Contents
- What is truncus arteriosus
What is truncus arteriosus
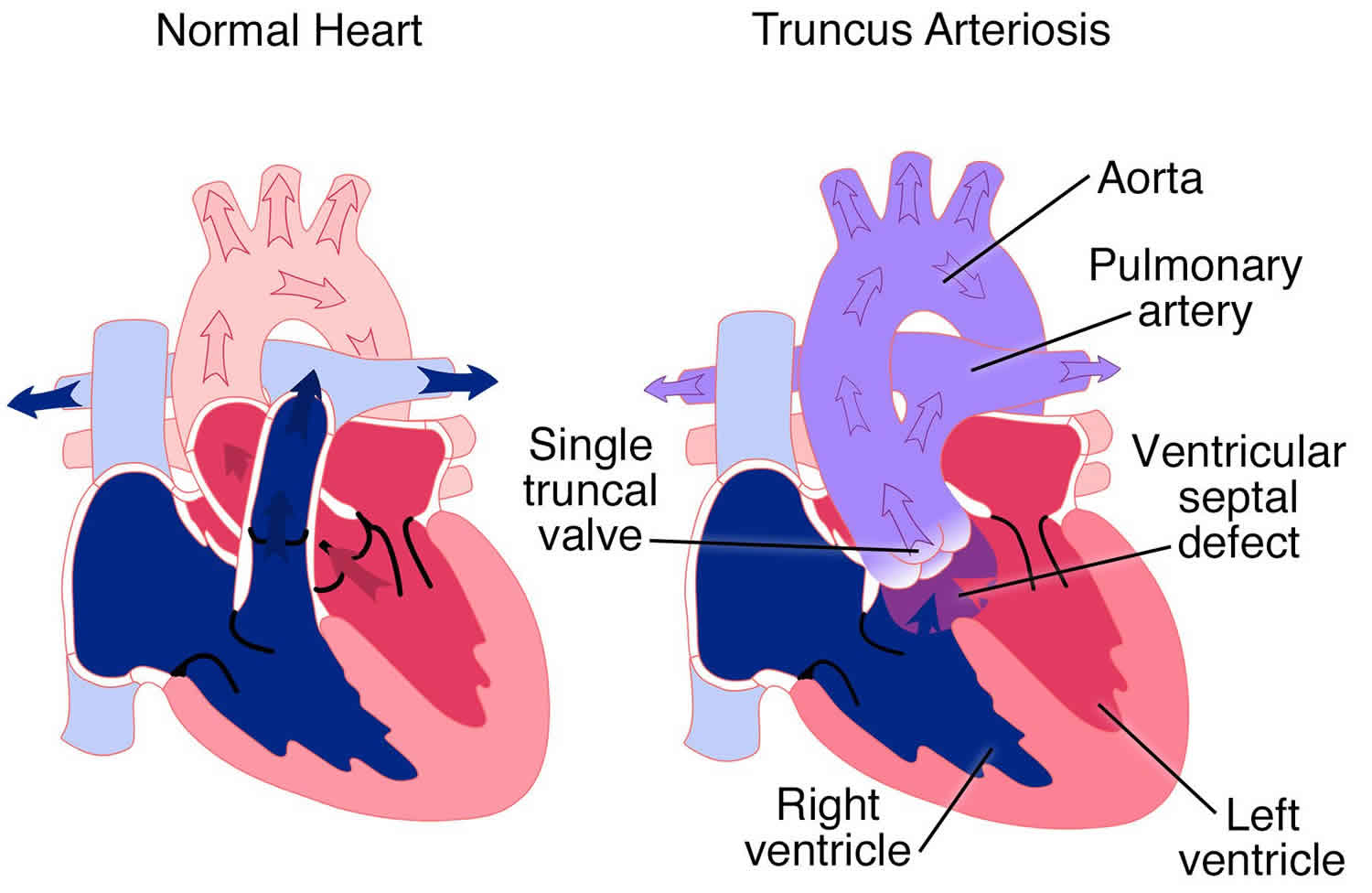
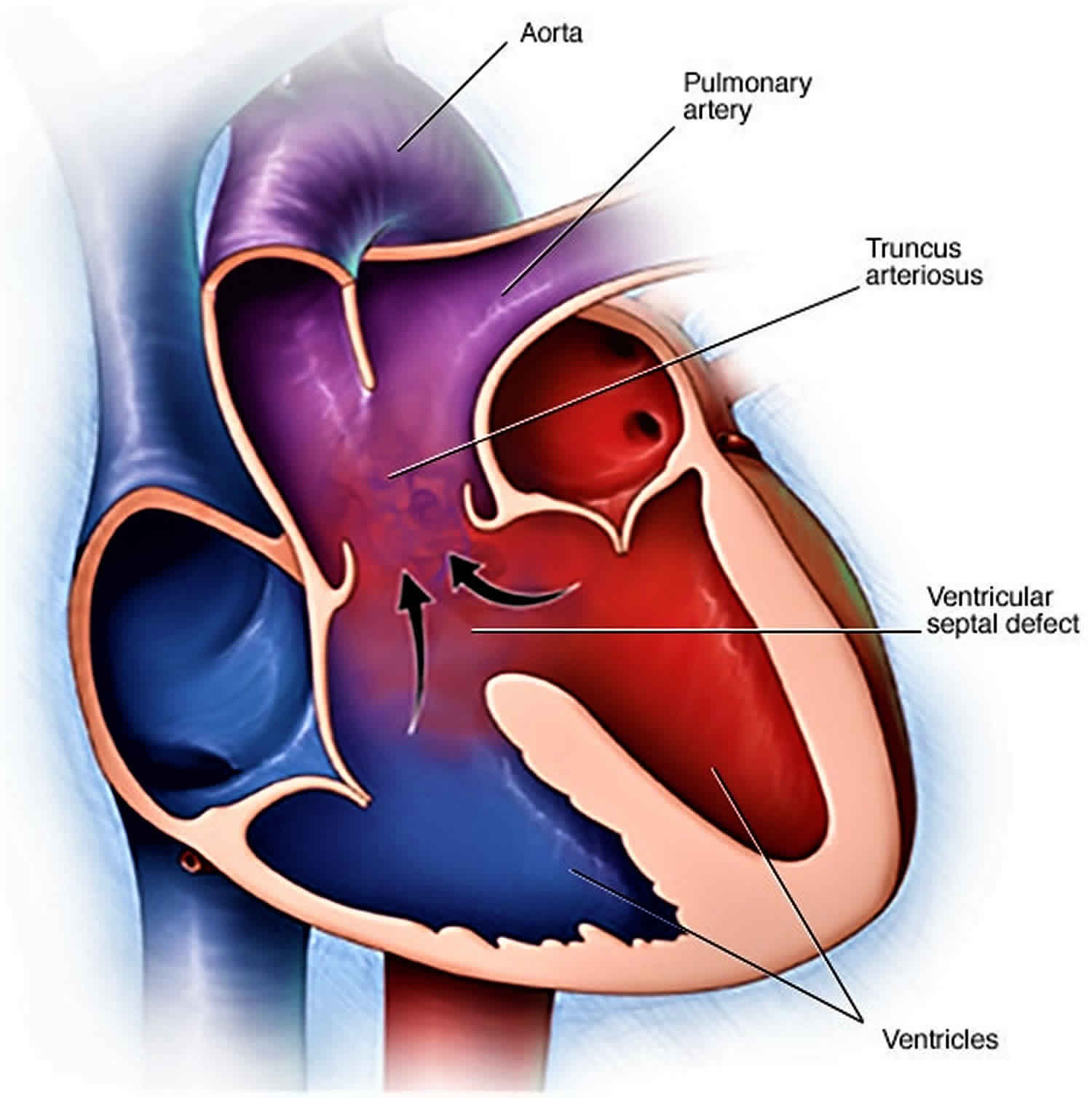
Persistent truncus arteriosus is a rare congenital (present at birth) heart defect where one large blood vessel (truncus arteriosus) comes out of the right and left ventricles instead of two separate blood vessels (pulmonary artery and aorta) coming out of the heart. In addition, there is usually a hole — known as a ventricular septal defect (VSD) — between the two lower chambers of the heart. As a result of truncus arteriosus, oxygen-poor blood that should go to the lungs and oxygen-rich blood that should go to the rest of the body are mixed together. Some of this mixed blood goes to the lungs, and some goes to the rest of the body. Often, more blood than usual ends up going to the lungs. This creates severe circulatory problems. If left untreated, truncus arteriosus can be fatal.
If truncus arteriosus is not treated, two problems occur:
- Too much blood circulation in the lungs may cause extra fluid to build up in and around them. This makes it hard to breathe.
- If left untreated and more than normal blood flows to the lungs for a long time, the blood vessels to the lungs become permanently damaged. Over time, it becomes very hard for the heart to force blood to them. This is called pulmonary hypertension, which can be life threatening.
Truncus arteriosus occurs in less than one out of every 10,000 live births 1. While truncus arteriosus accounts for less than 1% of all congenital heart lesions, it accounts for 4% of critical congenital heart defects 2. Truncus arteriosus can occur by itself or as part of certain genetic disorders. There are about 300 cases of truncus arteriosus per year in the United States 3.
