Contents
What is a penile implant
Penile implants are devices placed inside the penis to allow men with erectile dysfunction to get an erection. Erectile dysfunction has been defined as the inability to achieve or maintain an erection sufficient for sexual performance 1. The term penile implant, penile prosthesis, inflatable penile prosthesis and internal penile prosthesis pump are often used interchangeably and all refer to the multicomponent inflatable penile prosthesis. Penile implants are typically recommended after other treatments such as oral pharmacotherapy, a vacuum erection device, intracavernosal injection, and intraurethral suppositories for erectile dysfunction have failed 2. The first penile implant was introduced by Lash et al. in 1964 as part of a novel surgical reconstruction for Peyronie’s disease 3. Dramatic increase in penile prosthesis implantation occurred in the 1970’s, specifically for men with erectile dysfunction (ED). Scott et al. introduced the world’s first inflatable penile prosthesis in 1973 4. Although prosthetic implants have changed over the years, original design principles remain largely intact with continued improvement to minimize perioperative complications in two or three-piece designs 5.
There are two main types of penile implants, semirigid and inflatable. Each type of penile implant works differently and has various pros and cons.
The placement of penile implants requires surgery. Before choosing penile implants, make sure you understand what surgery involves, including possible risks, complications and follow-up care.
With continuous improvements of penile prostheses and surgical techniques, mechanical failure and postoperative complications, such as prosthesis infection and erosions, have been decreasing since the penile prosthesis was first introduced to the market 6. Several studies reported that mechanical and overall survival rates at 5 years of American Medical Systems 700 CX/CXM range from 85% to 93% and from 77% to 91%, respectively 7.
Why is penile implant surgery done?
For most men, erectile dysfunction can be successfully treated with medications or use of a penis pump (vacuum constriction device). You might consider penile implants if you aren’t a candidate for other treatments or you can’t get an erection sufficient for sexual activity by using other methods.
Penile implants can also be used to treat severe cases of a condition that causes scarring inside the penis, leading to curved, painful erections (Peyronie’s disease).
Although penile implants are the most invasive and least often chosen treatment for erectile dysfunction, most men and their partners report satisfaction with the devices. The 10-year device survival is between 60 and 80 percent.
Penile implants aren’t for everyone. Your doctor might caution against penile implants if you have:
- Erectile dysfunction that’s situational, the result of a relationship conflict or potentially reversible
- An infection, such as a pulmonary infection or urinary tract infection
- Diabetes that isn’t well-controlled
