
Contents
What is ischemic colitis
Ischemic colitis is a form of bowel disorder caused by ischemia (inadequate blood flow) to the colon (see Figures 1 and 2 below). In response to lack of blood, the colon becomes inflamed and causes symptoms such as fecal urgency and bloody diarrhea. The condition is often temporary and resolves without treatment. However, the inflammation can cause permanent damage to the colon. It is important to seek medical advice if you experience symptoms suggestive of ischemic colitis.
Ischemic colitis is a common disorder of the large bowel with an average incidence of 16.5 cases per 100,000 hospital admissions. Ischemic colitis is frequently seen in older patients with a peak incidence in the 7th decade and is the most common form of intestinal ischemic injury. Women are affected more than men. Ischemic colitis accounts for about 50–60% of all gastrointestinal ischemic episodes, most often in the absence of major vessel occlusion 1. Ischemic colitis is a result of inadequate blood flow to the colon, causing mucosal injury that is mediated by hypoxia, followed by reperfusion injury 2. The pattern of injury is usually segmental, mainly involving the “watershed” zones of the splenic flexure, descending colon, and the rectosigmoid junction; however, any part of the colon can be affected, including isolated right-sided colon, which carries a higher morbidity and mortality rate 3. Ischemic colitis presentations are highly variable, making diagnosis and management clinically challenging 4. Because the presentation of colon ischemia is nonspecific and patients with colon ischemia usually are not severely ill, the disease often is not diagnosed or misdiagnosed as another occurrence such as Crohn’s disease, diverticulitis, or infectious colitis. Common clinical manifestations include sudden presentation of mild-to-moderate abdominal pain that is usually located over the affected area of the colon, followed by bloody diarrhea 2. The severity of clinical symptoms varies, including fever, diarrhea, peritonitis, and septic shock, depending on the extent of colonic injury.
Clinically, the disease process varies from self-limiting and transient to fulminant and life-threatening 5. In the more common and milder form of ischemic colitis, only the mucosa and submucosa are affected and most of these occurrences resolve spontaneously or with just conservative measures. In contrast, the severe forms of colon ischemia are marked by transmural necrosis of the bowel, often requiring surgery and frequently leading to death 6.
Any part of the colon may be affected by ischemia and isolated right colon ischemia has been reported to occur in about 10% of cases 7. Isolated right colon ischemia, however, also may be the heralding event of otherwise clinically silent focal obstruction or vasoconstriction of the superior mesenteric artery (see Figure 2 below), because the superior mesenteric artery constitutes the blood supply of both the small intestine and much of the colon, including the right side. Over many years, scientists have observed that several patients with isolated right colon ischemia have developed acute mesenteric ischemia within weeks of their presentation with colon ischemia; acute mesenteric ischemia has a high mortality and requires different management than does colon ischemia 8. In contrast to colon ischemia for which mesenteric angiography generally is not helpful and which responds to conservative medical treatment in most cases, acute mesenteric ischemia benefits from an aggressive diagnostic and therapeutic approach utilizing mesenteric angiography and intrarterial infusion of vasodilators in combination with surgery. The mortality rate of acute mesenteric ischemia is 70–90% when managed by surgery alone and approximately 50% when an aggressive management plan is utilized 9. Thus, it can be questioned whether isolated right colon ischemia should be considered an emergency situation with a potentially grave prognosis just as is acute mesenteric ischemia. To date, only a few studies have documented isolated right colon ischemia to be among the more severe forms of colon ischemia: one showed it to be associated with hemodialysis and chronic renal failure, while the others showed it to occur with increased frequency in patients with shock 10; situations precipitating isolated right colon ischemia usually are associated with reductions in circulating blood volume, marked fluid shifts, and hypotension, thereby potentially causing superior mesenteric artery vasoconstriction.
Seek immediate medical care if you have sudden, severe abdominal pain. Abdominal pain that makes you so uncomfortable that you can’t sit still or find a comfortable position is a medical emergency.
Contact your doctor if you develop worrisome signs and symptoms, such as bloody diarrhea. Early diagnosis and treatment can help prevent serious complications.
