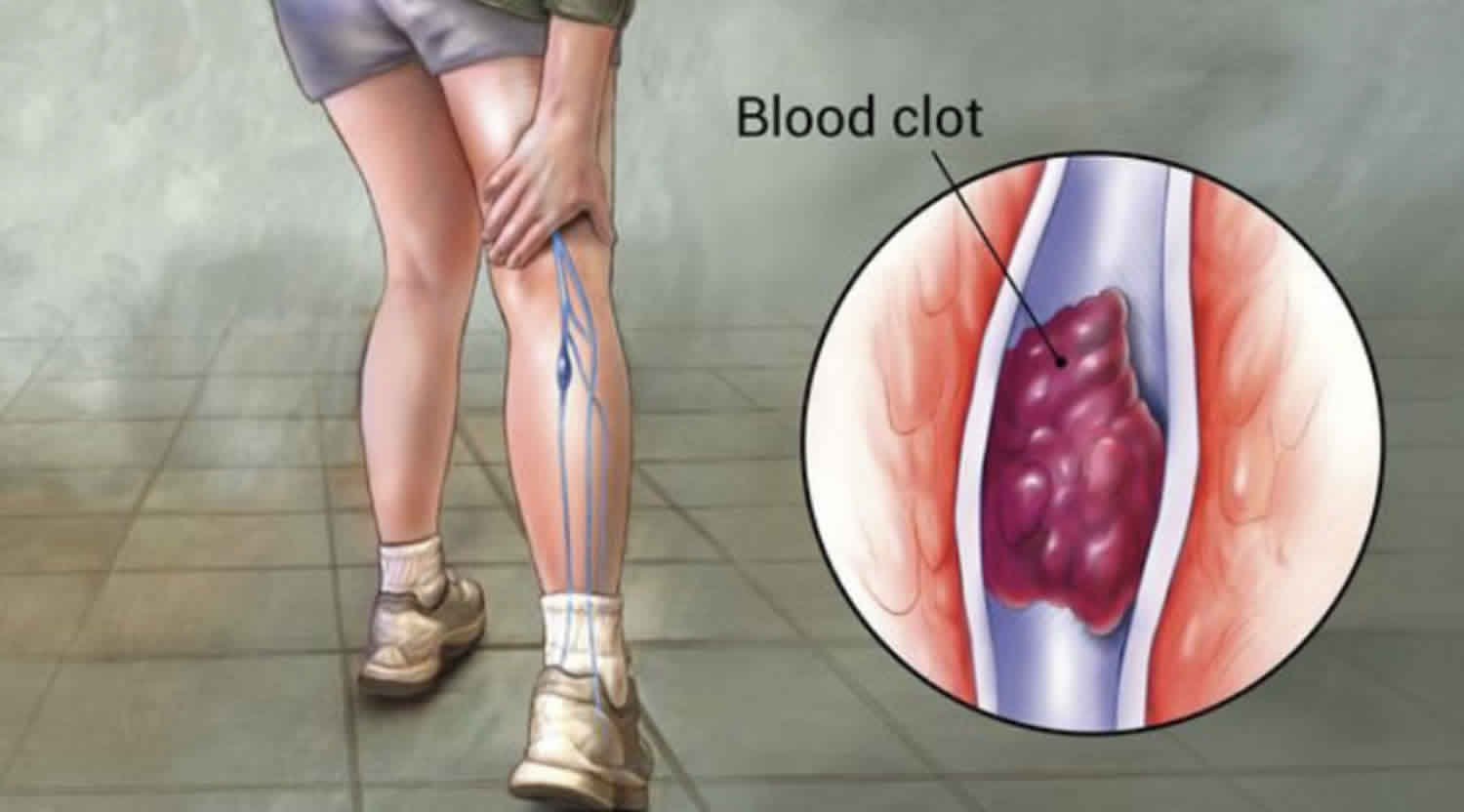
What is thrombus
Thrombus is a blood clot that forms either in a vein or an artery even though you are not bleeding. Normally, thrombi (thrombus plural) or blood clots only occur when you bleed. The blood gets thicker so that the bleeding stops. If you did not get blood clots, you would bleed to death. Thrombus is classified into 3 major groups depending on the relative amount of platelets and red blood cell 1. Three major groups are white thrombus, characterized by a predominance of platelets; red thrombus characterized by a predominance of red blood cell; and mixed with features of both white and red thrombus. Thrombus may be mobile, a characteristic which has been associated with a higher embolic potential. On occasion, fresh thrombus take on a cystic appearance. This is due to a combination of factors including varying degrees of maturity of the clot and results in acoustic boundaries between relatively fresh and more organized regions.
