Contents
Trichomonas vaginalis
Trichomonas vaginalis is a sexually transmitted protozoan parasite that causes trichomoniasis or “trich”, which is a very common sexually transmitted disease (STD) worldwide. Trichomonas vaginalis infection is the most common curable sexually transmitted disease (STD). An estimated 3.7 million people have Trichomonas vaginalis infection in the United States, with approximately 1.1 million new cases occurring each year 1. The prevalence of Trichomonas vaginalis infection among reproductive-age women in the United States is estimated at 3.1%, but rates are at least four times higher among non-Hispanic black women 2. In addition, trichomoniasis prevalence increases with age, is higher among incarcerated women and female sex workers, and yet still afflicts a substantial number of adolescent and young adult women who are tested in the primary care setting 3. Importantly, Trichomonas vaginalis symptoms vary, most people who have the parasite cannot tell they are infected and only about 30% develop any symptoms of Trichomonas vaginalis infection: in one study of women attending STD clinics, prevalence was 26.2% among symptomatic women and 6.5% among asymptomatic women 4. Men are not routinely tested for trichomoniasis; nevertheless, studies have reported rates from 3% to 17% in men attending STD clinics, and as high as 72% among heterosexual men whose female partners are diagnosed with trichomoniasis 5. Men who have sex with men appear to be at low risk of acquiring trichomoniasis whereas transmission between female sex partners has been documented 6.
Figure 1. Trichomonas vaginalis
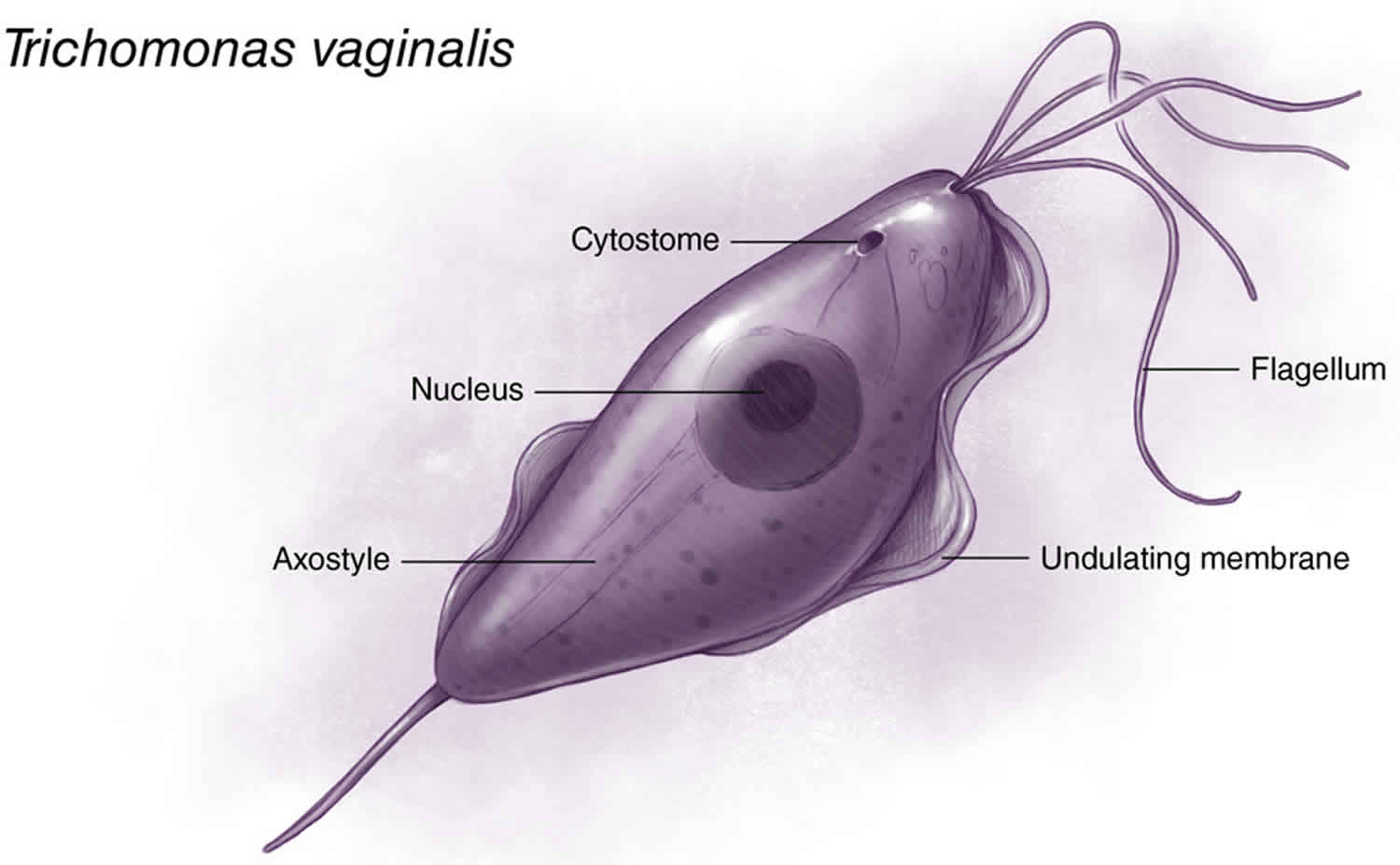
Footnote: Trichomonas vaginalis is a pear-shaped flagellated protozoan parasitic organism that is approximately 10 by 7 micrometers. The organism achieves a quivering motion via the anterior flagella and the undulating membrane. After attaching to vaginal epithelial cells, the organism takes on a more ameboid-like appearance.
