unhealthy fats include:
- Saturated fat. Saturated fat and trans fat are ‘unhealthy’ fats. They can raise your ‘bad’ (non-HDL) cholesterol in your blood. Too much cholesterol can increase your risk of having:
- a stroke
- a heart attack
- vascular dementia.
- Trans fat. Trans fatty acids are unhealthy fats that form when vegetable oil goes through a process called hydrogenation. This leads the fat to harden and become solid at room temperature. Hydrogenated fats, partially hydrogenated oils (PHOs) or “trans fats,” are often used to keep some foods fresh for a long time. Trans fats are unsaturated fats that are artificially turned into saturated fats and increase heart disease and stroke risk by raising bad LDL cholesterol and decreasing good HDL cholesterol levels. High LDL (bad) cholesterol along with low HDL (good) cholesterol levels can cause cholesterol to build up in your arteries (blood vessels). This increases your risk for heart disease and stroke. Trans fats have also been known to increase the risk of developing type 2 diabetes. Trans fats are most commonly found in fried foods, frozen baked products such as pizza, non-dairy coffee creamers, vegetable shortenings, some margarines, crackers, cookies, snack foods, and other foods made with or fried in partially hydrogenated oils (PHOs). Because of the health risks from trans fats, the United States Food and Drug Administration (FDA) has banned food manufacturers from adding partially hydrogenated oils (PHOs) to foods. Although the food industry has greatly reduced the use of trans fat in recent years, trans fat may still be found in many fried, packaged, or processed foods. There are very small amounts of naturally occurring trans fat in meats and dairy from grazing animals, such as cows, sheep and goats. You should avoid foods made with hydrogenated and partially hydrogenated oils (such as hard butter and margarine). They may contain high levels of trans fatty acids. It is important to read nutrition labels on foods. This will help you know what kinds of fats, and how much, your food contains.
Foods rich in unhealthy fats include:
- Animal fats including butter, ghee and lard along with the visible fat/skin on meat
- Hydrogenated plant oils like copha, vegetable shortening and some margarines
- Coconut oil
- Processed foods such as baked goods (cakes, biscuits and pastries), processed meat ( bacon, sausages, salami) and fried and takeaway foods.
Replace foods rich in saturated and trans fats with foods rich in healthy unsaturated fats as part of a healthy diet.
It is important to choose foods with the healthiest type of fat such as avocados, olives, nuts and seeds, and use healthy oils for cooking, for example, olive, canola, sunflower, peanut and soybean oil.
Reduce the amount of highly processed food you eat such as baked goods including cakes, biscuits and pastries, along with processed meat, and fried and takeaway foods. These foods are high in saturated and trans fats, added sugar and salt, and are not part of a heart-healthy eating pattern. Try to have these foods only sometimes and in small amounts.
Many Americans eat more fat than they need, which can lead to weight gain and heart disease.
How much fat do I need?
To prevent any fatty acid deficiencies it is recommended that you consume at minimum 1g of fat per kg of body weight per day. According to the Dietary Guidelines for Americans 1, fats should make up 20 to 35 percent of your total daily calorie intake (for adults) with most fats coming from sources of polyunsaturated fats and monounsaturated fats, such as fish, nuts, and vegetable oils. The Dietary Guidelines for Americans also recommend getting less than 10 percent of your calories from saturated fats and keeping trans fat consumption as low as possible for general health and the prevention of chronic disease, including cancer and heart disease 1. The American Heart Association recommends aiming for a dietary pattern that achieves less than 6% of total calories from saturated fat 23, 24. For example, if you need about 2,000 calories a day, no more than 120 calories should come from saturated fat. That’s about 13 grams or less of saturated fat per day 23. Many Americans eat more fat than they need, which can lead to weight gain and heart disease. The nutrition labels on your food’s packaging will show you the amount of total fat and saturated fat you are eating. Looking at the amount of saturated fat in your food will help you keep to the recommended daily intake.
Fat needs will vary by individual and will depend largely on your body composition goals and body types. For example, dietary fat recommendations are slightly higher in competitive athletes than non-athletes to promote health, maintain healthy hormone function, and maintain energy balance. Typical recommendations for athletes are 30 to 50% of total energy intake. You need to eat some fat even when you are trying to lose weight. For those attempting to lose body fat, 0.5 to 1 fat per kg of body weight per day should be consumed per day to avoid essential fatty acid deficiency. For healthy children ages 1 to 3, ages 4 to 18, and adults, approximately 30 to 40%, 25 to 15%, and 20 to 35% of daily energy intake should come from fat, respectively 25. The human body needs small amounts (3 to 6 grams) of essential fatty acids (Omega-6 fatty acids and Omega-3 fatty acids). Fat is important for many body processes. Fat helps your body absorb nutrients and move nutrients around your body. Some fat is necessary as a carrier for the fat-soluble vitamins A, D, E, and K. Fat is the main source of energy storage in your body, fat contributes to cellular structure and function, fat keeps you warm, and protects your organs 26, 27, 28. Fat also helps with hormone production. Therefore your diet should not be devoid of fat. However, because fat is calorically dense (1 gram of fat has 9 calories of energy), it is often decreased on weight-loss diets to reduce energy intake.
Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are omega-3 fatty acids found in varying amounts in seafood such as cold-water fish like salmon, tuna, herring, and mackerel, as well as in fish oil supplements and seaweed. Eating 8 ounces per week of seafood may help reduce the risk for heart disease.
Approximately 5 to 10% of your daily fat energy intake should consist of Omega−6 fatty acids (linoleic acid) and 0.6 to 1.2% of Omega−3 fatty acids (alpha-linolenic acid, eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) 29. Both omega−6 fatty acids (linoleic acid) and omega−3 fatty acids (alpha-linolenic acid, eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) are considered essential fatty acids, meaning that they must be obtained from your diet 8. Apha-linolenic acid (ALA) can be converted into eicosapentaenoic acid (EPA) and then to docosahexaenoic acid (DHA), but the conversion which occurs primarily in your liver is very limited, with reported rates of less than 15% 9, 30. Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are essential fatty acids, meaning the body can’t produce them and they must come from your diet 7. Therefore, consuming eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) directly from foods and/or dietary supplements is the only practical way to increase levels of these fatty acids in your body.
Some researchers propose that the relative intakes of omega-6s and omega-3s, the omega-6/omega-3 ratio, may have important implications for the cause of many chronic diseases, such as heart and blood vessels disease (cardiovascular disease) and cancer 15, but the optimal ratio, if any, has not been defined 31. Others have concluded that the omega-6/omega-3 ratios are too nonspecific and are insensitive to individual fatty acid levels 18, 19, 20.. Most agree that raising EPA and DHA blood levels is far more important than lowering linoleic acid or arachidonic acid levels 30.
For someone who weighs 150lbs (68kg), this would equate to 34-68g fat per day. Using both of these references you can calculate your daily fat needs:
To calculate your daily fat needs:
- Convert body weight in pounds to kilograms (round to the nearest 10th). Multiply weight in kilograms by 1.
Let’s look at an example:
- Convert pounds into kilograms 150lbs / 2.2 = 68.2kg
The recommended fat intake is 1 gram per kilogram of body weight per day
- 68.2kg (1g grams of fat per kilogram) = 68.2g of fat per day
Weight loss diets that are moderate to low in fat (20 to 30% of calories) are called “balanced deficit” diets because they maintain a reasonable balance among macronutrients similar to that recommended in MyPlate, DASH, and the Dietary Guidelines for Americans 1, 32. They tend to achieve most of the caloric deficit by reducing fat from the typical level in North American Diets of about 34% or more of calories to 20 to 30% fat, 15% protein, and 55 to 65% of calories from carbohydrates. Some examples of low fat diets are the Weight Watchers Diet (25% fat, 20% protein, and 55% carbohydrate, with 26 grams of dietary fiber), Jenny Craig, the National Cholesterol Education Program Step 1 diet (25% fat), diets based on the MyPlate, the DASH diet, the Shape up and Drop 10 diet of Shape Up! America and the Nutrisystem diet 33. Popular diet books using this approach include The Biggest Loser Diet, The Mayo Clinic Diet and The Engine 2 Die 33. These dietary patterns have been extensively reviewed and appear to be effective for weight reduction on low calorie diets for most individuals 33.
Very low-fat diets such as the Pritikin Diet 34, the Ornish Diet 35 and The Spark Solution Diet 36 have been advocated not only for weight reduction, but also for improving cardiovascular risk profiles. The Ornish Diet 35, which is very low in fat (13% of calories) and saturated fat, very high in carbohydrate (81% of calories) and very high in fiber (38 grams), is part of a program that includes nonsmoking, exercise and behavior modification. The Ornish Diet 35 was shown to reduce some cardiovascular risk factors in a limited long term study. For those who can adhere to the Ornish regime it may be helpful. However, it may not be appropriate for all populations, such as diabetics.
Are ‘low fat’ and ‘lighter’ foods better for me?
A lower fat option might not be better for you. For a food or drink to be labelled as:
- ‘lite’, ‘light’ or ‘lighter’, it must have at least 30 percent less fat than the original product
- ‘low fat’ or ‘reduced fat’, it must have less than 3g of fat per 100g and in some countries, the pack’s label will have the fat content colored green.
Sometimes, the fat will be replaced with more sugar or salt to make it taste like the original product. This might not make the lower fat option healthier.
Even if your food’s packaging says it’s lower fat, you might want to check its nutrition label. You can check the amount of ‘total fat’ and the amount of ‘saturated fat’ per serving on the label.
How Much Good Fats Do You Really Need?
In 1999, the International Society for the Study of Fatty Acids and Lipids agreed upon a recommendation table on daily intake of fatty acids as a foundation for further discussions 3. Polyunsaturated fatty acids (PUFAs) with 18 carbon (C18) atoms such as linoleic (18:2 ω-6), and α-linolenic (18:3 ω-3) are known as essential fatty acids in human nutrition 37. These fatty acids, although regarded as an indispensable component for cell structure and development and function, cannot be synthesized by the human body. Nutritionists recommend a balanced lipid intake corresponding to a total amount of fats equal to 25 to 30% of total calories with a ratio in fatty acids as follows: 1-Saturates (6–8%), 2-Monounsaturates (12–14%), 3- Polyunsaturates as a ω-6 (6–7%), and 4-Polyunsaturates as a ω-3 (0.5–1.5%) 38. The American Heart Association recommends aiming for a dietary pattern that achieves 5% to 6% of calories from saturated fat 39. Saturated fatty acids increase plasma cholesterol level and acts as “promoters” of certain cancer development (e.g., colon, breast, and perhaps uterus and prostate).
Adequate intake levels for adults were specified with respect to α-linolenic acid (ALA or Omega-3 fatty acid 18:3ω-3), eicosapentaenoic acid (EPA or Long Chain Omega-3 fatty acid 20:5ω-3), docosahexaenoic acid (DHA or Long Chain Omega-3 fatty acid 22:6ω-3), as well as upper limits for linoleic acid (LA or Omega-6 fatty acids), trans-fatty acids, and saturated, given as % of total energy content, respectively. Given a total fat range from 15% to 40% of total energy content, there is no precise value (i.e., % of total energy content in the form of MUFA) was given by the panel 40. According to the Joint FAO/WHO Expert Consultation Committee, MUFA intakes should be determined by calculating the difference: MUFA (% of total energy content) = total fat (% of total energy content) − SFA (% of total energy content) − PUFA (% of total energy content) − TFA (% of total energy content). Accordingly, MUFA intakes (% of total energy content) will range with respect to the total fat and fatty acid composition of the diet 41.
The debate continues on the optimal dietary fatty acid composition, but the evidence supporting Monounsaturated Fatty Acid (MUFA) as the healthy dietary fatty acid is weak. Even when considering the food source of MUFA (plant vs animal), there is little evidence to support recommendations to increase dietary MUFA for coronary heart disease prevention. However, since no detrimental effects of MUFA-rich diets were reported in the literature to date, there is no evidence speaking against the consideration of MUFAs in dietary guidelines. Further studies dealing with long-term effects of MUFA on biomarkers of obesity, diabetes, and cardiovascular diseases as well as clinical endpoints are needed to clarify the potential benefits of MUFA-rich diets in primary and secondary prevention.
On the other hand, increasing dietary Polyunsaturated Fatty Acid (PUFA) consistently appears to provide benefit. A considerably larger number of meta-analyses explored the effects of Polyunsaturated Fatty Acids (PUFAs) on maintenance or reduction of body weight as well as biomarkers of impaired glucose metabolism or cardiovascular disease or coronary heart disease than there are systematic reviews and meta-analyses dealing with the corresponding impact of Monounsaturated Fatty Acids (MUFAs). Consequently, the international recommendations for Polyunsaturated Fatty Acid (PUFA) are more consistent than those for MUFA, averaging a value of 10% of total energy content for healthy persons for the most part. If MUFA recommendations are given at all, they vary between 12% and 25% of total energy content, equaling a remarkable range of ~30–70 g/day for a 2.500 kcal-diet. Prestigious authorities and organizations such as the National Institute of Medicine, the EFSA, the USDA and the ADA do not provide specific recommendation for MUFAs either for healthy people or for patients in need of diabetic or cardiovascular management.
Most of us get too much fat, and too much unhealthy fat. Most experts recommend that we get 30% of our calories from good fat, although we can survive fine on as little as 20%, even 10%. If you’re like most of us, you’re getting plenty of fat – most Americans consume about 40% of their calories from fats in meat, butter, cheese, baked goods, etc.
To make the switch to heart-healthy fats, start by avoiding the truly unhealthy fats – trans fatty acids. These trans fats come from vegetable oils that were chemically modified so they are solid like butter. Because these oils don’t spoil as quickly as butter, they are used in most packaged cookies, chips, crackers and other baked goods sold in the supermarket, as well as in margarines.
Focus on replacing foods high in saturated fat with foods that include monounsaturated fats and polyunsaturated fats.
But a word of caution — don’t go overboard even on healthy fats. All fats, including the healthy ones, are high in calories. So consume monounsaturated and polyunsaturated fats instead of other types of fat, not in addition to them.
Here are some tips to help you make over the fat in your diet:
- To avoid trans fat, check food labels and look for the amount of trans fat listed. By law a serving of food containing less than 0.5 grams of trans fat can be labeled as 0 grams. Therefore, it’s important to also check ingredient lists for the term “partially hydrogenated.”
- Use oil instead of solid fats. For example, saute with olive oil instead of butter, and use canola oil when baking.
- Prepare fish, such as salmon and mackerel, instead of meat at least twice a week to get healthy omega-3 fatty acids. Limit sizes to 4 to 6 ounces of cooked seafood a serving, and bake or broil seafood instead of frying.
- Choose lean meat and skinless poultry. Trim visible fat from meat and poultry, and remove skin from poultry.
- Snack smart. Many popular processed snack foods are high in fat, especially solid fats. Be sure to check food labels for saturated fat. Better yet, snack on whole fruits and vegetables.
The Truth About Fats and Oils: the good, the bad, and the in-between
Fat gets a bad rap even though it is a nutrient that you need in your diet, just not too much. Not all fats are equal. Learn all about dietary fats, which ones actually boost your health and how getting too much or too little affects your health.
Does my body need fats? Yes, it does. Dietary fats are essential to give your body energy and to support cell growth. They also help protect your organs and help keep your body warm. Fats help your body absorb some nutrients and produce important hormones, too. Your body definitely needs fat.
Dietary fats are found in both plant and animal foods. They supply calories and help with the absorption of the fat-soluble vitamins A, vitamin D, vitamin E, and vitamin K. Some also are good sources of two essential fatty acids—linoleic acid and α-linolenic acid.
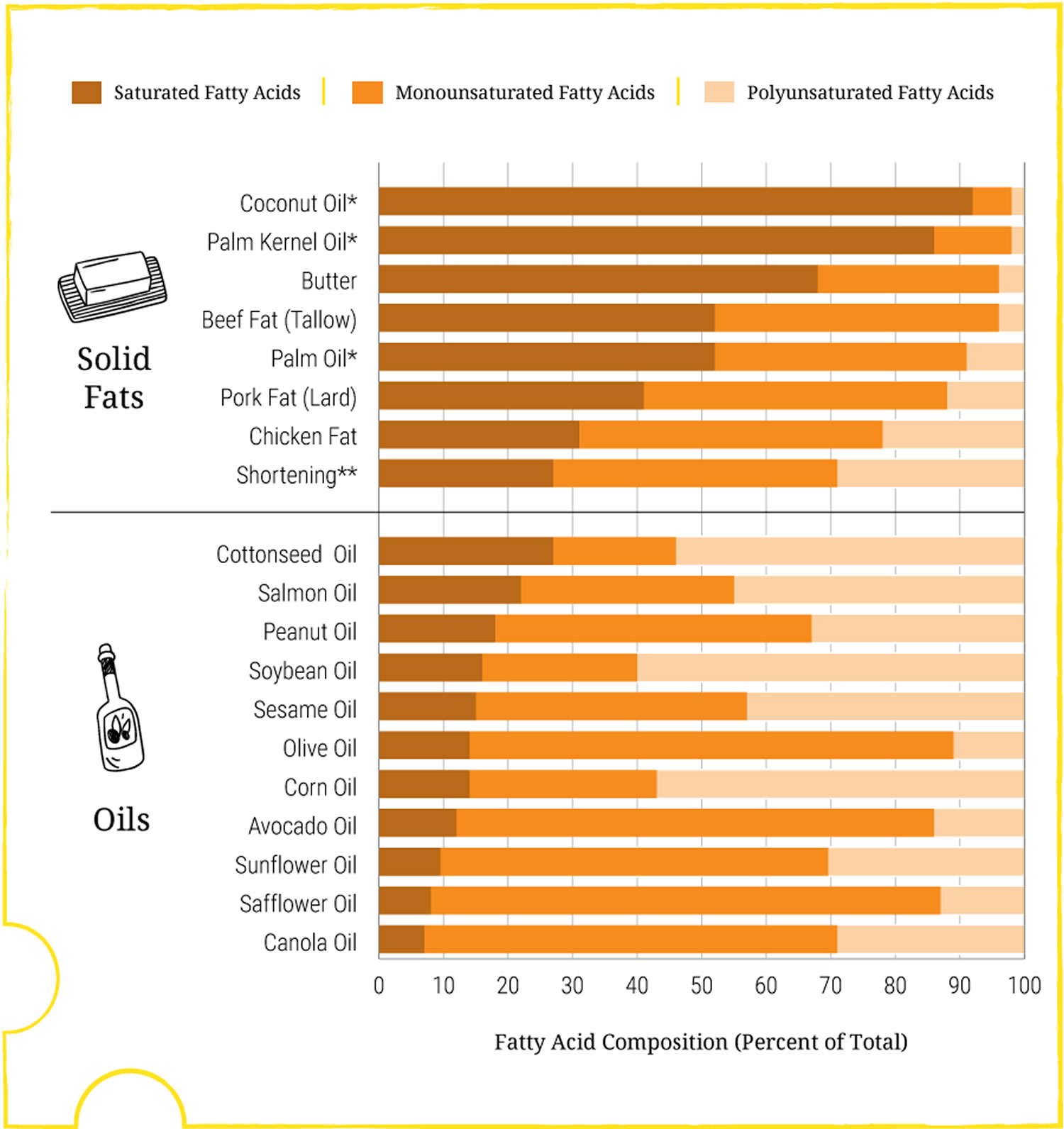
All dietary fats are composed of a mix of polyunsaturated, monounsaturated, and saturated fatty acids, in varied proportions (see Dietary Fats chart). For example, most of the fatty acids in butter are saturated, but it also contains some monounsaturated and polyunsaturated fatty acids. Oils are mostly unsaturated fatty acids, though they have small amounts of saturated fatty acids too.