Some babies with a truncus arteriosus have additional abnormalities. In particular, the valve in the single artery of the heart may not function normally. There may also be a narrowing in either the aorta or the pulmonary arteries.
Sometimes, there can also be a chromosome abnormality – most often an abnormality called ‘22q11 deletion’. Babies born with 22q11 deletion may have learning difficulties and may also have difficulty fighting some infections. If your baby has a chromosomal abnormality such as 22q11 or any other type, your child’s cardiologist will talk to you about it.
Surgery is needed to treat this condition. Surgery to repair truncus arteriosus is generally successful, especially if the repair occurs before your baby is one month old 1, but there are often residual and potential complications that require regular, long-term cardiology follow-up 4.
The surgery creates 2 separate arteries. In most cases, the truncal vessel is kept as the new aorta. A new pulmonary artery is created using tissue from another source or using a man-made tube. The branch pulmonary arteries are sewn to this new artery. The hole between the ventricles is closed.
In normal circulation, the pulmonary artery comes out of the right ventricle and the aorta comes out of the left ventricle, which are separate from each other. And in a normal heart, the blood follow this cycle: body-heart-lungs-heart-body. When a person has a truncus arteriosus, the blood leaving the heart does not follow this path. It has only one vessel, instead of two separate ones, pulmonary arteries for the lungs and the aorta for the body. With only one artery, there is no specific path to the lungs for oxygen before returning to the heart to deliver oxygen to the body.
If the skin, lips, or nail beds look blue or if the child seems to be very short of breath, take the child to the emergency room or have the child examined promptly.
