
Contents
What is water therapy
Water therapy is also called hydrotherapy, aquatic therapy, pool therapy or balneotherapy, is the external or internal use of water in any of its forms (water, ice, steam) for health promotion or treatment of various diseases with various temperatures, pressure, duration, and site 1. Water therapy is one of the naturopathic treatment modality used widely in ancient cultures including India, Egypt, China, etc. 2. Use of water in various forms and in various temperatures can produce different effects on different system of the body. Though many countries used water to produce different physiological/therapeutic effects on different part of the system for maintaining health, preventing, and treating the diseases, the scientific evidence-based effects are not well documented.
Water therapy in general
Superficial cold application may cause physiologic reactions such as decrease in local metabolic function, local edema, nerve conduction velocity, muscle spasm, and increase in local anesthetic effects 3. One hour head-out water immersions in various temperatures (57.2 °F [14°C], 68 °F [20°C] and 89.6 °F [32°C]) produced various effects.
Immersion at 89.6 °F [32°C] did not change metabolic rate and rectal temperature, but it lowered the heart rate (HR) by 15%, systolic blood pressure (SBP) and diastolic blood pressure (DBP) by 11% and 12%, respectively, compared, with controls at ambient air temperature 1. Along with heart rate and blood pressure (BP), the plasma renin activity, plasma cortisol, and aldosterone concentrations were also lowered by 46%, 34%, and 17%, respectively, while diuresis was increased by 107% 4.
Head-out water immersions at 68 °F [20°C] produced similar decrease in plasma renin activity, heart rate, systolic blood pressure, and diastolic blood pressure, in spite of lowered rectal temperature and increased metabolic rate by 93% 1. Plasma cortisol concentrations tended to decrease, while plasma aldosterone concentration was unchanged. Diuresis was increased by 89%. No significant differences in changes in plasma renin activity, aldosterone concentration, and diuresis compared with subjects immersed in 89.6 °F [32°C] 4.
Head-out water immersions at 57.2 °F [14°C] lowered rectal temperature and increased metabolic rate by 350%, heart rate, systolic blood pressure, and diastolic blood pressure by 5%, 7%, and 8%, respectively 1. Plasma noradrenaline and dopamine concentrations were increased by 530% and by 250%, respectively, while diuresis increased by 163%, which was more than at 89.6 °F [32°C]. Plasma aldosterone concentrations increased by 23%. Plasma renin activity was reduced. Cortisol concentrations tended to decrease. Plasma adrenaline concentrations remained unchanged. Changes in plasma renin activity were not related to changes in aldosterone concentrations 4.
Head-out water immersions therapy in different temperatures did not increase blood concentrations of cortisol 1. There was no correlation between changes in rectal temperature and changes in hormone production. The physiological changes induced by head-out water immersions are mediated by humoral control mechanisms, while responses induced by cold are mainly due to increased activity of the sympathetic nervous system 4.
Regular winter swimming significantly decreased tension, fatigue, memory, and mood negative state points with the duration of swimming period; significantly increased vigor-activity scores; relieved pain who suffered from rheumatism, fibromyalgia, or asthma; and improved general well-being in swimmers 5.
Water therapy benefits
The benefits of water therapy include enhanced aerobic capacity, improved muscle strength and endurance, increased joint range of motion (anti-spasticity), as well as decreased muscle fatigue and joint pain, enhanced cardiorespiratory functioning and a reduced cardiometabolic risk profile 6. Hot spring hydro-pressure therapy plays a crucial role in the recovery of burn patients 7 by contributing to the superficial improvement of the affected skin as well as by fostering a general sense of personal well-being. By targeting both the restoration of the skin’s physical properties and the strengthening of the patient’s psyche, their body’s ability to heal is increased. In France, hot spring water and hydro-pressure therapy are accepted as an important part of burn therapy with 2 annual sessions eligible for reimbursement through social insurance. Water physical therapy aids in reducing patients with spinal cord injury muscle spasticity and cardiometabolic risk profiles, while favourably enhancing underwater gait kinematics and cardiorespiratory capacity 8. However, more randomised control trials should be undertaken to increase the present body of knowledge.
Cardiovascular system
Cold exposure to small surface area produced compensatory vasodilatation in deeper vascular system resulting increased blood flow to the tissues underlying the site of exposure. This vascular reaction occurs mainly to maintain constant deep tissue temperature 9.
In patient with chronic heart failure, thermal vasodilatation following warm-water bathing and low-temperature sauna bathing at 140 °F (60°C) for 15 min improves cardiac function 10; repeated sauna-therapy (sauna-therapy) increased left ventricular ejection fraction; increased 6-min walk distance in association with improvement in flow-mediated dilation and increase in number of circulating CD34 (+) cells; reduced plasma levels of norepinephrine and brain natriuretic peptide. These indicates that sauna-therapy improves exercise tolerance in association with improvement in endothelial function 11. Low-temperature sauna bathing improves peripheral circulation in cerebral palsy (CP) 10.
After sauna-therapy reduced level of total and low density lipoprotein (LDL) “bad: cholesterol concentration, while increased level of high density lipoprotein (HDL) “good” cholesterol was observed. These changes are good prognoses for the prevention of ischemic heart disease 12. Sauna-therapy increases endothelial nitric oxide synthase (eNOS) activity and improves cardiac function in heart failure and improve peripheral blood flow in ischemic limbs. In myocardial infarction (heart attack)-induced Wistar rats sauna-therapy increases myocardial endothelial nitric oxide synthase (eNOS), vascular endothelial growth factor mRNA levels. It attenuates cardiac remodeling after heart attack through improving coronary vascularity in the noninfarcted myocardium and thus sauna-therapy might serve as a novel noninvasive therapy for patients with heart attack 13. Acute heart attack was thought to result from thrombosis or plaque rupture because of coronary artery spasm. The vasospasm might be induced by stimulation of the alpha-adrenergic receptors during alternating heat exposure during sauna bath followed by rapid cooling during cold water bath. This effect showed the dangers of rapid cooling after sauna bathing in patients with coronary risk factors 14. Regular sauna-therapy (either radiant heat or far-infrared units) appears to be safe and produce multiple health benefits but use of sauna-therapy in early pregnancy is a potential concern because evidence suggesting that hyperthermia might be teratogenic 15.
Cold water immersion (head-out cold water immersions) induces significant physiological and biochemical changes in the body such as increase in heart rate, BP, metabolism, and peripheral catecholamine concentration; and decrease in cerebral blood flow 16.
Reduction in heart rate, and increases in systolic and diastolic biventricular functions, were observed during acute warm-head-out water immersions 17. In contrast, increase in heart rate and a decrease in systolic blood pressure and diastolic blood pressure were observed in 30 min of head-out head-out water immersions (38.41 ± 0.04°C) 18.
Hyperthermic immersion produced shortening of activated partial thromboplastin time. During hyperthermic immersion, plasminogen activator inhibitor activity was decreased; thrombocyte count was increased; increases in tissue-type plasminogen activator concentration and leukocytes count were attributed to hemoconcentration. Immediately after hyperthermic immersion, fibrinogen concentration decreased but increased during recovery. During thermo-neutral immersion prothrombin time, plasminogen activator inhibitor activity and granulocyte count ecreased. Warm water bathing leads to hemoconcentration and minimal activation of coagulation; decrease in plasminogen activator inhibitor-1 activity. During warm water bathing, marked risk for thrombotic or bleeding complications in healthy males could not be ascertained 19. During contrast baths, longer duration in the second heating phase was required to produce sufficient fluctuation in blood flow 20.
Head-out water immersions up-to shoulder levels at different temperatures (77 °F [25°C], 93.2 °F [34°C], and 104 °F [40°C]) showed no significant effect on cardiac output in 77 °F [25°C] compared with 93.2 °F [34°C], but in 104 °F [40°C] a considerable increase in cardiac output was observed 21.
Carbon dioxide (CO2) enriched head-out water immersions reduced free radical plasma levels, raised antioxidants levels, and induce peripheral vasodilatation suggests improvement in microcirculation 22. Decrease in tympanic temperature; increase in cutaneous blood flow at immersed site was significantly greater in CO2-head-out water immersions compared with fresh head-out water immersions 23. The three main effects of CO2 enriched head-out water immersions are decline in core temperature, increase in cutaneous blood flow, and elevation of score on thermal sensation, which were analyzed 24.
Respiratory system
head-out water immersions up-to shoulder levels at different temperatures (77 °F [25°C], 93.2 °F [34°C], and 104 °F [40°C]) showed increased metabolic rate, oxygen (O2) consumption (VO2) only at 77 °F [25°C]. Two main factors affecting O2 transport during immersion are temperature and hydrostatic pressure. O2 transport was improved above neutral temperature, because of increase in cardiac output resulting from the combined actions of hydrostatic counter pressure and body heating. Below neutral temperature, O2 transport is altered. At any of the temperatures tested, the pulmonary tissue volume and arterial blood gases were not significantly affected 25.
Significant decrease in vital capacity (VC) with bath temperature was observed (i.e., vital capacity at 40°C >34°C >25°C). Significant increase in tidal volume (VT) in cold or hot water compared with thermo neutral water (i.e., tidal volume 40°C >34°C< 25°C). Alterations in respiratory muscles functioning might produce variations of the pulmonary volumes as a function of water temperature 26.
Cold water immersions was associated with increase in respiratory minute volume and decrease in end tidal CO2 partial pressure 16. Repeated cold water stimulations reduced frequency of infections; increased peak expiratory flow, lymphocyte counts, and expression of gamma-interferon; modulated interleukin expression; and improved quality of life (quality of life) in patients with chronic obstructive pulmonary disease 27.
In children suffering from recurrent and asthmatic bronchitis in remission, a single total air bath, or douche and local (cooling of the feet with water) exposure to mild cold did not raise noticeable disorders of the respiratory function. Local cold procedures improve bronchial patency but heat exposure resulted in its worsening 28.
Inhaling hot air while in a sauna produced no significant impact on overall symptom severity of common cold 29. A male track and field athlete, a case of breathing difficulties at rest and during exercise, was exacerbated in the supine position and during head-out water immersions 30.
Nervous system
Three cold modalities such as ice massage, ice pack, and cold water immersions applied to right calf region for 15 minutes reduced skin temperature (mean 64.76 °F [18.2°C]); reduced amplitude and increased latency and duration of compound action potential. It also reduced sensory nerve conduction velocity by 20.4, 16.7, and 22.6 m/s and motor nerve conduction velocity by 2.5, 2.1, and 8.3 m/s, respectively. Even though all three modalities effectively reduced skin temperature and sensory conduction at a physiological level, cold water immersions is the most indicated, effective modality for inducing therapeutic effects associated with the reduction of motor nerve conduction 31.
Temperature and pressure of water in aquatic or hydrotherapy can block nociceptors by acting on thermal receptors and mechanoreceptors and exert positive effect on spinal segmental mechanisms, which is useful for painful condition 32. Forty sessions of Ai Chi aquatic exercise program improves pain, spasms, disability, fatigue, depression, and autonomy in patient with multiple sclerosis 33.
In a study on physiotherapy on land or water in patient with Parkinson’s disease (Parkinson’s disease), functional reach test was improved in both therapies, but Berg Balance Scale (BBS) and Unified Parkinson’s Disease Rating Scale were improved only in aquatic therapy group. It indicates improvement in postural stability in Parkinson’s disease was significantly larger after aquatic therapy 34.
Sauna bath on paraplegic (P) group and tetraplegic (T) group, heart rate increased significantly during sauna but decreased significantly during postsauna phase in paraplegic group. diastolic blood pressure significantly reduced in tetraplegic group during postsauna phase but no significant changes in systolic blood pressure in both the groups.
