Contents
What is calciphylaxis
Calciphylaxis is called calcific uremic arteriolopathy, is a disease in which blood vessels (veins and arteries) become blocked by a build-up of calcium in the walls of the vessels, preventing blood from flowing to the skin or internal organs. The lack of blood flow (ischemia) damages healthy tissue and causes it to die (necrosis). Calciphylaxis is a condition characterized by necrosis (cellular death) of the skin and fatty tissue. Calciphylaxis predominantly affects chronic kidney failure (end stage kidney disease) patients treated by dialysis 1. However, calciphylaxis is not limited to patients treated by dialysis and also occurs in patients with normal kidney function and in those with earlier stages of chronic kidney disease (referred to as non-uremic calciphylaxis) 2. Both uremic and non-uremic calciphylaxis are associated with significant morbidity and mortality. The morbidity is related to severe pain, non-healing wounds, recurrent hospitalizations, and to adverse effects of treatments. Some studies also report that the incidence of calciphylaxis is increasing in dialysis population; however, whether this is truly an increase in incidence or enhanced awareness remains unclear 3.
Calciphylaxis is most commonly reported in patients in the 5th decade of life; however it has also been described in patients significantly younger including children 4. Calciphylaxis is more commonly seen in women compared to men with a 2:1 female predominance 5. Calciphylaxis as reported in the literature is also more common in whites compared to non-whites 6. The biological explanation for these observations is unclear.
The most obvious and frequent symptom of calciphylaxis is damage to the skin, as ulcers can develop and become infected easily. Calciphylaxis clinically presents with severe painful skin lesions (livedo reticularis, reticulate purpura, violaceous plaques, or indurated nodules) that demonstrate poor healing and are frequently complicated by blistering and ulcerations with superimposed infections (Figure 1) 2. Ulcerated lesions commonly demonstrate black eschar. Although, skin manifestations dominate the clinical presentation, calciphylaxis can also affect fat tissue, internal organs – brain, lungs, intestines, eyes, and mesentery, and skeletal muscle, causing infections, pain, and organ failure 7. In this regard, calciphylaxis can be considered as a continuum of a systemic process leading to arterial calcification in many vascular beds 8.
These symptoms are often irreversible, and many individuals with calciphylaxis may not survive more than a few months after they are diagnosed due to infection that spreads throughout the body (sepsis), or organ failure 9. The exact cause of calciphylaxis is unknown 10.
Histologically, calciphylaxis is characterized by calcification, microthrombosis, and fibrointimal hyperplasia of small dermal and subcutaneous arteries and arterioles leading to ischemia and intense septal panniculitis (Figure 3) 11. Calcification most commonly involves the medial layer of small arteries and arterioles; however, involvement of the intimal layer and the interstitium of subcutaneous adipose tissue has been reported 12. Calcification is considered to be an early and essential process in calciphylaxis plaque development and it is hypothesized that the vascular calcification leads to vascular endothelial dysfunction and injury 13. Despite the well characterized clinical and histological descriptions of calciphylaxis, its exact pathogenesis remains unclear and there is limited data regarding the diagnostic and therapeutic approaches for this devastating condition.
Treatments may include medications to reduce pain, antibiotics to treat infections, and various approaches to preventing the development or worsening of this condition 9.
Figure 1. Calciphylaxis wounds (calcific uremic arteriolopathy)

Figure 2. Calciphylaxis wounds

Calciphylaxis pathology
Calciphylaxis is seen almost exclusively in patients with end stage kidney disease. Calcification of vessels and soft tissue cause skin infarction and subsequent necrosis.
Professor Hans Selye and his colleagues coined the term calciphylaxis in 1961 14. Selye conducted laboratory experiments in rats to induce generalized subcutaneous soft tissue calcification by applying a 2-step process interrupted by a “critical time” period: 1) “Sensitization” by agents such as parathyroid extract, high dose vitamin D, high phosphorous diet, or induction of renal failure followed by, 2) Application of a “challenging agent” such as local trauma, egg albumin, or metallic salts. Development of cutaneous calcification in this animal model was thought to be an adaptive or phylactic reaction and was referred to as calciphylaxis (portmanteau of calcification and phylaxis).
It is important to understand the key differences between experimental calciphylaxis in Selye’s experimental model and human calciphylaxis. First and foremost, the animals in experimental calciphylaxis did not develop small artery or arteriolar calcifications although extensive soft tissue calcifications were present. Secondly, the animals in experimental calciphylaxis were able to cast off the calcified skin molt and replace it with new dermis that did not have any features of calciphylaxis. Thirdly, experimental calciphylaxis was prevented by administration of glucocorticosteroids, a fact that contradicts the available data in human calciphylaxis 15.
The differences between experimental calciphylaxis and human calciphylaxis, as well as a widely accepted recognition that calciphylaxis is not a hypersensitivity reaction, has led some authors to propose descriptive terms such as calcific uremic arteriolopathy for human calciphylaxis 12. Although descriptive terms incorporate pathological implications in a truer sense than calciphylaxis, it is important to take into account the ubiquitous use of calciphylaxis term in the medical community. Thus, the term calciphylaxis is used when referring to calciphylaxis patients on dialysis and non-uremic calciphylaxis to refer to patients with normal kidney function and those with earlier stages of chronic kidney disease 15.
