Contents
- Unsaturated fat
- What are the types of fat?
- Unsaturated fat vs Saturated fat
- Polyunsaturated fat vs Monounsaturated fat
- What kind of fats are the healthier?
- What are Healthy fats?
- What are Unhealthy fats?
- How much fat do I need?
- Are unsaturated fats bad?
- Foods high in unsaturated fat
- How to Make Healthy Lifestyle and Eating Choices
- What is the best way to lose weight?
Unsaturated fat
Unsaturated fats are fats that are liquid at room temperature. The two kinds of unsaturated fats are monounsaturated fat and polyunsaturated fat. Both of these unsaturated fats are typically liquid at room temperature. Unsaturated fats are in fish, such as salmon, trout and herring, and plant-based foods such as avocados, olives and walnuts. Liquid vegetable oils, such as soybean oil, corn oil, safflower oil, canola oil, olive oil, peanut oil, canola oil and sunflower oil, also contain unsaturated fats. Eaten in moderation, both kinds of unsaturated fats may help improve your blood cholesterol when used in place of saturated and trans fats. You want to include as many unsaturated fats in your diet because they can decrease bad LDL cholesterol, contain high amounts of antioxidants such as Vitamin E, and contain essential omega-3 fatty acids and omega-6 fatty acids. Unsaturated fats are typically classified by how many hydrogen bonds they have in their structure: either 1 (mono) or two or more (poly).
Unsaturated fats are those that are liquid at room temperature.
- Monounsaturated fats. Monounsaturated fat is a type of unsaturated fat. Monounsaturated fats are liquid at room temperature but start to harden when chilled. Monounsaturated fats is one of the healthy fats, along with polyunsaturated fat. Monounsaturated fats are good for your health in several ways:
- Monounsaturated fats can help lower your LDL (bad) cholesterol level. Cholesterol is a soft, waxy substance that can cause clogged, or blocked, arteries (blood vessels). Keeping your LDL level low reduces your risk for heart disease and stroke.
- Eating plant foods high in monounsaturated fats, particularly extra virgin olive oil and tree nuts, may benefit heart health and blood sugar regulation. Monounsaturated fats from plants may lower bad cholesterol and raise good cholesterol. They also may improve the control of blood sugar levels. Replacing saturated fats with monounsaturated fats in your diet may lower the level of bad cholesterol and triglycerides in your blood. Triglycerides are fat cells that circulate in the bloodstream and are stored in the body’s fat cells. A high level of triglycerides in the blood increases the risk of diseases of the heart and blood vessels.
- Monounsaturated fats help develop and maintain your cells.
- Monounsaturated fats are found in plant foods, such as nuts, avocados, and vegetable oils. Monounsaturated fats are found in red meats and dairy products. About half the fats in these foods are saturated and half monounsaturated. Many plants and plant oils are high in monounsaturated fats but low in saturated fats. These include:
- Oils from olives, peanuts, canola seeds, safflower seeds, and sunflower seeds.
- Avocadoes.
- Pumpkin seeds.
- Sesame seeds.
- Almonds.
- Cashews.
- Peanuts and peanut butter.
- Pecans.
- Polyunsaturated fats. Polyunsaturated fat is a type of unsaturated fat. Polyunsaturated fats are liquid at room temperature but start to harden when chilled. Polyunsaturated fats include omega-3 and omega-6 fats. These are essential fatty acids that your body needs for brain function and cell growth. Your body does not make essential fatty acids, so you must get them from food. Polyunsaturated fats can help lower your LDL (bad) cholesterol. Cholesterol is a soft, waxy substance that can cause clogged or blocked arteries (blood vessels). Having low LDL cholesterol reduces your risk for heart disease. Polyunsaturated fats is one of the healthy fats, along with monunsaturated fat. Polyunsaturated fat is found in plant and animal foods, such as salmon, vegetable oils, and some nuts and seeds.
- Omega-3 fatty acids are good for your heart in several ways. They help:
- Reduce triglycerides, a type of fat in your blood
- Reduce the risk of developing an irregular heartbeat (arrhythmia)
- Slow the buildup of plaque, a substance comprising fat, cholesterol, and calcium, which can harden and clog your arteries
- Slightly lower your blood pressure
- Sources of omega-3 fatty acids include:
- Fish such as salmon, anchovies, mackerel, herring, sardines and tuna.
- Oils from canola seeds, soybeans, walnuts and flaxseed.
- Soybeans.
- Chia seeds.
- Flaxseed.
- Walnuts.
- Omega-6 fatty acids may help:
- Control your blood sugar
- Reduce your risk for diabetes
- Lower your blood pressure
- Sources of omega-6 fatty acids include:
- Corn oil.
- Cottonseed oil.
- Peanut oil.
- Soybean oil.
- Sunflower oil.
- Omega-3 fatty acids are good for your heart in several ways. They help:
Figure 1. Unsaturated fat foods

Figure 2. Monounsaturated Fat Structure
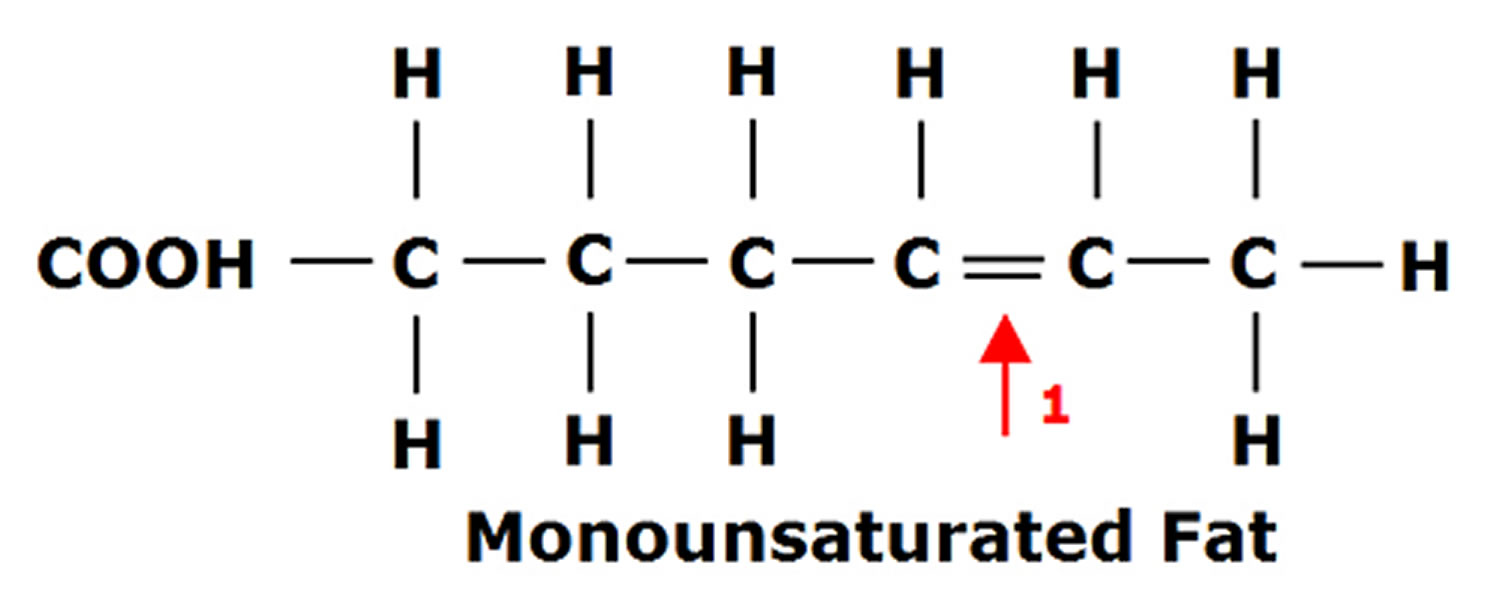
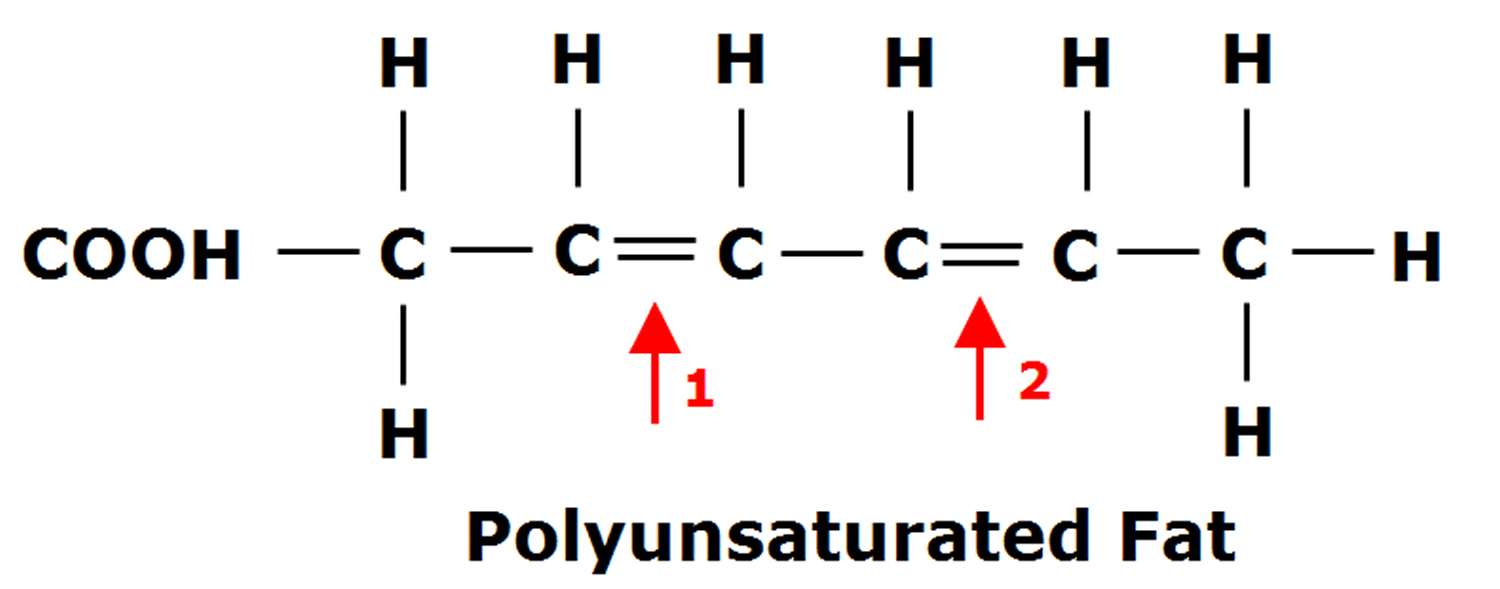
Figure 3. Polyunsaturated Fatty Acids Structure
What are the types of fat?
There are 4 main types of fats:
- Unsaturated fats are those that are liquid at room temperature. The two kinds of unsaturated fats are monounsaturated fat and polyunsaturated fat. Both of these unsaturated fats are typically liquid at room temperature. Unsaturated fats are in fish, such as salmon, trout and herring, and plant-based foods such as avocados, olives and walnuts. Liquid vegetable oils, such as soybean oil, corn oil, safflower oil, canola oil, olive oil, peanut oil, canola oil and sunflower oil, also contain unsaturated fats. Eaten in moderation, both kinds of unsaturated fats may help improve your blood cholesterol when used in place of saturated and trans fats. You want to include as many unsaturated fats in your diet because they can decrease bad cholesterol, contain high amounts of antioxidants such as Vitamin E, and contain essential omega-3 and omega-6 fatty acids. Unsaturated fats are typically classified by how many hydrogen bonds they have in their structure: either 1 (mono) or two or more (poly).
- Monounsaturated fats. Monounsaturated fat is a type of unsaturated fat. Monounsaturated fats are liquid at room temperature but start to harden when chilled. Monounsaturated fats is one of the healthy fats, along with polyunsaturated fat. Monounsaturated fats are good for your health in several ways:
- Monounsaturated fats can help lower your LDL (bad) cholesterol level. Cholesterol is a soft, waxy substance that can cause clogged, or blocked, arteries (blood vessels). Keeping your LDL level low reduces your risk for heart disease and stroke.
- Eating plant foods high in monounsaturated fats, particularly extra virgin olive oil and tree nuts, may benefit heart health and blood sugar regulation. Monounsaturated fats from plants may lower bad cholesterol and raise good cholesterol. They also may improve the control of blood sugar levels. Replacing saturated fats with monounsaturated fats in your diet may lower the level of bad cholesterol and triglycerides in your blood. Triglycerides are fat cells that circulate in the bloodstream and are stored in the body’s fat cells. A high level of triglycerides in the blood increases the risk of diseases of the heart and blood vessels.