Seek medical treatment if you notice that your baby has any of the following problems:
- Blue coloring of the skin (cyanosis)
- Poor feeding
- Excessive sleepiness
- Appears lethargic
- Appears overly tired or mildly short of breath
- Does not eat well
- Does not seem to be growing or developing normally
Some signs of truncus arteriosus may indicate a problem that needs urgent care. If your baby experiences any of the following signs and symptoms and you can’t see your baby’s doctor immediately, seek emergency medical care:
- Rapid, shallow or labored breathing
- Worsening of blue coloring of the skin
- Loss of consciousness
Figure 1. Normal heart
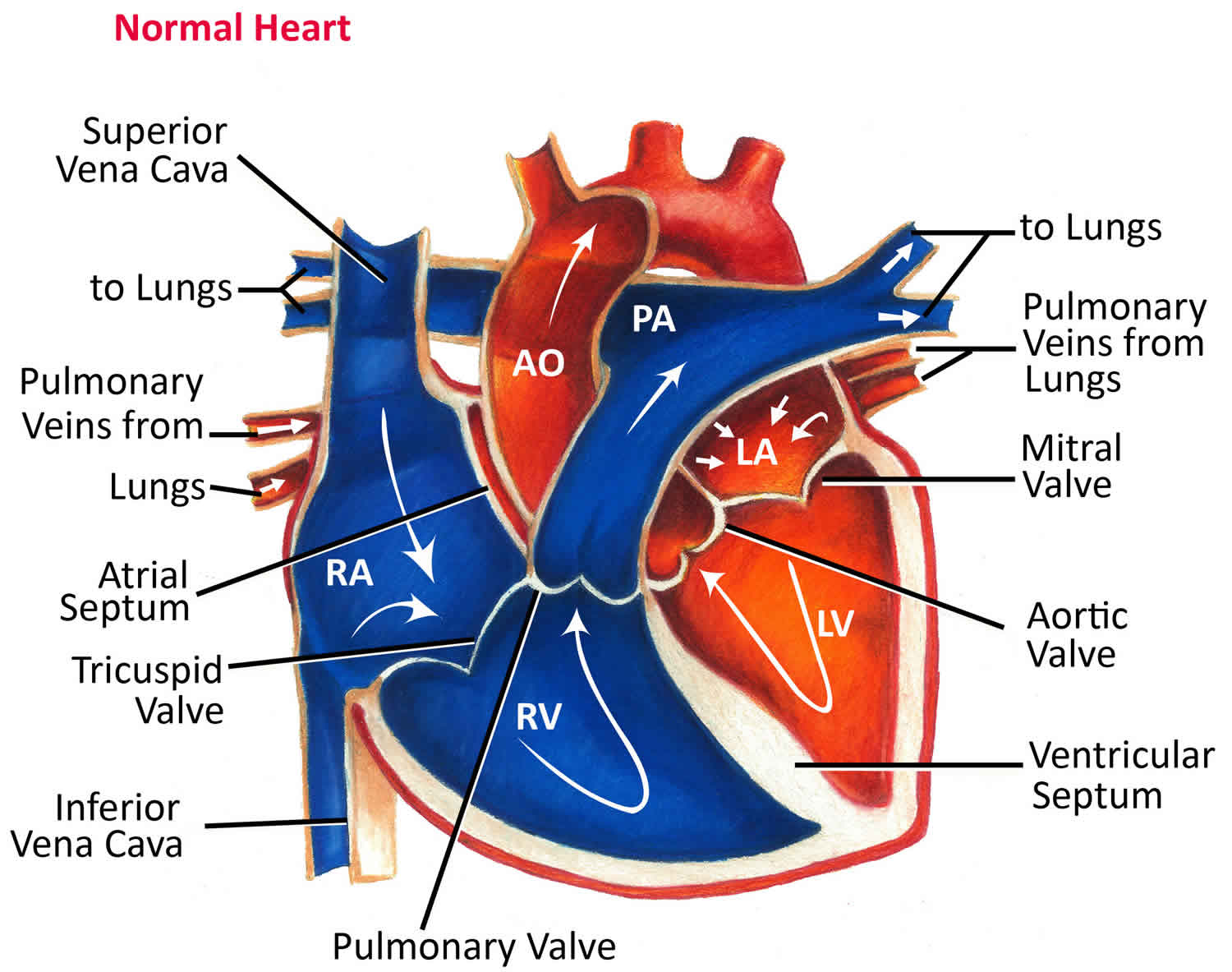
Figure 2. Truncus arteriosus
What happens as my child with truncus arteriosus grows up?
Although surgery can give your child a better quality of life, sadly it isn’t possible to completely correct the heart abnormality and we do not know how long children with this condition will live for.
Over time, the tube between the right ventricle and the pulmonary artery will need to be replaced. The timing of this will vary in every case and will depend on how well the tube and valve function with age. In children where the original single outlet valve (which acts as the aortic valve after surgery) does not function well, this valve will also need to be replaced periodically (every 10 to 15 years) throughout their life. This is usually done by open heart surgery, but some adults may be suitable for valve replacement by key hole catheter surgery.
Unfortunately, even many years after apparently successful surgery, new problems may arise which require further treatment. Such problems include narrowing of the arteries in the lungs and the development of abnormal heart rhythms. These complications can usually be treated, but some can be serious and in rare cases they may even be fatal. It’s very important that your child is regularly reviewed by a cardiologist in an outpatients clinic, even if they appear well.
Children with a truncus arteriosus are always limited to some extent in their physical activities, but specific restrictions on exercise are usually not necessary. It is usually best to allow children with this condition to join in with their friends’ activities, including some sport at school, and for them to judge for themselves what they are able to do.
Will I need more surgery?
Conduit Replacement
The conduit connecting the right ventricle to the pulmonary artery conduit may become obstructed (stenotic) over time and may need to be replaced (see above). Timing of the replacement varies. The peripheral pulmonary arteries also may become narrowed and require treatment.
Sometimes conduits and peripheral pulmonary artery obstructions may be dilated using a balloon-tipped catheter or an expandable stent in the cardiac catheterization laboratory. This procedure may help extend the time between conduit changes. Sometimes surgery is required to enlarge the narrowed area. Your cardiologist will decide whether a balloon/stent procedure or surgery is best for you.