For years, fat was a four-letter word and fat has been the bogeyman of bad health. We were urged to banish it from our diets whenever possible. We switched to low-fat foods. But the shift didn’t make us healthier, instead our low fat diet (& high sugar diet) are making us fatter and more un-healthy than ever before. This is because the world universally (based on faulty and misleading scientific conclusion) made a major public health ruling to eat low fat in our diet. This is partly because we cut back on healthy fats as well as harmful ones and partly the increase of refined sugar and high fructose corn syrup that have been added to our highly processed foods in order to make them tasty and palatable due to the lower fat/oil contents (emphasis of eating low-fat foods).
Increasingly, however, research is showing that not all fats are equal. Some oils and fatty foods contain chemicals called essential fatty acids, which our bodies need for good health.
Consuming high amounts of saturated fats linked to increased heart disease risk ! 42, 43, 44, 45. Heart and vascular disease includes heart attacks, angina, strokes, sudden cardiovascular death and the need for heart surgery.
In a new study appearing online in the Journal of the American College of Cardiology, Dr. Frank Hu and colleagues found that people who replace saturated fat (primarily found in meats and dairy foods) with refined carbohydrates do not lower their risk of heart disease, whereas those who replace saturated fats with unsaturated fats or whole grains lower their heart disease risk 46.
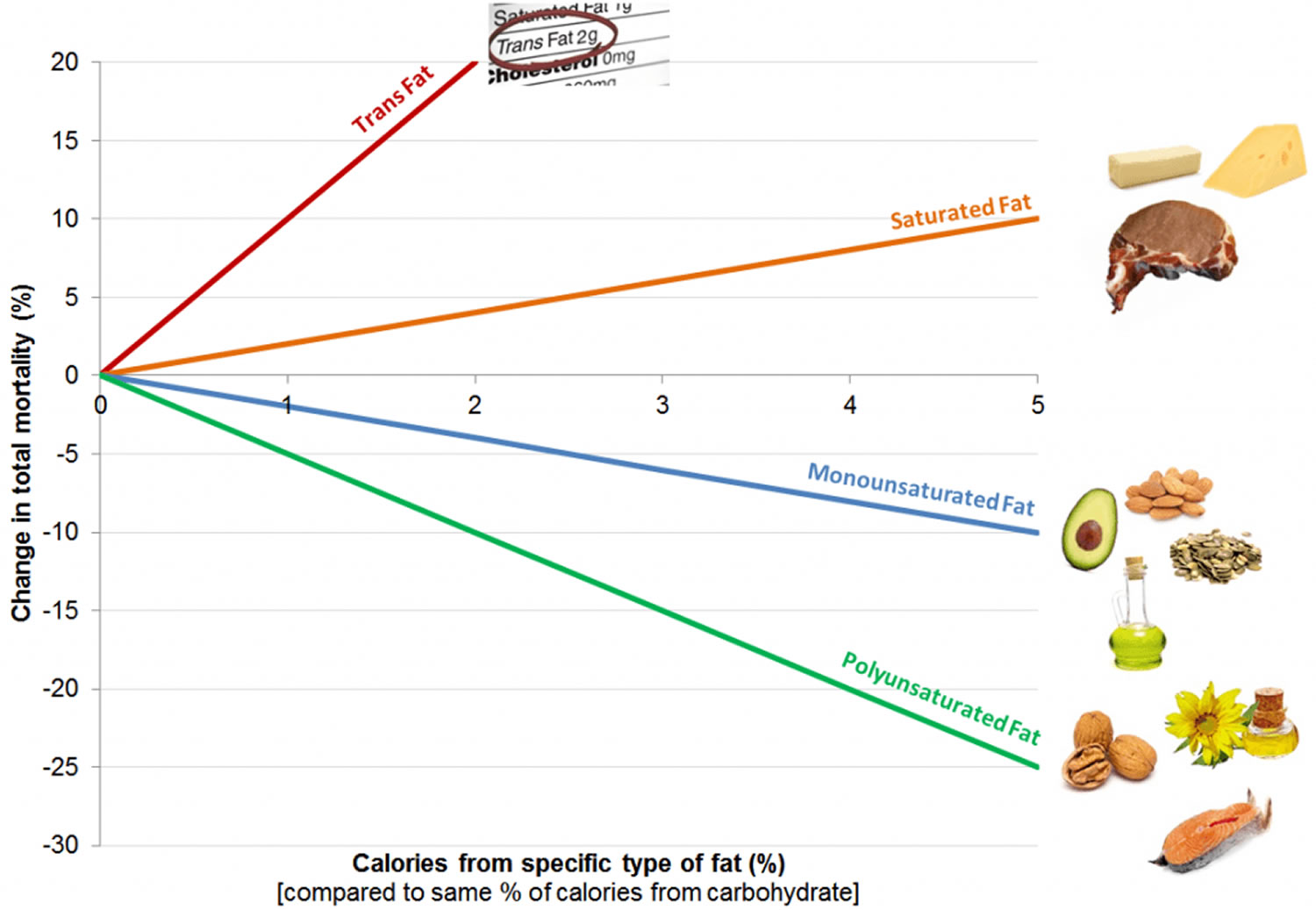
That study shows the importance of eliminating trans fat and replacing saturated fat with unsaturated fats, including both omega-6 and omega-3 polyunsaturated fatty acids 47. Different types of dietary fat had different associations with mortality, the researchers found. Trans fats—on their way to being largely phased out of food—had the most significant adverse impact on health. Every 2% higher intake of trans fat was associated with a 16% higher chance of premature death during the study period. Higher consumption of saturated fats was also linked with greater mortality risk. When compared with the same number of calories from carbohydrate, every 5% increase in saturated fat intake was associated with an 8% higher risk of overall mortality (see Figure 1. Dietary Fats and Mortality Rates). Conversely, intake of high amounts of unsaturated fats—both polyunsaturated and monounsaturated—was associated with between 11% and 19% lower overall mortality compared with the same number of calories from carbohydrates. Among the polyunsaturated fats, both omega-6, found in most plant oils, and omega-3 fatty acids, found in fish and soy and canola oils, were associated with lower risk of premature death.
These findings support current dietary recommendations to replace saturated fat and trans-fat with unsaturated fat.
- Scientists concluded that saturated fat should be no more than 5 percent to 6 percent of daily calories. So, for a diet of 2,000 calories a day, that would mean no more than 120 of them should come from saturated fats. That’s about 13 grams of saturated fats a day 48.
Figure 8. Dietary Fats and Mortality Rates
The Effect of Cutting Down Fat You Eat and Your Weight
Do all fats have the same number of calories? Yes. There are nine calories in every gram of fat, regardless of what type of fat it is. Fats are more energy-dense than carbohydrates and proteins, which provide four calories per gram. (Source 50).
Consuming high levels of calories – regardless of the source – can lead to weight gain or being overweight. Consuming high levels of saturated or trans fats can also lead to heart disease and stroke. Health experts generally recommend replacing saturated fats and trans fats with monounsaturated fats and polyunsaturated fats – while still maintaining a nutritionally-adequate diet.
The ideal proportion of energy from fat in your food and its relation to your body weight is not clear. This review (source 51) looked at the effect of cutting down the proportion of energy from fat in your food on body weight and fatness in both adults and children who are not aiming to lose weight. The review found that cutting down on the proportion of fat in your food leads to a small but noticeable decrease in body weight, body mass index and waist circumference. This effect was found both in adults and children. The effect did not change over time.
Trials where participants were randomised to a lower fat intake versus usual or moderate fat intake, but with no intention to reduce weight, showed a consistent, stable but small effect of low fat intake on body fatness: slightly lower weight, BMI and waist circumference compared with controls. Greater fat reduction and lower baseline fat intake were both associated with greater reductions in weight. This effect of reducing total fat was not consistently reflected in cohort studies assessing the relationship between total fat intake and later measures of body fatness or change in body fatness in studies of children, young people or adults.
How do you know the difference between good fats and bad fats?
Fats are essential for living organisms. Fatty acid molecules have a variable length carbon chain with a methyl terminus and a carboxylic acid head group 52. They can be categorized based on the degree of saturation of their carbon chains. Saturated fatty acids possess the maximal number of hydrogen atoms, while monounsaturated fatty acids (MUFAs) and polyunsaturated fatty acids (PUFAs) have one, or two or more, double bonds, respectively.
The proportions of fatty acids in a particular fat determine the physical form of the fat:
- Fats with a higher amount of polyunsaturated and monounsaturated fatty acids are usually liquid at room temperature and are referred to as “oils.”
- Fats with a higher amount of saturated fatty acids are usually solid at room temperature and are referred to as “solid fats.” Fats containing trans fatty acids are also classified as solid fats, although they may or may not be solid at room temperature.
Your body needs some fat from food. The two essential fatty acids most important to good health are omega-3 and omega-6. But we need these in the right balance in order to protect our hearts, joints, pancreas, mood stability, and skin. It’s a major source of energy. It helps you absorb some vitamins and minerals. Fats help your body absorb fat-soluble vitamins A, vitamin D, vitamin E and vitamin K and stores them in the liver and in fatty tissues for future use.
Fat is needed to build cell membranes, the vital exterior of each cell, and the sheaths surrounding nerves. It is essential for blood clotting, muscle movement, and inflammation. Cholesterol, which is created by fat, produces important hormones like estrogen and testosterone. For long-term health, some fats are better than others. Good fats include monounsaturated and polyunsaturated fats. Bad ones include industrial-made trans fats. Saturated fats fall somewhere in the middle.
All fats have a similar chemical structure: a chain of carbon atoms bonded to hydrogen atoms. What makes one fat different from another is the length and shape of the carbon chain and the number of hydrogen atoms connected to the carbon atoms. Seemingly slight differences in structure translate into crucial differences in form and function.
1) Unsaturated Fats (called the Good Fats) come mainly from vegetables, nuts, seeds, and fish. They differ from saturated fats by having fewer hydrogen atoms bonded to their carbon chains. Healthy fats are liquid at room temperature, not solid. There are two broad categories of beneficial fats: monounsaturated and polyunsaturated fats.
Good fats can improve blood cholesterol levels, ease inflammation and stabilize heart rhythms. Most of us don’t get enough of these healthy unsaturated fats. The traditional Greek diet gets up to 30 percent of its calories from monounsaturated fats, mostly from olive oil.
There are two broad categories of beneficial fats: monounsaturated and polyunsaturated fats. Scientists have now established that trans fats found in many fast foods, bakery products and margarines increase the risk of cardiovascular disease through inflammatory processes.
Are unsaturated fats bad?
No. Unsaturated fats are in fish, such as salmon, trout and herring, and plant-based foods such as avocados, olives and walnuts. Liquid vegetable oils, such as soybean oil, corn oil, safflower oil, canola oil, olive oil, peanut oil, canola oil and sunflower oil, also contain unsaturated fats. Eaten in moderation unsaturated fats may help improve your blood cholesterol when used in place of saturated and trans fats. You want to include as many unsaturated fats in your diet because they can decrease bad LDL cholesterol, contain high amounts of antioxidants such as Vitamin E, and contain essential omega-3 fatty acids and omega-6 fatty acids.
Two types of Unsaturated fats (Good Fats)
a) Monounsaturated Fats are found in high concentrations in olive oil, peanut oil, canola, avocados, almonds, safflower oils, hazelnuts, pecans, pumpkin seeds and sesame seeds and most nuts. Monounsaturated fats also are part of most animal fats such as fats from chicken, pork, beef, and wild game. When you dip your bread in olive oil at an Italian restaurant, you’re getting mostly monounsaturated fat. Monounsaturated fats have a single carbon-to-carbon double bond. The result is that it has two fewer hydrogen atoms than a saturated fat and a bend at the double bond. This structure keeps monounsaturated fats liquid at room temperature. Good sources of monounsaturated fats are olive oil, peanut oil, canola oil, avocados, most nuts, as well as high-oleic safflower and sunflower oils. The carbon-carbon double bond found in monounsaturated or polyunsaturated fatty acids can exist in the cis or trans configuration. When the two hydrogen atoms are on opposite sides of the double bond, the configuration is called trans. When the hydrogen atoms are on the same side of the double bond, the configuration is called cis.
The discovery that monounsaturated fat could be healthful came from the Seven Countries Study during the 1960s. It revealed that people in Greece and other parts of the Mediterranean region enjoyed a low rate of heart disease despite a high-fat diet. The main fat in their diet, though, was not the saturated animal fat common in countries with higher rates of heart disease. It was olive oil, which contains mainly monounsaturated fat. This finding produced a surge of interest in olive oil and the “Mediterranean Diet” a style of eating regarded as a healthful choice today.
Although there’s no recommended daily intake of monounsaturated fats, the Institute of Medicine recommends using them as much as possible along with polyunsaturated fats to replace saturated and trans fats.
Figure 9. Monounsaturated Fatty Acids Structure
b) Polyunsaturated Fats (polyunsaturated fatty acids) are found in high concentrations in sunflower, corn, soybean, flaxseed oils, walnuts, flax seeds, hemp seeds, pine nuts, sesame, cottonseed oils, pumpkin seeds and fish.
Polyunsaturated fatty acids (PUFAs) can be further subdivided on the basis of the location of the first double bond relative to the methyl terminus of the chain. For example, n-3 and n-6 fatty acids are two of the most biologically significant polyunsaturated fatty acid classes, and have their first double bond on either the third or sixth carbon from the chain terminus, respectively. The final carbon in the fatty acid chain is also known as the omega carbon, hence the common reference to these fatty acids as omega-3 or omega-6 PUFAs. The distinction between omega-6 and omega-3 fatty acids is based on the location of the first double bond, counting from the methyl end of the fatty acid molecule (see Figure 4). Omega-6 fatty acids are represented by Linoleic acid (LA) (18:2ω-6) and Arachidonic acid (AA) (20:4ω-6) and omega-3 fatty acids by Alpha-linolenic acid (ALA) (18:3ω-3), Eicosapentaenoic acid (EPA) (20:5ω-3) and Docosahexaenoic acid (DHA) (22:6ω-3).
Long-chain n-3 and n-6 PUFAs are synthesized from the essential fatty acids: alpha-linolenic acid (ALA) and linoleic acid (LA), respectively. Basic structures of these two parent PUFAs are shown in Figure 3 and Figure 4. An essential fatty acid cannot be made by the body and must be obtained through dietary sources. Animals and humans have the capacity to metabolize essential fatty acids to long-chain derivatives. Because the n-6 and n-3 pathways compete with one another for enzyme activity, the ratio of n-6 to n-3 PUFAs is very important to human health. An overabundance of fatty acids from one family will limit the metabolic production of the longer chain products of the other. The typical Western diet provides n-6 and n-3 PUFAs in a ratio ranging from 8:1 to 25:1 52, values in severe contrast with the recommendations from national health agencies of approximately 4:1 53. Lowering the n-6:n-3 ratio would reduce competition for the enzymes and facilitate the metabolism of more downstream products of ALA.
Mammalian cells cannot convert omega-6 to omega-3 fatty acids because they lack the converting enzyme, omega-3 desaturase. Omega-6 and omega-3 fatty acids are not interconvertible, are metabolically and functionally distinct, and often have important opposing physiological effects, therefore their balance in the diet is important 54.
This study showed a balanced omega-6/omega-3 ratio 1–2/1 is one of the most important dietary factors in the prevention of obesity, along with physical activity. A lower omega-6/omega-3 ratio should be considered in the management of obesity 54.
Because most diets are already very rich in n-6 PUFAs, greater focus needs to be placed on incorporating n-3 PUFAs into the diet. Dietary sources of n-3 PUFAs are readily available but in limited quantities. Many foods contain alpha-linolenic acid (ALA), including certain vegetable oils, dairy products, flaxseed, walnuts and vegetables 55. Fatty fish, such as mackerel, herring and salmon, provide an excellent source of the long-chain derivatives of ALA, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) 53.
Omega-3 fatty acids are a type of polyunsaturated fats found in seafood, such as salmon, trout, herring, tuna, and mackerel, and in flax seeds and walnuts. EPA and DHA are long chain n-3 fatty acids found in seafood. Omega-3 fats are one important type of polyunsaturated fat. Polyunsaturated fats are essential fats. That means your body can’t produce these and they’re required for normal body functions. So you must get them from food. Polyunsaturated fats are used to build cell membranes and the covering of nerves. They are needed for blood clotting, muscle movement, and inflammation.
A polyunsaturated fat has two or more double bonds in its carbon chain. There are two main types of polyunsaturated fats: omega-3 fatty acids and omega-6 fatty acids. The numbers refer to the distance between the beginning of the carbon chain and the first double bond (see Figure 4.). Both types offer health benefits.
Figure 10. Polyunsaturated Fatty Acids Structure
Polyunsaturated fatty acids (PUFAs) can be further subdivided on the basis of the location of the first double bond relative to the methyl terminus of the chain. For example, n-3 and n-6 fatty acids are two of the most biologically significant polyunsaturated fatty acid classes, and have their first double bond on either the third or sixth carbon from the chain terminus, respectively. The final carbon in the fatty acid chain is also known as the omega carbon, hence the common reference to these fatty acids as omega-3 or omega-6 PUFAs.
