
Contents
What is tonsillectomy
Tonsillectomy is the surgical procedure to remove the tonsils, two oval-shaped pads of lymphatic tissue at the back of the throat — one tonsil on each side. Tonsillectomy completely removes the tonsil, including its capsule, by dissecting the peritonsillar space between the tonsil capsule and the muscular wall. Depending on the context in which it is used, the term may indicate tonsillectomy with adenoidectomy, especially in relation to sleep-disordered breathing.
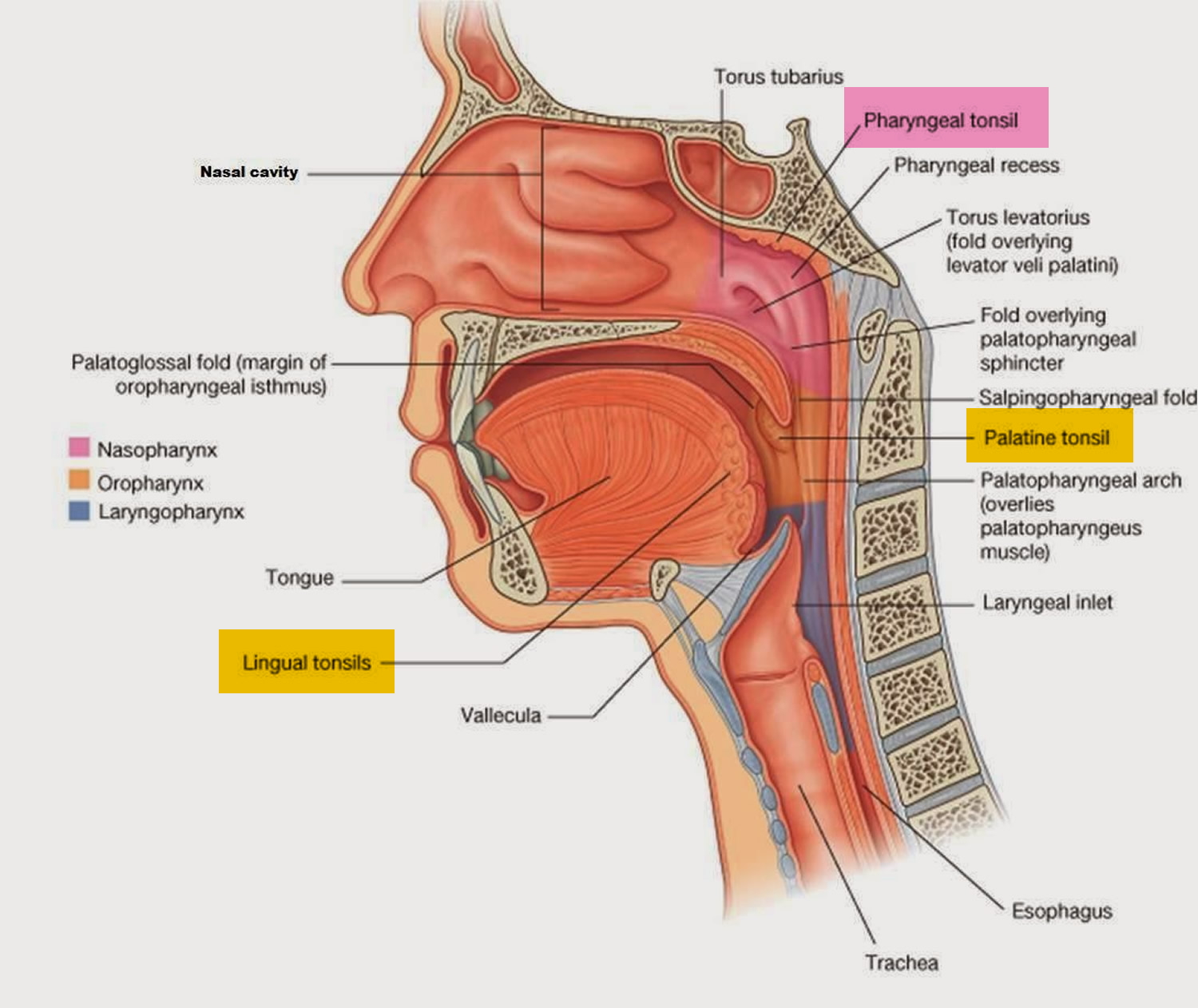
Your tonsils are two small glands in the back of the throat, on either side of the tongue and closely associated with the palate, are masses of lymphatic tissue called palatine tonsils (see Figures 1 and 2). Like other lymphatic tissues, the two palatine tonsils help protect your body against infection, particularly in childhood.