Trichomonas vaginalis transmission
The Trichomonas vaginalis parasite passes from an infected person to an uninfected person during sex. In women, the most commonly infected part of the body is the lower genital tract (vulva, vagina, cervix, or urethra). In men, the most commonly infected body part is the inside of the penis (urethra). During sex, the Trichomonas vaginalis parasite usually spreads from a penis to a vagina, or from a vagina to a penis. Trichomonas vaginalis can also spread from a vagina to another vagina. It is not common for the Trichomonas vaginalis parasite to infect other body parts, like the hands, mouth, or anus. It is unclear why some people with the infection get symptoms while others do not. It probably depends on factors like a person’s age and overall health. Infected people without symptoms can still pass the infection on to others.
Risk factors for Trichomonas vaginalis infection
Investigators have identified multiple risk factors associated with Trichomonas vaginalis infection that include the following 7:
- Older age
- Multiple sex partners
- Drug use (marijuana, crack cocaine, alcohol, cigarettes)
- Unprotected sex with non-primary partner
- Presence of sexually transmitted infections at baseline
- Low socioeconomic status
- Douching
- Black race
Trichomonas vaginalis infection prevention
The only way to avoid STDs is to not have vaginal, anal, or oral sex.
If you are sexually active, you can do the following things to lower your chances of getting trichomoniasis:
- Be in a long-term mutually monogamous relationship with a partner who has been tested and has negative STD test results;
- Use latex condoms the right way every time you have sex. This can lower your chances of getting trichomoniasis. But the parasite can infect areas that are not covered by a condom – so condoms may not fully protect you from getting trichomoniasis.
Another approach is to talk about the potential risk of STDs before you have sex with a new partner. That way you can make informed choices about the level of risk you are comfortable taking with your sex life.
If you or someone you know has questions about Trichomonas vaginalis infection or any other STD, talk to a health care provider.
Trichomonas vaginalis symptoms
About 70% of Trichomonas vaginalis infected people do not have any signs or symptoms. When Trichomonas vaginalis infection does cause symptoms, they can range from mild irritation to severe inflammation. Some people with symptoms get them within 5 to 28 days after being infected. Others do not develop symptoms until much later. Symptoms can come and go.
Men with Trichomonas vaginalis infection may notice:
- Itching or irritation inside the penis;
- Burning after urination or ejaculation;
- Discharge from the penis.
Trichomonas vaginalis may cause up to 11% to 13% of nongonococcal urethritis in males, but urethral infection in males is frequently asymptomatic 8. Men with Trichomonas vaginalis infection may also present with prostatitis or epididymitis 9.
Women with Trichomonas vaginalis infection may notice:
- Itching, burning, redness or soreness of the genitals;
- Discomfort with urination;
- A change in their vaginal discharge (i.e., thin discharge or increased volume) that can be clear, white, yellowish, or greenish with an unusual fishy smell.
Vaginitis due to acute infection with Trichomonas vaginalis can have a characteristic “frothy” gray or yellow-green vaginal discharge and pruritus, but many women are asymptomatic 10. Chronic infection may be associated with minimal discharge, mild pruritus and/or dyspareunia 10. The presence of cervical petechiae, often referred to as a “Strawberry cervix”, strongly suggests a diagnosis of trichomoniasis, but this occurs in fewer than 5% of women with trichomoniasis 10.