Large intestine
The large intestine extends from the distal end of the ileum to the anus, a distance of approximately 1.5 m in adults (5 ft) long and 6.5 cm (2.5 in.) in diameter. The large intestine is named for its relatively large diameter, not its length. The large intestine absorbs fluids and salts from the gut contents, thus forming feces. The large intestine consists of the cecum, appendix, colon, rectum, and anal canal.
Beginning in the right groin as the cecum, with its associated appendix, the large intestine continues upward as the ascending colon through the right flank and into the right hypochondrium. The ascending colon begins at the ileocecal valve and passes up the right side of the abdominal cavity. It makes a 90° turn at the right colic (hepatic) flexure, near the right lobe of the liver, and crosses the abdomen as the transverse colon to the left hypochondrium. At this position, just below the spleen, the large intestine bends downward, forming the left colic flexure (splenic flexure) and continues as the descending colon through the left flank and into the left groin. Ascending, transverse, and descending colons thus form a squarish, three-sided frame around the small intestine.
The cecum is a blind pouch in the lower right abdominal quadrant inferior to the ileocecal valve. Attached to its lower end is the appendix, a blind tube 2 to 7 cm long. The appendix is densely populated with lymphocytes and is a significant source of immune cells.
Figure 1. Large intestine
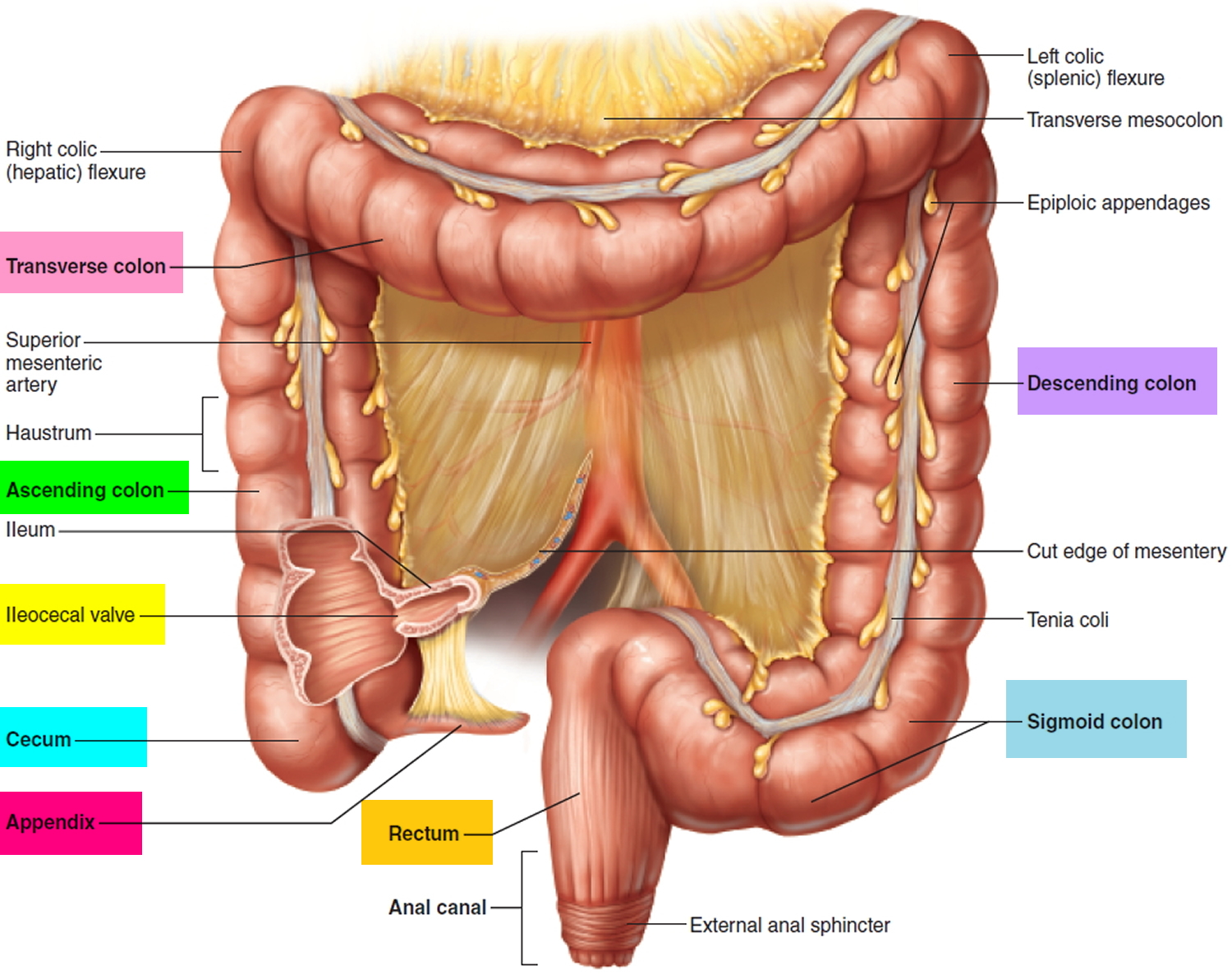 Figure 2. Large intestine blood supply – the two main arteries that supply blood to the colon are the superior mesenteric artery and the inferior mesenteric artery.