Tonsillectomy is the third most common surgical procedure (after circumcision and ear tubes) performed on children in the United States, with over 530,000 annual procedures (1 in 7 ambulatory surgeries under age 15 years) 1, 2. When performed in properly selected children, tonsillectomy can reduce throat infections, doctor visits, and antibiotic use, and can improve a child’s quality of life, daytime functioning, and ability to sleep soundly.
Indications for tonsillectomy include recurrent throat infections 3 and sleep-disordered breathing 4, both of which can substantially affect child health status 5 and quality of life 6. Although there are benefits of tonsillectomy, complications of surgery may include throat pain, postoperative nausea and vomiting, delayed feeding, voice changes, hemorrhage, and rarely death.
Watch for the following complications that require prompt medical care:
- Bleeding. You may see small specks of dark blood from the nose or in the saliva, but any bright red blood requires a trip to the emergency room for a prompt evaluation and treatment. Surgery to stop bleeding may be necessary.
- Fever. Call your doctor if you or your child has a fever of 102° F (38.9° C) or higher.
- Dehydration. Call your doctor if you observe signs of dehydration, such as reduced urination, thirst, weakness, headache, dizziness or lightheadedness.
- Common signs of dehydration in children include urinating fewer than two or three times a day or crying with no tears.
- Breathing problems. Snoring or noisy breathing is common during the first week or so of recovery. However, if you or your child is having difficulty breathing, get emergency care.
A tonsillectomy may be recommended to prevent frequent, recurring episodes of tonsillitis. Frequent is generally defined as:
- More than seven episodes a year
- More than five episodes a year in each of the preceding two years
- More than three episodes a year in each of the preceding three years
The tonsillectomy procedure may also be recommended if:
- A bacterial infection causing tonsillitis doesn’t improve with antibiotic treatment
- An infection that results in a collection of pus behind a tonsil (tonsillar abscess) doesn’t improve with drug treatment or a drainage procedure
- A tonsillectomy may also be used to treat other rare diseases or conditions of the tonsils, such as:
- Cancerous tissue in one or both tonsils
- Recurrent bleeding from blood vessels near the surface of the tonsils
Adenoids sit high in the throat behind the nose and the roof of the mouth. Tonsils and adenoids are often removed when they become enlarged and block the upper airway, leading to breathing difficulty. They are also removed when recurrence of tonsil infections or strep throat cannot be successfully treated by antibiotics.
The excision of the adenoids is an adenoidectomy. Both tonsillectomy and adenoidectomy procedures are often performed at the same time; hence the surgery is known as a tonsillectomy and adenoidectomy or T&A 7.
Tonsillectomy and adenoidectomy is an outpatient surgical procedure lasting between 30 and 45 minutes and performed under general anesthesia 7. Normally, you will remain at the hospital or clinic for several hours after surgery for observation. Children with severe obstructive sleep apnea (OSA) and very young children are usually admitted overnight to the hospital for close monitoring of respiratory status. An overnight stay may also be required if there are complications such as excessive bleeding, severe vomiting, or low oxygen saturation.
- Recovery time for a tonsillectomy is usually at least 10 days to two weeks.
- On average, the amount paid for a tonsillectomy without complication was $3,832 whereas tonsillectomy with hemorrhage resulted in an average expenditure of $6,388 8.
