
Contents
What is Meniere’s disease
Meniere’s disease is a disorder of the inner ear that can cause severe dizziness, a roaring sound in your ears called tinnitus, hearing loss that comes and goes and the feeling of ear pressure or pain. Meniere’s disease usually affects just one ear. But some people who have the disease have problems in both ears. People with Ménière’s disease have a sick inner ear and are more sensitive to factors, such as fatigue and stress, that may influence the frequency of attacks.
Meniere’s disease is a chronic (ongoing) problem and Meniere’s disease is a common cause of hearing loss. Meniere’s disease can occur at any age, but it usually starts between the ages of 20 and 60. Meniere’s disease is uncommon in children.
People who have Meniere’s disease don’t have symptoms all the time. When symptoms occur, it’s called an “attack.” Attacks may happen often, or only sometimes. Attacks may last from 20 minutes to 2 hours or longer. After an episode, signs and symptoms improve and might disappear entirely. Episodes can occur weeks to years apart.
Meniere’s disease is a condition of the inner ear that causes sudden attacks of:
- feeling like the room is spinning around you (vertigo) or dizziness
- a ringing noise inside the ear (tinnitus)
- a feeling of fullness in the ear or ear pressure felt deep inside the ear
- hearing loss
Meniere’s disease may cause problems with balance and make you feel unstable while walking. Because of the spinning feeling, some people sweat, feel nauseated, and vomit during an attack. You may also notice some hearing loss, especially with sounds that have a low tone.
Attacks of dizziness may come on suddenly or after a short period of tinnitus or muffled hearing. Some people have single attacks of dizziness once in a while. Others may have many attacks close together over several days. Some people with Meniere’s disease have “drop attacks” during which the dizziness is so bad they lose their balance and fall.
Scientists don’t yet know the cause. They think that it has to do with the fluid levels or the mixing of fluids in the canals of your inner ear. In some individuals, especially those with involvement of both ears, allergies or autoimmune disorders may play a role in producing Ménières disease. In some cases, other conditions may cause symptoms similar to those of Ménières disease. Doctors diagnose it based on a physical exam and your symptoms. A hearing test can check to see how it has affected your hearing.
There’s no cure for Meniere’s disease, but medication can help you control vertigo, nausea and vomiting. Treatments include medicines to control dizziness, limiting salt in your diet, and taking water pills. A device that fits into the outer ear and delivers air pulses to the middle ear can help. Severe cases may require surgery.
Inner ear anatomy
We rely on the inner ear, an intricate sensory organ, to hear and to maintain balance. The inner ear is a complex system of communicating chambers and tubes called a labyrinth. Each ear has two parts to the labyrinth—the bony (osseus) labyrinth and the membranous labyrinth (Figure 1). The bony labyrinth is a cavity within the temporal bone. The membranous labyrinth is a tube of similar shape that lies within the bony labyrinth. Between the bony and membranous labyrinths is a fluid called perilymph, which is secreted by cells in the wall of the bony labyrinth. The membranous labyrinth contains another fluid, called endolymph.
The parts of the labyrinths include three membranous semicircular ducts within three bony semicircular canals, and a cochlea. The semicircular canals and associated structures provide a sense of equilibrium (balance). The cochlea functions in hearing.
The cochlea has a bony core and a thin, bony shelf that extends out from the core and coils around it. The shelf divides the bony labyrinth of the cochlea into upper and lower compartments. The upper compartment, called the scala vestibuli, leads from the oval window to the tip of the cochlea. The lower compartment, the scala tympani, extends from the tip of the cochlea to a membrane-covered opening in the wall of the middle ear called the round window.
The part of the membranous labyrinth within the cochlea is called the cochlear duct. It lies between the two bony compartments and ends as a closed sac near the tip of the cochlea. The cochlear duct is separated from the scala vestibuli by a vestibular membrane (Reissner’s membrane) and from the scala tympani by a basilar membrane. The basilar membrane has many thousands of elastic fibers, allowing it to move in response to sound vibrations. Sound vibrations entering the perilymph at the oval window travel along the scala vestibuli and pass through the vestibular membrane and into the endolymph of the cochlear duct, where they move the basilar membrane.