Figure 2. Large intestine blood supply – the two main arteries that supply blood to the colon are the superior mesenteric artery and the inferior mesenteric artery.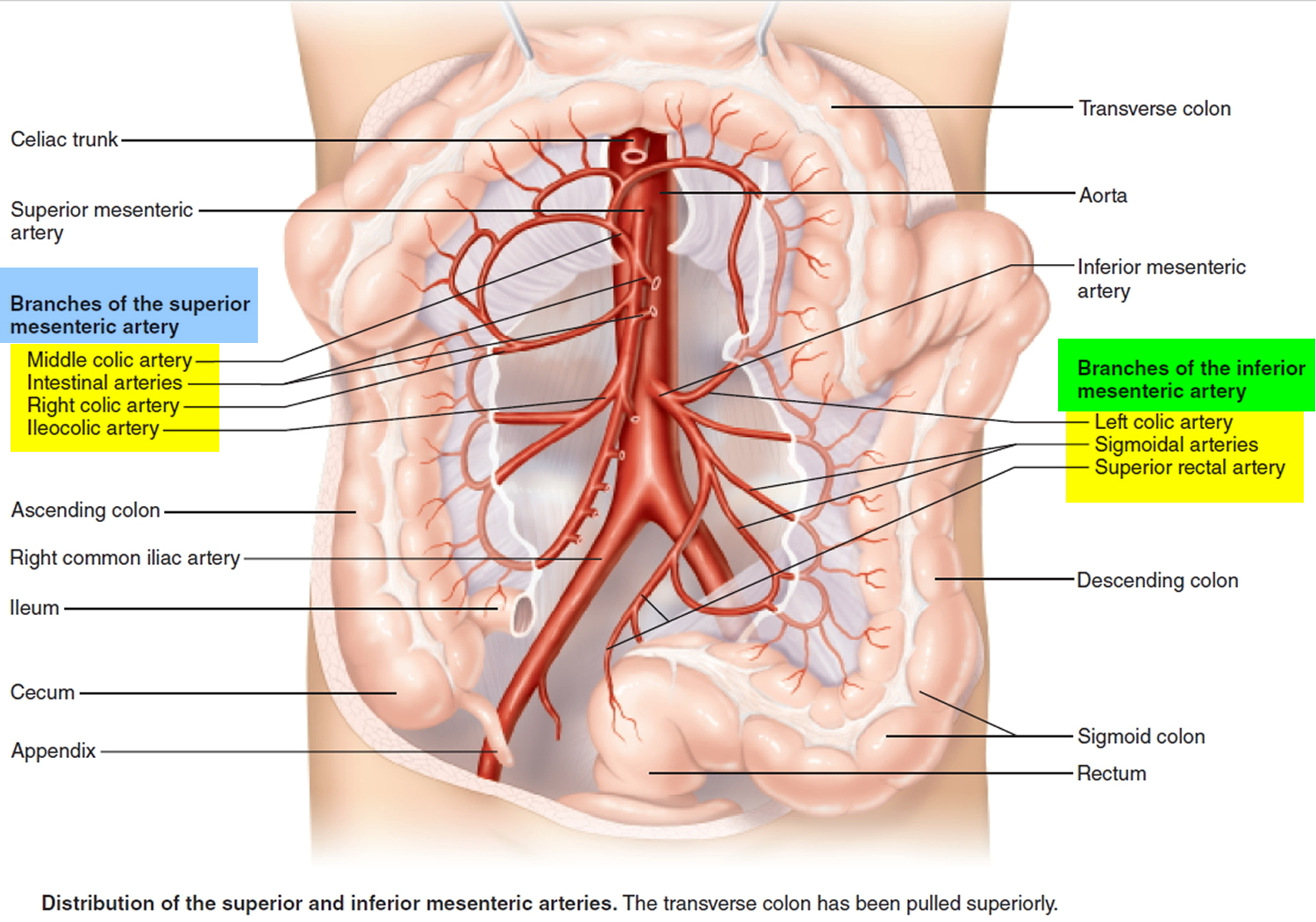
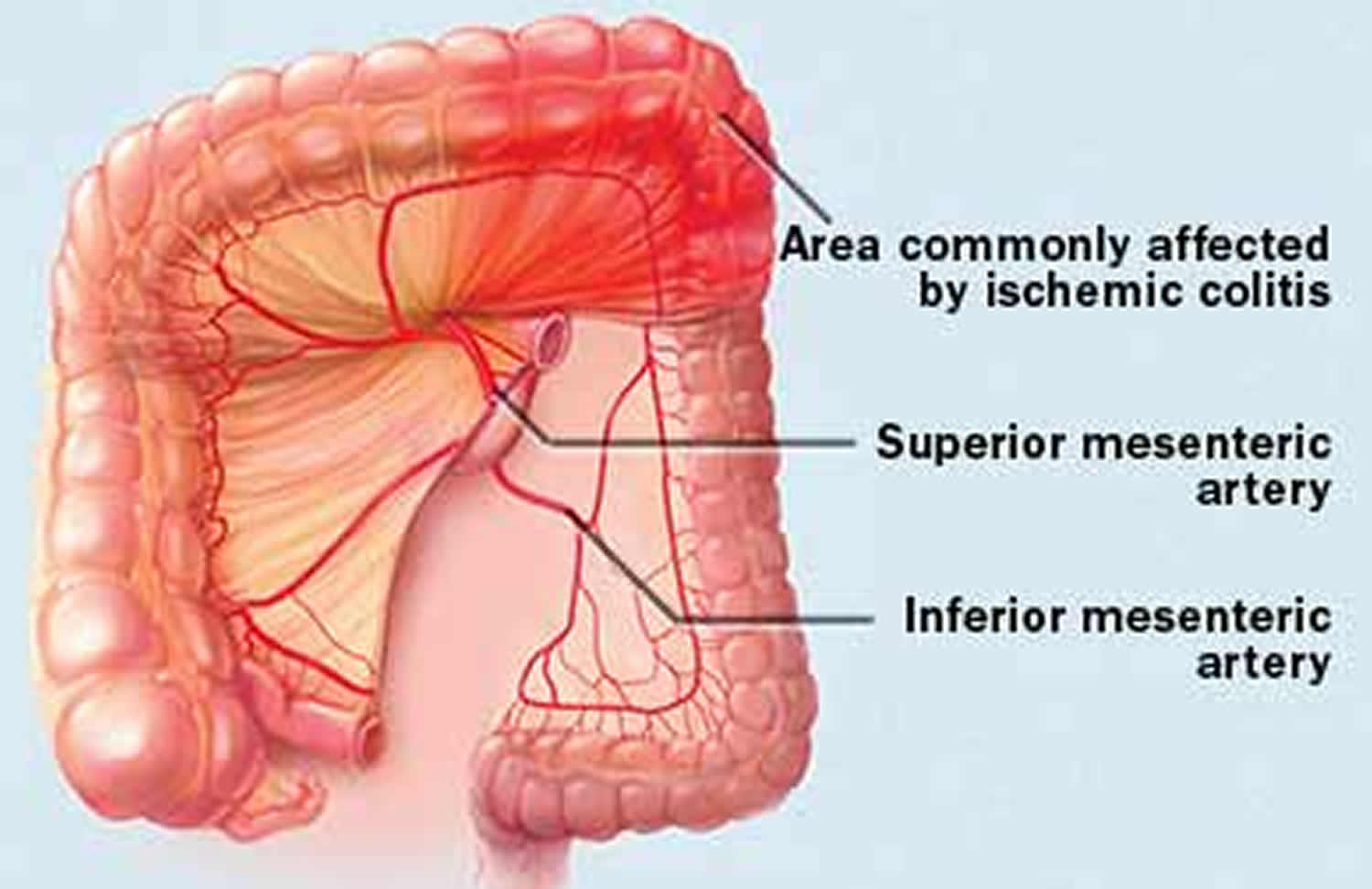
Figure 3. Ischemic colitis area commonly affected by ischemic colitis
Ischemic colitis vs Mesenteric ischemia
Mesenteric ischemia is a condition caused by poor blood supply to your intestines. Mesenteric ischemia usually affects the small intestine, colon or both. It may also involve other organs in the digestive system. Mesenteric ischemia represents an abdominal emergency accounting for approximately 2% of gastrointestinal illnesses 11. Despite recent advances in surgery and intensive therapy its mortality remains very high, ranging between 50-90% 12. Patients survival is dependent on prompt recognition and treatment before ischemia progresses to intestinal gangrene 13.
Mesenteric ischemia patients typically present in their 60s to 70s and often have a number of medical comorbidities. In case of acute blockage of the mesenteric artery, abdominal pain is the most common presenting symptom (94%) and patients usually complain of abdominal pain out of proportion to the abdominal examination. Other symptoms include nausea (56%), vomiting (38%), diarrhea (31%), and tachycardia (31%). In advanced phase, the patient develops peritoneal signs of distention, guarding, rigidity, and hypotension 14.