A tonsillectomy was once a common procedure to treat infection and inflammation of the tonsils (tonsillitis). Today, a tonsillectomy is usually performed for sleep-disordered breathing but may still be a treatment when tonsillitis occurs frequently or doesn’t respond to other treatments.
A tonsillectomy may also be necessary to treat breathing and other problems related to enlarged tonsils and to treat rare diseases of the tonsils.
Figure 1. Normal palatine tonsils
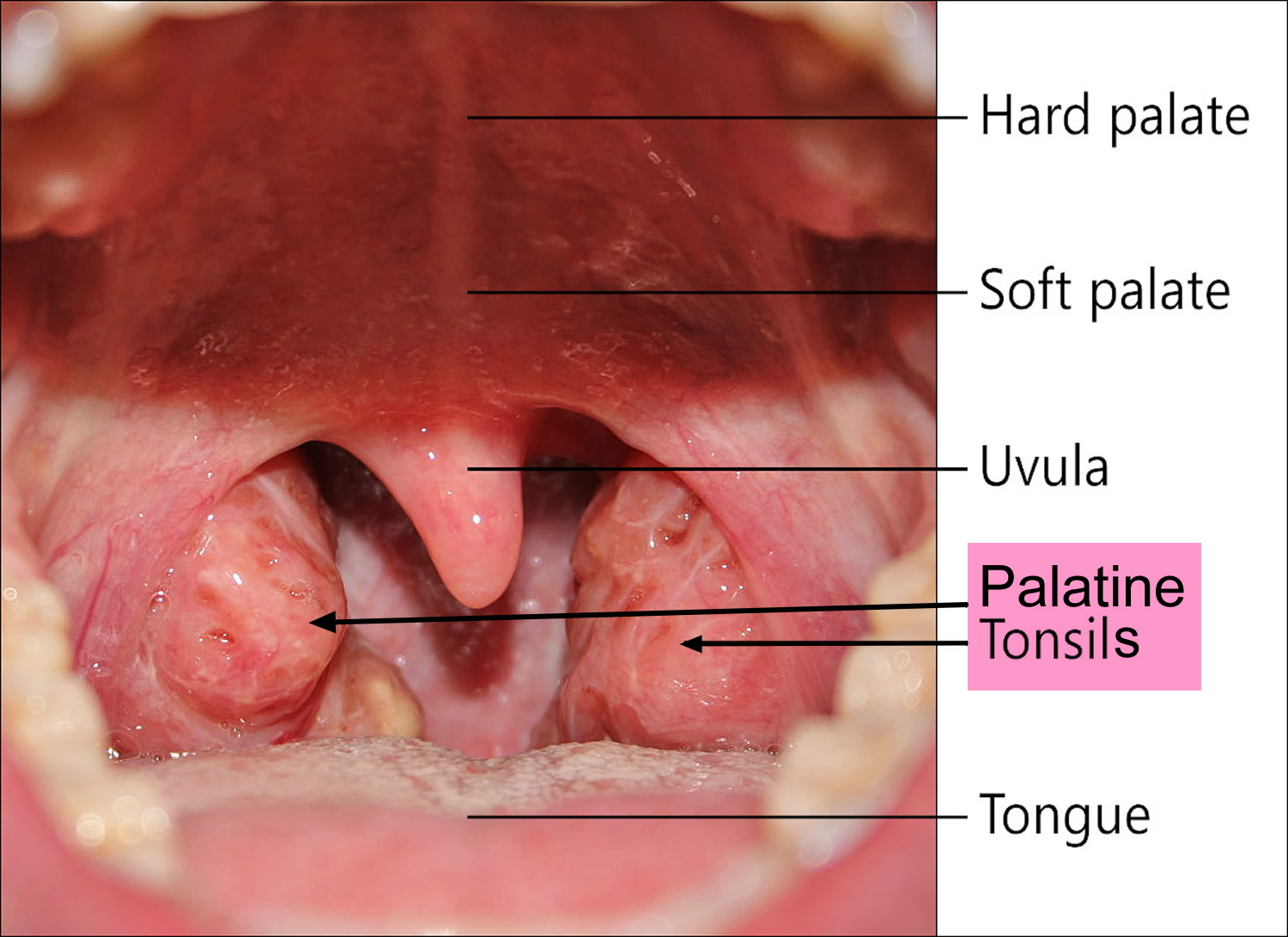
Figure 2. Palatine tonsil, Pharyngeal tonsil and Lingual tonsil
Post tonsillectomy
Most children take seven to ten days to recover from the surgery. Some may recover more quickly; others can take up to two weeks for a full recovery. The following guidelines are recommended:
- Drinking: The most important requirement for recovery is for the patient to drink plenty of fluids..Starting immediately after surgery, children may have fluids such as water or apple juice. Some patients experience nausea and vomiting after the surgery. This usually occurs within the first 24 hours and resolves on its own after the effects of anesthesia wear off. Contact your physician if there are signs of dehydration (urination less than 2-3 times a day or crying without tears).
