
What is Tinel’s sign
Tinel sign is the tapping on the wrist over the median nerve with a reflex hammer which may cause an electric shock-like sensation shooting from your wrist to your hand in people with carpal tunnel syndrome. Tinel’s sign over the median nerve is described as a tingling sensation in the thumb, index and middle finger after light tapping or percussion over that nerve. A true Tinel’s sign may be uncomfortable for the patient, but it is never painful. Another test called the Phalen test to diagnose carpal tunnel syndrome involves bending your wrist at a 90 degree angle for one minute may cause symptoms of numbness, tingling, or weakness to appear in your hand. The reverse Phalen’s, or ‘prayer test,’ is done by having the patient extend both of their wrists by placing palmar surfaces of both hands together for 1 minute (as if praying). Again a positive test is with reproduction of symptoms.
Diagnosis of carpal tunnel syndrome based on an accurate description of the symptoms a patient is experiencing. During physical examination, testing may identify weakness of the muscles supplied by the median nerve in the hand, including some thumb muscles affected by the syndrome. There may be decreased sensation in the hand when pricked with a pin or lightly touched.
Health care professionals can confirm the diagnosis of carpal tunnel syndrome and determine its severity with a two-part electrical test called the nerve conduction test. The nerve conduction test is the strongest evidence for carpal tunnel syndrome.
During the first part of the test, a small electrode that generates a mild electrical current is placed on the skin on the elbow side of the tunnel. This current stimulates the median nerve. The impulse from the stimulation travels down the nerve, through the tunnel, and to the hand – where the doctor will measure how long it took for the impulse to get there. If the median nerve is damaged, the impulse will take longer than expected to get to the hand. The worse the nerve damage is, the longer it will take for the impulse to get to the hand.
The second part of the test is called electromyography. It measures how badly the muscle is functioning. A small needle is placed in various muscles that receive impulses from the median nerve. The electrical impulses in the muscle are measured when the muscle is not being used and when the muscle is being used. If the median nerve is severely squeezed, these muscles can be affected and will not perform normally during the test.
Diagnostic ultrasonography and MRI have been used to help diagnose carpal tunnel syndrome and exclude other causes of hand and wrist symptoms. These technologies can identify swelling of the median nerve and abnormalities of the tunnel wall, its contents and surrounding area. They can also help determine why the median nerve is being squeezed, or compressed. For example, inflammation of structures in the tunnel like inflamed tendons might be causing the median nerve to be compressed. This can occur in rheumatoid arthritis. Other tendon abnormalities, such as excessive fat in the tunnel (also called a ganglion) also can be seen using MRI.
Tinel’s sign wrist
Carpal tunnel syndrome is an entrapment neuropathy caused by compression of the median nerve as it travels through the wrist’s carpal tunnel 1. Carpal tunnel syndrome is the most common nerve entrapment neuropathy, accounting for 90% of all neuropathies. In the United States, carpal tunnel syndrome has an incidence of 1 to 3 persons per 1000 per year, with a prevalence of 50 per 1000, with similar incidence and prevalence in most developed countries 1. Carpal tunnel syndrome most commonly affects whites, has up to a 10 to 1 predominance in females, and has a peak age of 46 to 60 2. The carpal tunnel is located at the wrist on the palm side of the hand just beneath the skin surface (palmar surface). Eight small wrist bones form three sides of the tunnel, giving rise to the name carpal tunnel. The remaining side of the tunnel, the palmar surface, is composed of soft tissues, consisting mainly of a ligament called the transverse carpal ligament. This ligament stretches over the top of the tunnel.
The median nerve and nine flexor tendons to the fingers pass through the carpal tunnel. Flexor tendons help flex or bend the fingers. When the median nerve in the wrist is squeezed (by swollen tissues, for example), it slows or blocks nerve impulses from travelling through the nerve. Because the median nerve provides muscle function and feeling in the hand, this causes symptoms ranging from mild occasional numbness to hand weakness, loss of feeling and loss of hand function.
Carpal tunnel syndrome results from increased pressure carpal tunnel pressure and subsequent compression of the median nerve. The most common causes of carpal tunnel syndrome include genetic predisposition, history of repetitive wrist movements such as typing, or machine work as well as obesity, autoimmune disorders such as rheumatoid arthritis, and pregnancy 3.