Truncal/Aortic Valve Replacement
The functional aortic valve is actually the large truncal valve from the single vessel, which arose over the ventricular septal defect before surgical repair. This valve sometimes becomes leaky over time and may need to be replaced.
What is the risk of having another child with a congenital heart condition?
If you have one child with a congenital heart condition, there is around a 1 in 40 chance that if you have another child, they will have a heart condition too 5. However, this risk may be higher (or lower) depending on the type of congenital heart condition your child has. Because your risk of having another child with congenital heart condition is higher than it is for other people, your doctor may offer you a special scan at an early stage in future pregnancies, to look at the baby’s heart.
Do ask your midwife or doctor for more information on having a scan earlier than usual. Do be aware that if you have more than one child with congenital heart condition, the specific condition may not always be the same.
Truncus arteriosus types
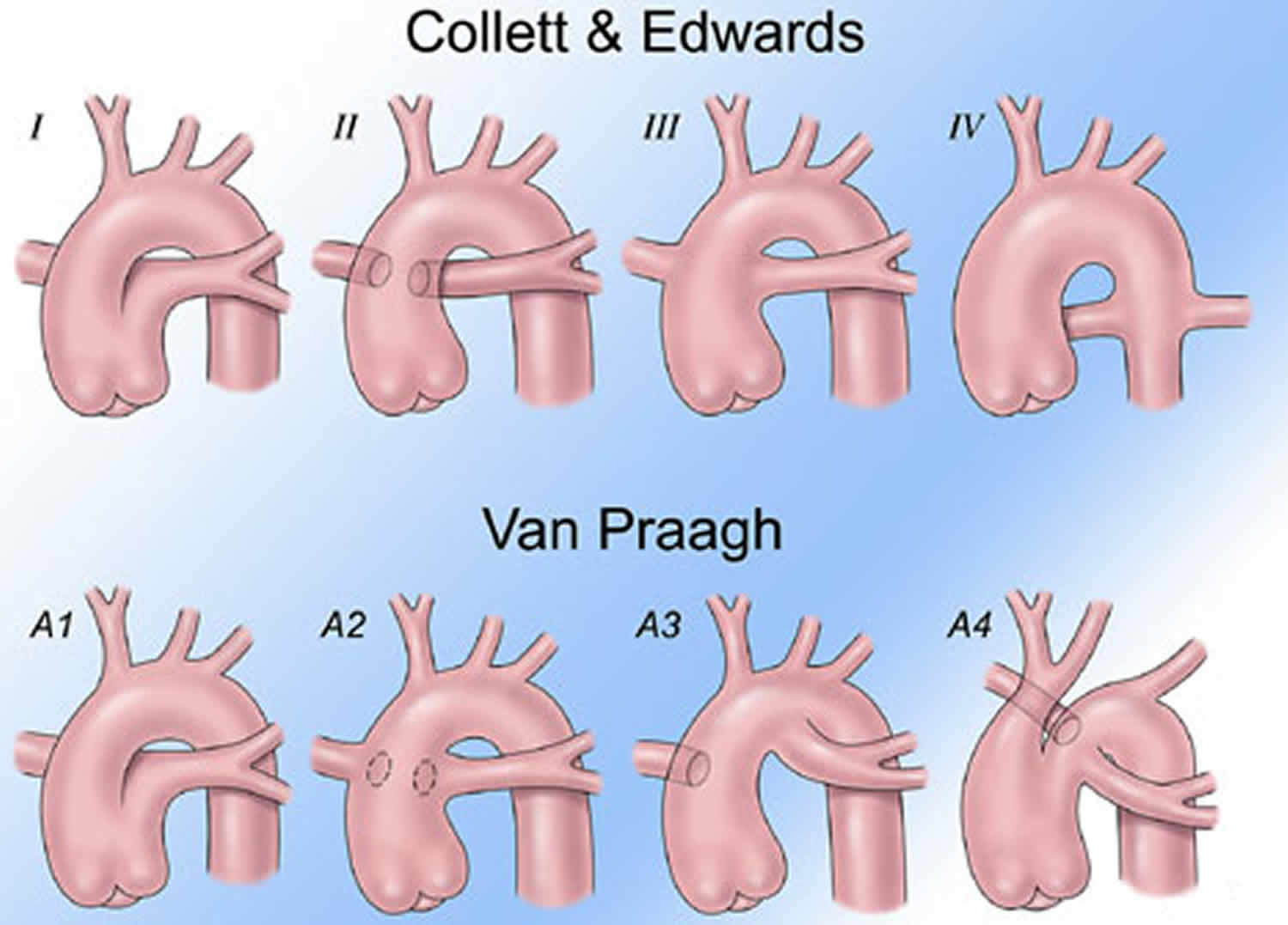
Several classification schemes have been proposed, none of which is ideal 6. The earliest classification, developed by Collett and Edwards in 1949, includes truncus arteriosus types 1-4, as follows 7:
- Truncus arteriosus type 1 is characterized by origin of a single pulmonary trunk from the left lateral aspect of the common trunk, with branching of the left and right pulmonary arteries from the pulmonary trunk.
- Truncus arteriosus type 2 is characterized by separate but proximate origins of the left and right pulmonary arterial branches from the posterolateral aspect of the common arterial trunk.
- In truncus arteriosus type 3, the branch pulmonary arteries originate independently from the common arterial trunk or aortic arch, most often from the left and right lateral aspects of the trunk. This occasionally occurs with origin of one pulmonary artery from the underside of the aortic arch, usually from a ductus arteriosus.
- Type 4 truncus arteriosus, originally proposed by Collett and Edwards as a form of the lesion with neither pulmonary arterial branch arising from the common trunk, is now recognized to be a form of pulmonary atresia with ventricular septal defect rather than truncus arteriosus.