- Eating: Generally, there are no food restrictions after surgery, but some physicians will recommend a soft diet during the recovery period. The sooner the child eats and chews, the quicker the recovery. Tonsillectomy patients may be reluctant to eat because of throat pain; consequently, some weight loss may occur, which is gained back after a normal diet is resumed.
- Fever: A low-grade fever may be observed the night of the surgery and for a day or two afterward. Contact your physician if the fever is greater than 102ºF
- (38.9° C).
- Activity: Activity may be increased slowly, with a return to school after normal eating and drinking resumes, pain medication is no longer required, and the child sleeps through the night. Travel on airplanes or far away from a medical facility is not recommended for two weeks following surgery.
- Breathing: The parent may notice snoring and mouth breathing due to swelling in the throat. Breathing should return to normal when swelling subsides, 10-14 days after surgery.
- Scabs: A scab will form where the tonsils and adenoids were removed. These scabs are thick, white, and cause bad breath. This is normal. Most scabs fall off in small pieces five to ten days after surgery.
- Bleeding: With the exception of small specks of blood from the nose or in the saliva, bright red blood should not be seen. If such bleeding occurs, contact your physician immediately or take your child to the emergency room.
- Pain: Nearly all children undergoing a tonsillectomy or adenoidectomy will have mild to severe pain in the throat after surgery. Some may complain of an earache (so called referred pain) and a few may have pain in the jaw and neck .
- Pain control: Your physician will prescribe pain medication for the young patient such as acetaminophen or ibuprofen acetaminophen. The pain medication will be in a liquid form or sometimes a rectal suppository will be recommended. Pain medication should be given as prescribed. Contact your physician if side effects are suspected or if pain is not well-controlled. If you are troubled about any phase of your childs recovery, contact your physician immediately.
Tonsillectomy in Children
American Academy of Otolaryngology — Head and Neck Surgery Clinical Practice Guideline 9
The panel made recommendations for:
- Watchful waiting for recurrent throat infection if there have been fewer than 7 episodes in the past year or fewer than 5 episodes per year in the past 2 years or fewer than 3 episodes per year in the past 3 years;
- Assessing the child with recurrent throat infection who does not meet criteria in statement 2 for modifying factors that may nonetheless favor tonsillectomy, which may include but are not limited to multiple antibiotic allergy/intolerance, periodic fever, aphthous stomatitis, pharyngitis and adenitis, or history of peritonsillar abscess;
- Asking caregivers of children with sleep-disordered breathing and tonsil hypertrophy about comorbid conditions that might improve after tonsillectomy, including growth retardation, poor school performance, enuresis, and behavioral problems;
- Counseling caregivers about tonsillectomy as a means to improve health in children with abnormal polysomnography who also have tonsil hypertrophy and sleep-disordered breathing;
- Counseling caregivers that sleep-disordered breathing may persist or recur after tonsillectomy and may require further management;
- Advocating for pain management after tonsillectomy and educating caregivers about the importance of managing and reassessing pain; and
- Clinicians who perform tonsillectomy should determine their rate of primary and secondary posttonsillectomy hemorrhage at least annually. The panel offered options to recommend tonsillectomy for recurrent throat infection with a frequency of at least 7 episodes in the past year or at least 5 episodes per year for 2 years or at least 3 episodes per year for 3 years with documentation in the medical record for each episode of sore throat and 1 or more of the following: temperature >38.3°C, cervical adenopathy, tonsillar exudate, or positive test for group A β-hemolytic streptococcus.