Keep in mind that while penile implants allow men to get an erection, they don’t increase sexual desire or sensation. Most penile implants also won’t make your penis any larger than it naturally is at the time of surgery. In fact, your erect penis might be slightly shorter than it used to be.
How long does penile implant last and do they need to be replaced regularly?
The penile implant can last for a long time and majority of the time 5 years after the penile implant, the patient will have an 85% chance of still having a functional device in their body. Ten years, this number is about 70%. In other words, 70% of people after penile implant will still have a working implant in them 10 years later. There are many of my patients who still have working implants after 20 years, so you don’t need to replace it regularly. Penile implant longevity depends on age. If you get a penile implant when you’re 18, you’re obviously going to have to replace it a couple of times in your life. But with in patients with average ages of about 60–70, when they get a penile implant, they’ll only need it once.
Male penis?
Used for urination and sexual intercourse, the penis is made up of two erectile cylinders (corpora cavernosa) that enlarge with blood during erection. A tough fibrous, partially elastic outer casing surrounds the cavernosa. The corpus spongiosum surrounds the urethra (urinary tube), a tube that runs from the bladder to the end of the penis. The urethra carries urine and semen out of the body.
Figure 1. Male reproductive system
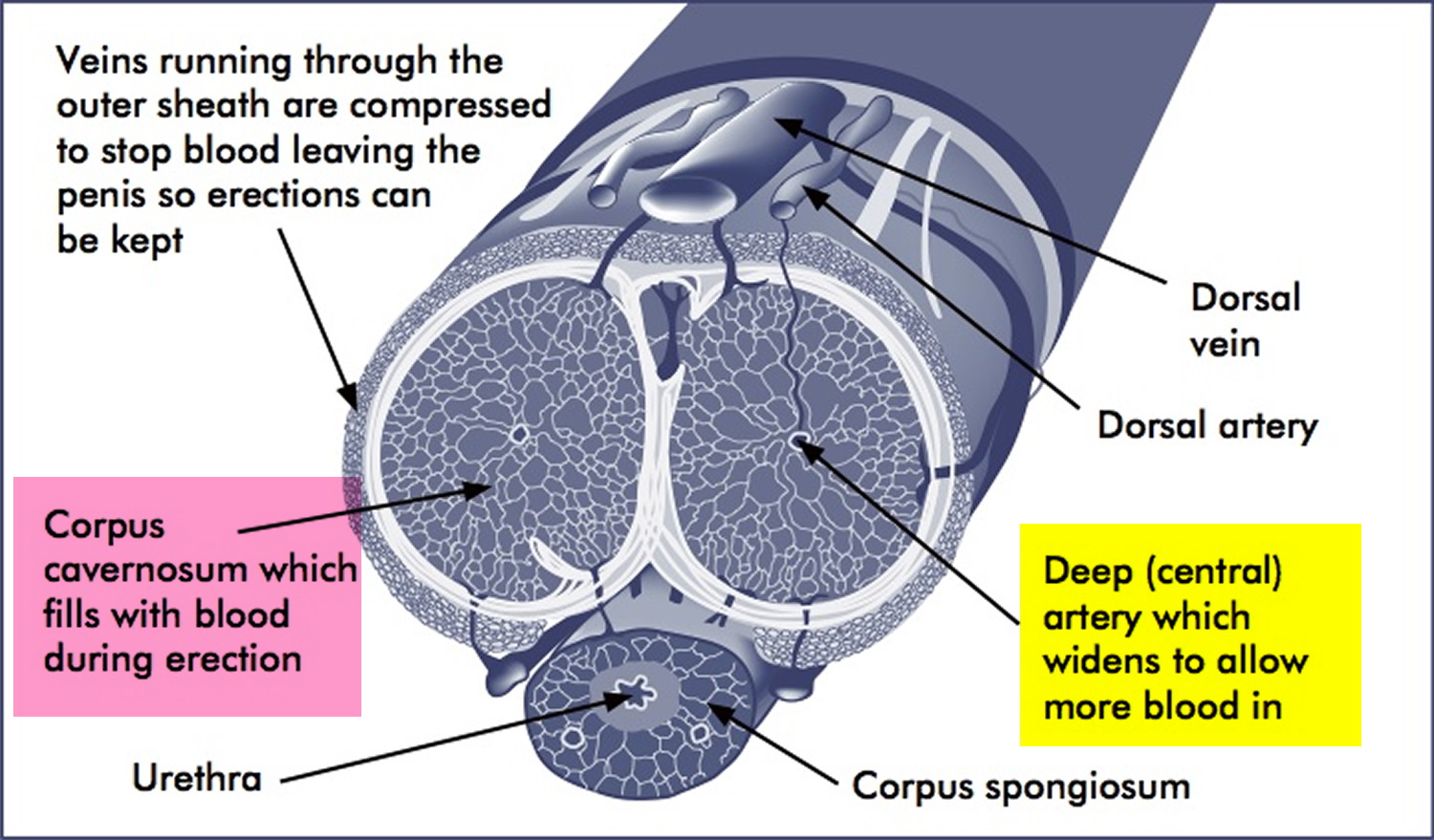
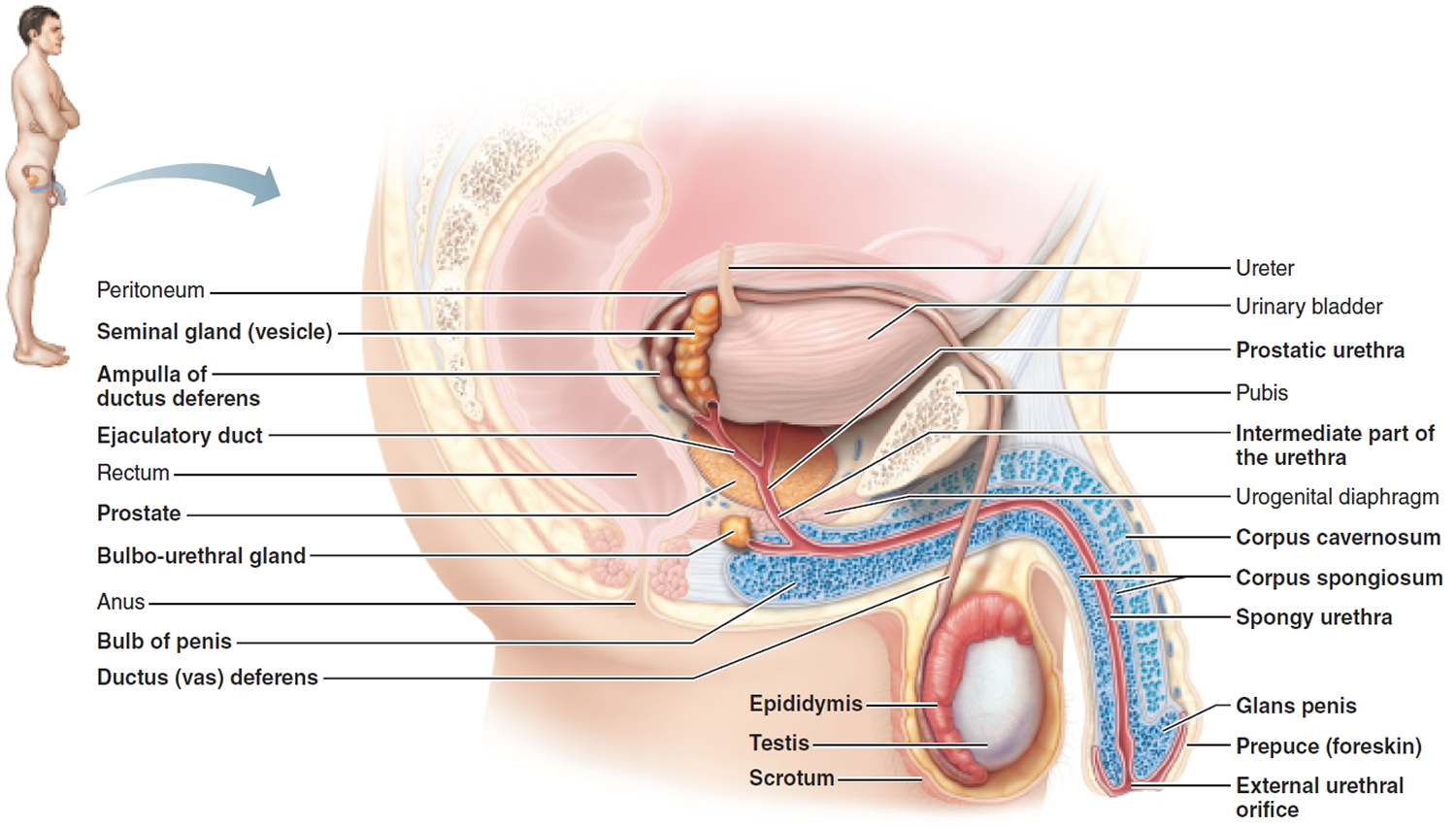 Figure 2. Penis (cross section)