Mesenteric ischemia may be acute or chronic.
Acute mesenteric ischemia occurs suddenly as a result of blockage to the flow of oxygen-rich blood and can permanently damage your intestines. You may experience sudden abdominal pain and, less often, bloody stools. This situation requires immediate medical care.
Chronic mesenteric ischemia occurs gradually from narrowing in one or more of the arteries supplying blood to your intestines (visceral arteries). You may develop pain 1 to 2 hours after eating, This pain may make it hard for you to eat, leading to weight loss. You may also notice changes in the frequency of your bowel movements, as well as bloating, nausea and vomiting.
At least the 65% of cases of intestinal ischemia are due to arterial embolism or thrombosis with blood flow impairment in the superior mesenteric artery distribution affecting all or portions of the small bowel and right colon 15. Most embolic events are thromboembolic in nature and arise from a cardiac source. Risk for a thromboembolic event include atrial tachyarrythmias, low ejection fraction (congestive heart failure, cardiomyopathy), recent myocardial ischemia or infarction, and ventricular aneurysms 16.
Mesenteric ischemia diagnosis
Diagnosis of mesenteric ischemia begins with a description of your current symptoms, a medical history, physical exam and blood tests. Your doctor will ask you questions about your symptoms. You may also need an evaluation by a gastroenterologist.
As part of the diagnosis, doctors who specialize in the interpretation of medical images (radiologists) may perform tests to rule out other conditions and evaluate blood flow, including:
- Doppler ultrasound. High-frequency sound waves help your doctor see images of your blood vessels.
- CT scan/CT angiography. A CT scan uses X-rays to create detailed images of your arteries and of some organs. A CT angiogram (CTA) is a noninvasive way for doctors to see the details of your blood vessels, including narrowing and blockages.
- Magnetic resonance angiography (MRA). Magnetic fields and radio waves produce detailed images of your blood vessels.
- Mesenteric angiogram. A mesenteric angiogram is the standard test for evaluating blood flow and finding the blockage in the blood vessel. In this test, your doctor guides a thin, flexible tube (catheter) through the artery and inserts a dye to make the artery visible on an X-ray. Sometimes the doctor can treat the blocked arteries with a balloon angioplasty or stent during the angiogram.
