Contents
What is Factor V Leiden thrombophilia
Factor V Leiden thrombophilia (also known as Activated Protein C Resistance) is an inherited disorder of blood clotting. Factor V Leiden (also known as Labile Factor) is the name of a specific gene mutation that results in thrombophilia, which is an increased tendency to form abnormal blood clots that can block blood vessels. Between 3 to 8% of healthy Caucasian (white) U.S. and European populations carry one copy of the factor V Leiden mutation, and about 1 in 5,000 people have two copies of the mutation. The mutation is less common in other populations. Factor V Leiden is also found in 20% of patients with venous thrombosis (clots in the veins).
Factor V Leiden protein is a catalyst, accelerating the process by which prothrombin is converted to thrombin, the initial step in clot formation. The coagulation system is controlled by several proteins, including a protein called activated protein C. Activated protein C normally inactivates (breaks down) coagulation factor V, which slows down the clotting process and prevents clots from growing too large. However, in people with factor V Leiden thrombophilia, coagulation factor V cannot be inactivated (broken down) normally by activated protein C. As a result, persistence of factor V in the bloodstream leads to a tendency for blood clots to occur, increasing the chance of developing abnormal blood clots.
Other factors also increase the risk of developing blood clots in people with factor V Leiden thrombophilia. These factors include increasing age, obesity, injury, surgery, smoking, pregnancy, and the use of oral contraceptives (birth control pills) or hormone replacement therapy. The risk of abnormal clots is also much higher in people who have a combination of the factor V Leiden mutation and another mutation in the F5 gene. Additionally, the risk is increased in people who have the factor V Leiden mutation together with a mutation in another gene involved in the coagulation system.