Collett and Edwards describe variations of each of these types.
In 1965, Van Praaghs proposed the other commonly cited classification scheme that also includes 4 primary types, as follows 8:
- Type A1 is identical to the type 1 of Collett and Edwards.
- Type A2 includes Collett and Edwards type 2 and most cases of type 3, namely those with separate origin of the branch pulmonary arteries from the left and right lateral aspects of the common trunk.
- Type A3 includes cases with origin of one branch pulmonary artery (usually the right) from the common trunk, with pulmonary blood supply to the other lung provided either by a pulmonary artery arising from the aortic arch (a subtype of Collett and Edwards type 3) or by systemic to pulmonary arterial collaterals.
- Type A4 is defined not by the pattern of origin of branch pulmonary arteries, but rather by the coexistence of an interrupted aortic arch. In the vast majority of cases of type A4, which fall into the type 1 of Collett and Edwards, the pulmonary arteries arise as a single pulmonary trunk that then branches. In any of these patterns, intrinsic stenosis, hypoplasia, or both may be present in one or both branch pulmonary arteries, which may have an effect on management and outcome.
The Van Praagh scheme is combined with Collett and Edwards types in Figure 3 below.
Figure 3. Truncus arteriosus types
Truncus arteriosus causes
Truncus arteriosus occurs during fetal growth when your baby’s heart is developing and is, therefore, present at birth (congenital). In most cases the cause is unknown. While no direct cause is known, truncus arteriosus is frequently associated with 22q11 genetic mutations 9. DiGeorge syndrome or velocardiofacial syndrome, often included together as variations of CATCH-22 syndrome, are present in approximately 30-35% of patients with truncus arteriosus; most of these patients have deletions in band 22q11 6.
The most common noncardiac anomalies in patients with truncus arteriosus are those typically found in association with CATCH-22 syndrome, such as velopharyngeal insufficiency, cleft palate, and thymic and parathyroid dysfunction.
Other noncardiac anomalies found sporadically in patients with truncus arteriosus include renal abnormalities, vertebral and rib anomalies, and anomalies of the alimentary tract 6.
The formation of the fetal heart is a complex process. At a certain point, all babies have a single large vessel (truncus arteriosus) exiting the heart. During normal development of the heart, however, this very large single vessel divides into two parts. One part becomes the lower portion of the aorta, which is attached to the left ventricle. The other part becomes the lower portion of the pulmonary artery, which is attached to the right ventricle.
Also during this process, the ventricles develop into two chambers separated by a wall (septum).
In babies born with truncus arteriosus, the single large vessel never finished dividing into two separate vessels. And the wall separating the two ventricles never closed completely, resulting in a single blood vessel arising from the heart, and a large hole between the two chambers (ventricular septal defect).
In addition to the primary defects of truncus arteriosus, the valve controlling blood flow from the ventricles to the singe large vessel (truncal valve) is often defective, allowing blood to flow backward into the heart.
Risk factors for truncus arteriosus
While the exact cause of congenital heart defects, such as truncus arteriosus, is unknown, several factors may increase the risk of a baby being born with a heart condition. These include:
- Viral illness during pregnancy. If a woman contracts rubella (German measles) or another viral illness during early pregnancy, the risk of congenital heart defects in her baby is increased.
- Poorly controlled diabetes during pregnancy. Diabetes that isn’t well-managed can increase the risk of birth defects, including heart defects.
- Certain medications taken during pregnancy. Many medications aren’t recommended for use during pregnancy because of potential risks to the fetus.
- Certain chromosomal disorders. Children with DiGeorge’s syndrome or velocardiofacial syndrome have an increased risk of truncus arteriosus. These conditions are caused by an extra or defective chromosome.
- Smoking during pregnancy. Continuing to smoke while pregnant increases the risk that the baby will be born with a heart defect.
Truncus arteriosus prevention
In most cases, congenital heart defects, such as truncus arteriosus, can’t be prevented. If you have a family history of heart defects or if you already have a child with a congenital heart defect, you and your partner may consider talking with a genetic counselor and a cardiologist experienced in congenital heart defects before you make a decision about becoming pregnant.
If you’re thinking about becoming pregnant, there are several steps you can take to help ensure a healthy baby, including:
- Getting vaccinated before getting pregnant. Certain viruses, such as rubella (German measles), can be very harmful during pregnancy, so it’s important to make sure your immunizations are up to date before you get pregnant.
- Avoiding dangerous medications. Check with your doctor before taking any medications if you’re pregnant or thinking about becoming pregnant. Many drugs aren’t recommended for use during pregnancy.
- Taking folic acid. One of the few steps you can take to help prevent birth defects, including spinal cord, brain and possibly heart defects, is to take 400 micrograms of folic acid daily.
- Controlling diabetes. If you’re a woman with diabetes, talk to your doctor about pregnancy risks associated with diabetes and how best to manage the disease during your pregnancy.
Truncus arteriosus symptoms
Infants with truncus arteriosus usually are in distress in the first few days of life because of the high amount of blood going to the lungs which makes the heart work harder. Infants with truncus arteriosus can have a bluish looking skin color, called cyanosis, because their blood doesn’t carry enough oxygen.
Signs and symptoms of truncus arteriosus often develop in the first few days of life. They include:
- Blue coloring of the skin (cyanosis)
- Poor feeding
- Pounding heart
- Excessive sleepiness
- Poor growth
- Shortness of breath (dyspnea)
- Rapid breathing (tachypnea)
- Delayed growth or growth failure
- Fatigue
- Lethargy
- Widening of the finger tips (clubbing)
Truncus arteriosus complications
The abnormal heart structures of truncus arteriosus result in severe problems with blood circulation.