Computed tomography angiography has surpassed angiography as the diagnostic test of choice and represents the gold standard due to its ability to define the arterial anatomy and to evaluate secondary signs of mesenteric ischemia, with sensitivity ranging from 82% to 96% and specificity of 94% 17.
Mesenteric ischemia treatment
The most appropriate treatment depends on the severity of your symptoms, the cause and extent of your artery blockage, and your other medical conditions. Lifestyle changes such as switching to a healthy diet, exercising and stopping smoking are important parts of treatment.
Acute mesenteric ischemia is a medical emergency and requires immediate treatment. Unlike chronic mesenteric ischemia, the treatment of acute mesenteric ischemia remains largely surgical. This is due to the emergent need for revascularization combined with an assessment of bowel viability 16. An alternative approach might consist in injecting the patients with autologous endothelial progenitor cells, to accelerate tissue revascularization and prevent a surgical approach 18.
Medication
If you have rapidly progressing (acute) mesenteric ischemia or blood clots in your intestinal veins (mesenteric venous thrombosis) you may need drugs to help prevent blood clots (anticoagulants).
Interventional procedures and surgery
Once your doctor determines that your stomach pain is caused by blocked intestinal arteries, you may need surgery. Doctors usually perform conventional and minimally invasive procedures to improve blood flow to your intestines.
Options include:
- Angioplasty (with or without stenting). Angioplasty is a minimally invasive procedure that opens narrowed arteries. This procedure is also called endovascular revascularization. During an angioplasty, your doctor inserts a long, flexible tube (catheter) that has a balloon on its tip and when inflated will open the narrowed blood vessel. The surgeon usually places a small wire tube (stent) in your artery to keep it open. If you have a blood clot, your doctor may remove it during your angiogram.
- Mesenteric artery bypass. A bypass creates an alternate route for blood to flow around the narrowed or blocked artery. Your surgeon sews a substitute blood vessel (graft) to a main artery to restore blood flow.
- Mesenteric endarterectomy. In an endarterectomy, your doctor makes an incision in the large blood vessel that branches off your heart (aorta) to reach the mesenteric arteries and remove fat and cholesterol buildup (plaques) or the blood clot blocking the artery.
Doctors generally recommend treatment for everyone with chronic mesenteric ischemia. Specific treatment depends on the extent of the blood vessel blockage and your overall health.
Ischemic colitis complications
Ischemic colitis usually gets better on its own within two to three days. In more-severe cases, complications can include:
- Tissue death (gangrene) resulting from diminished blood flow
- Hole (perforation) in your intestine or persistent bleeding
- Bowel inflammation (segmented ulcerating colitis)
- Bowel obstruction (ischemic stricture)
Ischemic colitis causes
What causes ischemic colitis
The precise cause of diminished blood flow to the colon isn’t always clear. But several factors can increase your risk of ischemic colitis:
- Buildup of fatty deposits on the walls of an artery (atherosclerosis)
- Dangerously low blood pressure (hypotension) associated with heart failure, major surgery, trauma or shock
- A blood clot in an artery supplying the colon or, less commonly, in a vein (venous thrombosis)
- Bowel obstruction caused by a hernia, scar tissue or a tumor
- Surgery involving the heart or blood vessels, or the digestive or gynecological systems
- Other medical disorders that affect your blood, such as inflammation of the blood vessels (vasculitis), lupus or sickle cell anemia
- Cocaine or methamphetamine use
- Colon cancer (rare)
The role of medications
Certain medicines also can lead to ischemic colitis, though this is rare. They include:
- Some heart and migraine medications
- Hormone medications, such as estrogen
- Antibiotics
- Pseudoephedrine
- Certain medications for irritable bowel syndrome
- Chemotherapy medications
Risk factors for ischemic colitis
Risk factors for ischemic colitis include:
- Age. The condition occurs mostly frequently in adults older than age 60. Ischemic colitis that occurs in a young adult may be a sign of a blood-clotting abnormality or inflammation of the blood vessels (vasculitis).
- Clotting abnormalities. Conditions that affect the way the blood clots, such as Factor V Leiden, may increase the risk of ischemic colitis.