Figure 2. Penis (cross section)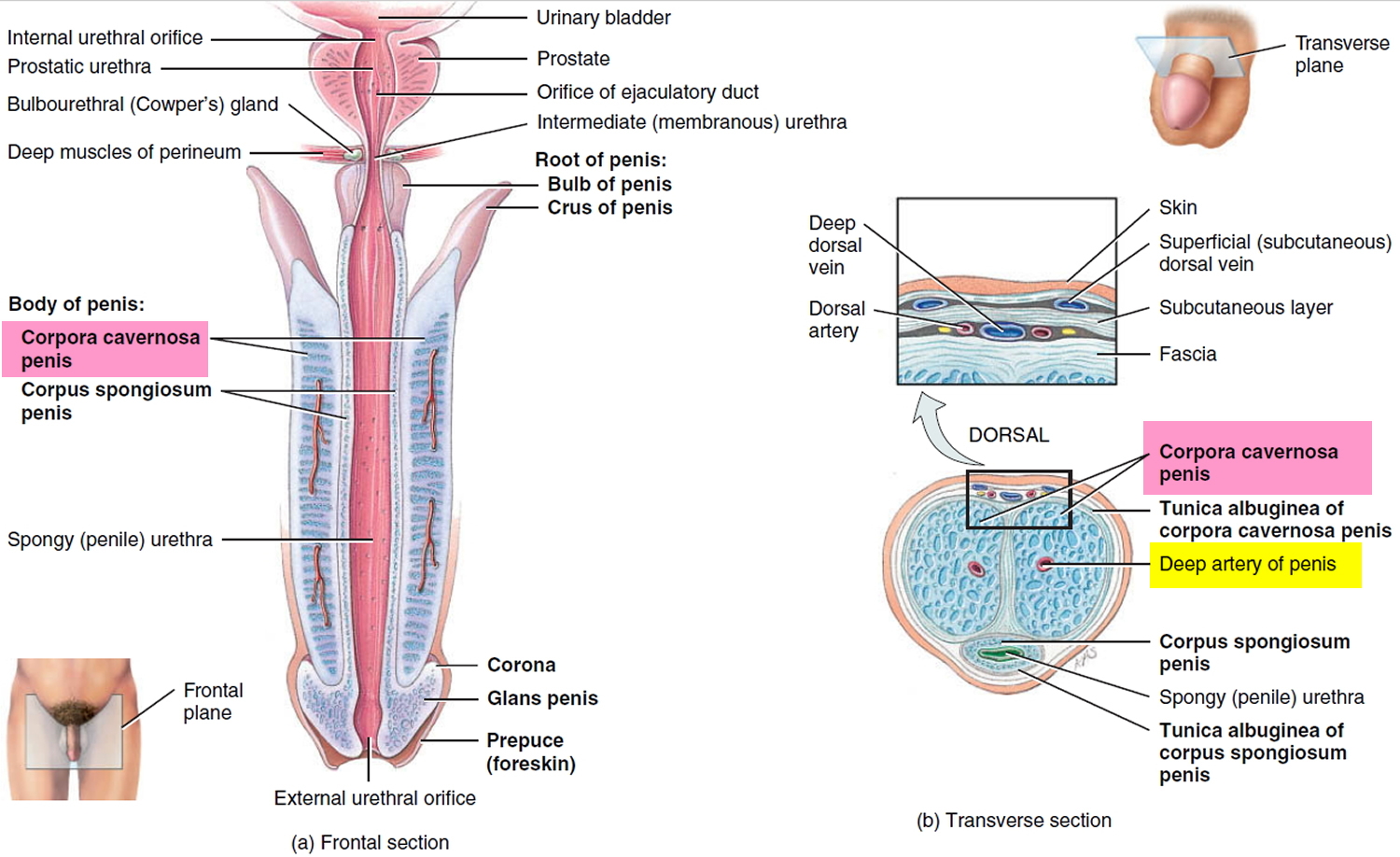
How does a penile implant work
Semirigid malleable prostheses are the simplest and easiest to implant, but they can be difficult to conceal because the penis is always erect (see Figure 4 below).
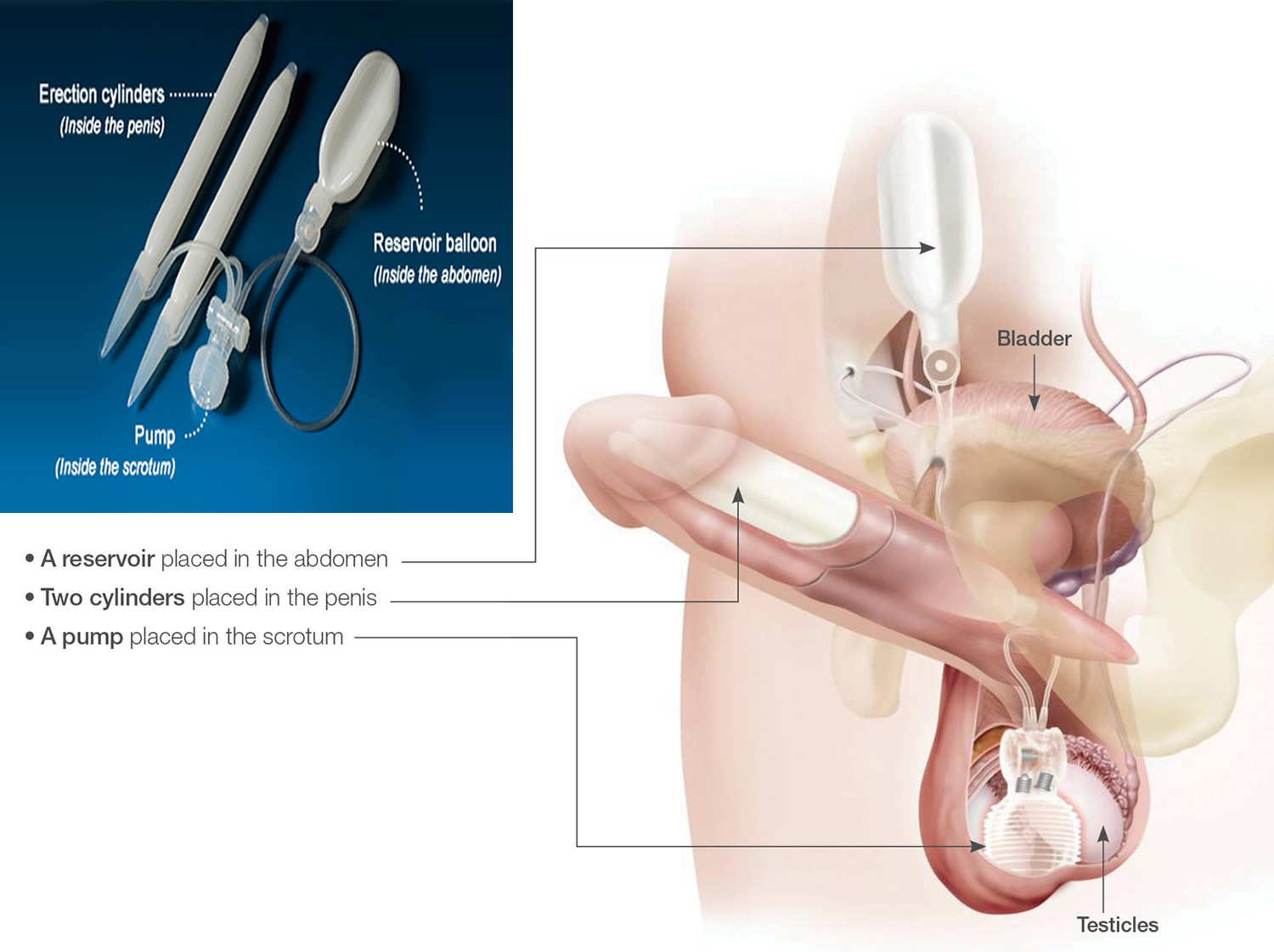
Inflatable prostheses typically consist of two tubes that replace the corpora cavernosa, plus a pump in the scrotum and an intra-abdominal reservoir (see Figures 3 and 5 below). The penile implant pump is a soft saline fluid-filled device (the liquid is water and salt) that can expand and contract without losing elasticity. It consists of three small components: very thin penile tubes, the pump, and the reservoir. The reservoir contains fluid, which is transferred by the pump into the tubes, causing the penis to expand and become rigid.
Figure 3. Penile prosthesis implant
There are two main types of penile implants:
- Inflatable implants. Inflatable devices, the most common type of penile implant used, can be inflated to create an erection and deflated at other times. Three-piece inflatable implants use a fluid-filled reservoir implanted under the abdominal wall, a pump and a release valve placed inside the scrotum, and two inflatable cylinders inside the penis. To achieve an erection, you pump the fluid from the reservoir into the cylinders. Afterward, you release the valve inside the scrotum to drain the fluid back into the reservoir. The two-piece model works in a similar way, but the fluid reservoir is part of the pump implanted in the scrotum.
