Contents
What is placenta accreta
Placenta accreta is a potentially life threatening obstetric condition in which the placenta is abnormally attached too deeply and too firmly into the uterus. This can lead to massive blood loss during or following delivery. This is thought to result from a defect in the layer of tissue that would normally separate the placenta from the uterus (deciduas basalis). As a result, projections of the placenta (chorionic villi) are able to invade the uterus to varying degrees.
In a placenta accreta, the placental villi extend beyond the confines of the endometrium and attach to the superficial aspect of the myometrium of the uterus but without deep invasion. The abnormal implantation is thought to result from a deficiency in the decidua basalis, in which the decidua is partially or completely replaced by loose connective tissue. In a placenta accreta, chorionic villi and/or cytotrophoblasts directly attach to the myometrium with little or no intervening decidua.
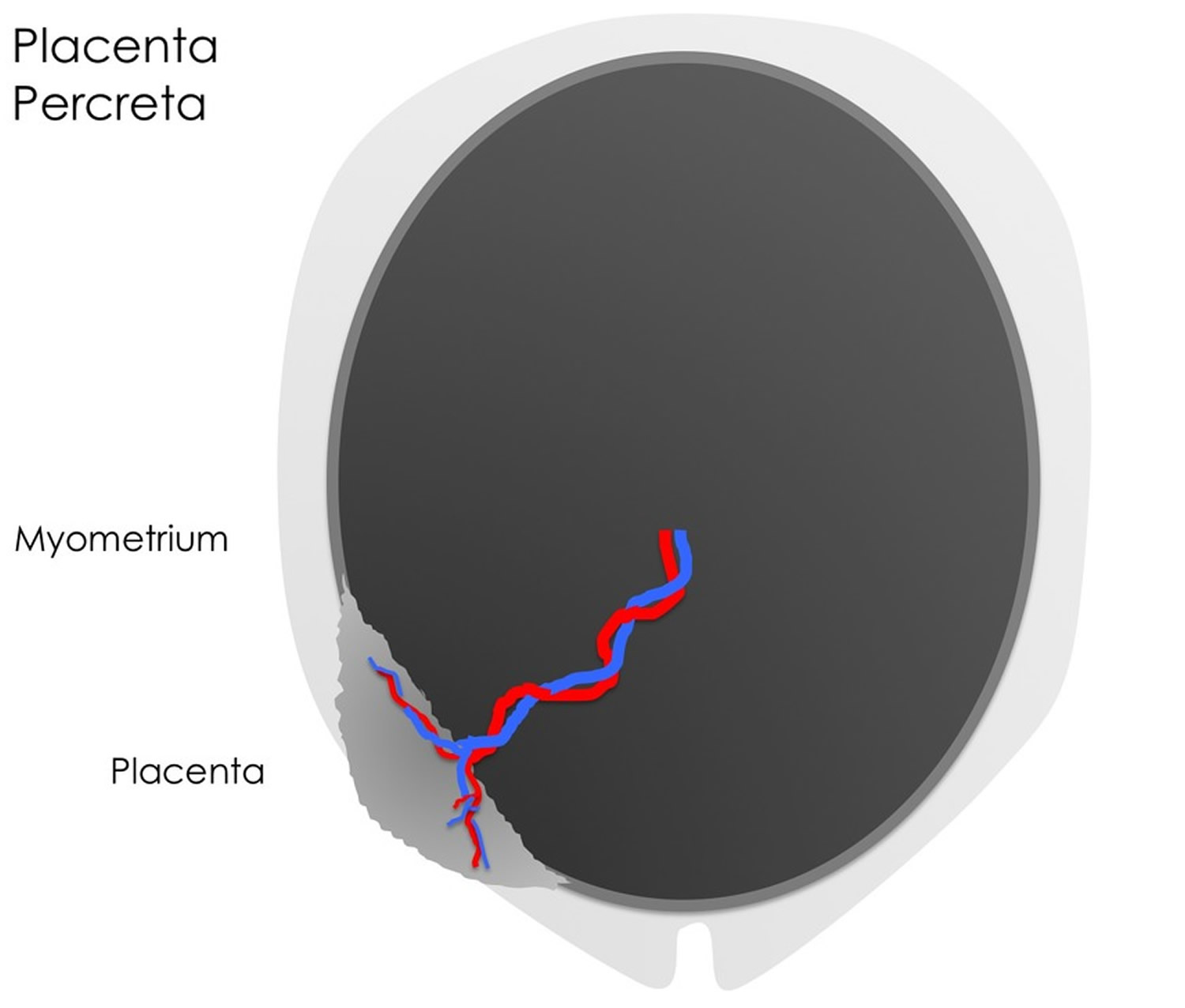
Where the chorionic villi invade the deeper muscular layer (the myometrium), this is termed placenta increta. Where infiltration occurs through the myometrium with or without infiltration of adjacent structures including the bladder this is termed placenta percreta.
Although the condition was quite rare 30 years ago, the incidence of placenta accreta has been steadily increasing, mirroring increased rates of caesarean section delivery, which is one of the principle risk factors for placenta accreta.
Placenta accreta is the most common form of placental invasion (~75% of cases). Currently, placenta accreta occurs in approximately 1 in 530 births in the United States each year. The incidence is increasing due to increased practice of cesarean sections. The combination of previous cesarean section and an anterior placenta previa should raise the possibility of a placenta accreta.
During the pregnancy, the placental tissue can invade the different layers of the uterus to varying degrees. The main concern is that following delivery of the baby the placenta will fail to separate from the uterus with the potential for massive, life threatening blood loss.
In these conditions, the placenta doesn’t completely separate from the uterus after you give birth. This can cause dangerous bleeding. Placenta accreta has a maternal mortality of up to 7% depending on location.
Placenta accreta often has no symptoms. As a result, sometimes you don’t even know you have it until you deliver your baby. In other cases, your provider sees signs of it in an ultrasound. And vaginal bleeding during the third trimester can be a warning sign. See your healthcare provider right away if you have vaginal bleeding anytime during your pregnancy. If the bleeding is severe, call your local emergency number for an ambulance or go to the hospital right way.
Placenta accreta is considered a high-risk pregnancy complication. If placenta accreta is suspected during pregnancy, you’ll likely need an early cesarean section (also called C-section) delivery followed by the surgical removal of your uterus (hysterectomy). This can help prevent bleeding from becoming life threatening. A c-section is surgery in which your baby is born through a cut that your provider makes in your belly and uterus. A hysterectomy is when your uterus is removed by surgery. Without a uterus, you can’t get pregnant again in the future.
A cesarean hysterectomy (cesarean section plus hysterectomy) should be done at a hospital that has an intensive care unit and is equipped to handle complications, such as severe bleeding. Your health care team for the surgery might include an obstetrical surgeon, a pelvic surgeon and an anesthesiologist, as well as a neonatologist to treat your baby.
Your health care provider might recommend scheduling the C-section and hysterectomy as early as week 34 of pregnancy to avoid an unscheduled emergency delivery.
What is uterus
The uterus is a hollow, muscular organ shaped somewhat like an inverted pear. The uterus receives the embryo that develops from an oocyte fertilized in the uterine tube, and sustains its development.