Mural thrombus
Mural thrombus is thrombus that attaches to the wall of a blood vessel and cardiac chamber 1. Mural thrombus occurrence in a normal or minimally atherosclerotic vessel is a rare entity in the absence of a hypercoagulative state or inflammatory, infectious, or familial aortic ailments. Mural thrombus can be seen in large vessels such as the heart and aorta and can restrict blood flow. They are mostly located in the descending aorta, and less commonly, in the aortic arch or the abdominal aorta. Mural thrombus can invade any cardiac chamber. Left ventricular thrombus is a frequent complication of acute myocardial infarction, mostly with the involvement of cardiac apex. This thrombus can separate from the ventricle and travel through arteries, blocking any blood vessels 2.
The mural thrombus may be symptomatic or may be diagnosed as an incidental finding 1. Symptoms are mainly related to localization of thrombus. Mural thrombus can be incidentally detected lying in walls of the aorta in an asymptomatic patient. Its embolization to brain induces cerebrovascular events, causes mesenteric ischemia in the gut, and causes renal infarction, coronary ischemia in heart, pulmonary infarction, among others. Its presence in the distal part of the vessel can induce ischemia, which can result in limb loss 3.
Before the lytic and urgent interventional era, left ventricular thrombus occurred in 25% to 40% of patients after a first anteroapical myocardial infarction. With the advent of acute reperfusion strategies, there has been a decline in prevalence. The major risk of left ventricular thrombus is subsequent embolization with stroke or major organ loss. Historically, the likelihood of embolic events was greatest in the first 2 weeks after the acute event and tapered off over the ensuing 6 weeks. After this time, there was presumed endothelization of the thrombus with a reduction in its embolic potential. Now, with the use of thrombolytics and anticoagulants, the incidence of thrombi has diminished but not to a great extent.
Mural thrombus causes
Virchow’s triad describes the pathogenesis of thrombus formation. Endothelial injury initiates the process. It is induced by trauma to the endothelium of blood vessels. Abnormal laminar flow induced by turbulence in arteries propagates the process. Valvulitis or an aneurysm induces it. Then hypercoagulability further enhances the thrombosis. Leukemia or coagulation disorders induce hypercoagulability. These 3 factors create a cascade of events leading to the propagation of thrombus that ultimately occludes the vessels and produces complications 4.
Thrombus formation starts in response to injury, activating the hemostatic process. Platelets are activated by exposure of collagen or tissue factor. This causes a further cascade of platelet activation with release of cytokines, ultimately causing thrombus formation. A number of cardiac conditions pose an increased risk to thrombus formation. These include atrial fibrillation, heart valve replacement, deep venous thrombosis, acute myocardial infarction, and genetic coagulation disorder. The whole process is regulated by thermoregulation. Large thrombus in a vessel can occlude a vessel and can induce ischemia, also termed as mural thrombi, resulting in the death of tissue. Sometimes thrombi are free-floating and can dislodge to the distal vessel. Embolization to the brain can lead to stroke. Embolization to the limb can lead to amputation.
Mural thrombus diagnosis
Various modalities can help in a diagnosis, but modality of choice for diagnosis of mural thrombus is CT or MRI angiography. These tools are best for determining the location and extent of mural thrombus. These modalities are costly but helpful in prognostication of disease 5. Transoesophageal echocardiography (TEE) is another, relatively noninvasive option and a good tool for diagnosis. Transoesophageal echocardiography (TEE) is an inexpensive, bedside procedure with a low risk of complications. Transoesophageal echocardiography (TEE) is also helpful in diagnosing left ventricle thrombus and aortic atheroma especially in ascending aorta. Both MRI and CT are more sensitive than transoesophageal echocardiography (TEE) in detecting the thrombus in an entire thoracic aorta. Both are usually well tolerated. Other modalities like intravascular ultrasound or optical coherence tomography have opened up a new era of defining thrombus.
