Contents
- Subacute thyroiditis
- Thyroid gland
- Subacute granulomatous thyroiditis (de Quervain’s thyroiditis)
- Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) causes
- Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) pathophysiology
- Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) symptoms
- Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) complications
- Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) diagnosis
- Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) treatment
- Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) prognosis
- Subacute lymphocytic thyroiditis
- Subacute postpartum thyroiditis
- Subacute thyroiditis causes
- Subacute thyroiditis symptoms
- Subacute thyroiditis diagnosis
- Subacute thyroiditis differential diagnoses
- Subacute thyroiditis treatment
- Subacute thyroiditis prognosis
Subacute thyroiditis
Subacute thyroiditis is a self-limiting inflammatory condition of the thyroid gland that is typically characterized by a painful tender thyroid gland along with systemic symptoms such as heart palpitations (feelings of having a fast-beating, fluttering or pounding heart), tremor, fever, malaise, and anorexia that often follows an upper respiratory infection 1.
3 forms of subacute thyroiditis are recognized 2:
- Subacute granulomatous thyroiditis also known as subacute painful de Quervain thyroiditis or giant cell thyroiditis 3. Subacute granulomatous thyroiditis or de Quervain’s thyroiditis is the most common cause of a painful thyroid gland 4.
- Subacute lymphocytic thyroiditis also known as subacute painless thyroiditis. Subacute lymphocytic thyroiditis is associated with a painless, firm enlargement of the thyroid gland and high thyroid hormone levels. Only suspicion by the clinician and use of radioactive iodine uptake (RAIU) measurement can distinguish Graves hyperthyroidism from subacute lymphocytic thyroiditis.
- Subacute postpartum thyroiditis – postpartum thyroiditis happens when a person’s thyroid gland becomes inflamed within 1 year of delivering a baby or having a miscarriage or abortion. Subacute postpartum thyroiditis affects a small percentage of pregnant women. The identifying feature is its occurrence 1 to 6 months after childbirth. Women may report lack of sleep, nervousness, fatigue, and easy weight loss 5, 6.
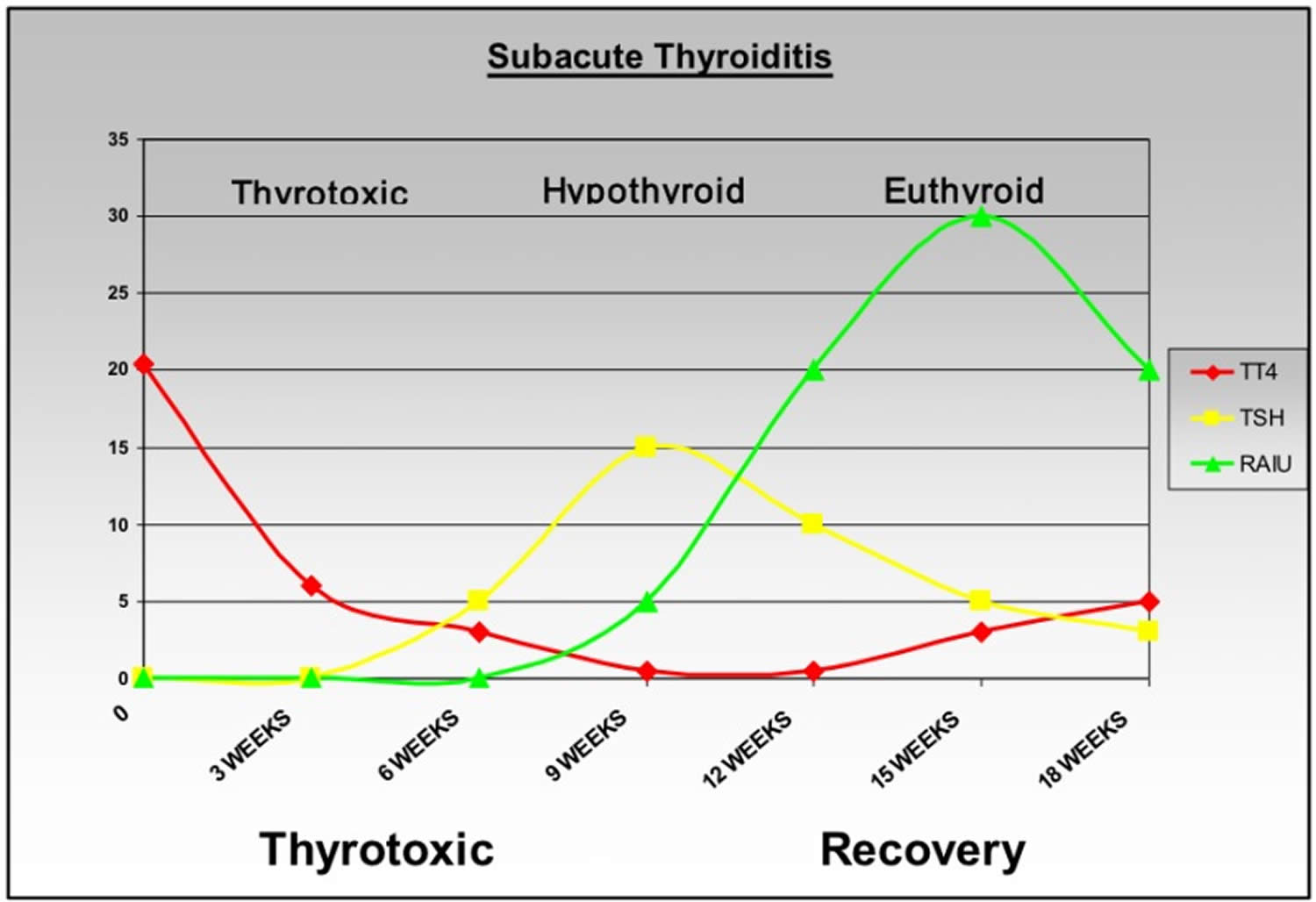
In most types of subacute thyroiditis, there are 3 phases of clinical course:
- Thyrotoxic phase: During this phase, your thyroid is inflamed and releases too many hormones, causing temporary thyrotoxicosis (hyperthyroidism).
- Hypothyroid phase: Following the excessive release of thyroid hormones for a few weeks or months, your thyroid won’t have enough thyroid hormones to release. This leads to a lack of thyroid hormones or underactive thyroid (hypothyroidism).
- Euthyroid phase: During the euthyroid phase, your thyroid hormone levels are normal. This phase may come temporarily after the thyrotoxic phase before going to the hypothyroid phase, or it may come at the end after your thyroid gland has recovered from the inflammation and can maintain a normal hormone level.
Subacute thyroiditis may be responsible for 15 to 20% of patients presenting with hyperthyroidism (thyrotoxicosis or having too much thyroid hormone in your body) and 10% of patients presenting with hypothyroidism (underactive thyroid) 2. Thyroid function testing will help to indicate the presence of subacute thyroiditis as well as determine its phase. Recognizing subacute thyroiditis is important, because it is self-limiting, no specific treatment (such as antithyroid or thyroid hormone replacement therapy) is necessary in most patients 2.
The best available epidemiologic data on the incidence of subacute thyroiditis is from a study conducted by Fatourechi V et al. in Olmstead County, Minnesota, USA, during the period from 1960 to 1997 7. The overall age and sex-adjusted incidence of subacute thyroiditis during this period were 4.9 cases per 100,000/year 7. The most common symptom was thyroid pain (96%); even though most patients achieved complete resolution and a normal thyroid state, about 15% of patients required continuous thyroid replacement therapy during long-term follow-up, and 1.6 to 4% of patients developed recurrence subacute thyroiditis after the initial episode 8, 9.
Subacute thyroiditis affects women almost 4 to 5 times as often as men and typically occurs between 25 to 35 years of age 3. With increasing age, the incidence of subacute thyroiditis decreases 3. The prevalence of subacute thyroiditis appears to be seasonal, as most cases occur in the summer and fall 10.
