
Contents
Valsalva maneuver
Valsalva maneuver, also known as Valsalva-Weber maneuver, is a forced expiratory effort against a closed airway (with mouth and nose closed) with the forced expiratory pressure during strain at 40 mmHg for 15 to 20 seconds 1, 2. To do Valsalva maneuver, you hold your breath and strain, as if you were trying to have a bowel movement. Performing the Valsalva maneuver causes an increase in intrathoracic (intrapleural) and intrabdominal pressures, leading to a reduction in preload to your heart. Cardiovascular changes occur during and after Valsalva maneuver due to baroreflex and other compensatory reflex mechanisms that are initiated by decreased preload.
The cardiovascular responses to the Valsalva maneuver are mediated by the autonomic nervous system and vary according to sympathetic and parasympathetic activation and/or inhibition, which makes Valsalva maneuver a useful tool to evaluate the function of the autonomic nervous system 3, 4, 1, 5. This dynamic pattern of cardiovascular autonomic activity is determined by different stimuli, such as breathing, muscle contraction, stimulation of arterial baroreceptors 6, postural changes 7 and ageing 8.
Similar changes occur whenever a person conducts a force expiration against either a closed glottis or high pulmonary outflow resistance, or when the thoracic and abdominal muscles are strongly contracted. This can occur when a person strains while having a bowel movement. Similar changes can also occur when a person lifts a heavy weight while holding their breath.
Valsalva maneuver phases
There are four phases of the Valsalva maneuver (Figure 1 and Table 1) 9:
- During phase 1, when you’re straining there is an increase in intrathoracic (intrapleural) and intrabdominal pressures that mechanically drives blood to the peripheral vasculatures causing a brief increase in your blood pressure (↑BP) and decrease your heart rate (↓HR) 10, 11
- Phase 2 is divided into early phase 2 (PIIE) and late phase 2 (PIIL).
- In early phase 2 (PIIE), there is a reduction of venous return and a subsequent decrease in stroke volume, causing your blood pressure (↓BP) and the amount of blood your heart pumps (lower cardiac output) to go down 12.
- In late phase 2, the decreased blood pressure activates the baroreflex that causes increased sympathetic activity in your heart rate, consequently, tachycardia and vasoconstriction are elicited. Your heart starts pumping out more blood and your blood pressure goes back to normal 11. This response corresponds to late phase 2 and is highly dependent on alpha-adrenergic activation 13. When you stop the Valsalva maneuver, blood refills the pulmonary vasculature.
- Phase 3 begins at the end of expiration and lasts 1–2 seconds. Phase 3 is due to an abrupt drop of intrathoracic pressure that increases venous return into the thorax. Thoracic blood vessels are expanded and this causes a sudden fall in blood pressure (↓BP) 12. Reflex tachycardia and vasoconstriction generated at phase 2 are maintained and potentiated 14.
- During phase 4, there is an increase in venous return that contributes to an increase in diastolic ventricular filling. This higher preload induces an increase in systolic volume and cardiac output, as explained by the Frank-Starling mechanism. As peripheral resistances are still high, due to sustained vasoconstriction, it results in an important increase in blood pressure (↑BP) called overshoot, which characterizes phase 4, which lasts for few seconds until there is complete recovery 15. Phase 4 is less dependent on vasoconstriction and relies mainly on beta-adrenergic stimulation 13. The blood pressure overshoot induces a strong baroreceptor activation which generates a marked vagal bradycardia (↓HR) and a vasodilation secondary to the decreased sympathetic flow. Blood pressure progressively decreases, although it remains elevated for a considerable time, partly due to the release of circulating catecholamines 12, 16.