Figure 1. Inner ear anatomy

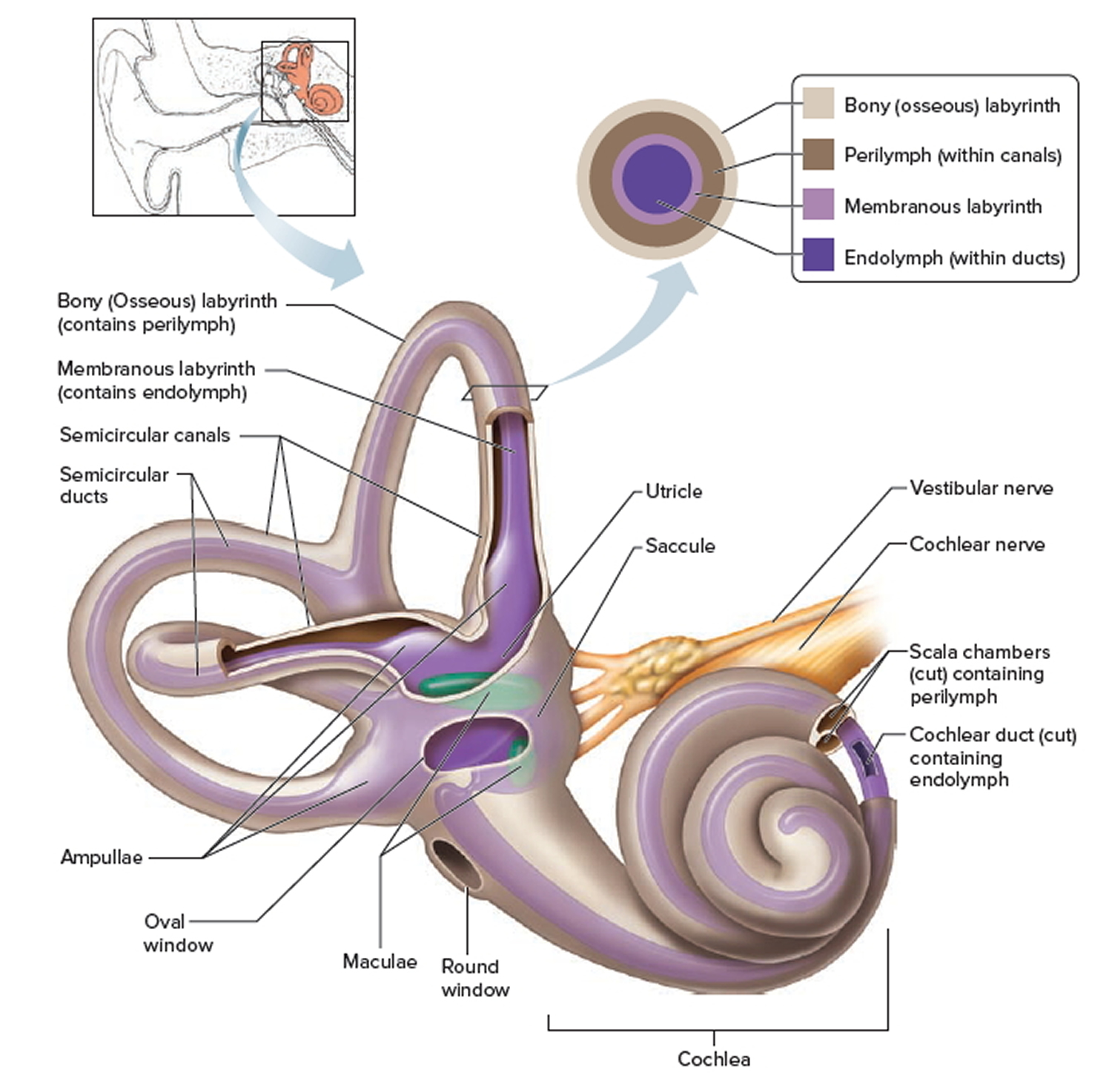
Figure 2. Parts of the inner ear
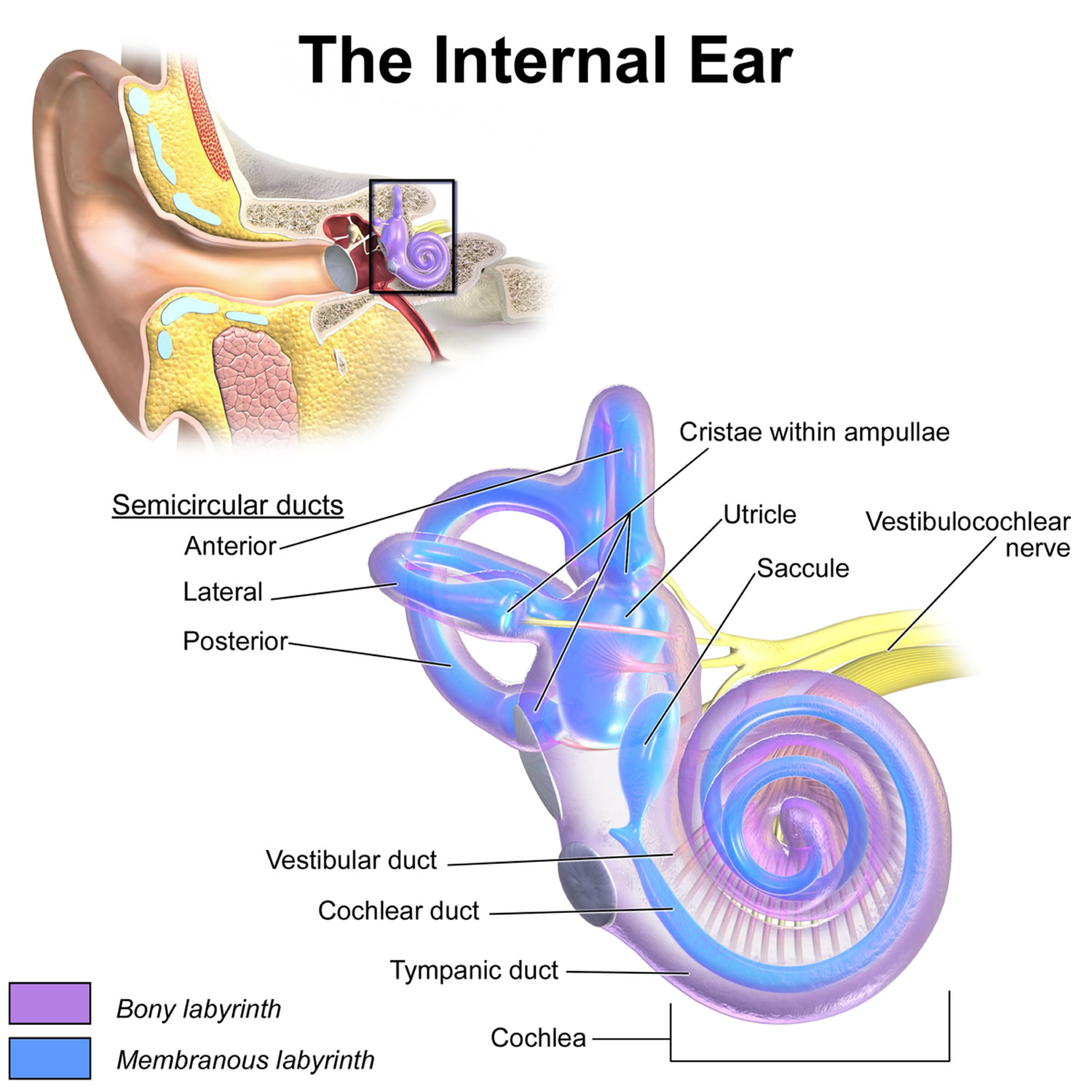
Figure 3. Inner ear bones
 Sense of Equilibrium
Sense of Equilibrium
The sense of equilibrium (balance) is really two senses:
- Static equilibrium and
- Dynamic equilibrium—that come from different sensory organs.
The organs of static equilibrium sense the position of the head, maintaining balance, stability and posture when the head and body are still. When the head and body suddenly move or rotate, the organs of dynamic equilibrium detect such motion and aid in maintaining balance.
Static Equilibrium
The organs of static equilibrium are in the vestibule, a bony chamber between the semicircular canals and the cochlea. The membranous labyrinth inside the vestibule consists of two expanded chambers—a utricle and a saccule (see Figures 2 and 3).
The saccule and utricle each have a tiny structure called a macula. Maculae have many hair cells, which serve as sensory receptors. The hairs of the hair cells project into a mass of gelatinous material, which has grains of calcium carbonate (otoliths) embedded in it. These particles add weight to the gelatinous structure.
Bending the head forward, backward, or to either side tilts the gelatinous masses of the maculae, and as they sag in response to gravity, the hairs projecting into them bend. This action causes the hair cells to signal the sensory neurons associated with them in a manner similar to that of hair cells associated with hearing. The resulting action potentials are conducted into the central nervous system on the vestibular branch of the vestibulocochlear nerve, informing the brain of the head’s new position. The brain responds by adjusting the pattern of motor impulses to skeletal muscles, which contract or relax to maintain balance (Figure 5).