The exact sequence of events in calciphylaxis pathogenesis remains to be determined but the arteriolar calcification is likely the first event, followed by thrombosis, and skin ischemia 16.
Histology of calciphylaxis
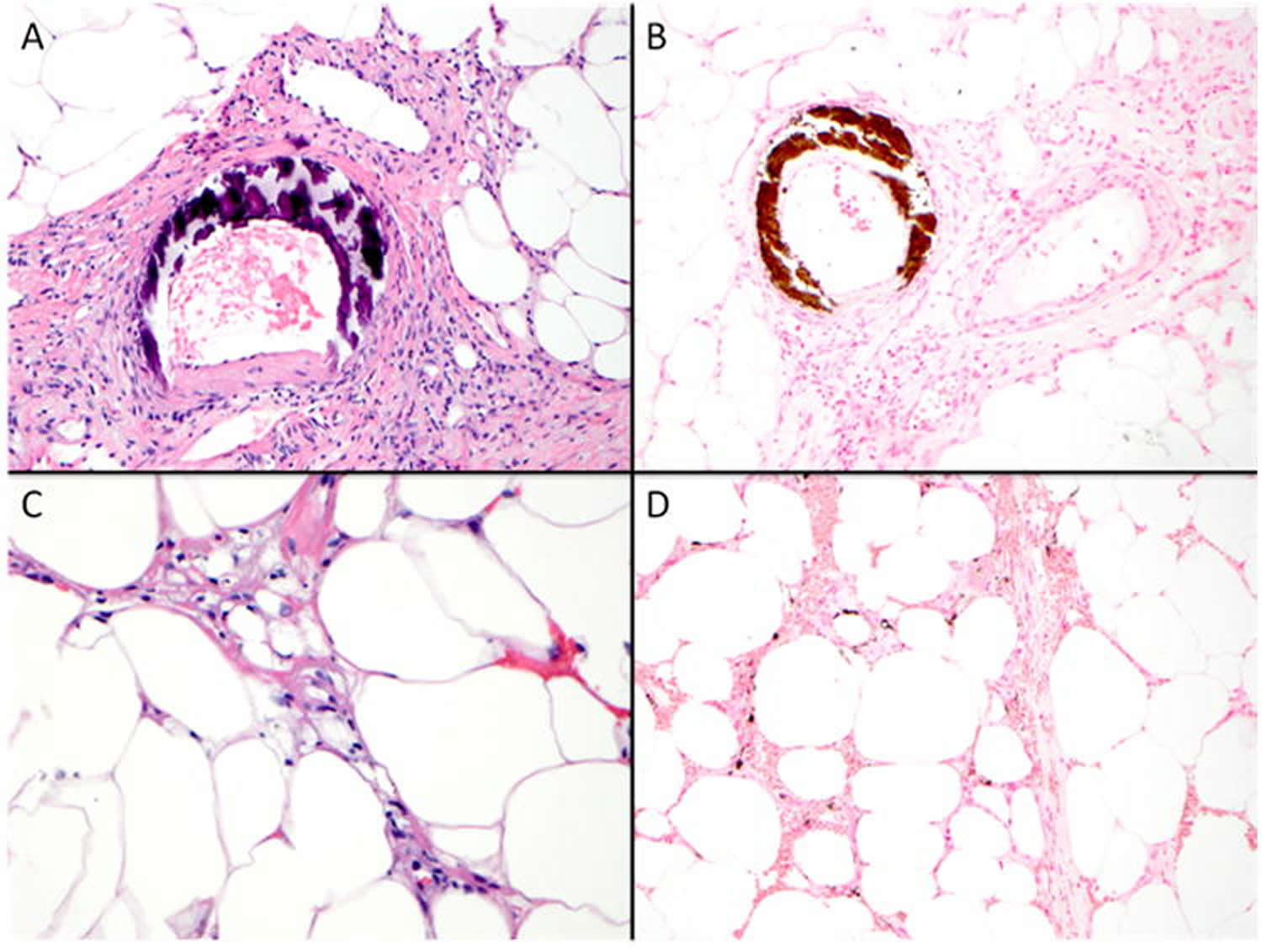
A deep biopsy to sample the subcutis is needed to make the diagnosis of calciphylaxis. The epidermis and dermis is often ulcerated and necrotic with numerous secondary changes. There is calcification of small-medium sized vessels (Figure 3 A and B). The intima of the vessels is commonly fibrosed and there may be intravascular thrombi. Diffuse calcium phosphate deposition of small capillaries in the fat is a characteristic feature (Figure 3 C). There may also be calcium phosphate deposition of adipocytes. A von Kossa histochemical stain aids in the detection of interstitial calcium deposits, which may not be identified on routine histologic sections (Figure 3 D).
Figure 3. Calciphylaxis pathology
Calciphylaxis life expectancy
The one-year mortality in calciphylaxis patients is reported at 45-80% with ulcerated lesions associated with higher mortality compared to non-ulcerated lesions and sepsis being the leading cause of death 17. Mortality rates in chronic hemodialysis patients with calciphylaxis were almost 3 times higher than for chronic hemodialysis patients without calciphylaxis in the United States Renal Data System 3.
