Contents
What are thoracic vertebrae
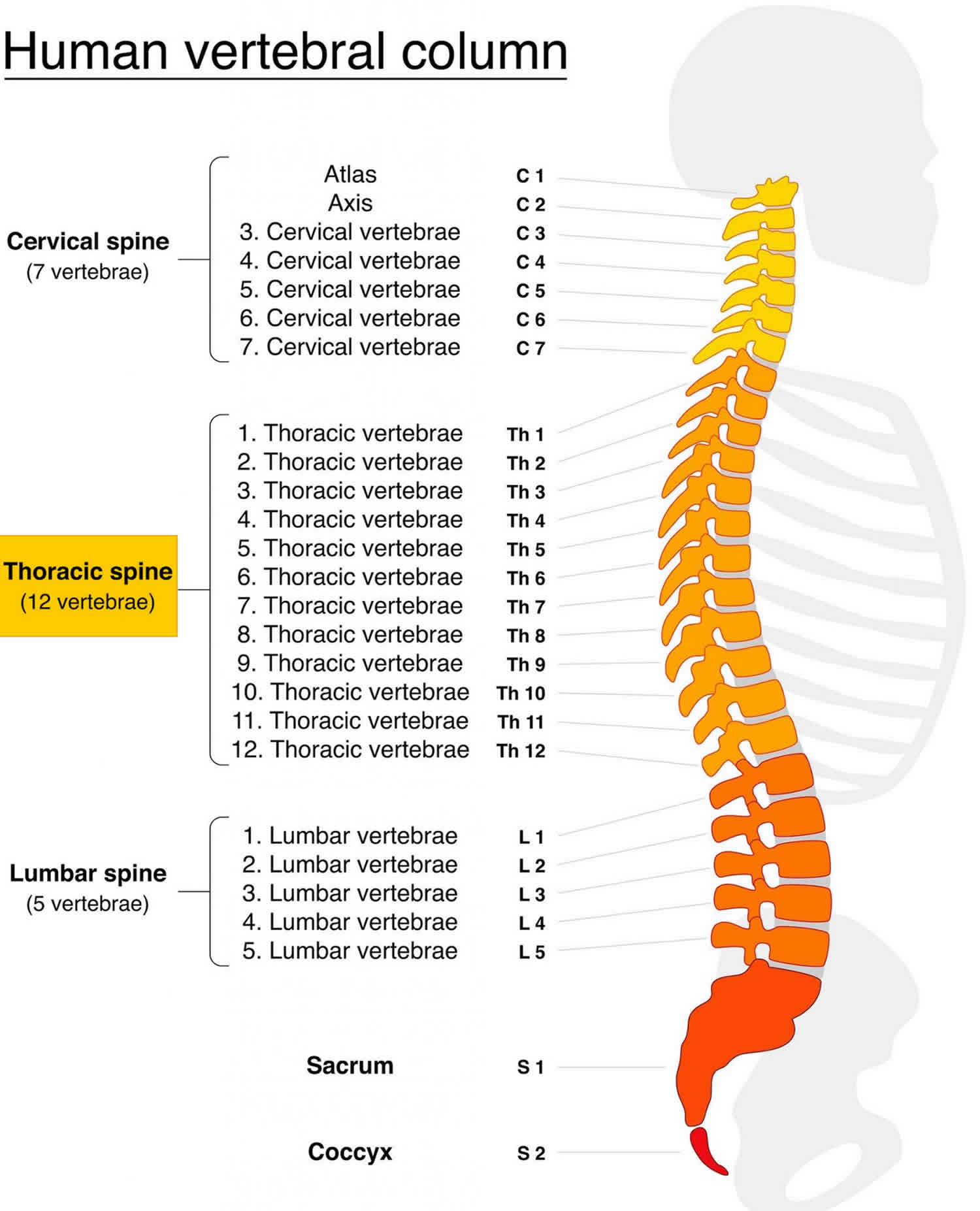
Your thoracic spine is the middle section of your vertebra between your neck and lower back and composes 12 thoracic vertebrae (denoted T1-T12) and your rib cage. The thoracic spine, as a group, produce a kyphotic curve. Thoracic vertebrae are unique in that they have the additional role of providing attachments for the ribs 1. Vertebrae, along with intervertebral discs, compose the vertebral column, or spine. It extends from the skull to the coccyx and includes the cervical, thoracic, lumbar and sacral regions. The spine has several major roles in the body that include: protection of the spinal cord and branching spinal nerves, support for thorax and abdomen, and enables flexibility and mobility of the body. The intervertebral discs are responsible for this mobility without sacrificing the supportive strength of the vertebral column. The intervertebral discs, along with the laminae, pedicles and articular processes of adjacent vertebrae, create a space through which spinal nerves exit.
