Contents
What is Klippel Trenaunay syndrome
Klippel-Trenaunay syndrome sometimes also called Klippel-Trenaunay-Weber syndrome, is a rare disorder found at birth (congenital) that affects the development of blood vessels, soft tissues (such as skin and muscles), bones and the lymphatic system. Klippel-Trenaunay syndrome has three characteristic features:
- A red birthmark called a port-wine stain,
- Abnormal overgrowth of soft tissues and bones, and
- Venous malformations of unusual distribution and varicose veins with or without lymphatic abnormalities.
However, Klippel-Trenaunay syndrome is the correct term used for the three of congenital anomalies outlined above. The eponym Klippel-Trenaunay syndrome has generated controversy in the medical literature since the first report of the condition in the early 20th century. The French physicians, Klippel and Trenaunay, described patients with capillary stains (improperly called “hemangiomas” at that time), venous varicosities, and overgrowth. At about the same time, the English dermatologist Parkes Weber reported the combination of “hemangiomas” and overgrowth of a limb. For many years, the names of all three physicians were linked as a confusing (and incorrect) term “Klippel-Weber-Trenaunay syndrome,” which still is (unfortunately) used to this day.
Since the latter 20th century, it is well-recognized that Parkes Weber and Klippel-Trenaunay syndromes are entirely different. Parkes Weber syndrome consists of fast-flow, multiple arteriovenous shunts and increased blood flow in the upper or lower limb (usually the lower extremity) are the hallmarks of Parkes Weber syndrome. By genetic testing, many of these patients have a dominant, germline mutation in the gene RASA1, it is known to be an autosomal dominant disorder. Nowadays Parkes-Weber syndrome is called a mixed hemolymphatic congenital vascular malformation with arteriovenous shunting, based on the Hamburg classification of congenital vascular malformations 1. In contrast, Klippel-Trenaunay syndrome is a slow-flow combined vascular disorder involving abnormal capillaries (C), lymphatics (L) and veins (V). Therefore, many investigators use the abbreviation CLVM, rather than Klippel-Trenaunay syndrome, and restrict the designation for patients who have all three vascular anomalies. However, recently, it has been recognized that many of these CLVM patients have another, specific disorder of combined vascular anomalies and enlarged tissues designated by the acronym CLOVES = congenital lipomatous overgrowth with vascular anomalies, epidermal nevus and skeletal anomalies. CLOVES is caused by a somatic mutation in the gene PIK3CA. This means the condition is not inheritable. Other authors apply the Klippel-Trenaunay syndrome term more broadly and include patients with only capillary stain (port wine stain) or only capillary and venous anomalies (CVM) in the limb in the absence of lymphatic abnormalities. Once the genetic cause for Klippel-Trenaunay syndrome is discovered, it will be possible to more precisely designate patients with these various combinations of vascular anomalies.
Most people with Klippel-Trenaunay syndrome are born with a port-wine stain. This type of birthmark is caused by swelling of small blood vessels (capillaries) near the surface of the skin. Port-wine stains are typically flat and can vary from pale pink to deep maroon in color. In people with Klippel-Trenaunay syndrome, the port-wine stain usually covers part of one limb. The affected area may become lighter or darker with age. Occasionally, port-wine stains develop small red blisters that break open and bleed easily.
Patients usually present in infancy. Features are often unilateral and typically affect one limb 2. Klippel-Trenaunay syndrome may be diagnosed in utero 3.
Klippel-Trenaunay syndrome is also associated with overgrowth of bones and soft tissues beginning in infancy. Usually this abnormal growth is limited to one limb, most often one leg. However, overgrowth can also affect the arms or, rarely, the torso. The abnormal growth can cause pain, a feeling of heaviness, and reduced movement in the affected area. If the overgrowth causes one leg to be longer than the other, it can also lead to problems with walking.
Malformations of veins are the third major feature of Klippel-Trenaunay syndrome. These abnormalities include varicose veins, which are swollen and twisted veins near the surface of the skin that often cause pain. Varicose veins usually occur on the sides of the upper legs and calves. Veins deep in the limbs can also be abnormal in people with Klippel-Trenaunay syndrome. Malformations of deep veins increase the risk of a type of blood clot called a deep vein thrombosis (DVT). If a DVT travels through the bloodstream and lodges in the lungs, it can cause a life-threatening blood clot known as a pulmonary embolism (PE).