Figure 11. Omega-3 fatty acids (ALA, EPA & DHA) and Omega-6 fatty acids (LA & AA) structure
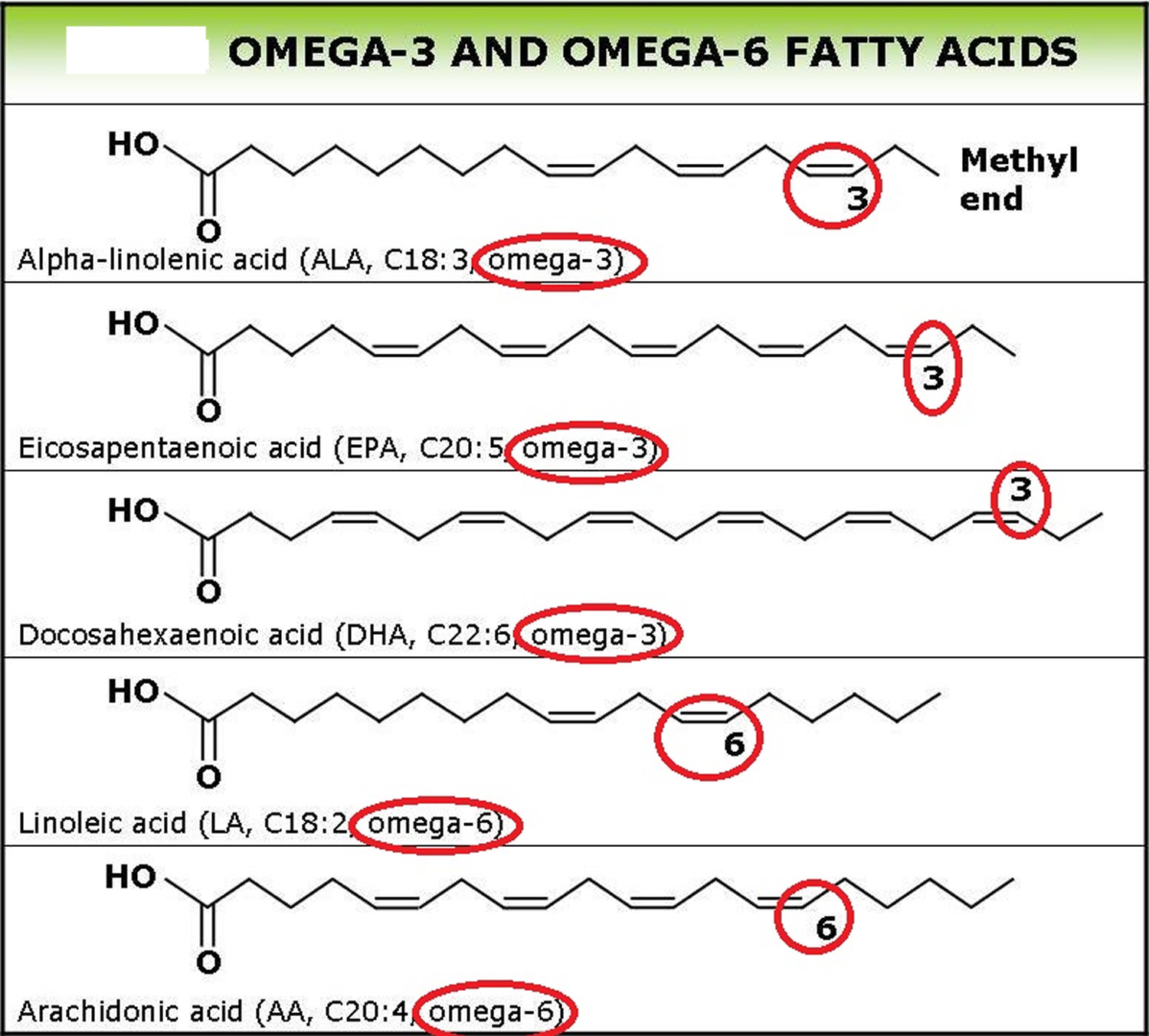
Note: Omega-6 fatty acids are represented by Linoleic acid (LA) (18:2ω-6) and Arachidonic acid (AA) (20:4ω-6) and Omega-3 fatty acids by Alpha-linolenic acid (ALA) (18:3ω-3), Eicosapentaenoic acid (EPA) (20:5ω-3) and Docosahexaenoic acid (DHA) (22:6ω-3).
Eating polyunsaturated fats in place of saturated fats or highly refined carbohydrates reduces harmful LDL cholesterol and improves the cholesterol profile. It also lowers triglycerides.
We don’t eat nearly enough omega-3, which can reduce our risk for heart disease and cancer. Good sources of omega-3 fatty acids include fatty fish such as salmon, mackerel, and sardines, all green leafy vegetables, flaxseeds, walnuts, canola oil, and unhydrogenated soybean oil.
Omega-3 fatty acids may help prevent and even treat heart disease and stroke. In addition to reducing blood pressure, raising HDL, and lowering triglycerides, polyunsaturated fats may help prevent lethal heart rhythms from arising. Evidence also suggests they may help reduce the need for corticosteroid medications in people with rheumatoid arthritis. Studies linking omega-3s to a wide range of other health improvements, including reducing risk of dementia, are inconclusive, and some of them have major flaws, according to a systematic review of the evidence by the Agency for Healthcare Research and Quality.
Omega-6 fatty acids have also been linked to protection against heart disease. Foods rich in linoleic acid and other omega-6 fatty acids include vegetable oils such as safflower, soybean, sunflower, walnut, and corn oils.
The latest research on nuts by the Harvard School of Public Health found that women who reported eating a half serving of peanut butter or a full serving of nuts five or more times a week showed as much as a 30% reduced risk of developing type 2 diabetes. And eating other nuts, like almonds, walnuts, and pecans, have been shown to have heart healthy benefits, including lowering “bad” LDL cholesterol. (Remember, walnuts are also a source of omega-3.)
Foods high in unsaturated fat
There are two types of “good” unsaturated fats:
- Monounsaturated fats are found in high concentrations in:
- Olive, peanut, and canola oils
- Avocados and their oils/spreads
- Nuts such as almonds, hazelnuts, peanuts, pecans and their butters/spreads
- Seeds such as pumpkin and sesame seeds.
- Polyunsaturated fats (omega-3 and omega-6) are found in high concentrations in:
- Soybean, sunflower, safflower, canola oil, corn, flaxseed and margarine spreads made from these oils
- Pine nuts, walnuts and brazil nuts.
- Flax seeds
- Tahini (sesame seed spread)
- Linseed (flaxseed) and chia seeds
- Oily fish like salmon, mackerel and sardines
- Canola oil – though higher in monounsaturated fat, it’s also a good source of polyunsaturated fat.
It is important to choose foods with the healthiest type of fat such as avocados, olives, nuts and seeds, and use healthy oils for cooking, for example, olive, canola, sunflower, peanut and soybean oil.
Reduce the amount of highly processed food you eat such as baked goods including cakes, biscuits and pastries, along with processed meat, and fried and takeaway foods. These foods are high in saturated and trans fats, added sugar and salt, and are not part of a heart-healthy eating pattern. Try to have these foods only sometimes and in small amounts.
Many Americans eat more fat than they need, which can lead to weight gain and heart disease.
2) Saturated Fats
Saturated fats also called saturated fatty acids (SFA) are fats that are solid at room temperature. Because saturated fats are typically solid at room temperature — think cooled bacon grease, butter, beef tallow, coconut oil, ghee or pork lard, they are sometimes called “solid fats”. The word “saturated” here refers to the number of hydrogen atoms surrounding each carbon atom. The chain of carbon atoms holds as many hydrogen atoms as possible — it’s saturated with hydrogens. Saturated fats are common in the American diet. Saturated fats include margarine, butter, whole fat dairy products, lard, the fat marbling in meats, coconut oil and palm oil. Saturated fats are also found in full-fat milk, yogurt, full-fat cheese, cakes, pastries, cookies, crackers, and biscuits 56. Coconut, palm kernel, and palm oil are called oils because they come from plants. However, they are solid or semi-solid at room temperature due to their high content of short-chain saturated fatty acids. They are considered solid fats for nutritional purposes. They also are found in other animal fats, such as pork and chicken fats and in other plant fats, such as nuts. Saturated fats don’t need to be avoided entirely, but diets high in saturated fats can increase bad LDL (low-density lipoprotein) cholesterol and triglycerides, increasing your risk of heart disease and stroke. The Dietary Guidelines for Americans suggest that less than 10% of calories a day should be from saturated fats. The American Heart Association recommends that saturated fats only make up 5 to 6% of your daily calories. For a 2,000 calorie diet, that is a total of 100 calories, or 11 grams a day. But just replacing saturated fat with refined carbohydrates, like sugary foods and drinks, won’t improve your health either. However, replacing saturated fat with unsaturated fats such as monounsaturated fats or polyunsaturated fats that are found in oily fish, nuts, or vegetable oils like rapeseed or sunflower oil, does seem to reduce your risk of heart attack and stroke.
Remember, though, all types of fat are high in calories, so eating too much can lead to weight gain. Being overweight or obese is a risk factor for heart and circulatory disease, and many other diseases.
Foods high in saturated fats include:
- Foods baked or fried using saturated fats.
- Meats, including beef, lamb, pork as well as poultry, especially with skin.
- Lard.
- Dairy products like butter and cream.
- Whole or 2% milk.
- Whole-milk cheese or yogurt.
- Oils from coconuts, palm fruits, or palm kernels.
Figure 12. Saturated Fatty Acids Structure
According to the American Heart Association Advisory 57, cardiovascular disease was lowered by about 30 percent, similar to the effect of cholesterol-lowering statin drugs when vegetable oil replaced saturated fat in the diet. The switch to healthier oils also was associated with lower rates of death from all causes. The American Heart Association recommends aiming for a dietary pattern that achieves 5% to 6% of calories from saturated fat, that’s about 13 grams of saturated fats a day 58.
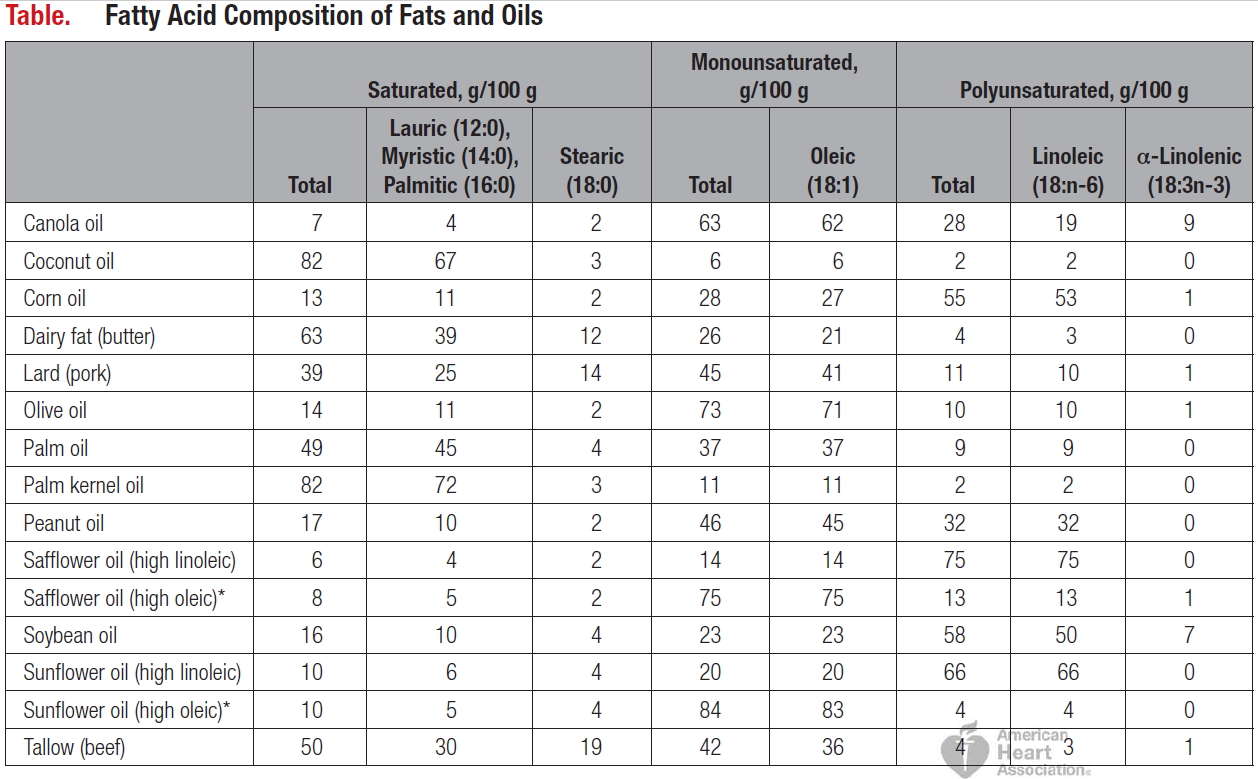
Note: A zero value equals <0.5 g/100 g.
*Primary safflower and sunflower oils of commerce.
Is Saturated Fat Bad for you?
Yes 60, 57, 58. The main sources of saturated fat to be decreased are dairy fat (butter), lard (pork), beef tallow, palm oil, palm kernel oil, and coconut oil. A diet rich in saturated fats can drive up total cholesterol, and tip the balance toward more harmful LDL cholesterol, which prompts blockages to form in arteries in the heart and elsewhere in the body. For that reason, most nutrition experts recommend limiting saturated fat to under 10% of calories a day. The American Heart Association recommends limiting saturated fats to less than 6% of total calories 23, 24, 61. For example, if you need about 2,000 calories a day, no more than 120 calories should come from saturated fat. That’s about 13 grams or less of saturated fat per day 23. Saturated fats are found in butter, cheese, red meat, other animal-based foods and tropical oils.
Recent published review on available clinical trials and scientific studies involving 15 studies with over 59,000 participants 62 — found the evidence on (current) to March 2014 —- that cutting down on saturated fat led to a 17% reduction in the risk of cardiovascular disease (including heart disease and strokes), but no effects on the risk of dying. The review 62 found no clear health benefits of replacing saturated fats with starchy foods or protein. Changing the type of fat we eat, replacing saturated fats with polyunsaturated fats, seems to protect us better, reducing our risk of heart and vascular problems. The greater the decrease in saturated fat, and the more serum total cholesterol is reduced, the greater the protection. People who are currently healthy appear to benefit as much as those at increased risk of heart disease or stroke (people with high blood pressure, high serum cholesterol or diabetes, for example), and people who have already had heart disease or stroke. There was no clear difference in effect between men and women.
However, some recent studies have also questioned the role saturated fat plays in heart disease and this has created confusion among patients, their physicians, and the public 63, 64, 65, 66, 67, 68, 69, 70, 71, 72. One meta-analysis of 21 studies said that there was not enough evidence to conclude that saturated fat increases the risk of heart disease, but that replacing saturated fat with polyunsaturated fat may indeed reduce risk of heart disease.
In a recent randomized clinical trials on saturated fat (published June 2017) 73 where the group that is assigned a diet lower in saturated fat is taught how to replace it with foods higher in ≥1 other macronutrients, typically carbohydrates or unsaturated fats, to maintain the same total energy intake. Other trials, often called controlled feeding trials, actually provide to the research participants their assigned diet high or low in saturated fat balanced with a similar amount of energy from another macronutrient. Essential to the interpretation of the results from these trials (and the reason for the divergent results in meta-analyses noted above) is the macronutrient composition of the comparator diet. Clinical trials that used polyunsaturated fat to replace saturated fat reduced the incidence of cardiovascular disease 66, 74. In contrast, trials that used mainly carbohydrates to replace saturated fat did not reduce cardiovascular disease. However, the types of carbohydrate-containing foods were often unspecified and typically included
sugar and other refined carbohydrates to maintain energy balance. Evidence from prospective observational studies indicates that carbohydrates from whole grains reduce cardiovascular disease when they replace saturated fat 75.
Prospective observational studies, also called cohort studies, are conducted in large populations in which dietary intake is assessed at the beginning of the study and in some studies reassessed repeatedly during the follow-up periods, and cardiovascular disease is assessed at various points during follow-up. In prospective observational studies, the participants eat whatever diet they themselves choose, and the researchers request that participants report their recent or past dietary history. Research participants in observational studies who eat a large amount of saturated fat eat less of various other macronutrients, usually carbohydrates, unsaturated fat, or both, to maintain energy intake. Participants who eat a comparatively small amount of saturated fat eat more carbohydrates or unsaturated fats. Because carbohydrates and unsaturated fats differ in their metabolic effects, it is necessary to evaluate the effects of low and high saturated fat intakes in the context of the replacement macronutrient. This is easier in a clinical trial because the trial controls the dietary intake but more complicated in observational studies in which the participants control their own diets.
Meta-analyses of prospective observational studies aiming to determine the effects on cardiovascular disease of saturated fat that did not take into consideration the replacement macronutrient have mistakenly concluded that there was no significant effect of saturated fat intake on cardiovascular disease risk 70, 76. In contrast, meta-analyses that specifically evaluated the effect of replacing saturated fat with polyunsaturated fat found significant benefit, whereas replacing saturated fat with carbohydrates, especially refined carbohydrates, yielded no significant benefit to cardiovascular disease risk 69, 72, 77. Thus, again, differences in the effects of the replacement or comparator nutrients, specifically carbohydrates and unsaturated fats, are at the root of the apparent discrepancies among studies and meta-analyses on whether lowering saturated fat reduces the risk of developing cardiovascular disease. In fact, the evidence to recommend reduction of saturated fat and its replacement by polyunsaturated and monounsaturated fat has strengthened as better methodology is more widely adopted for the analysis of dietary intake in observational studies. The study authors judge the evidence to favor recommending n-6 polyunsaturated fat, that is, linoleic acid, stronger than monounsaturated fat to replace saturated fat because of the positive results of randomized clinical trials that used polyunsaturated fat compared with the paucity of trials that used monounsaturated fat 78; the greater relative risk reduction for polyunsaturated fats in observational studies 69, 72, 77; the greater reduction in LDL cholesterol with polyunsaturated fat 79; and the regression of atherosclerosis in nonhuman primates by polyunsaturated but not monounsaturated fat 80. However, progress in reducing cardiovascular disease would be enhanced by replacing saturated fat by either type of unsaturated fat. Two other major studies narrowed the prescription slightly, concluding that replacing saturated fat with polyunsaturated fats like vegetable oils or high-fiber carbohydrates is the best bet for reducing the risk of heart disease, but replacing saturated fat with highly processed carbohydrates could do the opposite.