- Monounsaturated fats help develop and maintain your cells.
- Monounsaturated fats are found in plant foods, such as nuts, avocados, and vegetable oils. Monounsaturated fats are found in red meats and dairy products. About half the fats in these foods are saturated and half monounsaturated. Many plants and plant oils are high in monounsaturated fats but low in saturated fats. These include:
- Oils from olives, peanuts, canola seeds, safflower seeds, and sunflower seeds.
- Avocadoes.
- Pumpkin seeds.
- Sesame seeds.
- Almonds.
- Cashews.
- Peanuts and peanut butter.
- Pecans.
- Polyunsaturated fats. Polyunsaturated fat is a type of unsaturated fat. Polyunsaturated fats are liquid at room temperature but start to harden when chilled. Polyunsaturated fats include omega-3 and omega-6 fats. These are essential fatty acids that your body needs for brain function and cell growth. Your body does not make essential fatty acids, so you must get them from food. Polyunsaturated fats can help lower your LDL (bad) cholesterol. Cholesterol is a soft, waxy substance that can cause clogged or blocked arteries (blood vessels). Having low LDL cholesterol reduces your risk for heart disease. Polyunsaturated fats is one of the healthy fats, along with monunsaturated fat. Polyunsaturated fat is found in plant and animal foods, such as salmon, vegetable oils, and some nuts and seeds.
- Omega-3 fatty acids are good for your heart in several ways. They help:
- Reduce triglycerides, a type of fat in your blood
- Reduce the risk of developing an irregular heartbeat (arrhythmia)
- Slow the buildup of plaque, a substance comprising fat, cholesterol, and calcium, which can harden and clog your arteries
- Slightly lower your blood pressure
- Sources of omega-3 fatty acids include:
- Fish such as salmon, anchovies, mackerel, herring, sardines and tuna.
- Oils from canola seeds, soybeans, walnuts and flaxseed.
- Soybeans.
- Chia seeds.
- Flaxseed.
- Walnuts.
- Omega-6 fatty acids may help:
- Control your blood sugar
- Reduce your risk for diabetes
- Lower your blood pressure
- Sources of omega-6 fatty acids include:
- Corn oil.
- Cottonseed oil.
- Peanut oil.
- Soybean oil.
- Sunflower oil.
- Omega-3 fatty acids are good for your heart in several ways. They help:
- Saturated fats. Saturated fats are those that are solid at room temperature. Examples include margarine, butter, whole fat dairy products, the fat marbling in meats, and coconut oil. Saturated fats don’t need to be avoided entirely, but diets high in saturated fats can increase bad cholesterol and triglycerides, increasing the risk for heart disease. The Dietary Guidelines for Americans suggest that less than 10% of calories a day should be from saturated fats. The American Heart Association recommends that saturated fats only make up 5 to 6% of your daily calories. For a 2,000 calorie diet, that is a total of 100 calories, or 11 grams a day. Foods high in saturated fats include:
- Foods baked or fried using saturated fats.
- Meats, including beef, lamb, pork as well as poultry, especially with skin.
- Lard.
- Dairy products like butter and cream.
- Whole or 2% milk.
- Whole-milk cheese or yogurt.
- Oils from coconuts, palm fruits, or palm kernels.
- Trans fats. Trans fatty acids are unhealthy fats that form when vegetable oil goes through a process called hydrogenation. This leads the fat to harden and become solid at room temperature. Hydrogenated fats, partially hydrogenated oils (PHOs) or “trans fats,” are often used to keep some foods fresh for a long time. Trans fats are unsaturated fats that are artificially turned into saturated fats and increase heart disease and stroke risk by raising bad LDL cholesterol and decreasing good HDL cholesterol levels. High LDL (bad) cholesterol along with low HDL (good) cholesterol levels can cause cholesterol to build up in your arteries (blood vessels). This increases your risk for heart disease and stroke. Trans fats have also been known to increase the risk of developing type 2 diabetes. Trans fats are most commonly found in fried foods, frozen baked products such as pizza, non-dairy coffee creamers, vegetable shortenings, some margarines, crackers, cookies, snack foods, and other foods made with or fried in partially hydrogenated oils (PHOs). Because of the health risks from trans fats, the United States Food and Drug Administration (FDA) has banned food manufacturers from adding partially hydrogenated oils (PHOs) to foods. Although the food industry has greatly reduced the use of trans fat in recent years, trans fat may still be found in many fried, packaged, or processed foods. There are very small amounts of naturally occurring trans fat in meats and dairy from grazing animals, such as cows, sheep and goats. You should avoid foods made with hydrogenated and partially hydrogenated oils (such as hard butter and margarine). They may contain high levels of trans fatty acids. It is important to read nutrition labels on foods. This will help you know what kinds of fats, and how much, your food contains.
Cutting down on foods and drinks that are high in saturated and trans fats will help to keep your heart healthy and maintain your weight. You can replace some of them with unsaturated fats.
Unsaturated fat vs Saturated fat
Remember, though, all types of fat are high in calories, so eating too much can lead to weight gain. Being overweight or obese is a risk factor for heart and circulatory disease, and many other diseases.
Foods high in saturated fats include:
- Foods baked or fried using saturated fats.
- Meats, including beef, lamb, pork as well as poultry, especially with skin.
- Lard.
- Ghee.
- Suet.
- Dairy products like butter and cream.
- Whole or 2% milk.
- Whole-milk cheese, cream or yogurt.
- Oils from coconuts, palm fruits, or palm kernels.
- Ice cream
- Coconut and coconut oil
- Palm oil
- Palm kernel oil
- Some baked and fried foods
- Processed and fatty meats like sausages, ham, burgers and bacon.
Unsaturated fats are those that are liquid at room temperature. The two kinds of unsaturated fats are monounsaturated fat and polyunsaturated fat. Both of these unsaturated fats are typically liquid at room temperature. Unsaturated fats are in fish, such as salmon, trout and herring, and plant-based foods such as avocados, olives and walnuts. Liquid vegetable oils, such as soybean oil, corn oil, safflower oil, canola oil, olive oil, peanut oil, canola oil and sunflower oil, also contain unsaturated fats. Eaten in moderation, both kinds of unsaturated fats may help improve your blood cholesterol when used in place of saturated and trans fats. You want to include as many unsaturated fats in your diet because they can decrease bad cholesterol, contain high amounts of antioxidants such as Vitamin E, and contain essential omega-3 and omega-6 fatty acids. Unsaturated fats are typically classified by how many hydrogen bonds they have in their structure: either 1 (mono) or two or more (poly).
Figure 4. Saturated fat foods

Polyunsaturated fat vs Monounsaturated fat
Polyunsaturated fats (polyunsaturated fatty acids or PUFAs) have two or more carbon-to-carbon double bond. The result is that it has two fewer hydrogen atoms than a saturated fat and a bend at the double bond. This structure keeps polyunsaturated fats liquid at room temperature.Polyunsaturated fatty acids (PUFAs) are found in high concentrations in sunflower, corn, soybean, flaxseed oils, walnuts, flax seeds, hemp seeds, pine nuts, sesame, cottonseed oils, pumpkin seeds and fish.
Polyunsaturated fatty acids (PUFAs) can be further subdivided on the basis of the location of the first carbon-to-carbon double bond relative to the methyl terminus of the chain. For example, Omega-3 and Omega-6 fatty acids are two of the most biologically significant polyunsaturated fatty acid classes, and have their first carbon-to-carbon double bond on either the third or sixth carbon from the chain terminus, respectively. The final carbon in the fatty acid chain is also known as the omega carbon, hence the common reference to these fatty acids as omega-3 or omega-6 PUFAs. The distinction between omega-6 and omega-3 fatty acids is based on the location of the first carbon-to-carbon double bond, counting from the methyl end of the fatty acid molecule (see Figure 5). Omega-6 fatty acids are represented by Linoleic acid (LA) (18:2ω-6) and Arachidonic acid (AA) (20:4ω-6) and Omega-3 fatty acids by Alpha-linolenic acid (ALA) (18:3ω-3), Eicosapentaenoic acid (EPA) (20:5ω-3) and Docosahexaenoic acid (DHA) (22:6ω-3).
Long-chain Omega-3 and Omega-6 PUFAs are synthesized from the essential fatty acids: alpha-linolenic acid (ALA) and linoleic acid (LA), respectively. Basic structures of these two parent PUFAs are shown in Figure 2 and Figure 3. An essential fatty acid cannot be made by your body and must be obtained through dietary sources. Animals and humans have the capacity to breakdown essential fatty acids to long-chain derivatives. Because the Omega-6 and Omega-3 pathways compete with one another for enzyme activity, the ratio of Omega-6 to Omega-3 PUFAs is very important to human health. An overabundance of fatty acids from one family will limit the metabolic production of the longer chain products of the other. The typical Western diet provides Omega-6 and Omega-3 PUFAs in a ratio ranging from 8:1 to 25:1 1, values in severe contrast with the recommendations from national health agencies of approximately 4:1 2. Lowering the Omega-6:Omega-3 ratio would reduce competition for the enzymes and facilitate the metabolism of more downstream products of Alpha-linolenic acid (ALA) (18:3ω-3).
Key facts
- There is convincing evidence that Linoleic acid (LA) and Alpha-linolenic acid (ALA) are essential fatty acids since they cannot be synthesized by humans.
- The acceptable range for total Polyunsaturated fatty acids (PUFAs) (Omega-6 fatty acids and Omega-3 fatty acids) is between 6 and 11% of total calories. The adequate intake to prevent deficiency is 2.5 to 3.5% of total calories. Therefore, the recommended range for Polyunsaturated fatty acids (PUFAs) is 6 to 11% of total calories.
- There is convincing evidence that replacing saturated fats with Polyunsaturated fatty acids (PUFAs) decreases the risk of coronary heart disease.
- There is convincing and sufficient evidence from experimental studies to set an acceptable intake to meet essential fatty acid needs for Linoleic acid (LA) and Alpha-linolenic acid (ALA) consumption.
- There is possible evidence that Polyunsaturated fatty acids (PUFAs) affect the risk of alterations in indices related to the metabolic syndrome.
- There is possible evidence of a relationship between Polyunsaturated fatty acids (PUFAs) intake and reduced risk of diabetes.
- There is insufficient evidence for establishing any relationship between Polyunsaturated fatty acids (PUFAs) consumption and cancer.
- There is insufficient evidence for establishing relationships between Polyunsaturated fatty acids (PUFAs) consumption and body weight and percent adiposity.
Mammalian cells cannot convert omega-6 to omega-3 fatty acids because they lack the converting enzyme, omega-3 desaturase. Omega-6 and omega-3 fatty acids are not interconvertible, are metabolically and functionally distinct, and often have important opposing physiological effects, therefore their balance in the diet is important 3.
This study showed a balanced omega-6/omega-3 ratio 1–2/1 is one of the most important dietary factors in the prevention of obesity, along with physical activity. A lower omega-6/omega-3 ratio should be considered in the management of obesity 3.
Because most diets are already very rich in omega-6 PUFAs, greater focus needs to be placed on incorporating omega-3 PUFAs into the diet. Dietary sources of omega-3 PUFAs are readily available but in limited quantities. Many foods contain alpha-linolenic acid (ALA), including certain vegetable oils, dairy products, flaxseed, walnuts and vegetables 4. Fatty fish, such as mackerel, herring and salmon, provide an excellent source of the long-chain derivatives of ALA, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) 2.
Omega-3 fatty acids are a type of polyunsaturated fats found in seafood, such as salmon, trout, herring, tuna, and mackerel, and in flax seeds and walnuts. EPA and DHA are long chain omega-3 fatty acids found in seafood. Omega-3 fats are one important type of polyunsaturated fat. Polyunsaturated fats are essential fats. That means your body can’t produce these and they’re required for normal body functions. So you must get them from food. Polyunsaturated fats are used to build cell membranes and the covering of nerves. They are needed for blood clotting, muscle movement, and inflammation.
A polyunsaturated fat has two or more double bonds in its carbon chain. There are two main types of polyunsaturated fats: omega-3 fatty acids and omega-6 fatty acids. The numbers refer to the distance between the beginning of the carbon chain and the first double bond. Both types offer health benefits.