Usually carpal tunnel syndrome affects only one hand, but can affect both at the same time, causing symptoms in the thumb and the index, middle and ring fingers. In addition to numbness, patients with carpal tunnel syndrome may experience tingling, a pins and needle sensation or burning of the hand occasionally extending up to the forearm.
Frequently, symptoms appear in the morning after a person wakes up, but they can also happen during the night and interrupt their sleep. Symptoms can occur with certain activities such as driving, holding a book or other repetitive activity with the hands, especially activities that require a person to grasp something for long periods of time or bend their wrist. Activities that require use of the hands, such as buttoning a shirt, may become difficult, and carpal tunnel sufferers may drop things more easily. Individuals will often shake their hands trying to obtain relief and may feel that their hand is swollen when no swelling is present.
Because numbness and tingling may be mild and occur only periodically, many do not seek medical help. However, the disease can progress to more persistent numbness and burning. In some severe and chronic cases of carpal tunnel syndrome, loss of muscle mass occurs at the base of the thumb on the palm side of the hand. In these instances, especially when untreated, individuals can experience hand weakness, impaired use of the hand, and loss of sensation in their hand due to permanent nerve and muscle damage.
Carpal tunnel syndrome results from increased pressure carpal tunnel pressure and subsequent compression of the median nerve. The most common causes of carpal tunnel syndrome include genetic predisposition, history of repetitive wrist movements such as typing, or machine work as well as obesity, autoimmune disorders such as rheumatoid arthritis, and pregnancy 4.
Carpal tunnel syndrome treatment includes resting your hand, splints, pain and anti-inflammatory medicines, and sometimes surgery.
Figure 1. Carpal tunnel syndrome

Figure 2. Carpal tunnel (cross section view)

What causes carpal tunnel syndrome?
Carpal tunnel syndrome may occur in patients who are pregnant, overweight or have various medical conditions, including thyroid disease, diabetes or arthritis, or injuries such as wrist fractures. It is still debated whether repetitive work activities cause carpal tunnel syndrome, but it is thought that some repetitive hand activities, especially motions that can produce vibrations, can worsen the symptoms. Just as frequently, the syndrome occurs on its own.
However, many other conditions also can be responsible for symptoms of pain, swelling, numbness or weakness in the hands, such as diseases of the nerves located anywhere from the neck to the wrist. The pain and swelling in the hand joints and wrists caused by arthritis also can be responsible. For example, pain at the base of the thumb is commonly caused by osteoarthritis. Tendonitis – an inflammation of the tendons that connect muscles to bones – can cause pain, swelling, and impaired use of the hand or wrist. Raynaud’s phenomena can cause numbness and burning of the fingers as a result of cold exposure and sometimes due to autoimmune diseases. Raynaud’s also causes fingers to have a whitish, bluish or reddish color at various times; color changes are not seen in carpal tunnel syndrome. Health care professionals should exclude these and other diseases before diagnosing carpal tunnel syndrome.
Typical occupations of patients with carpal tunnel syndrome include those who use computers for extended periods of time, those who use equipment that has vibration such as construction workers, and any other occupation requiring frequent, repetitive movement 5.
Carpal tunnel syndrome symptoms
Early symptoms of carpal tunnel syndrome include pain, numbness, and paresthesias. These symptoms typically present, with some variability, in the thumb, index finger, middle finger, and the radial half (thumb side) of the ring finger. Pain also can radiate up the affected arm. With further progression, hand weakness, decreased fine motor coordination, clumsiness, and thenar atrophy can occur.
In the early presentation of the disease, symptoms most often present at night when lying down and are relieved during the day. With further progression of the disease, symptoms will also be present during the day, especially with certain repetitive activities, such as when drawing, typing, or playing video games. In more advanced disease, symptoms can be constant.
Carpal tunnel syndrome diagnosis
Diagnosis of carpal tunnel syndrome based on an accurate description of the symptoms a patient is experiencing. During physical examination, testing may identify weakness of the muscles supplied by the median nerve in the hand, including some thumb muscles affected by the syndrome. There may be decreased sensation in the hand when pricked with a pin or lightly touched. Bending the wrist at a 90 degree angle for one minute may cause symptoms to appear in the hand (Phalen test), or tapping on the wrist with a reflex hammer may cause an electric shock-like sensation (Tinel Sign). Late in the disease, the muscles might be thinning or declining at the base of the thumb.