Thyroid gland
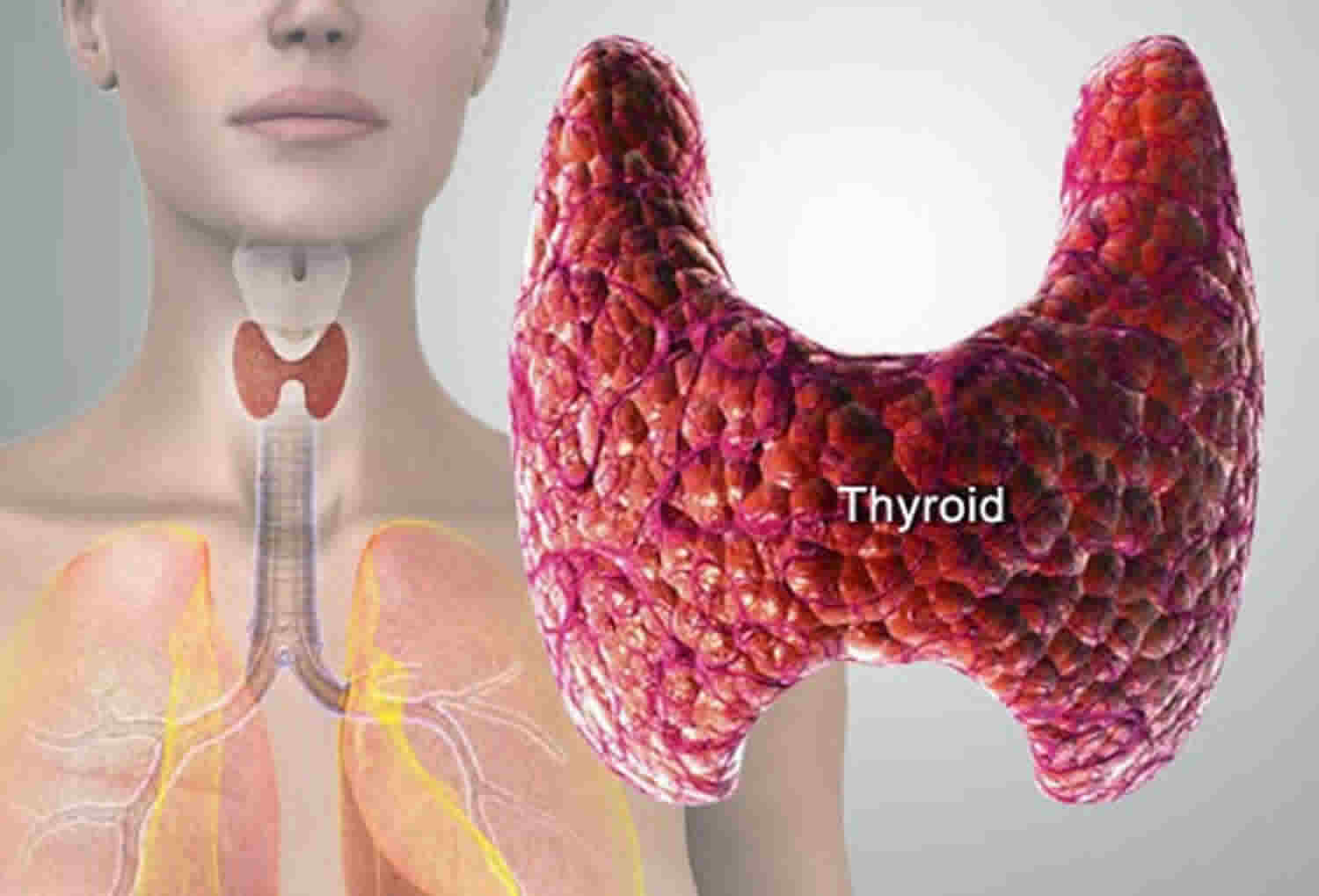
The thyroid gland is the largest adult gland to have a purely endocrine function, weighing about 25-30 g. The thyroid gland is a small butterfly shaped gland with 2 lobes, the right lobe and the left lobe joined by a narrow piece of the thyroid gland called the isthmus, that is located in front of your neck near the base of your throat, beneath the larynx (voice box or Adam’s apple). About 50% of thyroid glands have a small third lobe, called the pyramidal lobe. It extends superiorly from the isthmus. The thyroid gland makes and releases hormones. You can’t usually feel a thyroid gland that is normal.
The thyroid gland has 2 main types of cells:
- Follicular cells use iodine from the blood to make thyroid hormones, which help regulate a person’s metabolism. Having too much thyroid hormone (hyperthyroidism) can cause a fast or irregular heartbeat, trouble sleeping, nervousness, hunger, weight loss, and a feeling of being too warm. Having too little thyroid hormone (hypothyroidism) causes a person to slow down, feel tired, and gain weight. The amount of thyroid hormone released by the thyroid gland is regulated by the pituitary gland at the base of the brain, which makes a substance called thyroid-stimulating hormone (TSH) (see Figure 5).
- C cells also called parafollicular cells at the periphery of the follicles that make calcitonin, a hormone that helps control how your body uses calcium. The parafollicular cells (C cells) respond to rising levels of blood calcium by secreting the hormone calcitonin. Calcitonin antagonizes (blocks) parathyroid hormone (PTH) and stimulates osteoblast activity, thus promoting calcium deposition and bone formation. It is important mainly in children, having relatively little effect in adults. Parathyroid hormone is made by parathyroid glands. These sit behind and are attached to the thyroid gland (see Figure 1).
Other, less common cells in the thyroid gland include immune system cells (lymphocytes) and supportive (stromal) cells.
Thyroid hormone is secreted or inhibited in response to fluctuations in metabolic rate. The brain monitors the body’s metabolic rate and stimulates thyroid hormone secretion through the action of thyrotropin-releasing hormone (TRH) and thyroid stimulating hormone (TSH) as depicted in figure 5.
The primary effect of thyroid hormone (TH) is to increase one’s metabolic rate. As a result, it raises oxygen consumption and has a calorigenic effect—it increases heat production. To ensure an adequate blood and oxygen supply to meet this increased metabolic demand, thyroid hormone also raises the breathing (respiratory) rate, heart rate, and strength of the heartbeat. It stimulates the appetite and accelerates the breakdown of carbohydrates, fats, and protein for fuel. Thyroid hormone also promotes alertness and quicker reflexes; growth hormone secretion; growth of the bones, skin, hair, nails, and teeth; and development of the fetal nervous system.
Figure 1. Thyroid gland location and parathyroid gland
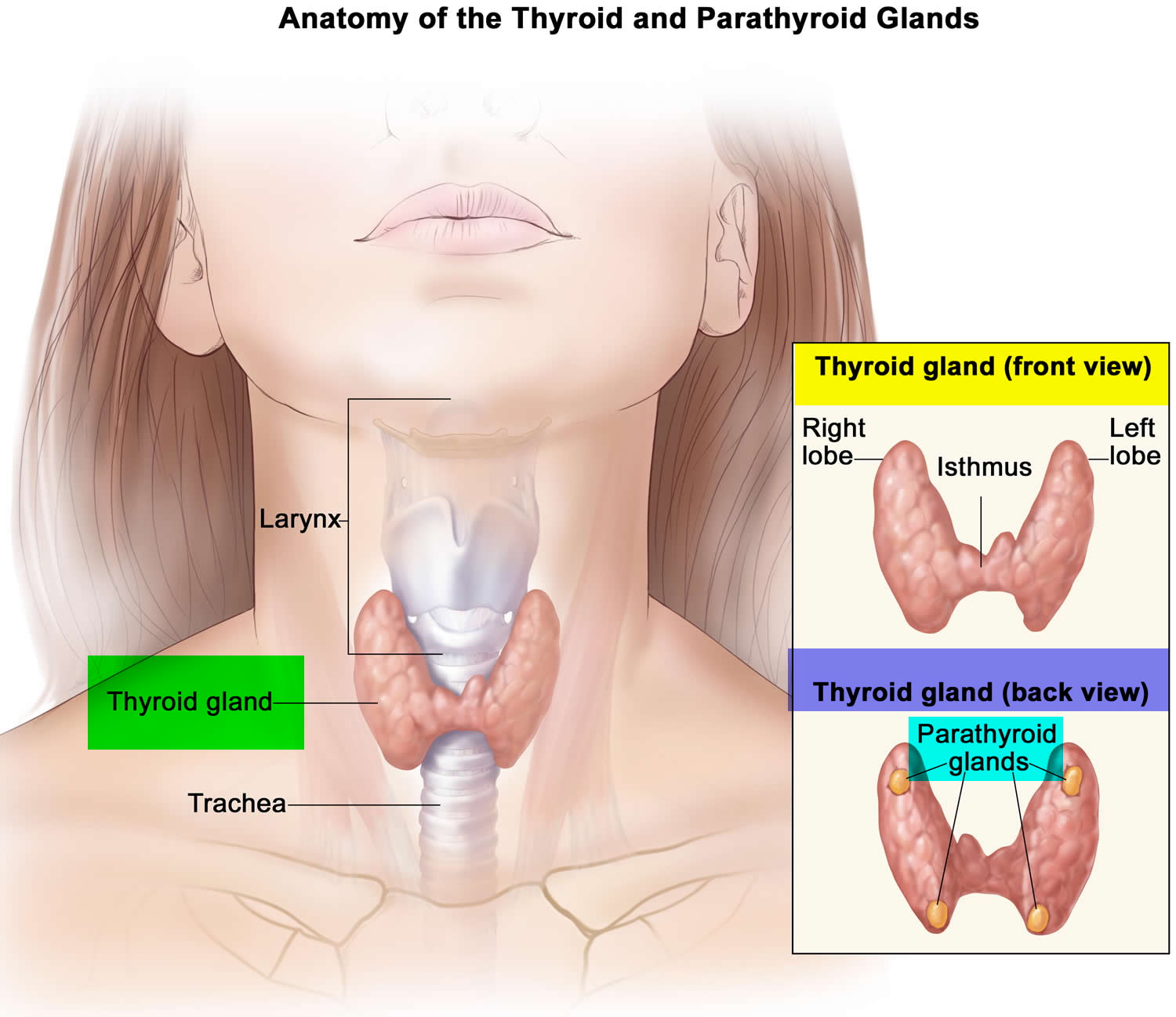
Footnotes: Anatomy of the thyroid and parathyroid glands. The thyroid gland lies at the base of the throat near the trachea. It is shaped like a butterfly, with the right lobe and left lobe connected by a thin piece of tissue called the isthmus. The parathyroid glands are four pea-sized organs found in the neck near the thyroid. The thyroid and parathyroid glands make hormones.