Mural thrombus treatment
Treatment of thrombus could reduce the risk of stroke, myocardial infarction, and pulmonary embolism. There are no standardized guidelines for treatment of mural thrombus. Heparin and warfarin are often used to inhibit the initiation and propagation of existing thrombus. Heparin binds to and activates the enzyme inhibitor antithrombusn III, and warfarin inhibits vitamin K epoxide reductase, both enzymes needed to produce clotting factors. Heparin is a preferred drug for dissolving the clot. If thrombus do not resolve after 2 weeks of heparin therapy, then surgery is an option. Thrombolytic therapy is another option for clot dissolution. It includes streptokinase, urokinase, reteplase, and tenecteplase. These are usually administered intravenously. Surgical candidates include younger patients, those having a low risk of perioperative complications, those in whom conservative treatment is unsuccessful, and those who have a highly mobile thrombus with high embolic risk. Surgical procedure includes thrombectomy, segmental aortic resection, thromboaspiration, and endoluminal stent grafts. No approach is definitively superior. Endoluminal stent grafting is the least invasive option, but it carries the high risk of distal embolization through wire manipulation and stent deployment 6.
Thrombus vs Embolus
An embolus is anything that travels through the blood vessels until it reaches a vessel that is too small to let it pass. When this happens, the blood flow is stopped by the embolus. An embolus is often a small piece of a blood clot that breaks off (thromboembolus).
Thrombus vs Thrombosis
Thrombosis is the formation of a blood clot (partial or complete blockage) within vein or an artery even though you are not bleeding, limiting the natural flow of blood and resulting in clinical consequences. The blood clot is known as a thrombus.
The ability of blood to flow freely in vessels relies on complex homeostasis that exists between blood cells (including platelets), plasma proteins, coagulation factors, inflammatory factors and cytokines, and the endothelial lining within the lumen of arteries and veins. When there is an imbalance with this physiologic process, there can be an increased risk of developing a thrombosis versus a coagulopathy (increased risk of bleeding) 7. In certain clinical circumstances, patients can be at increased risk of thrombosis and bleeding simultaneously (e.g., disseminated intravascular coagulopathy-DIC, or in patients with underlying malignancy who develop a coagulopathy). As such, the diagnosis and management of thrombosis are complex. They can arise in any organ system, and their clinical presentation can vary depending on underlying comorbidities and presence (or absence) of provoking factors. Many factors can impact management decisions including whether venous or arterial, acute or chronic, first or subsequent episode, family history, risk factor assessment, and hemodynamic stability. The use and duration of anticoagulation or antiplatelet therapy depend on a careful assessment of these factors. Furthermore, a decision to pursue an exhaustive hypercoagulable workup to further evaluate for inherited or acquired conditions that predispose to thrombosis is controversial and should only be completed in carefully selected patients or with subspecialty hematology evaluation prior.
Together, acute venous and arterial thrombosis accounts for the most common causes of death in developed countries 8. This mortality obviously depends on location and acuity of thrombosis, with myocardial infarction and cerebrovascular accident (CVA) or stroke accounting for the highest proportion of thrombosis-associated death in the United States 8. An understanding of the basic pathophysiology of thrombosis and provoking risk factors can aid clinicians in the diagnosis, workup, and management of this condition. However, the topic is incredibly broad with many management-specific differences and decisions depending on etiology, risk factors, the location of thrombus (venous or arterial), and selection of anticoagulant or antiplatelet therapy. Many patients may require subspecialty evaluation with cardiologists, pulmonologists, neurologist, and/or hematologists. The state of the science on arterial and venous thrombosis is continually evolving, as is our understanding of provoking risk factors, hypercoagulability testing, and medical management.