Health care professionals can confirm the diagnosis of carpal tunnel syndrome and determine its severity with a two-part electrical test called the nerve conduction test. The nerve conduction test is the strongest evidence for carpal tunnel syndrome.
During the first part of the test, a small electrode that generates a mild electrical current is placed on the skin on the elbow side of the tunnel. This current stimulates the median nerve. The impulse from the stimulation travels down the nerve, through the tunnel, and to the hand – where the doctor will measure how long it took for the impulse to get there. If the median nerve is damaged, the impulse will take longer than expected to get to the hand. The worse the nerve damage is, the longer it will take for the impulse to get to the hand.
The second part of the test is called electromyography. It measures how badly the muscle is functioning. A small needle is placed in various muscles that receive impulses from the median nerve. The electrical impulses in the muscle are measured when the muscle is not being used and when the muscle is being used. If the median nerve is severely squeezed, these muscles can be affected and will not perform normally during the test.
Diagnostic ultrasonography and MRI have been used to help diagnose carpal tunnel syndrome and exclude other causes of hand and wrist symptoms. These technologies can identify swelling of the median nerve and abnormalities of the tunnel wall, its contents and surrounding area. They can also help determine why the median nerve is being squeezed, or compressed. For example, inflammation of structures in the tunnel like inflamed tendons might be causing the median nerve to be compressed. This can occur in rheumatoid arthritis. Other tendon abnormalities, such as excessive fat in the tunnel (also called a ganglion) also can be seen using MRI.
Carpal tunnel syndrome treatment
Pain medications such as acetaminophen and nonsteroidal anti-inflammatory drugs can be used for symptom relief. Placing a splint on the affected wrist, especially at night, can help keep the wrist straight during the night and decrease the pressure on the median nerve. These splints are available in most drug stores and may relieve symptoms, especially in milder cases.
A cortisone injection into the carpal tunnel area often is helpful in relieving symptoms for weeks to months at a time and can be repeated. If an underlying disease like hypothyroidism (an underactive thyroid) or rheumatoid arthritis is causing the carpal tunnel syndrome, then treatment of the disease also may relieve symptoms.
When the above measures fail to relieve symptoms, surgery may be needed to open the carpal tunnel and relieve the pressure on the median nerve. This is known as a carpal tunnel release. In severe cases, physicians may consider surgery early on before trying other methods. The surgery may be an open surgical procedure or an endoscopic procedure and often can be done on an outpatient basis.
Tinel’s sign ankle
Tarsal tunnel syndrome, sometimes referred to as tibial nerve dysfunction or posterior tibial nerve neuralgia, is an entrapment neuropathy that is associated with the compression of the structures within the tarsal tunnel 6. Tarsal tunnel syndrome is similar to carpal tunnel syndrome of the wrist although much less common 7.
The tarsal tunnel is a narrow fibro-osseous space that runs behind and inferior to the medial malleolus. It is bounded by the medial malleolus anterosuperiorly, by the posterior talus and calcaneus laterally, and is held against the bone by the flexor retinaculum which extends from the medial malleolus to the medial calcaneus and prevents medial displacement of its contents.
The tarsal tunnel is a narrow space that lies on the inside of the ankle next to the ankle bones. The tunnel is covered with a thick ligament (the flexor retinaculum) that protects and maintains the structures contained within the tunnel—arteries, veins, tendons and nerves. One of these structures is the posterior tibial nerve, which is the focus of tarsal tunnel syndrome.
The tarsal tunnel includes multiple important structures. It contains the tendons of the posterior tibialis, flexor digitorum longus (FDL), and flexor hallucis longus (FHL) muscles. The posterior tibial artery and vein, as well as posterior tibial nerve (L4-S3), also pass through it. The orientation of these structures within the tarsal tunnel is noteworthy. From medial to lateral, they are the tibialis posterior tendon, FDL tendon, posterior tibial artery and vein, posterior tibial nerve, and FHL tendon.