Factor V Leiden mutation
Factor V Leiden is the most common inherited form of thrombophilia (an increased tendency to form abnormal blood clots in blood vessels). Between 3 and 8 percent of people with European ancestry carry one copy of the factor V Leiden mutation in each cell, and about 1 in 5,000 people have two copies of the mutation. The mutation is less common in other populations.
A particular mutation in the F5 gene causes factor V Leiden thrombophilia. The F5 (factor V) gene provides instructions for making a protein called coagulation factor V (factor 5). This protein plays a critical role in the coagulation system, which is a series of chemical reactions that forms blood clots in response to injury.
Figure 1. Blood clotting (coagulation) factors
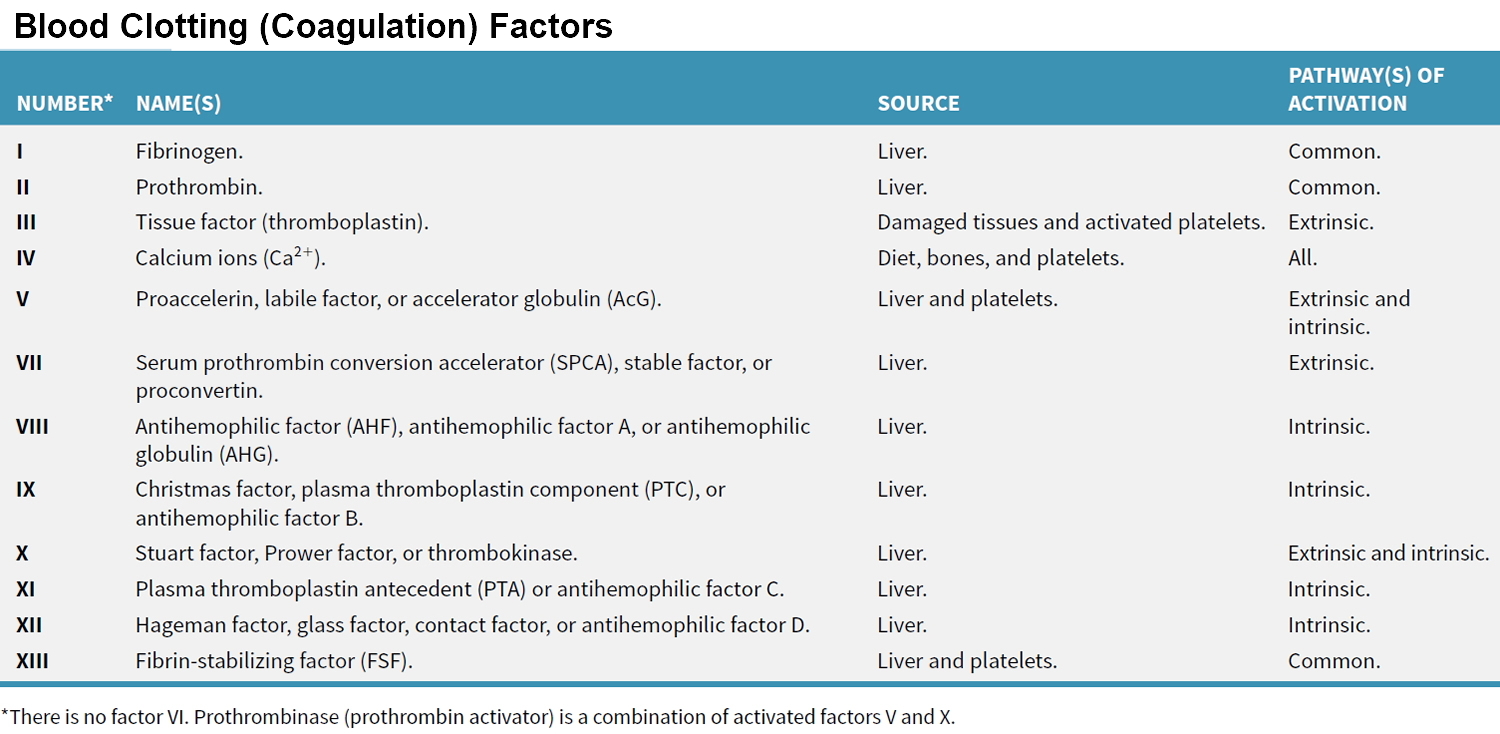
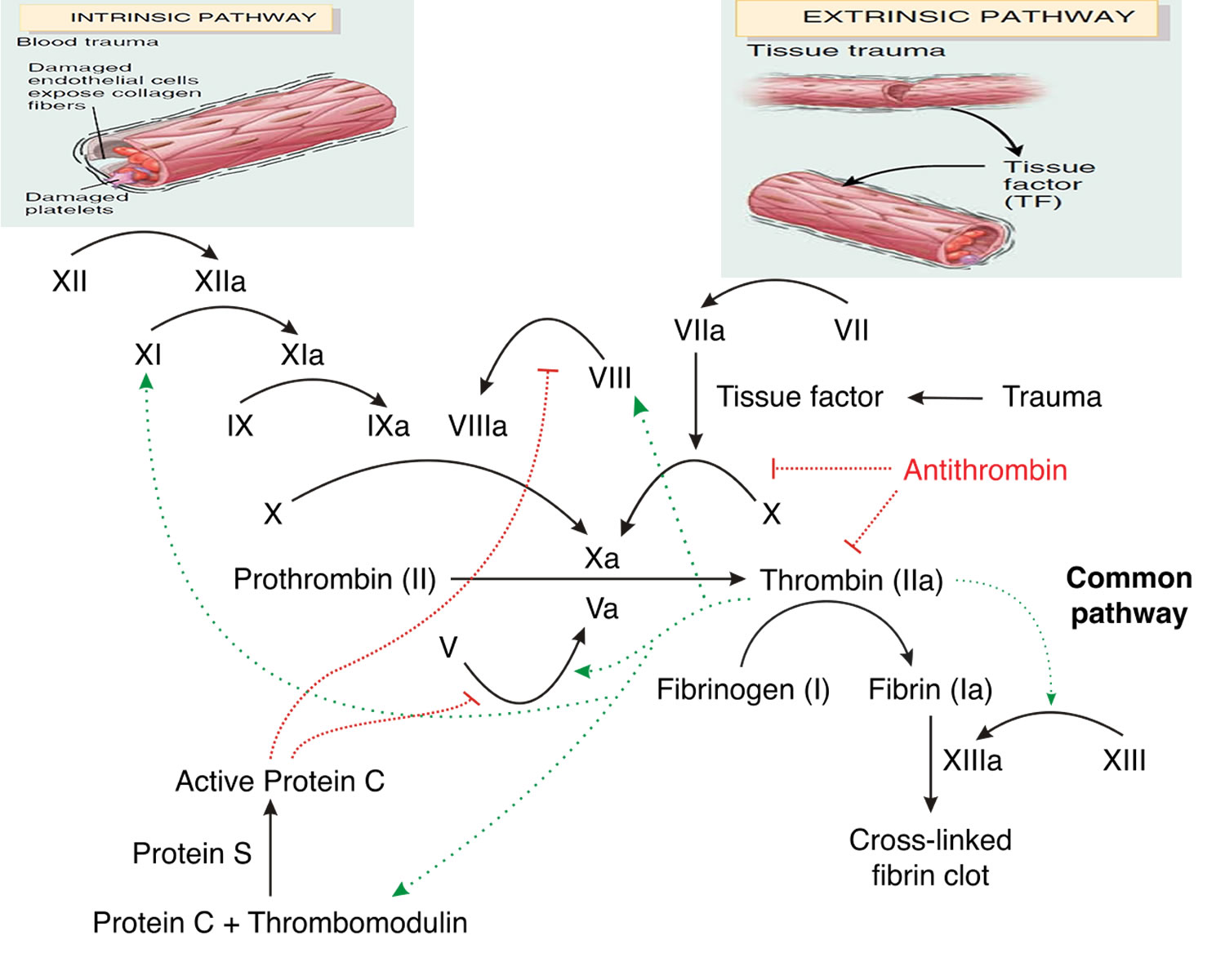
Figure 2. Blood-clotting cascade
People with factor V Leiden thrombophilia have a higher than average risk of developing a type of blood clot called a deep venous thrombosis (DVT). Deep venous thrombosis (DVTs) occur most often in the legs, although they can also occur in other parts of the body, including the brain, eyes, liver, and kidneys. Factor V Leiden thrombophilia also increases the risk that clots will break away from their original site and travel through the bloodstream. These clots can lodge in the lungs, where they are known as pulmonary emboli. Although factor V Leiden thrombophilia increases the risk of blood clots, only about 10 percent of individuals with the factor V Leiden mutation ever develop abnormal clots.
Factor V Leiden Pregnancy