Figure 2. Thyroid gland location
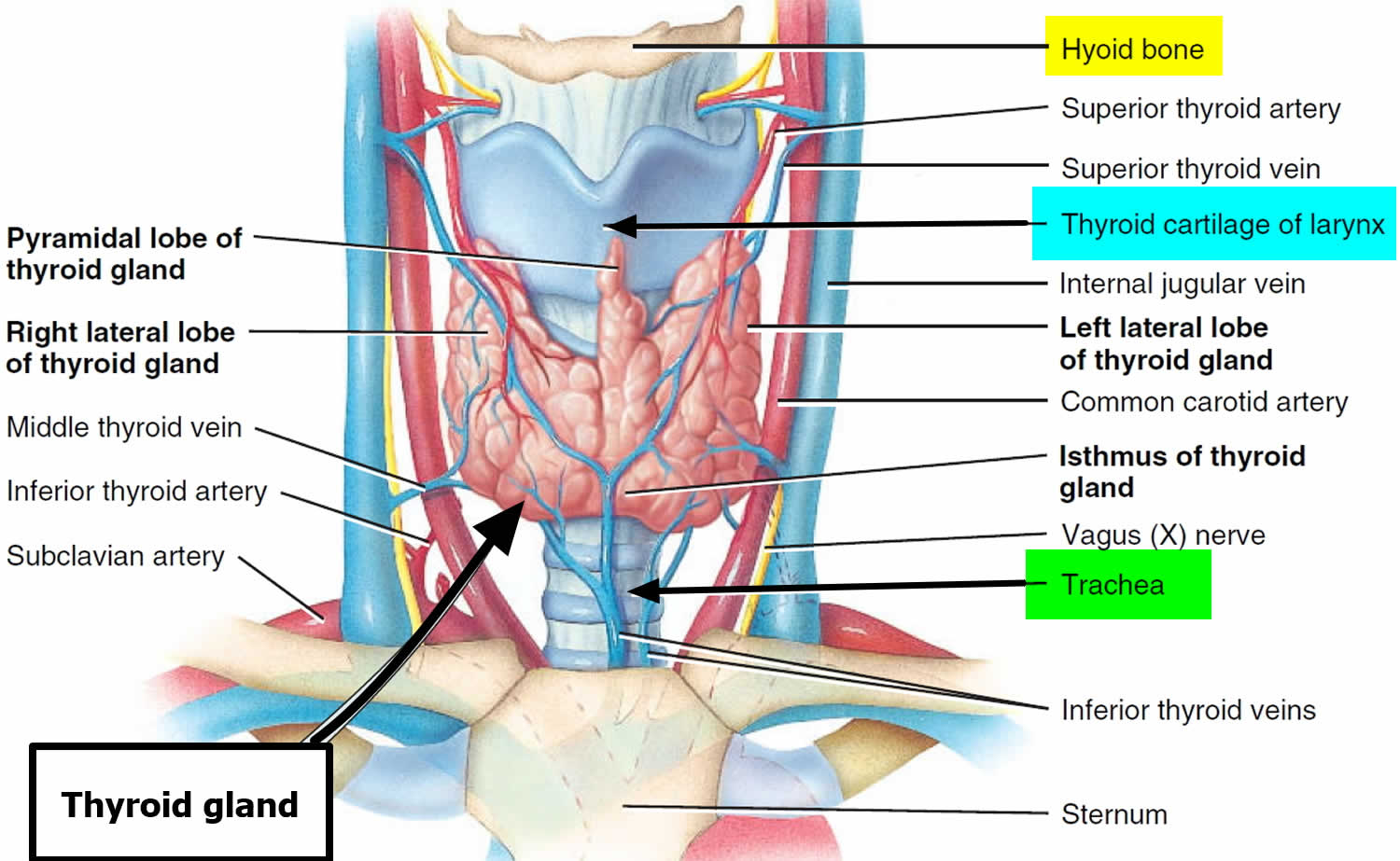
Figure 3. Thyroid gland anatomy
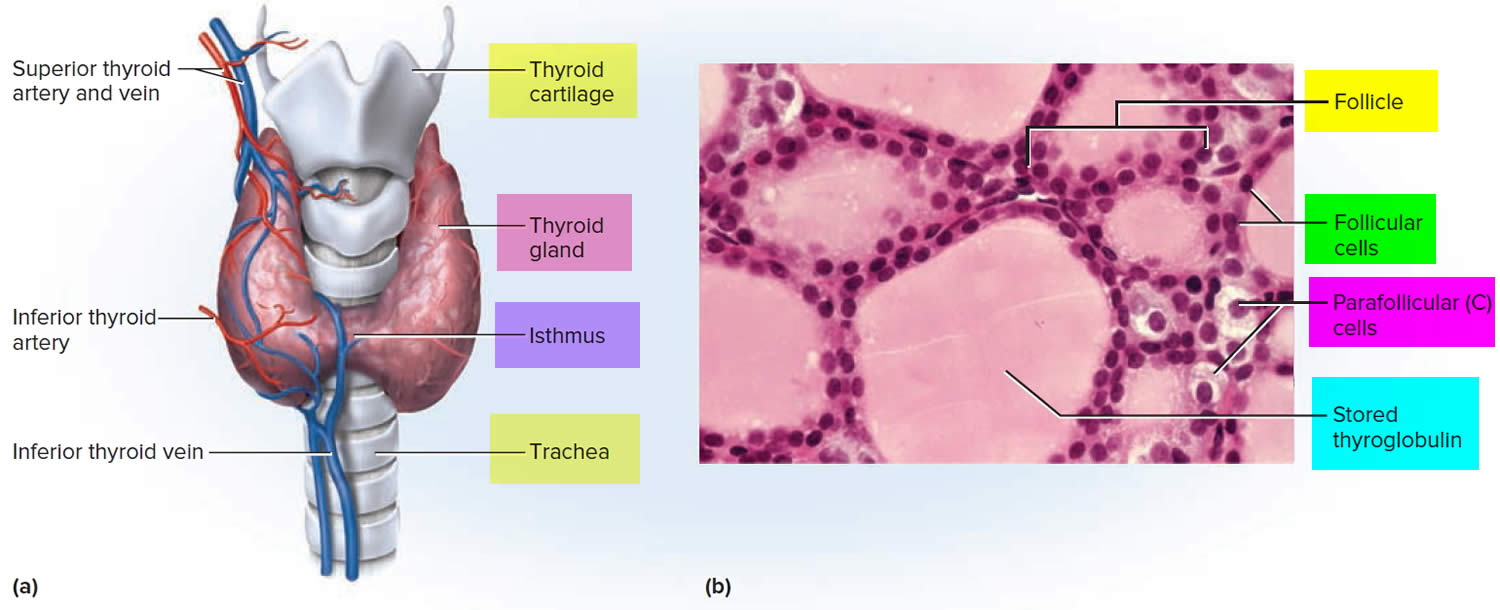
Footnote: (a) Gross anatomy, anterior view. (b) Histology, showing the saccular thyroid follicles (the source of thyroid hormone) and nests of C cells (the source of calcitonin).
What does the thyroid gland do?
Formation, storage, and release of thyroid hormones
The thyroid gland is the only endocrine gland that stores its secretory product in large quantities—normally about a 100-day supply. Synthesis and secretion of triiodothyronine (T3) and thyroxine or tetraiodothyronine (T4) occurs as follows:
- Iodide trapping. Thyroid follicular cells trap iodide ions (I −) by actively transporting them from the blood into the cytosol. As a result, the thyroid gland normally contains most of the iodide in the body.
- Synthesis of thyroglobulin. While the follicular cells are trapping I −, they are also synthesizing thyroglobulin (TGB), a large glycoprotein that is produced in the rough endoplasmic reticulum, modified in the Golgi complex, and packaged into secretory vesicles. The vesicles then undergo exocytosis, which releases thyroglobulin into the lumen of the follicle.
- Oxidation of iodide. Some of the amino acids in thyroglobulin are tyrosines that will become iodinated. However, negatively charged iodide (I −) ions cannot bind to tyrosine until they undergo oxidation (removal of electrons) to iodine: I −→ I. As the iodide ions are being oxidized, they pass through the membrane into the lumen of the follicle.
- Iodination of tyrosine. As iodine atoms (I) form, they react with tyrosines that are part of thyroglobulin molecules. Binding of one iodine atom yields monoiodotyrosine (T1), and a second iodination produces diiodotyrosine (T2). The thyroglobulin with attached iodine atoms, a sticky material that accumulates and is stored in the lumen of the thyroid follicle, is termed colloid.