The posterior tibial nerve passes between the FDL and FHL muscles before it bifurcates in the tarsal tunnel, forming the medial and lateral plantar nerves. In 5% of people, the bifurcation occurs before the tarsal tunnel. The medial plantar nerve passes deep to the abductor hallucis and FHL muscles and provides sensation to the medial half of the foot and first 3.5 digits and motor function to the lumbricals, abductor hallucis, flexor digitorum brevis, and flexor hallucis brevis. The lateral plantar nerve passes directly through the abductor hallucis muscle belly and provides sensory innervation of the medial calcaneus and lateral heel and motor function to the flexor digitorum brevis, quadratus plantae, and abductor digiti minimi. The medial calcaneal nerve typically branches off of the posterior tibial nerve proximal to the tarsal tunnel and provides sensory innervation to the posteromedial heel. In 25% of patients, it branches off of the lateral plantar nerve or runs superficial to the flexor retinaculum.
Figure 3. Tarsal tunnel syndrome

Figure 4. Tarsal tunnel anatomy
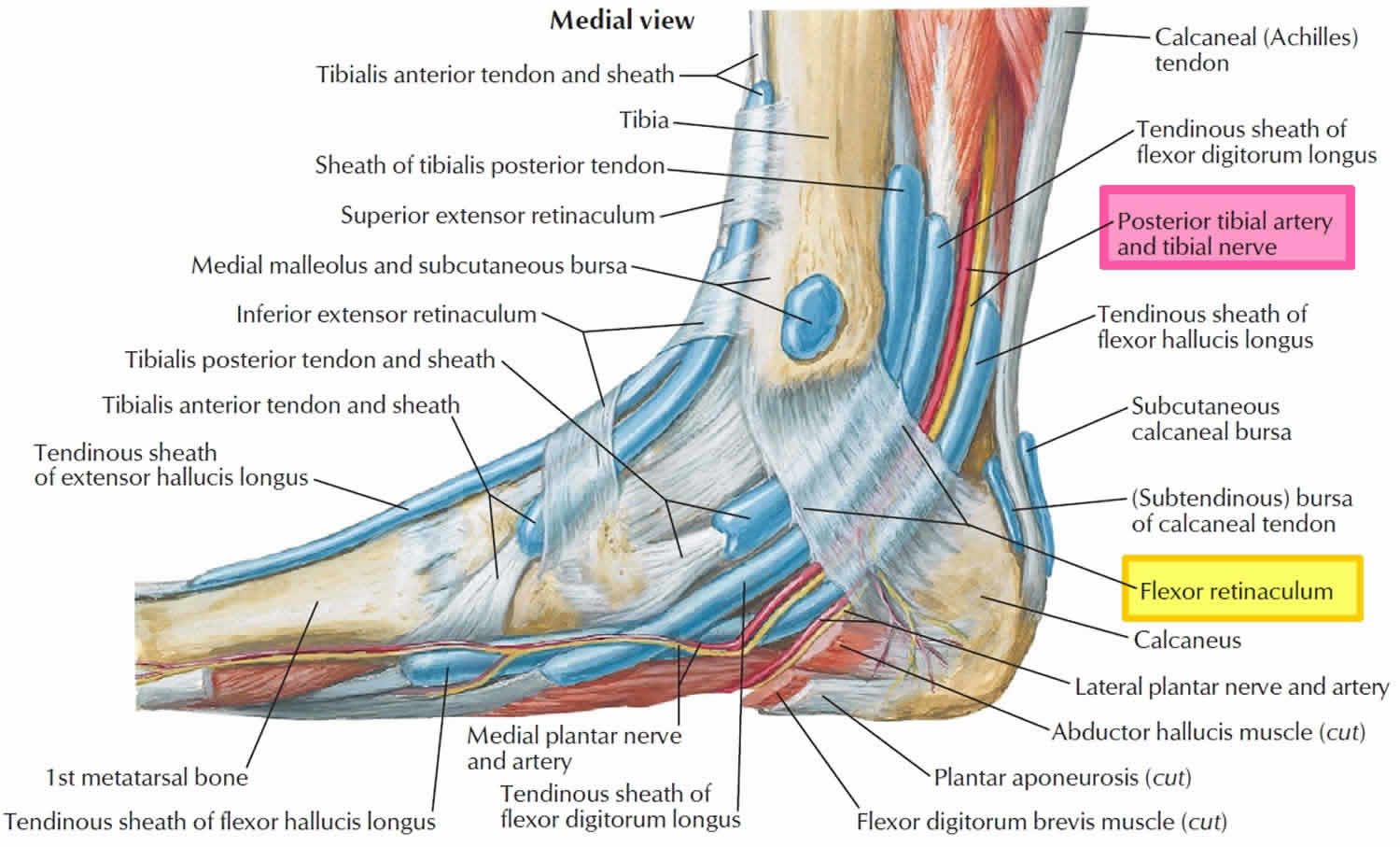
Figure 5. Tibial nerve (posterior tibial nerve and branches)

Tarsal tunnel syndrome causes
Tarsal tunnel syndrome is an unusual form of peripheral neuropathy. Tarsal tunnel syndrome occurs when there is damage to the tibial nerve.