Having Trichomonas vaginalis can make it feel unpleasant to have sex. Without treatment, the Trichomonas vaginalis infection can last for months or even years.
Trichomonas vaginalis infection complications
Trichomonas vaginalis infection can increase the risk of getting or spreading other sexually transmitted infections. For example, Trichomonas vaginalis infection can cause genital inflammation that makes it two- to three-fold risk of acquiring HIV infection, or to pass the HIV virus on to a sex partner 11. In women already infected with HIV, more than half are coinfected with Trichomonas vaginalis and these patients have been shown to have an increased risk for pelvic inflammatory disease and for shedding of HIV in the genital tract.[119,120,121,122,123,124] Importantly, antiretroviral therapy appears to lessen the potentiating effects of Trichomonas vaginalis infections on HIV transmission risk 12. HIV infection does not make a woman more likely to have persistent or recurrent Trichomonas vaginalis infection 13.
How does Trichomonas vaginalis affect a pregnant woman and her baby?
Pregnant women with Trichomonas vaginalis are more likely to have their babies too early (preterm delivery). Also, babies born to infected mothers are more likely to have a low birth weight (less than 5.5 pounds) 14. Neonatal trichomoniasis is unusual but can occur 15.
Trichomonas vaginalis diagnosis
It is not possible to diagnose Trichomonas vaginalis infection based on symptoms alone. For both men and women, your health care provider can examine you and get a laboratory test to diagnose trichomoniasis. In clinical practice, the wet mount preparation has been the most commonly used method for diagnosing trichomoniasis, primarily because of the low cost, convenience, and immediate diagnosis 1. This approach, however, has a sensitivity that is significantly lower than with newer nucleic acid amplification tests (NAATs).
Trichomonas vaginalis test
Wet Mount Preparation
In the clinical setting, the diagnosis of trichomoniasis can be made by microscopic visualization of motile trichomonads on a vaginal wet mount slide 16. Although the wet prep method is inexpensive and relatively simple to perform, it has a sensitivity of at most 60 and is operator-dependent 16. Once a vaginal fluid sample is collected, it should be stored in saline (for a maximum of one hour) until the operator is ready to perform microscopy 17. Once the specimen has been placed on the slide, microscopic evaluation is recommended as soon as possible and always within 10 minutes, since the trichomonads will become increasingly sluggish on the wet mount and motility is required for positive identification 16.
Culture
Obtaining a culture using modified Diamond’s medium was the previous gold standard for diagnosis of trichomoniasis, and culture is a more sensitive diagnostic tool than wet mount alone. Specialized culture systems (i.e. InPouch) are available to allow for transport of cultures when shipping to an off-site laboratory. Culture may be used for diagnosing Trichomonas vaginalis in both men and women. According to the 2015 STD Treatment Guidelines, culture in men may be performed on samples from a urethral swab, urine sediment or semen, but testing in women requires sampling of vaginal secretions 9.
Rapid Testing
Point-of-care tests for diagnosing trichomoniasis in women include the OSOM Trichomonas Rapid Test (an antigen-detection test) and the BD Affirm III Microbial Identification Test (a DNA hybridization probe) 18. The sensitivity, specificity, and clinical utility of these tests are higher than wet mount but lower than culture 19. Neither the OSOM nor Affirm tests are approved for testing in men.
Nucleic Acid Amplification Testing (NAAT)
Several different Nucleic Acid Amplification Testing (NAAT)-based methods are available, including transcription-mediated amplification (TMA) and polymerase chain reaction (PCR). The Trichomonas APTIMA test is a TMA assay that was approved in 2011 by the U.S. FDA for the diagnosis of vaginal trichomoniasis. This test is highly sensitive and specific, and, in women, can be performed on vaginal swab (self-collected or clinician-collected), urine, or liquid endocervical (in Thin Prep media) specimens 8. This test is considerably more sensitive than wet mount, culture, and the Affirm VPIII point-of-care DNA hybridization probe 20. The Trichomonas APTIMA test also appears to be the most sensitive testing method to detect trichomoniasis in asymptomatic women 21. The APTIMA test may be used to test urine or urethral swabs from men if validated by CLIA regulations; penile-meatal swabs are preferred to urine samples since they improve rates of detection 8. The FDA-cleared PCR assay for gonorrhea and chlamydia has been modified to test concurrently for Trichomonas vaginalis in endocervical and urine samples, with high sensitivity and specificity 22. There are no data to suggest Trichomonas vaginalis causes anorectal infection and therefore use of NAAT to detect Trichomonas vaginalis anorectal infection is not recommended 23.