Figure 4. Inner ear maculae respond to changes in head position
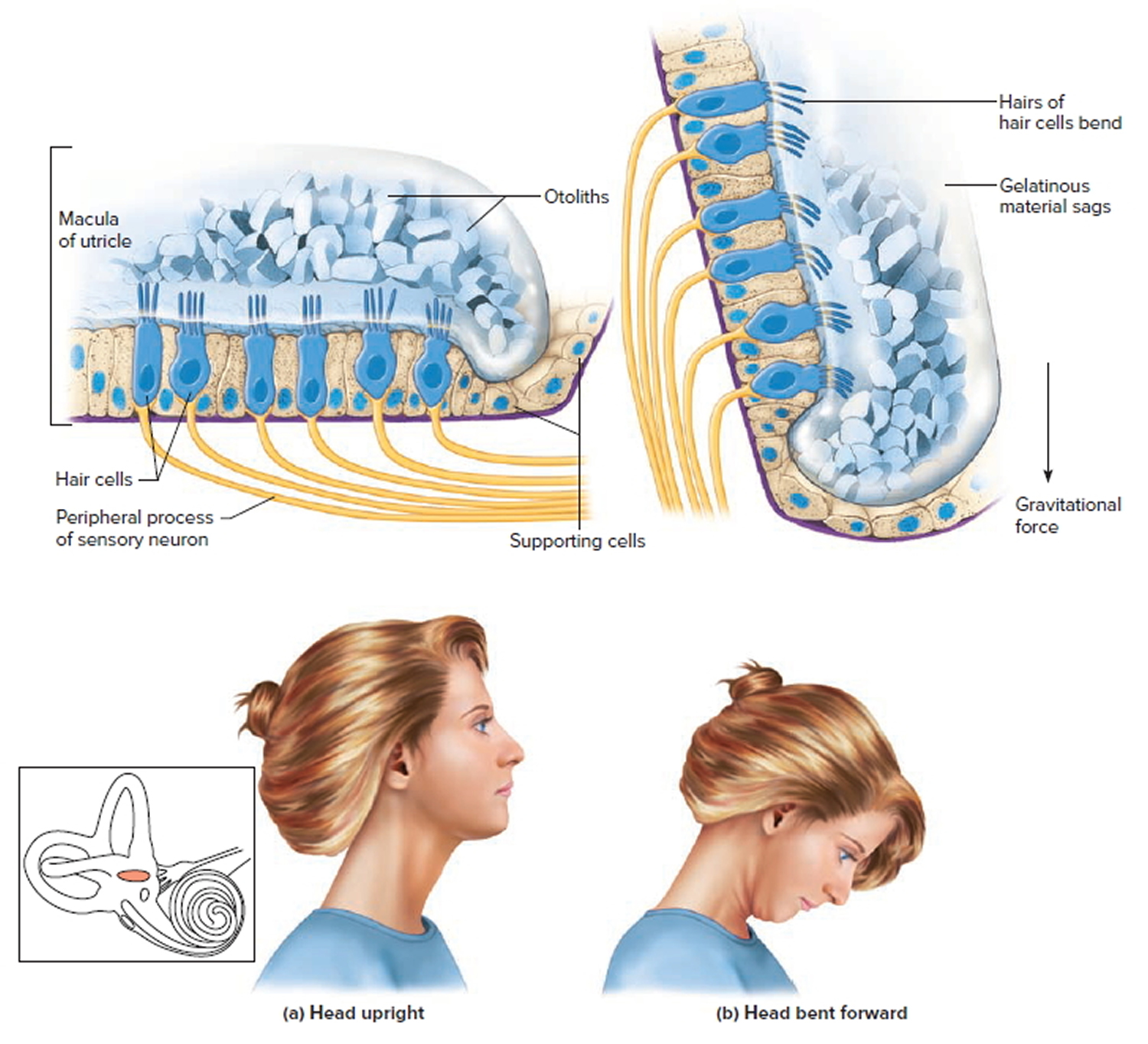
Note: (a) Macula of the utricle with the head in an upright position. (b) Macula of the utricle with the head bent forward.
Dynamic Equilibrium
The organs of dynamic equilibrium are the three semicircular canals in the labyrinth. They detect motion of the head and aid in balancing the head and body during sudden movement. These canals lie at right angles to each other (see Figure 2).