Indications for tonsillectomy
The 2 most common indications for tonsillectomy are recurrent throat infections and sleep-disordered breathing. Throat infection is defined as sore throat caused by viral or bacterial infection of the pharynx, palatine tonsils, or both, which may or may not be culture positive for group A streptococcus. This includes the terms strep throat and acute tonsillitis, pharyngitis, adenotonsillitis, or tonsillopharyngitis 10. Throat infections are a common reason to see a primary care physician and often result in antibiotic treatment 11. The cost of outpatient visits and the medications prescribed for sore throats including antibiotics are substantial. Indirect costs associated with throat infections and sleep-disordered breathing are substantial due to missed school and loss of time from work for caregivers.
Treatment of sleep-disordered breathing is associated with an increase in health care utilization and cost. Children with sleep-disordered breathing, compared with controls, have a significantly higher rate of antibiotic use, 40% more hospital visits, and an overall elevation of 215% in health care usage mostly from increased respiratory tract infections 12. Children with tonsillar disease, including children with throat infections and sleep-disordered breathing, also showed significantly lower scores on several quality of life subscales including general health, physical functioning, behavior, bodily pain, and caregiver impact when compared with healthy children 13.
Sleep-disordered breathing represents a spectrum of disorders ranging in severity from primary snoring to OSA (obstructive sleep apnea). The prevalence of OSA (obstructive sleep apnea) in the pediatric population is 1% to 4% 14; as many as 10% of children have primary snoring 15. Up to 30% to 40% of children with clinically diagnosed sleep-disordered breathing exhibit behavioral problems that include enuresis,28 hyperactivity, aggression, anxiety, depression, and somatization 16. OSA (obstructive sleep apnea) is also associated with poor school performance and a decrease in quality of life 17. The Quality of life of children with OSA is similar to children with chronic conditions such as asthma and juvenile rheumatoid arthritis 18.
Controversy persists about the actual benefits of tonsillectomy as compared with observation and medical treatment of throat infections. Although tonsillectomy for recurrent throat infections in severely affected children has been shown in a randomized controlled trial to reduce the frequency and severity of infections in the 2 years following surgery 19, the same cannot be shown for less severe cases or for a period greater than 2 years after surgery 20. Observational studies, however, show improved disease-specific and global quality of life after tonsillectomy for recurrent or chronic sore throat, as measured by validated instruments 21. These children suffered fewer infections after surgery, resulting in fewer antibiotics and physician visits.
A growing body of evidence indicates that tonsillectomy is an effective treatment for sleep-disordered breathing 22, based on the idea that tonsillar hypertrophy is a principal cause. A meta-analysis of case series 23 and a recent study 24 showed that tonsillectomy was effective at improving or resolving sleep-disordered breathing in most children. There is also evidence that behavioral parameters, school performance, and quality of life improve after resolution of this sleep disorder 17.
Harms and Adverse Events of Tonsillectomy
Tonsillectomy is a surgical procedure with an associated morbidity that includes possible hospitalization, risks of anesthesia, prolonged throat pain, and financial costs. A common complication of tonsillectomy is bleeding during or after the surgery. In published reports, the rate of primary hemorrhage (within 24 hours of surgery) has ranged from 0.2% to 2.2% and the rate of secondary hemorrhage (more than 24 hours after surgery) from 0.1% to 3% 25. Hemorrhage after tonsillectomy may result in readmission for observation or in further surgery to control bleeding.