The area in the foot where the nerve enters the back of the ankle is called the tarsal tunnel. This tunnel is normally narrow. When the tibial nerve is compressed, it results in the symptoms of tarsal tunnel syndrome.
Pressure on the tibial nerve may be due to any of the following:
- Swelling from an injury, such as a sprained ankle or nearby tendon
- An abnormal growth, such as a bone spur, lump in the joint (ganglion cyst), swollen (varicose) vein
- Flat feet or a high arch
- Body-wide (systemic) diseases, such as diabetes, low thyroid function, arthritis
In some cases, no cause can be found.
Tarsal tunnel syndrome symptoms
Patients with tarsal tunnel syndrome experience one or more of the following symptoms:
- Shooting pain in the foot
- Numbness
- Tingling or burning sensation
- Pain and tingling around the ankle
- Swelling in the foot
- Pain radiating up into the leg or down into the ankle and foot
- Pins and needles feeling in the foot
Symptoms are typically felt on the inside of the ankle and/or on the bottom of the foot. In some people, a symptom may be isolated and occur in just one spot. In others, it may extend to the heel, arch, toes and even the calf.
Sometimes the symptoms of the syndrome appear suddenly. They are often brought on or aggravated by overuse of the foot, such as in prolonged standing, walking, exercising or beginning a new exercise program.
It is important to seek early treatment if any of the symptoms of tarsal tunnel syndrome occur. If left untreated, the condition progresses and may result in permanent nerve damage. In addition, because the symptoms of tarsal tunnel syndrome can be confused with other conditions, proper evaluation is essential so that a correct diagnosis can be made and appropriate treatment initiated.
Tarsal tunnel syndrome diagnosis
Proper diagnosis of a tarsal tunnel syndrome requires the expert attention of experienced foot and ankle surgeon.
During your medical examination, the surgeon will position your foot and tap on the nerve to see if the symptoms can be reproduced. He or she will also press on the area to help determine if a small mass is present.
Advanced imaging studies may be ordered if a mass is suspected or if initial treatment does not reduce the symptoms. Studies used to evaluate nerve problems—electromyography and nerve conduction velocity (EMG/nerve conduction study)—may be ordered if the condition shows no improvement with nonsurgical treatment.
Tarsal tunnel syndrome test will include:
- Electrical testing (EMG or nerve conduction study)
- Imaging (X-rays, CT, or MRI scans)
Diagnosis is necessary to determine the severity of the condition, so the appropriate treatment plan, including a surgical option, can be considered.
Tarsal tunnel syndrome treatment
Nonsurgical treatment for tarsal tunnel syndrome
Whenever possible, doctors will prescribe nonsurgical treatment options before surgery is recommended. Possible treatment options may include anti-inflammatory medications or steroid injections into the nerves in the tarsal tunnel to relieve pressure and swelling. Orthosis (e.g., braces, splints, orthotic devices) may be recommended to reduce pressure on the foot and limit movement that could cause compression on the nerve.
Many treatment options, often used in combination, are available to treat tarsal tunnel syndrome. These include:
- Rest. Staying off the foot prevents further injury and encourages healing.
- Ice. Apply an ice pack to the affected area, placing a thin towel between the ice and the skin. Use ice for 20 minutes and then wait at least 40 minutes before icing again.
- Oral medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation.
- Immobilization. Restricting movement of the foot by wearing a cast is sometimes necessary to enable the nerve and surrounding tissue to heal.
- Physical therapy. Ultrasound therapy, exercises and other physical therapy modalities may be prescribed to reduce symptoms.
- Injection therapy. Injections of a local anesthetic provide pain relief, and an injected corticosteroid may be useful in treating the inflammation.
- Orthotic devices. Custom shoe inserts may be prescribed to help maintain the arch and limit excessive motion that can cause compression of the nerve.
- Shoes. Supportive shoes may be recommended.