- Coupling of monoiodotyrosine (T1) and diiodotyrosine (T2). During the last step in the synthesis of thyroid hormone, two diiodotyrosine (T2) molecules join to form thyroxine (T4) or one T1 and one T2 join to form triiodothyronine (T3).
- Pinocytosis and digestion of colloid. Droplets of colloid reenter follicular cells by pinocytosis and merge with lysosomes. Digestive enzymes in the lysosomes break down thyroglobulin, cleaving off molecules of triiodothyronine (T3) and thyroxine (T4).
- Secretion of thyroid hormones. Because T3 and T4 are lipid soluble, they diffuse through the plasma membrane into interstitial fluid and then into the blood. T4 normally is secreted in greater quantity than T3, but T3 is several times more potent. Moreover, after T4 enters a body cell, most of it is converted to T3 by removal of one iodine.
- Transport thyroid hormones in the blood. More than 99% of both the T3 and the T4 combine with transport proteins in the blood, mainly thyroxine binding globulin (TBG).
Figure 4. Thyroid hormones
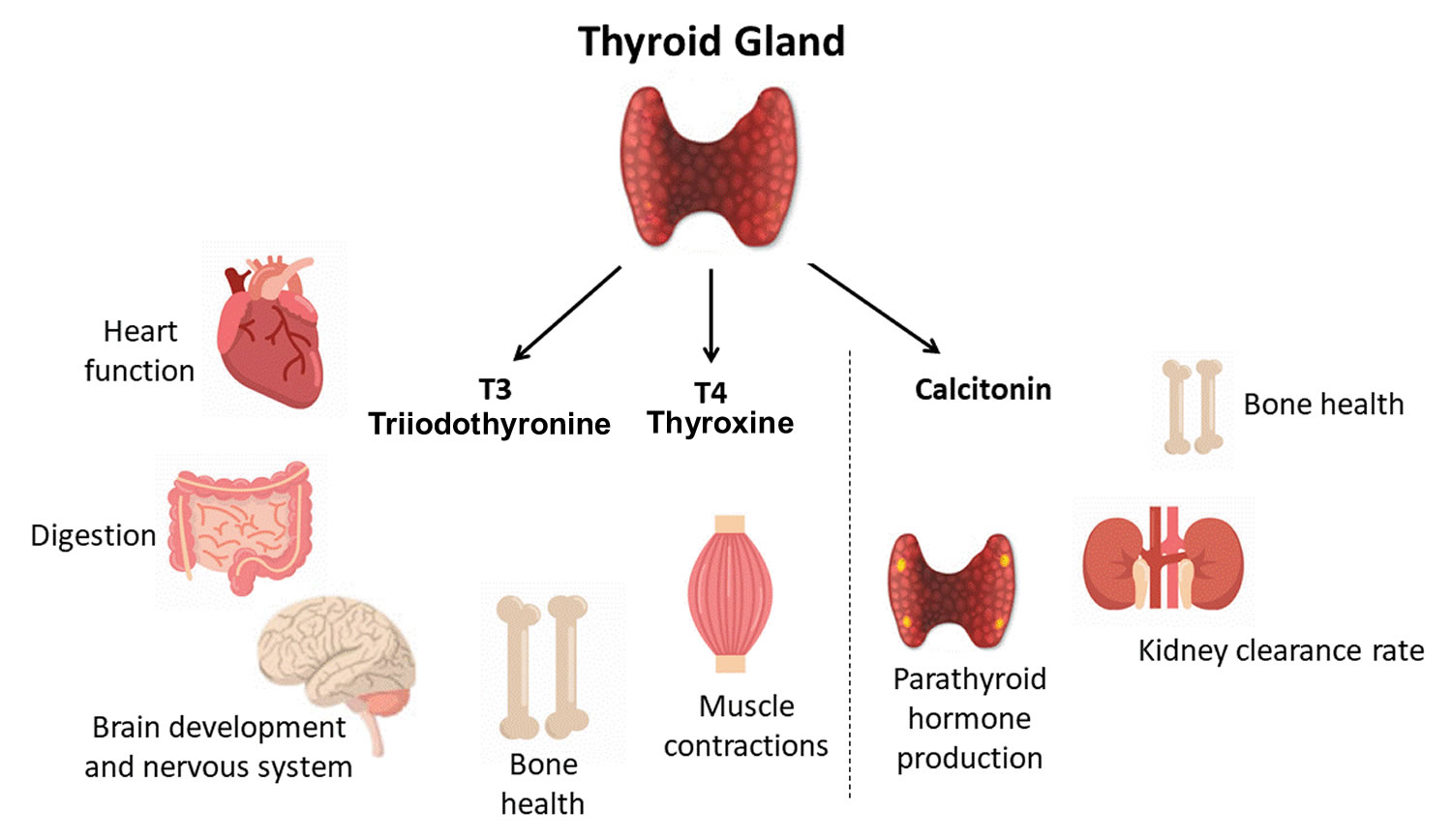
Actions of thyroid hormones
Because most body cells have receptors for thyroid hormones, triiodothyronine (T3) and thyroxine (T4) affect tissues throughout the body. Thyroid hormones act on their target cells mainly by inducing gene transcription and protein synthesis. The newly formed proteins in turn carry out the cellular response.
Functions of thyroid hormones include the following:
- Increase basal metabolic rate. Thyroid hormones raise the basal metabolic rate (BMR), the rate of energy expenditure under standard or basal conditions (awake, at rest, and fasting). When basal metabolic rate increases, cellular metabolism of carbohydrates, lipids, and proteins increases. Thyroid hormones increase BMR in several ways: (1) They stimulate synthesis of additional Na+/K+ ATPases, which use large amounts of ATP to continually eject sodium ions (Na+) from cytosol into extracellular fluid and potassium ions (K+) from extracellular fluid into cytosol; (2) they increase the concentrations of enzymes involved in cellular respiration, which increases the breakdown of organic fuels and ATP production; and (3) they increase the number and activity of mitochondria in cells, which also increases ATP production. As cells produce and use more ATP, basal metabolic rate increases, more heat is given off and body temperature rises, a phenomenon called the calorigenic effect. In this way, thyroid hormones play an important role in the maintenance of normal body temperature. Normal mammals can survive in freezing temperatures, but those whose thyroid glands have been removed cannot.
- Enhance actions of catechlolamines. Thyroid hormones have permissive effects on the catecholamines (epinephrine and norepinephrine) because they up-regulate β-adrenergic receptors. Catecholamines bind to β-adrenergic receptors, promoting sympathetic responses. Therefore, symptoms of excess levels of thyroid hormone include increased heart rate, more forceful heartbeats, and increased blood pressure.
- Regulate development and growth of nervous tissue and bones. Thyroid hormones are necessary for the development of the nervous system: They promote synapse formation, myelin production, and growth of dendrites. Thyroid hormones are also required for growth of the skeletal system: They promote formation of ossification centers in developing bones, synthesis of many bone proteins, and secretion of growth hormone (GH) and insulin-like growth factors (IGFs). Deficiency of thyroid hormones during fetal development, infancy, or childhood causes severe mental retardation and stunted bone growth.
Control of thyroid hormone secretion
Thyrotropin-releasing hormone (TRH) from the hypothalamus and thyroid-stimulating hormone (TSH) from the anterior pituitary stimulate secretion of thyroid hormones, as shown in Figure 5:
- Low blood levels of T3 and T4 or low metabolic rate stimulate the hypothalamus to secrete thyrotropin-releasing hormone (TRH).
- Thyrotropin-releasing hormone (TRH) enters the hypothalamic–hypophyseal portal system and flows to the anterior pituitary, where it stimulates thyrotrophs to secrete thyroid stimulating hormone (TSH).
- Thyroid stimulating hormone (TSH) stimulates virtually all aspects of thyroid follicular cell activity, including iodide trapping, hormone synthesis and secretion, and growth of the follicular cells.
- The thyroid follicular cells release T3 and T4 into the blood until the metabolic rate returns to normal.
- An elevated level of T3 inhibits release of TRH and TSH (negative feedback inhibition).
Conditions that increase ATP demand—a cold environment, hypoglycemia, high altitude, and pregnancy—increase the secretion of the thyroid hormones.