Trichomonas vaginalis treatment
Trichomonas vaginalis infection can be treated with medication (either metronidazole or tinidazole). These pills are taken by mouth. It is safe for pregnant women to take this medication. It is not recommended to drink alcohol within 24 hours after taking this medication.
Recommended Regimen
- Metronidazole 2 g orally in a single dose
OR - Tinidazole 2 g orally in a single dose
Alternative Regimen
- Metronidazole 500 mg orally twice a day for 7 days
Alcohol consumption should be avoided during treatment with nitroimidazoles. To reduce the possibility of a disulfiram-like reaction, abstinence from alcohol use should continue for 24 hours after completion of metronidazole or 72 hours after completion of tinidazole.
The nitroimidazoles are the only class of antimicrobial medications known to be effective against Trichomonas vaginalis infections. Of these drugs, metronidazole and tinidazole have been cleared by FDA for the oral or parenteral treatment of trichomoniasis. Tinidazole is generally more expensive, reaches higher levels in serum and the genitourinary tract, has a longer half-life than metronidazole (12.5 hours versus 7.3 hours), and has fewer gastrointestinal side effects 24. In randomized clinical trials, recommended metronidazole regimens have resulted in cure rates of approximately 84%–98% 25, and the recommended tinidazole regimen has resulted in cure rates of approximately 92%–100% 26. Randomized controlled trials comparing single 2 g doses of metronidazole and tinidazole suggest that tinidazole is equivalent or superior to metronidazole in achieving parasitologic cure and resolution of symptoms 27.
Metronidazole gel does not reach therapeutic levels in the urethra and perivaginal glands. Because it is less efficacious than oral metronidazole, it is not recommended.
People who have been treated for Trichomonas vaginalis infection can get it again. About 1 in 5 people get infected again within 3 months after receiving treatment. To avoid getting reinfected, make sure that all of your sex partners get treated. Also, wait 7- 10 days after you and your partner have been treated to have sex again. Get checked again if your symptoms come back.
Resumption of Sexual Activity
Patients should be instructed to avoid sex until they and their sex partners have been treated, and until they no longer have any symptoms of Trichomonas vaginalis infection. This usually takes about 7 days.
Post-Treatment Follow-Up
Because of the high rate of reinfection among women treated for trichomoniasis (17% within 3 months in one study) 28, retesting for Trichomonas vaginalis is recommended for all sexually active women within 3 months following initial treatment regardless of whether they believe their sex partners were treated. Testing by nucleic acid amplification can be conducted as soon as 2 weeks after treatment 29. Data are insufficient to support retesting men.
Management of Sex Partners
Concurrent treatment of all sex partners is critical for symptomatic relief, microbiologic cure, and prevention of transmission and reinfections. Current partners should be referred for presumptive therapy to avoid reinfection. Partners should be advised to abstain from intercourse until they and their sex partners have been adequately treated and any symptoms have resolved. Expedited Partner Therapy (EPT) might have a role in partner management for trichomoniasis 30 and can be used in states where permissible by law; however, no one partner management intervention has been shown to be superior in reducing reinfection rates. Though no definitive data exist to guide treatment for partners of persons with persistent or recurrent trichomoniasis in whom nonadherance and reinfection are unlikely, partners benefit from undergoing evaluation and receiving the same regimen as the patient.
Persistent or Recurrent Trichomonas vaginalis infection
Persistent or recurrent infection caused by antimicrobial-resistant Trichomonas vaginalis or other causes should be distinguished from the possibility of reinfection from an untreated sex partner. Although most recurrent Trichomonas vaginalis infections are thought to result from reinfection, some infections might be attributed to antimicrobial resistance. Metronidazole resistance occurs in 4%–10% of cases of vaginal trichomoniasis 31, and tinidazole resistance in 1% 32. In general, Trichomonas vaginalis isolates have lower minimum lethal concentrations to tinidazole than metronidazole 33. Emerging nitroimidazole-resistant trichomoniasis is concerning, because few alternatives to standard therapy exist. Single-dose therapy should be avoided for treating recurrent trichomoniasis that is not likely a result of reinfection. If treatment failure has occurred with metronidazole 2 g single dose and reinfection is excluded, the patient (and their partner[s]) can be treated with metronidazole 500 mg orally twice daily for 7 days. If this regimen fails, clinicians should consider treatment with metronidazole or tinidazole at 2 g orally for 7 days. If several 1-week regimens have failed in a person who is unlikely to have nonadherence or reinfection, testing of the organism for metronidazole and tinidazole susceptibility is recommended 34. Centers for Disease Control and Prevention (CDC) has experience with susceptibility testing for nitroimidazole-resistant Trichomonas vaginalis and treatment management of infected persons and can provide assistance. Higher dose tinidazole at 2–3g for 14 days, often in combination with intravaginal tinidazole, can be considered in cases of nitroimidazole-resistant infections; however, such cases should be managed in consultation with an expert.