Calciphylaxis complications
Calciphylaxis can lead to:
- Chronic and extensive ulceration
- Secondary infection with sepsis
- Death
Calciphylaxis prognosis
Mortality in patients with calciphylaxis associated with chronic renal disease is reported to be 60–80%. Death is usually from infection.
Death is less likely when warfarin is the cause of calciphylaxis, with 15 of 18 patients reported to have fully recovered.
Calciphylaxis causes
The cause of calciphylaxis is not properly understood. Calcification blocks small blood vessels deep in the skin, resulting in spreading skin necrosis (tissue death).
Small blood vessels become blocked with blood clots (thrombosis), which leads to the black painful, necrotic and ischaemic areas. It is thought that the clots occur because of calfication within the walls of the blood vessels.
In chronic renal failure, it is often associated with a condition known as secondary hyperparathyroidism. The damaged kidneys don’t excrete phosphate properly, which results in a build up of phosphate in the blood, which combines with calcium. Vitamin-D levels are reduced because of the kidney failure and reduced absorption through the gut. The bones become resistant to parathyroid hormone. The parathyroid glands therefore increase in size and produce more hormone increasing the amount of calcium circulating in the blood.
Calciphylaxis can occur in those with high or normal levels of serum calcium and phosphate, with or without vitamin D replacement, in dialysed patients and less often in those who have not yet commenced dialysis or in those who have received a renal transplant. It is more common in women than in men, in obese patients compared to those of normal weight, and in patients who have been taking corticosteroids or other immunosuppressive medicines.
Calciphylaxis can also occur in patients with normal kidney function, in the presence of hypercoagulability states. These may include liver disease, diabetes and treatment with warfarin. High levels of matrix metalloproteinases have been described and one theory suggests chemically altered elastin protein allows deposition of calcium on small vessels.
Calciphylaxis risk factors
Many case reports, case series, and observational studies have been published to understand risk-associations for calciphylaxis and in recent years there has been a significant increase in publications on calciphylaxis. Table 1 provides a summary of case-control studies conducted to understand the risk factors for calciphylaxis. It is important to recognize that the study populations in terms of case and control definitions have been heterogeneous and these studies suffer from limitations of small sample size, single center experience, and selection bias. Furthermore, like any other epidemiological study, these investigations do not determine causality.
Table 1. Summary of case-control studies evaluating risk factors for uremic calciphylaxis
| study | population | Main findings | comments |
|---|---|---|---|
| Nigwekar et al 6 | Cases: n=62; 100% on hemodialysis; biopsy confirmation in 100%; all cases were hospitalized at the time of calciphylaxis diagnosis Controls: n=124, hospitalized hemodialysis patients matched for gender and timing of hospitalization |
|
|
| Weenig et al 17 | Cases: n=49; 84% on hemodialysis and 16% on peritoneal dialysis; biopsy confirmation in 86% Controls: n=98, matched for age and gender |
|
|
| Fine et al 18 | Cases: n=36; 78% on peritoneal dialysis and 22% on hemodialysis; biopsy confirmation in 11% Controls: n=72, matched for duration of dialysis |
|
|
| Hayashi et al 19 | Cases: n=28; 100% on hemodialysis; unclear in how many cases biopsy confirmation was obtained Controls: n=56, matched for age and duration of dialysis |
|
|
| Mazhar et al 20 | Cases: n=19; 95% on hemodialysis and one patient had a functioning renal allograft; biopsy confirmation in 84% Controls: n=54, matched for the date of initiation of hemodialysis |
|
|
| Ahmed et al 5 | Cases: n=10; 80% on hemodialysis, 20% on peritoneal dialysis; biopsy confirmation in 100% Controls: n=180, dialysis patients |
|
|
| Angelis et al 21 | Cases: n=10; 100% on hemodialysis; unclear in how many cases biopsy confirmation was obtained Controls: n=232, chronic hemodialysis patients from the same center |
|
|
| Bleyer et al 22 | Cases: n=9; 67% on hemodialysis and 22% on peritoneal dialysis; biopsy confirmation in 100% Controls: n=347, chronic hemodialysis patients from the same center |
|
|
| Zacharias et al 23 | Cases: n=8; 100% on peritoneal dialysis; biopsy confirmation in 12.5 % Controls: n=37, matched for dialysis modality and length of time on dialysis |
|
|
Co-morbid conditions
- Diabetes mellitus is a frequently reported co-morbidity in patients with calciphylaxis 24. However, no data are available regarding whether diabetes control or duration affects calciphylaxis risk.
- Obesity is reported as a risk factor for proximal calciphylaxis (involving trunk, thighs, breasts, etc); although reasons for predilection for adipose tissue involvement remain speculative 22. The fibroelastic septa that anchor the skin to the body provide scaffolding for dermal arterioles. Obesity, due to expansion of the subcutaneous compartment by adipose tissue, subjects these septa and arterioles to increased tensile stress, further reducing the blood flow in already calcified arterioles in dialysis patients 25. Whether obesity is a risk factor for distal calciphylaxis (e.g. forearms, hands, feet, etc.) remains unknown.