In a study on cerebral palsy, low-temperature sauna bathing produced increase in heart rate and cardiac output; decrease in BP and total peripheral resistance; significant improvement in skin blood flow, blood flow velocity, pulsatile index, and resistive index; decrease in numbness and chronic myalgia of the extremities with no adverse effects 10.
Ten minutes of immersions in whirlpools produced increases in pulse and finger temperature with increased feelings of well-being and decreased state anxiety 35. CO2-head-out water immersions activates parasympathetic nerve activity in humans 23.
Adapted cold shower might have antipsychotic effect similar to that of electroconvulsive therapy because it could work as mild electroshock applied to sensory cortex. Additionally, cold shower is example of stress-induced analgesia and would also be expected to “crowd out” or suppress psychosis-related neurotransmission within mesolimbic system 36.
Cold exposure can activate components of reticular activating system such as locus ceruleus and raphe nuclei, which can result in activation of behavior and increased capacity of central nervous system (CNS) to recruit motoneurons 37. Cold exposure activates sympathetic nervous system; increase blood level of beta-endorphin and noradrenaline; and increase synaptic release of noradrenaline in brain. Antidepressive effect of cold shower attributed to presence of high density of cold receptors in skin expected to send an overwhelming amount of electrical impulses from peripheral nerve endings to the brain. It has significant analgesic effect and it does not cause dependence or noticeable side effects 38. Most narcotics administered rectally can cause intoxication. There is a significant co-morbidity of schizophrenia with intestinal illnesses and thus colon cleansing can significantly improve mental state 37.
Water therapy for arthritis
Walking in water at umbilical level increases the activity of erector spinae and activates rectus femoris to levels near to or higher than walking on dry ground 39. Osteoarthritis is one of the most prevalent musculoskeletal diseases in the world 40 Approximately 10% of the population aged 65 years and over present with osteoarthritis symptoms and more than half of the population have subclinical radiographic osteoarthritis 41. Exercise can be offered as water-based (hydrotherapy) or land-based exercises for hip and knee osteoarthritis 42. Water therapy is often recommended as a treatment option in the elderly population mostly because it is performed in a safer environment with a lower risk of falls than land-based exercises 43. Furthermore, patients with osteoarthritis show higher levels of treatment adherence with water physical therapy than other forms of conservative management 44. It is argued that water physical therapy offers additional physiological and biomechanical benefits compared to land-based exercises for patients with knee osteoarthritis and these could lead to better clinical outcomes. It is hypothesized that water physical therapy speeds patients’ early dynamic muscular strengthening and active mobilization even in the presence of severe pain 45. Furthermore, aquatic buoyancy potentially reduces weight-bearing stresses on joints, bones, and muscles. Hydrotherapy also allows the performance of closed-chain exercises, which are potentially painful with greater weight bearing 46. The results of this study 47 demonstrated that a structured six-week hydrotherapy program in conjunction with an educational program led to greater improvements in pain and function in the short term when compared to an educational program alone in women suffering from knee osteoarthritis. Furthermore, women with knee osteoarthritis who received hydrotherapy showed greater improvements in knee muscle performance such as knee flexor and extensor strength, knee flexor power, and knee extensor resistance. Water therapy exercises are usually advocated in the treatment of knee osteoarthritis because of the water properties, particularly those associated with buoyancy, which potentially reduces joint loading 48. Water pressure and temperature could also lead to an increased sensory input and further help in joint pain relief.
Musculoskeletal system
High performance athletes employ a variety of strategies with the intention of accelerating their recovery 49. Non-elite levels of athlete have also been shown to undertake a number of different recovery strategies post-exercise 50, potentially to decrease soreness and improve subsequent performance. The efficacy of numerous recovery strategies has been explored in scientific studies and also in practical sport applications, with some strategies being used without compelling supportive evidence 51.
Water immersion recovery strategies such as cold water immersion and contrast water therapy are used by athletes across a range of competition levels 50 to enhance post-exercise recovery 52. Cold water immersion reportedly minimises muscle oedema and provides analgesic effects post-exercise 53. Contrast water therapy is the alternation between hot and cold water 54 and is reported to decrease lactate accumulation 55, inflammation, edema, pain and muscle stiffness 54. The common explanation for contrast water therapy effectiveness is the pumping action of circulating blood, which is caused by alternation between vasodilation and vasoconstriction in response to hot and cold water 54.
Cold water immersions <59°F (<15°C) is one of the most popular intervention used after exercise 56, which significantly lowered ratings of fatigue and potentially improved ratings of physical recovery immediately after immersion with reduction in delayed onset muscle soreness at 24, 48, 72, and 96 hour follow-ups after exercise compared with passive interventions involving rest or no intervention 56.
Rate of decrease in plasma lactate concentration over 30 min recovery period after intense anaerobic exercise was significantly higher in contrast-head-out water immersions [hot 96.8 °F (36°C) and cold 53.6 °F (12°C)] compared with passive recovery on bed for both genders 57.
Leg immersion in warm water 111.2 ± 1°F (44 ± 1°C) for 45 min before stretch-shortening exercise reduced most of the indirect markers of exercise-induced muscle damage, including muscle soreness, creatine kinase activity in the blood, maximal voluntary contraction force, and jump height. Decreasing muscle damage did not improve voluntary performance, therefore clinical application of muscle prewarming may be limited 58.
Contrast water therapy (contrast water therapy) [alternating 1-min hot 100.4 °F (38°C) and 1-min cold 59 °F (15°C)] for 6/12/18 min lowered subjective measures of thermal sensation and muscle soreness compared with control (seated rest) but no consistent differences were observed in whole body fatigue. It indicates contrast water therapy for 6 min assisted acute recovery from high-intensity running and contrast water therapy duration did not have dose-response effect on running performance recovery 59. Contrast baths have been suggested for reducing pain; hand volume; and stiffness in affected extremities but it had no significant effect on pre- and/or postoperative hand volume in carpal tunnel syndrome 60.
Cold water or cold/thermoneutral water did not induce modifications of inflammatory and hematological markers. The performances of athletes were not negatively influenced by cold water immersions or contrast water therapy. Reduced perception of fatigue after training session was the principal effect of cold water immersions 61 because cold exposure increases opioid tone and high metabolic rate, which could diminish fatigue by reducing muscle pain and accelerating recovery of fatigued muscle, respectively 37, which can improve training and competitions in young soccer players 62.
A systematic review on management of fibromyalgia syndrome through hydrotherapy described as “there is strong evidence for the use of hydrotherapy in the management of fibromyalgia syndrome” and it showed positive outcomes for pain; tender point count; and health-status 63. Combination of sauna-therapy (once daily for 3 days/week) and underwater exercise (once daily for 2 days/week) for 12 weeks significantly reduced pain and symptoms (both short- and long-term); and improved quality of life in patients with fibromyalgia syndrome 64. Pool-based exercise using deep water running three times/week for 8 weeks is safe and effective intervention for fibromyalgia syndrome because it showed significant improvement in general health and quality of life compared with control; and significant improvement in fibromyalgia impact questionnaire score, incorporating pain; fatigue; physical function; stiffness; and psychological variables 65.
Hydrotherapy may have some short-term benefit to passive range of movement in rehabilitation after rotator cuff repair 66. Spa water 98.6 °F (37°C) and tap water heated to 98.6 °F (37°C) for the duration of 20 min/day for 5 days/week for the period of 2 weeks with home-based exercise program improved the clinical symptoms and quality of life in patient with osteoarthritis of knee. However, pain and tenderness statistically improved in spa water 61. It may be due to that spa waters are not only naturally warm, but their mineral content is also significant. Spa water has mechanical, thermal, and chemical effects.
In ankylosing spondilitis patients, balneotherapy statistically improved pain; physical activity; tiredness and sleep score; Bath Ankylosing Spondilitis Disease Activity Index (BASDAI); Nottingham Health Profile (NHP); patient’s global evaluation and physician’s global evaluation at 3 weeks, but only on modified Shober test and patient’s global evaluation parameters at 24 weeks. It indicates the effect of balneotherapy in improving disease activity and functional parameters in ankylosing spondilitis patients 67. Infrared sauna, a form of total-body hyperthermia was well tolerated; no adverse effects; and no exacerbation of disease were reported in patients with rheumatoid arthritis (RA) and ankylosing spondilitis in whom pain, stiffness, and fatigue showed clinical improvements during the 4 weeks treatment period but these did not reach statistical significance 68.
Aqua-jogging without caloric restrictions in obese persons for 6 weeks was associated with reductions in waist circumference and body fat; improvement of aerobic fitness and quality of life 69.
Water therapy exercises may be an excellent alternative to land exercise for individuals who lack confidence, have high risk of falling, or have joint pain 70. Water buoyancy reduces the weight that joints, bones, and muscles have to bear 71. Warmth and pressure of water also reduce swelling and reduces load on painful joints, remotes muscle relaxation 72. Water therapy exercises has significant effects on pain relief and related outcome measurements for locomotor diseases. Patients may become more active and improve their quality of life as a result of water therapy exercises 73. Water-based and land-based exercises reduced pain and improved function in patients with knee osteoarthritis and that water-based exercise was superior to land-based exercise for relieving pain before and after walking 74. Hydrotherapy is highly valued by rheumatoid arthritis patients who were treated with hydrotherapy (30-min session/week) reported feeling much better/very much better than those treated with land exercises (similar exercises on land) immediately on completion of the treatment program (6 weeks). But this benefit was not reflected on 10 m walk times, functional scores, quality of life measures, and pain scores by differences between groups 72. Hot compress with surrounding electro-acupuncture needling was significantly effective on rear thigh muscles strain and it was superior to conventional needling method and cupping in improving symptoms and physical signs as well as recovery of walking function of athletes 75.
Benefits of water exercise
Keeps joints moving
Pain in your joints may make you want to hold them very still as moving can be painful. However, immobilizing your joints or not using them will over time cause the joints, ligaments and muscles to lose range of motion and weaken. Muscles may also shorten and tighten up, causing you to feel more pain and stiffness and be less able to do the things you want to do.
Regular exercise helps keep joints moving, restores and preserves flexibility and strength, and protects joints against further damage. Exercise can also improve a person’s coordination, endurance and ability to perform daily tasks and can lead to an enhanced sense of self-esteem and accomplishment.
Exercising in water is a gentle way to exercise joints and muscles. The buoyancy of the water supports and lessens stress on the joints and encourages freer movement. Water may also act as resistance to help build muscle strength. Consult your doctor to determine whether water exercises are appropriate for you.
Heat
The use of heat is recommended for many people with arthritis, but not all. Your doctor can help you determine if it is appropriate for you. People whose arthritis symptoms respond well to heat have discovered many benefits. They have found that heat can to a great extent relax their muscles, decrease pain and stiffness and allow them to move through their exercises and daily activities with greater ease.
Warm water is an especially good way to deliver and distribute heat to many parts of the body. Extremely hot water is not safe and is not necessary to get results. Mild heat is just as effective and easier for the body to tolerate. The water temperature should feel soothing and comfortable, not hot. In a pool, water temperatures between 83 to 88 degrees are usually comfortable for people who are exercising. People who are just soaking or doing very gentle movements while sitting in a spa can usually tolerate higher temperatures. Soaking time will vary depending on the water temperature and an individual’s tolerance to heat. New spa users should vary the temperature and length of stay until they can determine what is most comfortable. Start slowly and extend the time in the spa as tolerated. For most people, soaking time should not exceed 10-15 minutes at temperatures between 98-104 degrees. Remember too that children and elderly persons are more prone to become overheated.
Doctors often advise that people with arthritis soak in warm water in the morning before beginning their daily activities. This is a time when many people find that pain and stiffness is at its worst. It may be just as beneficial to use spas or warm water pools at other times: in the afternoon to help relax muscles and joints after a full day of activities; to loosen muscles before doing exercises; in the evening before bedtime to bring on a restful sleep.