- Bracing. Patients with flatfoot or those with severe symptoms and nerve damage may be fitted with a brace to reduce the amount of pressure on the foot.
Tarsal tunnel syndrome surgery
The foot and ankle surgeon will determine if surgery is necessary and will select the appropriate procedure or procedures based on the cause of the condition. Depending on the severity of the condition, one of several surgical options may be recommended, including tarsal tunnel release.
Complications are associated with tarsal tunnel decompression surgery may include nerve or artery laceration and plantar fasciitis 8. One small study reviewed the results of 30 patients who underwent decompression surgery for tarsal tunnel syndrome and reported a 13 percent complication rate 9. In this study, three individuals had wound infections and one person had a delay in wound healing.
Tinel’s sign elbow
Tinel’s sign at the elbow is used to detect ulnar nerve entrapment at the elbow commonly known as cubital tunnel syndrome 10. To perform this test, have the patient’s elbow in a flexed position. Supporting the patient’s wrist with one hand, use the other hand to tap lightly at the medial cubital fossa. A positive test is reported when the patient experiences paraesthesias in the medial aspect of the forearm and/or into the medial one and a half fingers.
Cubital tunnel syndrome is a neuropathy of the ulnar nerve causing symptoms of numbness and shooting pain in the medial aspect of the forearm, also including the medial half of the fourth digit and the fifth digit, usually caused due compression or irritation of the nerve.
Ulnar nerve neuropathy is the second most common neuropathy of the arm 10. A study of 91 patients identified that close to 60% of these patients had anatomical changes in the cubital tunnel that caused the ulnar nerve neuropathy, of which nearly 20% of patients had a subluxation of the ulnar nerve. Other causes identified in this study were osteophytes in almost 7% of patients and luxation of the ulnar nerve in nearly 10% of patients. Post-traumatic lesions also can cause symptoms in about 3.3% of patients 11.
Ulnar Nerve anatomy: C8 and T1 nerve roots join and give rise to the medial cord in the brachial plexus. Ulnar nerve originates as a branch of medial cord. The ulnar nerve then travels down the arm along with the brachial artery towards the elbow joint, at which point it enters the posterior compartment of the forearm via the cubital tunnel. Cubital tunnel is the region where the ulnar nerve is most likely to be damaged due to its location and anatomy. At this point, the ulnar nerve travels between the olecranon and the medial epicondyle.
Figure 6. Ulnar nerve anatomy

Figure 7. Cubital tunnel syndrome

Cubital tunnel syndrome causes
Multiple causes can result in ulnar nerve compression and damage at the cubital tunnel and cause symptoms such as tingling in the medial aspect of the forearm along with the little finger and medial aspect of the ring finger.
- Pressure on the ulnar nerve is a common cause of symptoms. The ulnar nerve is superficial at the point of the medial epicondyle; this is why people may experience the feeling of shooting pain and electric shock in the forearm if they accidentally hit their elbow on a hard surface.
- Stretching the ulnar nerve can also result in similar symptoms. The ulnar nerve lies behind the medial epicondyle. During flexion of the elbow joint, the ulnar nerve gets stretched because of this anatomical position. Repetitive elbow flexion and extension can cause further damage and irritation to the ulnar nerve. Some individuals sleep with elbows bent which can stretch the ulnar nerve for an extended period during sleep, which is an identified cause of damage to the ulnar nerve.
- Injuries to the elbow joint (fractures, dislocations, swelling, effusions) can cause permanent anatomical damage which will cause symptoms because of compression/irritation of the ulnar nerve.
A study of 117 patients identified that direct pressure on the nerve because of habits while sitting, or secondary to occupational activities is a significant cause of the nerve damage as the nerve passes posterior to the medial epicondyle 12.
Risk factors for ulnar nerve compression
Some factors put you more at risk for developing ulnar nerve compression (cubital tunnel syndrome). These include:
- Prior fracture or dislocations of the elbow
- Bone spurs/ arthritis of the elbow
- Swelling of the elbow joint
- Cysts near the elbow joint
- Repetitive or prolonged activities that require the elbow to be bent or flexed
Cubital tunnel syndrome symptoms
Ulnar nerve compression can cause an aching pain on the inside of the elbow. Most of the symptoms, however, occur in your hand.