There are also many unique presentations that add complexity to the diagnosis and treatment decisions, such as in acquired anti-phospholipid syndrome or with heparin-induced thrombocytopenia & thrombosis (HITT). As such, many of these case- or disease-specific details and management aspects are beyond the scope of this review article. Readers are encouraged to consult additional references for further reading, including regularly updated subspecialty society guidelines (e.g., American Society of Chest Physicians, American Heart Association, & American Society of Hematology). This review will focus primarily on the basic pathophysiology of venous and arterial thrombosis, including assessment of provoking risk factors and further workup that may be advisable following the initial presentation. This article will also briefly review the management of venous thrombosis and thromboembolism.
Thrombus formation
The cause of thrombosis is multifactorial. As noted, thrombosis occurs when there is an imbalance in endogenous anticoagulation and hemostasis through a complex pathophysiologic mechanism. Historically, three common factors predispose to thrombosis: 1) damage to the endothelial lining of the vessel wall; 2) a hypercoagulable state, and 3) arterial or venous blood stasis. These three factors are known by the eponym “Virchow’s triad.” Rudolf Virchow proposed Virchow’s triad in 1856, and he described how the presence of these three factors increases thrombosis. Endothelial wall damage is caused by different factors, which can include direct disruption of the vessel via catheter placement, trauma, or surgery. Hypercoagulability is a general hematologic concept that merely means increased risk of thrombosis (i.e., thrombogenic) via enhanced levels of prothrombotic components in the bloodstream. This hypercoagulability is due to a variety of alterations in the coagulation and hemostatic system which can result from inflammatory factors, variations in the viscosity of blood and blood components, increased cytokines and prothrombotic proteins in circulation, or deficiencies of natural or endogenous anticoagulant factors. Hypercoagulable states can be acquired or inherited. Inherited forms are rare, but include examples such as antithrombin III deficiency, protein C and S deficiencies, factor V Leiden (activated protein C resistance), or prothrombin gene mutations (among many others). Acquired hypercoagulability is far more common and can result from medications (e.g., oral contraceptives, estrogen or other hormonal replacement), recent inflammatory conditions such as pregnancy, surgery, trauma, or infection and chronic inflammatory conditions (e.g., morbid obesity, rheumatologic disease, ulcerative colitis, heavy smoking). Two specific types of acquired hypercoagulable states that can lead to both venous and arterial thrombus include the acquired antiphospholipid syndrome and heparin-induced thrombocytopenia & thrombosis (HITT); although beyond the scope of this review, clinicians must be aware of these conditions as potential contributors to acute thrombosis. Malignancy (occult or diagnosed) is also a well-known risk factor for hypercoagulability, as tumor cells can express a variety of procoagulant proteins including increased expression tissue factor. In fact, some malignancies, especially solid tumors, are known to significantly increase the risk of thrombosis (e.g., pancreatic cancer). The third aspect of Virchow’s triad includes arterial or venous stasis of the blood, which could be due to immobility, pregnancy, or impaired blood flow resulting from previous thrombosis (e.g., residual blood clot, remodeling or fibrosis of blood vessels, or atherosclerosis). Long trips with limited mobility can also become a relative risk factor for thrombosis, especially if concurrent additional risk factors are present (as above).
Thus when evaluating any thrombosis, one must appreciate Virchow’s triad and carefully consider the various provoking risk factors that can predispose to thrombosis. Typically, venous thrombosis is initiated by endothelial damage while arterial thrombosis initiates by atherosclerosis. However, some studies have proven that there is a link between these two types of thrombosis. For instance, Prandoni et al. 9 speculated that these two types of thrombosis are triggered by the same biological stimuli that activate coagulation and inflammatory pathways. Both kinds of thrombosis have similar risk factors including age, obesity, smoking, chronic inflammation, metabolic syndrome as well as others previously described. Upon identification of a confirmed thrombosis, a clinician should carefully assess whether any provoking factors may have predisposed to the clot. In other words, it is paramount to determine whether the thrombosis was likely provoked or unprovoked, as each has management implications. Knowledge of the location (e.g., proximal vs. distal) and extent of the thrombosis can also guide further workup and may alter the treatment approach.