Gastrointestinal system
Drinking water significantly elevates the resting energy expenditure in adults but in overweight children transient decrease in resting energy expenditure was observed immediately after drinking 10 ml/kg cold water 39.2 °F (4°C). Then a subsequent rise in resting energy expenditure was observed, which was significant after 24 min and the maximal mean resting energy expenditure values were seen after 57 min, which was 25% higher than baseline. The recommended daily amount of water consumption in children could result in energy expenditure equivalent to additional weight loss of about 1.2 kg/year suggesting that water drinking could assist overweight children in weight loss or maintenance 76. Exposure to cold increases metabolic rate, for example, head-out immersion in cold water of 68 °F (20°C) almost doubles metabolic rate, while at 57.2 °F (14°C) it is more than quadrupled 77.
When very-hot compress applied to lumbar region of healthy female for 10-min blood flow to the back increased to 156% with increased blood flow to upper arm. Immediately after hot compress, bowel sounds increased 1.7 times compared with before application, which suggest that a very hot compress can be useful to promote flatus or defecation 78. Low mineral water intake normalizes the intestinal permeability of patients with atopic dermatitis 79.
Warm water is effective for colonic spasm in which significantly less discomfort was reported compared with control group and this may be useful as an alternative for glucagon (expensive) and hyoscyamine (has side effects) because it has no side effects and costs practically nothing 80.
In patients with acute anal pain due to hemorrhoids or anal fissures, neither cold water <59 °F (<15°C) nor hot water > 86 °F (>30°C) sitz bath did control pain statistically 81. Similarly, after sphincterotomy for anal fissure, sitz bath produced no significant difference in pain but significant relief in anal burning and better satisfaction score with no adverse effects were observed compared with control group 82. Healing and pain relief was not significant in sitz bath but it improved patient satisfaction in acute anal fissures 83.
Though there was no strong evidence to support the use of sitz bath for pain relief and to accelerate fissure or wound healing among adult patients with anorectal disorders, patients were satisfied with using sitz bath and no severe complications were reported 84. In contrast, warm-water sitz bath (104 °F [40°C], 113 °F [45°C], and 122 °F [50°C] for 10 min each time) in anorectal disorder, pain relief was more evident and lasted longer at higher bath temperatures. Pain relief after sitz bath might attribute to internal anal-sphincter relaxation, which might be due to thermosphincteric reflex, resulting in diminution of the rectal neck pressure. The higher the bath temperature, the greater the drop in rectal neck pressure and internal sphincter electromyographic activity, and longer the time needed to return to pretest levels 85.
In posthemorrhoidectomy care, water spray method could provide a safe and reliable alternative to sitz bath as a more convenient and satisfactory form of treatment 86.
Spa treatment with mineral water sulfate calcium induced clinical remission of the disease, normalization of the echoscopic picture of stomach and gallbladder, their motor function, tesiocrystalloscopic characteristics of saliva suggest its effectiveness in rehabilitation of patients with gastric and gallbladder motor-evacuatory dysfunction 87. Intake of sulfate-chloride-sodium mineral water activates regulation of carbohydrate metabolism by insulin and cortisol due to the formation of adaptive reactions. It promoted trophic effects of insulin and gastrin in animals with significant reduction in peptic ulcer size and enhanced resistance to stressful factors 88.
Immersion in Dead Sea water produced significant reduction in blood glucose in type-2 diabetes mellitus and no significant differences in insulin, cortisol, and c-peptide levels were observed between diabetes mellitus patients and healthy volunteers following immersion 89.
Genito urinary system
Mean labor pain scores were significantly higher in control group than immersion bath (immersion bath) group suggest that use of immersion bath as an alternative form of pain relief during labor 90. Head-out water immersions in primipara at any stage of labor, from 2 cm external opening of the uterine cervix, significantly decreased parturition duration compared with traditional delivery. It raised both the amplitude and frequency of uterine contractions proportional to uterine cervix gaping with no disturbances in contraction activity of the uterus. A 3-cm gaping of uterine cervix is the optimal timing for head-out water immersions in the primipara because earlier head-out water immersions at 2-cm uterine cervix gaping also accelerated the labor but required repetitions of head-out water immersions or use of oxytocin for correcting weakened uterine contraction 91.
In contrast, immersion bath did not influence the length of labor and uterine contractions frequency. However, contractions length was statistically shorter in immersion bath and it can be an alternative for woman’s comfort during labor, since it provides relief to her without interfering on labor progression or jeopardizing the baby 92.
Head-out water immersions during first stage of labor reduces the use of epidural/spinal/paracervical analgesia/anesthesia compared with controls and there is no evidence of increased adverse effects to fetus/neonate or woman from laboring in water or water birth 93. Neonatal swimming can accelerate babies growth in early stage 94. In a microbiological study, comparing neonatal bacterial colonization after water birth to conventional bed deliveries with or without relaxation bath showed no significant difference between three groups in neonatal outcome, infant’s and maternal infection rate 95.
Cold-sitz bath but not warm-sitz bath, significantly reduced edema during postepisiotomy period 96 and perineal pain, which was greatest immediately after the bath 97. Bakera, a steam bath prepared with various plants (commonly the essential oil plants) is traditionally used in Minahasa (Indonesia) mainly for recuperation after childbirth. It is based onthermotherapy with aromatherapy which attribute for its therapeutic effects. Thermotherapy soothes symptoms such as heaviness in limbs, edema, muscular strain, loss of appetite, and constipation. Essential oils of the plants used have antiseptic, antiphlogistic, and immunostimulant effect. Hence it can be an effective and safe method for recuperation after child birth 98. In postnatal mothers, alternate (hot and cold) compress and cold cabbage leaves were equally effective in reducing breast engorgement, but in relieving breast engorgement pain, alternate compresses were more effective than cold cabbage leaves 99.
Warm-sitz bath 104-113 °F (40-45°C) for 10 min, for at least 5 days immediately after the removal of Foley urethral catheter in patient undergone transurethral resection of prostate (TURP), significantly reduced urethral stricture compared with no sitz bath group who had 1.13-fold increased risk of re-hospitalization within 1 month after surgery due to postoperative complications compared with warm-sitz bath group 100. Thirty healthy volunteers and 21 patients with urinary retention after hemorrhoidectomy underwent sitz bath at 40°C, 45°C, and 50°C where the number of spontaneous micturitions increased with higher-temperature baths and it seems to be initiated by reflex (thermo-sphincter reflex) internal urethral sphincter relaxation. The urethral pressure both in normal and retention subjects showed significant reduction, which increased with higher temperature; and vesical pressure or EMG activity of the external urethral sphincter did not show significant differences 101.
Hematology and immunology
Subsequent cold exposure induced increase of leukocytes, granulocytes, circulating levels of interleukin (IL)-6, and natural killer (NK) cells and its activity. Leukocytes, granulocyte, and monocyte responses were augmented by pretreatment with exercise in water 64.4 °F (18°C) and thus acute-cold exposure has immune-stimulating effects 102.
Daily brief cold stress can increase both numbers and activity of peripheral cytotoxic T-lymphocytes and natural killer (NK) cells, the major effectors of adaptive and innate tumor immunity, respectively. It (for 8 days) improved survival of intracellular parasite Toxoplasma gondii infected mice, with consistent enhancement in cell-mediated immunity. The sustained/longer-term effects of cold stress repeated daily over the period of 5 days to 6 weeks increased plasma levels of tumor necrosis factor-α, IL-2, IL-6. A hypothesis describes, daily brief cold-water stress over many months could enhance antitumor immunity and improve nonlymphoid cancer survival rate. The possible mechanism of nonspecific stimulation of cellular immunity might attribute to transient activation of sympathetic nervous system, hypothalamic-pituitary-adrenal and hypothalamic-pituitary-thyroid axes. Though daily moderate cold hydrotherapy does not appear to have noticeable adverse effects on normal subjects, some studies showed that it can cause transient arrhythmias in patients with heart problems and can also inhibit humoral immunity. Sudden ice-cold head-out water immersions can produce transient pulmonary edema and increase blood-brain barrier permeability, thereby increasing mortality of neurovirulent infections. Studies are required to warrant this hypothesis for immunotherapy development for some (nonlymphoid) cancers, including those caused by viral infections 103.
Warm water 82.4 °F (28°C) treatment could not only cure bacterial cold-water disease but also immunize against causative agent Flavobacterium psychrophilum 104.
Head-out head-out water immersions 101.13 ± 0.04°F (38.41 ± 0.04°C) for 30 min decreased blood viscosity; red blood cells count; and mean hematocrit without significant changes in leukocytes and platelets count; mean corpuscular volume; plasma viscosity; erythrocyte filtration time and red cell deformability index 105. Application of hyper-thermic water bath produced significant reduction of relative B-lymphocyte. Whole-body hyperthermic water bath reduced relative total T-lymphocyte counts; increased relative CD8+ lymphocyte; NK cell counts and its activity, which were probably dependent on increased somatotropic hormone production 106.
Endocraine and hormonal system
During cold exposure increase levels of circulating norepinephrine was observed 102 and exercising hypothalamic-pituitary-adrenal system by repeated cold exposure could potentially restore its normal function in chronic fatigue syndrome, or at least increase net hypothalamic-pituitary-adrenal activity (without changing baseline activity) 107. It produces temporary increase in plasma levels of adrenocorticotropic hormone (ACTH), beta-endorphin, and cortisol 108. The sustained/longer-term effects of cold stress repeated daily produced increase in ACTH, corticosterone, and decrease in α-1-antitrypsin and testosterone 109. Cold stress reduces level of serotonin in most regions of brain (except brainstem) 108. Cold stress-induced analgesia might be mediated by increased production of opioid peptide beta-endorphin (an endogenous pain-killer) 110.
Exposure to sauna and ice-head-out water immersions significantly elevated epinephrine levels in winter swimmer 111. Steam bath produced increase in blood serum concentrations of gastric and aldosterone, with decrease in concentrations of cortisol in athlete-fighters 112. Whole-body hyperthermic bath increased sauna-therapyH activity in 8 out of 10 volunteers 106.
Eye, skin, and hair
Warm moist air device seems to be safe and produced improvement in tear stability and symptomatic relief in ocular fatigue in patients with meibomian gland dysfunction 113. Sauna 176 °F (80°C) produced stable epidermal barrier function; increase in stratum corneum hydration; faster recovery of both elevated water loss and skin pH; decrease in casual skin sebum content on skin surface of forehead; increase in ionic concentration in sweat and epidermal blood perfusion in volunteers. It suggests protective effect of sauna-therapy on skin physiology 114. Clinical remission of atopic dermatitis has been reported after intake of low-salt water 115. Application of heated mustard compress produced second-degree, partial-thickness burn followed by hyperpigmentation and hypertrophic scarring 116. Persistent use of cold pillow compress could reduce hair follicles inhibition or damage caused by chemotherapeutic agents. So alopecia can be decreased or prevented 117.
Temperature regulation
Very-hot compress applied to lumbar region of healthy female for 10 min increased back skin temperature to 105.98-109.58 °F (41.1-43.1°C) under hot compress, followed by decreased rapidly but no changes observed in body temperature 78. A case of 20% of 2nd degree burns and severe heat stroke followed by temperature rose up to 104.9 °F (40.5°C) and patient developed severe multiorgan failure and critical polyneuropathy was reported after exposure to extreme heat in sauna for unknown period of time 118. The most effective method of reducing body core temperature appears to be immersion in iced water, main predictor of outcome in exertional heatstroke is the duration and degree of hyperthermia where possible patients should be cooled using iced-head-out water immersions, but if it is not possible, combination of other techniques may be used to facilitate rapid cooling 119 such as fan-therapy, Chead-out water immersions, iced-baths, and evaporative cooling 120.