- Semirigid rods. Semirigid devices are always firm. The penis can be bent away from the body for sexual activity and toward the body for concealment. A positionable penile implant is a semirigid device with a central series of segments held together with a spring on each end. It can maintain upward and downward positions better than other semirigid rods can.
Other special designs can fit a shortened penis, or one that’s larger than average. Some inflatable penile implants are also available with antibiotic coatings, which might help reduce the risk of infection.
Comparing implant types
When choosing which type of penile implant is right for you, consider your personal preference and your medical history. Your doctor might suggest one type of design over another based on your age, risk of infection, and health conditions, injuries or medical treatments you’ve had in the past.
Figure 4. Penile implant semi-rigid. The semirigid penile implant is bent upward for sex and toward the body for concealment under clothing.
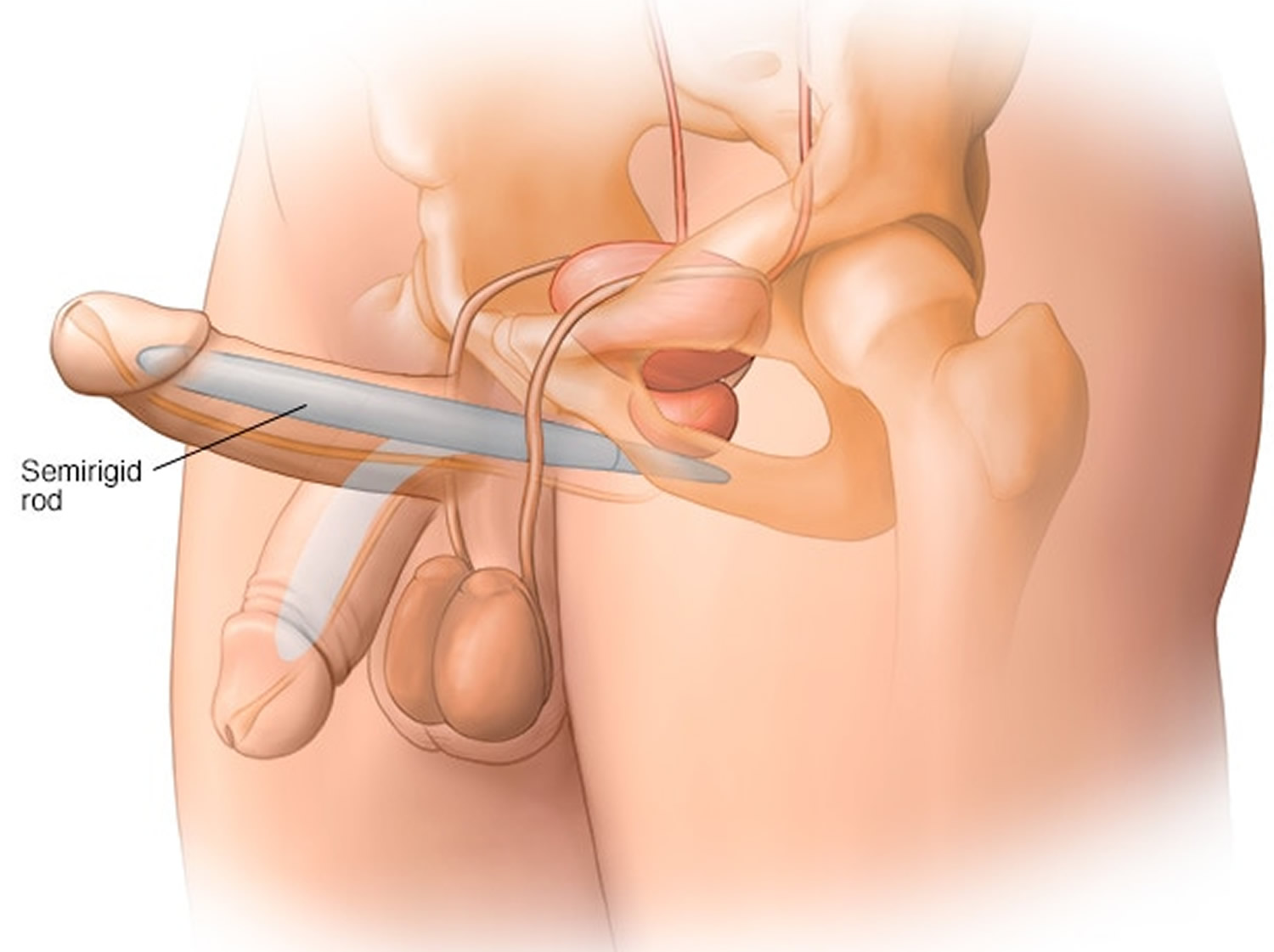
Figure 5. Penile implant two-piece. The two-piece inflatable penile implant consists of inflatable cylinders inside the shaft of the penis and a combined fluid reservoir and pump unit in the scrotum.
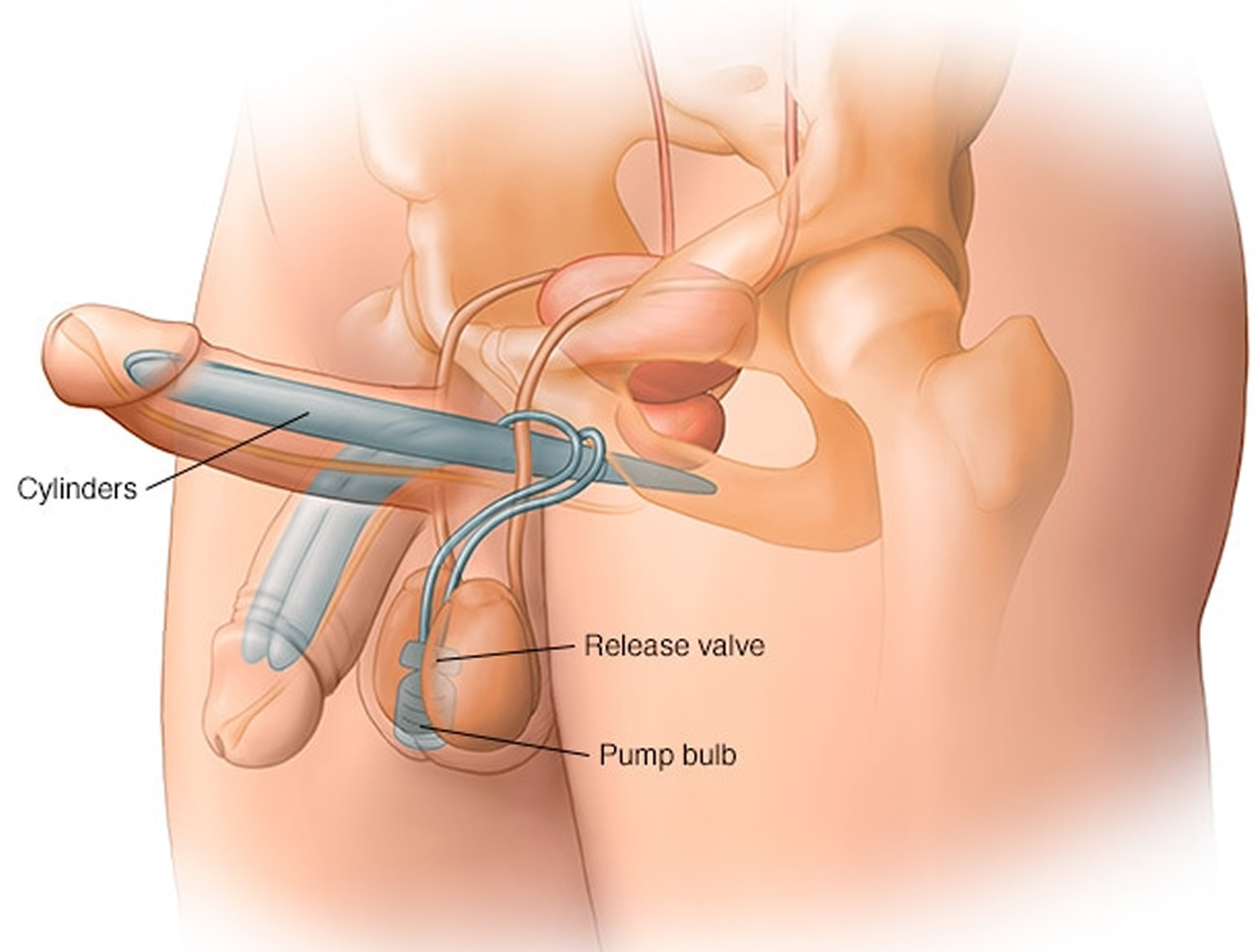
Figure 6. Penile implant three-piece. The three-piece inflatable penile implant consists of inflatable cylinders inside the shaft of the penis, a fluid reservoir under the abdominal wall, and a pump inside the scrotum.