Other complications of tonsillectomy are diverse and have been well described 26. Operative complications include trauma to the teeth, larynx, pharyngeal wall, or soft palate; difficult intubation; laryngospasm; laryngeal edema; aspiration; respiratory compromise; endotracheal tube ignition; and cardiac arrest. Injury to nearby structures has been reported, including lip burn, eye injury, and fracture of the mandibular condyle. Postoperative complications include nausea, vomiting, pain, dehydration, referred otalgia, postobstructive pulmonary edema, velopharyngeal insufficiency, and nasopharyngeal stenosis. Complications are more common in patients with craniofacial disorders, Down syndrome, cerebral palsy, major heart disease, or bleeding diatheses and in children younger than 3 years with polysomnography (PSG)–proven OSA 27, 28, 29.
After tonsillectomy, about 1.3% of patients experience delayed discharge during the initial hospital stay, and up to 3.9% have secondary complications requiring readmission 30. The primary reasons for readmission or prolonged initial stay included pain, vomiting, fever, and tonsillar hemorrhage. In addition to these common causes of morbidity, many unusual and rare complications of tonsillectomy have also been described 31. Among these are reports of vascular injury, subcutaneous emphysema, jugular vein thrombosis, atlantoaxial subluxation (Grisel syndrome), taste disorders (hypogeusia, ageusia, dysgeusia, and phantogeusia), and persistent neck pain (Eagle syndrome).
Mortality rates for tonsillectomy have been estimated at between 1 in 16 000 to 1 in 35 000, based on data from the 1970s 32. There are no current estimates of tonsillectomy mortality, but a prospective audit reported only 1 postoperative death after 33 921 procedures in England and Northern Ireland 30. About one-third of deaths are attributable to bleeding, while the remainder are related to aspiration, cardiopulmonary failure, electrolyte imbalance, or anesthetic complications 25. Similarly, airway compromise is the major cause of death or major injury in malpractice claims after tonsillectomy 33.
Effects of Tonsillitis and Tonsillectomy on Immunity
With chronic or recurrent tonsillitis, the controlled process of antigen transport and presentation is altered due to shedding of the M cells from the tonsil epithelium 34. The direct influx of antigens disproportionately expands the population of mature B-cell clones and, as a result, fewer early memory B cells go on to become J-chain–positive IgA immunocytes. In addition, the tonsillar lymphocytes can become so overwhelmed with persistent antigenic stimulation that they may be unable to respond to other antigens. Once this immunological impairment occurs, the tonsil is no longer able to function adequately in local protection, nor can it appropriately reinforce the secretory immune system of the upper respiratory tract. There would therefore appear to be a therapeutic advantage to removing recurrently or chronically diseased tonsils. On the other hand, some studies demonstrate minor alterations of Ig concentrations in the serum and adjacent tissues following tonsillectomy 35. Nevertheless, there are no studies to date that demonstrate a significant clinical impact of tonsillectomy on the immune system 36.
Adult tonsillectomy
Chronic infection remains the most common indication for adult tonsillectomy, in contrast to the pediatric population 37. Complication rates vary according to the indication for surgery.
Indications for surgery were chronic infection in 207 patients (57%) (71.3% recurrent, 9.2% tonsilliths/halitosis and 19.5% recurrent and tonsilliths/halitosis), upper airway obstruction secondary to tonsillar hypertrophy in 98 patients (27%), and suspected neoplasm in 56 patients (16%) 37. Indications for partial intracapsular tonsillectomies were 77.8% infection (28.6% recurrent, 50.0% tonsilliths/halitosis, and 21.4% recurrent and tonsilliths/halitosis), 19.4% upper airway obstruction, and 2.8% obstruction/infection 38.
Postoperative complications occurred in 54 cases (15%) with hemorrhage in 19 patients (5%), followed by pain and dehydration in 16 patients (4%) and admission for postoperative oxygen desaturations in 11 patients (3%) 37. Hospitalization beyond 24 hours occurred in 18 cases (5%), with emergency room visits for pain and dehydration in 16 patients (4%), and readmission for pain control in 17 cases (5%). Patients who underwent tonsillectomy for upper airway obstruction had an increased incidence of prolonged hospitalization or readmission (19% vs. 6%), while patients who underwent tonsillectomy for infection had an increased incidence of post-operative bleeding (6% vs. 4%) 37.