Figure 5. Control of thyroid hormone secretion
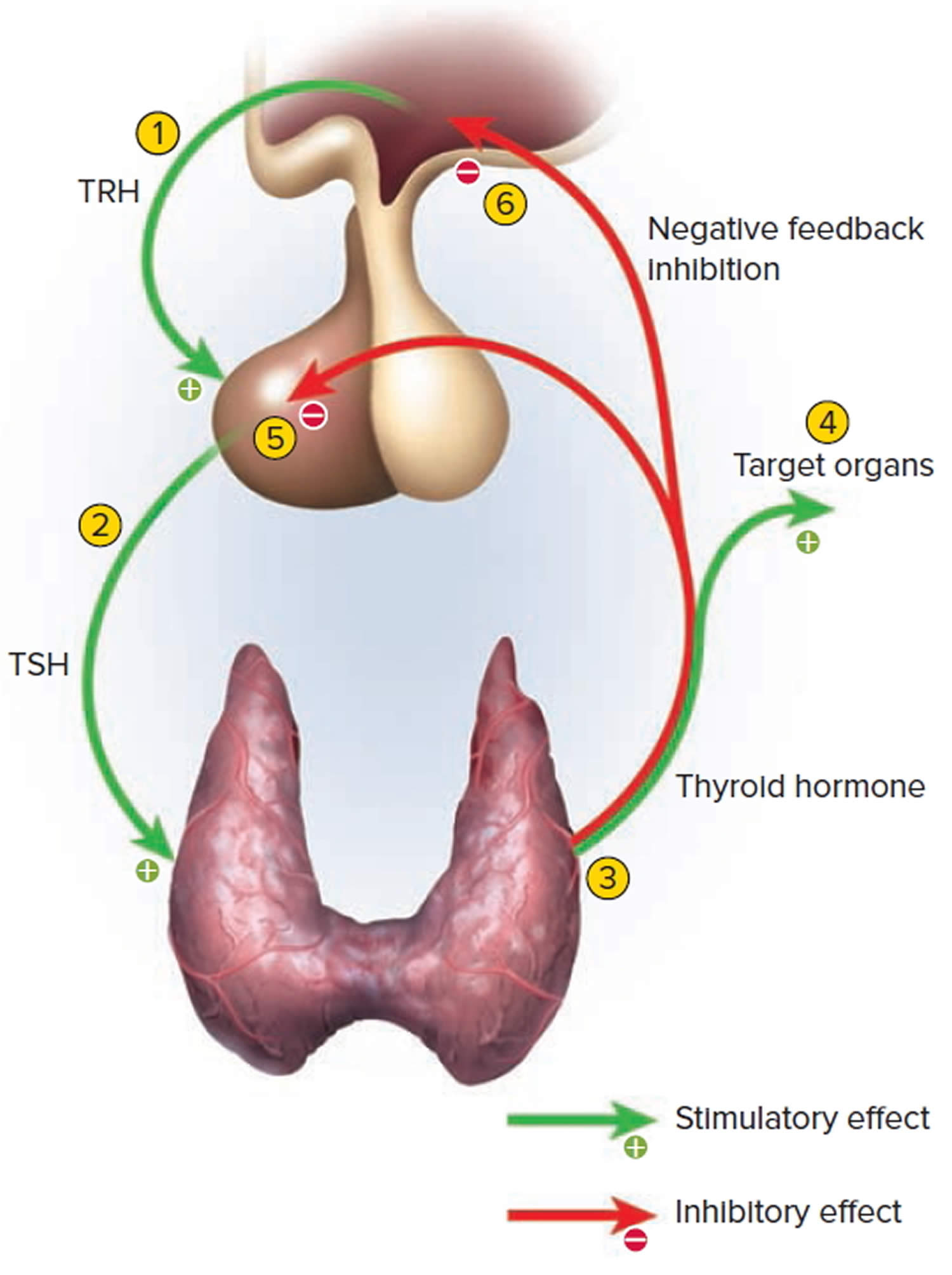
Footnote: Negative Feedback Inhibition of the Anterior Pituitary Gland by the Thyroid Gland
Control of calcium balance
The hormone produced by the parafollicular cells of the thyroid gland is calcitonin. Calcitonin can decrease the level of calcium in the blood by inhibiting the action of osteoclasts, the cells that break down bone extracellular matrix. The secretion of calcitonin is controlled by a negative feedback system (see Figure 7).
Calcitonin is produced by C cells (clear cells) of the thyroid gland. It is secreted when the blood calcium concentration rises too high, and it lowers the concentration by two principal mechanisms:
- Osteoclast inhibition. Within 15 minutes after it is secreted, calcitonin reduces osteoclast activity by as much as 70%, so osteoclasts liberate less calcium from the skeleton.
- Osteoblast stimulation. Within an hour, calcitonin increases the number and activity of osteoblasts, which deposit calcium into the skeleton.
Calcitonin plays an important role in children but has only a weak effect in most adults. The osteoclasts of children are highly active in skeletal remodeling and release 5 g or more of calcium into the blood each day. By inhibiting this activity, calcitonin can significantly lower the blood calcium level in children. In adults, however, the osteoclasts release only about 0.8 g of calcium per day. Calcitonin cannot change adult blood calcium very much by suppressing this lesser contribution. Calcitonin deficiency is not known to cause any adult disease. Calcitonin may, however, inhibit bone loss in pregnant and lactating women. Miacalcin, a calcitonin extract derived from salmon that is 10 times more potent than human calcitonin, is prescribed to treat osteoporosis.
Figure 6. Hormonal control of calcium balance
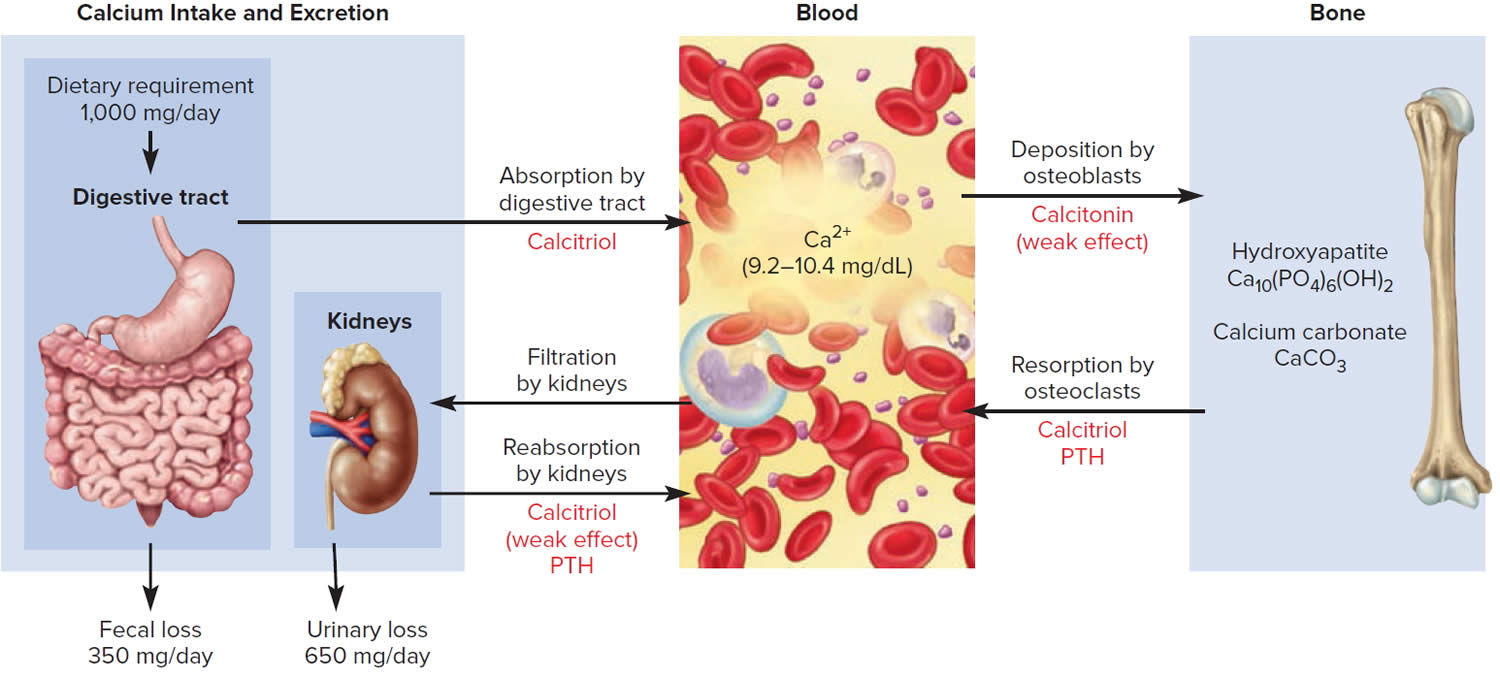
Footnote: The central panel represents the blood reservoir of calcium and shows its normal (safe) range. Calcitriol and Parathyroid Hormone (PTH) regulate calcium exchanges between the blood and the small intestine and kidneys (left). Calcitonin, calcitriol, and Parathyroid Hormone (PTH) regulate calcium exchanges between blood and bone (right).
Subacute granulomatous thyroiditis (de Quervain’s thyroiditis)
Subacute granulomatous thyroiditis also called giant cell thyroiditis, de Quervain’s thyroiditis or painful subacute thyroiditis is the most common cause of thyroid pain 11, 7, 3. de Quervain’s thyroiditis affects four times more women than men, and most often occurs at 40 to 50 years of age 7. Subacute granulomatous thyroiditis usually follows upper respiratory tract infections or sore throats suggesting it is caused by a viral infection 12, 13, 14. The summer peak incidence of de Quervain’s thyroiditis or subacute granulomatous thyroiditis coincides with the peak incidences of coxsackievirus groups A and B and echovirus infections 15, 3. Subacute granulomatous thyroiditis is also associated with mumps, measles, influenza, Covid-19, and other viruses 16, 15, 17.