Other complications of Klippel-Trenaunay syndrome can include a type of skin infection called cellulitis, swelling caused by a buildup of fluid (lymphedema), and internal bleeding from abnormal blood vessels. Less commonly, this condition is also associated with fusion of certain fingers or toes (syndactyly) or the presence of extra digits (polydactyly).
Most cases of Klippel-Trenaunay syndrome are sporadic and there is no recognized gender or racial predilection. The prevalence of Klippel-Trenaunay syndrome (as such including Klippel-Trenaunay-Weber) is ~1 in 100,000 people worldwide 3. Sporadic means that it occurs in people with no history of the disorder in their family. Studies suggest that the condition results from gene mutations that are not inherited. These genetic changes, which are called somatic mutations, arise randomly in one cell during the early stages of development before birth. However, a few cases are thought to be passed down through families (inherited) 4.
Although there is no cure for Klippel-Trenaunay syndrome, the goal is to manage symptoms and prevent complications.
Figure 1. Klippel trenaunay syndrome

Note: A port wine stain (capillary malformation)–usually of an extremity– along with underlying soft tissue hypertrophy. Bone length discrepancy. Dysfunction of the lymphatics along with lymphangiomas may be associated.
Figure 2. Klippel Trenaunay syndrome

Figure 3. Klippel trenaunay syndrome – note lower limb swelling, port wine stain and lateral marginal varicose veins
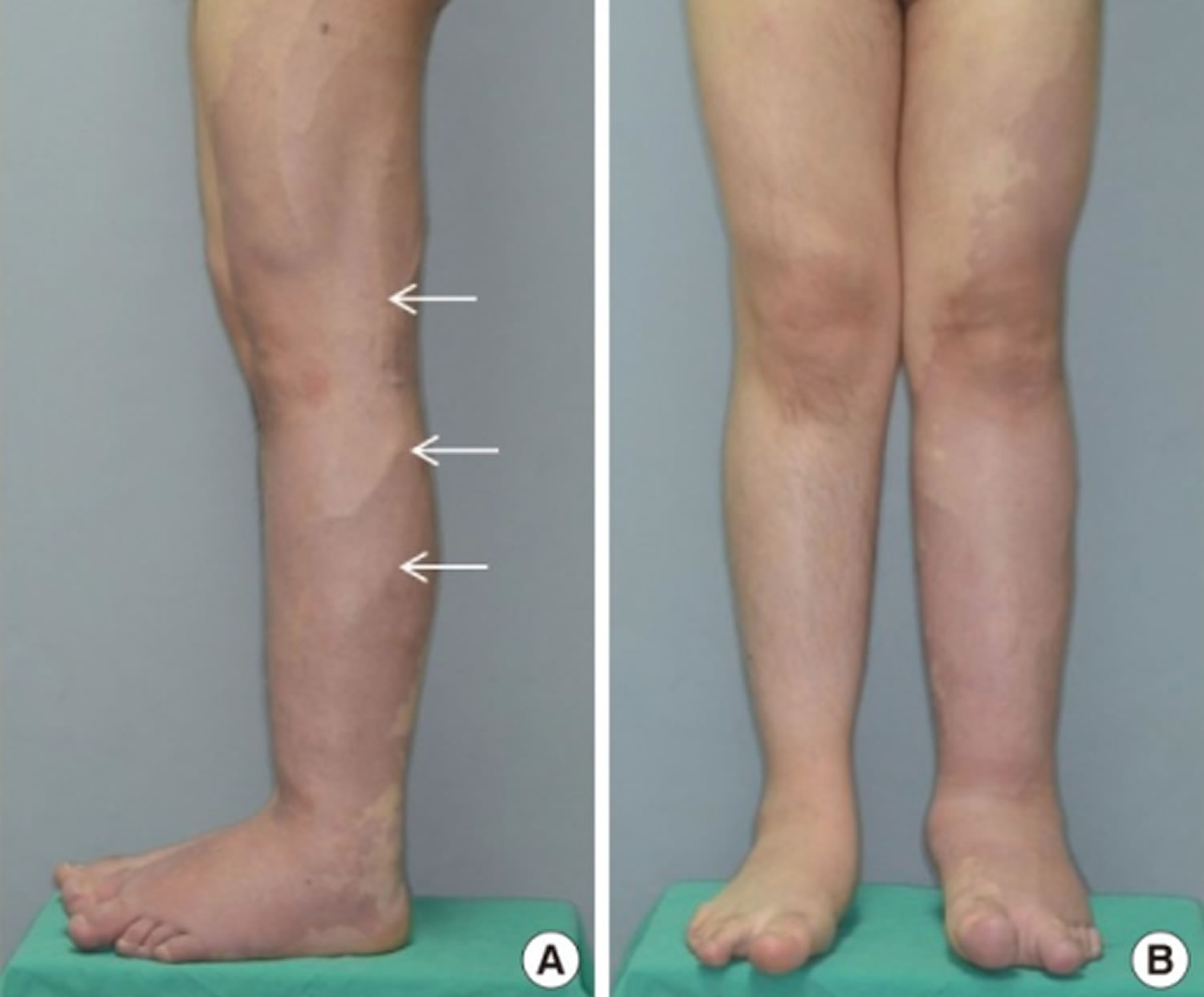
Figure 4. Klippel Trenaunay syndrome – Port Wine Stain

Klippel trenaunay weber syndrome life expectancy
Life expectancy depends on the severity of the malformation. Most people with Klippel-Trenaunay syndrome do well, although the condition may affect their appearance. Some people have psychological problems from the condition.
Klippel-Trenaunay syndrome is often a progressive disorder, and complications may be life-threatening. However, many individuals can live well while managing their symptoms.
Klippel-Trenaunay syndrome complications
Complications of Klippel-Trenaunay syndrome can result from abnormal development of blood vessels, soft tissues, bones and the lymphatic system. These can include:
- Port-wine stain complications. Some areas of the port-wine stain may thicken over time and may form blisters (blebs) that are prone to bleeding and infections.
- Vein malformations. Varicose veins can cause major pain and skin ulcers due to poor circulation. Deeper abnormal veins can increase the risk of blood clots (deep vein thrombosis) and cause a life-threatening condition called pulmonary embolism if they dislodge and travel to the lungs. Venous malformations in the pelvis and abdominal organs can cause internal bleeding. Superficial veins can develop less serious but painful clots and inflammation (superficial thrombophlebitis).