Alternative regimens might be effective but have not been systematically evaluated; therefore, consultation with an infectious-disease specialist is recommended. The most anecdotal experience has been with intravaginal paromomycin in combination with high-dose tinidazole 35; clinical improvement has been reported with other alternative regimens including intravaginal boric acid 36 and nitazoxanide 37. The following topically applied agents have shown minimal success (<50%) and are not recommended: intravaginal betadine (povidone-iodine), clotrimazole, acetic acid, furazolidone, gentian violet, nonoxynol-9, and potassium permanganate 38. No other topical microbicide has been shown to be effective against trichomoniasis 39.
Special Considerations
Allergy, Intolerance, and Adverse Reactions
Metronidazole and tinidazole are both nitroimidazoles. Patients with an IgE mediated-type allergy to a nitroimidazole can be managed by metronidazole desensitization according to a published regimen 40 and in consultation with a specialist.
Pregnancy
Trichomonas vaginalis infection in pregnant women is associated with adverse pregnancy outcomes, particularly premature rupture of membranes, preterm delivery, and delivery of a low birthweight infant 41. Although metronidazole treatment produces parasitologic cure, certain trials have shown no significant difference in perinatal morbidity following metronidazole treatment. One trial suggested the possibility of increased preterm delivery in women with Trichomonas vaginalis infection who received metronidazole treatment 42, yet study limitations prevented definitive conclusions regarding the risks of treatment. More recent, larger studies have shown no positive or negative association between metronidazole use during pregnancy and adverse outcomes of pregnancy 43. If treatment is considered, the recommended regimen in pregnant women is metronidazole 2 g orally in a single dose. Symptomatic pregnant women, regardless of pregnancy stage, should be tested and considered for treatment. Treatment of Trichomonas vaginalis infection can relieve symptoms of vaginal discharge in pregnant women and reduce sexual transmission to partners. Although perinatal transmission of trichomoniasis is uncommon, treatment also might prevent respiratory or genital infection of the newborn 44. Clinicians should counsel symptomatic pregnant women with trichomoniasis regarding the potential risks for and benefits of treatment and about the importance of partner treatment and condom use in the prevention of sexual transmission.
The benefit of routine screening for Trichomonas vaginalis in asymptomatic pregnant women has not been established. However, screening at the first prenatal visit and prompt treatment, as appropriate, are recommended for pregnant women with HIV infection, because Trichomonas vaginalis infection is a risk factor for vertical transmission of HIV 45. Pregnant women with HIV who are treated for Trichomonas vaginalis infection should be retested 3 months after treatment.
Although metronidazole crosses the placenta, data suggest that it poses a low risk to pregnant women 46. No evidence of teratogenicity or mutagenic effects in infants has been found in multiple cross-sectional and cohort studies of pregnant women 47. Women can be treated with 2 g metronidazole in a single dose at any stage of pregnancy.
Metronidazole is secreted in breast milk. With maternal oral therapy, breastfed infants receive metronidazole in doses that are lower than those used to treat infections in infants, although the active metabolite adds to the total infant exposure. Plasma levels of the drug and metabolite are measurable, but remain less than maternal plasma levels. Although several reported case series found no evidence of adverse effects in infants exposed to metronidazole in breast milk, some clinicians advise deferring breastfeeding for 12–24 hours following maternal treatment with a single 2-g dose of metronidazole 48. Maternal treatment with metronidazole (400 mg three times daily for 7 days) produced a lower concentration in breast milk and was considered compatible with breastfeeding over longer periods of time 49.
Data from studies involving human subjects are limited regarding use of tinidazole in pregnancy; however, animal data suggest this drug poses moderate risk. Thus, tinidazole should be avoided in pregnant women, and breastfeeding should be deferred for 72 hours following a single 2-g dose of tinidazole.