- Numbness and tingling in the ring finger and little finger are common symptoms of ulnar nerve entrapment. Often, these symptoms come and go. They happen more often when the elbow is bent, such as when driving or holding the phone. Some people wake up at night because their fingers are numb.
- The feeling of “falling asleep” in the ring finger and little finger, especially when your elbow is bent. In some cases, it may be harder to move your fingers in and out, or to manipulate objects.
- Weakening of the grip and difficulty with finger coordination (such as typing or playing an instrument) may occur. These symptoms are usually seen in more severe cases of nerve compression.
- If the nerve is very compressed or has been compressed for a long time, muscle wasting in the hand can occur. Once this happens, muscle wasting cannot be reversed. For this reason, it is important to see your doctor if symptoms are severe or if they are less severe but have been present for more than 6 weeks.
Cubital tunnel syndrome diagnosis
Your doctor will discuss your medical history and general health. He or she may also ask about your work, your activities, and what medications you are taking.
After discussing your symptoms and medical history, your doctor will examine your arm and hand to determine which nerve is compressed and where it is compressed. Some of the physical examination tests your doctor may do include:
- Tap over the nerve at the funny bone. If the nerve is irritated, this can cause a shock into the little finger and ring finger — although this can happen when the nerve is normal as well.
- Check whether the ulnar nerve slides out of normal position when you bend your elbow.
- Move your neck, shoulder, elbow, and wrist to see if different positions cause symptoms.
- Check for feeling and strength in your hand and fingers.
Ulnar nerve compression test
X-rays. These imaging tests provide detailed pictures of dense structures, like bone. Most causes of compression of the ulnar nerve cannot be seen on an x-ray. However, your doctor may take x-rays of your elbow or wrist to look for bone spurs, arthritis, or other places that the bone may be compressing the nerve.
Nerve conduction studies. These tests can determine how well the nerve is working and help identify where it is being compressed.
Nerves are like “electrical cables” that travel through your body carrying messages between your brain and muscles. When a nerve is not working well, it takes too long for it to conduct.
During a nerve conduction test, the nerve is stimulated in one place and the time it takes for there to be a response is measured. Several places along the nerve will be tested and the area where the response takes too long is likely to be the place where the nerve is compressed.
Nerve conduction studies can also determine whether the compression is also causing muscle damage. During the test, small needles are put into some of the muscles that the ulnar nerve controls. Muscle damage is a sign of more severe nerve compression.
Cubital tunnel syndrome treatment
Unless your nerve compression has caused a lot of muscle wasting, your doctor will most likely first recommend nonsurgical treatment.
Nonsurgical Treatment
- Non-steroidal anti-inflammatory (NSAIDs) medicines. If your symptoms have just started, your doctor may recommend an anti-inflammatory medicine, such as ibuprofen, to help reduce swelling around the nerve.
Although steroids, such as cortisone, are very effective anti-inflammatory medicines, steroid injections are generally not used because there is a risk of damage to the nerve.
- Bracing or splinting. Your doctor may prescribe a padded brace or split to wear at night to keep your elbow in a straight position.
- Nerve gliding exercises. Some doctors think that exercises to help the ulnar nerve slide through the cubital tunnel at the elbow and the Guyon’s canal at the wrist can improve symptoms. These exercises may also help prevent stiffness in the arm and wrist.
Home remedies
There are many things you can do at home to help relieve symptoms. If your symptoms interfere with normal activities or last more than a few weeks, be sure to schedule an appointment with your doctor.
- Avoid activities that require you to keep your arm bent for long periods of time.
- If you use a computer frequently, make sure that your chair is not too low. Do not rest your elbow on the armrest.
- Avoid leaning on your elbow or putting pressure on the inside of your arm. For example, do not drive with your arm resting on the open window.
- Keep your elbow straight at night when you are sleeping. This can be done by wrapping a towel around your straight elbow or wearing an elbow pad backwards.
Surgical Treatment
Your doctor may recommend surgery to take pressure off of the nerve if:
- Nonsurgical methods have not improved your condition
- The ulnar nerve is very compressed
- Nerve compression has caused muscle weakness or damage
There are a few surgical procedures that will relieve pressure on the ulnar nerve at the elbow. Your orthopaedic surgeon will talk with you about the option that would be best for you.
These procedures are most often done on an outpatient basis, but some patients do best with an overnight stay at the hospital.