Signs and symptoms of subacute granulomatous thyroiditis (de Quervain’s thyroiditis) include a prodrome of muscle aches and pain, pain or irritation in the throat, low-grade fever, and fatigue, followed by a tender, diffuse goiter and neck pain that often radiates up to the ear 10. As the disease progresses there may be a “march” of tenderness across the thyroid gland, with new parts of the thyroid becoming painful and tender as previously involved portions become less so 10.
The natural course of subacute granulomatous thyroiditis (de Quervain’s thyroiditis) can be divided into 4 phases that generally unfold over four to six months in which patients have an initial phase of hyperthyroidism (overactive thyroid) accompanied by elevated free thyroxine (free T4) and suppressed thyroid-stimulating hormone (TSH) levels, followed by a phase of hypothyroidism (underactive thyroid) with low free T4 and high TSH levels, which may last weeks or up to six months 10.
- Acute phase – Lasts three to six weeks or longer and presents primarily with pain; symptoms of hyperthyroidism also may be present
- Transient asymptomatic and normal thyroid phase (asymptomatic euthyroidism) – Lasts 1-3 weeks
- Hypothyroid phase – Lasts from weeks to months; it may become permanent in up to 5-15% of patients 18
- Recovery phase (the final phase) – Characterized by normalization of thyroid structure and function
Patients usually return to normal thyroid within six to 12 months. However, in 10 to 15 percent of patients, hypothyroidism (underactive thyroid) persists, requiring long-term levothyroxine therapy 7, 19. During transition from hyperthyroidism (overactive thyroid) to hypothyroidism (underactive thyroid), low TSH and free T4 levels may be found, which may be mistaken for central hypothyroidism (underactive thyroid caused by problem with the pituitary gland or hypothalamus in the brain).
Hyperthyroidism is seen in one half of affected individuals; it occurs when activated cytotoxic T lymphocytes damage the thyroid follicular cells, resulting in the unregulated release of large amounts of thyroxine (T4) and triiodothyronine (T3) into the circulation 10. This process usually is transient, lasting three to six weeks and ceasing when the thyroid stores are exhausted 10.
Other findings of subacute granulomatous thyroiditis or de Quervain’s thyroiditis are an elevated erythrocyte sedimentation rate (ESR) often greater than 50 mm per hour, elevated C-reactive protein (CRP) level, mild anemia, and slight leukocytosis 10. Levels of antithyroid peroxidase (anti-TPO) and antithyroglobulin antibodies (anti-thyroglobulin) generally are normal 10.
Hyperthyroidism from subacute thyroiditis must be differentiated from that found with Graves’ disease. Bulging eyes (exophthalmos) and pretibial myxedema (a skin condition that causes plaques of thick, scaly skin and swelling of your lower legs) are characteristics of Graves’ disease but are not found with subacute thyroiditis. The thyroid in patients with Graves’ disease may have a thrill or bruit from the hypervascularity; this does not occur in persons with subacute thyroiditis. These differences in vascularity also may be shown by Doppler ultrasonography. In patients with subacute thyroiditis, the radioactive iodine uptake (RAIU) at 24 hours is low (i.e., less than 5 percent), whereas in those with Graves’ disease it is elevated 10.
Subacute granulomatous thyroiditis or de Quervain’s thyroiditis affects women almost 3 to 5 times as often as men and typically occurs between 30 to 50 years of age 20. Subacute thyroiditis tends to be geographical and seasonal, occurring most often in the summer and fall 4, 20.
Treatment for subacute granulomatous thyroiditis (de Quervain’s thyroiditis) consists of relieving the thyroid pain and tenderness with nonsteroidal anti-inflammatory drugs (NSAIDs). The median time from start of therapy to complete alleviation of pain is five weeks 7. If no improvement occurs within one week, prednisone may be given in a dosage of 40 to 60 mg daily tapered to complete discontinuation over four to six weeks 10. Although steroids provide complete thyroid pain relief at a median of 48 hours, they do not prevent early- or late-onset thyroid dysfunction 7. Symptoms of hyperthyroidism are treated with beta blockers such as propranolol (Inderal) or atenolol (Tenormin) until the free T4 concentration returns to normal. Painful subacute thyroiditis recurs in about 2 percent of individuals 7.
Subacute thyroiditis usually resolves, and patients return to a normal thyroid state in 3 or 4 months 3. Rarely do patients have hypothyroidism which can be transient or permanent. Patients with hypothyroidism with TSH greater than 10 microU/L or having symptoms of hypothyroidism need levothyroxine treatment for 1 to 2 months 3. Levothyroxine should be discontinued, and thyroid function tests should be done in 1 month to ensure hypothyroidism is transient. Some patients may need treatment with levothyroxine for a long time.
After subacute thyroiditis is diagnosed, serial thyroid function tests should be done every 2 to 8 weeks to confirm the improvement of hyperthyroidism and follow the natural course of disease till they are normalized 3.
Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) causes
Subacute granulomatous thyroiditis or de Quervain’s thyroiditis is most likely caused by a viral infection and is generally preceded by an upper respiratory tract infection (URTI) 4, 3, 21, 7. Numerous etiologic agents have been implicated, including mumps virus, echovirus, coxsackievirus, Epstein-Barr virus, influenza, Covid-19 and adenovirus 22, 4, 16, 15, 23.
Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) pathophysiology
Destruction of follicular epithelium and loss of follicular integrity are the primary events in the pathophysiology of subacute granulomatous thyroiditis 24. Thyroglobulin (Tg), thyroid hormones, and other iodinated compounds are released into the blood, often in quantities sufficient to elevate the serum thyroxine (T4) and triiodothyronine (T3) concentrations and suppress thyroid-stimulating hormone (TSH) secretion 24. This state lasts until the stores of thyroglobulin are exhausted or until healing occurs. Thyroidal iodine uptake and new hormone synthesis temporarily ceases because of the low level of TSH 24.
As inflammation subsides, the thyroid follicles regenerate and thyroid hormone synthesis and secretion resume 24. In some patients, several months are required for thyroid hormone synthesis to return to a normal rate; during that period, clinical hypothyroidism may be evident 24.
Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) symptoms
Subacute granulomatous thyroiditis or de Quervain’s thyroiditis presents clinically with acute onset of pain in the thyroid region 10. The pain may be worsened by turning your head or swallowing, and may radiate to your jaw, ear or chest 22, 18, 20. Symptoms of hypermetabolism may be present. The thyroid is firm, nodular and exquisitely tender to touch.
Local symptoms of subacute granulomatous thyroiditis or de Quervain’s thyroiditis include the following 2:
- Difficulty swallowing (dysphagia)
- Hoarseness (uncommon)
- Pain over the thyroid area that is gradual or of sudden onset
Constitutional symptoms (often absent) of subacute granulomatous thyroiditis can include the following 2:
- Fever
- Malaise
- Anorexia
- Fatigue
- Muscle aches
Signs and symptoms of hyperthyroidism occurring in the acute phase of subacute granulomatous thyroiditis include the following 2:
- Fast heart rate (tachycardia)
- Tremors
- Heat intolerance
- Sweating
- Nervousness
- Warm skin
- Frequent bowel movements
Signs and symptoms of hypothyroidism occurring during the second phase of subacute granulomatous thyroiditis include the following 2:
- Fatigue
- Dry skin
- Lethargy
- Eyelid swelling
- Cold intolerance
- Constipation
Atypical presentations of subacute granulomatous thyroiditis—that is, extremely rare symptoms that have been documented as case reports—can include the following:
- Thyroid storm 25
- Fever of unknown origin
- Painless subacute granulomatous thyroiditis
- Occult de Quervain disease mimicking giant cell arteritis
- Prominent prostration and confusion lasting several weeks
- Solitary painless nodule
Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) complications
Acute complications
When acute complications do occur, they can include the following 26:
- Severe hyperthyroidism – May be observed during the inflammatory phase
- Severe anterior neck pain over the thyroid – Usual treatment is nonsteroidal therapy, but emerging studies suggest that prednisolone 15 mg/day with a taper of 5 mg every 2 weeks is safe and effective to quickly reduce pain; in a study of prednisolone use by Kubota et al 27, most patients had resolution of symptoms by 6-8 weeks, although the longest period of therapy was 40 weeks
- Multiple system organ failure – May complicate the course of the disease in exceptionally rare cases
- Pancreatitis or splenomegaly – Associated with de Quervain thyroiditis in case reports only
- Vocal cord paralysis – Occurs occasionally in cases with severe thyroid gland inflammation
- Cerebral venous thrombosis – has been reported in some cases; in one case, the patient was a heterozygous carrier for the G20210A mutation of the prothrombin gene, which predisposed her to this complication
Long-term complications
Permanent hypothyroidism is the most frequent long-term complication of de Quervain thyroiditis 26. It is observed in less than 5-10% of the patients and requires thyroid replacement therapy 26.