Thoracic spine provide points of attachment for numerous muscles: erector spinae, interspinales, intertransversarii, latissimus dorsi, multifidus, rhomboid major, rhomboid minor, rotatores, semispinalis, serratus posterior superior/inferior, splenius capitis, splenius cervicis, and trapezius.
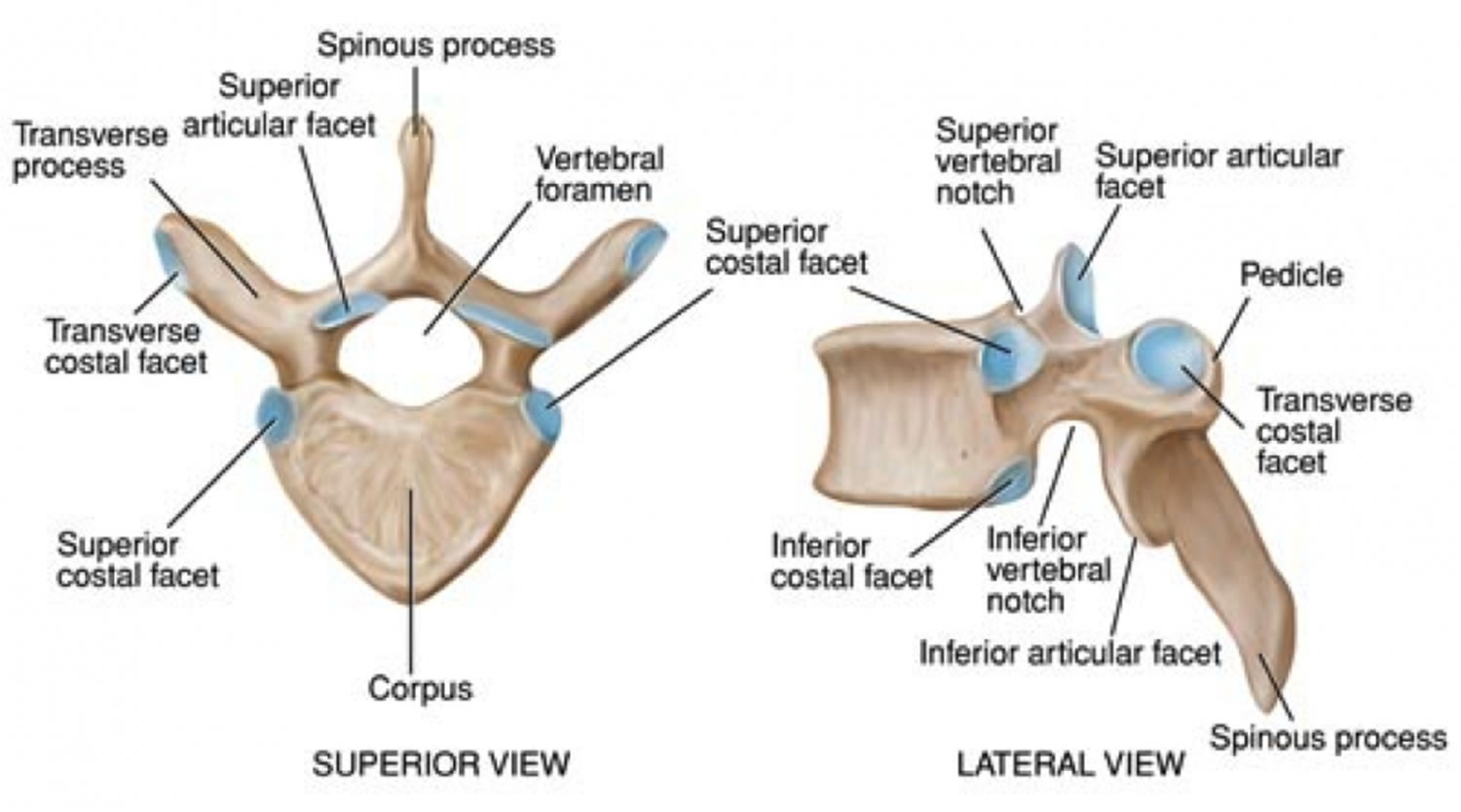
Typical thoracic vertebrae have several features distinct from those typical of cervical or lumbar vertebrae. T5-T8 tend to be the most “typical” in that they contain features present in all thoracic vertebrae. The primary characteristic of thoracic vertebrae is the presence of costal facets. There are six facets per thoracic vertebrae: two on the transverse processes and four demifacets. The facets of the transverse processes articulate with the tubercle of the associated rib. The demifacets are bilaterally paired and located on the superior and inferior posterolateral aspects of the vertebrae. They are positioned so that the superior demifacet of inferior vertebrae articulates with the head of the same rib that articulates with the inferior demifacet of a superior rib. For example, the inferior demifacets of T4 and the superior demifacets of T5 articulate with the head of rib 5. The length of the transverse processes decreases as the column descends. The positioning of the ribs and spinous processes greatly limits flexion and extension of thoracic vertebrae. However, T5-T8 have the greatest rotation ability of the thoracic region. Thoracic vertebrae have superior articular facets that face in a posterolateral direction. The spinous process is long, relative to other regions, and is directed posteroinferiorly. This projection gradually increases as the column descends before decreasing rapidly from T9-T12. The intervertebral disc height, is, on average, the least of the vertebral regions.