Because the ventricles aren’t separated and all blood exits from a single vessel, the oxygen-rich blood and the oxygen-poor blood mix together — resulting in blood that doesn’t carry enough oxygen. The mixed blood flows from the single large vessel to the lungs, the arteries of the heart and the rest of the body.
If your baby has truncus arteriosus, the abnormal circulation of blood usually results in:
- Respiratory problems. The abnormal distribution of blood results in too much blood flowing into the lungs. Excessive fluid in the lungs makes it difficult for your baby to breathe.
- High blood pressure in the lungs (pulmonary hypertension). Increased blood flow to the lungs causes the lungs’ blood vessels to narrow, increasing blood pressure in the lungs and making it increasingly difficult for your baby’s heart to pump blood into the lungs.
- Enlargement of the heart (cardiomegaly). Pulmonary hypertension and the increased blood flow through the heart force your baby’s heart to work harder than normal, causing it to enlarge. The enlarged heart gradually weakens.
- Heart failure. The increased workload and poor oxygen supply also result in weakening of your baby’s heart. These factors can contribute to heart failure, the inability of the heart to supply the body with enough blood.
Complications later in life
Even with successful surgical repair of the heart during infancy, other complications associated with truncus arteriosus may occur later in life:
- Progressive pulmonary hypertension
- Leaky heart valves (regurgitation)
- Heart rhythm disturbances (arrhythmias)
- Problems related to prior operation
Common signs and symptoms of these complications include shortness of breath when exercising, dizziness, fatigue, abdominal swelling, swelling in the legs and feet, and a sensation of rapid, fluttering heartbeats (palpitations).
Truncus arteriosus diagnosis
Truncus arteriosus may be diagnosed during pregnancy or soon after the baby is born. A murmur is most often heard when listening to the heart with a stethoscope.
During Pregnancy
During pregnancy, there are screening tests (also called prenatal tests) to check for birth defects and other conditions. Some heart defects might be seen during an ultrasound (which creates pictures of the body). If a health care provider suspect a baby might have truncus arteriosus, the health care provider can request a fetal echocardiogram to confirm the diagnosis. A fetal echocardiogram is a more detailed ultrasound of the baby’s heart. This test can show problems with the structure of the heart, like a single large vessel coming from the heart, and how the heart is working with this defect.
After a Baby is Born
For babies with truncus arteriosus, much of their medical care is provided by a pediatric cardiologist along with a pediatric cardiac surgeon and often a whole team of specialized staff. For adults with truncus arteriosus, much of their medical care is provided by an adult congenital cardiologist along with a congenital cardiac surgeon and often a whole team of specialized staff.
If a health care provider suspects a baby might have truncus arteriosus, the health care provider can request an echocardiogram to confirm the diagnosis. An echocardiogram is an ultrasound of the heart that can show problems with the structure of the heart, like the single large vessel coming from the heart or misshapen truncal valve. It can also show how the heart is working (or not) with this defect, like if the blood is leaking back into the heart or if it is moving through a hole between the ventricles. Echocardiograms are also useful for helping the doctor follow the child’s health over time.
Truncus arteriosus is a critical congenital heart defect that may be detected with newborn pulse oximetry screening (also known as pulse ox). Pulse oximetry is a simple bedside test to determine the amount of oxygen in a baby’s blood. Low levels of oxygen in the blood can be a sign of a critical congenital heart defect. Newborn screening using pulse oximetry can identify some infants with a critical congenital heart defect, like truncus arteriosus, before they show any symptoms.
In order for the pediatric or adult congenital cardiologist to check the condition of your or your baby’s heart and make a diagnosis, he or she will order one or more tests:
- Echocardiogram. An echocardiogram shows the structure and function of your or your baby’s heart. A transducer that emits high-pitched sound waves is moved across the skin over your or your baby’s heart. The sound waves echo off internal structures, producing images on a monitor. In a baby with truncus arteriosus, the echocardiogram reveals the single large vessel leading from the heart, a hole in the wall between the left and right ventricles, and abnormalities in the valve between the large vessel and the ventricles. The test can also show how much blood is flowing to your baby’s lungs, and whether there’s a risk of high blood pressure in the lungs.
- Chest x-ray. An X-ray exam uses radiation to produce still images of internal organs and structures. A chest X-ray of you or your baby can show the size of the heart, abnormalities in the lungs and excess fluid in the lungs.
- ECG
- Cardiac catheterization. Standard angiographic images from the truncal root can aid in the assessment of coronary arterial anatomy, if echocardiography is inadequate, and in the assessment of regurgitation through the truncal valve. Cardiac catheterization is generally not required prior to repair in neonates and young infants with truncus arteriosus 10. Catheterization is an important tool for evaluating some of the most common anatomic problems in patients with repaired truncus arteriosus, such as obstruction of the surgical reconstructed right ventricular outflow tract, branch pulmonary arterial stenosis, truncal valve regurgitation, and, in patients repaired later in life, pulmonary vascular obstructive disease.
- MRI or CT scan of the heart. MRI modality provides excellent imaging for characterizing anatomy, and may be especially useful in reconstructing complex pulmonary arterial anatomy in older patients with truncus arteriosus.
Truncus arteriosus treatment
Infants with truncus arteriosus must have surgery. Multiple procedures or surgeries may be necessary, especially as your child grows. Medications may be given before surgery to help improve the health of the heart.
Children and adults with surgically repaired truncus arteriosus must have regular follow-up with their cardiology team.
The good news is, most surgeries to repair a truncus arteriosus are successful, but the risks will depend very much on the exact abnormalities present. All heart operations are serious and carry a small risk of death, or of major complications such as brain damage, kidney damage, or lung complications such as pneumonia.