- Calciphylaxis has been reported in patients with autoimmune conditions such as systemic lupus erythematosus, anti-phospholipid antibody syndrome, temporal arteritis, and rheumatoid arthritis raising the possibility of a potential role for autoimmunity in its development 26. Furthermore, treatments used to manage autoimmune conditions such as corticosteroids, methotrexate, and ultraviolet light have been implicated as potential triggers for calciphylaxis 26.
- Hypercoagulable conditions may predispose patients to calciphylaxis. There are case reports of calciphylaxis in patients with both hereditary and acquired thrombophilic conditions such as protein C and protein S deficiency, antithrombin III deficiency, cryofibrinogenemia, and anti-phospholipid antibody syndrome 27. However, arguments against the potential causative role of hypercoagulable conditions have also been made. In a case control study of 49 uremic calciphylaxis patients and 98 control patients on dialysis, no significant difference between cases and controls for protein C activity, protein S antigen, or antithrombin III activity were noted 17. Thrombi formation in venules that are frequently noted in patients with thrombophilic conditions are not seen in calciphylaxis patients 28. Despite these arguments, evaluation for thrombophilic conditions in calciphylaxis patients should be considered since it has important treatment implications.
- Infectious, autoimmune, and alcoholic hepatitis have been reported as risk factors for calciphylaxis 17. Calciphylaxis in the setting of liver disease is thought to be mediated via either inflammation or acquired thrombophilia from protein C or protein S deficiency.
- Longer dialysis vintage of over 6-7 years has been reported as a risk factor for calciphylaxis 21. However, like most risk factors associated with calciphylaxis, this relationship has been inconsistent across studies and there are reports in the literature of patients with significantly shorter dialysis vintage developing calciphylaxis 6. In a large cohort of uremic calciphylaxis patients, median dialysis vintage was 3.1 years 24.
- Hypoalbuminemia in dialysis patients can result from a variety of conditions including poor nutrition and inflammation. Multiple case-control studies report lower albumin levels in calciphylaxis patients when compared to dialysis patients without calciphylaxis 6. However, methodological limitations of these studies restrict conclusions regarding whether hypoalbuminemia is pathogenic, or whether it is merely a marker of malnutrition or chronic inflammation, or whether it is a result of calciphylaxis itself.
Medications
Calcium supplements, calcium-based phosphate binders, active vitamin D, warfarin, corticosteroids, iron therapy, and trauma related to subcutaneous insulin or heparin injections have been associated with increased calciphylaxis risk 18.
Warfarin, a vitamin K antagonist, has been used for many years as an anticoagulant due to its properties to inhibit the carboxylation and activation of vitamin K-dependent clotting factors. Recent reports indicate that endogenous inhibitors of vascular calcification such as Matrix Gla Protein are also vitamin K-dependent for their activation 29. Patients on warfarin therapy may not be able to inhibit vascular calcification due to a reduction in the active forms of these proteins. The studies investigating the association of warfarin use and calciphylaxis suffer from the same methodological limitations as those described above for other risk factors and have been inconsistent. However, the warfarin-calciphylaxis association is intriguing as it provides a unique opportunity to understand the biological role of vitamin K in calciphylaxis. A pilot clinical trial to investigate the role of vitamin K in calciphylaxis is currently underway.
Calciphylaxis symptoms
Clinical characteristics of calciphylaxis skin lesions can be variable (Figures 1 and 2). Intense pain associated with cutaneous lesions and palpation of firm calcified subcutaneous tissue is suggestive of calciphylaxis in dialysis patients and in patients with other risk factors for calciphylaxis 30.
Calciphylaxis begins as surface purple-colored mottling of the skin (retiform purpura) then bleeding occurs within the affected area. There may be blood-filled blisters. The skin goes black in the center of star-shaped (stellate) purple lesions. The skin cells die because of lack of blood supply (dry gangrene). This causes deep and often extensive ulcers.
Patients with calciphylaxis usually experience severe pain, burning and sometimes itching at the lesion sites.
Calciphylaxis most often occurs on the lower limb especially in fatty areas. Lesions on the trunk, abdomen, buttocks or thighs, appear to be more dangerous than lesions on the lower legs and feet.
Calciphylaxis diagnosis
To determine if you have calciphylaxis, your doctor will review your medical history, assess your symptoms and do a physical exam.
A high index of clinical suspicion is required for early and accurate diagnosis of calciphylaxis. Table 2 provides a summary of clinical mimics of calciphylaxis.
A detailed history focused on the proposed risk factors should be obtained. A thorough physical examination should be performed to identify additional skin lesions. In patients on warfarin therapy, distinction should be made between warfarin necrosis and calciphylaxis (Table 2) 31.