How many thoracic vertebrae are there?
There are 12 thoracic vertebrae (denoted T1-T12)
There are three atypical vertebrae found in the thoracic region:
The superior costal facets of T1 are “whole” costal facets. They alone articulate with the first rib; C7 has no costal facets. T1 does, however, have typical inferior demifacets for articulation with the second rib. T1 also has a long, almost horizontal spinous process, similar to those of cervical vertebra that may be as long as the vertebra prominens of C7.
T11 and T12 are atypical in that they contain a single pair, “whole,” costal facet that articulate with the 11 and 12 ribs, respectively. They also lack facets on the transverse processes. It varies by the individual, but T10 may resemble the atypical nature of the 11 and 12 vertebrae. When that is the case, T9 lacks an inferior demifacet, as it would not be needed to articulate with the 10 rib.
Additionally, T12 is unique in that is represents a transition from thoracic to lumbar vertebra. It is thoracic in that it contains costal facets and superior articular facets that allow for rotation, flexion, and rotation. It is lumbar in that it has articular processes that do not allow for rotation, only flexion and extension. It also contains mammillary processes, small tubercles located on the posterior surface of the superior articular processes, which allow for attachment for the intertransversarii and multifidus muscles 2.
Figure 1. Thoracic spine anatomy
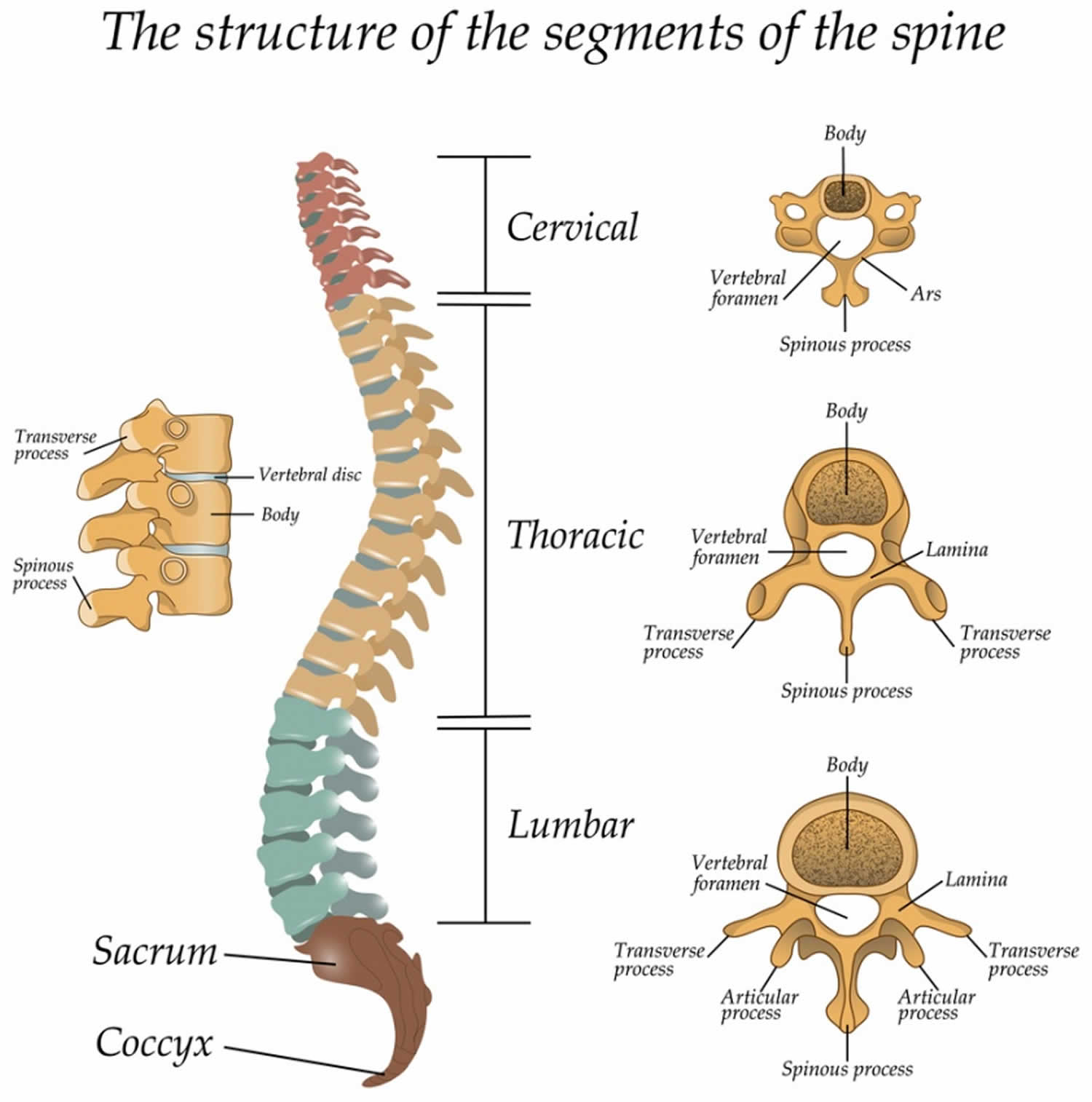

Figure 2. Thoracic vertebrae
Thoracic vertebrae blood supply and lymphatics