In its nonpregnant, adult state, the uterus is about 7 centimeters long, 5 centimeters wide (at its broadest point), and 2.5 centimeters in diameter. The size of the uterus changes greatly during pregnancy and it is somewhat larger in women who have been pregnant. The uterus is located medially in the anterior part of the pelvic cavity, superior to the vagina, and usually bends forward over the urinary bladder (see Figure 3).
The upper two-thirds or body (corpus), of the uterus has a domeshaped top called the fundus (see Figure 1). The uterine tubes (also called Fallopian tubes) connect at the upper lateral edges of the uterus. The lower third of the uterus is called the cervix. This tubular part extends downward into the upper part of the vagina. The cervix surrounds the opening called the cervical orifice, through which the uterus opens to the vagina.
The uterine wall is thick and has three layers (Figure 1). The endometrium, the inner mucosal layer, is covered with columnar epithelium and contains abundant tubular glands. The myometrium, a thick, middle, muscular layer, consists largely of bundles of smooth muscle cells. During the monthly female menstrual cycles and during pregnancy, the endometrium and myometrium change extensively. The perimetrium consists of an outer serosal layer, which covers the body of the uterus and part of the cervix.
Figure 1. Uterus anatomy
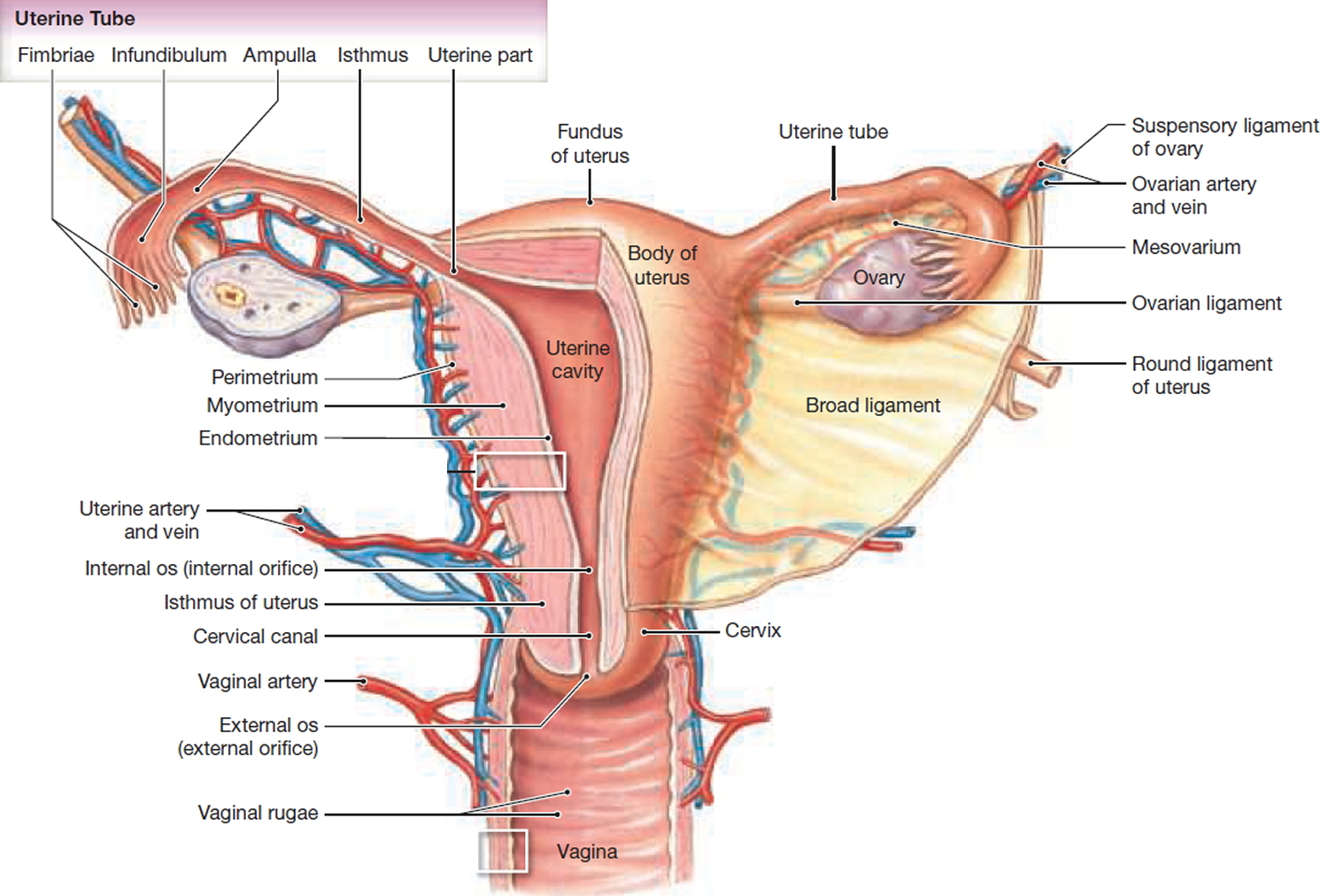
Figure 2. Blood supply to the uterus
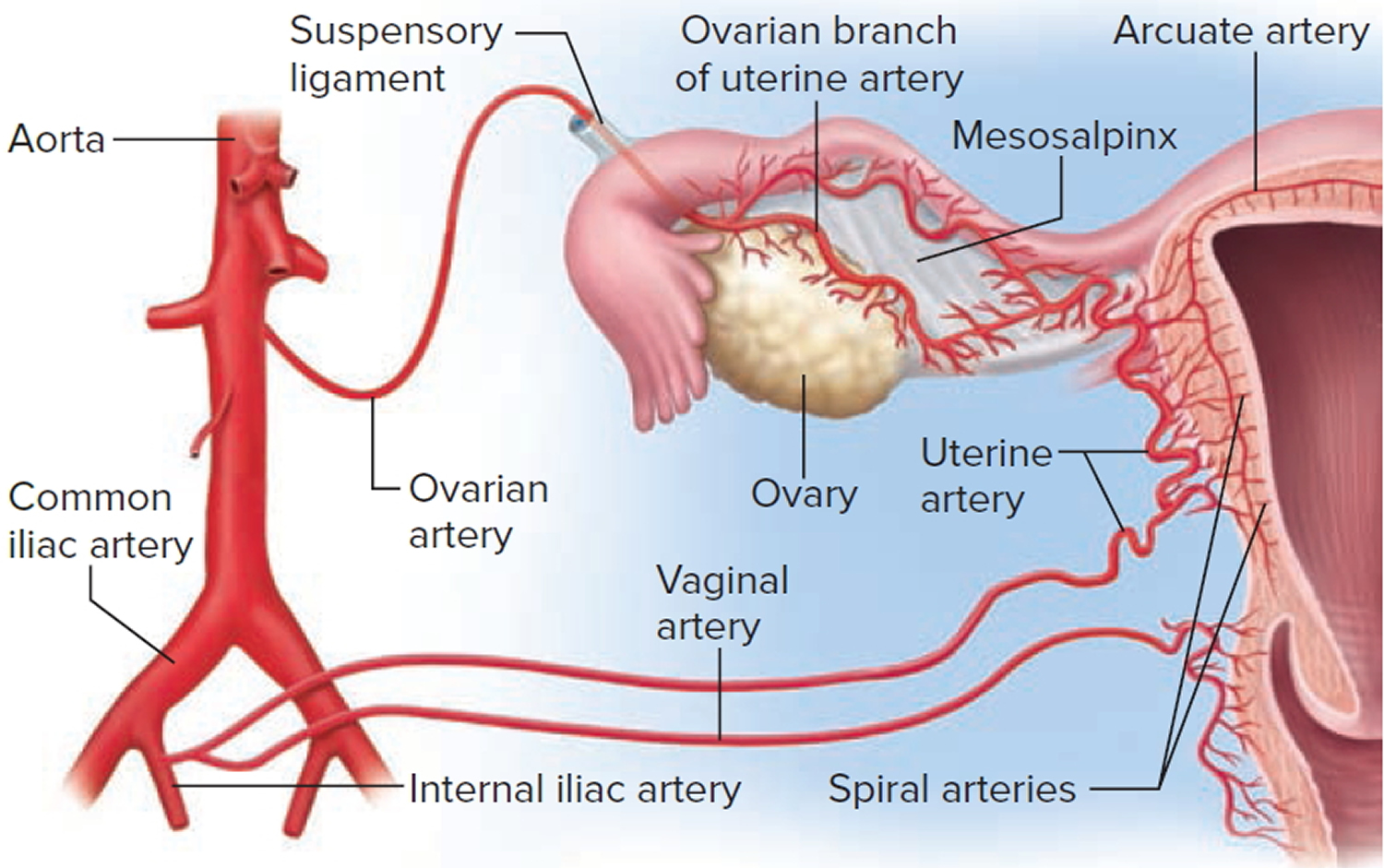
Figure 3. Uterus location
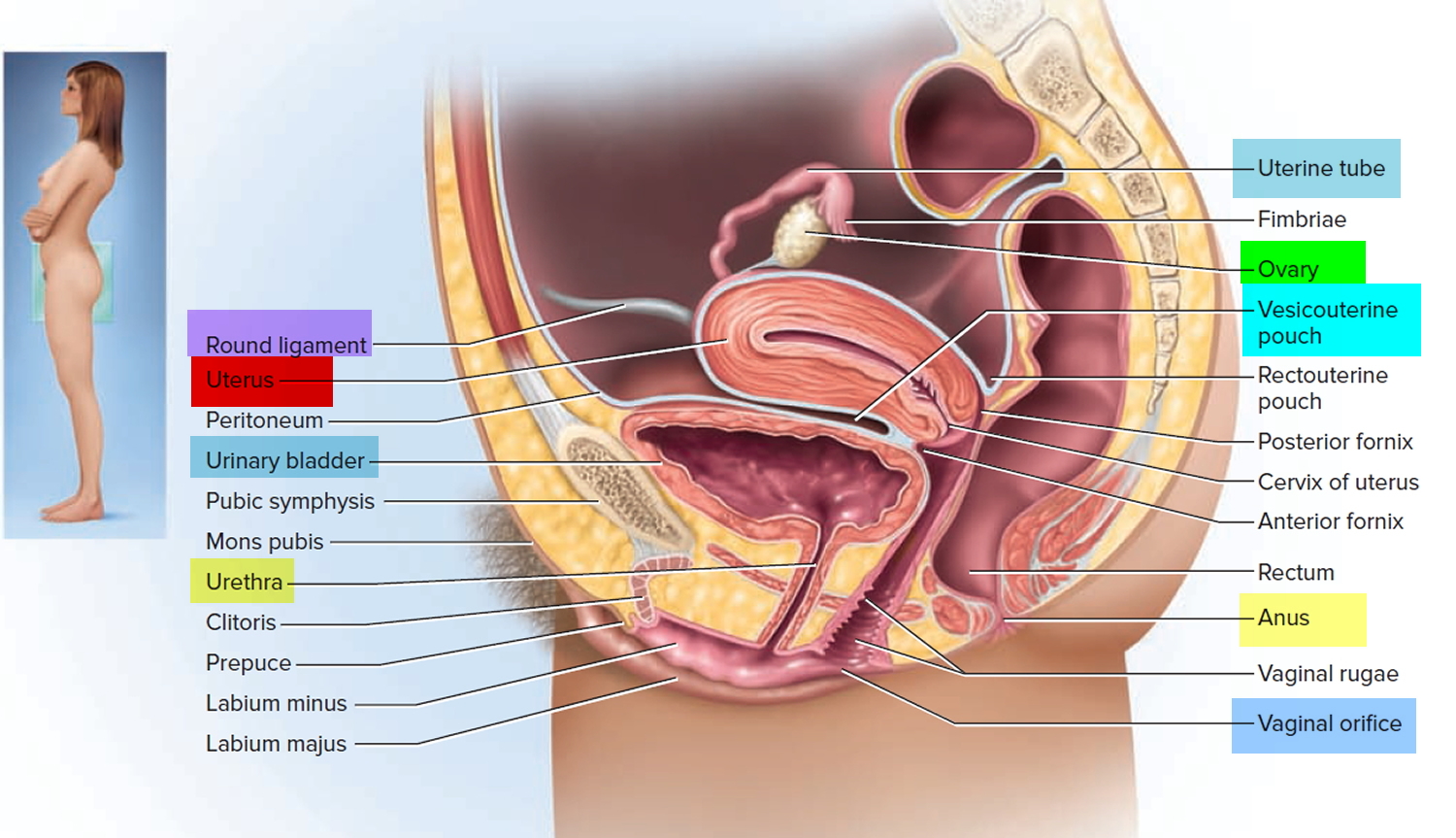
Figure 4. Endometrium of the uterus and its blood supply
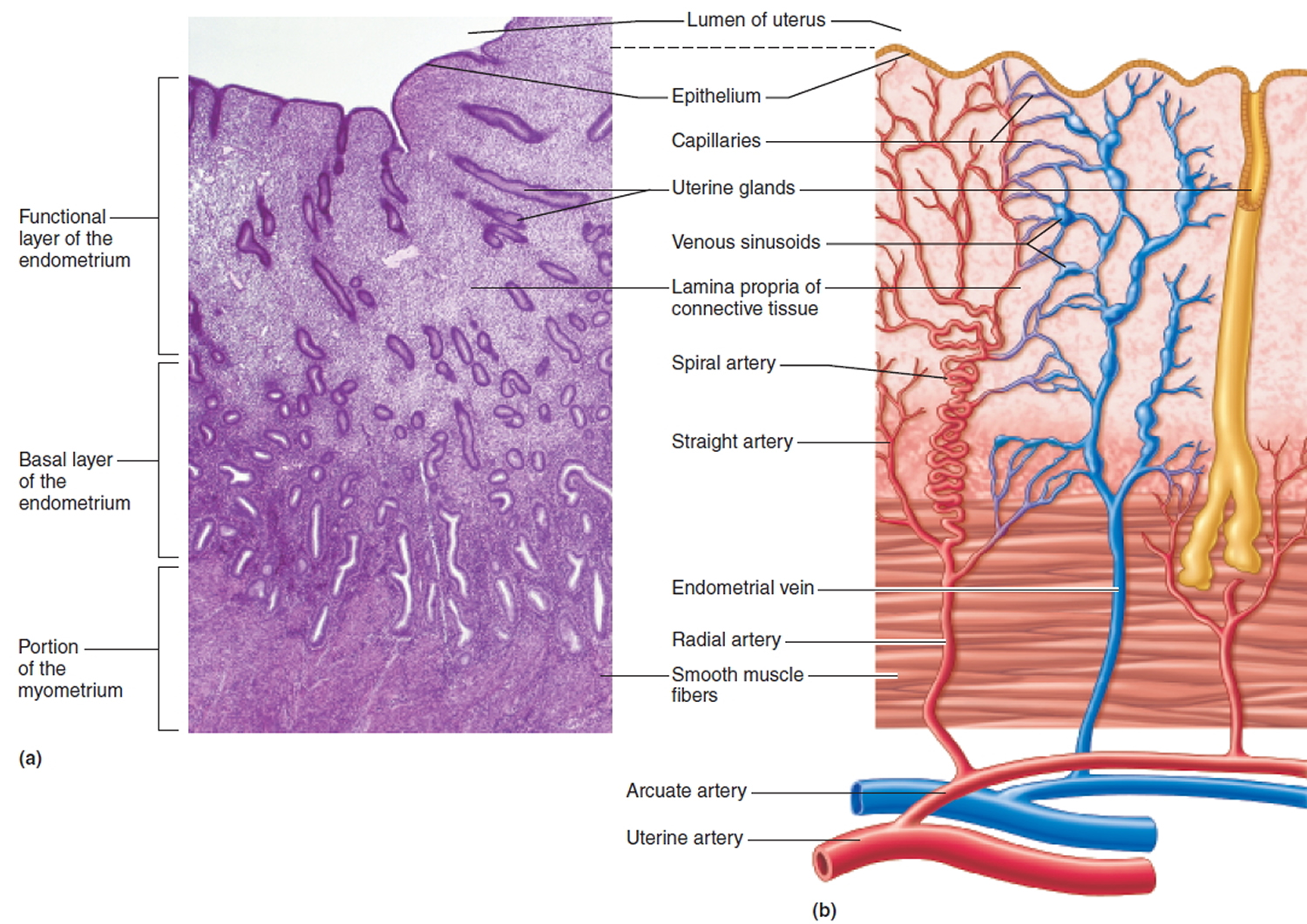
Figure 5. Normal placental adherence
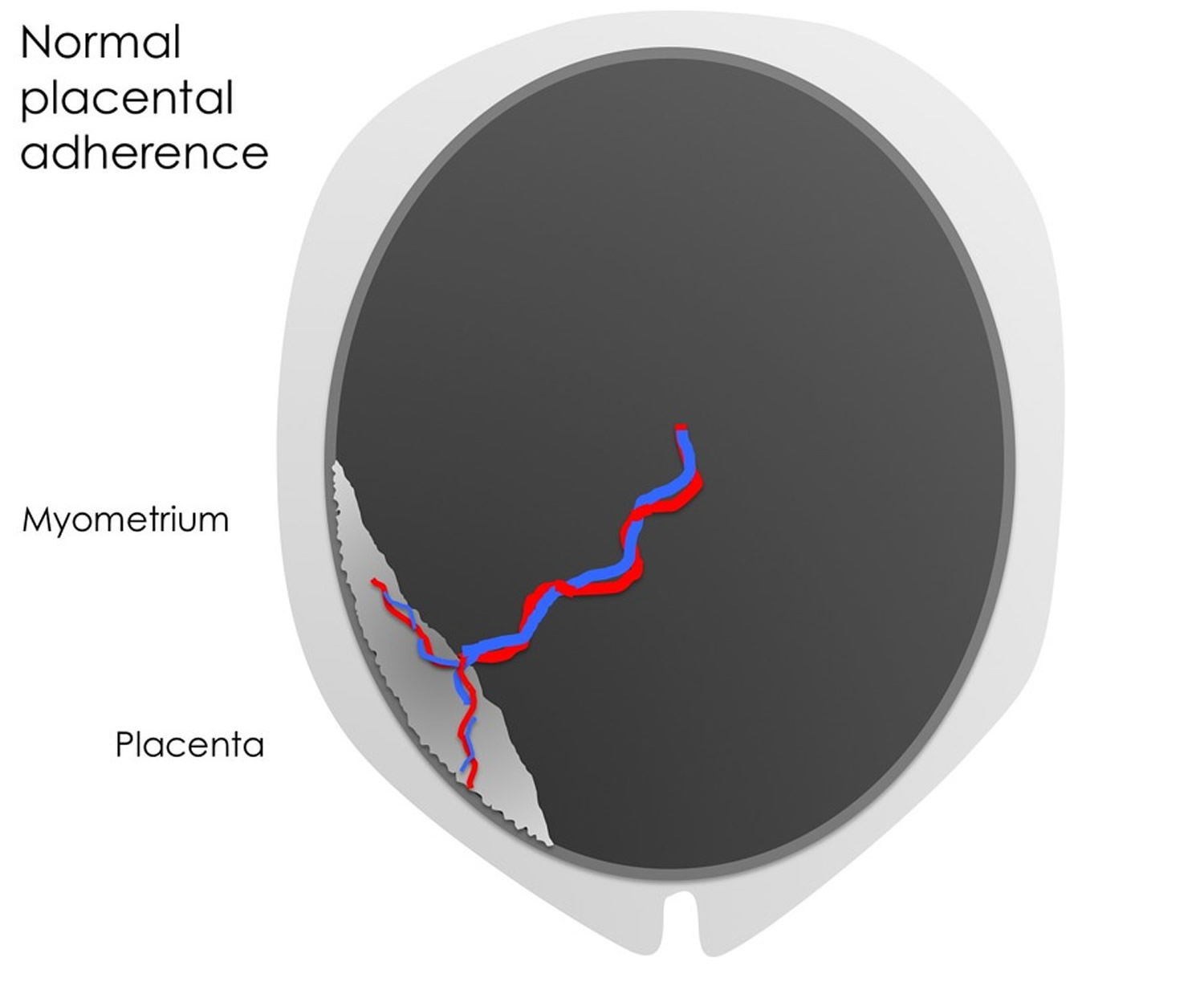
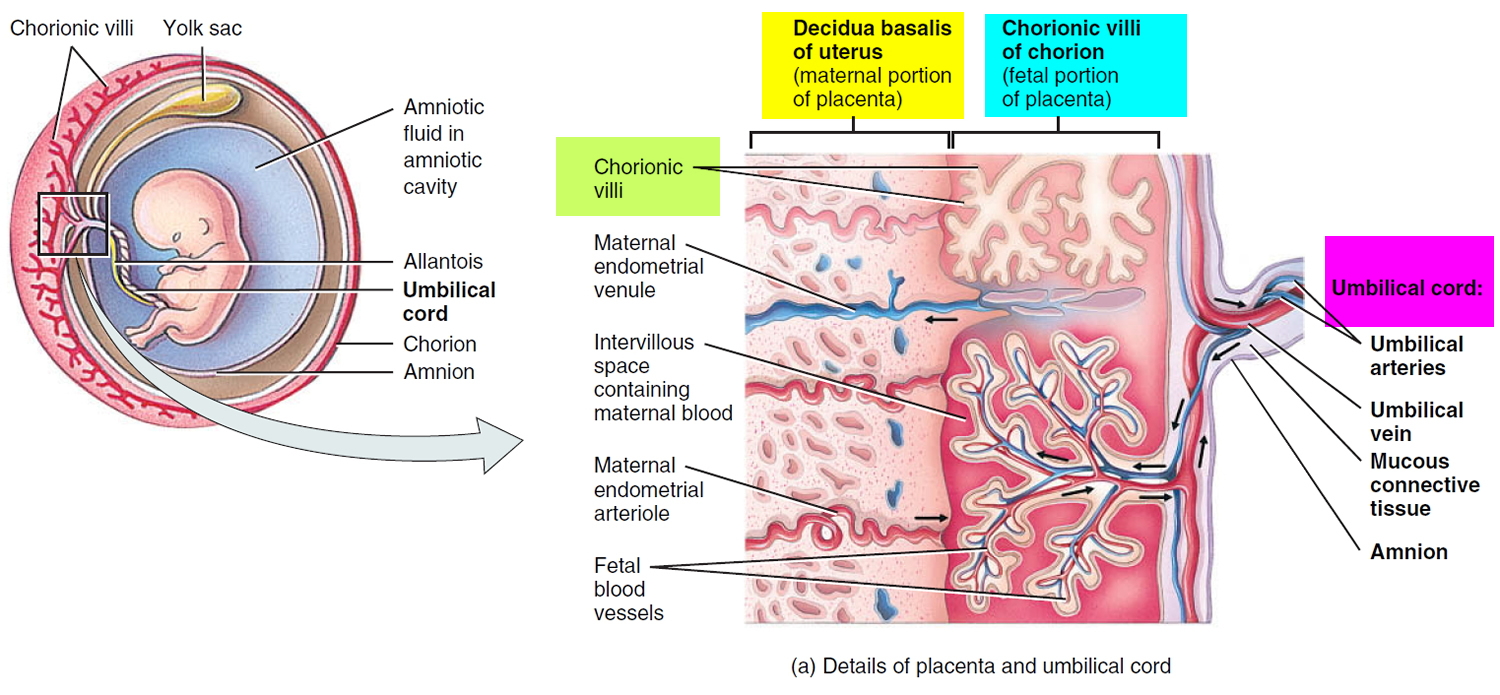
Figure 6. Placenta accreta
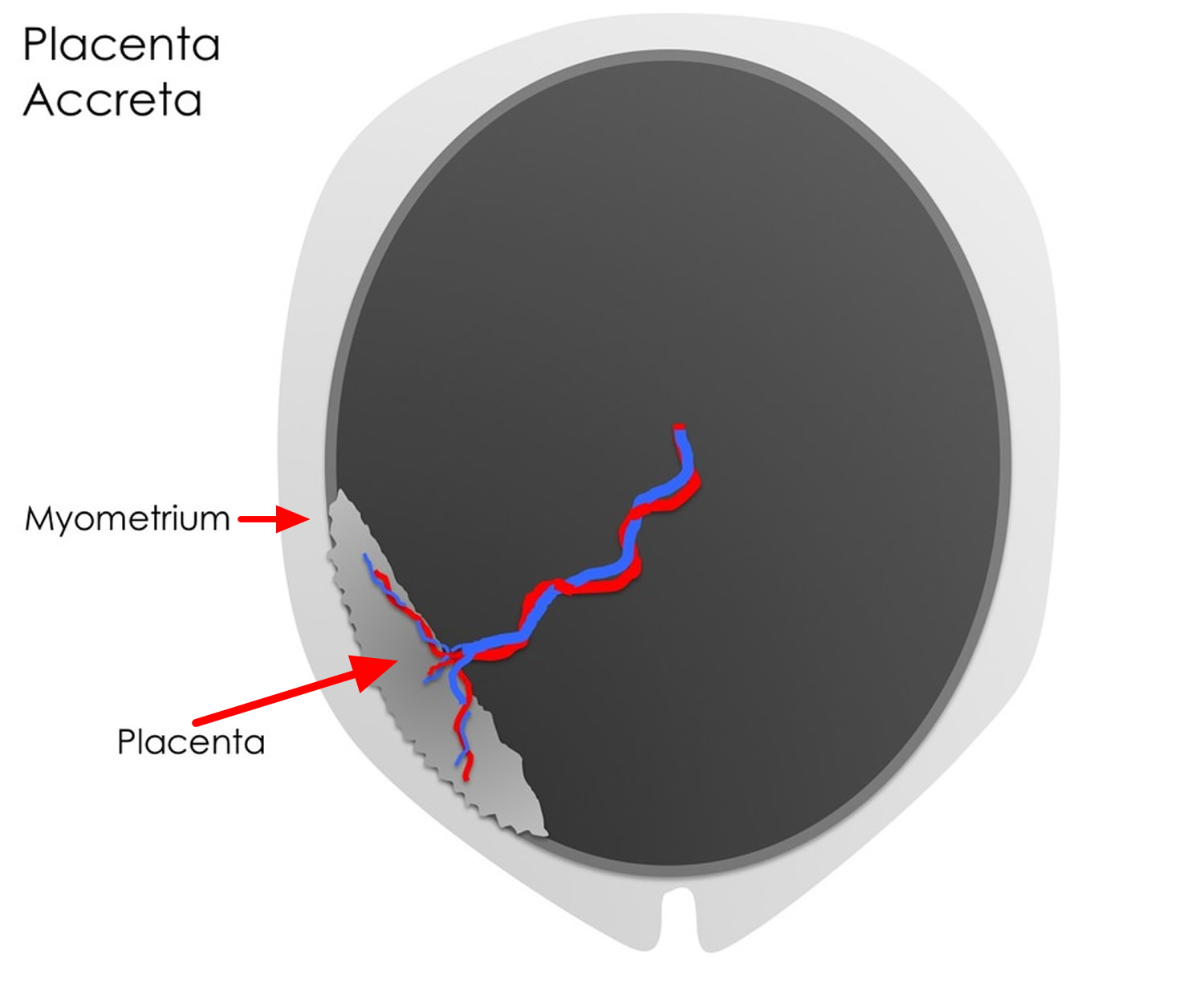 Figure 7. Placenta increta
Figure 7. Placenta increta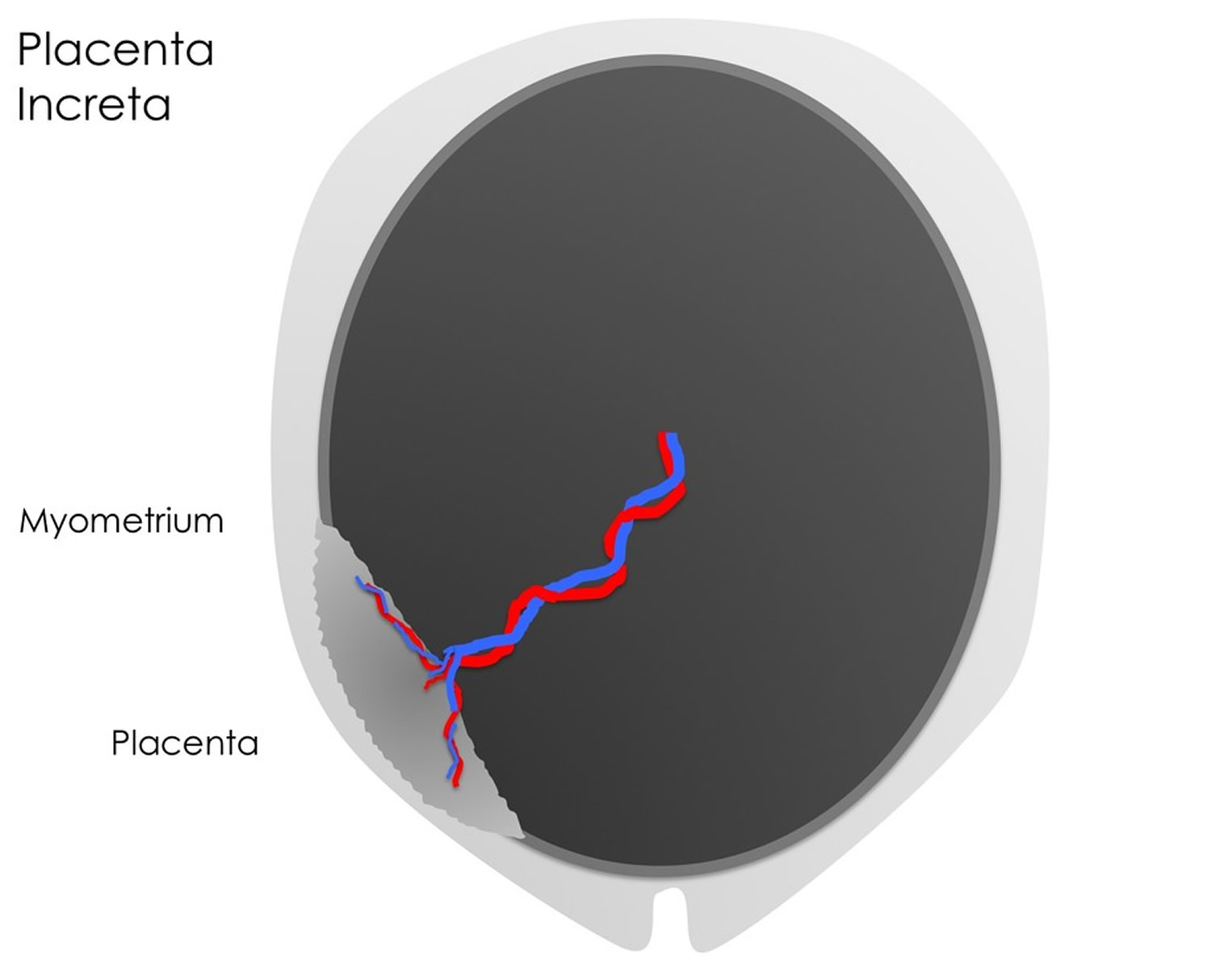 Figure 8. Placenta percreta
Figure 8. Placenta percreta
Placenta accreta prognosis
The probable outcomes of placenta accreta are largely dependant upon when it is diagnosed (during pregnancy vs. at delivery) and how it is treated. If diagnosed antenatally (during the pregnancy) this allows time for effective management planning and counseling. Currently, most women would undergo an elective cesarean section at approximately 38 weeks gestation to deliver the baby, followed by hysterectomy (surgical removal of the uterus). Indeed, placenta accreta is the most common reason for emergency hysterectomy during or following delivery.