Table 2. Clinical mimics of calciphylaxis
| Features of clinical mimic | Features of calciphylaxis | |
|---|---|---|
| Atherosclerotic vascular disease | Symptoms of claudication, weak peripheral pulses, distal distribution, abnormal ankle-brachial index | Can be proximal or distal distribution, severe pain, dermal arteriolar calcification on skin biopsy |
| Cholesterol embolization | Usually in acral distribution, may have features associated with renal or gastrointestinal ischemia, cholesterol clefts on skin biopsy | Can be proximal or distal distribution, dermal arteriolar calcification on skin biopsy |
| Nephrogenic systemic fibrosis | Brawny plaques, thickened skin, history of exposure to gadolinium, moderate intensity pain, marked increase in spindle cells and fibrosis on skin biopsy | Severe pain, dermal arteriolar calcification on skin biopsy |
| Oxalate vasculopathy | Acral distribution, history of calcium oxalate stones, birefringent, yellowish-brown, polarizable crystalline material deposition in the dermis and arteriolar wall on skin biopsy | Can be proximal or distal distribution, calcium deposits non-polarizable |
| Purpura fulminans | Usually seen in the settings such as septic shock or disseminated intravascular coagulation, diffuse body distribution, rapid progression, clinical features of shock | Unlikely to have diffuse whole body distribution, absence of serological features of disseminated intravascular coagulation, dermal arteriolar calcification on skin biopsy |
| Vasculitis | Systemic features of vasculitis, serological test abnormalities (e.g. cryoglobulins), no dermal arteriolar calcification on skin biopsy, unlikely to have full-thickness necrosis or large areas of involvement | Absence of systemic features and serological abnormalities of vasculitis (unless autoimmune disease is a trigger for calciphylaxis), black eschar, dermal arteriolar calcification on skin biopsy |
| Warfarin necrosis | Typically seen within the first 10 days of warfarin initiation, manifestation of paradoxical hypercoagulable state created by a transient imbalance in the procoagulant and anticoagulant pathways warfarin discontinuation associated with clinical improvement in majority of cases | Warfarin exposure of prolonged duration when calciphylaxis associated with warfarin therapy, black eschar, dermal arteriolar calcification on skin biopsy |
Tests may include:
- Deep skin biopsy. To diagnose calciphylaxis, your doctor may remove a small tissue sample from an area of affected skin for analysis.
- Blood tests. Mayo Clinic labs will analyze a blood sample to measure a variety of substances in your blood — calcium, phosphorus, parathyroid hormone, aluminum, urea nitrogen, creatinine and albumin, among others — to help your doctor assess your kidney and liver function.
- Imaging studies. X-rays may show branch-like calcium deposits in the blood vessels (vascular calcifications) that are common in calciphylaxis. However, vascular calcifications are also common in other advanced kidney diseases.
Skin biopsy
Definitive diagnosis of calciphylaxis requires a skin biopsy and should be considered whenever the calciphylaxis diagnosis is entertained. The following issues related to skin biopsy need attention:
- 1) Discussion of risks and benefits of skin biopsy is essential. Possible risks include ulceration, superimposed infection, propagation of new lesions, bleeding, and induction of necrosis. Benefits include exclusion of other conditions that can mimic calciphylaxis (Table 2),
- 2) In the hands of an experienced dermatologist or surgeon the potential yield can be maximized,
- 3) A punch or telescoping biopsy (4-5 mm deep) from the lesion margin or deep incisional wedge skin biopsy are likely to have the best yield 32. However, a punch biopsy is safer and is a preferred approach over an incisional biopsy. In general, biopsy at the center of the ulcer or of necrotic area is of low diagnostic yield.
The characteristic histological features of calciphylaxis include calcification, microthrombosis, and fibrointimal hyperplasia of small dermal and subcutaneous arteries and arterioles leading to cutaneous ischemia and intense septal panniculitis (Figure 3). Detection of micro-calcification often requires special stains such as von Kossa or Alizarin red. Performing both von Kossa and Alizarin red stains may increase the detection of calcium deposits over individual stain alone and should be considered when the clinical suspicion is high but calcium deposits are not readily apparent on routine histological sections 11.
Laboratory evaluation
Laboratory evaluation should be conducted to further evaluate potential risk factors: 1) Renal function evaluation- serum blood urea nitrogen, creatinine, and estimated glomerular filtration rate (urinalysis, urine protein: creatinine ratio, and 24 hour urine collection for creatinine clearance to be considered for non-dialysis patients), 2) Mineral bone parameters evaluation- serum calcium, phosphorous, alkaline phosphatase, intact parathyroid hormone, and 25-hydroxyvitamin D, 3) Liver evaluation-serum transaminases, alkaline phosphatase, and albumin, 4) Infection evaluation-complete blood count with differential (in all cases), and blood cultures (if leukocytosis or fever present), 5) Coagulation evaluation- prothrombin time, international normalized ratio, and partial thromboplastin time, 6) Inflammation evaluation- serum high sensitivity C-reactive protein and albumin, 7) Hypercoagulation evaluation- protein C, protein S, antithrombin III, and antiphospholipid antibody, and 8) Evaluation for autoimmune disease and malignancy as guided by the clinical suspicion.
Calciphylaxis treatment
No standard or universally effective treatment for calciphylaxis exists. Early diagnosis and treatment offer the best chance to reduce the effects.
A multi-disciplinary and multi-interventional approach involving input from the following disciplines is important: nephrology, dermatology, dermatopathology, wound or burn center, nutrition, and pain management. Input should be obtained as soon as the diagnosis of calciphylaxis is suspected to formulate a comprehensive and consistent management plan.