- Overgrowth of bones and soft tissue. Overgrowth of bone and tissue can cause pain, a feeling of heaviness, enlargement of the limb and problems with movement. Overgrowth that causes one leg to be longer than the other can cause problems with walking and may lead to hip and back problems.
- Lymphatic system abnormalities. An abnormality can cause fluid buildup and swelling in the tissues of the arms or legs (lymphedema), skin breakdown and skin ulcers, the development of small masses (lymphatic cysts) in the spleen, leakage of lymphatic fluid, or infection of the layer under the skin (cellulitis).
- Chronic pain. Pain can be a common problem that results from complications such as infections, swelling or vein problems.
Klippel-Trenaunay syndrome causes
Klippel-Trenaunay syndrome is almost always sporadic, which means that it occurs in people with no history of the disorder in their family. Studies suggest that the condition results from PIK3CA gene mutations that are not inherited. These genetic changes, which are called somatic mutations, arise randomly in one cell during the early stages of development before birth. As cells continue to divide during development, cells arising from the first abnormal cell will have the mutation, and other cells will not. This mixture of cells with and without a genetic mutation is known as mosaicism. However, a few cases are thought to be passed down through families (inherited) 4.
Klippel-Trenaunay syndrome can be caused by mutations in the PIK3CA gene. This gene provides instructions for making the p110 alpha (p110α) protein, which is one piece (subunit) of an enzyme called phosphatidylinositol 3-kinase (PI3K). PI3K plays a role in chemical signaling that is important for many cell activities, including cell growth and division (proliferation), movement (migration) of cells, and cell survival. These functions make PI3K important for the development of tissues throughout the body.
The PIK3CA gene mutations associated with Klippel-Trenaunay syndrome alter the p110α protein. The altered subunit makes PI3K abnormally active, which allows cells to grow and divide continuously. Increased cell proliferation leads to abnormal growth of the bones, soft tissues, and blood vessels.
Klippel-Trenaunay syndrome is one of several overgrowth syndromes, including megalencephaly-capillary malformation syndrome, that are caused by mutations in the PIK3CA gene. Together, these conditions are known as the PIK3CA-related overgrowth spectrum (PROS).