Polyunsaturated fatty acids (PUFAs) can be further subdivided on the basis of the location of the first carbon-to-carbon double bond relative to the methyl terminus of the chain. For example, omega-3 and omega-6 fatty acids are two of the most biologically significant polyunsaturated fatty acid classes, and have their first carbon-to-carbon double bond on either the third or sixth carbon from the chain terminus, respectively. The final carbon in the fatty acid chain is also known as the omega carbon, hence the common reference to these fatty acids as omega-3 or omega-6 PUFAs.
Eating polyunsaturated fats in place of saturated fats or highly refined carbohydrates reduces harmful LDL cholesterol and improves the cholesterol profile. It also lowers triglycerides.
We don’t eat nearly enough omega-3, which can reduce our risk for heart disease and cancer. Good sources of omega-3 fatty acids include fatty fish such as salmon, mackerel, and sardines, all green leafy vegetables, flaxseeds, walnuts, canola oil, and unhydrogenated soybean oil.
Omega-3 fatty acids may help prevent and even treat heart disease and stroke. In addition to reducing blood pressure, raising HDL, and lowering triglycerides, polyunsaturated fats may help prevent lethal heart rhythms from arising. Evidence also suggests they may help reduce the need for corticosteroid medications in people with rheumatoid arthritis. Studies linking omega-3s to a wide range of other health improvements, including reducing risk of dementia, are inconclusive, and some of them have major flaws, according to a systematic review of the evidence by the Agency for Healthcare Research and Quality.
Omega-6 fatty acids have also been linked to protection against heart disease. Foods rich in linoleic acid and other omega-6 fatty acids include vegetable oils such as safflower, soybean, sunflower, walnut, and corn oils.
The latest research on nuts by the Harvard School of Public Health found that women who reported eating a half serving of peanut butter or a full serving of nuts five or more times a week showed as much as a 30% reduced risk of developing type 2 diabetes. And eating other nuts, like almonds, walnuts, and pecans, have been shown to have heart healthy benefits, including lowering “bad” LDL cholesterol. (Remember, walnuts are also a source of omega-3.)
Figure 5. Omega-3 fatty acids (ALA, EPA & DHA) and Omega-6 fatty acids (LA & AA) structure
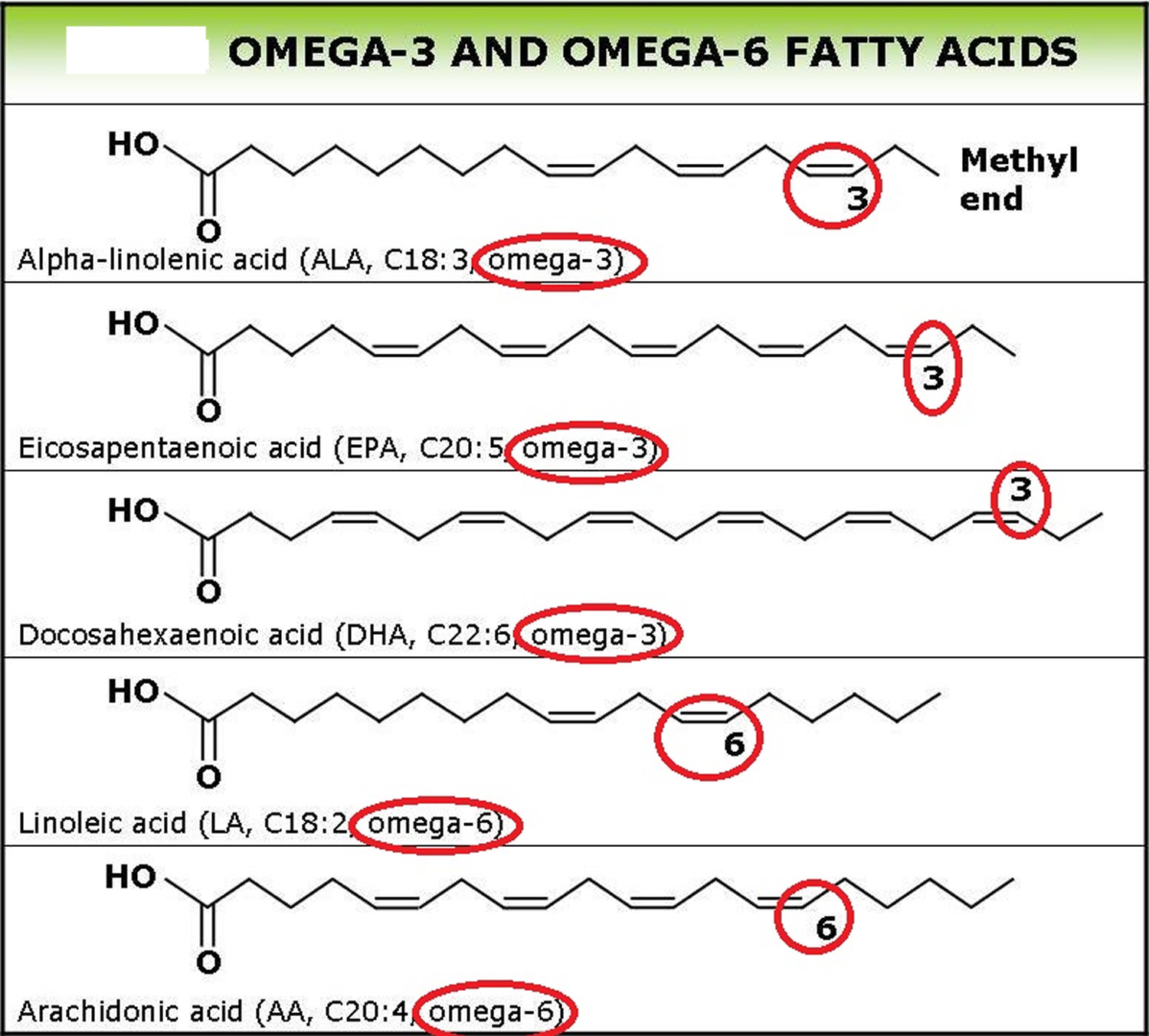
Footnotes: Omega-6 fatty acids are represented by Linoleic acid (LA) (18:2ω-6) and Arachidonic acid (AA) (20:4ω-6) and Omega-3 fatty acids by Alpha-linolenic acid (ALA) (18:3ω-3), Eicosapentaenoic acid (EPA) (20:5ω-3) and Docosahexaenoic acid (DHA) (22:6ω-3).
Monounsaturated fat
Monounsaturated fats (monounsaturated fatty acids or MUFAs) have a single carbon-to-carbon double bond. The result is that it has two fewer hydrogen atoms than a saturated fat and a bend at the double bond. This structure keeps monounsaturated fats liquid at room temperature. Eating food that has more monounsaturated fat (or “healthy fat”) instead of saturated fat (like butter) may help lower cholesterol and reduce heart disease risk. Research also shows that monounsaturated fats may benefit insulin levels and blood sugar control, which can be especially helpful if you have type 2 diabetes. However, monounsaturated fat has the same number of calories (9 calories or 37kJ) as other types of fat and may contribute to weight gain if you eat too much of it. Good sources of monounsaturated fats are olive oil, peanut oil, canola oil, avocados, most nuts, as well as high-oleic safflower and sunflower oils. The carbon-carbon double bond found in monounsaturated or polyunsaturated fatty acids can exist in the cis or trans configuration. When the two hydrogen atoms are on opposite sides of the double bond, the configuration is called trans. When the hydrogen atoms are on the same side of the double bond, the configuration is called cis. Monounsaturated fats (monounsaturated fatty acids) are found in high concentrations in olive oil, peanut oil, canola, avocados, almonds, safflower oils, hazelnuts, pecans, pumpkin seeds and sesame seeds and most nuts. Monounsaturated fats also are part of most animal fats such as fats from chicken, pork, beef, and wild game. When you dip your bread in olive oil at an Italian restaurant, you’re getting mostly monounsaturated fat.
The most common cis-configured monounsaturated fats (monounsaturated fatty acids or MUFAs) in daily nutrition is oleic acid (18:1 n-9), followed by palmitoleic acid (16:1 n-7), and vaccenic acid (18:1 n-7). Moreover, oleic acid represents the topmost monounsaturated fats (monounsaturated fatty acids or MUFAs) provided in the diet (~90% of all MUFAs) 5. The major trans-configured monounsaturated fats (monounsaturated fatty acids or MUFAs) is elaidic acid (trans 18:1 n-9). Some MUFA—such as mystrioleic (14:1 n-5), gondoic (20:1 n-9), erucic (22:1 n-9) and nervonic (24:1 n-9) acid—are synthesized in minor concentrations endogenously using other monounsaturated fats (monounsaturated fatty acids or MUFAs) as precursors 6.
Key facts
- There is convincing evidence that replacing carbohydrates with monounsaturated fats (monounsaturated fatty acids or MUFA) increases HDL “good” cholesterol concentrations.
- There is convincing evidence that replacing saturated fats (C12:0–C16:0) with monounsaturated fats reduces LDL “bad” cholesterol concentration and total/HDL cholesterol ratio.
- There is possible evidence that replacing carbohydrates with monounsaturated fats improves insulin sensitivity.
- There is insufficient evidence for establishing a relationship between monounsaturated fats consumption and chronic disease end points such as coronary heart disease or cancer.
- There is insufficient evidence for establishing a relationship between monounsaturated fats consumption and body weight and percent adiposity.
- There is insufficient evidence for establishing a relationship between monounsaturated fats intake and risk of diabetes.
What kind of fats are the healthier?
Unsaturated fats are those that are liquid at room temperature and can have beneficial effect on your heart. The two kinds of unsaturated fats are monounsaturated fat and polyunsaturated fat. Both of these unsaturated fats are typically liquid at room temperature. Unsaturated fats are in fish, such as salmon, trout and herring, and plant-based foods such as avocados, olives and walnuts. Liquid vegetable oils, such as soybean oil, corn oil, safflower oil, canola oil, olive oil, peanut oil, canola oil and sunflower oil, also contain unsaturated fats. Eaten in moderation, both kinds of unsaturated fats may help improve your blood cholesterol when used in place of saturated and trans fats. You want to include as many unsaturated fats in your diet because they can decrease bad cholesterol, contain high amounts of antioxidants such as Vitamin E, and contain essential omega-3 and omega-6 fatty acids. Unsaturated fats are typically classified by how many hydrogen bonds they have in their structure: either 1 (mono) or two or more (poly). Polyunsaturated fats are distinguished from saturated and monounsaturated fatty acids by the presence of two or more double bonds between carbons within the fatty acid chain. Polyunsaturated fatty acids (PUFAs) are frequently designated by their number of carbon atoms and double bonds. Alpha-linolenic acid (ALA), for example, is known as C18:3n-3 because it has 18 carbons and 3 double bonds and is an omega-3 (n-3) fatty acid. Similarly, eicosapentaenoic acid (EPA) is known as C20:5n-3 and docosahexaenoic acid (DHA) as C22:6n-3 7. Omega-6 fatty acids (omega-6s) have a carbon–carbon double bond that is six carbons away from the methyl end of the fatty acid chain. Linoleic acid (C18:2n-6) and arachidonic acid (C20:4n-6) are two of the major omega-6s 7.
Vegetable oils are the healthy choice for frying and baking, and plant-based spreads, avocados or nut butters for sandwiches, toast and potatoes. These are healthier choices than butter or lard. Check food labels and compare the fat content in different products to help you choose ones that are lower in saturated fats. But remember, while this will help to lower your cholesterol level, you need to look at your whole diet to reduce overall risk. Many factors affect heart disease risk, not one food or nutrient alone. The Mediterranean diet is associated with reducing your risk of heart and circulatory disease. It includes plenty of fruit and vegetables, pulses, fish, nuts and seeds, and less butter, meat, full-fat dairy products and high-fat snacks, so it’s naturally higher in unsaturated fats and lower in saturated fats.
Polyunsaturated fats
Polyunsaturated fats also called polyunsaturated fatty acids (PUFAs) can help reduce bad cholesterol levels in your blood, which can lower your risk of heart disease and stroke 8. Polyunsaturated fats also provide nutrients to help develop and maintain your body’s cells. Oils rich in polyunsaturated fats also provide vitamin E, an important antioxidant vitamin. Oils rich in polyunsaturated fats also provide essential fats that your body needs but can’t produce itself, including omega-3 and omega-6 fatty acids. You must get essential fats through food. Omega-6 and omega-3 fatty acids are important for many functions in your body.
Omega-3 fatty acids (omega-3s) have a carbon–carbon double bond located three carbons from the methyl end of the chain. Omega-3s, sometimes referred to as n-3s, are present in certain foods such as flaxseed and fish as well as dietary supplements such as fish oil. Several different omega-3 fatty acids exist, but the majority of scientific research focuses on three: alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) 7. Alpha-linolenic acid (ALA) contains 18 carbon atoms, whereas eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) are considered long-chain omega-3s because eicosapentaenoic acid (EPA) contains 20 carbons and docosahexaenoic acid (DHA) contains 22 7.