The factor V Leiden mutation is associated with a slightly increased risk of pregnancy loss (miscarriage). Women with this mutation are two to three times more likely to have multiple (recurrent) miscarriages or a pregnancy loss during the second or third trimester. Some research suggests that the factor V Leiden mutation may also increase the risk of other complications during pregnancy, including pregnancy-induced high blood pressure (preeclampsia), slow fetal growth, and early separation of the placenta from the uterine wall (placental abruption). However, the association between the factor V Leiden mutation and these complications has not been confirmed. Most women with factor V Leiden thrombophilia have normal pregnancies.
Factor V Leiden Heterozygous
Factor V Leiden is the most common inherited form of thrombophilia. The risk of developing a clot in a blood vessel depends on whether a person inherits one or two copies of the factor V Leiden mutation. People who inherit two copies of the mutation, one from each parent, have a higher risk of developing a clot than people who inherit one copy of the mutation. Inheriting one copy (Factor V Leiden Heterozygous) of the mutation from a parent increases by fourfold to eightfold the chance of developing a clot. People who inherit two copies (Factor V Leiden Homozygous) of the mutation, one from each parent, may have up to 80 times the usual risk of developing this type of blood clot. Considering that the risk of developing an abnormal blood clot averages about 1 in 1,000 per year in the general population, the presence of one copy of the factor V Leiden mutation increases that risk to 1 in 125 to 1 in 333 (or 3 to 8 in 1,000). Having two copies of the mutation may raise the risk as high as 1 in 12.5 (or 80 in 1,000).