Conclusion: While recurrent infection remains the most common indication for adult tonsillectomy, there is a growing rate of tonsillectomies performed for upper airway obstruction. Complication rates varied according to indication for surgery and surgical technique (total versus partial intracapsular tonsillectomy); however, neither was found to significantly increase risk of postoperative complications 38.
- AAO-HNSF Clinical Practice Guideline: Tonsillectomy in Children. http://www.entnet.org/sites/default/files/January2011_Tonsillectomy.pdf[↩]
- Cullen KA, Hall MJ, Golosinskiy A. Ambulatory Surgery in the United States, 2006. National Health Statistics reports no. 11, revised. Hyattsville, MD: National Center for Health Statistics; 2009.[↩]
- Goldstein NA, Stewart MG, Witsell DL, . Quality of life after tonsillectomy in children with recurrent tonsillitis. Otolaryngol Head Neck Surg. 2008;138:S9-S16.[↩]
- Rosenfeld RM, Green RP. Tonsillectomy and adenoidectomy: changing trends. Ann Otol Rhinol Laryngol. 1990;99:187-191.[↩]
- Wei JL, Mayo MS, Smith HJ, . Improved behavior and sleep after adenotonsillectomy in children with sleep-disordered breathing. Arch Otolaryngol Head Neck Surg. 2007;133:974-979[↩]
- Tran KD, Nguyen CD, Weedon J, . Child behavior and quality of life in pediatric obstructive sleep apnea. Arch Otolaryngol Head Neck Surg. 2005;131:52-57.[↩]
- Tonsillectomy and Adenoids PostOp. http://www.entnet.org/content/tonsillectomy-and-adenoids-postop[↩][↩]
- http://www.entnet.org/content/adult-tonsillectomy-complications-and-health-care-expenses[↩]
- American Academy of Otolaryngology — Head and Neck Surgery Clinical Practice Guideline. http://www.entnet.org/content/clinical-practice-guideline-tonsillectomy-children[↩]
- Clinical Practice Guideline: Tonsillectomy in Children. Otolaryngology-Head and Neck Surgery Vol 144, Issue 1_suppl, pp. S1 – S30[↩]
- Del Mar C. Managing sore throat: a literature review. II. Do antibiotics confer benefit? Med J Aust. 1992;156:644-649.[↩]
- Tarasiuk A, Greenberg-Dotan S, Simon-Tuval T, . Elevated morbidity and health care use in children with obstructive sleep apnea syndrome. Am J Respir Crit Care Med. 2007;175:55-61.[↩]
- Stewart MG, Friedman EM, Sulek M, . Quality of life and health status in pediatric tonsil and adenoid disease. Arch Otolaryngol Head Neck Surg. 2000;126:45-48.[↩]
- Ali NJ, Pitson DJ, Stradling JR. Snoring, sleep disturbance, and behaviour in 4-5 year olds. Arch Dis Child. 1993;68:360-366.[↩]
- Urschitz, MS, Wolff, J, Sokollik, C. Nocturnal arterial oxygen saturation and academic performance in a community sample of children. Pediatrics. 2005;115:e204-e209.[↩]
- Goldstein, NA, Post, JC, Rosenfeld, RM. Impact of tonsillectomy and adenoidectomy on child behavior. Arch Otolaryngol Head Neck Surg. 2000;126:494-498.[↩]
- Mitchell, RB, Kelly, J. Behavior, neurocognition and quality-of-life in children with sleep-disordered breathing. Int J Pediatr Otorhinolaryngol. 2006;70:395-406.[↩][↩]
- Georgalas, C, Tolley, N, Kanagalingam, J. Measuring quality of life in children with adenotonsillar disease with the Child Health Questionnaire: a first U.K. study. Laryngoscope. 2004;114:1849-1855.[↩]