The human body can only form carbon–carbon double bonds after the ninth carbon from the methyl end of a fatty acid 9. Therefore, alpha-linolenic acid (ALA) and linoleic acid are considered essential fatty acids, meaning that they must be obtained from your diet 10. Alpha-linolenic acid (ALA) can be converted into eicosapentaenoic acid (EPA) and then to docosahexaenoic acid (DHA), but the conversion which occurs primarily in your liver is very limited, with reported rates of less than 15% 11. Therefore, consuming eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) directly from foods and/or dietary supplements is the only practical way to increase levels of these fatty acids in your body 7.
Alpha-linolenic acid (ALA) is present in plant oils, such as flaxseed, soybean, and canola oils 11. Eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) are present in fish, fish oils, and krill oils, but they are originally synthesized by microalgae at the base of the marine food chain, not by the fish. As microalgae move up the food chain, fish acquire the omega-3s and accumulate them in their tissues 11.
After ingestion, dietary fats are brokendown in your intestines 9. The hydrolysis products—monoglycerides and free fatty acids—are then incorporated into bile-salt– containing micelles and absorbed into enterocytes, largely by passive diffusion. The process is efficient, with an absorption rate of about 95%, which is similar to that of other ingested fats 9. Within intestinal cells, free fatty acids are primarily incorporated into chylomicrons and enter the circulation via the lymphatic system 9, 12. Once in your bloodstream, lipoprotein particles circulate within your body, delivering lipids to various organs for subsequent oxidation, metabolism, or storage in fat tissue 12, 13.
Omega-3 fatty acids play important roles in your body as components of the phospholipids that form the structures of cell membranes 13. Docosahexaenoic acid (DHA), in particular, is especially high in the retina, brain, and sperm 13, 11, 14. In addition to their structural role in cell membranes, omega-3 fatty acids along with omega-6 fatty acids provide energy for your body and are used to form eicosanoids. Eicosanoids are signaling molecules that have similar chemical structures to the fatty acids from which they are derived; they have wide-ranging functions in the body’s cardiovascular, pulmonary, immune, and endocrine systems 15, 10.
The eicosanoids made from omega-6 fatty acids are generally more potent mediators of inflammation, vasoconstriction, and platelet aggregation than those made from omega-3 fatty acids, although there are some exceptions 11, 16. Because both classes of omega-6 and omega-3 fatty acids compete for the same desaturation enzymes, alpha-linolenic acid (ALA) is a competitive inhibitor of linoleic acid metabolism and vice versa 17. Similarly, eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) can compete with arachidonic acid for the synthesis of eicosanoids. Therefore, higher concentrations of eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) than arachidonic acid tip the eicosanoid balance toward less inflammatory activity 18.
Some researchers propose that the relative intakes of omega-6s and omega-3s, the omega-6/omega-3 ratio, may have important implications for the cause of many chronic diseases, such as cardiovascular disease (heart and blood vessel disease) and cancer 18, but the optimal omega-6/omega-3 ratio—if any—has not been defined 19. Others have concluded that such ratios are too nonspecific and are insensitive to individual fatty acid levels 20, 21, 22. Most agree that raising eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) blood levels is far more important than lowering linoleic acid or arachidonic acid levels.
Nontropical vegetable oils high in polyunsaturated fat include:
- Canola oil
- Corn oil
- Soybean oil
- Sunflower oil.
Foods high in polyunsaturated fats include:
- Fatty, or oily fish, including anchovies, herring, mackerel, black cod, salmon, sardines, bluefin tuna, whitefish, striped bass and cobia. These fish are high in omega-3 fatty acids.
- Some nuts and seeds, including walnuts, flaxseeds and sunflower seeds.
- Tofu/soybeans.
Figure 6. Polyunsaturated fat foods

Monounsaturated fats
Monounsaturated fats also called monounsaturated fatty acids (MUFAs) can also help reduce bad cholesterol levels in your blood, which can lower your risk of heart disease and stroke 23, 24. Monounsaturated fats also provide nutrients to help develop and maintain your body’s cells. Oils rich in monounsaturated fats also provide vitamin E, an important antioxidant vitamin. Olive oil is a type of oil that contains monounsaturated fats. For good health, consume foods that contain monounsaturated fats in place of those that contain saturated fats and/or trans fats. Oils that contain monounsaturated fats are typically liquid at room temperature but start to turn solid when chilled.
Nontropical vegetable oils high in monounsaturated fats include:
- Olive oil
- Canola oil
- Peanut oil
- Safflower oil
- Sesame oil
Foods high in monounsaturated fats include:
- Avocados.
- Peanut butter.
- Some nuts and seeds, including almonds, hazelnuts, pecans, pumpkin seeds and sesame seeds.
Figure 7. Monounsaturated fat foods

What are Healthy fats?
Healthy fats include:
- Monounsaturated fats
- Polyunsaturated fats (omega-3 and omega-6).
The healthier fats are unsaturated fats. They can be found in sunflower oil, safflower oil, peanut and olive oils, poly- and mono-unsaturated margarine spreads, nuts, seeds and avocado. These are much better for you than the saturated fat found in butter, cream, fatty meats, sausages, biscuits, cakes and fried foods.
Foods that contain healthy monounsaturated fats include:
- Avocados and their oils/spreads
- Unsalted nuts such as almonds, cashews and peanuts and their butters/spreads
- Olives and their oils/spreads
- Cooking oils made from plants or seeds, including: olive, canola, peanut, sunflower, soybean, sesame and safflower.
Foods that contain healthy polyunsaturated fats (omega-3 and omega-6) include:
- Oily fish like salmon, mackerel and sardines
- Tahini (sesame seed spread)
- Linseed (flaxseed) and chia seeds
- Soybean, sunflower, safflower, canola oil and margarine spreads made from these oils
- Pine nuts, walnuts and brazil nuts.
It is important to choose foods with the healthiest type of fat such as avocados, olives, nuts and seeds, and use healthy oils for cooking, for example, olive, canola, sunflower, peanut and soybean oil.
Reduce the amount of highly processed food you eat such as baked goods including cakes, biscuits and pastries, along with processed meat, and fried and takeaway foods. These foods are high in saturated and trans fats, added sugar and salt, and are not part of a heart-healthy eating pattern. Try to have these foods only sometimes and in small amounts.
Many Americans eat more fat than they need, which can lead to weight gain and heart disease.
What are Unhealthy fats?
Unhealthy fats include:
- Saturated fat. Saturated fat and trans fat are ‘unhealthy’ fats. They can raise your ‘bad’ (non-HDL) cholesterol in your blood. Too much cholesterol can increase your risk of having:
- a stroke
- a heart attack
- vascular dementia.
- Trans fat. Trans fatty acids are unhealthy fats that form when vegetable oil goes through a process called hydrogenation. This leads the fat to harden and become solid at room temperature. Hydrogenated fats, partially hydrogenated oils (PHOs) or “trans fats,” are often used to keep some foods fresh for a long time. Trans fats are unsaturated fats that are artificially turned into saturated fats and increase heart disease and stroke risk by raising bad LDL cholesterol and decreasing good HDL cholesterol levels. High LDL (bad) cholesterol along with low HDL (good) cholesterol levels can cause cholesterol to build up in your arteries (blood vessels). This increases your risk for heart disease and stroke. Trans fats have also been known to increase the risk of developing type 2 diabetes. Trans fats are most commonly found in fried foods, frozen baked products such as pizza, non-dairy coffee creamers, vegetable shortenings, some margarines, crackers, cookies, snack foods, and other foods made with or fried in partially hydrogenated oils (PHOs). Because of the health risks from trans fats, the United States Food and Drug Administration (FDA) has banned food manufacturers from adding partially hydrogenated oils (PHOs) to foods. Although the food industry has greatly reduced the use of trans fat in recent years, trans fat may still be found in many fried, packaged, or processed foods. There are very small amounts of naturally occurring trans fat in meats and dairy from grazing animals, such as cows, sheep and goats. You should avoid foods made with hydrogenated and partially hydrogenated oils (such as hard butter and margarine). They may contain high levels of trans fatty acids. It is important to read nutrition labels on foods. This will help you know what kinds of fats, and how much, your food contains.
Foods rich in unhealthy fats include:
- Animal fats including butter, ghee and lard along with the visible fat/skin on meat
- Hydrogenated plant oils like copha, vegetable shortening and some margarines
- Coconut oil
- Processed foods such as baked goods (cakes, biscuits and pastries), processed meat ( bacon, sausages, salami) and fried and takeaway foods.
Replace foods rich in saturated and trans fats with foods rich in healthy unsaturated fats as part of a healthy diet.
It is important to choose foods with the healthiest type of fat such as avocados, olives, nuts and seeds, and use healthy oils for cooking, for example, olive, canola, sunflower, peanut and soybean oil.
Reduce the amount of highly processed food you eat such as baked goods including cakes, biscuits and pastries, along with processed meat, and fried and takeaway foods. These foods are high in saturated and trans fats, added sugar and salt, and are not part of a heart-healthy eating pattern. Try to have these foods only sometimes and in small amounts.
Many Americans eat more fat than they need, which can lead to weight gain and heart disease.
How much fat do I need?
To prevent any fatty acid deficiencies it is recommended that you consume at minimum 1g of fat per kg of body weight per day. According to the Dietary Guidelines for Americans 25, fats should make up 20 to 35 percent of your total daily calorie intake (for adults) with most fats coming from sources of polyunsaturated fats and monounsaturated fats, such as fish, nuts, and vegetable oils. The Dietary Guidelines for Americans also recommend getting less than 10 percent of your calories from saturated fats and keeping trans fat consumption as low as possible for general health and the prevention of chronic disease, including cancer and heart disease 25. The American Heart Association recommends aiming for a dietary pattern that achieves less than 6% of total calories from saturated fat 26, 27. For example, if you need about 2,000 calories a day, no more than 120 calories should come from saturated fat. That’s about 13 grams or less of saturated fat per day 26. Many Americans eat more fat than they need, which can lead to weight gain and heart disease. The nutrition labels on your food’s packaging will show you the amount of total fat and saturated fat you are eating. Looking at the amount of saturated fat in your food will help you keep to the recommended daily intake.
Fat needs will vary by individual and will depend largely on your body composition goals and body types. For example, dietary fat recommendations are slightly higher in competitive athletes than non-athletes to promote health, maintain healthy hormone function, and maintain energy balance. Typical recommendations for athletes are 30 to 50% of total energy intake. You need to eat some fat even when you are trying to lose weight. For those attempting to lose body fat, 0.5 to 1 fat per kg of body weight per day should be consumed per day to avoid essential fatty acid deficiency. For healthy children ages 1 to 3, ages 4 to 18, and adults, approximately 30 to 40%, 25 to 15%, and 20 to 35% of daily energy intake should come from fat, respectively 28. The human body needs small amounts (3 to 6 grams) of essential fatty acids (Omega-6 fatty acids and Omega-3 fatty acids). Fat is important for many body processes. Fat helps your body absorb nutrients and move nutrients around your body. Some fat is necessary as a carrier for the fat-soluble vitamins A, D, E, and K. Fat is the main source of energy storage in your body, fat contributes to cellular structure and function, fat keeps you warm, and protects your organs 29, 30, 31. Fat also helps with hormone production. Therefore your diet should not be devoid of fat. However, because fat is calorically dense (1 gram of fat has 9 calories of energy), it is often decreased on weight-loss diets to reduce energy intake.
Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are omega-3 fatty acids found in varying amounts in seafood such as cold-water fish like salmon, tuna, herring, and mackerel, as well as in fish oil supplements and seaweed. Eating 8 ounces per week of seafood may help reduce the risk for heart disease.
Approximately 5 to 10% of your daily fat energy intake should consist of Omega−6 fatty acids (linoleic acid) and 0.6 to 1.2% of Omega−3 fatty acids (alpha-linolenic acid, eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) 32. Both omega−6 fatty acids (linoleic acid) and omega−3 fatty acids (alpha-linolenic acid, eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) are considered essential fatty acids, meaning that they must be obtained from your diet 10. Apha-linolenic acid (ALA) can be converted into eicosapentaenoic acid (EPA) and then to docosahexaenoic acid (DHA), but the conversion which occurs primarily in your liver is very limited, with reported rates of less than 15% 11, 33. Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are essential fatty acids, meaning the body can’t produce them and they must come from your diet 9. Therefore, consuming eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) directly from foods and/or dietary supplements is the only practical way to increase levels of these fatty acids in your body.