Suspended in the perilymph of the bony portion of each semicircular canal is a membranous semicircular duct that ends in a swelling called an ampulla, which
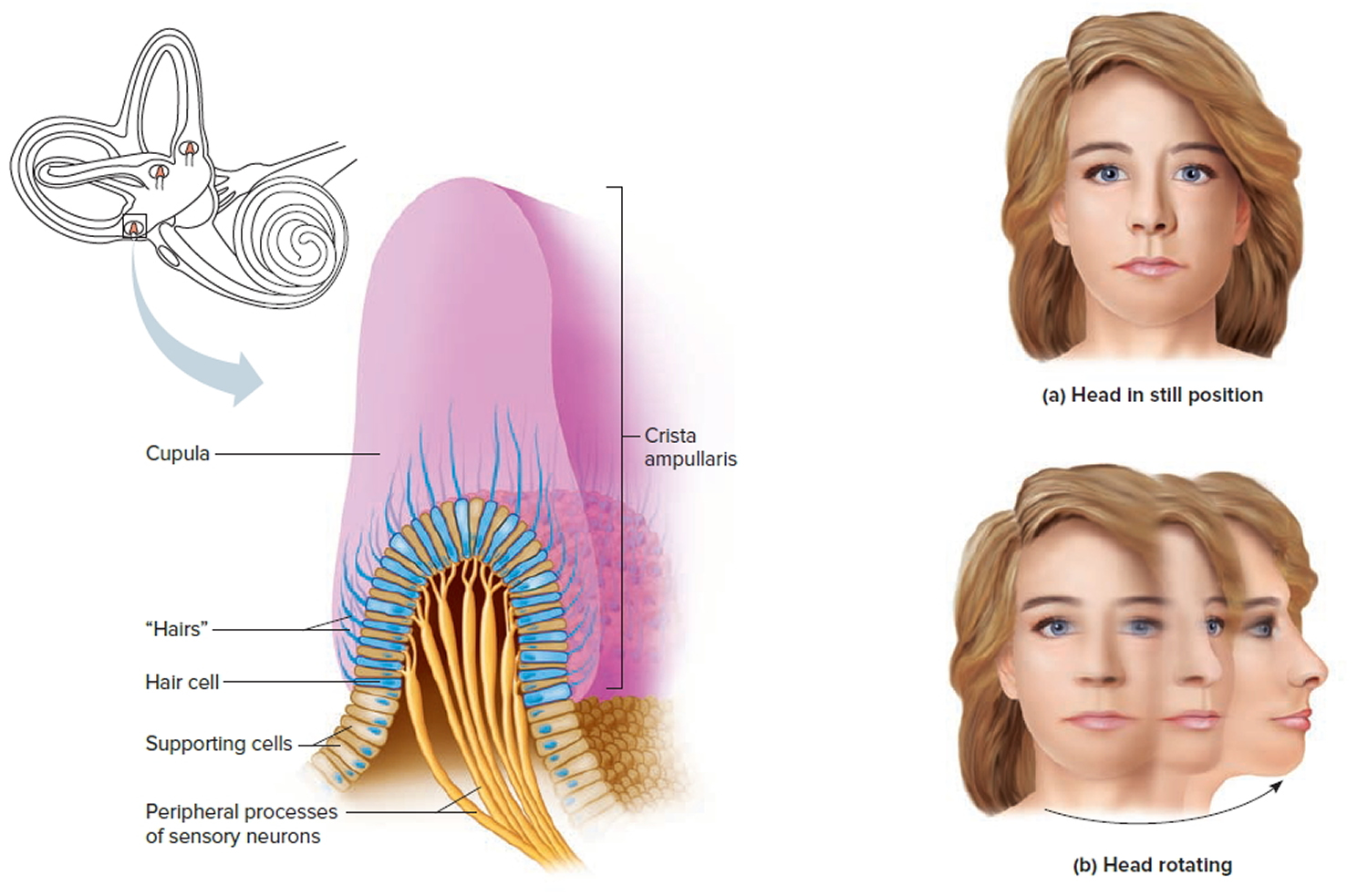
houses the sensory organs of the semicircular canals. Each of these sensory organs, called a crista ampullaris, contains a number of sensory hair cells and supporting cells. Like the hairs of the maculae, the hair cells of the crista ampullaris extend upward into a dome-shaped, gelatinous mass called the cupula (Figure 5). When the head is stationary, the cupula of the crista ampullaris remains upright. When the head is moving rapidly, the cupula bends opposite the motion of the head, stimulating sensory receptors.
Rapid movement of the head or body stimulates the hair cells of the crista ampullaris (Figure 5). At such times, the semicircular canals move with the head or body, but the fluid inside the membranous ducts remains stationary. Imagine turning rapidly while holding a full glass of water. This action bends the cupula in one or more of the canals in a direction opposite that of the head or body movement, and the hairs embedded in it also bend. The stimulated hair cells signal their associated neurons, which conduct impulses to the brain. The brain interprets these impulses as a movement in a particular direction.
Parts of the cerebellum are particularly important in interpreting impulses from the semicircular canals. Analysis of such information allows the brain to predict the consequences of rapid body movements. By modifying signals to appropriate skeletal muscles, the cerebellum can maintain balance.
Other sensory structures aid in maintaining equilibrium. For example, certain mechanoreceptors (proprioceptors), particularly those associated with the joints of the neck, inform the brain about the position of body parts. In addition, the eyes detect changes in position that result from body movements. Such visual information is so important that even if the organs of equilibrium are damaged, a person may be able to maintain normal balance by keeping the eyes open and moving slowly.
The nausea, vomiting, dizziness, and headache of motion sickness arise from sensations that don’t make sense. The eyes of a person reading in a moving car, for example, signal the brain that the person is stationary, because the print doesn’t move. However, receptors in the skin detect bouncing, swaying, starting, and stopping as the inner ear detects movement. The contradiction triggers the symptoms. Similarly, in a passenger of an airplane flying through heavy turbulence, receptors in the skin and inner ear register the chaos outside, but the eyes focus on the immobile seats and surroundings.