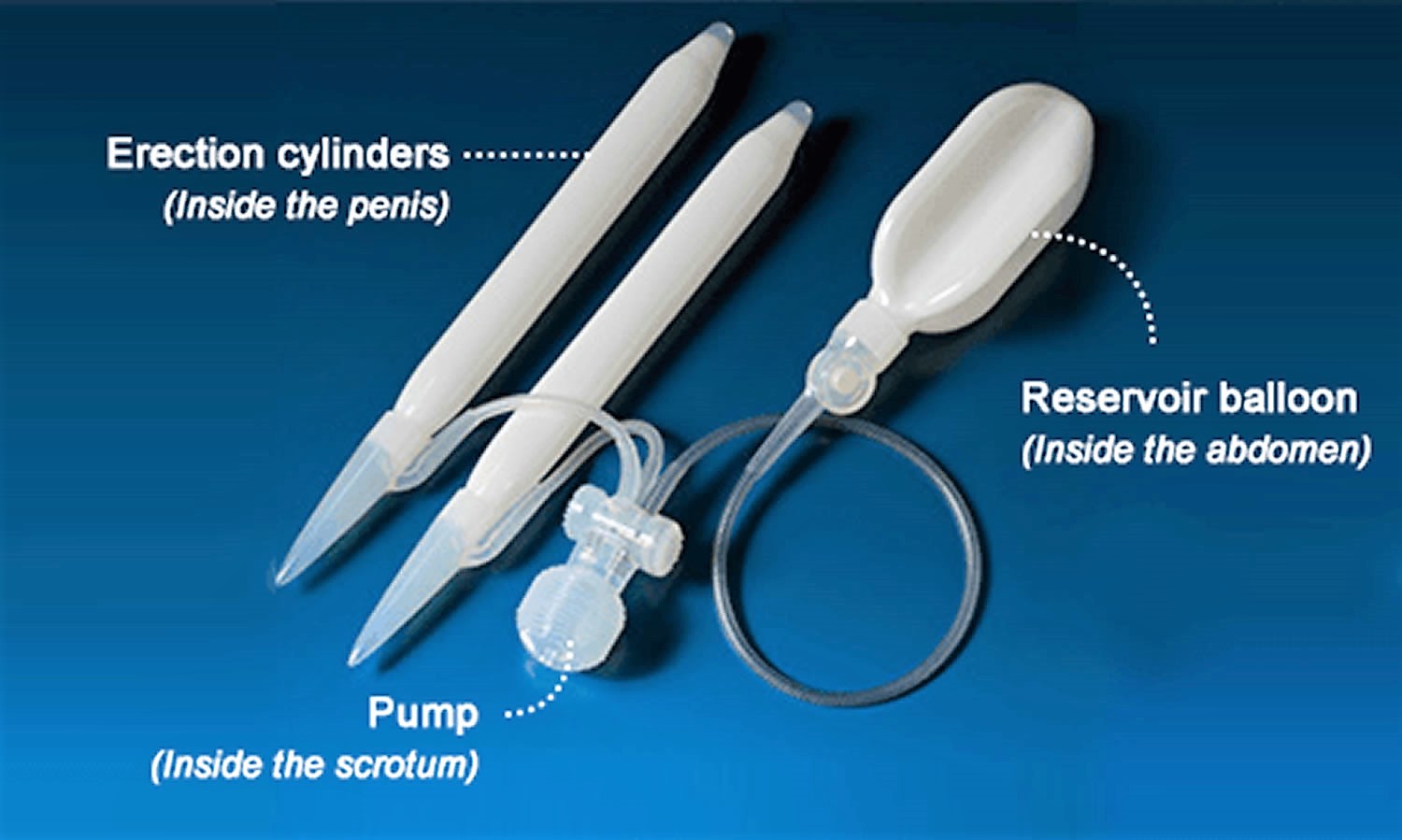
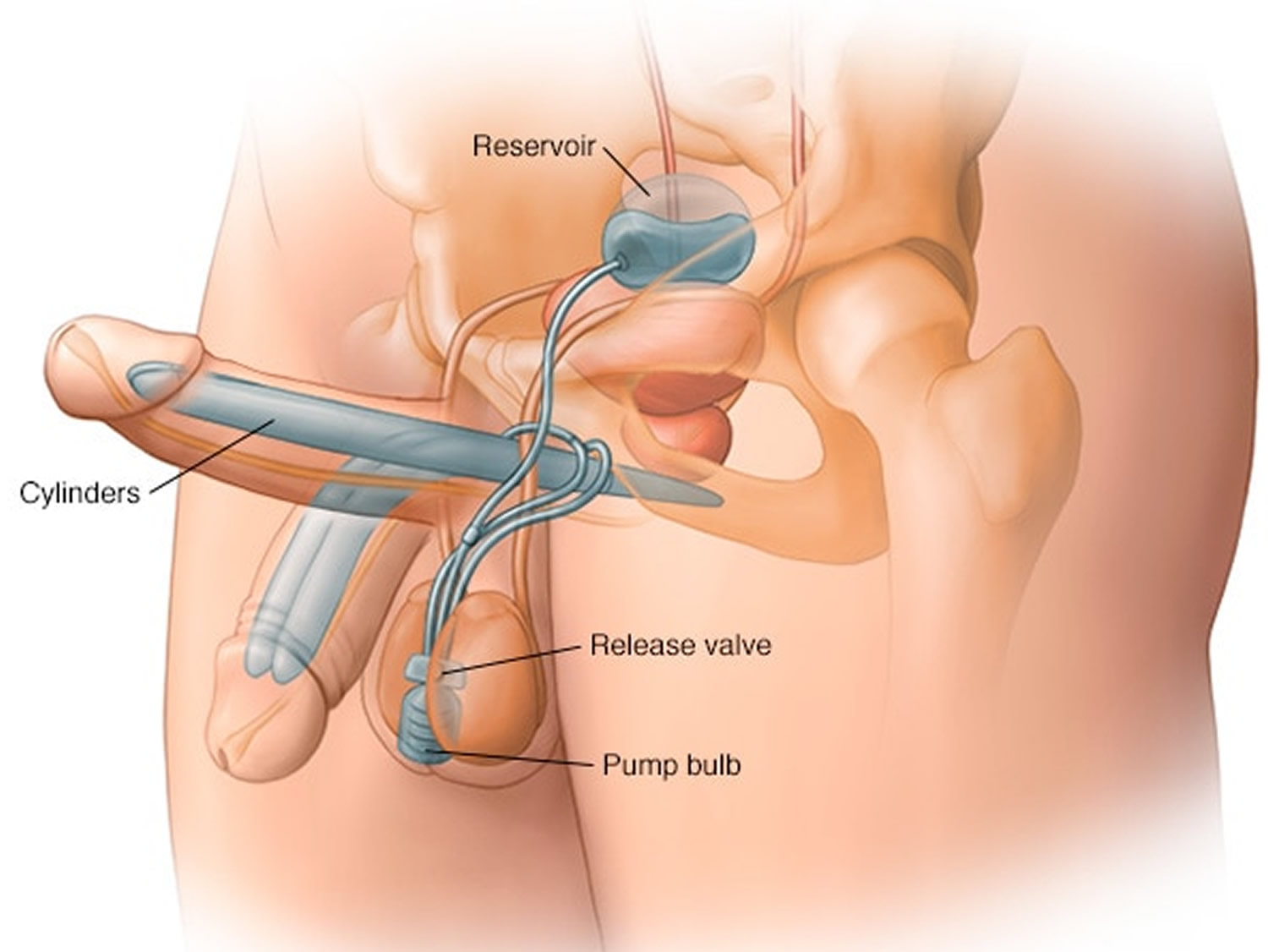
Table 1. Type of penile implants
| Type of penile implant | Pros | Cons |
|---|---|---|
| Three-piece inflatable |
|
|
| Two-piece inflatable |
|
|
| Semirigid rod |
|
|
Prosthetic penis surgery procedure
Initially, you’ll talk to your doctor or a urologist about penile implants. During your visit, your doctor will likely:
- Review your medical history. Be prepared to answer questions about current and past medical conditions, especially your experience with erectile dysfunction. Talk about any medications you’re taking or have taken recently, as well as any surgeries you’ve had.
- Do a physical exam. To make sure penile implants are the best options for you, your doctor will do a physical exam, including a complete urologic exam. Your doctor will confirm the presence and nature of erectile dysfunction, and make sure that your erectile dysfunction can’t be treated in another way. He or she will also try to determine whether there’s any reason that penile implant surgery is likely to cause complications. Your doctor will also examine your ability to use your hands, since some penile implants require greater manual dexterity than others.
- Discuss your expectations. Make sure you understand what the procedure involves and the type of penile implant that suits you best. It’s also important to know that the procedure is considered permanent and irreversible.
Your doctor will also explain the benefits and risks, including potential complications. Ideally, you’ll include your partner in the discussion with your doctor.
Before penile implant surgery you might also need to:
- Avoid certain medications. Your doctor might recommend that you temporarily stop taking aspirin and anti-inflammatory drugs, which can increase your risk of bleeding.
- Arrange for a ride home. Ask your doctor when you’ll be able to go home after surgery. Penile implant surgery typically involves an overnight stay.
- Limit food and liquids. Don’t eat or drink anything after midnight before your surgery, or follow specific instructions from your doctor.
During penile implant surgery
Penile implant surgery is usually done at a surgery center or hospital. Your doctor might give you medication to make you unconscious during the surgery (general anesthesia) or medication that blocks pain in the lower part of your body (spinal anesthesia).
- Your doctor will give you IV antibiotics to help prevent infection. The surgery site will also be shaved immediately before surgery to reduce the risk of infection.