Polyunsaturated fats are contained in canola oil, corn oil, soybean oil, peanut oil, safflower oil, sunflower oil, and walnuts. However, original high-linoleic varieties of safflower and sunflower oils are uncommon. High-oleic varieties of safflower and sunflower oil, olive oil, avocados, and tree nuts such as almonds, cashews, hazelnuts, pistachios, and pecans have mainly monounsaturated fats and are low in saturated fat.
Too much saturated fat in your diet can lead to heart disease and other health problems.
In large randomized clinical trials that used polyunsaturated fat to replace saturated fat reduced the incidence of cardiovascular disease 66, 74. Cardiovascular disease is the leading global cause of death, accounting for 17.3 million deaths per year, comprising 31.5% of total global deaths in 2013. Nearly 808 000 people in the United States died of heart disease, stroke, and other cardiovascular diseases in 2014, translating to about 1 of every 3 deaths.
This large cohort study 47 found that higher intake of saturated fat (found in foods like butter, lard, tallow and red meat) and especially trans fat (predominantly from partially hydrogenated vegetable oil), was associated with greater risk of mortality (death) when compared with the same number of calories from carbohydrate. When compared with carbohydrates, every 5% increase of total calories from saturated fat was associated with an 8% higher risk of overall mortality, and every 2% higher intake of trans fat was associated with a 16% higher risk of overall mortality 47. The study investigated 83,349 women from the Nurses’ Health Study (July 1, 1980, to June 30, 2012) and 42,884 men from the Health Professionals Follow-up Study (February 1, 1986, to January 31, 2012) who were free of cardiovascular disease, cancer, and types 1 and 2 diabetes at baseline 47. Dietary fat intake was assessed at baseline and updated every 2 to 4 years. Information on mortality was obtained from systematic searches of the vital records of states and the National Death Index, supplemented by reports from family members or postal authorities. Of the 126,233 participants who were followed up for as long as 32 years, the study found that higher intakes of saturated fat and trans-fat were associated with increased mortality, whereas higher intakes of polyunsaturated (PUFA) and monounsaturated (MUFA) fatty acids were associated with lower mortality. Replacing 5% of energy from saturated fats with equivalent energy from PUFA and MUFA was associated with reductions in total mortality of 27% and 13%, respectively 47.
People who replaced saturated fats with carbohydrates had only slightly lower mortality risk. In addition, replacing total fat with carbohydrates was associated with modestly higher mortality. This was not surprising, the authors said, because carbohydrates in the American diet tend to be primarily refined starch and sugar, which have a similar influence on mortality risk as saturated fats.
“Our study shows the importance of eliminating trans fat and replacing saturated fat with unsaturated fats, including both omega-6 and omega-3 polyunsaturated fatty acids. In practice, this can be achieved by replacing animal fats with a variety of liquid vegetable oils,” said senior author Frank Hu, professor of nutrition and epidemiology at Harvard Chan School and professor of medicine at Harvard Medical School.
This study is the most detailed and powerful examination to date on how dietary fats impact health. It suggests that replacing saturated fats like butter, lard, and fat in red meat with unsaturated fats from plant-based foods—like olive oil, canola oil, and soybean oil—can confer substantial health benefits and should continue to be a key message in dietary recommendations.
Meaning: Different types of dietary fat had different associations with mortality, the researchers found. Trans fats—on their way to being largely phased out of food—had the most significant adverse impact on health. Every 2% higher intake of trans fat was associated with a 16% higher chance of premature death during the study period. Higher consumption of saturated fats was also linked with greater mortality risk. When compared with the same number of calories from carbohydrate, every 5% increase in saturated fat intake was associated with an 8% higher risk of overall mortality.
Conversely, intake of high amounts of unsaturated fats—both polyunsaturated and monounsaturated—was associated with between 11% and 19% lower overall mortality compared with the same number of calories from carbohydrates. Among the polyunsaturated fats, both omega-6, found in most plant oils, and omega-3 fatty acids, found in fish and soy and canola oils, were associated with lower risk of premature death.
Is Saturated Fat Healthy?
Consuming high amounts of saturated fats linked to increased heart disease risk ! 42, 43, 44, 45
In a new study appearing online in the Journal of the American College of Cardiology, Dr. Frank Hu and colleagues found that people who replace saturated fat (primarily found in meats and dairy foods) with refined carbohydrates do not lower their risk of heart disease, whereas those who replace saturated fats with unsaturated fats or whole grains lower their heart disease risk 46.
Previous studies have shown that individual saturated fatty acids have different effects on blood lipids, but little is known about associations between individual saturated fatty acid intake and coronary heart disease risk. However, in a study that appeared online on 23rd November 2016, in The British Medical Journal 81, where the researchers analyzed data from 73,147 women involved in the Nurses’ Health Study between 1984 and 2012, and 42,635 men who were in the Health Professionals Follow-up Study between 1986 and 2010. Participants reported their diet and health status on questionnaires completed every four years. The study found that a higher intake of the most commonly consumed major saturated fatty acids—lauric acid, myristic acid, palmitic acid, and stearic acid—was associated with a 18% increased relative risk of coronary heart disease 81. This study dispels the notion that ‘butter is good’, said Dr. Hu the study co-author. Dr. Hu added, “individual saturated fatty acids share the same food sources, such as red meat, dairy, butter, lard, and palm oil. Therefore it is impractical to differentiate the types of saturated fatty acids in making dietary recommendations, an idea that some researchers have put forth. Instead, it is healthier to replace these fatty acids with unsaturated fats from vegetable oils, nuts, seeds, and seafood as well as high quality carbohydrates” 81. “Replacing sources of saturated fat in our diets with unsaturated fats is one of the easiest ways to reduce our risk of heart disease,” said Walter Willett, a co-author and professor of epidemiology and nutrition.
Replacing just 1% of daily consumption of these fatty acids with equivalent calories from polyunsaturated fats, whole grain carbohydrates, or plant proteins, was estimated to reduce relative coronary heart disease risk by 6%-8%. Replacing palmitic acid—found in palm oil, meat, and dairy fat—was associated with the strongest risk reduction.
A 2021 study with 114,285 participants has found a potential link between eating saturated fat from meat and developing heart disease 82. Over a median 8.5 years of follow-up, there were 4,365 total cardiovascular disease (heart and blood vessel disease), 3,394 coronary artery disease (a condition that occurs when the heart’s blood supply is reduced, depriving the heart muscle of oxygen and nutrients), and 1,041 stroke cases 82. However, there were no clear associations between total saturated fat and cardiovascular disease outcomes 82. The study found that consuming 5% higher total energy from saturated fat from meat was associated with 19% and 21% elevated risks of total cardiovascular disease and heart disease, respectively – but the associations did not remain significant after accounting for body mass index (BMI), because those consuming large amounts of meat also had a higher body mass index (BMI) than low consumers 82. The researchers also found that associations of saturated fat from dairy with heart disease went in the opposite direction, but this association was not clear after accounting for body mass index (BMI) suggesting that differences in body mass index (BMI) may be responsible, in part, for the association between cardiovascular disease and saturated fat from meat 82. It is also not possible to determine the why saturated fat from meat and saturated fat from dairy have different effect on cardiovascular disease because those with a higher body mass index (BMI) consume more meat or because of cholesterol-lowering medication use 82. The researchers concluded that further research is needed to ensure that these observations were not influenced by dietary or non-dietary factors that were not measured in this study 82.
However, there are meta-analyses that have not found an association between dietary saturated fat intake and heart and blood vessel disease 83, 84, 85, 86, 87, 88, 89. A possible explanation for this difference is whether the saturated fat in the diet is replaced by polyunsaturated fatty acids (PUFA) vs. replaced by carbohydrate. When saturated fat is replaced by polyunsaturated fatty acids (PUFA) there is a reduction in heart and blood vessel disease whereas replacement with carbohydrate has no benefit on heart and blood vessel disease 90, 91, 92, 93, 94. However, replacement of saturated fat with high quality carbohydrate may be beneficial 92, 93, 94. Additionally, in one study saturated fat from meat was associated with an increased risk of heart and blood vessel disease while saturated fat from dairy products was associated with a decrease in heart and blood vessel disease 95. Therefore, the source of saturated fat may be important.
A 2022 study adds evidence that saturated fat from dairy sources may be beneficially associated with HDL “good” cholesterol but more evidence is needed 96. In this study, the researchers found that higher mean intakes of saturated fat from dairy sources over 8 years were associated with lower levels of body fat in females 96. After accounting for differences in body fat and other risk factors among males, higher mean intakes of saturated fat from dairy sources were associated with a less atherogenic risk profile, including less inflammation, higher concentrations of HDL cholesterol, lower triglyceride (TG) concentrations, and a lower triglyceride (TG):HDL ratio 96. Furthermore, males in higher quintiles of saturated fat intake from dairy sources had higher HDL particle concentrations, lower very-low-density lipoprotein (VLDL), and larger HDL and LDL particle sizes. Very-low-density lipoprotein (VLDL) carries triglycerides (TG) to tissues, and is sometimes called a “bad” cholesterol because it can contribute to plaque buildup in your arteries. No such associations with lipids or inflammatory biomarkers were observed among females for intakes of dairy-derived saturated fats. Saturated fat from nondairy sources in females was inversely associated with the TG:HDL ratio 96. The study concluded that males with higher intakes of dairy-derived saturated fats had a less atherogenic profile than males with lower intakes of dairy-derived saturated fats 96. These effects were weaker in females. Nondairy saturated fats were not associated with these cardiometabolic outcomes 96.
Figure 13. Dietary Fats and Heart Disease Risk
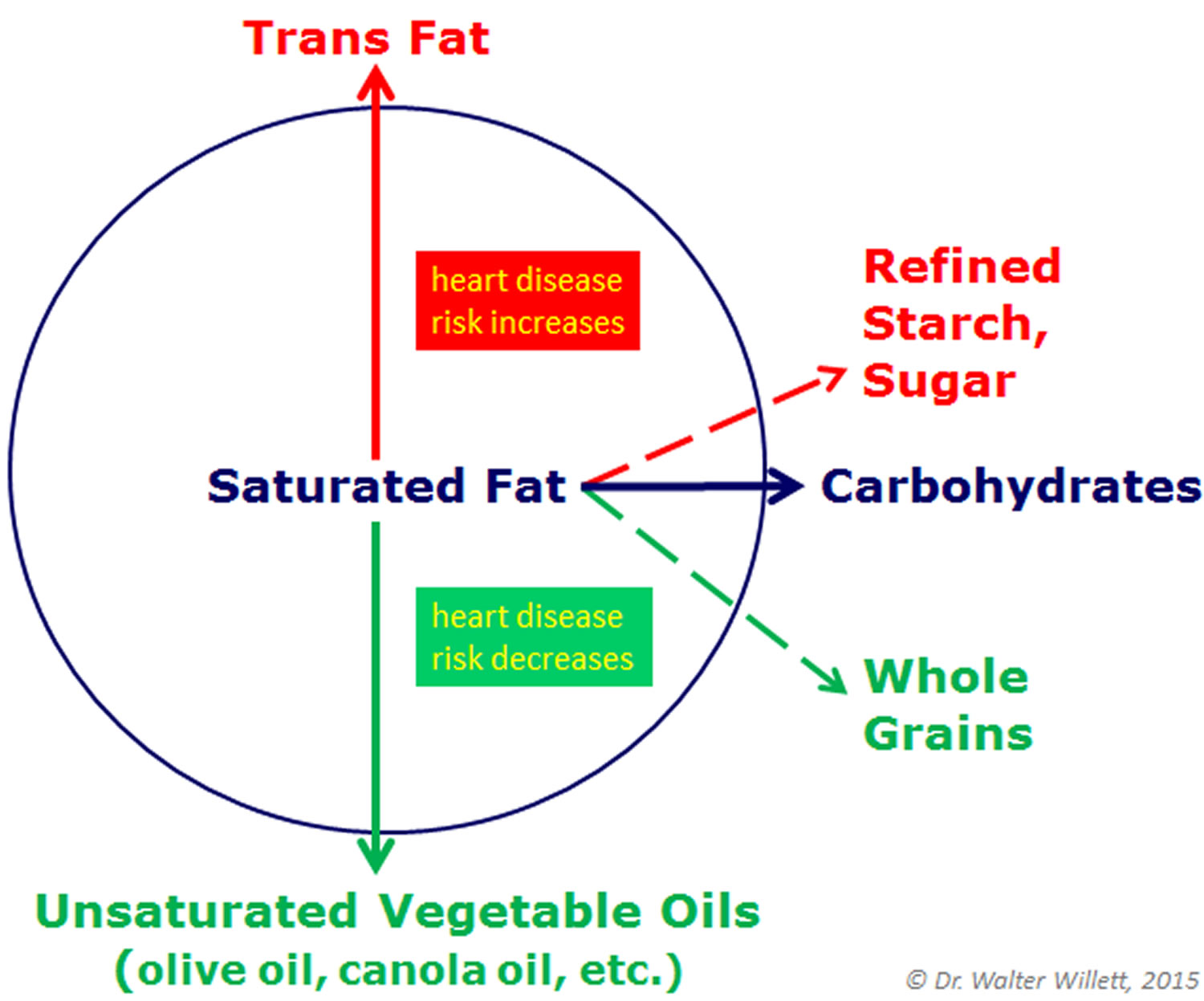
These findings support current dietary recommendations to replace saturated fat and trans-fat with unsaturated fat.
- Scientists concluded that saturated fat should be no more than 5 percent to 6 percent of daily calories. So, for a diet of 2,000 calories a day, that would mean no more than 120 of them should come from saturated fats. That’s about 13 grams of saturated fats a day 48.
There’s a lot of conflicting information about saturated fats. Should you eat them or not?
Saturated fats are bad for your health in several ways:
- Heart disease risk. Your body needs healthy fats for energy and other functions. But too much saturated fat can cause cholesterol to build up in your arteries (blood vessels). Saturated fats raise your LDL, or bad, cholesterol. High LDL cholesterol increases your risk for heart disease and stroke.
- Weight gain. Many high-fat foods such as pizza, baked goods, and fried foods have a lot of saturated fat. Eating too much fat can cause you to gain weight. All fats contain 9 calories per gram of fat. This is more than twice the amount found in carbohydrates and protein.
Cutting out high-fat foods can help keep your weight in check and keep your heart healthy. Staying at a healthy weight can reduce your risk of diabetes, heart disease, and other health problems.
The most recent American Heart Association and American College of Cardiology advisory 48, reaffirms that longstanding advice. Here are some of the scientific highlights:
- Randomized controlled trials that lowered intake of dietary saturated fat and replaced it with polyunsaturated vegetable oil reduced cardiovascular disease by about 30 percent – similar to results achieved by some cholesterol-lowering drugs known as statins 97.
- Prospective observational studies in many populations showed that a lower intake of saturated fat with a higher intake of polyunsaturated and monounsaturated fat is associated with lower rates of cardiovascular disease 57.
- Several studies found that coconut oil – which is predominantly saturated fat but has been widely touted recently as healthy – raised LDL cholesterol to the same degree as other saturated fats found in butter, beef fat, ghee and palm oil.
- Replacing saturated fat with mostly refined carbohydrate and sugars does not lower rates of heart disease, but replacing these fats with whole grains is associated with lower rates. This indicates that saturated fat and refined carbohydrate are equally bad relative to heart disease risk.
Saturated fats are found in all animal foods, and some plant sources.
The following foods are high in saturated fats. Many of them are also low in nutrients and have extra calories from sugar:
- Baked goods (cake, doughnuts, Danish)
- Fried foods (fried chicken, fried seafood, French fries)
- Fatty or processed meats (bacon, sausage, chicken with skin, cheeseburger, steak)
- Whole-fat dairy products (butter, ice cream, pudding, cheese, whole milk)
- Solid fats such as coconut oil, palm, and palm kernel oils (found in packaged foods)
Here are some examples of popular food items with the saturated fat content in a typical serving:
- 12 ounces (oz), or 340 g, steak — 20 g
- 12 oz (340 g) cream of mushroom soup — 22 g
- Cheeseburger — 10 g
- Vanilla shake — 8 g
- 1 tablespoon (15 mL) butter — 7 g
It is fine to treat yourself to these types of foods once in a while. But, it is best to limit how often you eat them and limit portion sizes when you do.
Foods high in saturated fat
Saturated fats occur naturally in many foods. Most come from animal sources, including meat and dairy products, as well as tropical fats such as coconut, palm and palm kernel.
Examples of foods with saturated fat are:
- Beef
- Lamb
- Pork
- Poultry, especially with skin
- Beef fat (tallow)
- Lard and cream
- Butter
- Lard
- Ghee
- Suet
- Cheese
- Ice cream
- Coconut and coconut oil
- Palm oil
- Palm kernel oil
- Some baked and fried foods
- Processed and fatty meats like sausages, ham, burgers and bacon.
- Whole milk, cream and ice cream.
Are there “good” saturated fats?
Some research suggests that different types of saturated fat can have different effects on your risk of heart and blood vessel disease. For example, a previous analysis in the Nurses’ Health Study, reported that intake of major saturated fatty acid (long-chain fatty acid [LCFA] and medium-chain fatty acid [MCFA]), including lauric (12:0), myristic (14:0), palmitic (16:0), and stearic (18:0), had an increased risk of coronary heart disease, whereas the sum of short-chain fatty acid (SCFA) such as butyric acid (4:0), caproic acid (6:0), caprylic acid (8:0), and capric acid (10:0) did not have an association with increased coronary heart disease risk 98, 99, 100, 101. But that doesn’t mean these foods are healthy – all foods contain a range of different saturated fatty acids. The visible fat on meat and in processed meat does contain saturated fats known to increase cholesterol levels. Processed meat is also often high in salt, which can raise your blood pressure, a risk factor for heart attack and stroke. And most of the chocolate you eat is high in added sugar and fat. Eating too much can lead to weight gain, which will also increase your risk of many health conditions.
At present, there isn’t enough evidence to choose one saturated fat over another – it’s better to swap them for oily fish, vegetable oils or nuts.
I’ve heard that grass-fed beef contains healthy fat, is this true?