Wet-ice, dry-ice, and cryogen packs applied to skin overlying right triceps surae muscle for 15 min on 10 females decreased mean skin temperature 53.6 °F (12°C), 49.82 °F (9.9°C), and 45.14 °F (7.3°C), respectively. None of the modalities produced skin temperature cooling below 62.6 °F (17°C) and no cooling was demonstrated 1 cm proximal or distal to any modalities after 15 min of application. Significant mean skin temperature reduction in between pretreatment rest interval (time 0) and 15 min after removal of modality (time 30) was observed only in wet-ice. It suggests wet-ice was significantly more efficient in reducing skin temperature than dry-ice and cryogen packs 121.
After exercise at 65% maximal oxygen consumption at ambient temperature of 102.2 °F (39°C) until rectal temperature increased to 104 °F (40°C) produced no difference in cooling rate between head-out water immersions at 46.4 °F (8°C), 57.2 °F (14°C), and 68 °F (20°C) but cooling rate was significantly greater during 35.6 °F (2°C), which was almost twice as much as other conditions. It suggests that 35.6 °F (2°C) head-out water immersions is the most effective treatment for exercise-induced hyperthermia 122. When hyperthermic individuals are immersed in 35.6 °F (2°C) water for approximately 9 min to rectal temperature cooling limit of (38.6°C) negated any risk associated with overcooling 123.
Whole body immersion in moderately cold water is effective cooling maneuver for lowering body temperature and body heat content of approximately 545 kJ at the end of immersion in absence of severe physiological responses generally associated with sudden cold stress 124. Significant less body temperature variability and an overall higher body temperature were observed in late preterm infants following tub bathing procedure 125.
How to do water therapy
Water therapy exercises
Exercises in water can be most helpful and enjoyable for people with arthritis. Water can provide warmth and support (buoyancy) which can facilitate the exercising of joints affected by arthritis. Spas can provide ready access to warm water exercises in the home. Soaking in warm water allows muscles to become relaxed which can then make it easier to perform exercises and carry out daily tasks. Relaxed muscles can also create an overall feeling of comfort. Pools also enable people with arthritis to relax and exercise their joints often in the company of others. Pools offer more space than spas, allowing for a wider variety and more vigorous exercises.
Warm water exercises
When first entering a spa or pool, relax and enjoy the soothing water. When your muscles and joints feel more comfortable and relaxed, slowly begin your exercise routine. Allow enough time after exercising to again relax muscles before getting out of the water.
The Arthritis Foundation recommends the following guidelines when doing water exercises:
- Submerge body part being exercised.
- Move the body part slowly and gently.
- Begin and end with easy exercises.
- Follow through complete joint range of motion if possible, but do not force movement. Stop if you experience any sudden or increased pain.
- Do three to eight repetitions as tolerated.
- Pain that lasts for more than one to two hours after exercise may indicate overuse. Cut back next time.
- Remember the weakening effects of heat when exercising in warm water.
- Start slowly and don’t overdo.
- Any individuals who have severe joint damage or joint replacement should check with their doctor or surgeon before doing any of the following exercises.
The following illustrations of exercises can be done while sitting in a spa or while sitting or standing in a pool. Consult your doctor or physical therapist to determine which exercises are appropriate for you.
Shoulder
Forward arm reach (flexion):
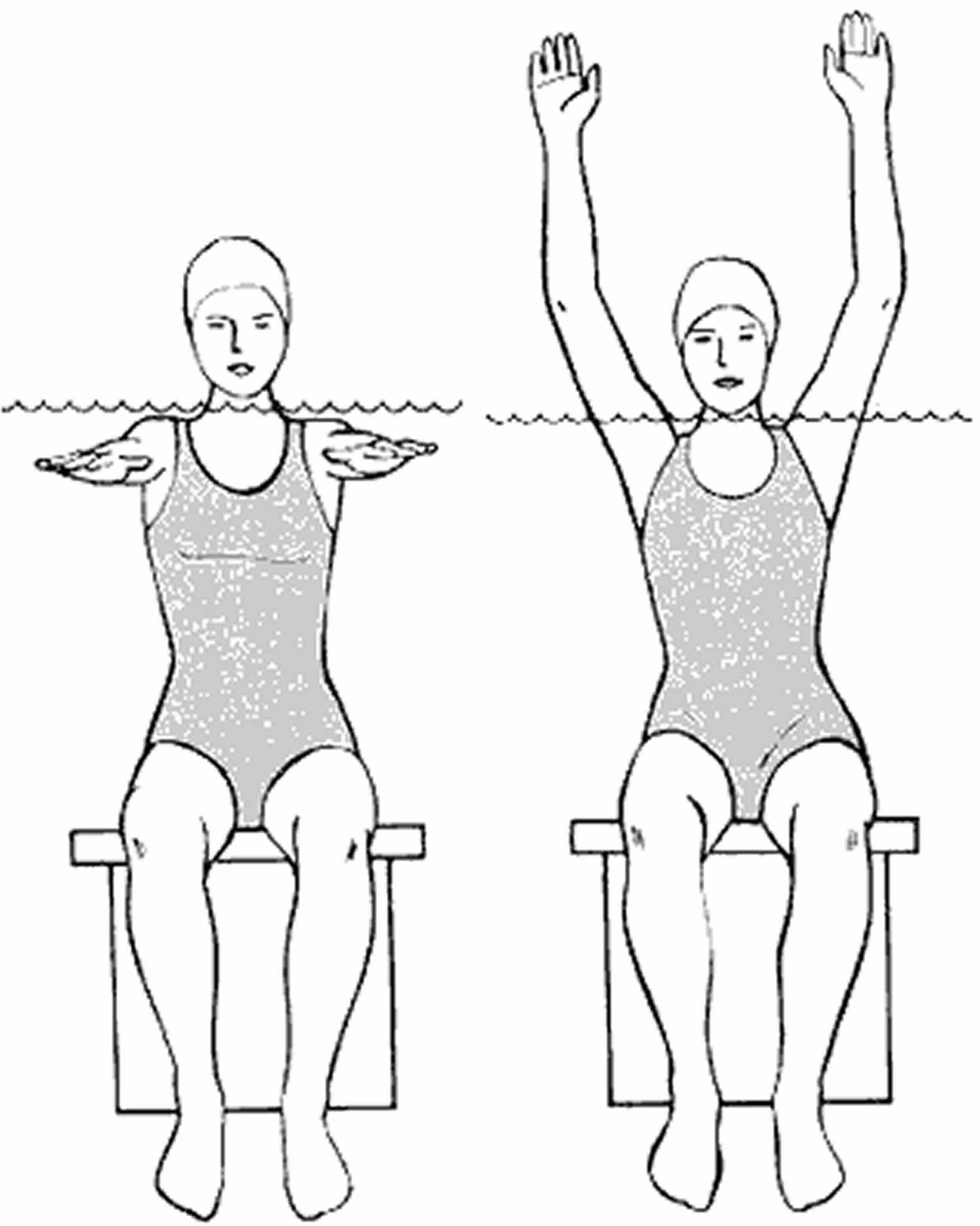
- Raise one or both arms forward and upward as high as possible. If one arm is very weak, you can help it with the other arm. See figure 1.
Figure 1. Forward arm reach
Sideways arm reach (abduction):
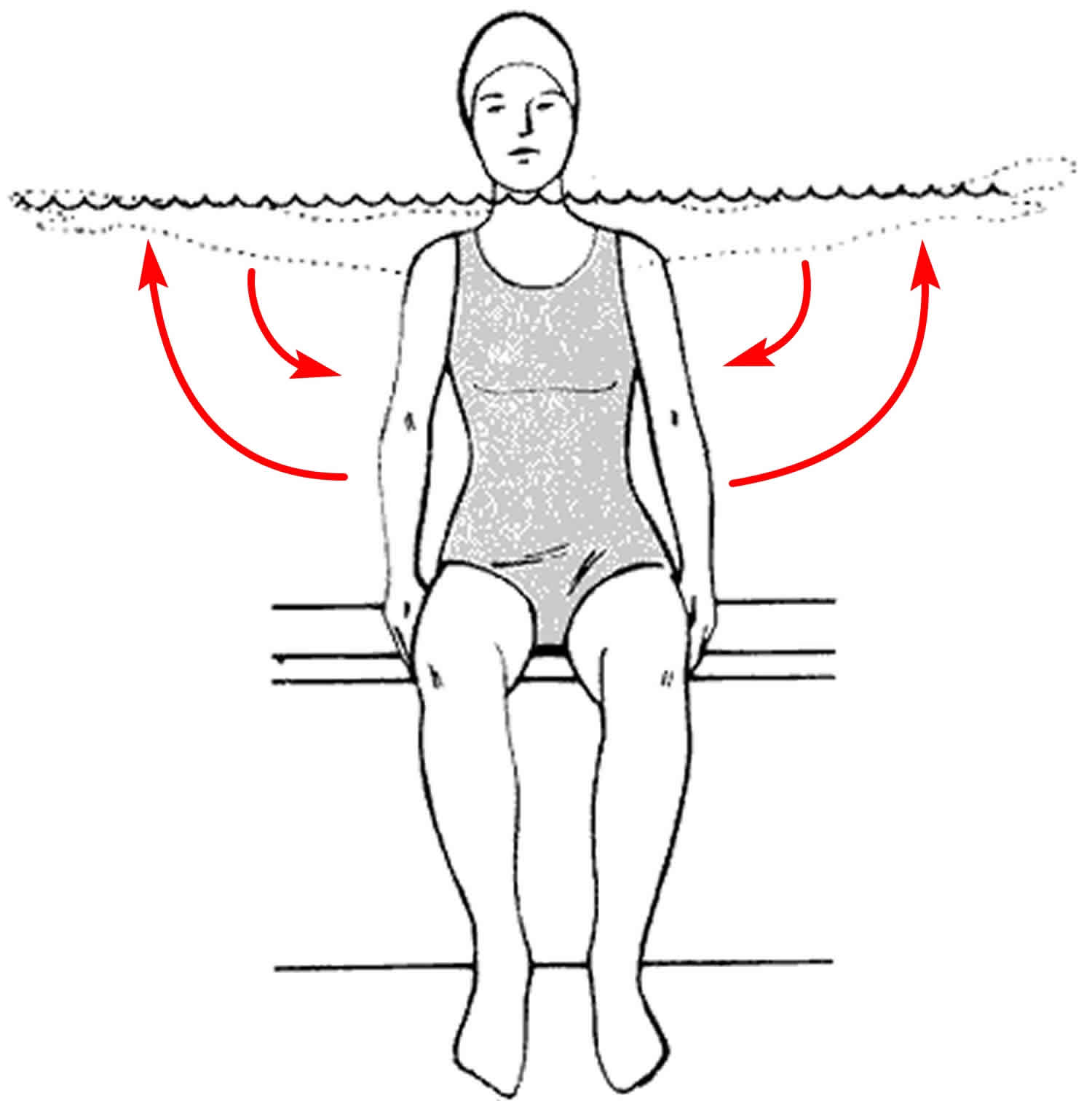
- Slowly raise both arms out to the side, keeping the palms down. Raise only to shoulder (water) level. Then lower arms. See figure 2.