- A tube (catheter) might be inserted into your bladder via your penis to collect urine at some point during surgery. Your surgeon will make an incision below the head of the penis, at the base of the penis or in the lower abdomen.
- Next, your surgeon will stretch the spongy tissue in the penis that would normally fill with blood during an erection. This tissue is inside each of the two hollow chambers called the corpora cavernosa.
- Your surgeon will choose the correct size implant and place the implant cylinders inside your penis. All sizes are customized to your exact body measurements.
If your doctor is implanting a two-piece inflatable device, a pump and valve are placed inside the scrotum. For a three-piece device, your doctor will also implant a fluid reservoir under the abdominal wall through an internal incision.
Once the device is in place, your surgeon will sew the incisions closed. Penile implant surgery usually takes 45 minutes to an hour.
After penile implant surgery
After penile implant surgery, you’ll likely need to take medications to ease pain. Mild pain might persist for several weeks. You might also need to take antibiotics for one week to prevent infection.
Your doctor might recommend keeping your penis up on your lower abdomen and pointing toward your bellybutton during the healing process to prevent downward curvature.
Your doctor will provide specific instructions about when you can resume normal activities. Most men can resume strenuous physical activity and sexual activity about four to six weeks after surgery. You’ll likely need to return to your doctor to have your stitches removed in about two weeks.
At this point, your doctor might recommend fully inflating and deflating inflatable penile implants twice a day to give you practice using them and stretch the area surrounding the cylinders.
Penile implant side effects
Penile implant complications include:
- Infection. As with any surgery, infection is possible. You might be at an increased risk of infection if you have a spinal cord injury or diabetes.
- Implant problems. New penile implant designs are reliable, but in rare cases the implants might malfunction. Surgery is necessary to remove, repair or replace a broken implant.
- Internal erosion or adhesion. In some cases, an implant might stick to the skin inside the penis or wear away the skin from inside the penis. Rarely, an implant breaks through the skin. These problems are sometimes linked to an infection.