Factor V Leiden Deficiency
Factor V deficiency (also known as Owren’s Disease or Parahemophilia) is a rare bleeding disorder because the body produces less Factor V than it should or because the factor V is not working properly, the clotting reaction is blocked prematurely and the blood clot does not form. Factor V deficiency should not be confused with Factor V Leiden, which is a clotting disorder. The signs and symptoms of Factor V deficiency can begin at any age, although the most severe cases are apparent in childhood. Factor V deficiency commonly causes nosebleeds; easy bruising; bleeding under the skin; bleeding of the gums; and prolonged or excessive bleeding following surgery, trauma, or childbirth. Babies with severe factor V deficiency are at increased risk of intracranial hemorrhage, or bleeding in the brain. Women with factor V deficiency can have heavy or prolonged menstrual bleeding (menorrhagia). Bleeding into joint spaces (hemarthrosis) can also occur, although it is rare. Severely affected individuals have an increased risk of bleeding inside the skull (intracranial hemorrhage), in the lungs (pulmonary hemorrhage), or in the gastrointestinal tract, which can be life-threatening.
Factor V deficiency was first described in a Norwegian patient in 1943 and reported by Dr. Paul Owren in 1947. Factor V deficiency affects an estimated 1 in 1 million people; fewer than 200 cases have been documented worldwide. Factor V deficiency is more common in countries such as Iran and southern India, where it occurs up to ten times more frequently than in western countries.
Factor V deficiency is usually caused by mutations in the F5 gene, which provides instructions for making a protein called coagulation factor V. This protein plays a critical role in the coagulation system, which is a series of chemical reactions that forms blood clots in response to injury. F5 gene mutations that cause factor V deficiency prevent the production of functional coagulation factor V or severely reduce the amount of the protein in the bloodstream. People with this condition typically have less than 10 percent of normal levels of coagulation factor V in their blood; the most severely affected individuals have less than 1 percent. A reduced amount of functional coagulation factor V prevents blood from clotting normally, causing episodes of abnormal bleeding that can be severe.
Factor V deficiency is inherited in an autosomal recessive pattern, which means that both parents must carry the F5 gene to pass it on to their children. It also means that the disorder affects both males and females. Factor V deficiency is very rare, but like all autosomal recessive disorders, it is found more frequently in areas of the world where marriage between close relatives is common.
Individuals with Factor V deficiency have both copies of the F5 gene (one from each parent) in each cell have mutations. Individuals with a mutation in a single copy of the F5 gene (only one copy of F5 gene) have a reduced amount of coagulation factor V in their blood and can have mild bleeding problems, although most have no related health effects.
Very rarely, a form of factor V deficiency is caused by abnormal antibodies that recognize coagulation factor V. Antibodies normally attach (bind) to specific foreign particles and germs, marking them for destruction, but the antibodies in this form of factor V deficiency attack a normal human protein, leading to its inactivation. These cases are called acquired factor V deficiency and usually occur in individuals who have been treated with substances that stimulate the production of anti-factor V antibodies, such as bovine thrombin used during surgical procedures. There is no known genetic cause for this form of the condition.
Factor V deficiency is also seen in people with:
- Liver diseases.
- Factor V inhibitor.
- Myeloproliferative disorders.
- Disseminated intravascular coagulation (DIC) and fibrinolysis.
- Mild decrease in the newborn.