Some of the complications that accompany hysterectomy include the need for blood transfusion, infection, injury to nearby tissues/organs and the formation of fistulas. As hysterectomy involves the surgical removal of the uterus, it means that the woman would no longer be able to bear children.
The rate of complications is minimized by performing the surgery as an elective procedure rather than in an emergency situation. Where the diagnosis is made during the pregnancy, planning the delivery at a suitable hospital with appropriate facilities such as obstetric anesthesia, appropriate surgical expertise and an intensive care unit also helps to minimize adverse outcomes.
Placenta accreta complications
Placenta accreta can cause serious complications, including:
- Heavy vaginal bleeding. Placenta accreta poses a major risk of severe vaginal bleeding (hemorrhage) after delivery. The bleeding can cause a life-threatening condition that prevents your blood from clotting normally (disseminated intravascular coagulopathy), as well as lung failure (adult respiratory distress syndrome) and kidney failure. A blood transfusion will probably be necessary.
- Premature birth. Placenta accrete might cause labor to begin early. If placenta accreta causes bleeding during your pregnancy, you might need to deliver your baby early.
Placenta accreta causes
Scientists don’t know what causes these kinds of placental conditions. But they often happen where you have a scar from a surgery, like removing a fibroid or having a c-section. A fibroid is a tumor that grows in the wall of the uterus (womb). If you’ve had a c-section, you’re more likely than if you had a vaginal birth to have placenta accreta. And the more c-sections you’ve had, the more likely you are to have these placental problems.
Things that may make you more likely to have these kinds of placenta accreta include:
- Smoking cigarettes
- Being 35 or older
- Being pregnant before
- Having placenta previa
Placenta accreta risk factors
Placenta accreta most commonly occurs in the setting of placenta previa with previous uterine surgery including cesarean section. In women with a previous cesarean section and current placenta previa, the risk of placenta accreta is 25%. For women with two or more previous cesarean sections, this risk rises to 40%.
Other predisposing factors have been identified including:
- Your risk of placenta accreta goes up with each uterine surgery, including surgery to remove uterine fibroids.
- Advanced maternal age
- Increased parity (number of pregnancies beyond 20 weeks gestation). The risk of placenta accreta increases each time you give birth.
- Certain other uterine conditions. The risk of placenta accreta is higher if you have uterine fibroids or scarring in the tissue that lines your uterus.
- Unexplained elevated maternal serum alpha-fetoprotein
- Cigarette smoking. Smoking raises the risk of placental problems.
- Uterine myomas
- Asherman’s syndrome
Placenta accreta prevention
One way to reduce your chances for having placenta accreta in future pregnancies is to have your babies by vaginal birth instead of cesarean section (C-section). Have a c-section only if there are health problems with you or your baby that make it medically necessary. For some moms and babies, health problems make c-section safer than vaginal birth. But if your pregnancy is healthy, it’s best to stay pregnant until labor begins on its own. Don’t schedule a c-section for non-medical reasons, like wanting to have your baby on a certain day or because you’re uncomfortable and want to have your baby earlier than your due date.
Even if you’ve already had a c-section, you may be able to have your next baby by vaginal birth. This is called vaginal birth after cesarean. You may be able to have a vaginal birth after cesarean depending on what kind of incision (cut) you had in your c-section and your overall pregnancy health. Talk to your healthcare provider if you think vaginal birth after cesarean may be right for you.
Placenta accreta symptoms
Placenta accreta often causes no signs or symptoms during pregnancy — although vaginal bleeding during the third trimester is possible. Often, placenta accreta is detected during a routine ultrasound.