HIV Infection
Up to 53% of women with HIV infection also are infected with Trichomonas vaginalis 50. Trichomonas vaginalis infection in these women is significantly associated with pelvic inflammatory disease 51, and treatment of trichomoniasis is associated with significant decreases in genital-tract HIV viral load and viral shedding 52. For these reasons, routine screening and prompt treatment are recommended for all women with HIV infection; screening should occur at entry to care and then at least annually thereafter. A randomized clinical trial involving women with HIV infection and Trichomonas vaginalis infection demonstrated that a single dose of metronidazole 2 g orally was less effective than 500 mg twice daily for 7 days 53. Thus, to improve cure rates, women with HIV infection who receive a diagnosis of Trichomonas vaginalis infection should be treated with metronidazole 500 mg orally twice daily for 7 days (rather than with a 2-g single dose of metronidazole). Factors that might interfere with standard single-dose treatment for trichomoniasis in these women include high rates of asymptomatic BV co-infections, use of antiretroviral therapy, changes in vaginal ecology, and impaired immunity 54.
Treatment
Treatment reduces symptoms and signs of Trichomonas vaginalis infection and might reduce transmission. Likelihood of adverse outcomes in women with HIV is also reduced with Trichomonas vaginalis therapy.
Recommended Regimen for Women with HIV Infection
- Metronidazole 500 mg orally twice daily for 7 days
In women with HIV infection who receive a diagnosis of Trichomonas vaginalis infection, retesting is recommended within 3 months following initial treatment; NAAT is encouraged because of higher sensitivity of these tests. Data are insufficient to recommend routine screening, alternative treatment regimens of longer duration, or retesting in men.
- Meites E, Gaydos CA, Hobbs MM, et al. A review of evidence-based care of symptomatic Trichomoniasis and asymptomatic Trichomonas vaginalis infections. Clin Infect Dis. 2015;61 Suppl 8:S837-48.[↩][↩]
- Sutton M, Sternberg M, Koumans EH, McQuillan G, Berman S, Markowitz L. The prevalence of Trichomonas vaginalis infection among reproductive-age women in the United States, 2001-2004. Clin Infect Dis. 2007;45:1319-26.[↩]
- Nijhawan AE, DeLong AK, Celentano DD, et al. The association between Trichomonas infection and incarceration in HIV-seropositive and at-risk HIV-seronegative women. Sex Transm Dis. 2011;38:1094-100.[↩]
- Meites E, Llata E, Braxton J, et al. Trichomonas vaginalis in selected U.S. sexually transmitted disease clinics: testing, screening, and prevalence. Sex Transm Dis. 2013;40:865-9.[↩]
- Kelley CF, Rosenberg ES, OʼHara BM, Sanchez T, del Rio C, Sullivan PS. Prevalence of urethral Trichomonas vaginalis in black and white men who have sex with men. Sex Transm Dis. 2012;39:739.[↩]
- Muzny CA, Rivers CA, Mena LA, Schwebke JR. Genotypic characterization of Trichomonas vaginalis isolates among women who have sex with women in sexual partnerships. Sex Transm Dis. 2012;39:556-8.[↩]
- Swartzendruber A, Sales JM, Brown JL, Diclemente RJ, Rose ES. Correlates of incident Trichomonas vaginalis infections among African American female adolescents. Sex Transm Dis. 2014;41:240-5[↩]
- Schwebke JR, Hobbs MM, Taylor SN, et al. Molecular testing for Trichomonas vaginalis in women: results from a prospective U.S. clinical trial. J Clin Microbiol. 2011;49:4106-11.[↩][↩][↩]
- Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. Diseases characterized by vaginal discharge: Trichomoniasis. MMWR Recomm Rep. 2015;64(No. RR-3):1-137.[↩][↩]
- Petrin D, Delgaty K, Bhatt R, Garber G. Clinical and microbiological aspects of Trichomonas vaginalis. Clin Microbiol Rev. 1998;11:300-17.[↩][↩][↩]
- Hughes JP, Baeten JM, Lingappa JR, et al. Determinants of per-coital-act HIV-1 infectivity among African HIV-1-serodiscordant couples. J Infect Dis. 2012;205:358-65.[↩]