To prevent or lessen the misery of motion sickness, focus on the horizon or an object in the distance ahead. Medications are available by pill (diphenhydramine and dimenhydrinate) and, for longer excursions, in a skin patch (scopolamine).
Figure 5. Dynamic inner ear balance organs (crista ampullaris) within the Semicricular ducts
Meniere’s disease causes
The exact cause of Meniere’s disease is unknown, but it’s associated with a problem with pressure deep inside the ear.
One popular theory that hasn’t been proved is that Meniere’s disease appears to be the result of the abnormal amount of fluid (endolymph) in the inner ear. This often shows on autopsies, but it’s not clear that it causes the episodes.
Factors that affect the fluid, which might contribute to Meniere’s disease, include:
- poor fluid drainage in your ear
- an immune system disorder
- allergies
- viral infection, such as meningitis
- family history of Meniere’s disease
- head injury
- migraines
It’s likely that Meniere’s disease is caused by a combination of these factors.
Meniere’s disease triggers
Avoid stress and excess salt ingestion, caffeine, smoking, and alcohol. Get regular sleep and eat properly. Remain physically active, but avoid excessive fatigue. Consult your otolaryngologist about other treatment options.
Meniere’s disease outlook (prognosis)
Scientists estimate that six out of 10 people either get better on their own or can control their vertigo with diet, drugs, or devices. However, a small group of people with Ménière’s disease will get relief only by undergoing surgery.
Meniere’s disease complications
The unpredictable episodes of vertigo and the prospect of permanent hearing loss can be the most difficult problems of Meniere’s disease. The disease can interrupt your life and cause fatigue, emotional stress, depression and anxiety.
Vertigo can cause you to lose balance, increasing your risk of falls and accidents while driving or operating heavy machinery.
Meniere’s disease symptoms
- Recurring episodes of vertigo. You have dizziness with a spinning sensation that starts and stops spontaneously. Episodes of vertigo occur without warning and usually last 20 minutes to several hours, but not more than 24 hours. Severe vertigo can cause nausea and vomiting.
- Hearing loss. Hearing loss in Meniere’s disease may come and go, particularly early on. Eventually, most people have some permanent hearing loss.
- Ringing in the ear (tinnitus). Tinnitus is the perception of a ringing, buzzing, roaring, whistling or hissing sound in your ear.
- Feeling of fullness in the ear. People with Meniere’s disease often feel pressure in the affected ears (aural fullness) or on the side of their heads.
- Feeling unsteady on your feet
- Feeling sick or vomit
- Hear ringing, roaring or buzzing inside the ear
- Have a sudden drop in hearing
These symptoms, which typically happen all at once, can last minutes or hours, but most commonly last two to three hours.
The condition usually starts in one ear, but can spread to both ears over time.
It can take a day or two for the symptoms to disappear completely. You may feel tired after an attack.
Symptoms vary from person to person, but an attack of hearing loss without vertigo is uncommon.
Attacks can occur in clusters or several times a week, or they may be separated by weeks, months or years.
See your doctor if you think you may have Meniere’s disease. It can lead to permanent hearing loss if it’s not treated.
Meniere’s disease diagnosis
Your doctor should refer you to see an ear, nose and throat (ENT) specialist to confirm whether or not you have Meniere’s disease.
Your doctor will conduct an exam and take a medical history.
A diagnosis of Meniere’s disease requires:
- Two episodes of vertigo, each lasting 20 minutes or longer but not longer than 24 hours
- Hearing loss verified by a hearing test
- Tinnitus or a feeling of fullness in your ear
- Exclusion of other known causes of these problems
The ENT specialist will check you have:
- vertigo – at least two attacks lasting 20 minutes within a short space of time
- fluctuating hearing loss – confirmed by a hearing test
- tinnitus or a feeling of pressure in your ear
Your doctor or specialist may also carry out a general physical examination and blood tests to rule out other possible causes of your symptoms.
Meniere’s disease can be confused with conditions with similar symptoms, such as:
- migraine
- ear infection
- vestibular neuronitis
- labyrinthitis
Hearing assessment
A hearing test (audiometry) assesses how well you detect sounds at different pitches and volumes and how well you distinguish between similar-sounding words. People with Meniere’s disease typically have problems hearing low frequencies or combined high and low frequencies with normal hearing in the mid frequencies.
Balance assessment
Between episodes of vertigo, the sense of balance returns to normal for most people with Meniere’s disease. But you might have some ongoing balance problems.