Figure 1. Valsalva maneuver phases
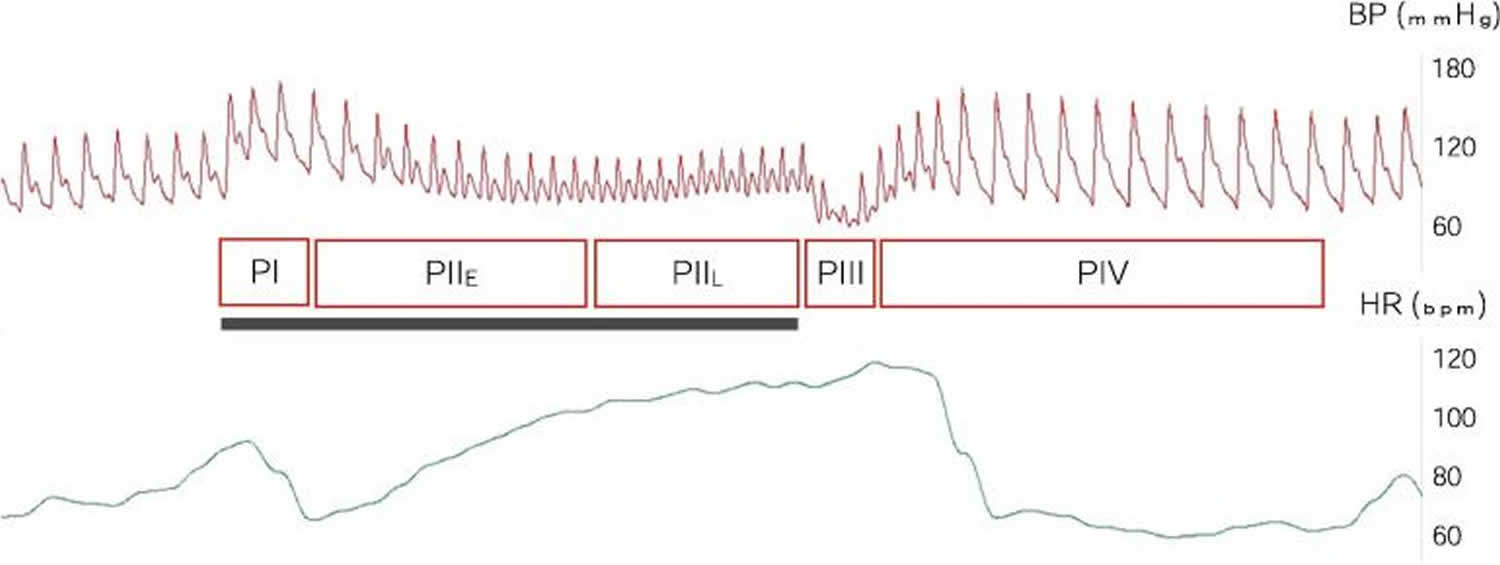
Footnote: Continuous arterial blood pressure (BP, superior panel) and heart rate (HR, inferior panel) recording during the Valsalva maneuver.
Abbreviations: PI = Phase 1; PIIE = early Phase 2; PIIL = late Phase 2; Phase III = Phase 3; Phase IV = Phase 4
[Source 17 ]Table 1. Valsalva maneuver phases
| Phase | Timing | Physiology | Heart rate | Blood pressure |
|---|---|---|---|---|
| 1 | Early valsalva | Increase in intrathoracic pressure | Decrease | Increase |
| 2 – Early | Decreased venous return | Decrease | Decrease | |
| 2 – Late | Baroreflex | Increase | Increase | |
| 3 | End of valsalva | Refills pulmonary vasculature | Increase | Decrease |
| 4 | Increase in venous return | Decrease | Increase | |
According to Smith et al. 18, the stroke volume decreases 40 ± 6% and the cardiac output 21 ± 3% during the Valsalva maneuver (the lowest values occurring at 15 seconds), which is followed by a progressive increase in stroke volume (47 ± 5%) at 10 seconds after end of the Valsalva maneuver. Moreover, Greenfield et al. 19 reported a decrease to 50% of the stroke volume at the end of phase 2 of the Valsalva maneuver. These results described above are in agreement with those reported in this study 20.