- Masese LN, Graham SM, Gitau R, et al. A prospective study of vaginal trichomoniasis and HIV-1 shedding in women on antiretroviral therapy. BMC Infect Dis. 2011;11:307.[↩]
- Cu-Uvin S, Ko H, Jamieson DJ, et al. Prevalence, incidence, and persistence or recurrence of trichomoniasis among human immunodeficiency virus (HIV)-positive women and among HIV-negative women at high risk for HIV infection. Clin Infect Dis. 2002;15;34:1406-11.[↩]
- Mann JR, McDermott S, Gill T. Sexually transmitted infection is associated with increased risk of preterm birth in South Carolina women insured by Medicaid. J Matern Fetal Neonatal Med. 2010;23:563-8.[↩]
- Trintis J, Epie N, Boss R, Riedel S. Neonatal Trichomonas vaginalis infection: a case report and review of literature. Int J STD AIDS. 2010;21:606-7.[↩]
- Bachmann LH, Hobbs MM, Seña AC, et al. Trichomonas vaginalis genital infections: progress and challenges. Clin Infect Dis. 2011;53 Suppl 3:S160-72.[↩][↩][↩]
- Stoner KA, Rabe LK, Meyn LA, Hillier SL. Survival of Trichomonas vaginalis in wet preparation and on wet mount. Sex Transm Infect. 2013;89:485-8.[↩]
- Hainer BL, Gibson MV. Vaginitis. Am Fam Physician. 2011;83:807-15.[↩]
- Campbell L, Woods V, Lloyd T, Elsayed S, Church DL. Evaluation of the OSOM Trichomonas rapid test versus wet preparation examination for detection of Trichomonas vaginalis vaginitis in specimens from women with a low prevalence of infection. J Clin Microbiol. 2008;46:3467-9.[↩]
- Andrea SB, Chapin KC. Comparison of Aptima Trichomonas vaginalis transcription-mediated amplification assay and BD affirm VPIII for detection of T. vaginalis in symptomatic women: performance parameters and epidemiological implications. J Clin Microbiol. 2011;49:866-9.[↩]
- Hollman D, Coupey SM, Fox AS, Herold BC. Screening for Trichomonas vaginalis in high-risk adolescent females with a new transcription-mediated nucleic acid amplification test (NAAT): associations with ethnicity, symptoms, and prior and current STIs. J Pediatr Adolesc Gynecol. 2010;23:312-6.[↩]
- Van Der Pol B, Kraft CS, Williams JA. Use of an adaptation of a commercially available PCR assay aimed at diagnosis of chlamydia and gonorrhea to detect Trichomonas vaginalis in urogenital specimens. J Clin Microbiol. 2006;44:366-73.[↩]
- Cosentino LA, Campbell T, Jett A, et al. Use of nucleic acid amplification testing for diagnosis of anorectal sexually transmitted infections. J Clin Microbiol. 2012;50:2005-8.[↩]
- Viitanen J, Haataja H, Mannisto PT. Concentrations of metronidazole and tinidazole in male genital tissues. Antimicrob Agents Chemother 1985;28:812–4.[↩]
- Spence MR, Harwell TS, Davies MC, et al. The minimum single oral metronidazole dose for treating trichomoniasis: a randomized, blinded study. Obstet Gynecol 1997;89(5 Pt 1):699–703.[↩]
- Prasertsawat PO, Jetsawangsri T. Split-dose metronidazole or single-dose tinidazole for the treatment of vaginal trichomoniasis. Sex Transm Dis 1992;19:295–7.[↩]
- Forna F, Gulmezoglu AM. Interventions for treating trichomoniasis in women. Cochrane Database Syst Rev 2003;2:CD000218[↩]
- Peterman TA, Tian LH, Metcalf CA, et al. High incidence of new sexually transmitted infections in the year following a sexually transmitted infection: a case for rescreening. Ann Intern Med 2006;145:564–72.[↩]
- Williams JA, Van Der Pol B, Ofner S, et al. Time from treatment to negative PCR results for C. trachomatis, N. gonorrhoeae and T. vaginalisExternal. National STD Prevention Conference; March 10-13, 2008, 2008; Chicago, IL.[↩]
- Schwebke JR, Desmond RA. A randomized controlled trial of partner notification methods for prevention of trichomoniasis in women. Sex Transm Dis 2010;37:392–6.[↩]
- Kirkcaldy RD, Augostini P, Asbel LE, et al. Trichomonas vaginalis antimicrobial drug resistance in 6 US cities, STD Surveillance Network, 2009-2010. Emerg Infect Dis 2012;18:939–43.[↩]