When considering venous thromboembolism (VTE), an appreciation of the anatomy of the deep veins of the extremities and the pulmonary system is helpful. For example, the deep veins of the lower extremity include the femoral, iliac and popliteal veins. Thrombosis can also occur in the veins of the upper extremity like in the subclavian, axillary, brachial veins. Other thrombosis sites include superior vena cava thrombosis, jugular vein thrombosis, cerebral venous sinus thrombosis, cavernous sinus thrombosis, retinal vein occlusion. The latter sites are less common, and with the identification of an isolated thrombus in one of these sites, one must consider the potential for other explanatory diagnoses or predisposing conditions (e.g., Budd-Chiari syndrome with hepatic thrombus or cirrhosis and associated splenic vein thrombus). Many myeloproliferative disorders or clonal disorders with acquired bone marrow failure have correlations with rare sites of venous or arterial thrombosis (e.g., paroxysmal nocturnal hemoglobinuria (PNH) may have cerebral venous or abdominal thrombosis as presenting feature). Thrombosis of superficial veins is also possible, especially with provoking factors such as intravenous catheterization or localized cellulitis; treatment of superficial vein thrombosis does not typically require any anticoagulation.
As noted, arterial thrombosis can present as an acute stroke, myocardial infarction, or as acute on chronic peripheral arterial disease. Other less common sites can include renal arteries, mesenteric arteries, and retinal arteries. In addition to acute management (not reviewed here), secondary prevention focuses on reducing cardiovascular risk factors such as obesity, high cholesterol, diabetes, high blood pressure and encouraging lifestyle modification such as smoking cessation. The increased incidence of obesity, hypertension, and hypercholesterolemia all contribute to the risk of acquiring an arterial thrombosis 10. Other risk factors include underlying connective tissue or rheumatologic conditions (e.g., SLE, vasculitis), as well as the aforementioned rare heparin-induced thrombocytopenia and thrombosis (HITT), antiphospholipid syndrome, myeloproliferative disorders and paroxysmal nocturnal hemoglobinuria (PNH) (all of these can predispose to both venous and arterial thrombosis).
Age and gender also contribute to the development of thrombosis, with advancing age associated with a relative increased risk of thrombosis. For instance, studies have shown that elderly persons have increased production of prothrombotic coagulation factors such as von Willebrand factor and thrombin. The elderly also may experience a normal physiologic activation of platelets compared to younger persons 11.
Thrombus pathophysiology
As noted, Virchow’s triad (i.e., endothelial damage, hypercoagulability, & venous or arterial blood stasis) plays a significant role in the pathophysiology of thrombosis. Damage to the vessel wall leads to the production of proinflammatory (and prothrombotic) cytokines, increase in available tissue factor, the proliferation of adhesion molecules and enhanced platelet activation. Cytokines initiate inflammation promoting interaction between leukocytes and endothelial cells 12. Inflammation is a normal body reaction to unwanted stimuli such as foreign pathogens or infection, and endothelial damage whether acute (e.g., trauma or surgery) or chronic (underlying inflammatory disorders or peripheral vascular disease). The activation of the leucocytes and endothelial cells causes the formation of adhesion molecules which will eventually initiate clot formation 12. The body’s endogenous anticoagulants, such as protein C and protein S and Antithrombin-III prevent the formation of thrombosis through a complex regulatory mechanism that maintains homeostasis. When an imbalance exists in the formation and lysis of clot, it can generate thrombosis; this explains why patients with thrombophilias such as protein C, protein S and antithrombin III deficiencies are prone to acquiring blood clots. As noted in the cause section, a myriad of additional acquired provoking risk factors and comorbidities (e.g., recent surgery, inflammation, infection, pregnancy, estrogen therapy, morbid obesity, or smoking among others) also increase a chance of developing thrombosis.