Figure 2. Sideways arm reach
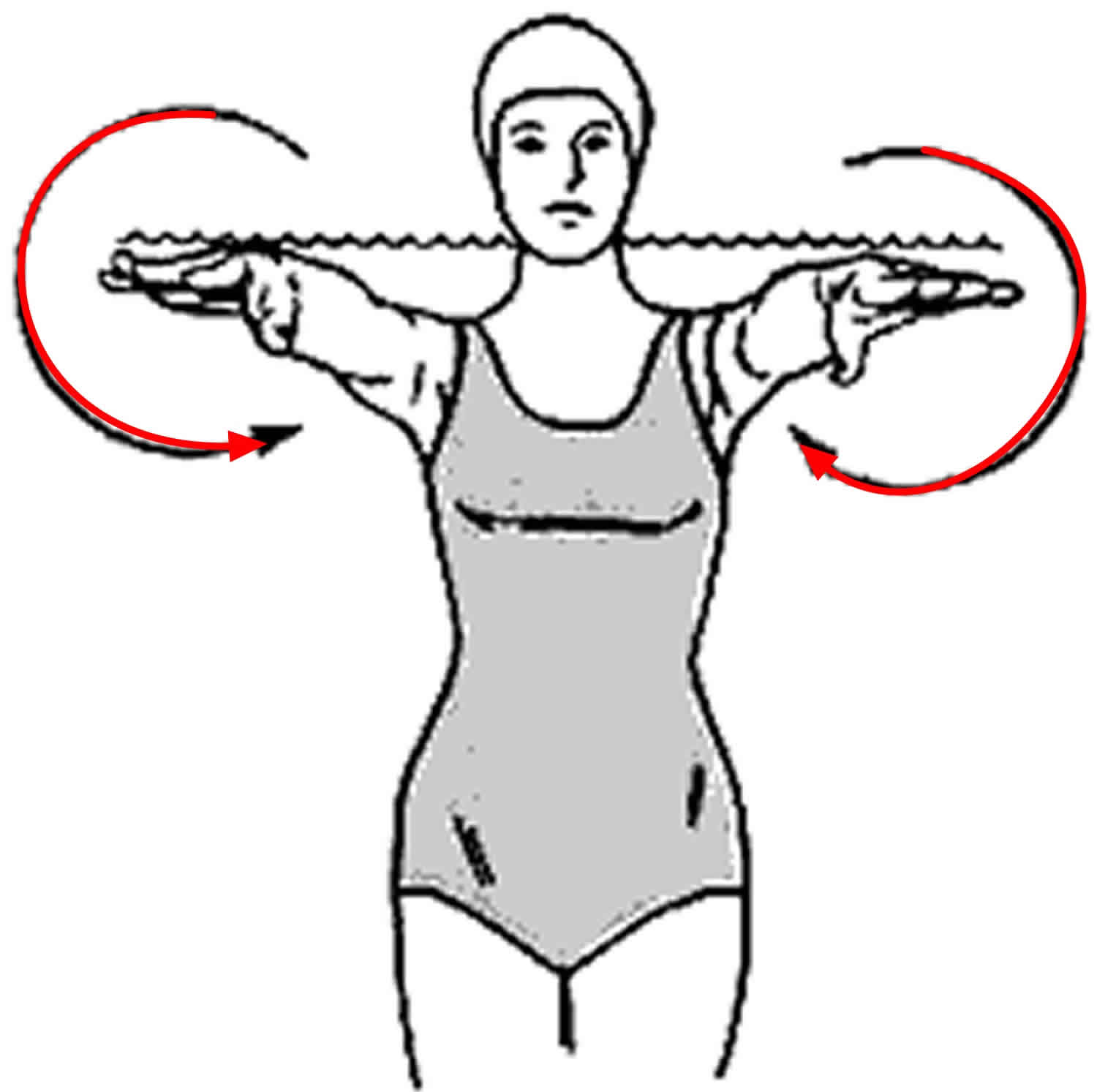
Arm circles (combined motions):
Raise both arms forward until they are a few inches below water level. Keep both elbows straight. Make small circles (about the size of a softball) with the arms. Gradually increase circle size (until the size of a basketball). Then decrease. First make inward, then outward circles. Do not raise your arms out of the water or let them cross. See figure 3.
Figure 3. Arm circles
Elbow
Elbow bend (flexion/extension):
- Bend the elbows and the thumbs to the shoulders. You do not have to touch. Relax elbows and straighten down along side of you.
Elbow bend and turn (combined motion):
- Turn the arms until the palms face forward. Bend the elbows until the fingertips touch the shoulders. Relax and straighten your elbows leading down with your palms.
Wrist and fingers
Wrist turn (supination/pronation):
- Turn the palms toward the ceiling, then turn them down to face the bottom of the spa or pool.
Wrist bend (flexion/extension):
- Bend the wrists backward and then forward.
Hand and fingers
Finger hold (thumb opposition):
- Touch the tip of the left thumb to the tips of the other fingers one at a time to form a round letter “O”. Repeat with right thumb. (May move both thumbs at the same time.)
Finger curl (flexion/extension):
- Curl the fingers into the palm (making a loose fist) and then straighten them out.
Thumb circles (circumduction):
- Move the thumb in a large circle.
Ankle and toes
Ankle bend:
- Sit with back supported and slowly straighten your knee. While holding the knee straight, bend the ankle and point the toes. Then reverse to point them toward the ceiling.
Toe curl (flexion/extension):
- Curl right toes down and then straighten them out. Repeat with left foot.
Ankle circles (dorsiflexion/plantar flexion and inversion/eversion):
- Sit with back supported and slowly straighten your knee. While holding the knee straight, make large inward circles with the foot moving from the ankle. Then repeat circles in the opposite direction. Repeat with other foot.
Hip and knee
Knee bend (flexion/extension):
- Slowly raise one foot up to straighten out your knee. Hold straight 3 seconds.
Knee to chest (combined stretch):
- Sit erect. Lift one knee and hug towards chest, hands under the thighs or over the knee to assist with the stretch.
Spread eagle hip (abduction with knee extension):
- Sitting on the edge of the seat, straighten one knee. While holding it straight, slowly move it out to the side, hold 3 seconds then bring it back to the center. Repeat with other leg.
Leg swing (hip flexion/extension):
- Stand with left side to pool wall, holding wall with left hand for balance. Keep knees straight. Lift right leg slowly forward to a comfortable height. If possible, hold leg for a count of 5 seconds, then slowly swing leg backward. Motion should only occur in hip (not waist or neck). Keep upper body straight at all times. Repeat with left leg–right side to wall.
Knee lift (hip and knee flexion/extension):
- Stand with back or left side against pool wall. Bend right knee, bringing thigh parallel to water surface. Straighten the knee; then bend it again. Lower leg, keeping knee bent. Repeat on left.
Calf stretch:
- Stand with left side to wall, holding wall with left hand for balance. Stand straight with legs slightly apart and left leg forward of right. Keeping body straight, lean forward slowly letting left knee bend. Keep right knee straight and heel on bottom. Return to starting position. Repeat with right leg forward, right side to pool.
Side leg lift (hip abduction and adduction):
- Stand with left side to pool wall, holding wall with left hand for balance, knees relaxed. Swing right leg out toward center of pool and back to midline. Do not cross in front of left leg. Repeat with left leg–right side to wall.
Walking:
- Walk normally across or in a circle in the pool. Swing your arms as you walk.
Trunk
Side bend (flexion):
- Place hands on hips and without moving your feet, bend slowly toward the right; then return to starting position and bend to the left. Do not twist or turn the trunk. Arms may hang at the side if preferred and as you lean to the right, let the right hand slide down the thigh. Repeat on the left.
Cold water immersion
The effect of cold water immersion on delayed onset muscle soreness and perceived fatigue was significant, but the effect size was small in terms of delayed onset muscle soreness. A previous meta-analysis indicated that cold water immersion induced a significant effect that was still observable at 96 h after exercise when compared with passive recovery 126. In the same publication, a lower rating of perceived fatigue was observed after cold water immersion 126. The improvement in overall fatigue through the use of cold water immersion has been reported in several circumstances after training and competition (e.g., soccer tournaments or basketball matches) 127. Another meta-analysis showed a positive effect of cold water immersion on lowering delayed onset muscle soreness after strenuous exercise in trained athletes and in untrained subjects or those who exercised recreationally 128. An exposure of 51.8-59 °F (11–15 °C) over 11–15 min was considered to be the optimal circumstance to obtain a positive impact of cold water immersion after exercise to reduce delayed onset muscle soreness 129. In this meta-analysis 130, the authors were able to detect significant differences depending on the water temperature. They observed that only immersion in water with a temperature lower than 59 °F (15°C) had a positive impact on inflammation. Depending on the type of exercise, the duration of immersion, the level of immersion and the water temperature, the outcomes were sometimes at variance.
Several mechanisms have been presented to explain the benefits of cold water immersion on recovery 131. A common explanation of the impact of cold water immersion on delayed onset muscle soreness and fatigue is a reduction in exercise-induced inflammation and muscle damage. Dupuy et al. 130 found a significant positive effect of cold water immersion on the creatine kinase concentration in the blood after intensive exercise, but the effect size was small. A moderate decrease of circulating creatine kinase has previously been reported with the use of cold water immersion after exercise 132. Both the level of immersion and the cold temperature of the water may reduce the formation of swelling and pain sensation after exhaustive physical exercise 133. Hydrostatic pressure may facilitate the transport of fluids from the muscle to the blood and therefore eliminate metabolites 128. Vasoconstriction due to cold temperature may also reduce fluid diffusion into the interstitial space 134 and locally diminish the inflammatory reaction 135, which in turn may reduce the feeling of pain 136. Cold alone has also a direct analgesic impact 137. However, some other authors did not detect any changes in the creatine kinase concentration after the use of cold water immersion following exhaustive physical exercise 138. No significant effect was observed in this meta-analysis 130 concerning changes in IL-6 and CRP concentrations in the blood. A similar observation has already been presented 138.
Contrast water therapy
Contrast water therapy is often used for recovery purposes and consists of bathing alternately in warm and cold water. We found that contrast water therapy had a significant impact on delayed onset muscle soreness (though the effect size was small) but not on perceived fatigue. A systematic review has previously expressed the significant impact of using this technique to improve recovery 139. A more recent work also showed the effectiveness of this technique after various forms of exhaustive and damaging exercises 140. Contrast water therapy was also able to significantly reduce the perception of pain at 24, 48, and 72 h post-eccentric exercise 141. Alternating therapy with cold and warm water immersion induces successive peripheral vasoconstriction and vasodilation 140 and may reduce the formation of oedema after exercise, influence inflammatory pathways and decrease the feeling of pain 142. Additionally, in this meta-analysis 130, the authors found that contrast water therapy reduced creatine kinase concentrations in the blood, indicating reduced muscle damage.
Compression garments
Similar to massage, both the use of compression garments and cold water immersion induced a significant and positive impact on delayed onset muscle soreness and perceived fatigue but had a less pronounced effect. It has been previously reported in a narrative review 143 and meta-analysis 144 that the use of compressive garments after damaging exercise affected delayed onset muscle soreness. Moreover, recent works confirmed these findings and showed that the effects were still significant at 96 h after exercise 144. This study 130 confirmed the significant impact of compression garments on delayed onset muscle soreness at 96 hour after exercise. The authors also found a significant decrease in perceived fatigue when compression garments were used. It has been shown that wearing a whole-body compression garment over a 24-h period after intense heavy resistance training significantly reduces perceived fatigue 145. The beneficial effect of compression garments on delayed onset muscle soreness and perceived fatigue might be explained by a possible reduction in the space available for swelling and oedema due to the compression applied to the limb, smaller changes in osmotic pressure that might diminish fluid diffusion in the interstitial space and better venous return 146.