Multiple interventions have been described in the management of calciphylaxis 33; however, the overall quality of evidence is poor and data mostly come from retrospective cohort studies, case series, and case reports. At present, there is no published data from a randomized controlled trial that addresses any of the proposed interventions. Treatment recommendations are largely an expert opinion based on the clinical experience and available observational published data.
A summary of one approach to calciphylaxis treatment is provided below and is described below.
Summary of treatment approach for uremic calciphylaxis
Wound management
- Wound care team should be involved for recommendations regarding selection of dressings, chemical debriding agents, frequency of dressing changes, and negative pressure wound therapy.
- Surgical wound debridement should be considered on a case-by-case basis.
- Hyperbaric oxygen therapy can be considered as a second line treatment if wounds not improving. Claustrophobia, access to treatment, and cost can be significant limiting factors of this therapy.
- Antibiotic administration should be guided by clinical appearance of lesions and accompanying systemic features.
Pain management
- Often narcotic analgesics are required to control severe pain associated with calciphylaxis.
- Fentanyl may be preferred over morphine to minimize potential hypotension episodes associated with morphine
Pain management is one of the most challenging aspects of calciphylaxis and many patients report severe pain despite administration of potent analgesics 34. The exact etiology of pain is unclear and is thought to be ischemic in origin but there may be a neuropathic component associated with nerve inflammation 35. Opioid analgesics are typically required to control severe pain, but morphine, codeine, and hydrocodone should be avoided in dialysis patients due to accumulation of neurotoxic metabolites.85,86 Oxycodone and hydromorphone can be used in patients with renal insufficiency but require close monitoring for side effects 36. Limited experience suggests multimodal analgesia combining opioids with non-opioid adjuvants, such as neuropathic agents, and ketamine, may improve symptomatic management of calciphylaxis. Use of non-steroidal anti-inflammatory drugs may be limited in patients with renal dysfunction. Because of severity, and complexity of pain in this population, pain medicine and palliative care teams play a critical role in calciphylaxis management.
Sodium thiosulfate
- Intravenous sodium thiosulfate at doses ranging from 12.5 to 25 grams in the last 30 minutes of each hemodialysis session for patients on 3 times a week dialysis schedule 24. For patients with other hemodialysis prescriptions dose adjustments are needed according to published algorithms.
- Nausea, metabolic acidosis, hypotension, and volume overload are potential adverse effects
- Intra-lesional sodium thiosulfate has been described to aid in the resolution of calciphylaxis lesions.
Intravenous sodium thiosulfate is probably the most common intervention used to treat calciphylaxis (off-label indication) 37. It is a reducing agent that forms water-soluble complexes with many metals and minerals. Its use in calciphylaxis was first reported over 10 years ago in a case report 38. However, there is no prospective trial data on this agent.
Management of mineral bone disease
- Serum calcium and phosphorous levels should be maintained in the normal range and serum parathyroid hormone level should be maintained between 150-300 ng/mL.
- Calcium supplements, high dialysate calcium bath, vitamin D preparations should be avoided and instead cinacalcet to be considered to treat secondary hyperparathyroidism in patients with calciphylaxis. Surgical parathyroidectomy is indicated in patients with refractory hyperparathyroidism.
- Excessive suppression of parathyroid hormone should be avoided.
Dialysis prescription
- Hemodialysis prescription should be optimized to achieve the recommended K/DOQI goals of adequacy.
- K/DOQI Clinical Practice Guidelines for Peritoneal Dialysis Adequacy should be followed for peritoneal dialysis patients.
Nutrition management
- Nutrition consult to address protein energy malnutrition should be obtained.
Management of other risk factors
- Risk vs. benefit discussion is needed to decide whether to continue warfarin and iron compounds in patients with calciphylaxis
Applying intensive wound treatment
Your doctor will recommend aggressive wound care. For sores to heal, some of the tissue damaged by calciphylaxis may need to be surgically removed (debridement). In some cases, tissue can be removed using other methods, such as wet dressings or whirlpool treatments, among others. Antibiotic treatment is part of treating and preventing wound infection. You may be offered medication to assist with pain due to the calciphylaxis or wound care.
Restoring oxygen and blood flow to the skin
Your doctor may recommend hyperbaric oxygen therapy to increase oxygen delivery to the affected parts of the body. Also, your doctor may use low-dose tissue plasminogen activator (TPA) to dissolve blood clots in the tiny blood vessels of the skin. Medication that helps keep your blood from clotting (anticoagulation medication) may be prescribed to restore blood flow to the tissues. Your doctor will go over with you the best anticoagulant for your case.
Decreasing calcium deposits
Reducing calcium deposits in your arteries may be helped by:
- Dialysis. Your doctor may change your dialysis prescription if you’re on kidney dialysis, including the medications used in and the frequency of your dialysis.
- Medications to reduce calcium. Your doctor will evaluate your current medications and eliminate potential triggers for calciphylaxis, such as corticosteroids or iron, and may modify the amount (dose) of your calcium or vitamin D supplements. Your doctor may also recommend a medication called cinacalcet (Sensipar), which can help control parathyroid hormone (PTH). Other medications may include sodium thiosulfate, which binds with calcium so it passes out of the body in urine, and medications to improve the balance of calcium and phosphorus.