Thrombosis occurs throughout our arterial system, especially in those with predisposing cardiovascular risk factors. In the heart, macrothrombi can develop as a result of blood stasis in the ventricles or atria due to underlying valvular heart disease, cardiomyopathies or arrhythmias such as atrial fibrillation predisposing to ischemic emboli and CVA. Arterial thrombosis (and microthrombi formation) typically initiates by the accumulation of lipid plaques in arterial wall provoking chronic inflammatory cells and platelet activation as can be seen with coronary artery disease 13. Platelets play a significant role in the development of arterial thrombosis compared to venous thrombosis, and this explains why antiplatelet agents form a cornerstone of the prevention and treatment of arterial thrombosis. The initial lipid plaques evolve into fibrous plaques. Fibrous plaques could rupture, and the erosion of the surfaces of some of these plaques could lead to the release of additional pro-coagulating factors 13. This process is called atherosclerosis. Atherosclerosis allows the activation of platelets, causing adhesion and aggregation, which leads to the formation of a clot. The occlusion of vessels due to atherosclerosis and thrombin formation in the coronary arteries of the heart may lead to ischemic heart disease and myocardial infarction.
Risk factors for deep vein thrombosis
Many factors can increase your risk of developing deep vein thrombosis (DVT). The more you have, the greater your risk of DVT. Risk factors include:
- Inheriting a blood-clotting disorder. Some people inherit a disorder that makes their blood clot more easily. This condition on its own might not cause blood clots unless combined with one or more other risk factors.
- Prolonged bed rest, such as during a long hospital stay, or paralysis. When your legs remain still for long periods, your calf muscles don’t contract to help blood circulate, which can increase the risk of blood clots.
- Injury or surgery. Injury to your veins or surgery can increase the risk of blood clots.
- Pregnancy. Pregnancy increases the pressure in the veins in your pelvis and legs. Women with an inherited clotting disorder are especially at risk. The risk of blood clots from pregnancy can continue for up to six weeks after you have your baby.
- Birth control pills (oral contraceptives) or hormone replacement therapy. Both can increase your blood’s ability to clot.
- Being overweight or obese. Being overweight increases the pressure in the veins in your pelvis and legs.
- Smoking. Smoking affects blood clotting and circulation, which can increase your risk of DVT.
- Cancer. Some forms of cancer increase substances in your blood that cause your blood to clot. Some forms of cancer treatment also increase the risk of blood clots.
- Heart failure. This increases your risk of DVT and pulmonary embolism. Because people with heart failure have limited heart and lung function, the symptoms caused by even a small pulmonary embolism are more noticeable.
- Inflammatory bowel disease. Bowel diseases, such as Crohn’s disease or ulcerative colitis, increase the risk of DVT.
- A personal or family history of deep vein thrombosis or pulmonary embolism. If you or someone in your family has had one or both of these, you might be at greater risk of developing a DVT.
- Age. Being older than 60 increases your risk of DVT, though it can occur at any age.
- Sitting for long periods of time, such as when driving or flying. When your legs remain still for hours, your calf muscles don’t contract, which normally helps blood circulate. Blood clots can form in the calves of your legs if your calf muscles don’t move for long periods.
Thrombosis prevention
Measures to prevent deep vein thrombosis include:
- Avoid sitting still. If you have had surgery or have been on bed rest for other reasons, try to get moving as soon as possible. If you’re sitting for a while, don’t cross your legs, which can hamper blood flow. If you’re traveling a long distance by car, stop every hour or so and walk around. If you’re on a plane, stand or walk occasionally. If you can’t do that, exercise your lower legs. Try raising and lowering your heels while keeping your toes on the floor, then raising your toes with your heels are on the floor.
- Make lifestyle changes. Lose weight and quit smoking.
- Exercise. Regular exercise lowers your risk of blood clots, which is especially important for people who sit a lot or travel frequently.
Thrombosis complications
A serious complication associated with deep vein thrombosis is pulmonary embolism.
Pulmonary embolism
A pulmonary embolism occurs when a blood vessel in your lung becomes blocked by a blood clot (thrombus) that travels to your lung from another part of your body, usually your leg.