The symptoms of factor V deficiency are generally mild. Some people may experience no symptoms at all. However, children with a severe deficiency of factor V may bleed very early. Some patients have experienced bleeding in the central nervous system (the brain and spinal cord) very early in life.
Factor V deficiency symptoms
Common symptoms
- nosebleeds (epistaxis)
- easy bruising
- heavy or prolonged menstrual bleeding (menorrhagia)
- bleeding in the mouth, particularly after dental surgery or tooth extraction
Other reported symptoms
- bleeding in the gut (gastrointestinal hemorrhage)
- muscle bleeds
- abnormal bleeding during or after injury, surgery, or childbirth
Rare symptoms
- bleeding into joints (hemarthrosis)
- bleeding in the central nervous system (the brain and spinal cord)
Factor V deficiency diagnosis
Factor V deficiency is diagnosed by a variety of blood tests that should be performed by a specialist at a hemophilia/bleeding disorders treatment center. Diagnosis is made through activated partial thromboplastin time (aPTT) test, prothrombin time (PT) test and thrombin clotting time (TCT) test. People with abnormal levels of factor V should also have their factor VIII levels checked to rule out combined factor V and factor VIII deficiency, which is a completely separate disorder. Diagnosis can be confirmed with a factor V assay. Factor V is found in both plasma and platelets, so platelet function may be affected.
Factor V deficiency treatment
Treatment for factor V deficiency is usually only needed for severe bleeds or before surgery. Fresh frozen plasma (FFP) is the usual treatment because there is no commercially available factor V concentrate exists. Platelet transfusions, which contain factor V, are also sometimes an option. Platelets are small blood cells that are involved in the formation of blood clots and the repair of damaged blood vessels. Certain clotting factors, including factor V, are stored in small sacs inside them. Platelet transfusions are sometimes used to treat factor V deficiency.
Plasma is the portion of blood that contains all the clotting factors, as well as other blood proteins. Fresh frozen plasma (FFP) is used to treat rare bleeding disorders when concentrates of the specific factor that is missing are not available. Fresh frozen plasma (FFP) is the usual treatment for factor V deficiency. However, it usually does not undergo viral inactivation, so the risk of transmission of infectious diseases is higher. Viral-inactivated fresh frozen plasma (FFP) is available in some countries and is preferable. Circulatory overload is a potential problem with this treatment: since the concentration of each coagulation factor in FFP is low, a large volume of it must be given over several hours in order to achieve an adequate rise in factor level. This large amount of FFP needed can overload the circulatory system and stress the heart. Other complications of treatment with fresh frozen plasma can occur, particularly allergic reactions or lung problems (transfusion-related lung injury). These problems are much less common if viral-inactivated pooled fresh frozen plasma is used. Fresh frozen plasma (FFP) is administered intravenously.
Excessive menstrual bleeding in women with factor V deficiency may be controlled with hormonal contraceptives (birth control pills), intra-uterine devices (IUDs) or antifibrinolytic drugs.
Combined factor VIII and factor V deficiency is a very rare disorder, found in fewer than 100 patients from 60 families worldwide, mostly in Iran, Israel and Italy. Most cases are mild to moderate. Symptoms can include frequent nosebleeds, easy bruising, and excessive bleeding after injury or surgery. Women can experience menorrhagia and postpartum hemorrhage. Treatment includes fresh frozen plasma. In some cases, bleeds may be treated with factor VIII concentrates and desmopressin acetate, the synthetic version of the hormone vasopressin.
Other names for Factor V deficiency
- Labile factor deficiency
- Owren disease
- Owren’s disease
- Parahemophilia
- Proaccelerin deficiency
Factor V Leiden complications
Factor V Leiden can be associated with a variety of serious and potentially serious clotting complications, including:
- Pregnancy complications. Most women with factor V Leiden have normal pregnancies. But the mutation has been linked with an increased risk of miscarriage and possibly other complications during pregnancy, including pregnancy-induced high blood pressure (preeclampsia), slow fetal growth and early separation of the placenta from the uterine wall (placental abruption). If you’re a pregnant woman with factor V Leiden, be sure your doctor monitors you carefully throughout your pregnancy.