Grass-fed beef generally comes from cattle that eat only grass and other foraged foods whereas conventional beef cattle often eat a diet that includes grains, such as corn. Although grass-fed beef is said to be leaner and contain more of the healthy polyunsaturated fats such as omega-3 fatty acids, there is limited long-term research to prove grass-fed beef is better for you. We do not recommend grass-fed or organic meat over other meats. If you are going to eat red meat, the most important thing is to choose the leanest type so you can limit the amount of saturated fat you eat.
What about coconut oil, isn’t that the healthy type of saturated fat?
Coconut oil, with its sweet smell of the tropics and its purported claims to cure what illness you have, is being heavily promoted 102. People are using coconut oil in their shampoos, skin creams, and even in their smoothies and coffee. Coconut oil is about 86 per cent saturated fat, about one-third more saturated fat than butter (at 54 per cent). Saturated fatty acids in coconut oil is mostly lauric acid (12:0) at 45 to 56 percent, myristic acid (14:0) at 16 to 21 percent, and palmitic acid (16:0) at 7.5 to 10.2 percent. Lauric acid is a saturated fatty acid (SFA) with a structure that is C12 : 0, classifying it as a medium-chain fatty acid (MCFA) 103, 104. One tablespoon of coconut oil adds up to more than 11 grams of saturated fats, according to the federal National Nutrient Database. That’s nearly the total daily limit of 13 grams recommended by the American Heart Association. Studies have shown coconut oil raises LDL “bad” cholesterol as much as butter, beef fat or palm oil. A new science advisory from the American Heart Association recommended against consuming coconut oil 105. The advisory, an analysis of more than 100 published research studies dating as far back as the 1950s, reaffirmed that saturated fats raise LDL “bad” cholesterol 105. Tropical vegetable oils such as coconut oil contain high levels of saturated fats, and the authors reported that coconut oil raised LDL “bad” cholesterol in seven controlled trials 105. The paper pointed out there are great benefits to replacing saturated fats such as coconut oil, butter, beef fat or palm oil with healthier, polyunsaturated fats. Some studies have even suggested that this could help lower cardiovascular disease risk as much as cholesterol-lowering statin drugs, the authors noted 105.
In 2014, the Academy of Nutrition and Dietetics position paper on dietary fatty acids concluded that coconut oil is not currently recommended for consumption and that additional peer-reviewed literature is needed before any statements about its health benefits are made. In a recent comprehensive review of 15 randomized controlled trials (RCTs) in humans, the authors concluded that coconut oil consumption increased total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C), and that removing coconut oil from the diet reduced total cholesterol and low-density lipoprotein cholesterol (LDL-C) with variable effects on high-density lipoprotein cholesterol (HDL-C). The specific type of coconut oil used in these trials is not known.
However, there has been speculation that some of the saturated fatty acid in coconut oil, lauric acid, may be better for us than other saturated fats. But so far there are no quality studies to indicate that coconut oil has the edge over polyunsaturated or monounsaturated oils that we know are better for us, like rapeseed or olive oil. If you like the taste of coconut oil, then, as with butter, it is fine to use it every now and then. However, be careful not to overdo it, and use unsaturated oils as an everyday choice instead.
Because the saturated fat in coconut oil is largely composed of the medium-chain triglyceride (MCT) 12:0, this differentiates coconut oil from other saturated fat food sources, such as lard and beef tallow. These MCTs, which are made up of fatty acids that are six, eight, 10, or 12 carbons in length (6:0, 8:0, 10:0, and 12:0, respectively), are transported directly from the intestinal tract through the portal vein to the liver and primarily are used as an immediate source of energy. This is considered beneficial as a higher rate of fatty acid oxidation in the liver is thought to reduce the accumulation of lipid in adipocytes. Medium chain triglycerides (MCT) enhance thermogenesis and may reduce food intake 106. Dr St-Onge, an associate professor of nutritional medicine at Columbia University, conducted research that showed a type of fat in coconut oil, medium-chain triglycerides (MCTs), can increase metabolism and boost weight loss 107, 106, 108. St-Onge’s study reported that medium-chain triglycerides (MCTs) are processed by the body differently than other dietary fats. In addition to higher saturated fat content, St-Onge noted that coconut oil has a higher proportion of these than most other fats or oils 106, 108. However, she said, many people tend to overlook an important catch in her research. The oil she used in her study was a special 100 percent medium-chain coconut oil. Most coconut oils typically have 13 percent to 14 percent of this medium-chain triglyceride, she said. So, people would have to eat large quantities to replicate the results 106, 108.
Aren’t nuts and olives healthy, do I have to worry about the saturated fat in those?
Nuts have a high fat content, so are high in energy (calories). In most nuts, the fat is mostly unsaturated fats: either polyunsaturated fats (walnuts and pine nuts) or monounsaturated fats (almonds, pistachios, pecans, peanuts and hazelnuts). There are some exceptions. Brazil nuts, cashews and macadamia nuts are higher in saturated fat, so only eat them occasionally. Chestnuts are lower in all types of fat and higher in starchy carbohydrate than other nuts. Nuts (apart from chestnuts) are also high in protein, making them a satisfying snack.
Olives are also high in monounsaturated fats, and compared with nuts they contain fewer calories, though they are high in salt. One olive contains about 5 kcal (5000 calories), while a pecan contains 14 kcal (14,000 calories). As a substitute for foods high in saturated fat and sugar, such as biscuits, chocolates or cakes, olives or unsalted nuts can be a healthy snack choice. But watch your portion size to avoid consuming too much salt or fat, and choose unsalted nuts where possible.
Do I have to completely remove saturated fat from my diet?
It’s almost impossible to completely remove saturated fat from your diet. Instead, keep an eye on how often you eat foods high in saturated fat, watch your portion size and substitute for healthier options where possible. All fats are a combination of saturated fatty acids and monounsaturated fatty acids (MUFAs) and polyunsaturated fatty acids (PUFAs). They tend to be classified by the fat that makes up the largest percentage. Olive oil is mostly monounsaturated (73 per cent), but still contains saturated fat (14 per cent), while butter is mostly saturated fat (54 per cent) but still contains monounsaturated fat (20 per cent).
What’s my daily limit for foods with saturated fats?
The American Heart Association recommends aiming for a dietary pattern that achieves 5% to 6% of calories from saturated fat.
For example, if you need about 2,000 calories a day, no more than 120 of them should come from saturated fats.
That’s about 13 grams of saturated fats a day.
How to eat less saturated and trans fats
The American Heart Association 109 recommends that adults who would benefit from lowering LDL cholesterol reduce their intake of trans fat and limit their consumption of saturated fat to 5 to 6 percent of total calories.
Are all foods labeled “trans fat-free” healthy foods ?
Not necessarily. Foods labeled “0 trans fat” or cooked with “trans fat-free” oils may contain a lot of saturated fats, which raise your bad cholesterol levels. “Trans fat-free” foods may also be unhealthy in terms of their general nutrient content. For example, baked goods also tend to be high in added sugars and low in nutrients.
Here are some ways to eat less saturated and trans fats:
- Eat a dietary pattern that emphasizes fruits, vegetables, whole grains, low-fat dairy products, poultry, fish and nuts. Also limit red meat and sugary foods and beverages.
- Use naturally occurring unhydrogenated vegetable oils such as canola, safflower, sunflower or olive oil most often.
- Look for processed foods made with unhydrogenated oil rather than partially hydrogenated or hydrogenated vegetable oils or saturated fat.
- Use soft margarine as a substitute for butter, and choose soft margarines (liquid or tub varieties) over harder stick forms. Look for “0 g trans fat” on the Nutrition Facts label.
- Doughnuts, cookies, crackers, muffins, pies and cakes are examples of foods high in trans fat. Don’t eat them often.
- Limit commercially fried foods and baked goods made with shortening or partially hydrogenated vegetable oils. These foods very high in fat, and it’s likely to be trans at.
- Limit fried fast food. Commercial shortening and deep-frying fats are still made by hydrogenation and contain saturated fat and trans fat.
What are alternatives to replace saturated fats in the foods you eat ?
To get the nutrients you need, eat a dietary pattern that emphasizes:
- fruits, vegetables,
- whole grains,
- low-fat dairy products,
- poultry, fish and nuts,
- while limiting red meat and sugary foods and beverages.
Choose lean meats and poultry without skin and prepare them without added saturated and trans fat.
You should replace foods high in saturated fats with foods high in monounsaturated and/or polyunsaturated fats. This means eating foods made with liquid vegetable oil but not tropical oils. It also means eating fish and nuts. You also might try to replace some of the meat you eat with beans or legumes.
3) Bad Fats (Trans Fat or Hydrogenated Oils)
The worst type of dietary fat is the kind known as trans fat. The right amount of trans fats is zero ! These fats have no nutritional value and we know for certain they are bad for heart health. Trans fats increase LDL cholesterol and triglyceride levels while reducing levels of HDL cholesterol. The trans fats also known as hydrogenated oils because the trans fats come from vegetable oils that were chemically modified so they are solid like butter. The solidifying process – called hydrogenation – that is used to turn healthy oils into solids and to prevent them from becoming rancid. When vegetable oil is heated in the presence of hydrogen and a heavy-metal catalyst such as palladium, hydrogen atoms are added to the carbon chain. This turns oils into solids. It also makes healthy vegetable oils more like not-so-healthy saturated fats. On food label ingredient lists, this manufactured substance is typically listed as “partially hydrogenated oil” in order to extend the shelf life of food, but it also turns polyunsaturated oils into a kind of man-made cholesterol. Trans fats can increase your level of “bad” LDL cholesterol and may increase your risk of heart disease. What’s more, these man-made fats are taken up by the body much easier than are omega-3s. So trans fatty acids not only harm your health, they also block the absorption of healthy fats.
Because these oils don’t spoil as quickly as butter, they are used in most packaged cookies, chips, crackers and other baked goods sold in the supermarket, as well as in margarines. Trans Fat (Hydrogenated Oils) are found in most processed food, including margarine, potato chips, baked goods, cookies, pastries to fast-food French fries, etc. They are toxic, blocking absorption of essential fatty acids and eating foods rich in trans fats increases the amount of harmful LDL cholesterol in the bloodstream and reduces the amount of beneficial HDL cholesterol. Trans fats create inflammation, which is linked to heart disease, stroke, diabetes, and other chronic conditions. They contribute to insulin resistance, which increases the risk of developing type 2 diabetes. Research from the Harvard School of Public Health and elsewhere indicates that trans fats can harm health in even small amounts: for every 2% of calories from trans fat consumed daily, the risk of heart disease rises by 23%.
The American Heart Association recommends limiting your trans fat daily consumption to less than 1 percent.
Trans fats have no known health benefits and that there is no safe level of consumption. Recently, the FDA banned trans fats from the U.S. food supply. The phasing-out process is expected to take three years. The encouraging news is that many major food suppliers and restaurants have already substituted healthier fats for trans fats. Today, these mainly man-made fats are rapidly fading from the food supply.
The consumption of trans fats has been directly linked to an increase in coronary heart disease. Trans fats appear to have a detrimental effect on serum lipids by increasing LDL “bad” cholesterol and triglyceride levels, and reducing high-density (HDL “good”) lipoprotein cholesterol levels 110, 111, 112, 113, 114. Studies have shown that substituting 2 percent of total energy intake with trans-fatty acids is associated with a 14 to 36 percent increase in the incidence of coronary artery disease (Table 2) 115, 116, 117, 118. Observational data from the Nurses’ Health Study suggests that replacing 5 percent of energy from saturated fat with energy from unsaturated fats could reduce the risk of coronary heart disease by 42 percent; however, replacing only 2 percent of energy from trans fats with energy from non-hydrogenated, unsaturated fats could reduce the risk of coronary heart disease by 53 percent 115.
Table 2. Trans Fat Consumption and Coronary Heart Disease
| Study | Number of patients | Years of follow-up | Relative risk of coronary heart disease with trans-fat consumption* |
|---|---|---|---|
| Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study 116 | 21,930 men who smoke | 6.1 | 1.14 |
| Zutphen Elderly Study 114 | 667 men | 10 | 1.28 |
| Health Professionals Follow-up Study 117 | 43,757 men | 6 | 1.36 |
| Nurses’ Health Study 115 | 80,082 women | 14 | 1.33 |
Footnote: * For each isocaloric substitution of 2 percent of total energy intake with trans-fatty acids
Abbreviation: CHD = coronary heart disease
[Source 119 ]How Much Good Fats Do You Really Need?
In 1999, the International Society for the Study of Fatty Acids and Lipids agreed upon a recommendation table on daily intake of fatty acids as a foundation for further discussions 3. Polyunsaturated fatty acids (PUFAs) with 18 carbon (C18) atoms such as linoleic (18:2 ω-6), and α-linolenic (18:3 ω-3) are known as essential fatty acids in human nutrition 37. These fatty acids, although regarded as an indispensable component for cell structure and development and function, cannot be synthesized by the human body. Nutritionists recommend a balanced lipid intake corresponding to a total amount of fats equal to 25 to 30% of total calories with a ratio in fatty acids as follows: 1-Saturates (6–8%), 2-Monounsaturates (12–14%), 3- Polyunsaturates as a ω-6 (6–7%), and 4-Polyunsaturates as a ω-3 (0.5–1.5%) 38. The American Heart Association recommends aiming for a dietary pattern that achieves 5% to 6% of calories from saturated fat 39. Saturated fatty acids increase plasma cholesterol level and acts as “promoters” of certain cancer development (e.g., colon, breast, and perhaps uterus and prostate).
Adequate intake levels for adults were specified with respect to α-linolenic acid (ALA or Omega-3 fatty acid 18:3ω-3), eicosapentaenoic acid (EPA or Long Chain Omega-3 fatty acid 20:5ω-3), docosahexaenoic acid (DHA or Long Chain Omega-3 fatty acid 22:6ω-3), as well as upper limits for linoleic acid (LA or Omega-6 fatty acids), trans-fatty acids, and saturated, given as % of total energy content, respectively. Given a total fat range from 15% to 40% of total energy content, there is no precise value (i.e., % of total energy content in the form of MUFA) was given by the panel 40. According to the Joint FAO/WHO Expert Consultation Committee, MUFA intakes should be determined by calculating the difference: MUFA (% of total energy content) = total fat (% of total energy content) − SFA (% of total energy content) − PUFA (% of total energy content) − TFA (% of total energy content). Accordingly, MUFA intakes (% of total energy content) will range with respect to the total fat and fatty acid composition of the diet 41.
The debate continues on the optimal dietary fatty acid composition, but the evidence supporting Monounsaturated Fatty Acid (MUFA) as the healthy dietary fatty acid is weak. Even when considering the food source of MUFA (plant vs animal), there is little evidence to support recommendations to increase dietary MUFA for coronary heart disease prevention. However, since no detrimental effects of MUFA-rich diets were reported in the literature to date, there is no evidence speaking against the consideration of MUFAs in dietary guidelines. Further studies dealing with long-term effects of MUFA on biomarkers of obesity, diabetes, and cardiovascular diseases as well as clinical endpoints are needed to clarify the potential benefits of MUFA-rich diets in primary and secondary prevention.
On the other hand, increasing dietary Polyunsaturated Fatty Acid (PUFA) consistently appears to provide benefit. A considerably larger number of meta-analyses explored the effects of Polyunsaturated Fatty Acids (PUFAs) on maintenance or reduction of body weight as well as biomarkers of impaired glucose metabolism or cardiovascular disease or coronary heart disease than there are systematic reviews and meta-analyses dealing with the corresponding impact of Monounsaturated Fatty Acids (MUFAs). Consequently, the international recommendations for Polyunsaturated Fatty Acid (PUFA) are more consistent than those for MUFA, averaging a value of 10% of total energy content for healthy persons for the most part. If MUFA recommendations are given at all, they vary between 12% and 25% of total energy content, equaling a remarkable range of ~30–70 g/day for a 2.500 kcal-diet. Prestigious authorities and organizations such as the National Institute of Medicine, the EFSA, the USDA and the ADA do not provide specific recommendation for MUFAs either for healthy people or for patients in need of diabetic or cardiovascular management.
Most of us get too much fat, and too much unhealthy fat. Most experts recommend that we get 30% of our calories from good fat, although we can survive fine on as little as 20%, even 10%. If you’re like most of us, you’re getting plenty of fat – most Americans consume about 40% of their calories from fats in meat, butter, cheese, baked goods, etc.
To make the switch to heart-healthy fats, start by avoiding the truly unhealthy fats – trans fatty acids. These trans fats come from vegetable oils that were chemically modified so they are solid like butter. Because these oils don’t spoil as quickly as butter, they are used in most packaged cookies, chips, crackers and other baked goods sold in the supermarket, as well as in margarines.
Summary
- Decreased saturated fatty acid intake decreases blood total cholesterol and LDL cholesterol concentrations.
- Replacement of saturated fatty acids with polyunsaturated and/or monounsaturated fatty acids decreases blood total cholesterol and LDL cholesterol concentrations.
- Most of us eat too much fat, and too much unhealthy fat. Most experts recommend that we get 30% of our calories from good fat, although we can survive fine on as little as 20%, even 10%. If you’re like most of us, you’re getting plenty of fat – most Americans consume about 40% of their calories from fats in meat, butter, cheese, baked goods, etc.
Conclusion
Different types of dietary fat had different associations with mortality, the researchers found. Trans fats—on their way to being largely phased out of food—had the most significant adverse impact on health. Every 2% higher intake of trans fat was associated with a 16% higher chance of premature death during the study period. Higher consumption of saturated fats was also linked with greater mortality risk. When compared with the same number of calories from carbohydrate, every 5% increase in saturated fat intake was associated with an 8% higher risk of overall mortality.
Conversely, intake of high amounts of unsaturated fats—both polyunsaturated and monounsaturated—was associated with between 11% and 19% lower overall mortality compared with the same number of calories from carbohydrates. Among the polyunsaturated fats, both omega-6, found in most plant oils, and omega-3 fatty acids, found in fish and soy and canola oils, were associated with lower risk of premature death.
Because fat is an essential nutrient to give your body energy, help your body absorb some nutrients and produce important hormones and to support cell growth. Eating foods with fat is definitely part of a healthy diet. A healthy diet can include the foods you love. You don’t have to avoid treats entirely, but you do need to eat less of foods that are low in nutrition and high in calories.
Just remember to choose foods that provide good fats (monounsaturated and polyunsaturated fats) and balance the amount of calories you eat from all foods with the amount of calories you burn. Whether it is olive oil, ghee, butter or coconut oil — they are all 100 percent fat. All fat have calories.