A pulmonary embolism can be life-threatening. It’s important to watch for signs and symptoms of a pulmonary embolism and seek medical attention if they occur. Signs and symptoms of a pulmonary embolism include:
- Sudden shortness of breath
- Chest pain or discomfort that worsens when you take a deep breath or when you cough
- Feeling lightheaded or dizzy, or fainting
- Rapid pulse
- Coughing up blood
Postphlebitic syndrome
A common complication that can occur after deep vein thrombosis is known as postphlebitic syndrome, also called postthrombotic syndrome. Damage to your veins from the blood clot reduces blood flow in the affected areas, which can cause:
- Persistent swelling of your legs (edema)
- Leg pain
- Skin discoloration
- Skin sores
Thrombosis diagnosis
To diagnose deep vein thrombosis, your doctor will ask you about your symptoms. You’ll also have a physical exam so that your doctor can check for areas of swelling, tenderness or discoloration on your skin. Depending on how likely you are to have a blood clot, your doctor might suggest tests, including:
- Ultrasound. A wandlike device (transducer) placed over the part of your body where there’s a clot sends sound waves into the area. As the sound waves travel through your tissue and reflect back, a computer transforms the waves into a moving image on a video screen. A clot might be visible in the image. Sometimes a series of ultrasounds are done over several days to determine whether a blood clot is growing or to check for a new one.
- Blood test. Almost all people who develop severe deep vein thrombosis have an elevated blood level of a substance called D dimer.
- Venography. A dye is injected into a large vein in your foot or ankle. An X-ray creates an image of the veins in your legs and feet, to look for clots. However, less invasive methods of diagnosis, such as ultrasound, can usually confirm the diagnosis.
- CT or MRI scans. Either can provide visual images of your veins and might show if you have a clot. Sometimes these scans performed for other reasons reveal a clot.
Thrombosis treatment
Deep vein thrombosis (DVT) treatment is aimed at preventing the clot from getting bigger and preventing it from breaking loose and causing a pulmonary embolism. Then the goal becomes reducing your chances of deep vein thrombosis happening again.
Deep vein thrombosis treatment options include:
- Blood thinners. Deep vein thrombosis is most commonly treated with anticoagulants, also called blood thinners. These drugs, which can be injected or taken as pills, decrease your blood’s ability to clot. They don’t break up existing blood clots, but they can prevent clots from getting bigger and reduce your risk of developing more clots. The injectable medications can be given as a shot under the skin or by injection into your arm vein (intravenous). Heparin is typically given intravenously. Other similar blood thinners, such as enoxaparin (Lovenox), dalteparin (Fragmin) or fondaparinux (Arixtra), are injected under the skin. You might receive an injectable blood thinner for a few days, after which pills such as warfarin (Coumadin, Jantoven) or dabigatran (Pradaxa) are started. Once warfarin has thinned your blood, the injectable blood thinners are stopped. Other blood thinners can be given in pill form without the need for an injectable blood thinner. These include rivaroxaban (Xarelto), apixaban (Eliquis) or edoxaban (Savaysa). You might need to take blood thinner pills for three months or longer. It’s important to take them exactly as your doctor instructs because taking too much or too little can cause serious side effects. If you take warfarin, you’ll need periodic blood tests to check how long it takes your blood to clot. Pregnant women shouldn’t take certain blood-thinning medications.
- Clot busters. If you have a more serious type of deep vein thrombosis or pulmonary embolism, or if other medications aren’t working, your doctor might prescribe drugs that break up clots quickly, called clot busters or thrombolytics. These drugs are either given through an IV line to break up blood clots or through a catheter placed directly into the clot. These drugs can cause serious bleeding, so they’re generally reserved for severe cases of blood clots.
- Filters. If you can’t take medicines to thin your blood, you might have a filter inserted into a large vein — the vena cava — in your abdomen. A vena cava filter prevents clots that break loose from lodging in your lungs.
- Compression stockings. To help prevent swelling associated with deep vein thrombosis, these are worn on your legs from your feet to about the level of your knees. This pressure helps reduce the chances that your blood will pool and clot. You should wear these stockings during the day for at least two years, if possible.
Lifestyle and home remedies
Once you receive treatment for deep vein thrombosis (DVT), you need to watch your diet and watch for signs of excessive bleeding, as well as take steps to prevent another DVT. Some things you can do include:
- Check in with your doctor regularly to see if your treatment needs to be modified. If you’re taking warfarin (Coumadin, Jantoven), you’ll need a blood test to see how well your blood is clotting.