Regarding the Valsalva maneuver, the cardiovascular responses observed during phases 2 and 4 of the Valsalva maneuver 21 explain the heart rate responses. During phase 2, the changes in intrathoracic pressure stimulate the pulmonary stretch receptors, cardiopulmonary mechanoreceptors, arterial baroreceptors and chemoreceptors. These receptors are responsible for activation of the baroreflex pathway and result in mechanical effects on the pulmonary and cardiovascular systems, especially heart rate and peripheral vascular resistance. The former is attributable to cardiac parasympathetic withdrawal and the latter is a result of peripheral sympathetic activation 22. As intrathoracic pressure remains elevated, there is a decrease in cardiac output and blood pressure attributable to the reduction in venous return and a decrease in left ventricular filling. At this point, there is an increase in baroreceptor response that results in increased heart rate and peripheral vascular resistance in an attempt to return to baseline the values of blood pressure and cardiac output (late phase 2) 23. Regarding phase 4, the release of venous return results in an increase in blood pressure (overshoot), which stimulates the baroreceptors to inhibit the sympathetic afferent reflex and increase vagal tone, causing reflex bradycardia and arteriolar vasodilatation and a subsequent decrease in heart rate to values lower than those observed at rest 23.
Valsalva maneuver uses
Many clinical applications of Valsalva maneuver have been described in medical practice. The Valsalva maneuver can:
- Slow down your heart rate and stop supraventricular tachycardia (SVT), an abnormal heart rhythm. The Valsalva maneuver is a drug-free way to quickly return an abnormal fast heart rhythm called supraventricular tachycardia (SVT) to normal 24. Valsalva maneuver is also useful for the termination of paroxysmal supraventricular tachycardia (PSVT) with variable success. Increased vagal activity, leading to increased refractoriness of atrioventricular (AV) nodal tissue interrupting re-entry, has been proposed as the mechanism for the termination of paroxysmal supraventricular tachycardia (PSVT) 25. If the Valsalva maneuver fails, you’ll need cardioversion to get your heart back into a normal rhythm.
- Help your doctor decide which kind of heart murmur you have. Valsalva maneuver may be used to differentiate between different murmurs. Since Valsalva maneuver reduces preload and thus end-diastolic volume, it can help accentuate some murmurs while diminishing others. The murmur of aortic stenosis (AS) is reduced in intensity on the administration of Valsalva maneuver because reduced end-diastolic volume diminishes the blood available for ejection through the stenosed aortic orifice 26. Contrary to aortic stenosis, the murmur of hypertrophic obstructive cardiomyopathy (HOCM) accentuates in response to Valsalva maneuver because reduced end-diastolic volume during Valsalva maneuver leads to the worsening of the obstruction in hypertrophic obstructive cardiomyopathy (HOCM) 26, 1, 27.
- Tell your doctor if you have heart failure. Patients with heart failure show an abnormal blood pressure overshoot in response to the Valsalva maneuver due to impaired ventricular function 28.
- Help diagnose other problems, such as venous (vein) disease or a varicocele (a swollen vein in your scrotum).
- Help diagnose an issue with your autonomic nervous system (which controls your heartbeat, breathing and other functions without you thinking about it). By monitoring your heart rate during the Valsalva maneuver, the Valsalva ratio can be measured. Valsalva ratio is defined as the maximum heart rate during the Valsalva maneuver divided by the lowest heart rate obtained within 30 seconds of the peak heart rate 1. Valsalva maneuver can assist the neurologist to identify patients suffering from autonomic neuropathy. Dysautonomia usually manifests as an absence of blood pressure overshoot and reflex bradycardia after Valsalva maneuver 29. Valsalva ratio varies with age, but a ratio less than 1.1 is abnormal at any age 26, 1, 27. Also, beat-to-beat blood pressure and heart rate can be used to evaluate the integrity of the baroreflex arc by computation of baroreflex sensitivity.