- Paradise, JL, Bluestone, CD, Bachman, RZ. Efficacy of tonsillectomy for recurrent throat infection in severely affected children: results of parallel randomized and nonrandomized clinical trials. N Engl J Med. 1984;310:674–683.[↩]
- Paradise, JL, Bluestone, CD, Colborn, DK. Tonsillectomy and adenotonsillectomy for recurrent throat infection in moderately affected children. Pediatrics. 2002;110:7-15.[↩]
- Goldstein, NA, Stewart, MG, Witsell, DL. Quality of life after tonsillectomy in children with recurrent tonsillitis. Otolaryngol Head Neck Surg. 2008;138:S9–S16.[↩]
- Friedman, M, Wilson, M, Lin, HC. Updated systematic review of tonsillectomy and adenoidectomy for treatment of pediatric obstructive sleep apnea/hypopnea syndrome. Otolaryngol Head Neck Surg. 2009;140:800–808.[↩]
- Brietzke, SE, Gallagher, D. The effectiveness of tonsillectomy and adenoidectomy in the treatment of pediatric obstructive sleep apnea/hypopnea syndrome: a meta-analysis. Otolaryngol Head Neck Surg. 2006;134:979–984.[↩]
- Mitchell, RB, Kelly, J. Outcomes and quality of life following adenotonsillectomy for sleep-disordered breathing in children. ORL J Otorhinolaryngol Relat Spec. 2007;69:345–348.[↩]
- Windfuhr, JP, Chen, YS, Remmert, S. Hemorrhage following tonsillectomy and adenoidectomy in 15,218 patients. Otolaryngol Head Neck Surg. 2006;132:281–286.[↩][↩]
- Johnson, LB, Elluru, RG, Myer, CM. Complications of adenotonsillectomy. Laryngoscope. 2002;112:35–36. [↩]
- Kavanagh, KT, Beckford, NS. Adenotonsillectomy in children: indications and contraindications. South Med J. 1988;81:507–514. [↩]
- Colclasure, JB, Graham, SS. Complications of outpatient tonsillectomy and adenoidectomy: a review of 3,340 cases. Ear Nose Throat J. 1990;69:155–160.[↩]
- Wiatrak, BJ, Myer, CM, Andrews, TM. Complications of adenotonsillectomy in children under 3 years of age. Am J Otolaryngol. 1991;12:170–172.[↩]
- Royal College of Surgeons of England. National prospective tonsillectomy audit: final report of an audit carried out in England and Northern Ireland between July 2003 and September 2004. May 2005. [↩][↩]
- Leong, SC, Karkos, PD, Papouliakos, SM. Unusual complications of tonsillectomy: a systematic review. Am J Otolaryngol. 2007;28:419–422[↩]
- Pratt, LW, Gallagher, RA. Tonsillectomy and adenoidectomy: incidence and mortality, 1968–1972. Otolaryngol Head Neck Surg. 1979;87:159–166.[↩]
- Morris, LG, Lieberman, SM, Reitzen, SD. Characteristics and outcomes of malpractice claims after tonsillectomy. Otolaryngol Head Neck Surg. 2008;138:315–320.[↩]
- Brandtzaeg, P. In: Immune functions and immunopathology of palatine and nasopharyngeal tonsils. Bernstein, JM, Ogra, PL, eds. Immunology of the Ear. New York, NY: Raven Press; 1987:63–106.[↩]
- Friday, GA, Paradise, JL, Rabin, BS. Serum immunoglobulin changes in relation to tonsil and adenoid surgery. Ann Allergy. 1992;69:225–230.[↩]
- Paulussen, CCJ, Claes, G, Jorissen, M. Adenoids and tonsils, indications for surgery and immunological consequences of surgery. Acta Otorhinolaryngol Belg. 2000;54:403-408.[↩]
- Adult Tonsillectomy: Current Indications and Outcomes. Otolaryngology-Head and Neck Surgery Vol 139, Issue 2_suppl, pp. P33 – P33. http://journals.sagepub.com/doi/pdf/10.1016/j.otohns.2008.05.108[↩][↩][↩][↩]
- http://journals.sagepub.com/doi/pdf/10.1177/0194599812451426a27[↩][↩]





{kind=link}