It has been suggested that using a compression garment may also reduce exercise-induced muscle damage and inflammation 147. However, in our meta-analysis, we did not observe any significant changes in creatine kinase, IL-6, or CRP concentrations after the use of compression garments following exercise. This result is in contrast with a former meta-analysis that found that the use of compression garments was effective for reducing the creatine kinase concentration 148. Additionally, in the scientific literature concerning creatine kinase concentration and compression garments, there is a very wide range of study protocols. Some discrepancies in the findings exist and may nevertheless be explained by the different recovery period lengths, the lengths of the applied compression 149, the amount of pressure applied and the place (upper limbs, lower limbs, and even on whole-body) where the compression is applied 150. Additionally, individual variability in the sensitivity to blood flow changes may also be of importance 128. Similar remarks can be made for the absence of changes in IL-6 and CRP concentrations. Moreover, it previously been expressed that in the majority of the published works concerning the use of compression garments, the exercise protocols were not intense enough to induce a sufficient degree of muscle damage 151.
Water therapy summary
Based on available literature, water therapy or hydrotherapy was widely used to improve immunity and for the management of pain, heart failure, heart attack, chronic obstructive pulmonary diseases (COPD), asthma, Parkinson’s disease, ankylosing spondilitis, rheumatoid athritis, osteoarthritis of knee, fibromyalgia syndrome, anorectal disorders, fatigue, anxiety, obesity, hypercholesterolemia, hyperthermia, labor, etc. It produces different effects on various systems of the body depending on the temperature of water and though these effects are scientifically evidence based, there is lack of evidences for the mechanism on how hydrotherapy improves these diseases, which is one of the limitations of hydrotherapy, and further studies are required to find the mechanism of hydrotherapy on various diseases.
- Mooventhan A, Nivethitha L. Scientific evidence-based effects of hydrotherapy on various systems of the body. N Am J Med Sci. 2014;6(5):199-209. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4049052[↩][↩][↩][↩][↩]
- Naturopathy and the primary care practice. Fleming SA, Gutknecht NC. Prim Care. 2010 Mar; 37(1):119-36.[↩]
- Weston M, Taber C, Casagranda L, Cornwall M. Changes in local blood volume during cold gel pack application to traumatized ankles. J Orthop Sports Phys Ther. 1994;19:197–9.[↩]
- Srámek P, Simecková M, Janský L, Savlíková J, Vybíral S. Human physiological responses to immersion into water of different temperatures. Eur J Appl Physiol. 2000;81:436–42.[↩][↩][↩][↩]
- Huttunen P, Kokko L, Ylijukuri V. Winter swimming improves general well-being. Int J Circumpolar Health. 2004;63:140–4.[↩]
- The use of hydrotherapy for the management of spasticity. Kesiktas N, Paker N, Erdogan N, Gülsen G, Biçki D, Yilmaz H. Neurorehabil Neural Repair. 2004 Dec; 18(4):268-73.[↩]
- Moufarrij S, Deghayli L, Raffoul W, et al. How important is hydrotherapy? Effects of dynamic action of hot spring water as a rehabilitative treatment for burn patients in Switzerland. Ann Burns Fire Disasters. 2014;27(4):184-91. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4544428/[↩]
- Ellapen TJ, Hammill HV, Swanepoel M, Strydom GL. The benefits of hydrotherapy to patients with spinal cord injuries. Afr J Disabil. 2018;7(0):450. Published 2018 May 16. doi:10.4102/ajod.v7i0.450 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5968875/[↩]
- Weston M, Taber C, Casagranda L, Cornwall M. Changes in local blood volume during cold gel pack application to traumatized ankles. J Orthop Sports Phys Ther. 1994;19:197–9[↩]
- Iiyama J, Matsushita K, Tanaka N, Kawahira K. Effects of single low-temperature sauna bathing in patients with severe motor and intellectual disabilities. Int J Biometeorol. 2008;52:431–7[↩][↩][↩]
- Ohori T, Nozawa T, Ihori H, Shida T, Sobajima M, Matsuki A, et al. Effect of repeated sauna treatment on exercise tolerance and endothelial function in patients with chronic heart failure. Am J Cardiol. 2012;109:100–4[↩]
- Pilch W, Szyguła Z, Klimek AT, Pałka T, Cisoń T, Pilch P, et al. Changes in the lipid profile of blood serum in women taking sauna baths of various duration. Int J Occup Med Environ Health. 2010;23:167–74[↩]
- Sobajima M, Nozawa T, Shida T, Ohori T, Suzuki T, Matsuki A, et al. Repeated sauna therapy attenuates ventricular remodeling after myocardial infarction in rats by increasing coronary vascularity of noninfarcted myocardium. Am J Physiol Heart Circ Physiol. 2011;301:H548–54[↩]
- Imai Y, Nobuoka S, Nagashima J, Awaya T, Aono J, Miyake F, et al. Acute myocardial infarction induced by alternating exposure to heat in a sauna and rapid cooling in cold water. Cardiology. 1998;90:299–301.[↩]
- Crinnion WJ. Sauna as a valuable clinical tool for cardiovascular, autoimmune, toxicant- induced and other chronic health problems. Altern Med Rev. 2011;16:215–25.[↩]
- Bleakley CM, Davison GW. What is the biochemical and physiological rationale for using cold-water immersion in sports recovery? A systematic review. Br J Sports Med. 2010;44:179–87[↩][↩]
- Grüner Sveälv B, Cider A, Täng MS, Angwald E, Kardassis D, Andersson B. Benefit of warm water immersion on biventricular function in patients with chronic heart failure. Cardiovasc Ultrasound. 2009;7:33[↩]
- Digiesi V, Cerchiai G, Mannini L, Masi F, Nassi F. Hemorheologic and blood cell changes in humans during partial immersion with a therapeutic method, in 38 °C water. Minerva Med. 1986;77:1407–11.[↩]
- Boldt LH, Fraszl W, Röcker L, Schefold JC, Steinach M, Noack T, et al. Changes in the haemostatic system after thermoneutral and hyperthermic water immersion. Eur J Appl Physiol. 2008;102:547–54.[↩]
- Shih CY, Lee WL, Lee CW, Huang CH, Wu YZ. Effect of time ratio of heat to cold on brachial artery blood velocity during contrast baths. Phys Ther. 2012;92:448–53.[↩]
- Choukroun ML, Varene P. Adjustments in oxygen transport during head-out immersion in water at different temperatures. J Appl Physiol. 1990;68:1475–80.[↩]
- Dogliotti G, Galliera E, Iorio E, De Bernardi Di Valserra M, Solimene U, Corsi MM. Effect of immersion in CO2-enriched water on free radical release and total antioxidant status in peripheral arterial occlusive disease. Int Angiol. 2011;30:12–7.[↩]
- Sato M, Kanikowska D, Iwase S, Nishimura N, Shimizu Y, Belin de Chantemele E, et al. Effects of immersion in water containing high concentrations of CO2 (CO2-water) at thermoneutral on thermoregulation and heart rate variability in humans. Int J Biometeorol. 2009;53:25–30[↩][↩]
- Pagourelias ED, Zorou PG, Tsaligopoulos M, Athyros VG, Karagiannis A, Efthimiadis GK. Carbon dioxide balneotherapy and cardiovascular disease. Int J Biometeorol. 2011;55:657–63.[↩]
- Choukroun ML, Varene P. Adjustments in oxygen transport during head-out immersion in water at different temperatures. J Appl Physiol. 1990;68:1475–80[↩]
- Choukroun ML, Kays C, Varène P. Effects of water temperature on pulmonary volumes in immersed human subjects. Respir Physiol. 1989;75:255–65[↩]
- Goedsche K, Förster M, Kroegel C, Uhlemann C. Repeated cold water stimulations (hydrotherapy according to Kneipp) in patients with COPD. Forsch Komplementmed. 2007;14:158–66[↩]
- Iarosh AM, Kurch TK. The effect of cold exposure on the respiratory function in children suffering from inflammatory lung diseases. Vopr Kurortol Fizioter Lech Fiz Kult. 1995;1:9–11[↩]
- Pach D, Knöchel B, Lüdtke R, Wruck K, Willich SN, Witt CM. Visiting a sauna: Does inhaling hot dry air reduce common cold symptoms? A randomised controlled trial. Med J Aust. 2010;193:730–4.[↩]
- Whyte GP, Harries M, Dickinson J, Polkey MI. Breathless in the bath. Br J Sports Med. 2006;40:554–5.[↩]
- Herrera E, Sandoval MC, Camargo DM, Salvini TF. Motor and sensory nerve conduction are affected differently by ice pack, ice massage, and cold water immersion. Phys Ther. 2010;90:581–91[↩]
- Bender T, Karag¨ulle Z, B´alint GP, Gutenbrunner C, B´alint PV, Sukenik S. Hydrotherapy, balneotherapy, and spa treatment in pain management. Rheumatol Int. 2005;25:220–4.[↩]
- Castro-Sánchez AM, Matarán-Peñarrocha GA, Lara-Palomo I, Saavedra-Hernández M, Arroyo-Morales M, Moreno-Lorenzo C. Hydrotherapy for the treatment of pain in people with multiple sclerosis: A randomized controlled trial. Evid Based Complement Alternat Med 2012. 2012 473963.[↩]
- Vivas J, Arias P, Cudeiro J. Aquatic therapy versus conventional land-based therapy for Parkinson’s disease: An open-label pilot study. Arch Phys Med Rehabil. 2011;92:1202–10.[↩]
- Gerner HJ, Engel P, Gass GC, Gass EM, Hannich T, Feldmann G. The effects of sauna on tetraplegic and paraplegic subjects. Paraplegia. 1992;30:410–9.[↩]
- Shevchuk NA. Hydrotherapy as a possible neuroleptic and sedative treatment. Med Hypotheses. 2008;70:230–8.[↩]
- Shevchuk NA. Possible use of repeated cold stress for reducing fatigue in chronic fatigue syndrome: A hypothesis. Behav Brain Funct. 2007;3:55.[↩][↩][↩]
- Shevchuk NA. Adapted cold shower as a potential treatment for depression. Med Hypotheses. 2008;70:995–1001[↩]
- Chevutschi A, Lensel G, Vaast D, Thevenon A. An Electromyographic Study of Human Gait both in Water and on Dry Ground. J Physiol Anthropol. 2007;26:467–73[↩]
- Felson D. Osteoarthritis of knee. N Engl J Med. 2006;354:841–848.[↩]
- O’Connor M. Sex differences in osteoarthritis of the hip and knee. J Am Acad Orthop Surg. 2007;15:522–525.[↩]
- Hochberg M., Altman R., April K. American college of rheumatology recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken) 2012;64:465–474.[↩]
- Geytenbeek J. Evidence for effective hydrotherapy. Physiotherapy. 2002;88:514–529.[↩]
- Bartels E.M., Juhl C.B., Christensen R. Aquatic exercise for the treatment of knee and hip osteoarthritis. Cochrane Database Syst Rev. 2016;3:CD005523[↩]