All fats, whether good or bad, no matter how good the oil sounds — remember that it is still a fat, with 120 calories per tablespoon. Consuming a high fat diet may lead to becoming overweight and that is not healthy !
Aim to eat a dietary pattern that emphasizes intake of vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, non-tropical vegetable oils and nuts; and limits intake of sodium, sweets, sugar sweetened beverages and red meats. Doing so means that your diet will be low in both saturated fats and trans fats.
While you switch to a heart-healthy diet you may need to keep tabs on your calorie intake for a while.
How to Make Healthy Lifestyle and Eating Choices
It’s the overall eating pattern of your life choices that counts. Here are some tips for making healthy lifestyle and eating choices:
- Balance calorie intake (Calorie IN) with calorie needs (Calorie OUT) to achieve and maintain a healthy weight. Start by knowing how many calories you should eat and drink to maintain your weight. You may need fewer or more calories depending on several factors including age, gender and level of physical activity. Increase the amount and intensity of your physical activity to burn more calories. Aim for at least 150 minutes of moderate physical activity or 75 minutes of vigorous physical activity (or an equal combination of both) each week. Ideally, your activity should be spread throughout the week. Regular physical activity can help you maintain your weight, keep off weight that you lose and reach physical and cardiovascular fitness. If it’s hard to schedule regular exercise, look for ways to build short bursts of activity into your daily routine such as parking farther away and taking the stairs instead of the elevator.
- Don’t smoke, vape or use tobacco or nicotine products — and avoid secondhand smoke or vapor.
- Limit salt, sugar, animal fat, processed foods and alcohol.
- Eat a variety of foods. Eat a variety of foods from each of the five food groups daily. Healthy choices include fruits, vegetables, whole grains, protein foods, and fat-free or low-fat dairy. Foods are grouped together because they provide similar amounts of key nutrients. For example, key nutrients of the milk, yoghurt, cheese and alternatives group include calcium and protein, while the fruit group is a good source of vitamins, minerals, antioxidants. As a bonus, choosing a variety of foods will help to make your meals interesting, so that you don’t get bored with your diet.
- Eat fruit instead of drinking it. Eating fruit is linked to a reduced risk of several health conditions, but fruit juices are more likely to spike blood sugar levels.
- Add healthy fats. Healthy fats like monounsaturated and polyunsaturated fats can help lower cholesterol and protect your heart. You can find healthy fats in foods like olive oil, nuts, avocados, and some types of fish.
- Drink water. Sipping water throughout the day can help keep you full and hydrated. Sometimes thirst is mistaken for hunger.
- Reduce added sugar. Too much added sugar in your diet can contribute to weight gain, obesity, type 2 diabetes, and heart disease.
- Chew your food well. Chewing your food well can help you make healthier food choices.
- Sit at the table to eat. Sitting at the table to eat can help you focus on your food and internal cues for hunger or fullness.
To lose weight you’ll need to start with finding a way to eat fewer calories than you need. A calorie is a unit of energy, which is in the foods and drinks you consume. Scientifically, the calorie (a unit of energy) was originally defined as the amount of heat required at a pressure of 1 standard atmosphere to raise the temperature of 1 gram of water 1° Celsius. When you hear something contains 100 calories, it’s a way of describing how much energy your body could get from eating or drinking it. However, since calories are too small of a measurement to use when discussing nutrition and exercise, kilocalorie (kcal) measurements are used instead and the term is interchangeable with calories. Kilocalorie (kcal) is a unit of measurement for energy that is equivalent to 1,000 calories. Also,1 kcal or 1 kilocalorie is equivalent to 1 large Calorie (with an uppercase C) or 1,000 calories.
Some countries use kilojoules (kJ) to measure how much energy people get from consuming a food or drink.
- 1 calorie = 4.184 joule
- 1 kilocalorie (kcal) = 4.184 kilojoules (kJ)
- 1 Calorie (1,000 calories) = 4.184 kilojoules (kJ)
Here’s how many calories are in your foods and drinks 29:
- 1 gram of carbohydrate = 4 calories
- 1 gram of protein = 4 calories
- 1 gram of fat = 9 calories
- 1 gram of water = 0 calorie
Most foods and drinks contain calories. You can find out how many calories are in a food by looking at the nutrition facts label. The label also will describe the components of the food such as how many grams of carbohydrate, protein, and fat it contains.
That means if you know how many grams of each one are in a food, you can calculate the total calories. You would multiply the number of grams by the number of calories in a gram of that food component. For example, if a serving of potato chips (about 20 chips) has 10 grams of fat, 90 calories are from fat. That’s 10 grams x 9 calories per gram. Some foods, such as lettuce, contain few calories (1 cup of shredded lettuce has less than 10 calories). Other foods, like peanuts, contain a lot of calories (½ cup of peanuts has 427 calories).
Being overweight or obese is the result of an energy imbalance between your daily energy intake and your energy expenditure resulting in excessive weight gain 120. The amount of energy or calories you get from food and drinks (energy IN) is balanced with the energy your body uses for things like breathing, digesting, and being physically active (energy OUT):
- The same amount of energy IN and energy OUT over time = weight stays the same (Energy Balance)
- More energy IN than OUT over time = Weight Gain
- More energy OUT than IN over time = Weight Loss
In order to lose weight, energy expenditures must exceed energy intake. To lose weight, most people need to reduce the number of calories they get from food and beverages (energy IN) and increase their physical activity (energy OUT). To achieve this imbalance, you can decrease energy intake, increase energy expenditures or combine a decrease in intake with an increase in expenditures. Being physically active and eating fewer calories will help you lose weight and keep the weight off over time. As a result, most weight loss recommendations advise combining a low caloric diet with an exercise program in order to achieve a significant energy deficit 121. A long-standing consistent observation is that regular exercise by itself is prescribed in small to moderate amounts resulting in modest weight loss or in some cases weight gain 122.
How many calories do I need per day?
The total number of calories you need each day varies depends on a number of factors, namely your age, sex, height, weight, level of physical activity, and pregnancy or lactation status. According to the Dietary Guidelines for Americans, American female adult estimated calorie needs range from 1,600 to 2,400 calories per day and for males 2,000 to 3,000 calories per day 123. The average, healthy, adult, American male consumes approximately 2,800 calories per day, and the average female about 1,800 calories 33. But most people need different amounts of calories based on how their bodies work, how active they are and any weight management goals. And if you want to lose weight you’ll have to reduce your calorie intake.
Here is a general estimate of calories you need each day:
- Sedentary lifestyle (little to no exercise)
- Women: 1,800 to 2,400 calories
- Men: 2,200 to 3,000 calories
- Moderately active lifestyle (engages in moderate exercise/physical activity like walking or light yard work:
- Women: 2,000 to 2,600 calories
- Men: 2,400 to 2,800 calories
- Very active lifestyle (engages in hard exercise/physical activity, or has a physically demanding job):
- Women: 2,200 to 2,800 calories
- Men: 2,800 to 3,200 calories
These are just general guidelines. It’s essential to consult with a nutritionist or a doctor who can give personalized advice based on your specific situation. Remember, it’s not just the quantity but also the quality of calories that matters for overall health.
Obesity results from the accumulation of excessive body fat, which is stored as adipose tissue. An energy deficit of approximately 3,500 calories is required to lose one pound of fat. However, there are several factors that can influence this particular number. These include compensatory changes in your resting metabolism (basal metabolic rate [BMR]), the energy cost of work, and discretionary physical activity, which can sometimes alter this figure by 100 to 200 calories. Your basal metabolic rate (BMR) also known as resting metabolic rate (RMR) is the number of calories your body burns while performing basic life-sustaining functions, such as breathing and keeping your heart beating. Your basal metabolic rate (BMR) is typically between 1,000 and 2,000 calories per day.
How to calculate calories you need for weight loss
You can calculate your basal metabolic rate (BMR) or resting metabolic rate (RMR) using the Mifflin-St Jeor equation 124, which is considered more accurate than the Harris-Benedict equation, especially for lean people. According to the Academy of Nutrition and Dietetics Evidence Analysis Library (EAL), the Mifflin-St. Jeor equation accurately predicted resting metabolic rate (RMR) using actual body weight within +/- 10% of measured RMR in 70% of obese individuals 125. Of the remaining 30%, 9% were overestimations and 21% were underestimations. The individual error range was a maximum overestimate of 15% to a maximum underestimate of 20%” 126. While the Harris-Benedict and WHO equations are often used in clinical practice with reasonable accuracy, results have been mixed regarding their applications to individuals who are overweight or obese 33.
The Mifflin-St Jeor formula for calculating your basal metabolic rate (BMR) or resting metabolic rate (RMR):
- Males Basal metabolic rate [BMR] (kcal/day) = (10 X weight in kilograms) + (6.25 X height in centimeters) – (5 X age in years) + 5 (kcal/day)
- Females Basal metabolic rate [BMR] (kcal/day) = (10 X weight in kilograms) + (6.25 X height in centimeters) – (5 X age in years) – 161 (kcal/day)
You can also use the free online Basal Metabolic Rate (BMR) calculator here: https://www.nasm.org/resources/calorie-calculator
Or the Body Weight Planner (https://www.niddk.nih.gov/health-information/weight-management/body-weight-planner).
The Body Weight Planner allows you to make personalized calorie and physical activity plans to reach a goal weight within a specific time period and to maintain it afterwards.
The Basal Metabolic Rate (BMR) calculator factor in your activity levels, overall goals, and calorie usage to help you craft a weight-loss plan.
Once you have found your basal metabolic rate (BMR), multiply your BMR by your Physical Activity Levels to provide a baseline daily caloric level for weight maintenance:
- Sedentary (light physical activity associated with typical day-to-day life) = 1
- Low Active (walking about 1.5 to 3 miles per day at 3 to 4 miles per hour, in addition to the light physical activity associated with typical day-to-day life), For males = 1.11 and females = 1.20
- Active (walking more than 3 miles per day at 3 to 4 miles per hour, in addition to light physical activity associated with typical day-to-day life: 60 minutes of at least moderate intensity physical activity). For males = 1.25 and females = 1.27
- Very Active (walking more than 7.5 miles per day at 3 to 4 miles per hour, in addition to light physical activity associated with typical day-to-day life: 60 minutes of at least moderate to vigorous intensity physical activity). For males = 1.48 and females = 1.45
Your Total Daily Energy Expenditure (TDEE) gives you the estimated number of calories you need to maintain your current weight based on your activity level.
To find your Total Daily Energy Expenditure (TDEE) multiply your Basal Metabolic Rate (BMR) by your Physical Activity Levels
For example:
- Sedentary (little to no exercise): BMR x 1
- Lightly active (walking about 1.5 to 3 miles per day at 3 to 4 miles per hour, in addition to the light physical activity associated with typical day-to-day life): BMR x For males = 1.11 and females = 1.20
- Moderately active (moderate exercise/sports 3-5 days/week): BMR x 1.55
- Very active (walking more than 7.5 miles per day at 3 to 4 miles per hour, in addition to light physical activity associated with typical day-to-day life: 60 minutes of at least moderate to vigorous intensity physical activity): BMR x For males = 1.48 and females = 1.45
- Super active (very hard exercise & physical job or 2x training): BMR x 1.9
You can increase your basal metabolic rate (BMR) by:
- Exercising more, especially interval training
- Weight training to build muscle mass
- Eating fat-burning foods
- Getting enough sleep
After calculating your basal metabolic rate (BMR) or resting metabolic rate (RMR), your RMR should be multiplied by an appropriate physical activity factor to provide your baseline daily caloric level for weight maintenance. Once your baseline caloric level is known, your recommended calorie intake should be reduced to facilitate your weight loss.
If you want to lose weight, subtract 500 to 1000 calories from your Total Daily Energy Expenditure (TDEE) to get a daily intake goal. For weight gain, add extra calories. Reducing your calorie intake by 500 calories is a common strategy to yield a weight loss of approximately one pound per week, although reductions of up to 750 calories per day are sometimes used 127.
Another approach is to reduce your current caloric intake by 30% 127. Diets that reduce caloric intake relative to energy expenditure result in weight loss, regardless of macronutrient composition 127.
Here’s how to estimate how long it will take to reach your goal:
Jessie’s current weight is 150 lbs. She wants to lose 20 lbs.
- 150lbs – 20lbs = 130lbs.
- 20lbs loss at 2lbs/week = 10 weeks.
- It will take Jessie about 10 week to lose the weight.
Remember, these are general guidelines only. It’s crucial to monitor your progress and adjust as necessary. Consulting with a nutritionist or health professional is always recommended for personalized advice.
How many calories should I eat to lose weight?
For a healthy and sustainable weight loss journey, it’s typically recommended you not to shed more than 2 pounds of fat weekly. This translates to a daily calorie deficit of 1,000 calories. It’s essential to note that when weight loss surpasses 2lbs within a week, it’s often water weight being lost, not just fat.
For those leading a more sedentary lifestyle, aiming to lose 1lb per week is a good starting point. This means creating a daily calorie deficit of 500 calories.
On the other hand, those who are more active naturally have higher daily calorie needs. So, when they’re trying to lose weight, they can afford to eat a bit more since their maintenance calories are already elevated.
For such individuals, aiming for a daily calorie deficit of 500-1,000 calories is realistic, potentially leading to a weight loss rate of up to 2lbs weekly.
What happens when your calories are too low?
Consuming calories below your body’s needs for an extended period can lead to various physiological and psychological consequences. Here’s what can happen when your caloric intake is too low:
- Slower metabolism: Your body might slow down its metabolic rate as a defense mechanism to conserve energy. This can make weight loss harder over time and weight regain more likely once normal eating resumes.
- Nutrient deficiencies: Low calorie intake can lead to inadequate intake of essential vitamins and minerals. Over time, this can result in conditions like anemia, osteoporosis, and impaired immune function.
- Loss of muscle mass: Your body might start breaking down muscle tissue for energy, especially if protein intake is inadequate. This can further slow down metabolism and lead to weakness.
- Hormonal changes: Reduced calorie intake can affect hormone levels, leading to disruptions in menstrual cycles for women, reduced bone density, and other hormonal imbalances.
- Reduced energy and fatigue: You might feel constantly tired or find it difficult to concentrate.
- Mood changes: Low caloric intake can influence mood. This can result in irritability, depression, or anxiety.
- Impaired Immune Function: Your body might become more susceptible to infections due to a weakened immune system.
- Hair and skin problems: You might experience hair loss, dry skin, or brittle nails due to inadequate nutrient intake.
- Digestive problems: Constipation or other digestive issues can occur as a result of reduced fiber and fluid intake.
- Fertility issues: Low calorie and nutrient intake can lead to fertility problems in both men and women.
- Cardiovascular problems: Chronic low calorie intake can affect heart health, leading to low blood pressure, irregular heart rhythms, or other cardiovascular issues.
- Increased risk of gallstones: Rapid weight loss from very low-calorie diets can lead to the development of gallstones.
What is the best way to lose weight?
There is no one best way to lose weight, which is why doctors and dietitians work to understand your personal circumstances when making recommendations. There is no quick fix. Improving your diet and increasing activity can be key to losing weight, although are not the only factors that need to be considered. When aiming to lose weight it is important to have realistic goals that are achievable. Success boosts confidence in your ability to lose weight. A weight loss of between 0.5 to 2 pounds (0.5-1kg) a week is a safe and realistic target. Experts recommend losing 5 to 10 percent of your body weight within the first 6 months of treatment 128. If you weigh 200 pounds, this means losing as little as 10 pounds. Moreover, it’s not just about your weight on the scales, losing inches from your waist helps to lower your risk of conditions like type 2 diabetes and high blood pressure. To reach and stay at a healthy weight over the long term, you must focus on your overall health and lifestyle habits, not just on what you eat. Successful weight-loss programs should promote healthy behaviors that help you lose weight safely, that you can stick with every day, and that help you keep the weight off. People who successfully lose weight and keep it off develop techniques to make their new lifestyle and activity habits an enjoyable way of life and also make them life long.
You weight loss programs and weight loss maintenance programs should focus on changing your behavior to reduce energy intake by cutting unhealthy foods, decreasing sugar‐sweetened beverage consumption and fat intake, portion control, increasing fruit and vegetable intake, and adhering to a diet 129. Additionally, energy expenditure should be promoted through increasing physical activity.
American College of Sports Medicine recommendations for physical activity for Weight Loss and Prevention of Weight Regain for Adults 130:
- Maintain and improving health: 150 minutes/week
- Prevention of weight gain: 150 – 250 minutes/week
- Promote clinically significant weight loss: 225 – 420 minutes/week
- Prevention of weight gain after weight loss: 200 – 300 minutes/week
Strong evidence exists that exercise (physical activity) can reduce weight gain in those at risk for obesity, and many exercise training programs are capable of producing at least modest weight loss (~2 kg) 130. A question often encountered in the clinical setting from patients is how much exercise is needed to lose weight and what type of exercise training should be performed. Overall, the changes in weight in response to exercise training without caloric restriction are highly heterogeneous and individual differences can span weight gain to clinically significant weight loss 131. Patients should should consult their clinicians or dietitians on what are reasonable expectations based on their specific weight loss program. However, research data suggest that physical activity has an important role in the amount of weight regain following successful weight loss 132. Therefore, patients attempting to reduce recidivism after weight loss should engage in physical activity levels above 200 minutes/week 130.
Furthermore, high levels of physical activity and cardiorespiratory fitness (fitness) are inversely associated with cardiovascular disease, type 2 diabetes and all-cause mortality 133. Several epidemiological studies even suggest that high levels of physical activity or cardiorespiratory fitness reduces the health risk of obesity 134, 135. Moreover, cardiorespiratory fitness levels have been shown to alter the relationship of the obesity paradox, where high cardiorespiratory fitness level is associated with greater survival in all body mass index (BMI) categories 136. In summary, patients are encourage to adhere to exercise programs or engage in regular physical activity regardless of the weight loss achieved.
Another question that is often encountered in the clinical setting is if there is a difference between weight loss achieved through dietary means or through exercise training in terms of cardiovascular and type 2 diabetes mellitus risk factors. In an elegantly designed study, Ross et al. 137 randomized obese men (n= 52) to diet-induced weight loss, exercise induced weight loss, exercise without weight loss, or a control group for 3 months. The diet-induced and exercise-induced weight loss groups lost approximately 7 kg of weight (8% weight reduction), and had significant reductions in total fat mass, visceral fat and increased glucose disposal 137. However, the exercise-induced weight loss group had a greater reduction in total fat mass compared to the diet induced weight loss group 137. Importantly, the exercise-induced weight loss improved cardiorespiratory fitness (fitness) whereas the dietary group did not. In the group who performed exercise training without weight loss, the participants still experienced reductions in visceral fat and increased cardiorespiratory fitness.