- Get something out of your middle ear that shouldn’t be there.
- To detect bleeding points towards the end of thyroid surgery.
- To confirm hemostasis and absence of cerebrospinal fluid (CSF) leak after neurosurgical procedures.
- To assist in the radiological diagnosis of liver hemangiomas, venous disease, and foramen ovale 28, 30, 25.
- To reduce venipuncture pain in pregnant women 31.
Who should avoid the Valsalva maneuver?
Because the Valsalva maneuver increases pressure in your eyes and abdomen, you shouldn’t do Valsalva maneuver if you have retinopathy (a problem with blood vessels in the retina of your eye) and intraocular lens implants in your eyes, such as after cataract surgery.
You need to be careful with the Valsalva maneuver if you have:
- Heart valve disease.
- Coronary artery disease.
- Congenital (since birth) heart disease.
How to perform the Valsalva maneuver
- Sit down or lie on your back.
- Take a breath.
- Push that breath out against your closed mouth and nose while straining as if you’re trying to poop. Hold for 15 to 20 seconds.
- Open your nose or mouth and breathe out.
Two versions of the Valsalva maneuver can help with supraventricular tachycardia (SVT):
- Modified Valsalva maneuver, your doctor raises your legs right after you stop straining 24. Modified Valsalva maneuver may work better than the standard Valsalva maneuver. The REVERT trial found the standard method worked for 16% of people, while the modified version worked for 46% of people 24. It may work better because having your legs up helps more blood come back to your heart.
- Reverse Valsalva maneuver, you sit and inhale against resistance for ten seconds while keeping the nose pinched and having your mouth closed tightly. This leads to increased vagal tone and decreased sympathetic activity, which in turn leads to bradycardia and arterial hypotension (the Bezold–Jarich reflex), causing supraventricular tachycardia (SVT) to resolve in the next 15 seconds if effective 32.
What happens after the Valsalva maneuver?
If the Valsalva maneuver is successful, which happens 5% to 20% of the time, your fast heart rate will slow down in about one minute. If it doesn’t stop your supraventricular tachycardia (SVT) after three tries, your healthcare provider will proceed with the next steps in treatment. These steps may include carotid massage, medications or electric cardioversion depending on your symptoms, vital signs and the type of supraventricular tachycardia.
What are the advantages of the Valsalva maneuver?
The Valsalva maneuver is a fast, drug-free way to stop a supraventricular tachycardia (SVT). If it works, you can avoid medications or cardioversion.
What are the risks or complications of the Valsalva maneuver?
Most people can do the Valsalva maneuver safely and not have complications 33.
Side effects are extremely rare but some people experience 3:
- Dizziness,
- Headache,
- Nausea,
- Blurred vision,
- Chest pain,
- Fainting (syncope),
- Hypotension
- Severe hypertension,
- Abnormal heart rhythms (arrhythmias)
- Stroke.
These secondary effects are limited to high risk population, that is, patients with coronary or cerebrovascular disease 2, 34.