Disease recurrence has been documented in occasional cases (up to 20% of cases in some series). Recurrence is more frequent in the first year but has been reported even 30 years after the initial diagnosis. The risk of recurrence cannot be correlated with initial thyroid function, inflammatory syndrome, or ultrasonographic aspect (ie, thyroid volume, echogenicity).
Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) diagnosis
Your doctor will perform a physical exam, including assessing your thyroid, and ask you questions about your symptoms and medical history. If your doctor suspect you may have subacute thyroiditis, he/she will likely order any combination of the following tests to help diagnose it:
- Thyroid function tests: These are blood tests that measure the levels of thyroid-related hormones and thyroid hormones in your body, including:
- Thyroid-stimulating hormone (TSH)
- T3 (triiodothyronine)
- T4 (thyroxine)
- Thyroid stimulating hormone (TSH) comes from your pituitary gland and stimulates your thyroid gland to produce the hormones T4 (thyroxine) and T3 (triiodothyronine), which together are called thyroid hormones.
- Thyroglobulin (Tg). Thyroglobulin (Tg) is a protein made by the thyroid gland. Thyroglobulin (Tg) plays a key role in helping the body create, store and release thyroid hormones. Thyroglobulin (Tg) may be present in the blood when the thyroid has been damaged. Some doctors may check thyroglobulin (Tg) levels when diagnosing hyperthyroidism and hypothyroidism, thyroid disorders that are not thyroid cancer. If you recently had surgery for thyroid cancer, your doctor may measure thyroglobulin (Tg) levels to determine whether your treatment successfully removed all of your thyroid cells, including noncancerous and cancerous cells. This postoperative evaluation of thyroglobulin (Tg) levels is usually ordered four to six weeks following surgery. The presence of detectable thyroglobulin (Tg), particularly a rising thyroglobulin level, may give an early warning of a recurrence of thyroid cancer.
- Thyroid ultrasound: Providers often use ultrasound to evaluate the anatomy of your thyroid gland. It can show a nodule (a growth) in your thyroid gland, a change in blood flow to your thyroid and the density of the gland.
- Thyroid antibody tests: These are blood tests that measure thyroid antibodies that include antithyroid (microsomal) antibodies (TPO) or thyroid receptor stimulating antibodies (TRAb). These antibodies could signal that you have a type of thyroiditis caused by autoimmune disease.
- Erythrocyte sedimentation rate (ESR or sed rate): This is a blood test that helps detect inflammation in your body. The ESR is high in subacute thyroiditis.
- C-reactive protein (CRP): C-reactive protein (CRP) test that measures the level of c-reactive protein (CRP) in your blood. CRP increases when there’s inflammation in your body, and it’s usually significantly elevated in acute infectious thyroiditis.
- Radioactive iodine uptake (RAIU) test: Radioactive iodine uptake (RAIU) test measures the amount of radioactive iodine (taken by mouth) that your thyroid gland absorbs. The amount is always low in the thyrotoxic phase of thyroiditis.
The erythrocyte sedimentation rate (ESR) usually is markedly elevated 4. A normal ESR essentially rules out the diagnosis of subacute granulomatous thyroiditis 4. The leukocyte count is normal or slightly elevated 4. Thyrotoxicosis is present in 50 percent of patients in the acute phase, and the serum T4 concentration is disproportionately elevated relative to the T3 level 4, 20. Serum TSH concentrations are low to undetectable 4. Thyroglobulin is elevated. A normal thyroglobulin level essentially rules out the diagnosis of subacute granulomatous thyroiditis 20. The radioactive iodine uptake (RAIU) is notably low, often less than 2 percent at 24 hours 4. In summary, the physical examination, an elevated ESR, an elevated thyroglobulin level and a depressed RAIU confirm the diagnosis 10.
Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) treatment
Subacute granulomatous thyroiditis or de Quervain’s thyroiditis treatment consists of relieving the thyroid pain and tenderness with nonsteroidal anti-inflammatory drugs (NSAIDs). Patients with mild to moderate pain are generally treated with rest and aspirin usually taken every 4 to 6 hours as needed to treat thyroid pain, naproxen 500 to 1000 mg twice a day, or ibuprofen 400 to 800 mg orally every 8 hours. The median time from start of therapy to complete alleviation of pain is five weeks 7. If no improvement occurs within 1 week, oral corticosteroids (Prednisone) may be given in a dosage of 20 to 60 mg daily tapered to complete discontinuation over two to six weeks 22. Usually, symptoms improve in 2 to 3 days with NSAIDS; prednisone should be initiated if no improvement is noted. Steroids should provide pain relief in 1 to 2 days. The typical steroid course can be two months, occasionally longer. The persistence of pain beyond two days should need a further workup for other causes of thyroid pain 3. Once thyroid pain is improved, an attempt should be made to use the lowest prednisone dose, and dosing can be titrated by decreasing 5 to 10 mg every week 3. Recurrent pain should require up-titration of prednisone dose. Unfortunately, prednisone has no role in preventing thyroid dysfunction 28. Up to 20 percent of patients experience the recurrence of thyroid pain on discontinuation of prednisone 4, 20. Radioactive iodine uptake (RAIU) can assist clinicians in determining patients at high risk for relapse. Low radioactive iodine uptake (RAIU) uptake implies ongoing inflammation, and steroid therapy should be continued 22.
Mild and transient symptoms of hyperthyroidism do not require any treatment 3. Heart palpitations, anxiety, and tremors need to be treated with beta blockers such as propranolol or atenolol with close follow-up 3. Therapy with antithyroid drugs should not be used to treat hyperthyroidism of subacute thyroiditis, because the disorder is caused by the release of preformed thyroid hormone from destroyed follicles instead of the synthesis of new T3 and T4 29, 4, 20.
Subacute granulomatous thyroiditis (de Quervain’s thyroiditis) prognosis
De Quervain thyroiditis or subacute granulomatous thyroiditis is generally self-limited, with patients returning to a normal thyroid state in 3 or 4 months 3. Most of the time, de Quervain thyroiditis or subacute granulomatous thyroiditis resolves completely, and rarely it can cause permanent hypothyroidism 3. Some patients may have severe symptoms from hypothyroidism, but it is usually transient. Hypothyroidism may become permanent in 5% of cases 29. Recurrence is uncommon but can occur in up to 2% of patients 3. Rarely de Quervain thyroiditis or subacute granulomatous thyroiditis has been known to cause thyroid storm (thyrotoxic crisis or an acute, life-threatening complication of hyperthyroidism that presents with multi-system involvement), ventricular tachycardia, and fever of unknown origin 30, 31.
Subacute lymphocytic thyroiditis
Subacute lymphocytic thyroiditis also known as silent sporadic thyroiditis or painless sporadic thyroiditis is clinically and pathologically similar to postpartum thyroiditis but occurs in the absence of pregnancy 10, 4. Subacute lymphocytic thyroiditis appears to be autoimmune in origin; the thyroid contains a lymphocytic infiltrate partially resembling Hashimoto’s disease but without the fibrosis, Askanazy cells, and extensive lymphoid follicle formation 32, 33. Four times more women are affected than men, and the risk is increased in persons who live in areas of iodine deficiency 34, 19.
About one half of patients with subacute lymphocytic thyroiditis present with a small goiter 33. Between 5 and 20 percent of patients exhibit hyperthyroidism from release of pre-formed T4 and T3, which may be followed by hypothyroidism and then a return to normal in the majority of patients 10. The hyperthyroid stage averages three to four months, and total duration of illness is less than one year 10. About one half of patients have antithyroid peroxidase antibodies (anti-TPO).
Subacute lymphocytic thyroiditis is distinguished from subacute granulomatous thyroiditis (de Quervain’s thyroiditis) by the absence of thyroid pain and tenderness 10. Subacute lymphocytic thyroiditis is differentiated from Graves’ disease by the lack of a thyroid thrill or bruit, ophthalmopathy, pretibial myxedema, and thyroid-stimulating immunoglobulins, and by a low or absent rather than elevated radioactive iodine uptake (RAIU). Treatment is similar to that of postpartum thyroiditis, that depends on the phase of thyroiditis and degree of symptoms that a patient has. Patients presenting with thyrotoxicosis may be treated with beta blockers to decrease symptoms such as palpitations and tremors. As symptoms improve, the medication can be reduced and stopped since the thyrotoxic phase is transient. Antithyroid medications are not used for the thyrotoxic phase since the thyroid is not overactive.
Occasionally, subacute lymphocytic thyroiditis patients have recurrent episodes of painless thyrotoxicosis 35. No treatment exists to prevent the recurrences except subtotal thyroidectomy. However, subacute lymphocytic thyroiditis generally resolves completely in more than 90-95% of patients. Patients with goiters or permanent thyroid dysfunction should be monitored with a thyroid examination and thyroid function tests every 6 months.