Medications
Some babies with truncus arteriosus also will need medicines to help strengthen the heart muscle, lower their blood pressure, and help their body get rid of extra fluid.
Medications that may be prescribed before surgery include:
- Diuretics. Often called water pills, diuretics increase the frequency and volume of urination, preventing fluid from collecting in the body, which is a common effect of heart failure.
- Ionotropic agents. This type of medication strengthens the heart’s contractions.
Nutrition
Some babies with truncus arteriosus might become tired while feeding and might not eat enough to gain weight. To make sure babies have a healthy weight gain, a special high-calorie formula might be prescribed. Some babies become extremely tired while feeding and might need to be fed through a feeding tube.
Truncus arteriosus repair
Most infants with truncus arteriosus have surgery within the first few weeks after being born. The exact procedure will depend on your baby’s condition. Most commonly your baby’s surgeon will:
- Close the ventricular septal defect between the two ventricles with a patch
- Use the original single blood vessel to create a new aorta to carry oxygen-rich blood from the left ventricle out to the body.
- Use an artificial tube (conduit) with an artificial valve to connect the right ventricle to the arteries going to the lungs in order to carry oxygen-poor blood to the lungs.
After corrective surgery, your child will need lifelong follow-up care with a cardiologist to monitor his or her heart health. The cardiologist may recommend that your child limit physical activity, particularly intense competitive sports.
Your child will need to take antibiotics before dental procedures and other surgical procedures to prevent infections.
Because the artificial conduit does not grow with your child, follow-up surgeries to replace the conduit valve are necessary as he or she gets older.
Figure 4. Truncus arteriosus repair
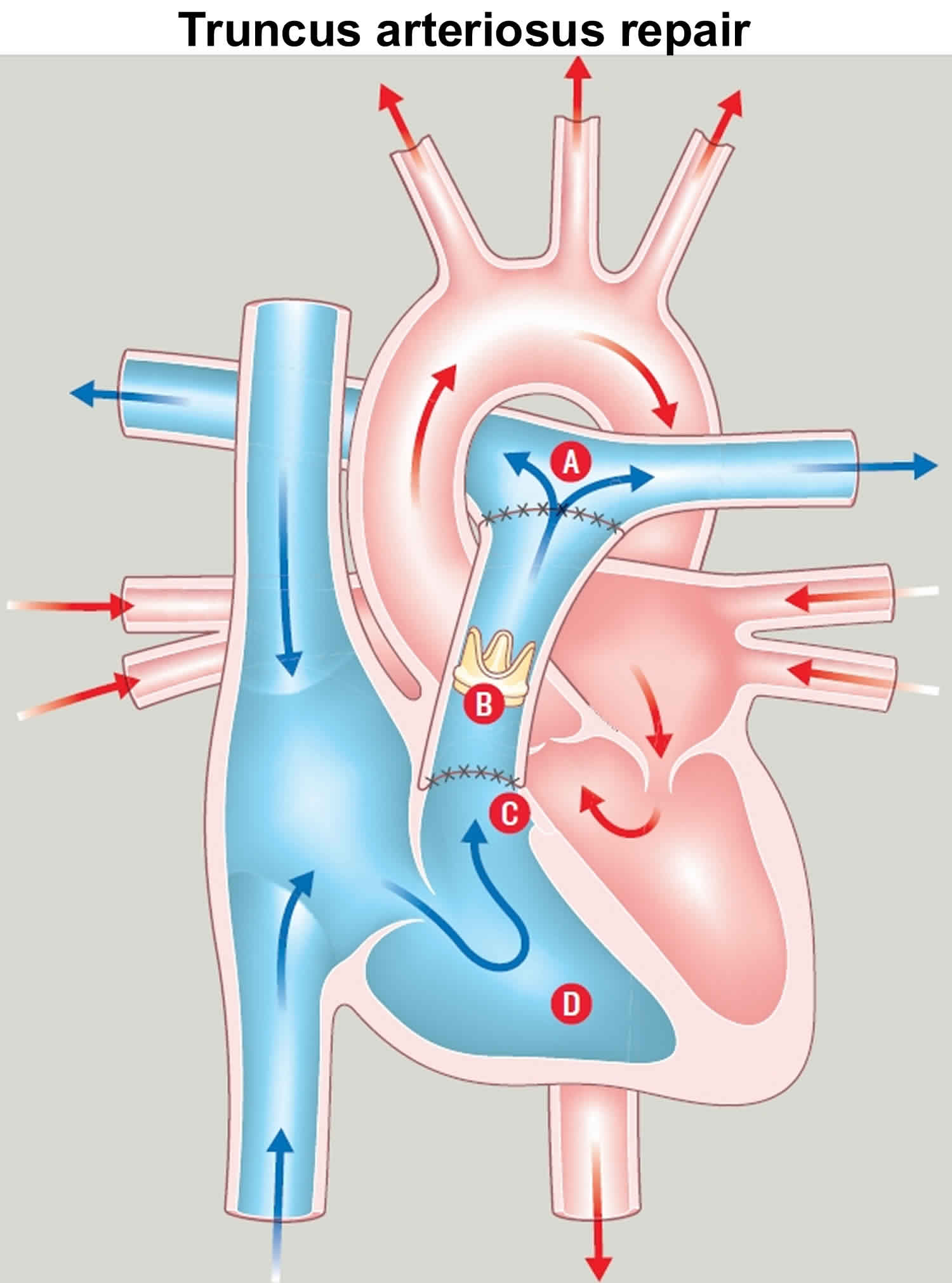
Footnote: (A) Pulmonary artery; (B) Tube connecting right ventricle to pulmonary artery; (C) Patch closing ventricular septal defect (VSD); (D) Right ventricle
Cardiac catheterization
Newer minimally invasive procedures use a cardiac catheter to avoid the need for traditional heart surgery as your child grows or previously placed artificial valves deteriorate. The catheter is inserted into a blood vessel in the leg that is then threaded slowly up to the heart to replace the conduit.