- High cholesterol, which can lead to atherosclerosis.
- Reduced blood flow, due to heart failure, low blood pressure and shock.
- Previous abdominal surgery. Scar tissue that forms after surgery may cause reduced blood flow.
- Heavy exercise, such as marathon running, which can lead to reduced blood flow to the colon.
- Surgery involving the large artery (aorta) that pumps blood from your heart to the rest of your body.
Ischemic colitis prevention
Since the cause of ischemic colitis isn’t always clear, there’s no certain way to prevent the disorder. Most people who have ischemic colitis recover quickly and may never have another episode.
To prevent recurrent episodes of ischemic colitis, your doctor may recommend eliminating any medication that might cause ischemic colitis. He or she may also test for clotting abnormalities, especially if no other cause for ischemic colitis was apparent.
Ischemic colitis symptoms
Signs and symptoms of ischemic colitis can include:
- Pain, tenderness or cramping in your belly, which can occur suddenly or gradually
- Bright red or maroon-colored blood in your stool or, at times, passage of blood alone without stool
- A feeling of urgency to move your bowels
- Diarrhea
- Nausea
The risk of severe complications is higher when you have symptoms on the right side of your abdomen. That’s because the arteries that feed the right side of your colon also feed part of your small intestine, and may be blocked too. Pain tends to be more severe with this type of ischemic colitis.
Blocked blood flow to the small intestine can quickly lead to death of intestinal tissue (necrosis). If this life-threatening situation occurs, you’ll need surgery to clear the blockage and to remove the portion of the intestine that has been damaged.
Ischemic colitis diagnosis
Ischemic colitis can often be confused with other disorders because their symptoms overlap, especially inflammatory bowel disease (IBD). Based on your signs and symptoms, your doctor may recommend these imaging tests:
- Ultrasound and abdominal CT scans, to provide images of your colon that can be helpful in ruling out other disorders, such as inflammatory bowel disease (IBD).
- Stool analysis, to rule out infection as a cause of your symptoms.
- CT or MRI angiography, to provide detailed images of blood flow in your small intestine and to look for blocked arteries. This test is usually used only if ischemia is suspected in your small bowel as well as in your colon.
- Colonoscopy. This test, which provides detailed images of your colon, can be helpful in diagnosing ischemic colitis. Colonoscopy can also be used to check for cancer, and to see how well a treatment worked.
Ischemic colitis treatment
Treatment for ischemic colitis depends on the severity of your condition.
Signs and symptoms often diminish in two to three days in mild cases. But your doctor may recommend:
- Antibiotics, to prevent infections
- Intravenous fluids, if you are dehydrated
- Treatment for any underlying medical condition, such as congestive heart failure or an irregular heartbeat
- Avoiding medications that constrict your blood vessels, such as migraine drugs, hormone medications and some heart drugs
Your doctor will schedule follow-up colonoscopies to monitor healing and look for complications.
Surgery
While most cases resolve on their own, if your symptoms are severe, or your colon has been damaged, you may need surgery to:
- Remove dead tissue
- Repair a hole in your colon
- Bypass a blockage in an intestinal artery
- Remove part of the colon that has narrowed because of scarring and is causing a blockage
The likelihood of surgery may be higher if you have an underlying condition, such as heart disease or low blood pressure.