Because not everyone with Klippel-Trenaunay syndrome has a mutation in the PIK3CA gene, it is possible that mutations in unidentified genes may also cause this condition.
Klippel-Trenaunay syndrome symptoms
Typical symptoms include hemangiomas (abnormal benign growths on the skin consisting of masses of blood vessels) and varicose veins. Fused toes or fingers, or extra toes or fingers, may be present. In some cases, internal bleeding may occur as a result of blood vessel malformations involving organs such as the stomach, rectum, vagina, liver, spleen, bladder, kidneys, lungs, or heart. Individuals are also at risk for blood clots.
People who have Klippel-Trenaunay syndrome may have the following features, which can range from mild to more extensive:
- Port-wine stain. This pink to reddish-purple birthmark is caused by extra tiny blood vessels (capillaries) in the top layer of skin. The birthmark usually covers part of one leg, but can involve any portion of the skin, and may get darker or lighter with age.
- Vein malformations. These include swollen, twisted veins (varicose veins) usually on the surface of the legs. Deeper abnormal veins in the arms, legs, abdomen and pelvis can occur. There may be spongy tissue filled with small veins in or under the skin. Venous abnormalities may become more prominent with age.
- Overgrowth of bones and soft tissue. This begins in infancy and is usually limited to one leg, but it can occur in an arm or, rarely, in the trunk or face. This overgrowth of bone and tissue creates a larger and longer extremity. Rarely, fusion of fingers or toes, or having extra fingers or toes occurs.
- Lymphatic system abnormalities. The lymphatic system — part of the immune system that protects against infection and disease and transports lymphatic fluid — can be abnormal. Extra lymphatic vessels can be present that don’t work properly and can lead to leakage and swelling.
- Other conditions. Klippel-Trenaunay syndrome can also include cataracts, glaucoma, hip dislocation at birth and blood-clotting problems.
Capillary Malformation
This is the most common cutaneous manifestation of Klippel-Trenaunay syndrome. Typically, capillary malformations involve the enlarged limb, although skin changes may be seen on any part of the body. The lower limb is the affected site in ~95% of patients.
At birth, Klippel-Trenaunay syndrome presents with scattered, geographic capillary stains. With age, the surface of the capillary malformation becomes studded with tiny lymphatic vesicles that often ooze clear fluid and turn black due to intralesional bleeding.
Lymphatic Malformation
Lymphatic malformation presents as localized or generalized overgrowth caused by micro- and macrocystic anomalies, sometimes in association with lymphedema. Often there is lymphatic swelling and fatty deposition on the contralateral foot. The lymphatic anomalies can also occur in the pelvis, bladder and lower gastrointestinal tract. Lymphatic cysts in the spleen are also common. Lymphatic malformation is documented by ultrasonography and/or MRI. Lymphography shows that lymphedema is the result of diminished number or absence of lymphatic channels.
Episodic infections (cellulitis) are common and probably related to poor lymphatic drainage in the limb.
Venous Malformation and varicose veins
Venous abnormalities are always present but variable and involve the entire affected extremity. Present in a majority of patients with Klippel-Trenaunay syndrome, commonly located on the lateral aspect of the affected limb/leg 5. Typically there are anomalous embryonic veins called the “lateral marginal vein” (the vein of Servelle) has been a most typical finding (68-80% of patients) 6. Dilatation of superficial veins may not be apparent in infancy, but becomes more prominent with age. Lymphatic malformation and venous malformation can also involve the pelvic or abdominal organs resulting in bleeding from the rectum, vagina or urinary bladder. Abnormal fatty deposits accompany the venous and lymphatic anomalies.
Venous malformations can occur in both the superficial and deep venous systems. Superficial venous abnormalities range from ectasia of small veins to persistent embryological veins and large venous malformations. Deep venous abnormalities include aneurysmal dilatation, aplasia, hypoplasia, duplications, and venous incompetence.
Many patients with extensive abnormal veins have a low-grade hematologic condition called “localized intravascular coagulopathy” which can be determined by measuring increased D-dimers in the blood. Stagnant blood in the dilated veins may clot and trigger a generalized bleeding disorder called “disseminated intravascular coagulopathy” (DIC).
Visceral manifestations
Rectal and bladder hemorrhage are serious complications of pelvic vascular malformations and have been reported in 1% of Klippel Trenaunay syndrome cases 2.