Some researchers propose that the relative intakes of omega-6s and omega-3s, the omega-6/omega-3 ratio, may have important implications for the cause of many chronic diseases, such as heart and blood vessels disease (cardiovascular disease) and cancer 17, but the optimal ratio, if any, has not been defined 34. Others have concluded that the omega-6/omega-3 ratios are too nonspecific and are insensitive to individual fatty acid levels 20, 21, 22.. Most agree that raising EPA and DHA blood levels is far more important than lowering linoleic acid or arachidonic acid levels 33.
For someone who weighs 150lbs (68kg), this would equate to 34-68g fat per day. Using both of these references you can calculate your daily fat needs:
To calculate your daily fat needs:
- Convert body weight in pounds to kilograms (round to the nearest 10th). Multiply weight in kilograms by 1.
Let’s look at an example:
- Convert pounds into kilograms 150lbs / 2.2 = 68.2kg
The recommended fat intake is 1 gram per kilogram of body weight per day
- 68.2kg (1g grams of fat per kilogram) = 68.2g of fat per day
Weight loss diets that are moderate to low in fat (20 to 30% of calories) are called “balanced deficit” diets because they maintain a reasonable balance among macronutrients similar to that recommended in MyPlate, DASH, and the Dietary Guidelines for Americans 25, 35. They tend to achieve most of the caloric deficit by reducing fat from the typical level in North American Diets of about 34% or more of calories to 20 to 30% fat, 15% protein, and 55 to 65% of calories from carbohydrates. Some examples of low fat diets are the Weight Watchers Diet (25% fat, 20% protein, and 55% carbohydrate, with 26 grams of dietary fiber), Jenny Craig, the National Cholesterol Education Program Step 1 diet (25% fat), diets based on the MyPlate, the DASH diet, the Shape up and Drop 10 diet of Shape Up! America and the Nutrisystem diet 36. Popular diet books using this approach include The Biggest Loser Diet, The Mayo Clinic Diet and The Engine 2 Die 36. These dietary patterns have been extensively reviewed and appear to be effective for weight reduction on low calorie diets for most individuals 36.
Very low-fat diets such as the Pritikin Diet 37, the Ornish Diet 38 and The Spark Solution Diet 39 have been advocated not only for weight reduction, but also for improving cardiovascular risk profiles. The Ornish Diet 38, which is very low in fat (13% of calories) and saturated fat, very high in carbohydrate (81% of calories) and very high in fiber (38 grams), is part of a program that includes nonsmoking, exercise and behavior modification. The Ornish Diet 38 was shown to reduce some cardiovascular risk factors in a limited long term study. For those who can adhere to the Ornish regime it may be helpful. However, it may not be appropriate for all populations, such as diabetics.
Are ‘low fat’ and ‘lighter’ foods better for me?
A lower fat option might not be better for you. For a food or drink to be labelled as:
- ‘lite’, ‘light’ or ‘lighter’, it must have at least 30 percent less fat than the original product
- ‘low fat’ or ‘reduced fat’, it must have less than 3g of fat per 100g and in some countries, the pack’s label will have the fat content colored green.
Sometimes, the fat will be replaced with more sugar or salt to make it taste like the original product. This might not make the lower fat option healthier.
Even if your food’s packaging says it’s lower fat, you might want to check its nutrition label. You can check the amount of ‘total fat’ and the amount of ‘saturated fat’ per serving on the label.
Are unsaturated fats bad?
No. Unsaturated fats are in fish, such as salmon, trout and herring, and plant-based foods such as avocados, olives and walnuts. Liquid vegetable oils, such as soybean oil, corn oil, safflower oil, canola oil, olive oil, peanut oil, canola oil and sunflower oil, also contain unsaturated fats. Eaten in moderation unsaturated fats may help improve your blood cholesterol when used in place of saturated and trans fats. You want to include as many unsaturated fats in your diet because they can decrease bad LDL cholesterol, contain high amounts of antioxidants such as Vitamin E, and contain essential omega-3 fatty acids and omega-6 fatty acids.
Foods high in unsaturated fat
There are two types of “good” unsaturated fats:
- Monounsaturated fats are found in high concentrations in:
- Olive, peanut, and canola oils
- Avocados and their oils/spreads
- Nuts such as almonds, hazelnuts, peanuts, pecans and their butters/spreads
- Seeds such as pumpkin and sesame seeds.
- Polyunsaturated fats (omega-3 and omega-6) are found in high concentrations in:
- Soybean, sunflower, safflower, canola oil, corn, flaxseed and margarine spreads made from these oils
- Pine nuts, walnuts and brazil nuts.
- Flax seeds
- Tahini (sesame seed spread)
- Linseed (flaxseed) and chia seeds
- Oily fish like salmon, mackerel and sardines
- Canola oil – though higher in monounsaturated fat, it’s also a good source of polyunsaturated fat.
It is important to choose foods with the healthiest type of fat such as avocados, olives, nuts and seeds, and use healthy oils for cooking, for example, olive, canola, sunflower, peanut and soybean oil.
Reduce the amount of highly processed food you eat such as baked goods including cakes, biscuits and pastries, along with processed meat, and fried and takeaway foods. These foods are high in saturated and trans fats, added sugar and salt, and are not part of a heart-healthy eating pattern. Try to have these foods only sometimes and in small amounts.
Many Americans eat more fat than they need, which can lead to weight gain and heart disease.
Table 1. Avocado nutrition facts
| Name | Average Amount | Unit |
|---|---|---|
| Proximates | ||
| Water | 67 | g |
| Energy (Atwater General Factors) | 223 | kcal |
| Energy (Atwater Specific Factors) | 206 | kcal |
| Nitrogen | 0.29 | g |
| Protein | 1.81 | g |
| Total lipid (fat) | 20.3 | g |
| Ash | 2.55 | g |
| Carbohydrates | ||
| Carbohydrate, by difference | 8.32 | g |
| Minerals | ||
| Calcium, Ca | 14 | mg |
| Iron, Fe | 0.61 | mg |
| Magnesium, Mg | 32.8 | mg |
| Phosphorus, P | 42 | mg |
| Potassium, K | 576 | mg |
| Sodium, Na | <2.49 | mg |
| Zinc, Zn | 0.46 | mg |
| Copper, Cu | 0.285 | mg |
| Manganese, Mn | 0.197 | mg |
| Vitamins and Other Components | ||
| Vitamin C, total ascorbic acid | <4 | mg |
| Vitamin B-6 | 0.167 | mg |
| Folate, total | 129 | µg |
Footnote: Hass avocado, peeled, raw.
[Source 40 ]Table 2. Olive oil (extra virgin) nutrition facts
| Name | Average Amount | Unit |
|---|---|---|
| Proximates | ||
| Total fat (NLEA) | 85 | g |
| Lipids: | ||
| Saturated fatty acids (SFA), total | 14 | g |
| SFA 14:0 | 0.012 | g |
| SFA 15:0 | 0.005 | g |
| SFA 16:0 | 11 | g |
| SFA 17:0 | 0.073 | g |
| SFA 18:0 | 2.35 | g |
| SFA 20:0 | 0.373 | g |
| SFA 21:0 | 0.013 | g |
| SFA 22:0 | 0.107 | g |
| SFA 24:0 | 0.056 | g |
| Monounsaturated fatty acids (MUFAs), total | 62.8 | g |
| MUFA 16:1 c | 0.934 | g |
| MUFA 18:1 c | 61.5 | g |
| MUFA 20:1 c | 0.25 | g |
| Polyunsaturated fatty acids (PUFAs), total | 8.23 | g |
| PUFA 18:2 c | 7.62 | g |
| PUFA 18:2 n-6 c,c | 7.62 | g |
| PUFA 18:3 c | 0.59 | g |
| PUFA 18:3 n-3 c,c,c (ALA) | 0.59 | g |
| PUFA 20:3 c | 0 | g |
| PUFA 20:3 n-6 | 0 | g |
| Phytosterols | ||
| Stigmasterol | 0.925 | mg |
| Campesterol | 5.15 | mg |
| Brassicasterol | 0 | mg |
| Beta-sitosterol | 114 | mg |
| Campestanol | 0 | mg |
| Beta-sitostanol | 2.31 | mg |
| Delta-5-avenasterol | 21 | mg |
| Phytosterols, other | 24.4 | mg |
Footnote: 100 ml extra virgin olive oil
[Source 41 ]Table 3. Peanut raw nutrition facts
| Name | Average Amount | Unit |
|---|---|---|
| Proximates | ||
| Water | 4.82 | g |
| Energy (Atwater General Factors) | 588 | kcal |
| Energy (Atwater Specific Factors) | 551 | kcal |
| Nitrogen | 4.25 | g |
| Protein | 23.2 | g |
| Total lipid (fat) | 43.3 | g |
| Ash | 2.2 | g |
| Carbohydrates | ||
| Carbohydrate, by difference | 26.5 | g |
| Fiber, total dietary | 8 | g |
| Minerals | ||
| Calcium, Ca | 49 | mg |
| Iron, Fe | 1.55 | mg |
| Magnesium, Mg | 180 | mg |
| Phosphorus, P | 380 | mg |
| Potassium, K | 636 | mg |
| Sodium, Na | 1 | mg |
| Zinc, Zn | 2.78 | mg |
| Copper, Cu | 0.46 | mg |
| Manganese, Mn | 1.68 | mg |
| Selenium, Se | 17.8 | µg |
Footnote: Per 100 g raw peanut
[Source 42 ]Table 4. Peanut butter nutrition facts
| Name | Average Amount | Unit |
|---|---|---|
| Proximates | ||
| Water | 1.1 | g |
| Energy (Atwater General Factors) | 632 | kcal |
| Energy (Atwater Specific Factors) | 589 | kcal |
| Nitrogen | 4.39 | g |
| Protein | 24 | g |
| Total lipid (fat) | 49.4 | g |
| Ash | 2.77 | g |
| Carbohydrates | ||
| Carbohydrate, by difference | 22.7 | g |
| Fiber, total dietary | 6.3 | g |
| Minerals | ||
| Calcium, Ca | 50 | mg |
| Iron, Fe | 1.85 | mg |
| Magnesium, Mg | 193 | mg |
| Phosphorus, P | 393 | mg |
| Potassium, K | 654 | mg |
| Sodium, Na | 221 | mg |
| Zinc, Zn | 3.06 | mg |
| Copper, Cu | 0.54 | mg |
| Manganese, Mn | 1.68 | mg |
| Selenium, Se | 20.2 | µg |
| Vitamins and Other Components | ||
| Thiamine | 0.121 | mg |
| Niacin | 17.2 | mg |
| Vitamin B-6 | 0.38 | mg |
| Biotin | 87.8 | µg |
| Folate, total | 97 | µg |
| Vitamin E (alpha-tocopherol) | 5.41 | mg |
| Vitamin K (phylloquinone) | <0.1 | µg |
| Lipids | ||
| Saturated fatty acids (SFA), total | 8.42 | g |
| SFA 16:0 | 4.11 | g |
| SFA 18:0 | 1.29 | g |
| SFA 20:0 | 0.683 | g |
| SFA 22:0 | 1.42 | g |
| SFA 24:0 | 0.824 | g |
| Monounsaturated fatty acids (MUFAs), total | 30.7 | g |
| MUFA 18:1 c | 29.8 | g |
| MUFA 20:1 c | 0.801 | g |
| MUFA 22:1 n-9 | 0.132 | g |
| Polyunsaturated fatty acids (PUFAs), total | 9.78 | g |
| PUFA 18:2 n-6 c,c | 9.73 | g |
| SFA 24:0 | 0.824 | g |
| Amino acids | ||
| Tryptophan | 0.229 | g |
| Threonine | 0.806 | g |
| Isoleucine | 0.92 | g |
| Leucine | 1.88 | g |
| Lysine | 0.951 | g |
| Methionine | 0.29 | g |
| Phenylalanine | 1.5 | g |
| Tyrosine | 1.06 | g |
| Valine | 1.12 | g |
| Arginine | 3.32 | g |
| Histidine | 0.676 | g |
| Alanine | 1.16 | g |
| Aspartic acid | 3.42 | g |
| Glutamic acid | 5.82 | g |
| Glycine | 1.69 | g |
| Proline | 1.24 | g |
| Serine | 1.42 | g |
| Hydroxyproline | 0.162 | g |
| Cysteine | 0.514 | g |
| Isoflavones | ||
| Daidzein | 11.5 | mg |
| Genistein | <0.013 | mg |
| Daidzin | 0.649 | mg |
| Genistin | 1.932 | mg |
| Glycitin | 0.41 | mg |
Footnote: Per 100 g creamy peanut butter.