Cubital tunnel release. In this operation, the ligament “roof” of the cubital tunnel is cut and divided. This increases the size of the tunnel and decreases pressure on the nerve.
After the procedure, the ligament begins to heal and new tissue grows across the division. The new growth heals the ligament, and allows more space for the ulnar nerve to slide through.
Cubital tunnel release tends to work best when the nerve compression is mild or moderate and the nerve does not slide out from behind the bony ridge of the medial epicondyle when the elbow is bent.
Ulnar nerve anterior transposition. In many cases, the nerve is moved from its place behind the medial epicondyle to a new place in front of it. Moving the nerve to the front of the medial epicondyle prevents it from getting caught on the bony ridge and stretching when you bend your elbow. This procedure is called an anterior transposition of the ulnar nerve.
The nerve can be moved to lie under the skin and fat but on top of the muscle (subcutaneous transposition), or within the muscle (intermuscular transposition), or under the muscle (submuscular transposition).
Medial epicondylectomy. Another option to release the nerve is to remove part of the medial epicondyle. Like ulnar nerve transposition, this technique also prevents the nerve from getting caught on the boney ridge and stretching when your elbow is bent.
Surgical Recovery
Depending on the type of surgery you have, you may need to wear a splint for a few weeks after the operation. A submuscular transposition usually requires a longer time (3 to 6 weeks) in a splint.
Your surgeon may recommend physical therapy exercises to help you regain strength and motion in your arm. He or she will also talk with you about when it will be safe to return to all your normal activities.
Surgical Outcome
The results of surgery are generally good. Each method of surgery has a similar success rate for routine cases of nerve compression. If the nerve is very badly compressed or if there is muscle wasting, the nerve may not be able to return to normal and some symptoms may remain even after the surgery. Nerves recover slowly, and it may take a long time to know how well the nerve will do after surgery.
Nerve gliding exercises. Some doctors think that exercises to help the ulnar nerve slide through the cubital tunnel at the elbow and the Guyon’s canal at the wrist can improve symptoms. These exercises may also help prevent stiffness in the arm and wrist.
- Sevy JO, Varacallo M. Carpal Tunnel Syndrome. [Updated 2019 Apr 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448179[↩][↩]
- Hegmann KT, Merryweather A, Thiese MS, Kendall R, Garg A, Kapellusch J, Foster J, Drury D, Wood EM, Melhorn JM. Median Nerve Symptoms, Signs, and Electrodiagnostic Abnormalities Among Working Adults. J Am Acad Orthop Surg. 2018 Aug 15;26(16):576-584[↩]
- Sevy JO, Varacallo M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Nov 15, 2018. Carpal Tunnel Syndrome[↩]
- Sevy JO, Varacallo M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Nov 15, 2018. Carpal Tunnel Syndrome.[↩]
- Mezian K, Bruthans J. Why do local corticosteroid injections work in carpal tunnel syndrome, But not in ulnar neuropathy at the elbow? Muscle Nerve. 2016 Aug;54(2):344[↩]
- Kiel J, Kaiser K. Tarsal Tunnel Syndrome. [Updated 2019 Feb 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513273[↩]
- Calvo-Lobo C, Painceira-Villar R, López-López D, García-Paz V, Becerro-de-Bengoa-Vallejo R, Losa-Iglesias ME, Palomo-López P. Tarsal Tunnel Mechanosensitivity Is Increased in Patients with Asthma: A Case-Control Study. J Clin Med. 2018 Dec 12;7,12[↩]
- Tarsal Tunnel Syndrome. https://emedicine.medscape.com/article/1236852-overview[↩]
- Pfeiffer WH, Cracchiolo A 3rd. Clinical results after tarsal tunnel decompression. J Bone Joint Surg Am. 1994;76:1222-1230[↩]
- Chauhan M, M Das J. Cubital Tunnel Syndrome. [Updated 2019 Apr 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538259[↩][↩]
- Filippou G, Mondelli M, Greco G, Bertoldi I, Frediani B, Galeazzi M, Giannini F. Ulnar neuropathy at the elbow: how frequent is the idiopathic form? An ultrasonographic study in a cohort of patients. Clin. Exp. Rheumatol. 2010 Jan-Feb;28(1):63-7[↩]
- Omejec G, Podnar S. What causes ulnar neuropathy at the elbow? Clin Neurophysiol. 2016 Jan;127(1):919-924.[↩]





{kind=link}