Vascular malformations can involve the:
- Gastrointestinal tract (20%)
- bleeding is the most common symptom and range from occult bleeding to massive, life-threatening haemorrhages and consumptive coagulopathy
- the most frequently reported sites are the distal colon and rectum
- upper gastrointestinal bleeding from jejunal haemangiomas may also occur 7
- Genitourinary tracts
- involved in more severe cases
- the absence of severe limb varicosities or venous malformations does not preclude the presence of pelvic involvement
- gross haematuria, which is recurrent and painless, is usually the first clinical sign of bladder involvement and frequently manifests early in life
- renal hypertrophy and venous enlargement may occur ipsilaterally to affected side 8
- vascular malformations are often located on the anterior bladder wall and dome
- the trigone and bladder neck are rarely involved
- genital lesions usually do not cause clinical problems for patients with Klippel-Trenaunay syndrome; however, some patients who report erectile dysfunction have abnormal penile veins
- Spleen
- Splenic hemangiomas may occur 9
Overgrowth
Enlargement of the extremity consists of bone elongation, circumferential soft-tissue hypertrophy or both. This often manifests as leg-length discrepancy, although any limb may be affected.
Enlargement of the limb can be minimal to grotesque. Overgrowth in length is typical; however, in some patients the affected limb is shorter than normal. Frequently there is enlargement of the opposite foot.
Skeletal manifestations
These are usually secondary to leg-length difference 10:
- ipsilateral hip dislocation
- scoliosis
Klippel Trenaunay syndrome diagnosis
Diagnosis of Klippel-Trenaunay syndrome begins with a physical exam. Referral to a vascular malformations specialist is helpful for evaluation and treatment recommendations. During the evaluation your doctor:
- Asks questions about your family and medical history
- Does an exam to look for swelling, varicose veins and port-wine stains
- Visually evaluates growth of bones and soft tissues
Several diagnostic tests can help your doctor evaluate and identify the type and severity of the condition and help determine treatment. Some tests include:
- Duplex scanning. This test uses high-frequency sound waves to create detailed images of blood vessels.
- Scanogram. Also called scanner photography, this X-ray technique helps to see images of bones and measure their lengths.
- MRI and magnetic resonance angiography. These procedures help differentiate between bone, fat, muscle and blood vessels.
- CT scan. A CT scan creates 3-D images of the body that helps look for blood clots in veins.
- Contrast venography. This procedure involves injecting a dye into veins and taking X-rays that can reveal abnormal veins, blockages or blood clots.
Klippel-Trenaunay syndrome radiology
Intrauterine ultrasound
Prenatal ultrasound may diagnose Klippel-Trenaunay syndrome as early as 15th week of gestation, based on limb hypertrophy and associated subcutaneous cystic lesions. 3D US may reveal leg width difference. Possible additional features include 4:
- fetal hydrops
- cardiac failure
- polyhydramnios
Plain radiograph
On conventional radiography, bone elongation contributing to leg length discrepancy, soft-tissue thickening, or calcified phleboliths may be seen.
Figure 5. Klippel-Trenaunay syndrome plain x-ray of both arms showing overgrowth of bone and soft tissue seen in the hands bilaterally

MRI
T2-weighted MR images may show malformed venous and lymphatic lesions as areas of high signal intensity.
MR imaging depicts deep extension of low-flow vascular malformations into muscular compartments and the pelvis and their relationship to adjacent organs as well as bone or soft-tissue hypertrophy.
Figure 6. Klippel-Trenaunay syndrome MRI suggestive of mixed vascular malformation involving the entire upper limb, involving skin, subcutaneous tissues, muscles and bone.

Angiography
Typical angiographic findings, which may also be seen on contrast-enhanced CT-scan or MRI, include lower leg superficial varicoid drainage without a deep venous system. The marginal vein of Servelle is a pathognomonic finding (a subcutaneous vein found in the lateral calf and thigh) 11.
Klippel Trenaunay syndrome treatment
Although there’s no cure for Klippel-Trenaunay syndrome, your doctor can help you manage symptoms and prevent complications.
Because Klippel-Trenaunay syndrome may affect many systems in the body, your health care team may include specialists in vascular medicine and surgery, skin diseases (dermatology), interventional radiology, orthopedic surgery, physical therapy and rehabilitation, and other areas as needed.