- Deep vein thrombosis (DVT). People with factor V Leiden have an increased risk of developing deep vein thrombosis compared with someone without the mutation, though the overall risk of developing deep vein thrombosis is still low.
- Pulmonary embolism (PE). Deep vein thrombosis puts you at risk of a clot breaking off and traveling to your lungs or, rarely, your brain. A pulmonary embolism can be fatal. It’s important to watch for signs and symptoms of a pulmonary embolism, such as shortness of breath or chest pain, and to seek prompt medical attention.
Factor V Leiden causes
A blood clot (thrombus) normally forms to stop the bleeding when an artery or vein is damaged, such as when you experience a cut. Clots are formed by chemical reactions between specialized blood cells (platelets) and proteins in your blood (clotting factors). Anti-clotting factors prevent an excessive formation of blood clots.
Normally, factor V is a clotting protein. Anti-clotting proteins break up factor V, keeping it from forming clots when clotting isn’t needed.
Factor V Leiden makes it harder for anti-clotting proteins to break up factor V. This keeps factor V in the blood longer and increases the chance of clotting.
If you have factor V Leiden, you inherited either one copy (heterozygous) or, rarely, two copies (homozygous) of the defective gene. Inheriting one copy slightly increases your risk of developing blood clots. Inheriting two copies — one from each parent — significantly increases your risk of developing blood clots.
Risk factors for Factor V Leiden
As Factor V Leiden is a disease based on a genetic abnormality, the most important predisposing factor is a family history of the disease.
A family history of factor V Leiden increases your risk of inheriting the disorder. The disorder is most common in people who are white and of European descent.
Factor V Leiden symptoms
Factor V Leiden is present from birth. However, patients are often affected later in life (young adult-middle age), if at all.
The symptoms of factor V Leiden vary among individuals. There are some individuals who have the F5 gene and who never develop thrombosis, while others have recurring thrombosis before the age of 30 years. This variability is influenced by the number of F5 gene mutations a person has, the presence of other gene alterations related to blood clotting, and circumstantial risk factors, such as surgery, use of oral contraceptives and pregnancy.
Symptoms of Factor V Leiden include:
- Having a first DVT (deep vein thrombosis) or PE (pulmonary embolism) before 50 years of age.
- Having recurring DVT or PE.
- Having venous thrombosis in unusual sites in the body such as the brain or the liver.
- Having a DVT or PE during or right after pregnancy.
- Having a history of unexplained pregnancy loss in the second or third trimester.
- Having a DVT or PE and a strong family history of venous thromboembolism.
A proportion of the population with Factor V Leiden will suffer venous thrombosis. Thomboembolism, including pulmonary embolism, carries significant morbidity and mortality.
A clot in a deep vein (DVT)
This is known as deep vein thrombosis (DVT). Deep vein thrombosis may not cause any symptoms. If signs and symptoms do occur, they commonly affect your legs, including swelling of your ankles and feet. Other signs and symptoms may include:
- Pain
- Significant swelling
- Redness
- Warmth
A clot closer to the surface of your skin
This is referred to as superficial venous thrombosis, phlebitis or thrombophlebitis. Signs and symptoms usually include:
- Warmth
- Tenderness or pain, often in or around the vein with the blood clot
- Redness
A clot that travels to your lungs – pulmonary embolism (PE)
Known as a pulmonary embolism (PE), this occurs when a deep vein clot breaks free and travels through the right side of your heart to your lung, where it blocks blood flow. This can be a life-threatening situation. Signs and symptoms may include:
- Sudden shortness of breath
- Chest pain when breathing in
- A cough that produces bloody or blood-streaked sputum
- Rapid heartbeat (tachycardia)
The use of hormones, such as oral contraceptive pills (OCPs) and hormone replacement therapy (HRT), including estrogen and estrogen-like drugs) taken after menopause, increases the risk of developing DVT and PE. Healthy women taking oral contraceptive pills have a three- to four-fold increased risk of developing a DVT or PE compared with women who do not take oral contraceptive pill. Women with factor V Leiden who take oral contraceptive pills have about a 35-fold increased risk of developing a DVT or PE compared with women without factor V Leiden and those who do not take oral contraceptive pills. Likewise, postmenopausal women taking hormone replacement therapy (HRT) have a two- to three-fold higher risk of developing a DVT or PE than women who do not take HRT, and women with factor V Leiden who take HRT have a 15-fold higher risk. Women with heterozygous factor V Leiden who are making decisions about oral contraceptive pill or HRT use should take these statistics into consideration when weighing the risks and benefits of treatment.