During the operation the most important complications can involve the urethra, the bladder and intestine. Urethral injuries may occur during the dilatation of the corpora cavernosa and can especially affect scarred tissues. Bladder and visceral injuries can happen during the positioning of the reservoir with the penoscrotal incision, due to the blindness of this procedure. The opening of the fascia to have access to the Retzius space is a delicate phase because the peritoneum and the bladder can be perforated 8.
Breakage or mechanical failure of the device are complications which may be checked before the implant procedure. Any kind of injury to the prosthesis can be easily avoided by putting sutures on the corpora before the placement of the cylinders, while correct functioning should be tested before the end of the operation in order to allow substitution at this stage.
Infection (ranges from 1.7% to 15%) 9 is an important complication which could cause the revision or the removal of the device. Infections are generally caused by Staphylococcus epidermidis and S. aureus, followed by Gram-negative bacteria, S. aureus and anaerobic organisms 10. Clinically it is characterized by fever, persistent scrotal pain, erythema and evidence of purulent material from the wound. Systemic antibiotic therapy is not sufficient to treat this complication; the removal of the prosthesis is recommended either with immediate replacement or replacement after some months 8. The importance of this aspect is stressed by the introduction of the InhibiZone™ prostheses by AMS® and Titan™ prostheses by Coloplast Ltd®, conceived to inhibit bacterial adhesion and proliferation with a proven reduction in infection rates from 2% to 1.06% 11.
Mechanical disorders of the prosthesis (ranging from 1.4% to 13.7%) 9 are becoming less common thanks to improvement of the devices. The most common complications are fluid loss, cylinder rupture and mechanical breakage, and require removal of the prostheses 11. Auto-inflation (ranging from 2.4% to 11%) 12 is a mechanical disorder which can happen in the implanted prosthesis. In order to avoid this kind of complication Coloplast Ltd® and AMS® introduced antireflux ‘lock-out’ valves with a consequent reduction of auto-inflation to 1.3% 12.
Treating an infection
Infections after penile implant surgery typically occur in the first few weeks or possibly years later. Early infections can cause swelling of the scrotum, pus buildup and fever. Later infections might involve persistent or recurrent long-term pain.
Surgery to remove the implant is likely necessary to treat an infection. Replacing a penile implant can be complicated and can lead to a buildup of scar tissue and a decrease in penis length.
- Consensus development conference statement. National Institutes of Health. Impotence. December 7-9, 1992. Int J Impot Res. 1993 Dec; 5(4):181-284. https://www.ncbi.nlm.nih.gov/pubmed/8173631/[↩]
- Implants, mechanical devices, and vascular surgery for erectile dysfunction. Hellstrom WJ, Montague DK, Moncada I, Carson C, Minhas S, Faria G, Krishnamurti S. J Sex Med. 2010 Jan; 7(1 Pt 2):501-23. https://www.ncbi.nlm.nih.gov/pubmed/20092450/[↩]
- SILICONE IMPLANTATION: INLAY METHOD. LASH H, ZIMMERMAN DC, LOEFFLER RA. Plast Reconstr Surg. 1964 Jul; 34():75-80. https://www.ncbi.nlm.nih.gov/pubmed/14200523/[↩]
- Management of erectile impotence. Use of implantable inflatable prosthesis. Scott FB, Bradley WE, Timm GW. Urology. 1973 Jul; 2(1):80-2. https://www.ncbi.nlm.nih.gov/pubmed/4766860/[↩]
- Penile prostheses. Bettocchi C, Palumbo F, Spilotros M, Palazzo S, Saracino GA, Martino P, Battaglia M, Selvaggi FP, Ditonno P. Ther Adv Urol. 2010 Feb; 2(1):35-40. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3126066/[↩]
- Ji YS, Ko YH, Song PH, Moon KH. Long-term survival and patient satisfaction with inflatable penile prosthesis for the treatment of erectile dysfunction. Korean Journal of Urology. 2015;56(6):461-465. doi:10.4111/kju.2015.56.6.461. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4462637[↩]
- Long-term mechanical reliability of AMS 700 series inflatable penile prostheses: comparison of CX/CXM and Ultrex cylinders. Daitch JA, Angermeier KW, Lakin MM, Ingleright BJ, Montague DK. J Urol. 1997 Oct; 158(4):1400-2. https://www.ncbi.nlm.nih.gov/pubmed/9302130/[↩]
- Penile prosthesis: what should we do about complications? Bettocchi C, Ditonno P, Palumbo F, Lucarelli G, Garaffa G, Giammusso B, Battaglia M. Adv Urol. 2008; ():573560. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2581729/[↩][↩]
- Outcome of penile prosthesis implantation for treating erectile dysfunction: experience with 504 procedures. Minervini A, Ralph DJ, Pryor JP. BJU Int. 2006 Jan; 97(1):129-33. https://www.ncbi.nlm.nih.gov/pubmed/16336342/[↩][↩]
- The use of penile prostheses in the treatment of impotence. Evans C. Br J Urol. 1998 Apr; 81(4):591-8. https://www.ncbi.nlm.nih.gov/pubmed/9598633/[↩]
- Efficacy, safety and patient satisfaction outcomes of the AMS 700CX inflatable penile prosthesis: results of a long-term multicenter study. AMS 700CX Study Group. Carson CC, Mulcahy JJ, Govier FE. J Urol. 2000 Aug; 164(2):376-80. https://www.ncbi.nlm.nih.gov/pubmed/10893589/[↩][↩]
- The mentor Alpha 1 penile prosthesis with reservoir lock-out valve: effective prevention of auto-inflation with improved capability for ectopic reservoir placement. Wilson SK, Henry GD, Delk JR Jr, Cleves MA. J Urol. 2002 Oct; 168(4 Pt 1):1475-8. https://www.ncbi.nlm.nih.gov/pubmed/12352421/[↩][↩]





{kind=link}