- Surgery. If your doctor determines that an overactive parathyroid gland (hyperparathyroidism) is contributing to the abnormal calcium metabolism by producing too much parathyroid hormone (PTH), surgery to remove all or part of the parathyroid glands may be recommended.
- Brandenburg VM, Cozzolino M, Ketteler M. Calciphylaxis: a still unmet challenge. Journal of nephrology. 2011;24(2):142–148. https://www.ncbi.nlm.nih.gov/pubmed/21337312[↩]
- Brandenburg VM, Kramann R, Specht P, Ketteler M. Calciphylaxis in CKD and beyond. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association – European Renal Association. 2012;27(4):1314–1318. https://www.ncbi.nlm.nih.gov/pubmed/22344774[↩][↩]
- Nigwekar SU, Solid CA, Ankers E, et al. Quantifying a rare disease in administrative data: the example of calciphylaxis. Journal of general internal medicine. 2014;29(Suppl 3):724–731. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4124115/[↩][↩]
- Araya CE, Fennell RS, Neiberger RE, Dharnidharka VR. Sodium thiosulfate treatment for calcific uremic arteriolopathy in children and young adults. Clinical journal of the American Society of Nephrology : CJASN. 2006;1(6):1161–1166. http://cjasn.asnjournals.org/content/1/6/1161.long[↩]
- Ahmed S, O’Neill KD, Hood AF, Evan AP, Moe SM. Calciphylaxis is associated with hyperphosphatemia and increased osteopontin expression by vascular smooth muscle cells. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2001;37(6):1267–1276. https://www.ncbi.nlm.nih.gov/pubmed/11382698[↩][↩]
- Nigwekar SU, Bhan I, Turchin A, et al. Statin use and calcific uremic arteriolopathy: a matched case-control study. American journal of nephrology. 2013;37(4):325–332. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4110510/[↩][↩][↩][↩]
- Stavros K, Motiwala R, Zhou L, Sejdiu F, Shin S. Calciphylaxis in a dialysis patient diagnosed by muscle biopsy. Journal of clinical neuromuscular disease. 2014;15(3):108–111. https://www.ncbi.nlm.nih.gov/pubmed/24534833[↩]
- Moe SM, Chen NX. Calciphylaxis and vascular calcification: a continuum of extra-skeletal osteogenesis. Pediatric nephrology. 2003;18(10):969–975. https://www.ncbi.nlm.nih.gov/pubmed/15152617[↩]
- Wilmer WA, Magro CM. Calciphylaxis: emerging concepts in prevention, diagnosis, and treatment. Seminars in Dialysis. 2002; 15:172-186. http://onlinelibrary.wiley.com/wol1/doi/10.1046/j.1525-139X.2002.00052.x/full[↩][↩]
- Nigwekar SU, Kroshinksy D, Nazarian RM, et al. Calciphylaxis: Risk Factors, Diagnosis, and Treatment. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2015;66(1):133-146. doi:10.1053/j.ajkd.2015.01.034. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4696752/[↩][↩][↩]
- Mochel MC, Arakaki RY, Wang G, Kroshinsky D, Hoang MP. Cutaneous calciphylaxis: a retrospective histopathologic evaluation. The American Journal of dermatopathology. 2013;35(5):582–586. https://www.ncbi.nlm.nih.gov/pubmed/23328789[↩][↩]
- Dauden E, Onate MJ. Calciphylaxis. Dermatologic clinics. 2008;26(4):557–568. ix. https://www.ncbi.nlm.nih.gov/pubmed/18793990[↩][↩]
- Hayden MR, Kolb LG, Khanna R. Calciphylaxis and the cardiometabolic syndrome. Journal of the cardiometabolic syndrome. 2006;1(1):76–79. https://www.ncbi.nlm.nih.gov/pubmed/17675891[↩]
- Selye H, Gentile G, Prioreschi P. Cutaneous molt induced by calciphylaxis in the rat. Science. 1961;134(3493):1876–1877. http://science.sciencemag.org/content/134/3493/1876.long[↩]
- Nigwekar SU, Wolf M, Sterns RH, Hix JK. Calciphylaxis from nonuremic causes: a systematic review. Clinical journal of the American Society of Nephrology : CJASN. 2008;3(4):1139–1143. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2440281/[↩][↩]
- Au S, Crawford RI. Three-dimensional analysis of a calciphylaxis plaque: clues to pathogenesis. Journal of the American Academy of Dermatology. 2002;47(1):53–57. https://www.ncbi.nlm.nih.gov/pubmed/12077581[↩]
- Weenig RH, Sewell LD, Davis MD, McCarthy JT, Pittelkow MR. Calciphylaxis: natural history, risk factor analysis, and outcome. Journal of the American Academy of Dermatology. 2007;56(4):569–579. https://www.ncbi.nlm.nih.gov/pubmed/17141359[↩][↩][↩][↩]
- Fine A, Zacharias J. Calciphylaxis is usually non-ulcerating: risk factors, outcome and therapy. Kidney international. 2002;61(6):2210–2217. https://www.ncbi.nlm.nih.gov/pubmed/12028462[↩][↩]