- Novak P. Quantitative autonomic testing. J Vis Exp. 2011 Jul 19;(53):2502. doi: 10.3791/2502[↩][↩][↩][↩][↩]
- Junqueira L.F., Jr. Teaching cardiac autonomic function dynamics employing the Valsalva (Valsalva-Weber) maneuver. Adv Physiol Educ. 2008;32(1):100–106. doi: 10.1152/advan.00057.2007[↩][↩]
- Pstras L., Thomaseth K., Waniewski J., Balzani I., Bellavere F. The Valsalva manoeuvre: physiology and clinical examples. Acta Physiol (Oxf) 2016;217(2):103–119. doi: 10.1111/apha.12639[↩][↩]
- Low PA, Tomalia VA & Park KJ (2013). Autonomic function tests: some clinical applications. J Clin Neurol 9, 1–8.[↩]
- Cooke W.H., Reynolds B.V., Yandl M.G., Carter J.R., Tahvanainen K.U., Kuusela T.A. Effects of exercise training on cardiovagal and sympathetic responses to Valsalva’s maneuver. Med Sci Sports Exerc. 2002;34(6):928–935. doi: 10.1097/00005768-200206000-00004[↩]
- Wada N, Singer W, Gehrking TL, Sletten DM, Schmelzer JD, Kihara M & Low PA (2014). Determination of vagal baroreflex sensitivity in normal subjects. Muscle Nerve 50, 535–540.[↩]
- Minatel V, Karsten M, Neves LM, Beltrame T, Borghi‐Silva A & Catai AM (2012). Heart rate assessment during maximal static expiratory pressure and Valsalva maneuver in healthy young men. Rev Bras Fisioter 16, 406–413.[↩]
- Catai A, Takahashi A, Perseguini N, Milan J, Minatel V, Rehder‐Santos P, Marchi A, Bari V & Porta A (2014). Effect of the postural challenge on the dependence of the cardiovascular control complexity on age. Entropy 16, 6686–6704.[↩]
- Valsalva ratio: a measure of stress in first year medical students. International Journal of Research in Medical Sciences. Loni SA. Int J Res Med Sci. 2015 Jul;3(7):1599-1604. https://www.msjonline.org/index.php/ijrms/article/download/1561/1483[↩]
- Eckberg D.L. Parasympathetic cardiovascular control in human disease: a critical review of methods and results. Am J Physiol. 1980;239(5):H581–H593. doi: 10.1152/ajpheart.1980.239.5.H581[↩]
- Hilz M.J., Dutsch M. Quantitative studies of autonomic function. Muscle Nerve. 2006;33(1):6–20. doi: 10.1002/mus.20365[↩][↩]
- Looga R. The Valsalva manoeuvre–cardiovascular effects and performance technique: a critical review. Respir Physiol Neurobiol. 2005;147(1):39–49. doi: 10.1016/j.resp.2005.01.003[↩][↩][↩]
- Sandroni P., Benarroch E.E., Low P.A. Pharmacological dissection of components of the Valsalva maneuver in adrenergic failure. J Appl Physiol. 1991;71(4):1563–1567. doi: 10.1152/jappl.1991.71.4.1563[↩][↩]
- Hamilton W.F., Woodbury R.A., Harper H.T., Jr. Physiologic relationships between intrathoracic, intraspinal and arterial pressures. JAMA. 1936;107(11):853–856. doi: 10.1001/jama.1936.02770370017005[↩]
- Sarnoff S.J., Hardenbergh E., Whittenberger J.L. Mechanism of the arterial pressure response to the Valsalva test; the basis for its use as an indicator of the intactness of the sympathetic outflow. Am J Physiol. 1948;154(2):316–327. doi: 10.1152/ajplegacy.1948.154.2.316[↩]
- Sandroni P., Novak V., Opfer-Gehrking T.L., Huck C.A., Low P.A. Mechanisms of blood pressure alterations in response to the Valsalva maneuver in postural tachycardia syndrome. Clin Auton Res. 2000;10(1):1–5. doi: 10.1007/BF02291382[↩]
- Saldaña García J, Torremocha López A, Dawid Milner MS. Influence of repetitions on the Valsalva maneuver. Clin Neurophysiol Pract. 2020 May 15;5:104-111. doi: 10.1016/j.cnp.2020.04.003[↩]