In addition, cardiac catheterization with an inflatable balloon tip can be used to open up an obstructed or narrowed artery, which may delay the need for follow-up surgery.
Coping and support
Caring for a baby with a serious heart problem, such as truncus arteriosus, can be challenging. Here are some strategies that may help make it easier:
- Seek support. Ask for help from family members and friends. Contact nonprofit organizations, such as the American Heart Association, Adult Congenital Heart Association or Mended Hearts for information about support groups in your area.
- Record your baby’s health history. Write down your baby’s diagnosis, medications, surgery and other procedures, the dates they were performed, your pediatric cardiologist’s name and phone number, and any other important information about your baby’s care. It’s also helpful to include a copy of the operative report from your child’s surgeon in your records. This information will help you recall the care your child has received, and it will be useful to doctors unfamiliar with your child who need to review his or her health history. It will also be helpful when your child moves from pediatric to adult health care.
- Talk about your concerns. You may worry about the risks of vigorous activity, even after your child has had corrective surgery. Talk with the cardiologist about which activities are safe for your child. If some activities are off-limits, encourage your child in other pursuits rather than focusing on what he or she can’t do. If other issues about your child’s health concern you, discuss them with your child’s primary care doctor or pediatric cardiologist.
Truncus arteriosus prognosis
Complete repair most often provides good results. Another procedure may be needed as the child grows, because the rebuilt pulmonary artery that uses tissue from another source will not grow with the child.
Untreated cases of truncus arteriosus result in death, often during the first year of life.
Truncus arteriosus in adults
In rare cases, a person with truncus arteriosus can survive infancy without surgical repair of the heart and live into adulthood. However, people with this condition will almost certainly develop heart failure and pulmonary hypertension (Eisenmenger syndrome).
This syndrome is caused by permanent lung damage from pulmonary hypertension that results in much of the blood flow bypassing the lungs entirely.
Pregnancy
Women who’ve had surgery to repair truncus arteriosus in infancy need to be evaluated by a cardiologist with expertise in adult congenital heart defects and an obstetrician specializing in high-risk pregnancies before attempting to become pregnant.
Depending on the level of lung damage that occurred before surgery, pregnancy may or may not be recommended. In addition, some drugs taken for heart problems can be harmful to an unborn baby.
Truncus arteriosus life expectancy
The natural history of truncus arteriosus without surgical intervention is not well characterized. In numerous earlier series, the median age at death without surgery ranged from 2 weeks to 3 months, with almost 100% mortality by age 1 year 6. Cases of patients surviving into adulthood with unrepaired truncus arteriosus are reported, but they are extremely uncommon. Cause of death in unrepaired patients is usually cardiac arrest or multiple organ failure in the face of systemic perfusion that is inadequate to meet the body’s metabolic demands; progressive metabolic acidosis and myocardial dysfunction results.
Currently, for patients undergoing complete repair in the neonatal or early infant periods, early postoperative mortality is generally less than 10% 6. This represents a substantial improvement from earlier eras; as recently as 20 years ago, the early mortality rate after complete repair was higher than 25% in most series.
Truncus arteriosus survival rate
Among patients surviving the initial postoperative period, the survival rate at a 10- to 20-year follow-up is higher than 80%, with most deaths resulting from sequelae of late repair (pulmonary vascular obstructive disease), reinterventions, or residual/recurrent physiologic abnormalities.
- Bhansali S, Phoon C. Truncus Arteriosus. [Updated 2018 Nov 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534774[↩][↩]
- Reller MD, Strickland MJ, Riehle-Colarusso T, Mahle WT, Correa A. Prevalence of congenital heart defects in metropolitan Atlanta, 1998-2005. J. Pediatr. 2008 Dec;153(6):807-13.[↩]
- Parker SE, Mai CT, Canfield MA, et al; for the National Birth Defects Prevention Network. Updated national birth prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol. 2010;88:1008-16.[↩]
- Chen Q, Gao H, Hua Z, Yang K, Yan J, Zhang H, Ma K, Zhang S, Qi L, Li S. Outcomes of Surgical Repair for Persistent Truncus Arteriosus from Neonates to Adults: A Single Center’s Experience. PLoS ONE. 2016;11(1):e0146800[↩]
- Gill HR, Splitt M, Sharland GK, Simpson JM. 2003. Patterns of recurrence of congenital heart disease: An analysis of 6,640 consecutive pregnancies evaluated by detailed fetal echocardiography. Journal of the American College of Cardiology; 42: 923-9.[↩]
- Truncus arteriosus. https://emedicine.medscape.com/article/892489-overview[↩][↩][↩][↩][↩]
- Collett RW, Edwards JE. Persistent truncus arteriosus: a classification according to anatomic types. Surg Clin North Am. 1949. 29:1245-70.[↩]
- Van Praagh R, Van Praagh S. The anatomy of common aorticopulmonary trunk (truncus arteriosus communis) and its embryologic implications. A study of 57 necropsy cases. Am J Cardiol. 1965 Sep. 16(3):406-25[↩]
- McElhinney DB, Driscoll DA, Emanuel BS, Goldmuntz E. Chromosome 22q11 deletion in patients with truncus arteriosus. Pediatr Cardiol. 2003 Nov-Dec;24(6):569-73[↩]
- Rao PS. Diagnosis and management of cyanotic congenital heart disease: part I. Indian J Pediatr. 2009 Jan. 76(1):57-70.[↩]





{kind=link}