The observations by Ross et al. 137 reaffirm that an exercise training program still confers health benefits to obese patients even in the absence of weight loss. Although dieting without exercise training has potential cardiovascular benefits, exercise training should be encouraged by to help patients improve cardiorespiratory fitness levels, which is an independent risk factor for cardiovascular diseases, type 2 diabetes mellitus and mortality 10, and may further augment the negative energy balance created by caloric restriction. Lastly, Ross’ observations suggest that there is a rationale for exercise training to be a part of weight loss programs as the authors observed greater changes in visceral fat, oral glucose tolerance, and glucose disposal in the exercise training group with clinically significant weight loss compared to the group with exercise without weight loss group 137.
- Dietary Guidelines for Americans. https://www.dietaryguidelines.gov/[↩][↩][↩][↩]
- Schwingshackl L, Hoffmann G. Monounsaturated fatty acids, olive oil and health status: a systematic review and meta-analysis of cohort studies. Lipids in Health and Disease. 2014;13:154. doi:10.1186/1476-511X-13-154. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4198773/[↩][↩]
- Schwingshackl L, Hoffmann G. Monounsaturated Fatty Acids and Risk of Cardiovascular Disease: Synopsis of the Evidence Available from Systematic Reviews and Meta-Analyses . Nutrients. 2012;4(12):1989-2007. doi:10.3390/nu4121989. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3546618/[↩][↩][↩][↩]
- AHA Science Advisory. Monounsaturated fatty acids and risk of cardiovascular disease. American Heart Association. Nutrition Committee. Circulation. 1999 Sep 14;100(11):1253-8. https://www.ncbi.nlm.nih.gov/pubmed/10484550/[↩]
- Omega-3 Fatty Acids. https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional[↩][↩][↩][↩][↩]
- Polyunsaturated Fats. https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/fats/polyunsaturated-fats[↩]
- Jones PJH, Rideout T. Lipids, sterols, and their metabolites. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2014.[↩][↩][↩][↩][↩]
- Jones PJH, Papamandjaris AA. Lipids: cellular metabolism. In: Erdman JW, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. Washington, DC: Wiley-Blackwell; 2012:132-48.[↩][↩][↩]
- Harris WS. Omega-3 fatty acids. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements. 2nd ed. London and New York: Informa Healthcare; 2010:577-86.[↩][↩][↩][↩][↩][↩]
- Lichtenstein AH, Jones PJH. Lipids: absorption and transport. In: Erdman JW, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. Washington, DC: Wiley-Blackwell; 2012:118-31.[↩][↩]
- Institute of Medicine, Food and Nutrition Board. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids (macronutrients). Washington, DC: National Academy Press; 2005.[↩][↩][↩]
- SanGiovanni JP, Chew EY. The role of omega-3 long-chain polyunsaturated fatty acids in health and disease of the retina. Prog Retin Eye Res. 2005 Jan;24(1):87-138. doi: 10.1016/j.preteyeres.2004.06.002[↩]
- Jones PJH, Rideout T. Lipids, sterols, and their metabolites. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2014[↩]
- Gabbs M, Leng S, Devassy JG, Monirujjaman M, Aukema HM. Advances in Our Understanding of Oxylipins Derived from Dietary PUFAs. Adv Nutr. 2015 Sep 15;6(5):513-40. doi: 10.3945/an.114.007732[↩]
- Simopoulos AP. The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp Biol Med (Maywood). 2008 Jun;233(6):674-88. doi: 10.3181/0711-MR-311[↩][↩]
- James M, Proudman S, Cleland L. Fish oil and rheumatoid arthritis: past, present and future. Proc Nutr Soc. 2010 Aug;69(3):316-23. doi: 10.1017/S0029665110001564[↩][↩]
- Wang C, Chung M, Lichtenstein A, Balk E, Kupelnick B, DeVine D, et al. Effects of omega-3 fatty acids on cardiovascular disease. Summary, evidence report/technology assessment no. 94. (Prepared by the Tufts New England Medical Center Evidence-based Practice Center, Boston, MA.) AHRQ Publication No. 04-E009-1. Agency for Healthcare Research and Quality, 2004. https://archive.ahrq.gov/downloads/pub/evidence/pdf/o3cardio/o3cardio.pdf[↩]
- Stanley JC, Elsom RL, Calder PC, Griffin BA, Harris WS, Jebb SA, Lovegrove JA, Moore CS, Riemersma RA, Sanders TA. UK Food Standards Agency Workshop Report: the effects of the dietary n-6:n-3 fatty acid ratio on cardiovascular health. Br J Nutr. 2007 Dec;98(6):1305-10. doi: 10.1017/S000711450784284X[↩][↩]
- Harris WS, Davidson MH. RE: Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst. 2014 Apr;106(4):dju019. doi: 10.1093/jnci/dju019[↩][↩]
- Fritsche KL. Too much linoleic acid promotes inflammation-doesn’t it? Prostaglandins Leukot Essent Fatty Acids. 2008 Sep-Nov;79(3-5):173-5. doi: 10.1016/j.plefa.2008.09.019[↩][↩]
- Monounsaturated Fats. https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/fats/monounsaturated-fats[↩]
- DiNicolantonio JJ, O’Keefe JH. Monounsaturated Fat vs Saturated Fat: Effects on Cardio-Metabolic Health and Obesity. Mo Med. 2022 Jan-Feb;119(1):69-73 https://pmc.ncbi.nlm.nih.gov/articles/PMC9312452[↩]
- Saturated Fat. https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/fats/saturated-fats[↩][↩][↩][↩]
- Eckel RH, Jakicic JM, Ard JD, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014 Jun 24;129(25 Suppl 2):S76-99. doi: 10.1161/01.cir.0000437740.48606.d1. Epub 2013 Nov 12. Erratum in: Circulation. 2014 Jun 24;129(25 Suppl 2):S100-1. Erratum in: Circulation. 2015 Jan 27;131(4):e326.[↩][↩]
- Morris AL, Mohiuddin SS. Biochemistry, Nutrients. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554545[↩]
- Del Razo Olvera FM, Melgarejo Hernández MA, Mehta R, Aguilar Salinas CA. Setting the Lipid Component of the Diet: A Work in Process. Adv Nutr. 2017 Jan 17;8(1):165S-172S. doi: 10.3945/an.116.013672[↩]
- Tvrzicka E, Kremmyda LS, Stankova B, Zak A. Fatty acids as biocompounds: their role in human metabolism, health and disease–a review. Part 1: classification, dietary sources and biological functions. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2011 Jun;155(2):117-30. doi: 10.5507/bp.2011.038[↩]
- Jacobs DR, Tapsell LC. Food synergy: the key to a healthy diet. Proc Nutr Soc. 2013 May;72(2):200-6. doi: 10.1017/S0029665112003011[↩]
- Trumbo P, Schlicker S, Yates AA, Poos M; Food and Nutrition Board of the Institute of Medicine, The National Academies. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J Am Diet Assoc. 2002 Nov;102(11):1621-30. doi: 10.1016/s0002-8223(02)90346-9. Erratum in: J Am Diet Assoc. 2003 May;103(5):563.[↩][↩]
- Omega-3 Fatty Acids, https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional[↩][↩]
- Wang C, Chung M, Lichtenstein A, Balk E, Kupelnick B, DeVine D, et al. Effects of omega-3 fatty acids on cardiovascular disease. Summary, evidence report/technology assessment no. 94. https://archive.ahrq.gov/downloads/pub/evidence/pdf/o3cardio/o3cardio.pdf[↩]
- Very Low-Calorie Diets. https://www.govinfo.gov/content/pkg/GOVPUB-HE20-PURL-LPS78142/pdf/GOVPUB-HE20-PURL-LPS78142.pdf[↩]
- Dwyer JT, Melanson KJ, Sriprachy-anunt U, et al. Dietary Treatment of Obesity. [Updated 2015 Feb 28]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK278991[↩][↩][↩][↩][↩]
- Pritikin M, McGrady PM. The Pritikin Program for Diet and Exercise. New York: Bantum Books, 1980.[↩]
- Ornish D. Can lifestyle changes reverse coronary heart disease? World Rev Nutr Diet. 1993;72:38-48. doi: 10.1159/000422326[↩][↩][↩]
- Hand B and Romine S. The Spark Solution. HarperOne, 2014.[↩]
- Ghanbari R, Anwar F, Alkharfy KM, Gilani A-H, Saari N. Valuable Nutrients and Functional Bioactives in Different Parts of Olive (Olea europaea L.)—A Review. International Journal of Molecular Sciences. 2012;13(3):3291-3340. doi:10.3390/ijms13033291. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3317714/[↩][↩]
- Viola P., Viola M. Virgin olive oil as a fundamental nutritional component and skin protector. Clin. Dermatol. 2009;27:159–165. https://www.ncbi.nlm.nih.gov/pubmed/19167997[↩][↩]
- American Heart Association. Saturated Fat. https://healthyforgood.heart.org/eat-smart/articles/saturated-fats[↩][↩]
- International Society for the Study of Fatty Acids and Lipids. http://www.issfal.org/[↩][↩]
- Fats and Fatty Acids in Human Nutrition. Report of an Expert Consultation. http://www.fao.org/docrep/013/i1953e/i1953e00.pdf[↩][↩]
- Siri-Tarino, P.W., et al., Saturated fatty acids and risk of coronary heart disease: modulation by replacement nutrients. Curr Atheroscler Rep, 2010. 12(6): p. 384-90.[↩][↩]
- Hu, F.B., et al., Dietary fat intake and the risk of coronary heart disease in women. N Engl J Med, 1997. 337(21): p. 1491-9.[↩][↩]
- Ascherio, A., et al., Dietary fat and risk of coronary heart disease in men: cohort follow up study in the United States. BMJ, 1996. 313(7049): p. 84-90.[↩][↩]
- Hu, F.B., J.E. Manson, and W.C. Willett, Types of dietary fat and risk of coronary heart disease: a critical review. J Am Coll Nutr, 2001. 20(1): p. 5-19.[↩][↩]
- Journal of the American College of Cardiology Volume 66, Issue 14, October 2015. DOI: 10.1016/j.jacc.2015.07.055. Saturated Fats Compared With Unsaturated Fats and Sources of Carbohydrates in Relation to Risk of Coronary Heart Disease. http://www.onlinejacc.org/content/66/14/1538[↩][↩]
- Wang DD, Li Y, Chiuve SE, Stampfer MJ, Manson JE, Rimm EB, Willett WC, Hu FB. Association of Specific Dietary Fats With Total and Cause-Specific Mortality. JAMA Intern Med. 2016;176(8):1134–1145. doi:10.1001/jamainternmed.2016.2417. http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2530902[↩][↩][↩][↩][↩]
- American Heart Association. Cutting through the saturated fat – meats, butter and tropical oils still need limits. http://news.heart.org/cutting-saturated-fat-meats-butter-tropical-oils-still-need-limits/[↩][↩][↩]
- Harvard University, Harvard School of Public Health. Different Dietary Fat, Different Risk of Mortality. https://www.hsph.harvard.edu/nutritionsource/2016/07/05/different-dietary-fat-different-risk-of-mortality/[↩]
- American Heart Association – Dietary Fats – https://healthyforgood.heart.org/Eat-smart/Articles/Dietary-Fats[↩]
- Cochrane Review 7 August 2015 – Effect of cutting down the fat we eat on body weight – http://www.cochrane.org/CD011834/VASC_effect-cutting-down-fat-we-eat-body-weight[↩]
- Salem N., Jr Introduction to polyunsaturated fatty acids. Backgrounder. 1999;3:1–8.[↩][↩]
- Clinical nutrition: 4. Omega-3 fatty acids in cardiovascular care. Holub BJ. CMAJ. 2002 Mar 5; 166(5):608-15. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC99405/[↩][↩]
- Simopoulos AP. An Increase in the Omega-6/Omega-3 Fatty Acid Ratio Increases the Risk for Obesity. Nutrients. 2016;8(3):128. doi:10.3390/nu8030128. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4808858/[↩][↩]
- Alpha-linolenic acid and cardiovascular diseases. Lanzmann-Petithory D. J Nutr Health Aging. 2001; 5(3):179-83. https://www.ncbi.nlm.nih.gov/pubmed/11458289/[↩]
- U.S. National Library of Medicine. Facts about saturated fats. https://medlineplus.gov/ency/patientinstructions/000838.htm[↩]
- American Heart Association. Advisory: Replacing saturated fat with healthier fat could lower cardiovascular risks. http://news.heart.org/advisory-replacing-saturated-fat-with-healthier-fat-could-lower-cardiovascular-risks/[↩][↩][↩]
- American Heart Association. Saturated Fats. https://healthyforgood.heart.org/Eat-smart/Articles/Saturated-Fats[↩][↩]
- US Department of Agriculture, Agricultural Research Service, National Nutrient Database for Standard Reference, release 28, 2016. https://ndb.nal.usda.gov/ndb/search/list. Accessed May 23, 2017.[↩]
- American Heart Association. Recipes for Cholesterol Management. http://www.heart.org/HEARTORG/Conditions/Cholesterol/CholesterolToolsResources/Recipes-for-Cholesterol-Management_UCM_305655_Article.jsp[↩]
- Mozaffarian D, Benjamin EJ, Go AS, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2015 update: a report from the American Heart Association. Circulation. 2015 Jan 27;131(4):e29-322. doi: 10.1161/CIR.0000000000000152. Epub 2014 Dec 17. Erratum in: Circulation. 2015 Jun 16;131(24):e535. doi: 10.1161/CIR.0000000000000219. Erratum in: Circulation. 2016 Feb 23;133(8):e417. doi: 10.1161/CIR.0000000000000386[↩]
- Cochrane Review 15 June 2015 – “Effect of cutting down on the saturated fat we eat on our risk of heart disease” – http://www.cochrane.org/CD011737/VASC_effect-of-cutting-down-on-the-saturated-fat-we-eat-on-our-risk-of-heart-disease[↩][↩]
- Chowdhury R, Warnakula S, Kunutsor S et al. (2014) Association of dietary, circulating, and supplement fatty acids with coronary risk: a systematic review and meta-analysis. Annals of Internal Medicine 160: 398–406.[↩]
- Malhotra A (2013) Saturated fat is not the major issue. BMJ 347.[↩]
- Nevin K & Rajamohan T (2004a) Beneficial effects of virgin coconut oil on lipid parameters and in vitro LDL oxidation. Clinical Biochemistry 37: 830–5. https://www.ncbi.nlm.nih.gov/pubmed/15329324[↩]
- Mozaffarian D, Micha R, Wallace S. Effects on coronary heart disease of increasing polyunsaturated fat in place of saturated fat: a systematic review and meta-analysis of randomized controlled trials. PLoS Med. 2010;7:e1000252. doi: 10.1371/journal. pmed.1000252.[↩][↩][↩]
- Siri-Tarino PW, Sun Q, Hu FB et al. (2010) Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. The American Journal of Clinical Nutrition 91: 535–46. https://www.ncbi.nlm.nih.gov/pubmed/20071648[↩]
- Hooper L, Martin N, Abdelhamid A, Davey Smith G. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst Rev. 2015:CD011737. doi: 10.1002/14651858.CD011737.[↩]
- Farvid MS, Ding M, Pan A, Sun Q, Chiuve SE, Steffen LM, Willett WC, Hu FB. Dietary linoleic acid and risk of coronary heart disease: a systematic review and meta-analysis of prospective cohort studies. Circulation. 2014;130:1568–1578. doi: 10.1161/ CIRCULATIONAHA.114.010236.[↩][↩][↩]
- Siri-Tarino PW, Sun Q, Hu FB, Krauss RM. Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. Am J Clin Nutr. 2010;91:535–546. doi: 10.3945/ajcn.2009.27725.[↩][↩]
- Chowdhury R, Warnakula S, Kunutsor S, Crowe F, Ward HA, Johnson L, Franco OH, Butterworth AS, Forouhi NG, Thompson SG, Khaw KT, Mozaffarian D, Danesh J, Di Angelantonio E. Association of dietary, circulating, and supplement fatty acids with coronary risk: a systematic review and meta-analysis [published correction appears in Arch Intern Med. 2014;160:658]. Ann Intern Med. 2014;160:398–406. doi: 10.7326/M13-1788.[↩]
- Jakobsen MU, O’Reilly EJ, Heitmann BL, Pereira MA, Bälter K, Fraser GE, Goldbourt U, Hallmans G, Knekt P, Liu S, Pietinen P, Spiegelman D, Stevens J, Virtamo J, Willett WC, Ascherio A. Major types of dietary fat and risk of coronary heart disease: a pooled analysis of 11 cohort studies. Am J Clin Nutr. 2009;89:1425– 1432. doi: 10.3945/ajcn.2008.27124.[↩][↩][↩]
- Circulation June 15, 2017;CIR.510. – Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association – http://circ.ahajournals.org/content/early/2017/06/15/CIR.0000000000000510 [↩]
- Hooper L, Martin N, Abdelhamid A, Davey Smith G. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst Rev. 2015:CD011737. doi: 10.1002/14651858. CD011737.[↩][↩]
- Li Y, Hruby A, Bernstein AM, Ley SH, Wang DD, Chiuve SE, Sampson L, Rexrode KM, Rimm EB, Willett WC, Hu FB. Saturated fats compared with unsaturated fats and sources of carbohydrates in relation to risk of coronary heart disease: a prospective cohort study. J Am Coll Cardiol. 2015;66:1538–1548. doi: 10.1016/j. jacc.2015.07.055.[↩]