Tests that assess function of the inner ear include:
- Videonystagmography. This test evaluates balance function by assessing eye movement. Balance-related sensors in the inner ear are linked to muscles that control eye movement. This connection enables you to move your head while keeping your eyes focused on a point. In a videonystagmography evaluation, warm and cool water or warm and cool air are introduced into the ear canal. Measurements of involuntary eye movements in response to this stimulation are performed using a special pair of video goggles.
- Rotary-chair testing. Like a videonystagmography , this measures inner ear function based on eye movement. You sit in a computer-controlled rotating chair, which stimulates your inner ear.
- Vestibular evoked myogenic potentials testing. This newer test shows promise for not only diagnosing, but also monitoring Meniere’s disease. It shows characteristic changes in the affected ears of people with Meniere’s disease.
- Posturography. This computerized test reveals which part of the balance system — vision, inner ear function, or sensations from the skin, muscles, tendons and joints — you rely on the most and which parts may cause problems. While wearing a safety harness, you stand in bare feet on a platform and keep your balance under various conditions.
- Video head impulse test. This newer test uses video to measure eye reactions to abrupt movement. While you focus on a point, your head is turned quickly and unpredictably. If your eyes move off the target when your head is turned, you have an abnormal reflex.
- Electrocochleography. This test looks at the inner ear in response to sounds. It might help to determine if there is an abnormal buildup of fluid in the inner ear, but isn’t specific for Meniere’s disease.
- The auditory brain stem response (ABR), a computerized test of the hearing nerves and brain pathways.
Tests to rule out other conditions
Blood tests and others may be used to rule out disorders that can cause problems similar to those of Meniere’s disease, such as a tumor in the brain or multiple sclerosis. An imaging test, such as an MRI, also might be used.
Meniere’s disease treatment
No cure exists for Meniere’s disease, but medication can help you control vertigo, nausea and vomiting.
There are no treatments for the hearing loss that occurs with Meniere’s disease. All of the treatments — some conservative, some aggressive — are to stop the spells of vertigo.
Medications for vertigo
The three medicines usually recommended by doctors are:
- Prochlorperazine or promethazine – helps relieve severe nausea and vomiting
- Antihistamines – help relieve mild nausea, vomiting and vertigo
- Motion sickness medications, such as meclizine or diazepam (Valium), may reduce the spinning sensation and help control nausea and vomiting.
The aim is to get the medicine into the body as soon as possible at the first sign of any symptoms.
If these medicines work, your doctor may give you a supply to keep for you to take quickly during an attack.
Long-term medication use
Your doctor may prescribe a medication to reduce fluid retention (diuretic). For some people, a diuretic helps control the severity and frequency of Meniere’s disease symptoms. A diuretic is usually combined with limiting dietary salt intake.
You may also need treatment for:
- tinnitus
- hearing loss
- loss of balance (vestibular rehabilitation)
Distress is common in people with Meniere’s disease, as it’s difficult and unpredictable.
Your doctor can offer advice and support if you’re finding it difficult to cope with the effect Meniere’s disease is having on your life.
You may be offered:
- Counseling – including cognitive behavioural therapy (CBT)
- Relaxation therapy – including breathing techniques and yoga
There are also a number of support groups, such as the Meniere’s Society, that can provide assistance and advice.
What to do during an attack
Vertigo can cause you to lose balance. At the first sign of it:
- take your medication
- sit or lie down and focus on an unmoving object. Often people fall asleep while lying down and feel better when they awaken.
- close your eyes, or keep them fixed on an object in front of you
- don’t turn your head quickly
- if you need to move, do so slowly and carefully
Once the attack is over, try to move around to help your eyesight and other senses compensate for the problems in your inner ear.
Treating severe attacks
You may be advised to have prochlorperazine or promethazine as an injection instead of a tablet for quicker action to deal with severe symptoms.
In rare cases, you may need to be admitted to hospital to receive fluids through a vein to keep you hydrated.
Surgery
Surgery may be an option to control vertigo in severe cases, but it’s usually only considered if other treatments have failed.
There are very few clinical trials that have looked at the effectiveness of surgery for Meniere’s disease, which is why it’s rarely used.
Surgical procedures include:
- Endolymphatic sac procedure. The endolymphatic sac plays a role in regulating inner ear fluid levels. These surgical procedures may alleviate vertigo by decreasing fluid production or increasing fluid absorption. In endolymphatic sac decompression, a small portion of bone is removed from over the endolymphatic sac. In some cases, this procedure is coupled with the placement of a shunt, a tube that drains excess fluid from your inner ear. Endolymphatic sac shunt or decompression procedure relieves attacks of vertigo in one-half to two-thirds of cases and the sensation of ear fullness is often improved. Control is often temporary. Endolymphatic sac surgery does not improve hearing, but only has a small risk of worsening it. Recovery time after this procedure is short compared to the other procedures.