- Smith SA, Salih MM & Littler WA (1987). Assessment of beat to beat changes in cardiac output during the Valsalva maneuver using electrical bioimpedance cardiography. Clin Sci (Lond) 72, 423–428.[↩]
- Greenfield JC Jr, Cox RL, Hernandez RR, Thomas C & Schoonmaker FW (1967). Pressure‐flow studies in man during the Valsalva maneuver with observations on the mechanical properties of the ascending aorta. Circulation 35, 653–661.[↩]
- Minatel, V. , Takahashi, A. C., Perseguini, N. M., Milan, J. C., Castello‐Simões, V. , Gomes, E. C., Borghi‐Silva, A. and Catai, A. M. (2016), Maximal expiratory pressure and Valsalva manoeuvre do not produce similar cardiovascular responses in healthy men. Exp Physiol, 101: 599-611. doi:10.1113/EP085203 [↩]
- Looga R (2005). The Valsalva manoeuvre—cardiovascular effects and performance technique: a critical review. Respir Physiol Neurobiol 147, 39–49.[↩]
- Schrezenmaier C, Singer W, Swift NM, Sletten D, Tanabe J & Low PA (2007). Adrenergic and vagal baroreflex sensitivity in autonomic failure. Arch Neurol 64, 381–386.[↩]
- Liang F & Liu H (2006). Simulation of hemodynamic responses to the Valsalva maneuver: an integrative computational model of the cardiovascular system and the autonomic nervous system. J Physiol Sci 56, 45–65.[↩][↩]
- Appelboam A, Reuben A, Mann C, Gagg J, Ewings P, Barton A, Lobban T, Dayer M, Vickery J, Benger J; REVERT trial collaborators. Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial. Lancet. 2015 Oct 31;386(10005):1747-53. doi: 10.1016/S0140-6736(15)61485-4[↩][↩][↩]
- Rodrigues AC, Picard MH, Carbone A, Arruda AL, Flores T, Klohn J, Furtado M, Lira-Filho EB, Cerri GG, Andrade JL. Importance of adequately performed Valsalva maneuver to detect patent foramen ovale during transesophageal echocardiography. J Am Soc Echocardiogr. 2013 Nov;26(11):1337-43. doi: 10.1016/j.echo.2013.07.016[↩][↩]
- Ewing DJ, Martyn CN, Young RJ, Clarke BF. The value of cardiovascular autonomic function tests: 10 years experience in diabetes. Diabetes Care. 1985 Sep-Oct;8(5):491-8. doi: 10.2337/diacare.8.5.491[↩][↩][↩]
- Ravits, J.M. (1997), Aaem minimonograph #48: Autonomic nervous system testing. Muscle Nerve, 20: 919-937. https://doi.org/10.1002/(SICI)1097-4598(199708)20:8<919::AID-MUS1>3.0.CO;2-9[↩][↩]
- Ricci S, Moro L, Minotti GC, Incalzi RA, De Maeseneer M. Valsalva maneuver in phlebologic practice. Phlebology. 2018 Mar;33(2):75-83. doi: 10.1177/0268355516678513[↩][↩]
- Low PA. Testing the autonomic nervous system. Semin Neurol. 2003 Dec;23(4):407-21. doi: 10.1055/s-2004-817725[↩]
- Won, H.J., Kim, P.N. and Lee, J.S. (2017), Changes in echogenicity of hepatic hemangiomas during the valsalva maneuver. J. Clin. Ultrasound, 45: 328-331. https://doi.org/10.1002/jcu.22456[↩]
- Höbek Akarsu R, Kuş B, Doğukan Akarsu G. Effects of Valsalva Maneuver, EMLA Cream, and Stress Ball for Pregnant Women’s Venipuncture Pain. Altern Ther Health Med. 2021 Sep;27(5):108-114.[↩]
- Gaudart P, Cazes N, Simon K, Larger D, Deharo JC. The reverse vagal manoeuvre: A new tool for treatment of supraventricular tachycardia? Am J Emerg Med. 2021 Mar;41:66-69. doi: 10.1016/j.ajem.2020.12.061[↩]
- Srivastav S, Jamil RT, Zeltser R. Valsalva Maneuver. [Updated 2022 Oct 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537248[↩]
- Levin A.B. A simple test of cardiac function based upon the heart rate changes induced by the Valsalva maneuver. Am J Cardiol. 1966;18(1):90–99. doi: 10.1016/0002-9149(66)90200-1[↩]





{kind=link}