[Source 43 ]Table 5. Peanut oil nutrition facts
| Name | Average Amount | Unit |
|---|---|---|
| Proximates | ||
| Total fat (NLEA) | 93.4 | g |
| Vitamins and Other Components | ||
| Vitamin E (alpha-tocopherol) | 15.2 | mg |
| Tocopherol, beta | <9.97 | mg |
| Tocopherol, gamma | 13.4 | mg |
| Tocopherol, delta | <10.8 | mg |
| Tocotrienol, alpha | <21.5 | mg |
| Tocotrienol, beta | <21.5 | mg |
| Tocotrienol, gamma | <21.5 | mg |
| Tocotrienol, delta | <21.5 | mg |
| Vitamin K (phylloquinone) | 4.3 | µg |
| Vitamin K (Dihydrophylloquinone) | 0 | µg |
| Vitamin K (Menaquinone-4) | 0 | µg |
| Lipids | ||
| Saturated fatty acids (SFA), total | 16.2 | g |
| SFA 4:0 | 0.004 | g |
| SFA 5:0 | 0 | g |
| SFA 6:0 | 0 | g |
| SFA 7:0 | 0 | g |
| SFA 8:0 | 0.004 | g |
| SFA 9:0 | 0 | g |
| SFA 10:0 | 0.006 | g |
| SFA 11:0 | 0 | g |
| SFA 12:0 | 0.017 | g |
| SFA 14:0 | 0.04 | g |
| SFA 15:0 | 0.01 | g |
| SFA 16:0 | 8.26 | g |
| SFA 17:0 | 0.072 | g |
| SFA 18:0 | 2.58 | g |
| SFA 20:0 | 1.14 | g |
| SFA 21:0 | 0.021 | g |
| SFA 22:0 | 2.58 | g |
| SFA 23:0 | 0 | g |
| SFA 24:0 | 1.48 | g |
| Monounsaturated fatty acids (MUFAs), total | 57.1 | g |
| MUFA 12:1 | 0 | g |
| MUFA 14:1 c | 0 | g |
| MUFA 15:1 | 0 | g |
| MUFA 16:1 c | 0.075 | g |
| MUFA 17:1 | 0.055 | g |
| MUFA 17:1 c | 0.055 | g |
| MUFA 18:1 c | 55.4 | g |
| MUFA 20:1 c | 1.41 | g |
| MUFA 22:1 c | 0.136 | g |
| MUFA 22:1 n-9 | 0.133 | g |
| MUFA 22:1 n-11 | 0.003 | g |
| MUFA 24:1 c | 0.013 | g |
| Polyunsaturated fatty acids (PUFAs), total | 19.9 | g |
| PUFA 18:2 c | 19.6 | g |
| PUFA 18:2 n-6 c,c | 19.6 | g |
| PUFA 18:2 CLAs | 0.021 | g |
| PUFA 18:3 c | 0.318 | g |
| PUFA 18:3 n-3 c,c,c (ALA) | 0.318 | g |
| PUFA 18:3 n-6 c,c,c | 0 | g |
| PUFA 18:4 | 0 | g |
| PUFA 20:2 c | 0.017 | g |
| PUFA 20:2 n-6 c,c | 0.017 | g |
| PUFA 20:3 c | 0.001 | g |
| PUFA 20:3 n-3 | 0.001 | g |
| PUFA 20:3 n-6 | 0 | g |
| PUFA 20:3 n-9 | 0 | g |
| PUFA 22:3 | 0.013 | g |
| PUFA 20:4 | 0.003 | g |
| PUFA 20:4c | 0.003 | g |
| PUFA 20:5c | 0.001 | g |
| PUFA 20:5 n-3 (EPA) | 0.001 | g |
| PUFA 22:2 | 0.001 | g |
| PUFA 22:5 c | 0 | g |
| PUFA 22:4 | 0.001 | g |
| PUFA 22:5 n-3 (DPA) | 0 | g |
| PUFA 22:6 c | 0 | g |
| PUFA 22:6 n-3 (DHA) | 0 | g |
| Trans fatty acids (TFA), total | 0.172 | g |
| Fatty acids, total trans-monoenoic | 0.034 | g |
| TFA 14:1 t | 0 | g |
| TFA 16:1 t | 0 | g |
| TFA 18:1 t | 0.034 | g |
| TFA 20:1 t | 0 | g |
| TFA 22:1 t | 0 | g |
| TFA 18:2 t not further defined | 0.139 | g |
| TFA 18:2 t | 0.139 | g |
| Fatty acids, total trans-polyenoic | o | g |
| TFA 18:3 t | 0 | g |
| Phytosterols | ||
| Stigmastadiene | <1 | mg |
| Stigmasterol | 17.8 | mg |
| Campesterol | 33 | mg |
| Brassicasterol | <0.5 | mg |
| Beta-sitosterol | 122 | mg |
| Campestanol | 0.14 | mg |
| Beta-sitostanol | 3.58 | mg |
| Delta-5-avenasterol | 16.4 | mg |
| Delta-7-Stigmastenol | 8.2 | mg |
Footnote: Per 100 g peanut oil.
[Source 40 ]How to Make Healthy Lifestyle and Eating Choices
It’s the overall eating pattern of your life choices that counts. Here are some tips for making healthy lifestyle and eating choices:
- Balance calorie intake (Calorie IN) with calorie needs (Calorie OUT) to achieve and maintain a healthy weight. Start by knowing how many calories you should eat and drink to maintain your weight. You may need fewer or more calories depending on several factors including age, gender and level of physical activity. Increase the amount and intensity of your physical activity to burn more calories. Aim for at least 150 minutes of moderate physical activity or 75 minutes of vigorous physical activity (or an equal combination of both) each week. Ideally, your activity should be spread throughout the week. Regular physical activity can help you maintain your weight, keep off weight that you lose and reach physical and cardiovascular fitness. If it’s hard to schedule regular exercise, look for ways to build short bursts of activity into your daily routine such as parking farther away and taking the stairs instead of the elevator.
- Don’t smoke, vape or use tobacco or nicotine products — and avoid secondhand smoke or vapor.
- Limit salt, sugar, animal fat, processed foods and alcohol.
- Eat a variety of foods. Eat a variety of foods from each of the five food groups daily. Healthy choices include fruits, vegetables, whole grains, protein foods, and fat-free or low-fat dairy. Foods are grouped together because they provide similar amounts of key nutrients. For example, key nutrients of the milk, yoghurt, cheese and alternatives group include calcium and protein, while the fruit group is a good source of vitamins, minerals, antioxidants. As a bonus, choosing a variety of foods will help to make your meals interesting, so that you don’t get bored with your diet.
- Eat fruit instead of drinking it. Eating fruit is linked to a reduced risk of several health conditions, but fruit juices are more likely to spike blood sugar levels.
- Add healthy fats. Healthy fats like monounsaturated and polyunsaturated fats can help lower cholesterol and protect your heart. You can find healthy fats in foods like olive oil, nuts, avocados, and some types of fish.
- Drink water. Sipping water throughout the day can help keep you full and hydrated. Sometimes thirst is mistaken for hunger.
- Reduce added sugar. Too much added sugar in your diet can contribute to weight gain, obesity, type 2 diabetes, and heart disease.
- Chew your food well. Chewing your food well can help you make healthier food choices.
- Sit at the table to eat. Sitting at the table to eat can help you focus on your food and internal cues for hunger or fullness.
To lose weight you’ll need to start with finding a way to eat fewer calories than you need. A calorie is a unit of energy, which is in the foods and drinks you consume. Scientifically, the calorie (a unit of energy) was originally defined as the amount of heat required at a pressure of 1 standard atmosphere to raise the temperature of 1 gram of water 1° Celsius. When you hear something contains 100 calories, it’s a way of describing how much energy your body could get from eating or drinking it. However, since calories are too small of a measurement to use when discussing nutrition and exercise, kilocalorie (kcal) measurements are used instead and the term is interchangeable with calories. Kilocalorie (kcal) is a unit of measurement for energy that is equivalent to 1,000 calories. Also,1 kcal or 1 kilocalorie is equivalent to 1 large Calorie (with an uppercase C) or 1,000 calories.
Some countries use kilojoules (kJ) to measure how much energy people get from consuming a food or drink.
- 1 calorie = 4.184 joule
- 1 kilocalorie (kcal) = 4.184 kilojoules (kJ)
- 1 Calorie (1,000 calories) = 4.184 kilojoules (kJ)
Here’s how many calories are in your foods and drinks 32:
- 1 gram of carbohydrate = 4 calories
- 1 gram of protein = 4 calories
- 1 gram of fat = 9 calories
- 1 gram of water = 0 calorie
Most foods and drinks contain calories. You can find out how many calories are in a food by looking at the nutrition facts label. The label also will describe the components of the food such as how many grams of carbohydrate, protein, and fat it contains.
That means if you know how many grams of each one are in a food, you can calculate the total calories. You would multiply the number of grams by the number of calories in a gram of that food component. For example, if a serving of potato chips (about 20 chips) has 10 grams of fat, 90 calories are from fat. That’s 10 grams x 9 calories per gram. Some foods, such as lettuce, contain few calories (1 cup of shredded lettuce has less than 10 calories). Other foods, like peanuts, contain a lot of calories (½ cup of peanuts has 427 calories).
Being overweight or obese is the result of an energy imbalance between your daily energy intake and your energy expenditure resulting in excessive weight gain 44. The amount of energy or calories you get from food and drinks (energy IN) is balanced with the energy your body uses for things like breathing, digesting, and being physically active (energy OUT):
- The same amount of energy IN and energy OUT over time = weight stays the same (Energy Balance)
- More energy IN than OUT over time = Weight Gain
- More energy OUT than IN over time = Weight Loss
In order to lose weight, energy expenditures must exceed energy intake. To lose weight, most people need to reduce the number of calories they get from food and beverages (energy IN) and increase their physical activity (energy OUT). To achieve this imbalance, you can decrease energy intake, increase energy expenditures or combine a decrease in intake with an increase in expenditures. Being physically active and eating fewer calories will help you lose weight and keep the weight off over time. As a result, most weight loss recommendations advise combining a low caloric diet with an exercise program in order to achieve a significant energy deficit 45. A long-standing consistent observation is that regular exercise by itself is prescribed in small to moderate amounts resulting in modest weight loss or in some cases weight gain 46.
How many calories do I need per day?
The total number of calories you need each day varies depends on a number of factors, namely your age, sex, height, weight, level of physical activity, and pregnancy or lactation status. According to the Dietary Guidelines for Americans, American female adult estimated calorie needs range from 1,600 to 2,400 calories per day and for males 2,000 to 3,000 calories per day 47. The average, healthy, adult, American male consumes approximately 2,800 calories per day, and the average female about 1,800 calories 36. But most people need different amounts of calories based on how their bodies work, how active they are and any weight management goals. And if you want to lose weight you’ll have to reduce your calorie intake.
Here is a general estimate of calories you need each day:
- Sedentary lifestyle (little to no exercise)
- Women: 1,800 to 2,400 calories
- Men: 2,200 to 3,000 calories
- Moderately active lifestyle (engages in moderate exercise/physical activity like walking or light yard work:
- Women: 2,000 to 2,600 calories
- Men: 2,400 to 2,800 calories
- Very active lifestyle (engages in hard exercise/physical activity, or has a physically demanding job):
- Women: 2,200 to 2,800 calories
- Men: 2,800 to 3,200 calories
These are just general guidelines. It’s essential to consult with a nutritionist or a doctor who can give personalized advice based on your specific situation. Remember, it’s not just the quantity but also the quality of calories that matters for overall health.
Obesity results from the accumulation of excessive body fat, which is stored as adipose tissue. An energy deficit of approximately 3,500 calories is required to lose one pound of fat. However, there are several factors that can influence this particular number. These include compensatory changes in your resting metabolism (basal metabolic rate [BMR]), the energy cost of work, and discretionary physical activity, which can sometimes alter this figure by 100 to 200 calories. Your basal metabolic rate (BMR) also known as resting metabolic rate (RMR) is the number of calories your body burns while performing basic life-sustaining functions, such as breathing and keeping your heart beating. Your basal metabolic rate (BMR) is typically between 1,000 and 2,000 calories per day.