Factor V Leiden diagnosis
Your doctor will likely suspect factor V Leiden if you’ve had one or more episodes of thrombosis or pregnancy loss or if you have a strong family history of thrombotic disease. Your doctor can confirm that you have factor V Leiden with a blood test. Two types of tests can be done.
Factor V Leiden test
- Activated protein C resistance test. Your blood sample may be tested to determine whether your blood is resistant to activated protein C, one of the anti-clotting proteins that help control factor V. This is known as an activated protein C (APC) resistance assay. If your blood is resistant to activated protein C, you likely have a mutation in the factor V gene.
- Genetic test. A genetic test is done to determine whether you have a factor V gene mutation. It may also be used to confirm the results of the APC resistance test or to determine whether you’ve inherited one or two copies of the gene mutation.
If you’re taking blood-thinning medications (anticoagulants), you may have only the genetic test. Anticoagulants interfere with the activated protein C resistance test.
Testing babies before or soon after birth isn’t recommended. Children who don’t have symptoms of clotting problems also don’t need screening. Blood clots are rare, even in children with factor V Leiden. Testing isn’t recommended until adulthood.
When your child is an adult, he or she will be better able to fully understand the risks and benefits associated with genetic testing. Chances are good that your child may never have any signs or symptoms related to factor V Leiden.
Factor V Leiden treatment
The management of individuals with factor V Leiden depends on the clinical circumstances. People with factor V Leiden who have had a DVT or PE are usually treated with blood thinners, or anticoagulants.
Doctors generally use blood-thinning (anticoagulant) medications, such as warfarin (Coumadin, Jantoven), heparin or low molecular weight heparin to treat people who develop blood clots.
If genetic tests have confirmed that you have factor V Leiden, but you haven’t had any blood clots, then your doctor probably won’t prescribe blood thinners on a regular basis. But you may be given a course of blood thinners to reduce your risk of DVT during high-risk situations, such as having surgery or being hospitalized.
If you have a blood clot, standard initial treatment involves a combination of heparin and warfarin. Your doctor will discontinue the heparin after the initial treatment and continue the warfarin. How long you need to take medication will depend on the circumstances of your thrombosis.
- Heparin. This anticoagulant medication works more quickly than warfarin does. It can be administered directly into a vein (intravenously) or under the skin (subcutaneously). You can inject yourself with some forms of heparin, including enoxaparin (Lovenox) and dalteparin (Fragmin). Heparin is considered safe to take during pregnancy. Possible risks of heparin include excess bleeding and allergic reaction. Heparin doesn’t have a standard dose, so it requires regular blood tests and adjustments to get the right dose for you.
- Warfarin (Coumadin, Jantoven). This anticoagulant comes in pill form, so it’s easier to take than heparin. Warfarin may cause birth defects, so it isn’t usually recommended during pregnancy, especially the first trimester. Bleeding is the most common side effect of warfarin. This drug interacts with many other medications and herbs, so be sure to check with your doctor or pharmacist before taking anything else. As with heparin, there isn’t a standard dose for warfarin, so you’ll need regular blood tests and dose adjustments while taking warfarin.