You and your doctor can work together to determine which of the following treatments are most appropriate for you.
Treatments may include:
- Compression therapy. Bandages or elastic garments are wrapped around affected limbs to help prevent swelling, problems with varicose veins and skin ulcers. These bandages or elastic garments often need to be custom-fit. Intermittent pneumatic compression devices — leg or arm sleeves that automatically inflate and deflate at set intervals — may be used.
- Physical therapy. Massage, compression and limb movement as appropriate may help relieve lymphedema in arms or legs and swelling of the blood vessels.
- Orthopedic devices. These may include orthopedic shoes or shoe inserts to compensate for differences in leg length.
- Epiphysiodesis (surgical closure of the growth plate ). This is an orthopedic surgical procedure that effectively can stop length overgrowth of the lower limb.
- Embolization. This procedure, performed through small catheters placed into the veins or arteries, blocks blood flow to certain blood vessels.
- Laser therapy. Laser therapy is available to lighten or remove the port wine stain. Laser and pulse-light therapy are also used to heat the blood vessel to shrink it. Laser therapy is most effective for the treatment of small varicose veins. Laser therapy may be used as an additional treatment after sclerotherapy, endovenous procedures, or surgery of larger veins. Lasers are also being used for endovenous ablation of larger varicose veins. Laser treatments may require several sessions, spaced at six-week intervals, to properly treat the vein.
- Laser or radiofrequency ablation of veins. Endovenous thermal ablation is a newer version of ligation and stripping. During this procedure, a laser or high-frequency radio waves are used to create intense local heat in the varicose vein. The technology is different with each type of energy source, but both forms of local heat close up the targeted vessel. This treatment closes off the problem veins but leaves them in place so there is minimal bleeding and bruising. Compared with ligation and stripping, endovenous thermal ablation results in less pain and a faster return to normal activities, with similar cosmetic results.
- Sclerotherapy. Sclerotherapy involves the injection of a solution directly into the varicose veins that cause them to collapse and disappear. Several sclerotherapy treatments usually are required to achieve the desired results. Foam sclerotherapy is a variation of the procedure performed under ultrasound guidance that involves the injection of a foaming agent mixed with a sclerosing agent. The foaming agent moves blood out of the vein so the sclerosing agent will have better contact with the vein wall. Sclerotherapy can eliminate the pain and discomfort of varicose veins and helps prevent complications such as venous hemorrhage and ulceration.
- Ligation and Stripping. Ligation means the surgical tying of veins through a small incision in the skin to prevent pooling of blood. Ligation may be used in conjunction with vein stripping, or removal of the vein. In many instances, the vein is removed using a minimally invasive surgical procedure called venous ablation.
- Surgery. In some cases, surgical removal or reconstruction of affected veins, removal of excess tissue, and correction of the overgrowth of bone may be beneficial.
- Medication. Early research indicates that a drug called sirolimus (Rapamune) may help to treat symptomatic complex vascular malformations, but it may have significant side effects and more studies are needed.
In addition, treatment may be needed for complications such as bleeding, pain, infection, blood clots or skin ulcers.
Recommended management for the following malformations associated with Klippel-Trenaunay syndrome is as follows:
Capillary Malformation
The vesicles in the capillary malformation can be improved by laser therapy, sclerotherapy or sometimes resection and closure of the skin or replacement with a split-thickness skin graft.
Lymphatic Malformation
Macrocystic lymphatic malformation can be deflated by sclerotherapy (injection of irritating solutions), whereas, microcystic lymphatic malformation may require resection.
Venous Malformation
Blood stagnates in large dilated veins, and thus there is a risk for initiating a clotting disorder or thrombosis and pulmonary embolism. Anticoagulation with heparin is often necessary prior to radiologic or surgical intervention. Large venous channels can be obliterated by sclerotherapy or endovascular laser. Chronic bleeding from the colon may require surgical resection. Bleeding lesions in the bladder can be controlled by laser done through a cystoscope. An elastic compressive stocking is often useful to minimize discomfort and swelling due to venous distension in the limb.
Overgrowth
Enlarged toes may require amputation to narrow the foot and permit footwear. Discrepancy in leg length can be corrected by inserting a lift in the shoe on the normal foot to prevent compensatory curvature of the spine (scoliosis). Surgical closure of the growth plate at the knee (epiphysiodesis) is often needed to equalize leg length.