- Peter W., Jansen M., Hurkmans E. Physiotherapy in hip and knee osteoarthritis: development of a practice guideline concerning initial assessment, treatment and evaluation. Acta Reumatol Port. 2011;36:268–281[↩]
- Hinman R., Heywood S., Day A. Aquatic physical therapy for hip and knee osteoarthritis: results of a single-blind randomized controlled trial. Phys Ther. 2007;87:32–43.[↩]
- Dias JM, Cisneros L, Dias R, et al. Hydrotherapy improves pain and function in older women with knee osteoarthritis: a randomized controlled trial. Braz J Phys Ther. 2017;21(6):449-456. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5693429/[↩]
- Kidd B. Osteoarthritis and joint pain. Pain. 2006;123:6–9.[↩]
- Crowther F, Sealey R, Crowe M, Edwards A, Halson S. Influence of recovery strategies upon performance and perceptions following fatiguing exercise: a randomized controlled trial. BMC Sports Sci Med Rehabil. 2017;9:25. Published 2017 Dec 28. doi:10.1186/s13102-017-0087-8 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5745760/[↩]
- Crowther F, Sealey R, Crowe M, Edwards A, Halson S. Team sport athletes’ perceptions and use of recovery strategies: a mixed-methods survey study. BMC Sports Sci Med Rehab. 2017;9:1–10. doi: 10.1186/s13102-016-0066-5[↩][↩]
- Bleakley CM, Davison GW. What is the biochemical and physiological rationale for using cold-water immersion in sports recovery? A systematic review. Br J Sports Med. 2010;44:179–187. doi: 10.1136/bjsm.2009.065565[↩]
- Versey NG, Halson SL, Dawson BT. Water immersion recovery for athletes: effect on exercise performance and practical recommendations. Sports Med. 2013;43:1101–1130. doi: 10.1007/s40279-013-0063-8[↩]
- Wilcock IM, Cronin JB, Hing WA. Physiological response to water immersion: a method for sport recovery? Sports Med. 2006;36:747–765. doi: 10.2165/00007256-200636090-00003[↩]
- Hing WA, White SG, Bouaaphone A. Contrast therapy- a systematic review. Phys Ther Sport. 2008;9:148–146. doi: 10.1016/j.ptsp.2008.06.001[↩][↩][↩]
- Coffey V, Leveritt M, Gill N. Effect of recovery modality on 4-hour repeated treadmill running performance and changes in physiological variables. J Sci Med Sport. 2004;7:1–10. doi: 10.1016/S1440-2440(04)80038-0[↩]
- Bleakley C, McDonough S, Gardner E, Baxter GD, Hopkins JT, Davison GW. Cold-water immersion (cryotherapy) for preventing and treating muscle soreness after exercise. Cochrane Database Syst Rev. 2012;2:CD008262[↩][↩]
- Morton RH. Contrast water immersion hastens plasma lactate decrease after intense anaerobic exercise. J Sci Med Sport. 2007;10:467–70.[↩]
- Skurvydas A, Kamandulis S, Stanislovaitis A, Streckis V, Mamkus G, Drazdauskas A. Leg immersion in warm water, stretch-shortening exercise, and exercise-induced muscle damage. J Athl Train. 2008;43:592–9[↩]
- Versey NG, Halson SL, Dawson BT. Effect of contrast water therapy duration on recovery of running performance. Int J Sports Physiol Perform. 2012;7:130–40[↩]
- Janssen RG, Schwartz DA, Velleman PF. A randomized controlled study of contrast baths on patients with carpal tunnel syndrome. J Hand Ther. 2009;22:200–7[↩]
- Yurtkuran M, Yurtkuran M, Alp A, Nasircilar A, Bingöl U, Altan L, et al. Balneotherapy and tap water therapy in the treatment of knee osteoarthritis. Rheumatol Int. 2006;27:19–27.[↩][↩]
- De Nardi M, La Torre A, Barassi A, Ricci C, Banfi G. Effects of cold-water immersion and contrast-water therapy after training in young soccer players. J Sports Med Phys Fitness. 2011;51:609–15.[↩]
- McVeigh JG, McGaughey H, Hall M, Kane P. The effectiveness of hydrotherapy in the management of fibromyalgia syndrome: A systematic review. Rheumatol Int. 2008;29:119–30[↩]
- Matsumoto S, Shimodozono M, Etoh S, Miyata R, Kawahira K. Effects of thermal therapy combining sauna therapy and underwater exercise in patients with fibromyalgia. Complement Ther Clin Pract. 2011;17:162–6.[↩]
- Cuesta-Vargas AI, Adams N. A pragmatic community-based intervention of multimodal physiotherapy plus deep water running (DWR) for fibromyalgia syndrome: A pilot study. Clin Rheumatol. 2011;30:1455–62.[↩]
- Hay L, Wylie K. Towards evidence-based emergency medicine: Best BETs from the Manchester Royal Infirmary. BET 4: Hydrotherapy following rotator cuff repair. Emerg Med J. 2011;28:634–5[↩]
- Altan L, Bingöl U, Aslan M, Yurtkuran M. The effect of balneotherapy on patients with ankylosing spondylitis. Scand J Rheumatol. 2006;35:283–9.[↩]
- Oosterveld FG, Rasker JJ, Floors M, Landkroon R, van Rennes B, Zwijnenberg J, et al. Infrared sauna in patients with rheumatoid arthritis and ankylosing spondylitis. A pilot study showing good tolerance, short-term improvement of pain and stiffness, and a trend towards long-term beneficial effects. Clin Rheumatol. 2009;28:29–34[↩]
- Wouters EJ, Van Nunen AM, Geenen R, Kolotkin RL, Vingerhoets AJ. Effects of Aquajogging in Obese Adults: A Pilot Study. J Obes 2010. 2010 231074[↩]
- Arnold CM, Busch AJ, Schachter CL, Harrison EL, Olszynski WP. A Randomized clinical trial of aquatic versus land exercise to improve balance, function, and quality of life in older women with osteoporosis. Physiother Can. 2008;60:296–306[↩]
- Biscarini A, Cerulli G. Modeling of the knee joint load in rehabilitative knee extension exercises under water. J Biomech. 2006;17:1–11[↩]
- Eversden L, Maggs F, Nightingale P, Jobanputra P. A pragmatic randomised controlled trial of hydrotherapy and land exercises on overall well being and quality of life in rheumatoid arthritis. BMC Musculoskelet Disord. 2007;8:23.[↩][↩]
- Honda T, Kamioka H. Curative and health enhancement effects of aquatic exercise: Evidence based on interventional studies. Open Access J Sports Med. 2012;3:27–34[↩]
- Silva LE, Valim V, Pessanha AP, Oliveira LM, Myamoto S, Jones A, et al. Hydrotherapy versus conventional land-based exercise for the management of patients with osteoarthritis of the knee: A randomized clinical trial. Phys Ther. 2008;88:12–21.[↩]
- Xu XS, Lin WP, Chen JY, Yu LC, Huang ZH. Efficacy observation on rear thigh muscles strain of athletes treated with surrounding needling of electroacupuncture and hot compress of Chinese medicine. Zhongguo Zhen Jiu. 2012;32:511–4.[↩]
- Dubnov-Raz G, Constantini NW, Yariv H, Nice S, Shapira N. Influence of water drinking on resting energy expenditure in overweight children. Int J Obes (Lond) 2011;35:1295–300.[↩]
- Srámek P, Simecková M, Janský L, Savlíková J, Vybíral S. Human physiological responses to immersion into water of different temperatures. Eur J Appl Physiol. 2000;81:436–42[↩]
- Hishinuma M, Hiramatsu N, Kasuga M, Ooyoshi M, Kaharu C, Misao H, et al. The effect on bowel sounds of very hot compresses applied to the lumbar region. Nihon Kango Kagakkaishi. 1997;17:32–9.[↩][↩]
- Dupuy P, Cassé M, André F, Dhivert-Donnadieu H, Pinton J, Hernandez-Pion C. Low-salt water reduces intestinal permeability in atopic patients. Dermatology. 1999;198:153–5.[↩]
- Church JM. Warm water irrigation for dealing with spasm during colonoscopy: Simple, inexpensive, and effective. Gastrointest Endosc. 2002;56:672–4.[↩]
- Maestre Y, Parés D, Salvans S, Ibáñez-Zafón I, Nve E, Pons MJ, et al. Cold or hot sitz baths in the emergency treatment of acute anal pain due to anorectal disease? Results of a randomised clinical trial. Cir Esp. 2010;88:97–102.[↩]
- Gupta PJ. Effects of warm water sitz bath on symptoms in post-anal sphincterotomy in chronic anal fissure – a randomized and controlled study. World J Surg. 2007;31:1480–4.[↩]
- Gupta P. Randomized, controlled study comparing sitz-bath and no-sitz-bath treatments in patients with acute anal fissures. ANZ J Surg. 2006;76:718–21[↩]
- Lang DS, Tho PC, Ang EN. Effectiveness of the Sitz bath in managing adult patients with anorectal disorders. Jpn J Nurs Sci. 2011;8:115–28.[↩]
- Shafik A. Role of warm-water bath in ano-rectal conditions. The thermo-sphincteric reflex. J Clin Gastroenterol. 1993;16:304–8.[↩]
- Hsu KF, Chia JS, Jao SW, Wu CC, Yang HY, Mai CM, et al. Comparison of clinical effects between warm water spray and sitz bath in post-hemorrhoidectomy period. J Gastrointest Surg. 2009;13:1274–8.[↩]
- Guliaeva SF, Pomaskina TV, Guliaev PV, Martusevich AK, Aistov VI. Efficacy of sulfate calcium mineral water in disorders of motor evacuatory function of the stomach and gallbladder. Vopr Kurortol Fizioter Lech Fiz Kult. 2004;6:20–2[↩]
- Razumov AN, Surkov NV, Frolkov VK, Ziniakov NT. Therapeutic and preventive effects of sulfate-chloride-sodium mineral water in experimental peptic ulcer. Vopr Kurortol Fizioter Lech Fiz Kult. 2009;3:22–5.[↩]
- Mizrahi E, Liberty I, Tsedek I, Harari M, Friger M, Sukenik S. The influence of single immersion in Dead Sea water on glucose, insulin, cortisol and C-peptide levels in type 2 diabetes mellitus patients. Harefuah. 2011;150:646–9. 689, 688.[↩]
- Da Silva FM, de Oliveira SM, Nobre MR. A randomised controlled trial evaluating the effect of immersion bath on labour pain. Midwifery. 2009;25:286–94[↩]
- Malarewicz A, Wydrzynski G, Szymkiewicz J, Adamczyk-Gruszka O. The influence of water immersion on the course of first stage of parturition in primiparous women. Med Wieku Rozwoj. 2005;9:773–80.[↩]
- Da Silva FM, de Oliveira SM. The effect of immersion baths on the length of childbirth labor. Rev Esc Enferm USP. 2006;40:57–63.[↩]
- Cluett ER, Burns E. Immersion in water in labour and birth. Cochrane Database Syst Rev. 2009;2:CD000111[↩]
- Zhao S, Xie L, Hu H, Xia J, Zhang W, Ye N, et al. A study of neonatal swimming (water therapy) applied in clinical obstetrics. J Matern Fetal Neonatal Med. 2005;17:59–62[↩]
- Fehervary P, Lauinger-Lörsch E, Hof H, Melchert F, Bauer L, Zieger W. Water birth: Microbiological colonisation of the newborn, neonatal and maternal infection rate in comparison to conventional bed deliveries. Arch Gynecol Obstet. 2004;270:6–9[↩]
- LaFoy J, Geden EA. Post episiotomy pain: Warm versus cold sitz bath. J Obstet Gynecol Neonatal Nurs. 1989;18:399–403[↩]
- Ramler D, Roberts J. A comparison of cold and warm sitz baths for relief of postpartum perineal pain. J Obstet Gynecol Neonatal Nurs. 1986;15:471–4[↩]