How to calculate calories you need for weight loss
You can calculate your basal metabolic rate (BMR) or resting metabolic rate (RMR) using the Mifflin-St Jeor equation 48, which is considered more accurate than the Harris-Benedict equation, especially for lean people. According to the Academy of Nutrition and Dietetics Evidence Analysis Library (EAL), the Mifflin-St. Jeor equation accurately predicted resting metabolic rate (RMR) using actual body weight within +/- 10% of measured RMR in 70% of obese individuals 49. Of the remaining 30%, 9% were overestimations and 21% were underestimations. The individual error range was a maximum overestimate of 15% to a maximum underestimate of 20%” 50. While the Harris-Benedict and WHO equations are often used in clinical practice with reasonable accuracy, results have been mixed regarding their applications to individuals who are overweight or obese 36.
The Mifflin-St Jeor formula for calculating your basal metabolic rate (BMR) or resting metabolic rate (RMR):
- Males Basal metabolic rate [BMR] (kcal/day) = (10 X weight in kilograms) + (6.25 X height in centimeters) – (5 X age in years) + 5 (kcal/day)
- Females Basal metabolic rate [BMR] (kcal/day) = (10 X weight in kilograms) + (6.25 X height in centimeters) – (5 X age in years) – 161 (kcal/day)
You can also use the free online Basal Metabolic Rate (BMR) calculator here: https://www.nasm.org/resources/calorie-calculator
Or the Body Weight Planner (https://www.niddk.nih.gov/health-information/weight-management/body-weight-planner).
The Body Weight Planner allows you to make personalized calorie and physical activity plans to reach a goal weight within a specific time period and to maintain it afterwards.
The Basal Metabolic Rate (BMR) calculator factor in your activity levels, overall goals, and calorie usage to help you craft a weight-loss plan.
Once you have found your basal metabolic rate (BMR), multiply your BMR by your Physical Activity Levels to provide a baseline daily caloric level for weight maintenance:
- Sedentary (light physical activity associated with typical day-to-day life) = 1
- Low Active (walking about 1.5 to 3 miles per day at 3 to 4 miles per hour, in addition to the light physical activity associated with typical day-to-day life), For males = 1.11 and females = 1.20
- Active (walking more than 3 miles per day at 3 to 4 miles per hour, in addition to light physical activity associated with typical day-to-day life: 60 minutes of at least moderate intensity physical activity). For males = 1.25 and females = 1.27
- Very Active (walking more than 7.5 miles per day at 3 to 4 miles per hour, in addition to light physical activity associated with typical day-to-day life: 60 minutes of at least moderate to vigorous intensity physical activity). For males = 1.48 and females = 1.45
Your Total Daily Energy Expenditure (TDEE) gives you the estimated number of calories you need to maintain your current weight based on your activity level.
To find your Total Daily Energy Expenditure (TDEE) multiply your Basal Metabolic Rate (BMR) by your Physical Activity Levels
For example:
- Sedentary (little to no exercise): BMR x 1
- Lightly active (walking about 1.5 to 3 miles per day at 3 to 4 miles per hour, in addition to the light physical activity associated with typical day-to-day life): BMR x For males = 1.11 and females = 1.20
- Moderately active (moderate exercise/sports 3-5 days/week): BMR x 1.55
- Very active (walking more than 7.5 miles per day at 3 to 4 miles per hour, in addition to light physical activity associated with typical day-to-day life: 60 minutes of at least moderate to vigorous intensity physical activity): BMR x For males = 1.48 and females = 1.45
- Super active (very hard exercise & physical job or 2x training): BMR x 1.9
You can increase your basal metabolic rate (BMR) by:
- Exercising more, especially interval training
- Weight training to build muscle mass
- Eating fat-burning foods
- Getting enough sleep
After calculating your basal metabolic rate (BMR) or resting metabolic rate (RMR), your RMR should be multiplied by an appropriate physical activity factor to provide your baseline daily caloric level for weight maintenance. Once your baseline caloric level is known, your recommended calorie intake should be reduced to facilitate your weight loss.
If you want to lose weight, subtract 500 to 1000 calories from your Total Daily Energy Expenditure (TDEE) to get a daily intake goal. For weight gain, add extra calories. Reducing your calorie intake by 500 calories is a common strategy to yield a weight loss of approximately one pound per week, although reductions of up to 750 calories per day are sometimes used 51.
Another approach is to reduce your current caloric intake by 30% 51. Diets that reduce caloric intake relative to energy expenditure result in weight loss, regardless of macronutrient composition 51.
Here’s how to estimate how long it will take to reach your goal:
Jessie’s current weight is 150 lbs. She wants to lose 20 lbs.
- 150lbs – 20lbs = 130lbs.
- 20lbs loss at 2lbs/week = 10 weeks.
- It will take Jessie about 10 week to lose the weight.
Remember, these are general guidelines only. It’s crucial to monitor your progress and adjust as necessary. Consulting with a nutritionist or health professional is always recommended for personalized advice.
How many calories should I eat to lose weight?
For a healthy and sustainable weight loss journey, it’s typically recommended you not to shed more than 2 pounds of fat weekly. This translates to a daily calorie deficit of 1,000 calories. It’s essential to note that when weight loss surpasses 2lbs within a week, it’s often water weight being lost, not just fat.
For those leading a more sedentary lifestyle, aiming to lose 1lb per week is a good starting point. This means creating a daily calorie deficit of 500 calories.
On the other hand, those who are more active naturally have higher daily calorie needs. So, when they’re trying to lose weight, they can afford to eat a bit more since their maintenance calories are already elevated.
For such individuals, aiming for a daily calorie deficit of 500-1,000 calories is realistic, potentially leading to a weight loss rate of up to 2lbs weekly.
What happens when your calories are too low?
Consuming calories below your body’s needs for an extended period can lead to various physiological and psychological consequences. Here’s what can happen when your caloric intake is too low:
- Slower metabolism: Your body might slow down its metabolic rate as a defense mechanism to conserve energy. This can make weight loss harder over time and weight regain more likely once normal eating resumes.
- Nutrient deficiencies: Low calorie intake can lead to inadequate intake of essential vitamins and minerals. Over time, this can result in conditions like anemia, osteoporosis, and impaired immune function.
- Loss of muscle mass: Your body might start breaking down muscle tissue for energy, especially if protein intake is inadequate. This can further slow down metabolism and lead to weakness.
- Hormonal changes: Reduced calorie intake can affect hormone levels, leading to disruptions in menstrual cycles for women, reduced bone density, and other hormonal imbalances.
- Reduced energy and fatigue: You might feel constantly tired or find it difficult to concentrate.
- Mood changes: Low caloric intake can influence mood. This can result in irritability, depression, or anxiety.
- Impaired Immune Function: Your body might become more susceptible to infections due to a weakened immune system.
- Hair and skin problems: You might experience hair loss, dry skin, or brittle nails due to inadequate nutrient intake.
- Digestive problems: Constipation or other digestive issues can occur as a result of reduced fiber and fluid intake.
- Fertility issues: Low calorie and nutrient intake can lead to fertility problems in both men and women.
- Cardiovascular problems: Chronic low calorie intake can affect heart health, leading to low blood pressure, irregular heart rhythms, or other cardiovascular issues.
- Increased risk of gallstones: Rapid weight loss from very low-calorie diets can lead to the development of gallstones.
What is the best way to lose weight?
There is no one best way to lose weight, which is why doctors and dietitians work to understand your personal circumstances when making recommendations. There is no quick fix. Improving your diet and increasing activity can be key to losing weight, although are not the only factors that need to be considered. When aiming to lose weight it is important to have realistic goals that are achievable. Success boosts confidence in your ability to lose weight. A weight loss of between 0.5 to 2 pounds (0.5-1kg) a week is a safe and realistic target. Experts recommend losing 5 to 10 percent of your body weight within the first 6 months of treatment 52. If you weigh 200 pounds, this means losing as little as 10 pounds. Moreover, it’s not just about your weight on the scales, losing inches from your waist helps to lower your risk of conditions like type 2 diabetes and high blood pressure. To reach and stay at a healthy weight over the long term, you must focus on your overall health and lifestyle habits, not just on what you eat. Successful weight-loss programs should promote healthy behaviors that help you lose weight safely, that you can stick with every day, and that help you keep the weight off. People who successfully lose weight and keep it off develop techniques to make their new lifestyle and activity habits an enjoyable way of life and also make them life long.
You weight loss programs and weight loss maintenance programs should focus on changing your behavior to reduce energy intake by cutting unhealthy foods, decreasing sugar‐sweetened beverage consumption and fat intake, portion control, increasing fruit and vegetable intake, and adhering to a diet 53. Additionally, energy expenditure should be promoted through increasing physical activity.
American College of Sports Medicine recommendations for physical activity for Weight Loss and Prevention of Weight Regain for Adults 54:
- Maintain and improving health: 150 minutes/week
- Prevention of weight gain: 150 – 250 minutes/week
- Promote clinically significant weight loss: 225 – 420 minutes/week
- Prevention of weight gain after weight loss: 200 – 300 minutes/week
Strong evidence exists that exercise (physical activity) can reduce weight gain in those at risk for obesity, and many exercise training programs are capable of producing at least modest weight loss (~2 kg) 54. A question often encountered in the clinical setting from patients is how much exercise is needed to lose weight and what type of exercise training should be performed. Overall, the changes in weight in response to exercise training without caloric restriction are highly heterogeneous and individual differences can span weight gain to clinically significant weight loss 55. Patients should should consult their clinicians or dietitians on what are reasonable expectations based on their specific weight loss program. However, research data suggest that physical activity has an important role in the amount of weight regain following successful weight loss 56. Therefore, patients attempting to reduce recidivism after weight loss should engage in physical activity levels above 200 minutes/week 54.
Furthermore, high levels of physical activity and cardiorespiratory fitness (fitness) are inversely associated with cardiovascular disease, type 2 diabetes and all-cause mortality 57. Several epidemiological studies even suggest that high levels of physical activity or cardiorespiratory fitness reduces the health risk of obesity 58, 59. Moreover, cardiorespiratory fitness levels have been shown to alter the relationship of the obesity paradox, where high cardiorespiratory fitness level is associated with greater survival in all body mass index (BMI) categories 60. In summary, patients are encourage to adhere to exercise programs or engage in regular physical activity regardless of the weight loss achieved.
Another question that is often encountered in the clinical setting is if there is a difference between weight loss achieved through dietary means or through exercise training in terms of cardiovascular and type 2 diabetes mellitus risk factors. In an elegantly designed study, Ross et al. 61 randomized obese men (n= 52) to diet-induced weight loss, exercise induced weight loss, exercise without weight loss, or a control group for 3 months. The diet-induced and exercise-induced weight loss groups lost approximately 7 kg of weight (8% weight reduction), and had significant reductions in total fat mass, visceral fat and increased glucose disposal 61. However, the exercise-induced weight loss group had a greater reduction in total fat mass compared to the diet induced weight loss group 61. Importantly, the exercise-induced weight loss improved cardiorespiratory fitness (fitness) whereas the dietary group did not. In the group who performed exercise training without weight loss, the participants still experienced reductions in visceral fat and increased cardiorespiratory fitness.
The observations by Ross et al. 61 reaffirm that an exercise training program still confers health benefits to obese patients even in the absence of weight loss. Although dieting without exercise training has potential cardiovascular benefits, exercise training should be encouraged by to help patients improve cardiorespiratory fitness levels, which is an independent risk factor for cardiovascular diseases, type 2 diabetes mellitus and mortality 10, and may further augment the negative energy balance created by caloric restriction. Lastly, Ross’ observations suggest that there is a rationale for exercise training to be a part of weight loss programs as the authors observed greater changes in visceral fat, oral glucose tolerance, and glucose disposal in the exercise training group with clinically significant weight loss compared to the group with exercise without weight loss group 61.