Staged contour resection is possible to diminish girth of the limb. These procedures are less effective if the abnormal fat and vasculature extends beneath the deep fascia of the leg into the muscle layer.
Home remedies
Strategies to help manage Klippel-Trenaunay syndrome symptoms include:
- Keep appointments. Regularly scheduled appointments can help your doctor identify and address problems early. Ask your doctor about a schedule of appointments appropriate for you.
- Use orthopedic shoes, if recommended. Orthopedic shoes or shoe inserts may improve your physical function.
- Follow your doctor’s recommendations on physical activity. Encouraging use of affected limbs as appropriate may help relieve lymphedema and swelling of the blood vessels.
- Elevate affected limbs. When possible, raising your leg or other affected limb can help reduce lymphedema.
- Notify your doctor of changes. Work with your doctor to manage your symptoms and prevent complications. Contact your doctor if you have symptoms of blood clots or an infection or if you experience increased pain or swelling.
Coping and support
Living with Klippel-Trenaunay syndrome can be a challenge. Support and advocacy groups can provide a connection with other people who have Klippel-Trenaunay syndrome. The K-T Support Group (https://k-t.org/), Vascular Birthmarks Foundation (https://www.birthmark.org) and other organizations provide educational materials, resources and information about support groups. Ask your doctor if there is a local support group in your area.
Talking with a psychologist, psychiatrist or other mental health professional may also be helpful to many people with Klippel-Trenaunay syndrome.
- Hamburg classification system of vascular malformations. https://radiopaedia.org/articles/hamburg-classification-system-of-vascular-malformations[↩]
- Cha SH, Romeo MA, Neutze JA. Visceral manifestations of Klippel-Trénaunay syndrome. Radiographics. 25 (6): 1694-7. doi:10.1148/rg.256055042 https://pubs.rsna.org/doi/10.1148/rg.256055042[↩][↩]
- Copel J. Obstetric Imaging. Elsevier Health Sciences. (2012) ISBN:1437725562.[↩][↩]
- Marler JJ, Fishman SJ, Upton J et-al. Prenatal diagnosis of vascular anomalies. J. Pediatr. Surg. 2002;37 (3): 318-26. J. Pediatr. Surg. https://www.ncbi.nlm.nih.gov/pubmed/11877641[↩][↩][↩]
- Beard JD, Gaines PA, Loftus I. Vascular and Endovascular Surgery, Companion to Specialist Surgical Practice. Elsevier Health Sciences. (2013) ISBN:0702049662.[↩]
- Zea MI, Hanif M, Habib M, Ansari A. Klippel-Trenaunay Syndrome: a case report with brief review of literature. Journal of dermatological case reports. 3 (4): 56-9. doi:10.3315/jdcr.2009.1038 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3163347/[↩]
- Samo S, Sherid M, Husein H et-al. Klippel-Trenaunay Syndrome Causing Life-Threatening GI Bleeding: A Case Report and Review of the Literature. Case Rep Gastrointest Med. 2013;2013 : 813653. doi:10.1155/2013/813653 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3686071/[↩]
- Turkmen M, Kavukçu S, Çakmakci H et-al. A girl of Klippel-Trenaunay Weber syndrome coexistence of recurrent bloody vaginal discharge. Int Urol Nephrol. 2010;42 (3): 575-8. doi:10.1007/s11255-009-9640-z https://www.ncbi.nlm.nih.gov/pubmed/19768566[↩]
- Pakter RL, Fishman EK, Nussbaum A et-al. CT findings in splenic hemangiomas in the Klippel-Trenaunay-Weber syndrome. J Comput Assist Tomogr. 11 (1): 88-91 https://www.ncbi.nlm.nih.gov/pubmed/3027143[↩]
- Meier S. Klippel-Trenaunay syndrome: a case study. Adv Neonatal Care. 2009;9 (3): 120-4. doi:10.1097/ANC.0b013e3181a68b15 https://www.ncbi.nlm.nih.gov/pubmed/19542774[↩]
- Dubois J, Alison M. Vascular anomalies: what a radiologist needs to know. Pediatr Radiol. 2010;40 (6): 895-905. doi:10.1007/s00247-010-1621-y https://www.ncbi.nlm.nih.gov/pubmed/20432007[↩]





{kind=link}