- Zumsteg IS, Weckerle CS. Bakera, a herbal steam bath for postnatal care in Minahasa (Indonesia): Documentation of the plants used and assessment of the method. J Ethnopharmacol. 2007;111:641–50[↩]
- Arora S, Vatsa M, Dadhwal V. A Comparison of cabbage leaves vs. hot and cold compresses in the treatment of breast engorgement. Indian J Community Med. 2008;33:160–2[↩]
- Park SU, Lee SH, Chung YG, Park KK, Mah SY, Hong SJ, et al. Warm sitz bath: Are there benefits after transurethral resection of the prostate? Korean J Urol. 2010;51:763–6.[↩]
- Shafik A. Role of warm water bath in inducing micturition in postoperative urinary retention after anorectal operations. Urol Int. 1993;50:213–7.[↩]
- Brenner IK, Castellani JW, Gabaree C, Young AJ, Zamecnik J, Shephard RJ, et al. Immune changes in humans during cold exposure: Effects of prior heating and exercise. J Appl Physiol. 1999;87:699–710.[↩][↩]
- Shevchuk NA, Radoja S. Possible stimulation of anti-tumor immunity using repeated cold stress: A hypothesis. Infect Agent Cancer. 2007;2:20[↩]
- Sugahara K, Eguchi M. The use of warmed water treatment to induce protective immunity against the bacterial cold-water disease pathogen Flavobacterium psychrophilum in ayu (Plecoglossus altivelis) Fish Shellfish Immunol. 2012;32:489–93.[↩]
- Digiesi V, Cerchiai G, Mannini L, Masi F, Nassi F. Hemorheologic and blood cell changes in humans during partial immersion with a therapeutic method, in 38 o C water. Minerva Med. 1986;77:1407–11[↩]
- Blazícková S, Rovenský J, Koska J, Vigas M. Effect of hyper thermic water bath on parameters on cellular immunity. Int J Clin Pharmacol Res. 2000;20:41–6.[↩][↩]
- Dorfman M, Arancibia S, Fiedler JL, Lara HE. Chronic intermittent cold stress activates ovarian sympathetic nerves and modifies ovarian follicular development in the rat. Biol Reprod. 2003;68:2038–43[↩]
- Shevchuk NA. Possible use of repeated cold stress for reducing fatigue in chronic fatigue syndrome: A hypothesis. Behav Brain Funct. 2007;3:55[↩][↩]
- Shevchuk NA, Radoja S. Possible stimulation of anti-tumor immunity using repeated cold stress: A hypothesis. Infect Agent Cancer. 2007;2:20.[↩]
- Glickman-Weiss EL, Nelson AG, Hearon CM, Goss FL, Robertson RJ. Are beta-endorphins and thermoregulation during coldwater immersion related? Undersea Hyperb Med. 1993;20:205–13.[↩]
- Kauppinen K, Pajari-Backas M, Volin P, Vakkuri O. Some endocrine responses to sauna, shower and ice water immersion. Arctic Med Res. 1989;48:131–9.[↩]
- Panov SF, Pleshakov AA. Effect of steam bath on gastric secretion and some endocrine changes of athlete-fighters. Fiziol Cheloveka. 2011;37:92–9[↩]
- Matsumoto Y, Dogru M, Goto E, Ishida R, Kojima T, Onguchi T, et al. Efficacy of a new warm moist air device on tear functions of patients with simple meibomian gland dysfunction. Cornea. 2006;25:644–50[↩]
- Kowatzki D, Macholdt C, Krull K, Schmidt D, Deufel T, Elsner P, et al. Effect of regular sauna on epidermal barrier function and stratum corneum water-holding capacity in vivo in humans: A controlled study. Dermatology. 2008;217:173–80.[↩]
- Dupuy P, Cassé M, André F, Dhivert-Donnadieu H, Pinton J, Hernandez-Pion C. Low-salt water reduces intestinal permeability in atopic patients. Dermatology. 1999;198:153–5[↩]
- Linder SA, Mele JA, 3rd, Harries T. Chronic hyperpigmentation from a heated mustard compress burn: A case report. J Burn Care Rehabil. 1996;17:351–2[↩]
- Li LC, Wang M, Ning XC. Study on preventing alopecia caused by chemotherapy with cold pillow compresses. Chin J Nurs. 1995;30:643–5.[↩]
- Rünitz K, Jensen TH. Heat stroke and burns resulting from use of sauna. Ugeskr Laeger. 2009;171:305–6[↩]
- Smith JE. Cooling methods used in the treatment of exertional heat illness. Br J Sports Med. 2005;39:503–7[↩]
- Harker J, Gibson P. Heat-stroke: A review of rapid cooling techniques. Intensive Crit Care Nurs. 1995;11:198–202.[↩]
- Belitsky RB, Odam SJ, Hubley-Kozey C. Evaluation of the effectiveness of wet ice, dry ice, and cryogen packs in reducing skin temperature. Phys Ther. 1987;67:1080–4.[↩]
- Proulx CI, Ducharme MB, Kenny GP. Effect of water temperature on cooling efficiency during hyperthermia in humans. J Appl Physiol. 2003;94:1317–23[↩]
- Gagnon D, Lemire BB, Casa DJ, Kenny GP. Cold-water immersion and the treatment of hyperthermia: Using 38.6°C as a safe rectal temperature cooling limit. J Athl Train. 2010;45:439–44[↩]
- Marino F, Booth J. Whole body cooling by immersion in water at moderate temperatures. J Sci Med Sport. 1998;1:73–82.[↩]
- Loring C, Gregory K, Gargan B, LeBlanc V, Lundgren D, Reilly J, et al. Tub bathing improves thermoregulation of the late preterm infant. J Obstet Gynecol Neonatal Nurs. 2012;41:171–9.[↩]
- Bleakley C., McDonough S., Gardner E., Baxter D. G., Hopkins T. J., Davison G. W., et al. (2012). Cold-water immersion (cryotherapy) for preventing and treating muscle soreness after exercise. Sao Paulo Med. J. 130, 348–348. 10.1590/S1516-31802012000500015[↩][↩]
- Including stretches to a massage routine improves recovery from official matches in basketball players. Delextrat A, Hippocrate A, Leddington-Wright S, Clarke ND. J Strength Cond Res. 2014 Mar; 28(3):716-27.[↩]
- Cold water immersion and recovery from strenuous exercise: a meta-analysis. Leeder J, Gissane C, van Someren K, Gregson W, Howatson G. Br J Sports Med. 2012 Mar; 46(4):233-40.[↩][↩][↩]
- Can Water Temperature and Immersion Time Influence the Effect of Cold Water Immersion on Muscle Soreness? A Systematic Review and Meta-Analysis. Machado AF, Ferreira PH, Micheletti JK, de Almeida AC, Lemes ÍR, Vanderlei FM, Netto Junior J, Pastre CM. Sports Med. 2016 Apr; 46(4):503-14.[↩]
- Dupuy O, Douzi W, Theurot D, Bosquet L, Dugué B. An Evidence-Based Approach for Choosing Post-exercise Recovery Techniques to Reduce Markers of Muscle Damage, Soreness, Fatigue, and Inflammation: A Systematic Review With Meta-Analysis. Front Physiol. 2018;9:403. Published 2018 Apr 26. doi:10.3389/fphys.2018.00403 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5932411/[↩][↩][↩][↩][↩]
- What are the Physiological Mechanisms for Post-Exercise Cold Water Immersion in the Recovery from Prolonged Endurance and Intermittent Exercise? Ihsan M, Watson G, Abbiss CR. Sports Med. 2016 Aug; 46(8):1095-109.[↩]
- Sanchez-Ureña B. A., Barrantes-Brais K., Ureña-Bonilla P., Calleja-González J., Ostojic S. (2015). Effect of water immersion on recovery from fatigue: a meta-analysis. Eur. J. Hum. Mov. 34, 1–14.[↩]
- Physiological response to water immersion: a method for sport recovery? Wilcock IM, Cronin JB, Hing WA. Sports Med. 2006; 36(9):747-65.[↩]
- Effects of cold water immersion on the symptoms of exercise-induced muscle damage. Eston R, Peters D. J Sports Sci. 1999 Mar; 17(3):231-8.[↩]
- Comparison of three treatment procedures for minimizing ankle sprain swelling. Coté DJ, Prentice WE Jr, Hooker DN, Shields EW. Phys Ther. 1988 Jul; 68(7):1072-6.[↩]
- Acute inflammation: the underlying mechanism in delayed onset muscle soreness? Smith LL. Med Sci Sports Exerc. 1991 May; 23(5):542-51.[↩]
- Effects of long-term whole-body cold exposures on plasma concentrations of ACTH, beta-endorphin, cortisol, catecholamines and cytokines in healthy females. Leppäluoto J, Westerlund T, Huttunen P, Oksa J, Smolander J, Dugué B, Mikkelsson M. Scand J Clin Lab Invest. 2008; 68(2):145-53.[↩]
- The Effect of Post-Exercise Cryotherapy on Recovery Characteristics: A Systematic Review and Meta-Analysis. Hohenauer E, Taeymans J, Baeyens JP, Clarys P, Clijsen R. PLoS One. 2015; 10(9):e0139028.[↩][↩]
- Contrast therapy–a systematic review. Hing WA, White SG, Bouaaphone A, Lee P. Phys Ther Sport. 2008 Aug; 9(3):148-61.[↩]
- Contrast water therapy and exercise induced muscle damage: a systematic review and meta-analysis. Bieuzen F, Bleakley CM, Costello JT. PLoS One. 2013; 8(4):e62356.[↩][↩]
- Effect of cold water immersion on repeat cycling performance and thermoregulation in the heat. Vaile J, Halson S, Gill N, Dawson B. J Sports Sci. 2008 Mar; 26(5):431-40.[↩]
- Contrast therapy does not cause fluctuations in human gastrocnemius intramuscular temperature. Higgins D, Kaminski TW. J Athl Train. 1998 Oct; 33(4):336-40.[↩]
- Compression garments and exercise: garment considerations, physiology and performance. MacRae BA, Cotter JD, Laing RM. Sports Med. 2011 Oct 1; 41(10):815-43.[↩]
- Are compression garments effective for the recovery of exercise-induced muscle damage? A systematic review with meta-analysis. Marqués-Jiménez D, Calleja-González J, Arratibel I, Delextrat A, Terrados N. Physiol Behav. 2016 Jan 1; 153():133-48.[↩][↩]
- Effects of a whole body compression garment on markers of recovery after a heavy resistance workout in men and women. Kraemer WJ, Flanagan SD, Comstock BA, Fragala MS, Earp JE, Dunn-Lewis C, Ho JY, Thomas GA, Solomon-Hill G, Penwell ZR, Powell MD, Wolf MR, Volek JS, Denegar CR, Maresh CM. J Strength Cond Res. 2010 Mar; 24(3):804-14[↩]
- Kraemer W. J., Bush J. A., Wickham R. B., Denegar C. R., Gomez A. L., Gotshalk L. A., et al. (2001). Continuous compression as an effective therapeutic intervention in treating eccentric-exercise-induced muscle soreness. J. Sport Rehabil. 10, 11–23. 10.1123/jsr.10.1.11[↩]
- Kraemer W. J., French D. N., Spiering B. A. (2004). Compression in the treatment of acute muscle injuries in sport: review article. Int. J. Sport Med. 5, 200–208[↩]
- Compression garments and recovery from exercise-induced muscle damage: a meta-analysis. Hill J, Howatson G, van Someren K, Leeder J, Pedlar C. Br J Sports Med. 2014 Sep; 48(18):1340-6.[↩]
- Effects of compression stockings during exercise and recovery on blood lactate kinetics. Rimaud D, Messonnier L, Castells J, Devillard X, Calmels P. Eur J Appl Physiol. 2010 Sep; 110(2):425-33.[↩]
- The Effects of Compression-Garment Pressure on Recovery After Strenuous Exercise. Hill J, Howatson G, van Someren K, Gaze D, Legg H, Lineham J, Pedlar C. Int J Sports Physiol Perform. 2017 Sep; 12(8):1078-1084.[↩]
- Effect of wearing compression stockings on recovery after mild exercise-induced muscle damage. Bieuzen F, Brisswalter J, Easthope C, Vercruyssen F, Bernard T, Hausswirth C. Int J Sports Physiol Perform. 2014 Mar; 9(2):256-64.[↩]





{kind=link}