- Hayashi M, Takamatsu I, Kanno Y, et al. A case-control study of calciphylaxis in Japanese end-stage renal disease patients. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association – European Renal Association. 2012;27(4):1580–1584. https://www.ncbi.nlm.nih.gov/pubmed/22121234[↩]
- Mazhar AR, Johnson RJ, Gillen D, et al. Risk factors and mortality associated with calciphylaxis in end-stage renal disease. Kidney international. 2001;60(1):324–332. https://www.ncbi.nlm.nih.gov/pubmed/11422768[↩]
- Angelis M, Wong LL, Myers SA, Wong LM. Calciphylaxis in patients on hemodialysis: a prevalence study. Surgery. 1997;122(6):1083–1089. discussion 1089-1090. https://www.ncbi.nlm.nih.gov/pubmed/9426423[↩][↩]
- Bleyer AJ, Choi M, Igwemezie B, de la Torre E, White WL. A case control study of proximal calciphylaxis. American journal of kidney diseases : the official journal of the National Kidney Foundation. 1998;32(3):376–383. https://www.ncbi.nlm.nih.gov/pubmed/9740152[↩][↩]
- Zacharias JM, Fontaine B, Fine A. Calcium use increases risk of calciphylaxis: a case-control study. Peritoneal dialysis international : journal of the International Society for Peritoneal Dialysis. 1999;19(3):248–252. https://www.ncbi.nlm.nih.gov/pubmed/10433161[↩]
- Nigwekar SU, Brunelli SM, Meade D, Wang W, Hymes J, Lacson E., Jr Sodium thiosulfate therapy for calcific uremic arteriolopathy. Clinical journal of the American Society of Nephrology : CJASN. 2013;8(7):1162–1170. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3700696/[↩][↩][↩]
- Janigan DT, Hirsch DJ, Klassen GA, MacDonald AS. Calcified subcutaneous arterioles with infarcts of the subcutis and skin (“calciphylaxis”) in chronic renal failure. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2000;35(4):588–597. https://www.ncbi.nlm.nih.gov/pubmed/10739777[↩]
- Lee JL, Naguwa SM, Cheema G, Gershwin ME. Recognizing calcific uremic arteriolopathy in autoimmune disease: an emerging mimicker of vasculitis. Autoimmunity reviews. 2008;7(8):638–643. https://www.ncbi.nlm.nih.gov/pubmed/18774119[↩][↩]
- Harris RJ, Cropley TG. Possible role of hypercoagulability in calciphylaxis: review of the literature. Journal of the American Academy of Dermatology. 2011;64(2):405–412. https://www.ncbi.nlm.nih.gov/pubmed/20708299[↩]
- Wilmer WA, Magro CM. Calciphylaxis: emerging concepts in prevention, diagnosis, and treatment. Seminars in dialysis. 2002;15(3):172–186. https://www.ncbi.nlm.nih.gov/pubmed/12100455[↩]
- Danziger J. Vitamin K-dependent proteins, warfarin, and vascular calcification. Clinical journal of the American Society of Nephrology : CJASN. 2008;3(5):1504–1510. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4571144/[↩]
- Brewster UC. Dermatological disease in patients with CKD. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2008;51(2):331–344. https://www.ncbi.nlm.nih.gov/pubmed/18215712[↩]
- Nazarian RM, Van Cott EM, Zembowicz A, Duncan LM. Warfarin-induced skin necrosis. Journal of the American Academy of Dermatology. 2009;61(2):325–332. https://www.ncbi.nlm.nih.gov/pubmed/19615543[↩]
- Ng AT, Peng DH. Calciphylaxis. Dermatologic therapy. 2011;24(2):256–262. https://www.ncbi.nlm.nih.gov/pubmed/21410615[↩]
- Vedvyas C, Winterfield LS, Vleugels RA. Calciphylaxis: a systematic review of existing and emerging therapies. Journal of the American Academy of Dermatology. 2012;67(6):e253–260. https://www.ncbi.nlm.nih.gov/pubmed/21821309[↩]
- Polizzotto MN, Bryan T, Ashby MA, Martin P. Symptomatic management of calciphylaxis: a case series and review of the literature. Journal of pain and symptom management. 2006;32(2):186–190. https://www.ncbi.nlm.nih.gov/pubmed/16877187[↩]
- Nayak-Rao S. Achieving effective pain relief in patients with chronic kidney disease: a review of analgesics in renal failure. Journal of nephrology. 2011;24(1):35–40. https://www.ncbi.nlm.nih.gov/pubmed/20383865[↩]
- Dean M. Opioids in renal failure and dialysis patients. Journal of pain and symptom management. 2004;28(5):497–504. https://www.ncbi.nlm.nih.gov/pubmed/15504625[↩]
- Sood AR, Wazny LD, Raymond CB, et al. Sodium thiosulfate-based treatment in calcific uremic arteriolopathy: a consecutive case series. Clinical nephrology. 2011;75(1):8–15. https://www.ncbi.nlm.nih.gov/pubmed/21176746[↩]
- Cicone JS, Petronis JB, Embert CD, Spector DA. Successful treatment of calciphylaxis with intravenous sodium thiosulfate. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2004;43(6):1104–1108. https://www.ncbi.nlm.nih.gov/pubmed/15168392[↩]





{kind=link}