New oral blood thinners
Three new oral medications have been approved by the Food and Drug Administration for the prevention and treatment of blood clots in certain people. They have an advantage over warfarin, as they don’t require blood test monitoring or dose adjustments. Bleeding complications are the most serious side effect of these medications, but that risk appears to be lower with these drugs than with warfarin:
- Dabigatran (Pradaxa)
- Rivaroxaban (Xarelto)
- Apixaban (Eliquis)
Excessive bleeding caused by these new oral blood thinners can’t be easily reversed. Bleeding caused by heparin and warfarin, on the other hand, can be quickly reversed.
These newer medications also haven’t been well-studied in pregnant women. They may interact with certain medications, but do have far fewer food or drug interactions compared with warfarin.
Talk with your doctor about the risks and benefits for you of new oral blood thinners compared with warfarin.
Follow-up care
If you’re taking an anticoagulant medication that increases the risk of excessive bleeding, your doctor will follow you closely. You’ll have blood tests to help your doctor make sure your blood is capable of clotting enough to stop bleeding if you bruise or cut yourself.
Factor V Leiden during pregnancy
Most women with factor V Leiden have normal pregnancies. However, the risk of blood clots during pregnancy is higher. Factor V Leiden increases the risk of developing a DVT during pregnancy by about seven-fold. Women with factor V Leiden who are planning pregnancy should discuss this with their obstetrician and/or hematologist. Pregnant women with factor V Leiden need close medical supervision throughout their pregnancies. There’s no evidence that preventive treatment with blood-thinning medications would be effective enough to outweigh the potential risks of using these drugs during pregnancy or delivery. For those with a history of DVT or PE, treatment with an anticoagulant during a subsequent pregnancy can prevent recurrent problems.
Home remedies
If you have factor V Leiden, avoiding certain situations might help reduce your risk of developing blood clots. These include:
- Uninterrupted long car or airline trips. When your legs remain still for long periods — more than two hours — your calf muscles don’t contract, which normally helps blood circulate.
- If you can, try to move around whenever possible on a plane. Drink extra water to prevent dehydration, and avoid alcohol. On a car trip, take periodic breaks and walk around.
- If you sit for long periods of time for any reason, get up periodically and stretch your legs.
- Prolonged bed rest, such as during a long illness, or paralysis. Your doctor may suggest the use of compression stockings to keep the blood in your legs moving.
- Injury or surgery. Injury to your veins or surgery can slow blood flow, increasing the risk of blood clots. General anesthetics used during surgery can dilate your veins, which can increase the risk of blood pooling and then clotting. Let your doctor know that you have factor V Leiden.
- Oral contraceptives or estrogen replacement therapy. Because these medications can increase the risk of blood clots on their own, be sure to discuss the risks and the benefits of estrogen-containing medications with your doctor if you have factor V Leiden.
- Being overweight or obese. Being overweight increases the pressure in the veins in your pelvis and legs. Losing weight can lower your risk.
- Smoking. Smoking affects blood clotting and circulation. If you’re a smoker, take steps to quit.
Donating blood
One situation you don’t have to avoid if you have factor V Leiden is donating blood. People with factor V Leiden can usually donate blood if interested in doing so.
If you’re taking blood-thinning medications, you can’t donate blood until those medications are fully out of your system. If you’ve taken blood thinners, check with your doctor before donating blood.
Preventing excessive bleeding
If your factor V Leiden requires you to take anticoagulant medication, here are some steps that might help you prevent injury and avoid excessive bleeding:
- Avoid playing contact sports or engaging in other activities that could result in physical injury. Regular noncontact exercise, such as walking or swimming, is still recommended for good health.
- Use a soft toothbrush and waxed floss.
- Avoid shaving cuts by using an electric razor.
- Be cautious with household tasks involving knives, scissors and other sharp tools.





{kind=link}