- Chowdhury R, Warnakula S, Kunutsor S, Crowe F, Ward HA, Johnson L, Franco OH, Butterworth AS, Forouhi NG, Thompson SG, Khaw KT, Mozaffarian D, Danesh J, Di Angelantonio E. Association of dietary, circulating, and supplement fatty acids with coronary risk: a systematic review and meta-analysis [published correction appears in Arch Intern Med. 2014;160:658]. Ann Intern Med. 014;160:398–406. doi: 10.7326/M13-1788.[↩]
- Li Y, Hruby A, Bernstein AM, Ley SH, Wang DD, Chiuve SE, Sampson L, Rexrode KM, Rimm EB, Willett WC, Hu FB. Saturated fats compared with unsaturated fats and sources of carbohydrates in relation to risk of coronary heart disease: a prospective cohort tudy. J Am Coll Cardiol. 2015;66:1538–1548. doi: 10.1016/j. jacc.2015.07.055.[↩][↩]
- Keys A. Seven Countries: A Multivariate Analysis of Death and Coronary Heart Disease. Cambridge, MA: Harvard University Press, 1980.[↩]
- Mensink RP. Effects of Saturated Fatty Acids on Serum Lipids and Lipoproteins: A Systematic Review and Regression Analysis. Geneva, Switzerland: World Health Organization; 2016.[↩]
- Rudel LL, Parks JS, Sawyer JK. Compared with dietary monounsaturated and saturated fat, polyunsaturated fat protects African green monkeys from coronary artery atherosclerosis. Arterioscler Thromb Vasc Biol. 1995;15:2101–2110.[↩]
- BMJ 2016;355:i5796. Intake of individual saturated fatty acids and risk of coronary heart disease in US men and women: two prospective longitudinal cohort studies. http://www.bmj.com/content/355/bmj.i5796[↩][↩][↩]
- R K Kelly, T Y N Tong, M Guasch-Ferre, K Papier, C Piernas, G K Fensom, J L Carter, T J Key, A Perez-Cornago, Associations between saturated fatty acids from different dietary sources and cardiovascular disease risk in 114,285 UK Biobank study participants, European Heart Journal, Volume 42, Issue Supplement_1, October 2021, ehab724.2418, https://doi.org/10.1093/eurheartj/ehab724.2418[↩][↩][↩][↩][↩][↩][↩]
- Houston M. The relationship of saturated fats and coronary heart disease: fa(c)t or fiction? A commentary. Ther Adv Cardiovasc Dis. 2018 Feb;12(2):33-37. doi: 10.1177/1753944717742549[↩]
- Ruiz-Núñez B, Dijck-Brouwer DA, Muskiet FA. The relation of saturated fatty acids with low-grade inflammation and cardiovascular disease. J Nutr Biochem. 2016 Oct;36:1-20. doi: 10.1016/j.jnutbio.2015.12.007[↩]
- Siri-Tarino PW, Sun Q, Hu FB, Krauss RM. Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. Am J Clin Nutr. 2010 Mar;91(3):535-46. doi: 10.3945/ajcn.2009.27725[↩]
- Chowdhury R, Warnakula S, Kunutsor S, Crowe F, Ward HA, Johnson L, Franco OH, Butterworth AS, Forouhi NG, Thompson SG, Khaw KT, Mozaffarian D, Danesh J, Di Angelantonio E. Association of dietary, circulating, and supplement fatty acids with coronary risk: a systematic review and meta-analysis. Ann Intern Med. 2014 Mar 18;160(6):398-406. doi: 10.7326/M13-1788. Erratum in: Ann Intern Med. 2014 May 6;160(9):658.[↩]
- de Souza RJ, Mente A, Maroleanu A, Cozma AI, Ha V, Kishibe T, Uleryk E, Budylowski P, Schünemann H, Beyene J, Anand SS. Intake of saturated and trans unsaturated fatty acids and risk of all cause mortality, cardiovascular disease, and type 2 diabetes: systematic review and meta-analysis of observational studies. BMJ. 2015 Aug 11;351:h3978. doi: 10.1136/bmj.h3978[↩]
- Skeaff CM, Miller J. Dietary fat and coronary heart disease: summary of evidence from prospective cohort and randomised controlled trials. Ann Nutr Metab. 2009;55(1-3):173-201. doi: 10.1159/000229002[↩]
- Yamagishi K, Iso H, Yatsuya H, Tanabe N, Date C, Kikuchi S, Yamamoto A, Inaba Y, Tamakoshi A; JACC Study Group. Dietary intake of saturated fatty acids and mortality from cardiovascular disease in Japanese: the Japan Collaborative Cohort Study for Evaluation of Cancer Risk (JACC) Study. Am J Clin Nutr. 2010 Oct;92(4):759-65. doi: 10.3945/ajcn.2009.29146[↩]
- Jakobsen MU, O’Reilly EJ, Heitmann BL, Pereira MA, Bälter K, Fraser GE, Goldbourt U, Hallmans G, Knekt P, Liu S, Pietinen P, Spiegelman D, Stevens J, Virtamo J, Willett WC, Ascherio A. Major types of dietary fat and risk of coronary heart disease: a pooled analysis of 11 cohort studies. Am J Clin Nutr. 2009 May;89(5):1425-32. doi: 10.3945/ajcn.2008.27124[↩]
- Lichtenstein AH. Dietary Fat and Cardiovascular Disease: Ebb and Flow Over the Last Half Century. Adv Nutr. 2019 Nov 1;10(Suppl_4):S332-S339. doi: 10.1093/advances/nmz024[↩]
- Li Y, Hruby A, Bernstein AM, Ley SH, Wang DD, Chiuve SE, Sampson L, Rexrode KM, Rimm EB, Willett WC, Hu FB. Saturated Fats Compared With Unsaturated Fats and Sources of Carbohydrates in Relation to Risk of Coronary Heart Disease: A Prospective Cohort Study. J Am Coll Cardiol. 2015 Oct 6;66(14):1538-1548. doi: 10.1016/j.jacc.2015.07.055[↩][↩]
- Clifton PM, Keogh JB. A systematic review of the effect of dietary saturated and polyunsaturated fat on heart disease. Nutr Metab Cardiovasc Dis. 2017 Dec;27(12):1060-1080. doi: 10.1016/j.numecd.2017.10.010[↩][↩]
- Sacks FM, Lichtenstein AH, Wu JHY, Appel LJ, Creager MA, Kris-Etherton PM, Miller M, Rimm EB, Rudel LL, Robinson JG, Stone NJ, Van Horn LV; American Heart Association. Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association. Circulation. 2017 Jul 18;136(3):e1-e23. doi: 10.1161/CIR.0000000000000510. Epub 2017 Jun 15. Erratum in: Circulation. 2017 Sep 5;136(10):e195. doi: 10.1161/CIR.0000000000000529[↩][↩]
- de Oliveira Otto MC, Mozaffarian D, Kromhout D, Bertoni AG, Sibley CT, Jacobs DR Jr, Nettleton JA. Dietary intake of saturated fat by food source and incident cardiovascular disease: the Multi-Ethnic Study of Atherosclerosis. Am J Clin Nutr. 2012 Aug;96(2):397-404. doi: 10.3945/ajcn.112.037770[↩]
- Yuan M, Singer MR, Pickering RT, Moore LL. Saturated fat from dairy sources is associated with lower cardiometabolic risk in the Framingham Offspring Study. Am J Clin Nutr. 2022 Dec 19;116(6):1682-1692. doi: 10.1093/ajcn/nqac224[↩][↩][↩][↩][↩][↩]
- American Heart Association. Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association. http://circ.ahajournals.org/content/early/2017/06/15/CIR.0000000000000510[↩]
- Hu FB, Stampfer MJ, Manson JE, Ascherio A, Colditz GA, Speizer FE, Hennekens CH, Willett WC. Dietary saturated fats and their food sources in relation to the risk of coronary heart disease in women. Am J Clin Nutr. 1999 Dec;70(6):1001-8. doi: 10.1093/ajcn/70.6.1001[↩]
- Praagman J, Beulens JW, Alssema M, Zock PL, Wanders AJ, Sluijs I, van der Schouw YT. The association between dietary saturated fatty acids and ischemic heart disease depends on the type and source of fatty acid in the European Prospective Investigation into Cancer and Nutrition-Netherlands cohort. Am J Clin Nutr. 2016 Feb;103(2):356-65. doi: 10.3945/ajcn.115.122671[↩]
- Zong G, Li Y, Wanders AJ, Alssema M, Zock PL, Willett WC, Hu FB, Sun Q. Intake of individual saturated fatty acids and risk of coronary heart disease in US men and women: two prospective longitudinal cohort studies. BMJ. 2016 Nov 23;355:i5796. doi: 10.1136/bmj.i5796[↩]
- Flock MR, Kris-Etherton PM. Diverse physiological effects of long-chain saturated fatty acids: implications for cardiovascular disease. Curr Opin Clin Nutr Metab Care. 2013 Mar;16(2):133-40. doi: 10.1097/MCO.0b013e328359e6ac[↩]
- Yong JW, Ge L, Ng YF, Tan SN. The chemical composition and biological properties of coconut (Cocos nucifera L.) water. Molecules. 2009 Dec 9;14(12):5144-64. doi: 10.3390/molecules14125144[↩]
- Babu A. S., Veluswamy S. K., Arena R., Guazzi M., Lavie C. J. Virgin coconut oil and its potential cardioprotective effects. Postgraduate Medicine. 2014;126(7):76–83. doi: 10.3810/pgm.2014.11.2835[↩]
- Eyres L., Eyres M. F., Chisholm A., Brown R. C. Coconut oil consumption and cardiovascular risk factors in humans. Nutrition Reviews. 2016;74(4):267–280. doi: 10.1093/nutrit/nuw002[↩]
- Sacks FM, Lichtenstein AH, Wu JHY, Appel LJ, Creager MA, Kris-Etherton PM, Miller M, Rimm EB, Rudel LL, Robinson JG, Stone NJ, Van Horn LV; American Heart Association. Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association. Circulation. 2017 Jul 18;136(3):e1-e23. https://www.ahajournals.org/doi/10.1161/CIR.0000000000000510 Erratum in: Circulation. 2017 Sep 5;136(10):e195. doi: 10.1161/CIR.0000000000000529[↩][↩][↩][↩]
- St-Onge MP, Mayrsohn B, O’Keeffe M, Kissileff HR, Choudhury AR, Laferrère B. Impact of medium and long chain triglycerides consumption on appetite and food intake in overweight men. Eur J Clin Nutr. 2014 Oct;68(10):1134-40. doi: 10.1038/ejcn.2014.145[↩][↩][↩][↩]
- Bhavsar N, St-Onge MP. The diverse nature of saturated fats and the case of medium-chain triglycerides: how one recommendation may not fit all. Curr Opin Clin Nutr Metab Care. 2016 Mar;19(2):81-7. doi: 10.1097/MCO.0000000000000249[↩]
- St-Onge MP, Bosarge A. Weight-loss diet that includes consumption of medium-chain triacylglycerol oil leads to a greater rate of weight and fat mass loss than does olive oil. Am J Clin Nutr. 2008 Mar;87(3):621-6. doi: 10.1093/ajcn/87.3.621[↩][↩][↩]
- American Heart Association – The Skinny on Fats – http://www.heart.org/HEARTORG/Conditions/Cholesterol/PreventionTreatmentofHighCholesterol/Know-Your-Fats_UCM_305628_Article.jsp[↩]
- Mensink RP, Katan MB. Effect of dietary trans fatty acids on high-density and low-density lipoprotein cholesterol levels in healthy subjects. N Engl J Med. 1990;323(7):439–445.[↩]
- Zock PL, Katan MB. Hydrogenation alternatives: effects of trans fatty acids and stearic acid versus linoleic acid on serum lipids and lipoproteins in humans. J Lipid Res. 1992;33(3):399–410.[↩]
- Judd JT, Clevidence BA, Muesing RA, Wittes J, Sunkin ME, Podczasy JJ. Dietary trans fatty acids: effects on plasma lipids and lipoproteins of healthy men and women. Am J Clin Nutr. 1994;59(4):861–868.[↩]
- Lichtenstein AH, Ausman LM, Jalbert SM, Schaefer EJ. Effects of different forms of dietary hydrogenated fats on serum lipoprotein cholesterol levels [published correction in N Engl J Med. 1999;341(11):856]. N Engl J Med. 1999;340(25):1933–1940.[↩]
- de Roos N, Schouten E, Katan M. Consumption of a solid fat rich in lauric acid results in a more favorable serum lipid profile in healthy men and women than consumption of a solid fat rich in trans-fatty acids. J Nutr. 2001;131(2):242–245.[↩][↩]
- Hu FB, Stampfer MJ, Manson JE, et al. Dietary fat intake and the risk of coronary heart disease in women. N Engl J Med. 1997;337(21):1491–1499.[↩][↩][↩]
- Pietinen P, Ascherio A, Korhonen P, et al. Intake of fatty acids and risk of coronary heart disease in a cohort of Finnish men. The Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study. Am J Epidemiol. 1997;145(10):876–887.[↩][↩]
- Oomen CM, Ocké MC, Feskens EJ, van Erp-Baart MA, Kok FJ, Kromhout D. Association between trans fatty acid intake and 10-year risk of coronary heart disease in the Zutphen Elderly Study: a prospective population-based study. Lancet. 2001;357(9258):746–751.[↩][↩]
- Ascherio A, Rimm EB, Giovannucci EL, Spiegelman D, Stampfer M, Willett WC. Dietary fat and risk of coronary heart disease in men: cohort follow up study in the United States. BMJ. 1996;313(7049):84–90.[↩]
- Dietary Fatty Acids. Am Fam Physician. 2009 Aug 15;80(4):345-350. http://www.aafp.org/afp/2009/0815/p345.html[↩]
- Thomas, D. M., Bouchard, C., Church, T., Slentz, C., Kraus, W. E., Redman, L. M., Martin, C. K., Silva, A. M., Vossen, M., Westerterp, K., & Heymsfield, S. B. (2012). Why do individuals not lose more weight from an exercise intervention at a defined dose? An energy balance analysis. Obesity reviews : an official journal of the International Association for the Study of Obesity, 13(10), 835–847. https://doi.org/10.1111/j.1467-789X.2012.01012.x[↩]
- Aim for Healthy Weight. https://www.nhlbi.nih.gov/health/educational/lose_wt/index.htm[↩]
- Slentz CA, Duscha BD, Johnson JL, Ketchum K, Aiken LB, Samsa GP, Houmard JA, Bales CW, Kraus WE. Effects of the amount of exercise on body weight, body composition, and measures of central obesity: STRRIDE–a randomized controlled study. Arch Intern Med. 2004 Jan 12;164(1):31-9. doi: 10.1001/archinte.164.1.31[↩]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020-2025. 9th Edition. December 2020. https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf[↩]
- Mifflin MD, St Jeor ST, Hill LA, Scott BJ, Daugherty SA, Koh YO. A new predictive equation for resting energy expenditure in healthy individuals. Am J Clin Nutr. 1990 Feb;51(2):241-7. doi: 10.1093/ajcn/51.2.241[↩]
- American Dietetic Association (ADA). Adult Weight Management Guideline: Major Recommendations. ADA Evidence Analysis Library 2014. https://www.andeal.org/vault/pq132.pdf[↩]
- Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults–The Evidence Report. National Institutes of Health, 6: 51S-179S. https://doi.org/10.1002/j.1550-8528.1998.tb00690.x[↩]
- American College of Cardiology/American Heart Association Task Force on Practice Guidelines, Obesity Expert Panel, 2013. Expert Panel Report: Guidelines (2013) for the management of overweight and obesity in adults. Obesity (Silver Spring). 2014 Jul;22 Suppl 2:S41-410. doi: 10.1002/oby.20660[↩][↩][↩]
- Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults. Circulation. 2014;129:S102–S138.[↩]
- Varkevisser, R., van Stralen, M. M., Kroeze, W., Ket, J., & Steenhuis, I. (2019). Determinants of weight loss maintenance: a systematic review. Obesity reviews : an official journal of the International Association for the Study of Obesity, 20(2), 171–211. https://doi.org/10.1111/obr.12772[↩]
- Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, Smith BK; American College of Sports Medicine. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc. 2009 Feb;41(2):459-71. doi: 10.1249/MSS.0b013e3181949333. Erratum in: Med Sci Sports Exerc. 2009 Jul;41(7):1532.[↩][↩][↩]
- Church TS, Martin CK, Thompson AM, Earnest CP, Mikus CR, Blair SN. Changes in weight, waist circumference and compensatory responses with different doses of exercise among sedentary, overweight postmenopausal women. PLoS One. 2009;4(2):e4515. doi: 10.1371/journal.pone.0004515[↩]
- Swift, D. L., Johannsen, N. M., Lavie, C. J., Earnest, C. P., & Church, T. S. (2014). The role of exercise and physical activity in weight loss and maintenance. Progress in cardiovascular diseases, 56(4), 441–447. https://doi.org/10.1016/j.pcad.2013.09.012[↩]
- Swift DL, Lavie CJ, Johannsen NM, Arena R, Earnest CP, O’Keefe JH, Milani RV, Blair SN, Church TS. Physical activity, cardiorespiratory fitness, and exercise training in primary and secondary coronary prevention. Circ J. 2013;77(2):281-92. doi: 10.1253/circj.cj-13-0007[↩]
- Lee CD, Blair SN, Jackson AS. Cardiorespiratory fitness, body composition, and all-cause and cardiovascular disease mortality in men. Am J Clin Nutr. 1999 Mar;69(3):373-80. doi: 10.1093/ajcn/69.3.373[↩]
- Wei M, Kampert JB, Barlow CE, Nichaman MZ, Gibbons LW, Paffenbarger RS Jr, Blair SN. Relationship between low cardiorespiratory fitness and mortality in normal-weight, overweight, and obese men. JAMA. 1999 Oct 27;282(16):1547-53. doi: 10.1001/jama.282.16.1547[↩]
- McAuley, P. A., Kokkinos, P. F., Oliveira, R. B., Emerson, B. T., & Myers, J. N. (2010). Obesity paradox and cardiorespiratory fitness in 12,417 male veterans aged 40 to 70 years. Mayo Clinic proceedings, 85(2), 115–121. https://doi.org/10.4065/mcp.2009.0562[↩]
- Ross R, Dagnone D, Jones PJ, Smith H, Paddags A, Hudson R, Janssen I. Reduction in obesity and related comorbid conditions after diet-induced weight loss or exercise-induced weight loss in men. A randomized, controlled trial. Ann Intern Med. 2000 Jul 18;133(2):92-103. doi: 10.7326/0003-4819-133-2-200007180-00008[↩][↩][↩][↩][↩]
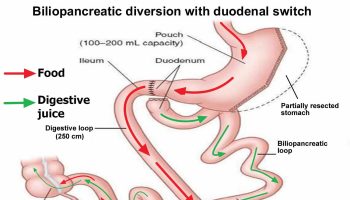
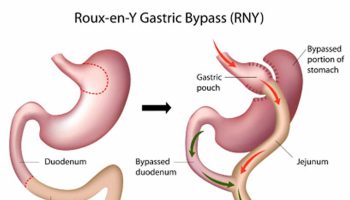


{kind=link}