Thoracic vertebrae are mainly supplied by branches of the posterior intercostal arteries. The first two posterior intercostal arteries branch off of the subclavian artery while the remaining branch off of the thoracic aorta. These main arteries branch out into the periosteal and equatorial arteries, which in turn branch into anterior and posterior canal branches. Anterior vertebral canal branches send nutrient arteries into the vertebral body to supply the red marrow.
Spinal veins form venous plexuses inside and outside the vertebral canal. These plexuses are valve-less and allow for the movement of blood superiorly or inferiorly depending on pressure gradients. The blood eventually drains into the segmental veins of the trunk.
Thoracic vertebrae nerves
Meningeal branches of spinal nerves innervate all thoracic vertebrae.
Thoracic vertebrae function
Thoracic vertebrae facets and demifacets devoted to rib articulation demonstrate the main function of the thoracic vertebrae. The zygapophyseal joints are tight enough to protect vital organs but loose enough to allow for respiratory movements as well as to allow the thoracic segment to have the greatest freedom of rotation of the entire spine. The zygapophyseal joints, as well as the relatively thin intervertebral discs, cause the thoracic region to have the least flexion/extension ability of the spine. Also, the noted increase in vertebral body size as the spinal column descends is directly related to the increased weight-bearing requirement; further down the column, the greater the proportion of body mass that rests upon it.
Thoracic vertebrae injury
Approximately 90% of all spinal injuries involve the thoracolumbar region (T10-L2), 50% of which can be unstable and lead to a neurological deficit 3.