If you experience vaginal bleeding during your third trimester, see your health care provider right away. If the bleeding is severe, seek emergency care.
Placenta accreta has the potential to cause massive, life threatening blood loss. It is for this reason that hysterectomy is the treatment of choice. Other treatment options, discussed in more detail below, include forced manual removal of the placenta but this is almost universally discouraged due to the potential for massive blood loss. The other treatment option involves taking a conservative approach whereby the placenta is left in position for variable lengths of time following delivery to allow it to resorb naturally. The latter has the benefit of preserving the woman’s fertility, but there still remains the possibility of massive blood loss and it also introduces the possibility of severe infection.
Placenta accreta diagnosis
There is very little for a doctor to find on clinical examination of a woman with placenta accreta.
Instead the doctor will be interested in your previous obstetric history including details about previous caesarean sections/uterine surgery and the location of the placenta in the current pregnancy if known. This information is especially important given that placenta accreta most frequently occurs in women with a current placenta previa and a history of uterine surgery.
If your provider suspects you have placenta accreta, an ultrasound or an magnetic resonance imaging (MRI) may be done to try and see how the placenta is implanted in your uterine wall.
Your blood may also be tested for a rise in alpha-fetoprotein (AFP). Maternal serum alpha-fetoprotein (AFP) is produced by your baby, and the amount tends to increase if you have placenta accreta. The defect in the layer normally separating the placenta and uterus allows leakage of fetal alpha-fetoprotein into the mother’s circulation. Up to 45% of women with placenta accreta have elevated maternal serum alpha-fetoprotein (AFP) levels in the absence of an obvious cause.
Placenta accreta ultrasound
Ultrasound is the most commonly used imaging method for the early diagnosis of placenta accreta. The most common feature on ultrasound that would suggest placenta accreta is a “moth-eaten” or “swiss cheese” appearance to the placenta. Ultrasound can be used from 15 weeks gestation, although it is more sensitive at gestations of 20 weeks or more.
According to one study 1, ultrasound has a sensitivity of 89.5%, positive predictive value of 68% and negative predictive value of 98% for the diagnosis of placenta accreta.
Several sonographic criteria for the diagnosis of placenta accreta have been reported:
- marked thinning or loss of the retroplacental hypoechoic zone
- interruption of the hyperechoic border between the uterine serosa and bladder
- presence of mass-like tissue with echogenicity similar to that of the placenta
- visualization of prominent vessels or lakes within the placenta or myometrium. Visualization of lacunae – “swiss cheese” appearance has the highest sensitivity in the diagnosis of placenta accreta,
- allowing identification in 78%–93% of cases after 15 weeks gestation, with a specificity of 78.6% 2.
When a placenta accreta occurs on the posterior or lateral walls of the uterus, it may be difficult to detect by ultrasound.
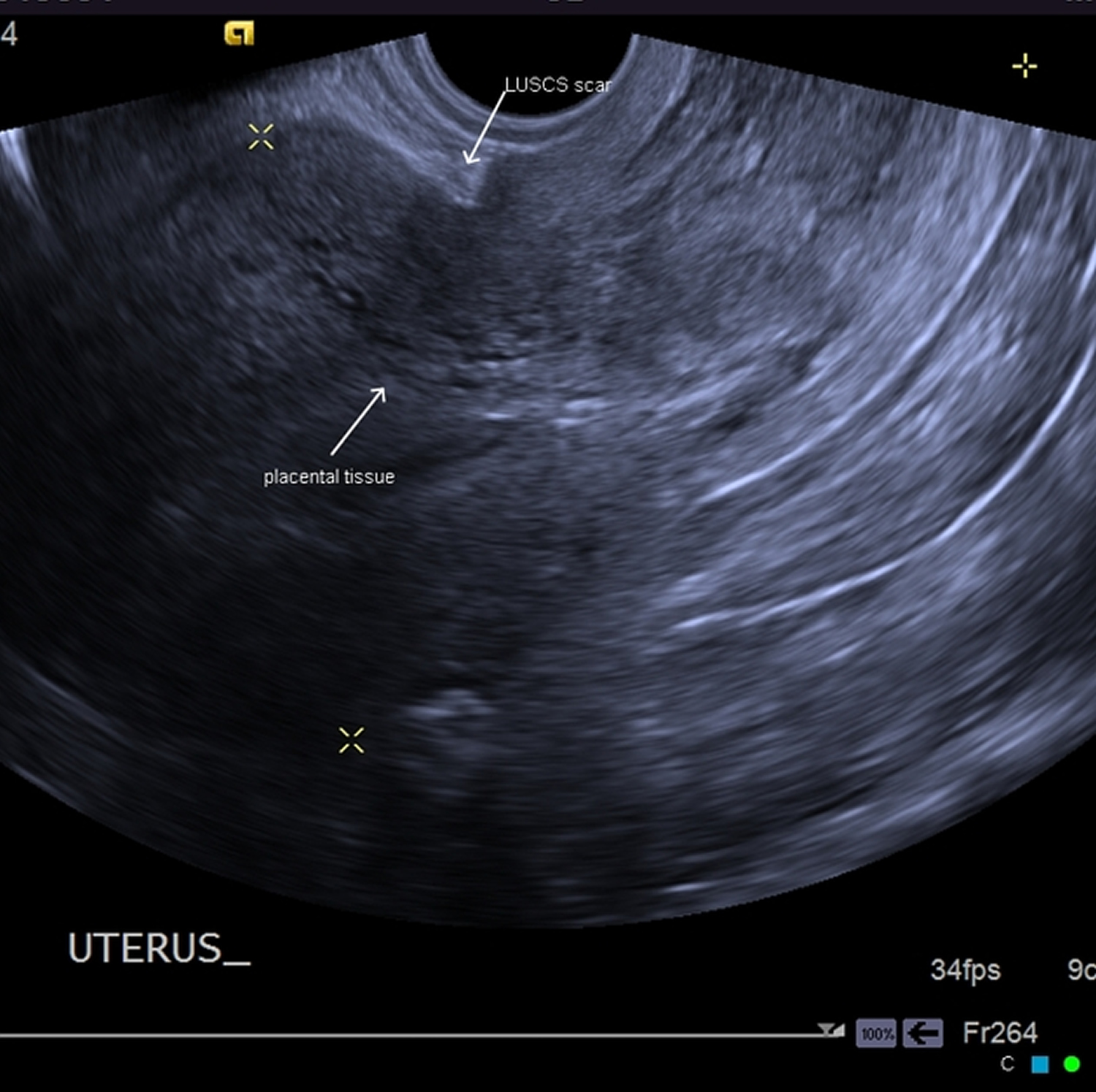
Figure 9. Placenta accreta ultrasound – post dilatation and curettage for post miscarriage in 2nd trimester with previous Cesarian section.
Ultrasound Video. Transabdominal and transvaginal ultrasound demonstrate an abnormally low position of the placenta, covering the anterior lower uterine segment, and also the internal cervical os, in keeping with a major grade placenta previa.
Multiple blood filled spaces are noted throughout the placenta (placental lacunae), a finding associated with abnormal placental adherence.
There is marked thinning of the anterior myometrium, with no appreciable myometrial tissue demonstrated between the placenta and the bladder serosa.