- Take your blood thinners as directed. If you’ve had DVT, you’ll be on blood thinners for at least three to six months.
- Watch for excessive bleeding, which can be a side effect of taking blood thinners. Talk to your doctor about activities that could cause you to bruise or get cut, as even a minor injury could become serious if you’re taking blood thinners.
- Move. If you’ve been on bed rest because of surgery or other factors, the sooner you get moving, the less likely blood clots will develop.
- Wear compression stockings to help prevent blood clots in the legs if your doctor recommends them.
- Singh DP, Basit H, Malik A, et al. Mural Thrombi. [Updated 2019 May 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534294[↩][↩][↩]
- Perini P, Bianchini Massoni C, Azzarone M, Ucci A, Rossi G, Gallitto E, Freyrie A. Significance and Risk Factors for Intraprosthetic Mural Thrombus in Abdominal Aortic Endografts: A Systematic Review and Meta-analysis. Ann Vasc Surg. 2018 Nov;53:234-242[↩]
- Cicenia M, Fedele F, Petronilli V, De Carlo C, Moscucci F, Schina M, Sciomer S. Hidden in the heart: A peculiar type of left ventricular remodeling after acute myocardial infarction. Echocardiography. 2017 Nov;34(11):1738-1739[↩]
- Eren N, Gungor O, Kocyigit I, Guzel FB, Erken E, Altunoren O, Tatar E, Eroglu E, Senel E, Kaya B, Paydaş S, Onan B, Sahin S, Yilmaz M, Ulu S, Gursu M, Ozkok A, Yildiz A, Kurultak I, Ucar AR, Tanrisev M, Turgutalp K, Turan MN, Huzmeli C, Soypacaci Z, Akdam H, Huddam B, Adibelli Z, Kara E, Inci A, Turkmen E, Tekce H, Dogukan A, Turkmen A. Acute renal infarction in Turkey: a review of 121 cases. Int Urol Nephrol. 2018 Nov;50(11):2067-2072[↩]
- Desouza N, Sood A, Baciewicz FA, Cardozo S. Traumatic Aortic Mural Thrombus Diagnosed Echocardiographically before Thoracic Endovascular Aortic Repair. Tex Heart Inst J. 2018 Jun;45(3):188-189[↩]
- DeKornfeld GM, Boll J, Ziegler KR, Ratcliff J, Naslund TC, Garrard CL, Valentine RJ, Curci JA. Initial and intermediate-term treatment of the phantom thrombus (primary non-occlusive mural thrombus on normal arteries). Vasc Med. 2018 Aug 19;:1358863X18788952[↩]
- Ashorobi D, Fernandez R. Thrombosis. [Updated 2019 May 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538430[↩]
- Mackman N. Triggers, targets and treatments for thrombosis. Nature. 2008 Feb 21;451(7181):914-8[↩][↩]
- Prandoni P. Venous and Arterial Thrombosis: Is There a Link? Adv. Exp. Med. Biol. 2017;906:273-283.[↩]
- Lowe GD. Venous and arterial thrombosis: epidemiology and risk factors at various ages. Maturitas. 2004 Apr 15;47(4):259-63[↩]
- Favaloro EJ, Franchini M, Lippi G. Aging hemostasis: changes to laboratory markers of hemostasis as we age – a narrative review. Semin. Thromb. Hemost. 2014 Sep;40(6):621-33[↩]
- Mosevoll KA, Johansen S, Wendelbo Ø, Nepstad I, Bruserud Ø, Reikvam H. Cytokines, Adhesion Molecules, and Matrix Metalloproteases as Predisposing, Diagnostic, and Prognostic Factors in Venous Thrombosis. Front Med (Lausanne). 2018;5:147[↩][↩]
- Insull W. The pathology of atherosclerosis: plaque development and plaque responses to medical treatment. Am. J. Med. 2009 Jan;122(1 Suppl):S3-S14[↩][↩]





{kind=link}