- Brandt LJ, Feuerstadt P, Blaszka MC. Anatomic patterns, patient characteristics, and clinical outcomes in ischemic colitis: A study of 313 cases supported by histology. Am J Gastroenterol. 2010;105(10):2245–52. https://www.nature.com/articles/ajg2010217[↩]
- Zou X, Cao J, Yao Y, et al. Endoscopic findings and clinicopathologic characteristics of ischemic colitis: A report of 85 cases. Dig Dis Sci. 2009;54(9):2009–15. https://link.springer.com/article/10.1007%2Fs10620-008-0579-1[↩][↩]
- Sotiriadis, J, Brandt LJ, Behin DS, Southern WN. Ischemic colitis has a worse prognosis when isolated to the right side of the colon. Am J Gastroenterol. 2007;102(10):2247–52. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2805903/[↩]
- Sreenarasimhaiah J. Diagnosis and management of ischemic colitis. Curr Gastroenterol Rep. 2005;7:421–426. https://www.ncbi.nlm.nih.gov/pubmed/16168242[↩]
- Brandt LJ. Intestinal ischemia. In: Feldman M, Friedman L, Brandt LJ, editors. Sleisenger & Fordtran’s gastrointestinal and liver disease: Pathophysiology, diagnosis, management. Philadelphia: Elsevier; 2006. pp. 2563–2586.[↩]
- Mitsudo S, Brandt LJ. Pathology of intestinal ischemia. Surg Clin North Am. 1992;72:43–63. https://www.ncbi.nlm.nih.gov/pubmed/1731389[↩]
- Brandt LJ, Boley SJ. Colonic ischemia. Surg Clin North Am. 1992;72:203–229. https://www.ncbi.nlm.nih.gov/pubmed/1731384[↩]
- Robert JH, Mentha G, Rohner A. Ischaemic colitis: two distinct patterns of severity. Gut. 1993;34(1):4-6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1374090/pdf/gut00552-0012.pdf[↩]
- Brandt LJ, Boley SJ. AGA technical review on intestinal ischemia. American Gastrointestinal Association. Gastroenterology. 2000;118:954–968. https://www.ncbi.nlm.nih.gov/pubmed/10784596[↩]
- Flobert C, Cellier C, Berger A, et al. Right colonic involvement is associated with severe forms of ischemic colitis and occurs frequently in patients with chronic renal failure requiring hemodialysis. Am J Gastroenterol. 2000;95:195–198. https://www.ncbi.nlm.nih.gov/pubmed/10638582[↩]
- Mazzei MA, Mazzei FG, Marrelli D, Imbriaco G, Guerrini S, Vindigni C, Civitelli S, Roviello F, Grassi R, Volterrani L. Computed tomographic evaluation of mesentery: diagnostic value in acute mesenteric ischemia. J Comput Assist Tomogr. 2012;36(1):1–7. Jan-Feb. https://www.ncbi.nlm.nih.gov/pubmed/22261763[↩]
- A Elder K, Lashner BA, Solaiman FAL. Clinical approach to colonic ischemia. Cleveland Clinic Journal of medicine. 2009;76(7):401–409. https://www.ncbi.nlm.nih.gov/pubmed/19570972[↩]
- Wyers MC. Acute mesenteric ischemia: diagnostic approach and surgical treatment. Seminars in vascular surgery. 2010;23(1):9–20. Mar. https://www.ncbi.nlm.nih.gov/pubmed/20298945[↩]
- Paterno F, Longo WE. The etiology and pathogenesis of vascular disorders of the intestine. Radiol Clin North Am. 2008;46(5):877–85. Sep. https://www.ncbi.nlm.nih.gov/pubmed/19103137[↩]
- Gore RM, Yaghmai V, Thakrar KH, Berlin JW, Mehta UK, Newmark GM, Miller FH. Imaging in Intestinal Ischemic Disorders. Radiologic Clinics of North America. 2008;46(5):845–875. https://www.ncbi.nlm.nih.gov/pubmed/19103136[↩]
- Wiesner W, Khurana B, Ji H, Ros PR. CT of acute bowel ischemia. Radiology. 2003;226:635–650. https://www.ncbi.nlm.nih.gov/pubmed/12601205[↩][↩]
- Wasnik A, Kaza RK, Al-Hawary MM, Liu PS, Platt JF. Multidetector CT imaging in mesenteric ischemia–pearls and pitfalls. Emergency radiology. 2011;18(2):145–56. https://www.ncbi.nlm.nih.gov/pubmed/21132342[↩]
- Moccia F, Bonetti E, Dragoni S, Fontana J, Lodola F, Berra Romani R, Laforenza U, Rosti V, Tanzi F. Hematopoietic progenitor and stem cells circulate by surfing on intracellular Ca2+ waves: A novel target for cell-based therapy and anti-cancer treatment? Curr Signal Transd T. 2012;7(2):161–176.[↩]





{kind=link}