- Salem N., Jr Introduction to polyunsaturated fatty acids. Backgrounder. 1999;3:1–8.[↩]
- Clinical nutrition: 4. Omega-3 fatty acids in cardiovascular care. Holub BJ. CMAJ. 2002 Mar 5; 166(5):608-15. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC99405/[↩][↩]
- Simopoulos AP. An Increase in the Omega-6/Omega-3 Fatty Acid Ratio Increases the Risk for Obesity. Nutrients. 2016;8(3):128. doi:10.3390/nu8030128. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4808858/[↩][↩]
- Alpha-linolenic acid and cardiovascular diseases. Lanzmann-Petithory D. J Nutr Health Aging. 2001; 5(3):179-83. https://www.ncbi.nlm.nih.gov/pubmed/11458289/[↩]
- Kris-Etherton P.M. AHA Science Advisory. Monounsaturated fatty acids and risk of cardiovascular disease. American Heart Association. Nutrition Committee. Circulation. 1999;100:1253–1258. doi: 10.1161/01.CIR.100.11.1253[↩]
- Schwingshackl L, Hoffmann G. Monounsaturated Fatty Acids and Risk of Cardiovascular Disease: Synopsis of the Evidence Available from Systematic Reviews and Meta-Analyses . Nutrients. 2012;4(12):1989-2007. doi:10.3390/nu4121989. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3546618/[↩]
- Omega-3 Fatty Acids. https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional[↩][↩][↩][↩][↩]
- Polyunsaturated Fats. https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/fats/polyunsaturated-fats[↩]
- Jones PJH, Rideout T. Lipids, sterols, and their metabolites. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2014.[↩][↩][↩][↩][↩]
- Jones PJH, Papamandjaris AA. Lipids: cellular metabolism. In: Erdman JW, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. Washington, DC: Wiley-Blackwell; 2012:132-48.[↩][↩][↩]
- Harris WS. Omega-3 fatty acids. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements. 2nd ed. London and New York: Informa Healthcare; 2010:577-86.[↩][↩][↩][↩][↩][↩]
- Lichtenstein AH, Jones PJH. Lipids: absorption and transport. In: Erdman JW, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. Washington, DC: Wiley-Blackwell; 2012:118-31.[↩][↩]
- Institute of Medicine, Food and Nutrition Board. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids (macronutrients). Washington, DC: National Academy Press; 2005.[↩][↩][↩]
- SanGiovanni JP, Chew EY. The role of omega-3 long-chain polyunsaturated fatty acids in health and disease of the retina. Prog Retin Eye Res. 2005 Jan;24(1):87-138. doi: 10.1016/j.preteyeres.2004.06.002[↩]
- Jones PJH, Rideout T. Lipids, sterols, and their metabolites. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2014[↩]
- Gabbs M, Leng S, Devassy JG, Monirujjaman M, Aukema HM. Advances in Our Understanding of Oxylipins Derived from Dietary PUFAs. Adv Nutr. 2015 Sep 15;6(5):513-40. doi: 10.3945/an.114.007732[↩]
- Simopoulos AP. The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp Biol Med (Maywood). 2008 Jun;233(6):674-88. doi: 10.3181/0711-MR-311[↩][↩]
- James M, Proudman S, Cleland L. Fish oil and rheumatoid arthritis: past, present and future. Proc Nutr Soc. 2010 Aug;69(3):316-23. doi: 10.1017/S0029665110001564[↩][↩]
- Wang C, Chung M, Lichtenstein A, Balk E, Kupelnick B, DeVine D, et al. Effects of omega-3 fatty acids on cardiovascular disease. Summary, evidence report/technology assessment no. 94. (Prepared by the Tufts New England Medical Center Evidence-based Practice Center, Boston, MA.) AHRQ Publication No. 04-E009-1. Agency for Healthcare Research and Quality, 2004. https://archive.ahrq.gov/downloads/pub/evidence/pdf/o3cardio/o3cardio.pdf[↩]
- Stanley JC, Elsom RL, Calder PC, Griffin BA, Harris WS, Jebb SA, Lovegrove JA, Moore CS, Riemersma RA, Sanders TA. UK Food Standards Agency Workshop Report: the effects of the dietary n-6:n-3 fatty acid ratio on cardiovascular health. Br J Nutr. 2007 Dec;98(6):1305-10. doi: 10.1017/S000711450784284X[↩][↩]
- Harris WS, Davidson MH. RE: Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst. 2014 Apr;106(4):dju019. doi: 10.1093/jnci/dju019[↩][↩]
- Fritsche KL. Too much linoleic acid promotes inflammation-doesn’t it? Prostaglandins Leukot Essent Fatty Acids. 2008 Sep-Nov;79(3-5):173-5. doi: 10.1016/j.plefa.2008.09.019[↩][↩]
- Monounsaturated Fats. https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/fats/monounsaturated-fats[↩]
- DiNicolantonio JJ, O’Keefe JH. Monounsaturated Fat vs Saturated Fat: Effects on Cardio-Metabolic Health and Obesity. Mo Med. 2022 Jan-Feb;119(1):69-73 https://pmc.ncbi.nlm.nih.gov/articles/PMC9312452[↩]
- Dietary Guidelines for Americans. https://www.dietaryguidelines.gov/[↩][↩][↩]
- Saturated Fat. https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/fats/saturated-fats[↩][↩]
- Eckel RH, Jakicic JM, Ard JD, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014 Jun 24;129(25 Suppl 2):S76-99. doi: 10.1161/01.cir.0000437740.48606.d1. Epub 2013 Nov 12. Erratum in: Circulation. 2014 Jun 24;129(25 Suppl 2):S100-1. Erratum in: Circulation. 2015 Jan 27;131(4):e326.[↩]
- Morris AL, Mohiuddin SS. Biochemistry, Nutrients. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554545[↩]
- Del Razo Olvera FM, Melgarejo Hernández MA, Mehta R, Aguilar Salinas CA. Setting the Lipid Component of the Diet: A Work in Process. Adv Nutr. 2017 Jan 17;8(1):165S-172S. doi: 10.3945/an.116.013672[↩]
- Tvrzicka E, Kremmyda LS, Stankova B, Zak A. Fatty acids as biocompounds: their role in human metabolism, health and disease–a review. Part 1: classification, dietary sources and biological functions. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2011 Jun;155(2):117-30. doi: 10.5507/bp.2011.038[↩]
- Jacobs DR, Tapsell LC. Food synergy: the key to a healthy diet. Proc Nutr Soc. 2013 May;72(2):200-6. doi: 10.1017/S0029665112003011[↩]
- Trumbo P, Schlicker S, Yates AA, Poos M; Food and Nutrition Board of the Institute of Medicine, The National Academies. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J Am Diet Assoc. 2002 Nov;102(11):1621-30. doi: 10.1016/s0002-8223(02)90346-9. Erratum in: J Am Diet Assoc. 2003 May;103(5):563.[↩][↩]
- Omega-3 Fatty Acids, https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional[↩][↩]
- Wang C, Chung M, Lichtenstein A, Balk E, Kupelnick B, DeVine D, et al. Effects of omega-3 fatty acids on cardiovascular disease. Summary, evidence report/technology assessment no. 94. https://archive.ahrq.gov/downloads/pub/evidence/pdf/o3cardio/o3cardio.pdf[↩]
- Very Low-Calorie Diets. https://www.govinfo.gov/content/pkg/GOVPUB-HE20-PURL-LPS78142/pdf/GOVPUB-HE20-PURL-LPS78142.pdf[↩]
- Dwyer JT, Melanson KJ, Sriprachy-anunt U, et al. Dietary Treatment of Obesity. [Updated 2015 Feb 28]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK278991[↩][↩][↩][↩][↩]
- Pritikin M, McGrady PM. The Pritikin Program for Diet and Exercise. New York: Bantum Books, 1980.[↩]
- Ornish D. Can lifestyle changes reverse coronary heart disease? World Rev Nutr Diet. 1993;72:38-48. doi: 10.1159/000422326[↩][↩][↩]
- Hand B and Romine S. The Spark Solution. HarperOne, 2014.[↩]
- Avocado, Hass, peeled, raw. https://fdc.nal.usda.gov/food-details/2710824/nutrients[↩][↩]
- Extra virgin olive oil. https://fdc.nal.usda.gov/food-details/748608/nutrients[↩]
- Peanuts, raw. https://fdc.nal.usda.gov/food-details/2515376/nutrients[↩]
- Peanut butter, creamy. https://fdc.nal.usda.gov/food-details/2262072/nutrients[↩]
- Thomas, D. M., Bouchard, C., Church, T., Slentz, C., Kraus, W. E., Redman, L. M., Martin, C. K., Silva, A. M., Vossen, M., Westerterp, K., & Heymsfield, S. B. (2012). Why do individuals not lose more weight from an exercise intervention at a defined dose? An energy balance analysis. Obesity reviews : an official journal of the International Association for the Study of Obesity, 13(10), 835–847. https://doi.org/10.1111/j.1467-789X.2012.01012.x[↩]
- Aim for Healthy Weight. https://www.nhlbi.nih.gov/health/educational/lose_wt/index.htm[↩]
- Slentz CA, Duscha BD, Johnson JL, Ketchum K, Aiken LB, Samsa GP, Houmard JA, Bales CW, Kraus WE. Effects of the amount of exercise on body weight, body composition, and measures of central obesity: STRRIDE–a randomized controlled study. Arch Intern Med. 2004 Jan 12;164(1):31-9. doi: 10.1001/archinte.164.1.31[↩]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020-2025. 9th Edition. December 2020. https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf[↩]
- Mifflin MD, St Jeor ST, Hill LA, Scott BJ, Daugherty SA, Koh YO. A new predictive equation for resting energy expenditure in healthy individuals. Am J Clin Nutr. 1990 Feb;51(2):241-7. doi: 10.1093/ajcn/51.2.241[↩]
- American Dietetic Association (ADA). Adult Weight Management Guideline: Major Recommendations. ADA Evidence Analysis Library 2014. https://www.andeal.org/vault/pq132.pdf[↩]
- Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults–The Evidence Report. National Institutes of Health, 6: 51S-179S. https://doi.org/10.1002/j.1550-8528.1998.tb00690.x[↩]
- American College of Cardiology/American Heart Association Task Force on Practice Guidelines, Obesity Expert Panel, 2013. Expert Panel Report: Guidelines (2013) for the management of overweight and obesity in adults. Obesity (Silver Spring). 2014 Jul;22 Suppl 2:S41-410. doi: 10.1002/oby.20660[↩][↩][↩]
- Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults. Circulation. 2014;129:S102–S138.[↩]
- Varkevisser, R., van Stralen, M. M., Kroeze, W., Ket, J., & Steenhuis, I. (2019). Determinants of weight loss maintenance: a systematic review. Obesity reviews : an official journal of the International Association for the Study of Obesity, 20(2), 171–211. https://doi.org/10.1111/obr.12772[↩]
- Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, Smith BK; American College of Sports Medicine. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc. 2009 Feb;41(2):459-71. doi: 10.1249/MSS.0b013e3181949333. Erratum in: Med Sci Sports Exerc. 2009 Jul;41(7):1532.[↩][↩][↩]
- Church TS, Martin CK, Thompson AM, Earnest CP, Mikus CR, Blair SN. Changes in weight, waist circumference and compensatory responses with different doses of exercise among sedentary, overweight postmenopausal women. PLoS One. 2009;4(2):e4515. doi: 10.1371/journal.pone.0004515[↩]
- Swift, D. L., Johannsen, N. M., Lavie, C. J., Earnest, C. P., & Church, T. S. (2014). The role of exercise and physical activity in weight loss and maintenance. Progress in cardiovascular diseases, 56(4), 441–447. https://doi.org/10.1016/j.pcad.2013.09.012[↩]
- Swift DL, Lavie CJ, Johannsen NM, Arena R, Earnest CP, O’Keefe JH, Milani RV, Blair SN, Church TS. Physical activity, cardiorespiratory fitness, and exercise training in primary and secondary coronary prevention. Circ J. 2013;77(2):281-92. doi: 10.1253/circj.cj-13-0007[↩]
- Lee CD, Blair SN, Jackson AS. Cardiorespiratory fitness, body composition, and all-cause and cardiovascular disease mortality in men. Am J Clin Nutr. 1999 Mar;69(3):373-80. doi: 10.1093/ajcn/69.3.373[↩]
- Wei M, Kampert JB, Barlow CE, Nichaman MZ, Gibbons LW, Paffenbarger RS Jr, Blair SN. Relationship between low cardiorespiratory fitness and mortality in normal-weight, overweight, and obese men. JAMA. 1999 Oct 27;282(16):1547-53. doi: 10.1001/jama.282.16.1547[↩]
- McAuley, P. A., Kokkinos, P. F., Oliveira, R. B., Emerson, B. T., & Myers, J. N. (2010). Obesity paradox and cardiorespiratory fitness in 12,417 male veterans aged 40 to 70 years. Mayo Clinic proceedings, 85(2), 115–121. https://doi.org/10.4065/mcp.2009.0562[↩]
- Ross R, Dagnone D, Jones PJ, Smith H, Paddags A, Hudson R, Janssen I. Reduction in obesity and related comorbid conditions after diet-induced weight loss or exercise-induced weight loss in men. A randomized, controlled trial. Ann Intern Med. 2000 Jul 18;133(2):92-103. doi: 10.7326/0003-4819-133-2-200007180-00008[↩][↩][↩][↩][↩]





{kind=link}