The thoracic vertebrae has a relatively narrow vertebral canal, which predisposes it to spinal cord damage and neurological deficit. However, due to the orientation of the facet joints, the thin intervertebral discs, and the ribcage, the thoracic vertebrae are functionally rigid. Therefore, it requires a greater amount of energy (force of trauma) to produce fractures and dislocations.
As T12 has characteristics of both thoracic and lumbar vertebrae, it is subject to transitional stresses. These transitional forces are due to the change from the rigid thoracic spine to the relatively mobile lumbar spine. This causes it to be the most commonly fractured vertebra.
The valve-less vertebral venous plexuses allow for the metastasis of cancer from the pelvis, such as that of the prostatic, to the vertebral column.
Thoracic vertebrae fracture
A thoracic vertebrae fracture is a serious condition.
There are twelve vertebrae (blocks of bone) in the thoracic (chest) region at the back. They form attachment for the ribs of the chest.
Types of thoracic vertebrae fractures
Fractures are categorized according to the patterns seen on imaging. These can help decide what treatment you will need.
Some of the types of fractures in the thoracic and lumbar region include:
- compression fracture
- axial burst fracture
- chance (extension) fracture
- transverse process fracture
- fracture dislocation
Thoracic vertebrae fracture causes
Any fracture may occur under direct force to the bone or if you stretch, bend or turn excessively.
Some scenarios that cause fractures in the thoracic and lumbar region include:
- High-impact accidents – car accidents, high-impact sports, fights.
- Fall onto a hard surface.
Less commonly:
- Conditions involving weak bone, such as tumors.
Risk factors for thoracic vertebrae fracture
- Activities that increase the risk of heavy impact to the back such as high-velocity sports.
- Osteoporosis in the elderly.
- Long-term steriod use causing weaken bones.
- A history of cancer.
- A history of infection in the back area.
Thoracic vertebrae fracture prevention
- Wear protective gear in high impact sports.
- Drive safely and carefully.
- Avoid fights.
- Ensure the health of your bones – ask your family doctor to check for osteporosis and take calcium supplements if necessary.
Thoracic vertebrae fracture symptoms
- Pain in upper back and neck that is worse with movement.
- Numbness and tingling sensations.
- Weakness of the arms and back.
- Problems with the bladder and bowel.
- Loss of consciousness (black-outs)
Spinal fractures can cause devastating consequences or mild changes depending on the mode and severity of injury.
Fractures especially caused by high energy impacts can leave a person without function of the muscles and nerves below it, that often cannot be recovered. High impact accidents usually cause other injuries to the rest of the body that increases the number of complications.
In certain cases where the fracture is caused by brittle bones (osteoporosis) or infection or tumor, function can regain if the cause is treated but residual weakness and deformity can often be the case.
Thoracic vertebrae fracture diagnosis
Immediately after the injury:
- It is important never to move a person with a spinal injury until a doctor has seen him or her. Call the ambulance immediately.
History and examination
Your doctor will want to know exactly what happened to cause the injury. It is important that a witness of the accident or event be present to describe the event. Your doctor will also perform a thorough examination to ascertain the severity of the injury and if anywhere else in your body is hurt.
Imaging
This is crucial in determining where is the fracture and what should be done about it.
Your doctor will request one or more of the following investigations:
- Xrays
- CT scan
- MRI
Thoracic vertebrae fracture treatment
The main goals of treatment are to restore stability of the spine and the function of the nerves as much as possible. This can be achieved by two ways:
Non-surgical
A brace can be worn around the back and chest for support as the injury heals. You will still be able to walk and move around and pain can be controlled by analgesic medications (pain killers).
Treatment goals include protecting nerve function and restoring alignment and stability of the spine. The doctor determines the best treatment method based upon fracture type and other factors.
Surgical
Often if the spine is found to be unstable, screws and metal plates will need to be inserted around the spine to prevent further injuries.
- DeSai C, Agarwal A. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Dec 13, 2018. Anatomy, Back, Vertebral Column[↩]
- Waxenbaum JA, Futterman B. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Dec 13, 2018. Anatomy, Back, Intervertebral Discs[↩]
- Waxenbaum JA, Futterman B. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Dec 6, 2018. Anatomy, Back, Cervical Vertebrae[↩]





{kind=link}