Placenta accreta MRI
Magnetic resonance imaging (MRI) has also been used to diagnose placenta accreta. Specific fast acquisition sequences (e.g. HASTE, true FISP) help to minimize fetal and maternal motion artefacts.
The demonstration of uterine bulging and loss of normal uterine contour.
T2
- on T2 weighted MR images, the mass is hyperintense and may be heterogeneous
- also, T2 weighted MR images are useful in the assessment of focal thinning of the myometrium and interruption of the junctional zone
Figure 10. Placenta accreta MRI (T2 weighted image)

Note: The placenta is completely covering the internal cervical os (grade IV placenta previa or complete placenta previa). Focal indistinctness of the uterine myometrium hypointense line with a dark T2 intraplacental band noted at the anterior lower uterine segment with mild placental heterogeneity as well as mild focal uterine bulge with bladder indentation.
Placenta accreta treatment
The first step in treatment of placenta accreta is recognition of risk factors. This allows further investigations such as ultrasound and/or MRI to be performed. Once an accurate diagnosis is made, this facilitates maternal counseling and effective management planning of the delivery to ensure safety.
Maternal counseling should include discussion pertaining to the choice and timing of an elective delivery, whether to make an attempt to separate the placenta at the time of delivery, the use of radiological interventions in an attempt to minimize blood loss and the use of particular drugs post-delivery.
If you have a placental condition, the best time for you to have your baby is unknown. But your healthcare provider may recommend that you give birth at around 34 to 38 weeks of pregnancy to help prevent dangerous bleeding. If you want to have future pregnancies, your obstetrician may use special treatments before the c-section to try to control bleeding and save your uterus.
Placenta accreta can cause you to go into premature labor. So your c-section may have to be scheduled as early as 34 weeks to avoid an unscheduled emergency delivery.
Delivery of a woman with a diagnosis or suspicion of placenta accreta should take place in a hospital with adequate facilities for high volume blood transfusion, interventional radiology and specialist obstetric, anesthetic and intensive care. Your healthcare team may include a maternal-fetal medicine specialist, an obstetrical surgeon, a pelvic surgeon, and an anesthesiologist, as well as a neonatologist to care for your premature baby and these specialists should be close at hand. Women with placenta accreta should reside close to the designated hospital throughout the third trimester of pregnancy in case of spontaneous labor, antepartum hemorrhage or other complications.
Effectively there are three treatment options including:
- Total abdominal hysterectomy – generally accepted as the treatment of choice;
- Forced manual removal – almost universally avoided due to the risk of massive hemorrhage and subsequent hysterectomy; and
- Conservative management – controversial as although it preserves future fertility, it exposes the woman to life threatening intra-abdominal infection and major bleeding.
Hysterectomy
Total abdominal hysterectomy is generally considered the treatment of choice for placenta accreta. This involves scheduled delivery of the fetus by cesarean section at 36-37 weeks provided there is fetal lung maturity. Once the fetus is delivered, no attempt is made to remove the placenta. The edges of the uterine incision are oversewn and hysterectomy performed. This will be performed by an experienced obstetric surgeon with a skilled obstetric anesthetist. Urology and gynecology oncology specialists should be close at hand.
Plans are made for emergency delivery should the women experience antepartum hemorrhage or go into spontaneous labor. However, emergency hysterectomy is associated with increased intraoperative blood losses and greater rates of blood transfusion.
During surgery
During the C-section, your health care provider will deliver your baby through an incision in your abdomen and a second incision in your uterus. After delivering your baby, your health care provider or another member of your health care team will remove your uterus — with the placenta still attached — to prevent severe bleeding.
After a hysterectomy, you no longer have the ability to become pregnant. If you had planned to become pregnant again in the future, discuss possible options with your health care provider.
Rarely, the uterus and placenta might be allowed to remain intact, allowing the placenta to dissolve over time. However, this approach can have serious complications, including:
- Severe vaginal bleeding
- Infection
- A blood clot that blocks one or more arteries in the lungs (pulmonary embolism)
- The need for a hysterectomy at a later date
In addition, limited research suggests that women who are able to avoid hysterectomy after having placenta accreta are at risk of pregnancy complications with subsequent pregnancies, including miscarriage, premature birth and recurrent placenta accreta.
If you’re interested in uterine conservation, ask your health care provider if it’s a possibility for you. If so, he or she can help you weigh the risks and benefits.
Undetected placenta accreta
Sometimes your healthcare provider doesn’t realize you have placenta accreta until you’ve delivered your baby and it’s time to deliver the placenta. If your placenta doesn’t detach from the uterine wall and you have heavy bleeding, placenta accreta may be the cause.
This situation can be life-threatening. You’re likely to need multiple blood transfusions and a hysterectomy to control the bleeding.
Conservative management
Conservative management of placenta accreta involves leaving the placenta in place without a forcible attempt to remove it. Within the scope of conservative management are the use of drugs to contract the uterus and to prevent infection (antibiotics), as well as procedures including pelvic arterial embolization, where selected arteries that feed blood into the uterus are blocked in an attempt to minimize bleeding.
In a study of 167 women from 25 University hospitals in France, conservative treatment was successful in 78.4% of cases. Spontaneous placental resorption occurred in 75% of women at a 13.5 week follow up. Surgical techniques were used to remove the retained placenta in 25% of women at a median follow up of 20 weeks. Just over 10% of women had hysterectomies performed within the first 24 hours following delivery and a further 10.8% had delayed hysterectomies.
Conservative management of placenta accreta remains highly controversial as although this technique preserves future fertility and avoids the complications of caesarean hysterectomy, it exposes the woman to potentially life threatening infection and massive hemorrhage.
Coping and support
If your health care provider suspects that you have placenta accreta, you’re likely worried about how your condition will affect your delivery, your baby and, possibly, your ability to become pregnant in the future.
To ease your anxiety:
- Find out about placenta accreta. Gathering information about your condition might help you feel less anxious. Talk to your health care provider, do some research and connect with other women who’ve had placenta accreta.
- Prepare for a C-section. If you’re disappointed that you won’t be able to have a vaginal birth, remind yourself that your baby’s health and your health are more important than the method of delivery.
- Prepare for a hysterectomy. After the hysterectomy, you’ll no longer have periods or be able to get pregnant. This might lead to a deep sense of loss. Ask your health care provider about what to expect during your recovery. If you need help coping with feelings of grief or depression, talk with a mental health provider.
- Take care of yourself. Set aside time for soothing activities that help you relax, such as reading or listening to music. Relaxation techniques, including meditation, deep breathing or guided imagery, may help ease stress and produce a feeling of calm.
- Esakoff TF, Sparks TN, Kaimal AJ et-al. Diagnosis and morbidity of placenta accreta. Ultrasound Obstet Gynecol. 2011;37 (3): 324-7. doi:10.1002/uog.8827 https://www.ncbi.nlm.nih.gov/pubmed/20812377[↩]
- W. Christopher Baughman, Jane E. Corteville. Placenta Accreta: Spectrum of US and MR Imaging Findings. Radiographics. 2008; 28 (7): 1905-1916. http://pubs.rsna.org/doi/10.1148/rg.287085060[↩]





{kind=link}