- Vestibular nerve section. This procedure involves cutting the nerve that connects balance and movement sensors in your inner ear to the brain (vestibular nerve). This procedure usually corrects problems with vertigo while attempting to preserve hearing in the affected ear. It requires general anesthesia and an overnight hospital stay. While vertigo attacks are permanently cured in a high percentage of cases, patients may continue to experience imbalance. Similar to endolymphatic sac procedures, hearing function is usually preserved.
- Labyrinthectomy and eighth nerve section. With this procedure, the surgeon removes both the balance portion of the inner ear and hearing function from the affected ear. This procedure is performed only if you already have near-total or total hearing loss in your affected ear. Labryrinthectomy and eighth nerve section result in the highest rates for control of vertigo attacks.
Noninvasive therapies and procedures
Some people with Meniere’s may benefit from other noninvasive therapies and procedures, such as:
- Rehabilitation. If you have balance problems between episodes of vertigo, vestibular rehabilitation therapy might improve your balance.
- Hearing aid. A hearing aid in the ear affected by Meniere’s disease might improve your hearing. Your doctor can refer you to an audiologist to discuss what hearing aid options would be best for you.
- Meniett device. For vertigo that’s hard to treat, this therapy involves applying pressure to the middle ear to improve fluid exchange. A device called a Meniett pulse generator applies pulses of pressure to the ear canal through a ventilation tube. You do the treatment at home, usually three times a day for five minutes at a time. Initial reports on the Meniett device show improvement in symptoms of vertigo, tinnitus and aural pressure, but its long-term effectiveness has not been determined.
If the conservative treatments listed above aren’t successful, your doctor might recommend some of these more aggressive treatments.
Middle ear injections
Medications injected into the middle ear, and then absorbed into the inner ear, may improve vertigo symptoms:
- Gentamicin, an antibiotic that’s toxic to your inner ear, reduces the balancing function of your ear, and your other ear assumes responsibility for balance. The procedure, which can be performed during local anesthesia in your doctor’s office, often reduces the frequency and severity of vertigo attacks. There is a risk, however, of further hearing loss.
- Steroids, such as dexamethasone, also may help control vertigo attacks in some people. This procedure can also be performed with local anesthesia applied by your doctor. Although dexamethasone may be slightly less effective than gentamicin, dexamethasone is less likely than gentamicin to cause further hearing loss.
Prevention
Medication
Your doctor may recommend a medication called betahistine to help reduce the frequency and severity of attacks of Meniere’s disease.
Betahistine is thought to reduce the pressure of the fluid in your inner ear, relieving symptoms of hearing loss, tinnitus and vertigo.
Meniere’s disease diet
There isn’t much proof that changes to your diet can help.
But some people claim their symptoms improve by:
- eating a low-salt diet
- avoiding alcohol
- avoiding caffeine
- stopping smoking
Salt and stress can affect hearing and balance. To avoid triggering a vertigo attack, try the following:
- Limit salt. Consuming foods and beverages high in salt can increase fluid retention. Aim for 1,500 to 2,000 milligrams of sodium each day and spread your salt intake evenly throughout the day.
- Manage stress. Managing stress might lessen the severity of symptoms and help you cope with Meniere’s disease. Psychotherapy can help you identify stressors and develop strategies for coping with your condition.
Home remedies for Meniere’s disease
Certain self-care tactics can help reduce the impact of Meniere’s disease. Consider these tips for use during an episode:
- Sit or lie down when you feel dizzy. During an episode of vertigo, avoid things that can make your signs and symptoms worse, such as sudden movement, bright lights, watching television or reading.
- Rest during and after attacks. Don’t rush to return to your normal activities.
- Be aware you might lose your balance. Falling could lead to serious injury. Use good lighting if you get up in the night. Consider walking with a cane for stability if you have chronic balance problems.
- Avoid driving a car or operating heavy machinery if you have frequent episodes of vertigo. Doing so could lead to an accident and injury.
Driving and other risks
You can’t predict your next attack, so you may need to change how you do things to avoid placing yourself or others in danger.
Consider the risks before doing activities like:
- driving
- swimming
- climbing ladders or scaffolding
- operating heavy machinery
You may also need to make sure someone’s with you most of the time in case you need help during an attack.
Driving
You shouldn’t drive when you feel dizzy or if you feel an attack of vertigo coming on.
It’s likely that you won’t be allowed to continue driving until you have control of your symptoms.
Flying
Most people with Meniere’s disease have no difficulty with flying.
These tips can help take the stress out of flying, which may reduce the risk of an attack:
- get an aisle seat if you’re worried about vertigo – you’ll be away from the window and will have quicker access to the toilets
- sit away from the plane’s engines if noise and vibration are an issue
- drink water regularly to stay hydrated and avoid alcohol
- ask if the airline has any special diets that suit your needs.





{kind=link}