- Schwebke JR, Barrientes FJ. Prevalence of Trichomonas vaginalis isolates with resistance to metronidazole and tinidazole. Antimicrob Agents Chemother 2006;50:4209–10.[↩]
- Crowell AL, Sanders-Lewis KA, Secor WE. In vitro metronidazole and tinidazole activities against metronidazole-resistant strains of Trichomonas vaginalis. Antimicrob Agents Chemother 2003;47:1407–9.[↩]
- Bosserman EA, Helms DJ, Mosure DJ, et al. Utility of antimicrobial susceptibility testing in Trichomonas vaginalis-infected women with clinical treatment failure. Sex Transm Dis 2011;38:983–7.[↩]
- Nyirjesy P, Gilbert J, Mulcahy LJ. Resistant trichomoniasis: successful treatment with combination therapy. Sex Transm Dis 2011;38:962–3.[↩]
- Muzny C, Barnes A, Mena L. Symptomatic Trichomonas vaginalis infection in the setting of severe nitroimidazole allergy: successful treatment with boric acid. Sex Health 2012;9:389–91.[↩]
- Dan M, Sobel JD. Failure of nitazoxanide to cure trichomoniasis in three women. Sex Transm Dis 2007;34:813–4.[↩]
- Sena AC, Bachmann LH, Hobbs MM. Persistent and recurrent Trichomonas vaginalis infections: epidemiology, treatment and management considerations. Expert Rev Anti Infect Ther 2014;12:673–85.[↩]
- Obiero J, Mwethera PG, Wiysonge CS. Topical microbicides for prevention of sexually transmitted infections. Cochrane Database Syst Rev 2012;6:CD007961.[↩]
- Helms DJ, Mosure DJ, Secor WE, et al. Management of Trichomonas vaginalis in women with suspected metronidazole hypersensitivity. Am J Obstet Gynecol 2008;198:e371–7.[↩]
- Mann JR, McDermott S. Are maternal genitourinary infection and pre-eclampsia associated with ADHD in school-aged children? J Atten Disord 2011;15:667–73.[↩]
- Klebanoff MA, Carey JC, Hauth JC, et al. Failure of metronidazole to prevent preterm delivery among pregnant women with asymptomatic Trichomonas vaginalis infection. New England Journal of Medicine 2001;345:487–93.[↩]
- Gulmezoglu AM, Azhar M. Interventions for trichomoniasis in pregnancy. Cochrane Database Syst Rev 2011:CD000220.[↩]
- Trintis J, Epie N, Boss R, et al. Neonatal Trichomonas vaginalis infection: a case report and review of literature. International journal of STD and AIDS 2010;21:606–7[↩]
- Gumbo FZ, Duri K, Kandawasvika GQ, et al. Risk factors of HIV vertical transmission in a cohort of women under a PMTCT program at three peri-urban clinics in a resource-poor setting. J Perinatol 2010;30:717–23.[↩]
- Briggs GC, Freeman RK, Yaffe SJ. Drugs in Pregnancy and Lactation, 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.[↩]
- Mann JR, McDermott S, Zhou L, et al. Treatment of trichomoniasis in pregnancy and preterm birth: an observational study. J Women’s Health 2009;18:493–7.[↩]
- Erickson SH, Oppenheim GL, Smith GH. Metronidazole in breast milk. Obstet Gynecol 1981;57:48–50.[↩]
- Golightly P, Kearney L. Metronidazole— is it safe to use with breastfeeding? United Kingdom National Health Service, UKMI;2012.[↩]
- Miller M, Liao Y, Wagner M, et al. HIV, the clustering of sexually transmitted infections, and sex risk among African American women who use drugs. Sex Transm Dis 2008;35:696–702.[↩]
- Moodley P, Wilkinson D, Connolly C, et al. Trichomonas vaginalis is associated with pelvic inflammatory disease in women infected with human immunodeficiency virus. Clin Infect Dis 2002;34:519–22.[↩]
- Anderson BL, Firnhaber C, Liu T, et al. Effect of trichomoniasis therapy on genital HIV viral burden among African women. Sex Transm Dis 2012;39:638–42.[↩]
- Kissinger P, Mena L, Levison J, et al. A randomized treatment trial: single versus 7-day dose of metronidazole for the treatment of Trichomonas vaginalis among HIV-infected women. J Acquir Immune Defic Syndr 2010;55:565–71.[↩]
- Balkus JE, Richardson BA, Mochache V, et al. A prospective cohort study comparing the effect of single-dose 2 g metronidazole on Trichomonas vaginalis infection in HIV-seropositive versus HIV-seronegative women. Sex Transm Dis 2013;40:499–505.[↩]




{kind=link}