Subacute postpartum thyroiditis
Subacute postpartum thyroiditis is also known as postpartum thyroiditis, autoimmune lymphocytic thyroiditis or inflammation of your thyroid gland that occurs in women within 12 months after the delivery of a baby (postpartum) without a history of thyroid disease prior to pregnancy 36, 37, 5, 38. Thyroiditis or inflammation of your thyroid gland can cause both thyrotoxicosis also known as overactive thyroid (high thyroid hormone levels in the blood) and hypothyroidism also known as underactive thyroid (low thyroid hormone levels in the blood). In postpartum thyroiditis, thyrotoxicosis (overactive thyroid or hyperthyroidism) occurs first followed by hypothyroidism (underactive thyroid). Your thyroid gland is an important organ of the endocrine system and is a butterfly-shaped gland with a right lobe and a left lobe located at the base of your neck just below the larynx (voice box). The thyroid gland usually cannot be felt through the skin. The thyroid produces thyroid hormone and calcitonin (control the amount of calcium in your blood) that help regulate many functions in your body including growth, heart rate, body temperature, and metabolism (the way every cell in the body uses energy).
The exact cause of postpartum thyroiditis is not known but it is believed to be an autoimmune disease (a disease in which your body’s immune system mistakenly attacks healthy cells in your thyroid) very similar to Hashimoto’s thyroiditis 37. As in Hashimoto’s thyroiditis, postpartum thyroiditis is associated with the presence of anti-thyroid antibodies (anti-thyroid peroxidase [TPOAb], anti-thyroglobulin [TgAb]). Women with positive antithyroid antibodies are at a much higher risk of developing postpartum thyroiditis than women who do not have have positive antibodies.
In the United Status, postpartum thyroiditis occurs in approximately 5% to 10% of women in the year after a birth, abortion or miscarriage. The incidence can be greater in certain high-risk populations. Women with type 1 diabetes or a history of thyroid problem are most likely to develop postpartum thyroiditis.
Postpartum thyroiditis occurs in any woman with 39:
- Autoimmune disorders (such as Type 1, or juvenile onset, Diabetes Mellitus)
- Positive anti-thyroid antibodies (risk correlates with antibody levels, the higher the antibody the higher the risk)
- History of previous thyroid dysfunction
- History of previous postpartum thyroiditis (20% of women will have recurrence of thyroiditis with additional pregnancies)
- Family history of thyroid dysfunction
- Chronic viral hepatitis
Postpartum thyroiditis usually unfolds in phases:
- Phase 1: The inflammation causes your thyroid to produce and release too many hormones (hyperthyroidism). This phase usually happens between 1 to 6 months after a pregnancy. It may last from one week up to three months.
- Phase 2: Your thyroid doesn’t produce or release enough hormones (hypothyroidism). This phase usually takes place 4 to 8 months after pregnancy. It can last as long as a year.
- Phase 3: Your thyroid usually returns to producing normal hormone levels.
Not everyone experiences all the phases in order, though. Some people skip over the hypothyroid phase. They have hyperthyroidism, and then their thyroid function returns to normal.
The classic description of postpartum thyroiditis includes thyrotoxicosis also known as overactive thyroid (high thyroid hormone levels in the blood) followed by hypothyroidism also known as underactive thyroid (low thyroid hormone levels in the blood). Not all women appear to go through both phases; approximately 1/3 of patients will manifest both, while 1/3 of patients will have only a overactive thyroid (thyrotoxic) or only a hypothyroid (underactive thyroid) phase.
The thyrotoxic (overactive thyroid) phase occurs 1 to 4 months after delivery of a child and lasts for 1 to 3 months. The thyrotoxic (overactive thyroid) phase is associated with symptoms including anxiety, insomnia, palpitations (fast heart rate), fatigue, weight loss, and irritability. Since these symptoms may often be attributed to changes after delivery and the stress of having a new baby, the thyrotoxic (overactive thyroid) phase of post-partum thyroiditis is often overlooked.
It is much more common for women to present during the hypothyroid (underactive thyroid) phase. This typically occurs 4 to 8 months after delivery of a baby and may last up to 9 to 12 months. Typical hypothyroid (underactive thyroid) symptoms include fatigue, weight gain, constipation, dry skin, depression and poor exercise tolerance. Most women will regain normal thyroid function within 12 to 18 months after the onset of symptoms. However, approximately 20% of those that go into a hypothyroid phase will remain hypothyroid. Women who remain hypothyroid will need hormone replacement therapy to make up for low thyroid hormone levels.
Postpartum thyroiditis treatment depends on the phase of thyroiditis and degree of symptoms that a patient has. Women presenting with thyrotoxicosis may be treated with beta blockers to decrease symptoms such as palpitations and tremors. As symptoms improve, the medication can be reduced and stopped since the thyrotoxic phase is transient. Antithyroid medications are not used for the thyrotoxic phase since the thyroid is not overactive.
The hypothyroid phase may be treated with thyroid hormone replacement. If the hypothyroidism is mild, and the patient has few, if any, symptoms, no therapy may be necessary. If thyroid hormone therapy is started, treatment should be continued for approximately 6 to 12 months and then reduced to see if thyroid hormone is required permanently.
Thyroid function in most of the cases with postpartum thyroiditis returns to a normal state within 12 to 18 months of the onset of the symptoms 36. However, some mothers do not recover from the hypothyroid phase, and they will develop permanent hypothyroidism 40.
Subacute postpartum thyroiditis causes
Postpartum thyroiditis is an autoimmune disorder where your body’s immune system creates antibodies to thyroid peroxidase (thyroid peroxidase antibodies [TPOAb]) that attack your thyroid cells as if they were bacteria, viruses or some other foreign body. It is not known why certain people make anti-thyroid antibodies, although this tends to run in families. Scientists are still researching what causes the antibodies to attack after a pregnancy. A popular theory is that you’re more likely to get diagnosed if you had an underlying autoimmune condition (that you didn’t know about) before pregnancy. An autoimmune condition happens when antibodies attack healthy cells and tissue.
Postpartum thyroiditis is also known as autoimmune lymphocytic thyroiditis with lymphocytic infiltration within the thyroid gland 36. Histological features of postpartum thyroiditis are similar to Hashimoto thyroiditis, and both are associated with HLA-D and HLA-B haplotypes 36. These findings indicate the importance of inherited risk factors 41, 42.
The presence of thyroid peroxidase antibodies (TPOAb) is also seen in other autoimmune thyroid diseases such as Graves disease and Hashimoto thyroiditis. The level of thyroid peroxidase antibodies (TPOAb) reflects the severity of the infiltration of lymphocytes within the thyroid gland. Thyroid peroxidase antibodies (TPOAb) are complement-fixing, which subsequently induce antibody-dependent cell-mediated cytotoxicity 43.
You’re more likely to develop postpartum thyroiditis if you 39:
- Have had postpartum thyroiditis before (20% of women will have recurrence of thyroiditis with additional pregnancies).
- Have type 1 diabetes (a type of autoimmune condition).
- Have a personal or family history of thyroid disease.
- Had anti-thyroid antibodies before you were pregnant (you may not have known because you didn’t notice symptoms).
- Chronic viral hepatitis.
Subacute postpartum thyroiditis symptoms
Postpartum thyroiditis usually unfolds in phases:
- Phase 1: The inflammation causes your thyroid to produce and release too many hormones (hyperthyroidism). This phase usually happens between one to six months after a pregnancy. It may last from one week up to three months.
- Most people don’t notice symptoms in the first phase, hyperthyroidism. If you do experience symptoms, they usually involve body functions (like metabolism) being “hyper” or sped up. They may include:
- Anxiety
- Hair loss
- Unexplained weight loss
- Rapid heart rate (tachycardia)
- Hypersensitivity to heat.
- Most people don’t notice symptoms in the first phase, hyperthyroidism. If you do experience symptoms, they usually involve body functions (like metabolism) being “hyper” or sped up. They may include:
- Phase 2: Your thyroid doesn’t produce or release enough hormones (hypothyroidism). This phase usually takes place four to eight months after pregnancy. It can last as long as a year.
- It isn’t until the second phase, hypothyroidism, that most people notice symptoms. Symptoms of hypothyroidism usually involve body functions (like metabolism) slowing down. They may include:
- Fatigue
- Weight gain
- Depression
- Dry skin
- Constipation
- Muscle pain
- Not having enough breast (chest) milk come in
- Hypersensitivity to cold.
- It isn’t until the second phase, hypothyroidism, that most people notice symptoms. Symptoms of hypothyroidism usually involve body functions (like metabolism) slowing down. They may include:
- Phase 3: Your thyroid usually returns to producing normal hormone levels.
Not everyone experiences all the phases in order, though. Some people skip over the hypothyroid phase. They have hyperthyroidism, and then their thyroid function returns to normal.
The classic description of postpartum thyroiditis includes thyrotoxicosis also known as overactive thyroid (high thyroid hormone levels in the blood) followed by hypothyroidism also known as underactive thyroid (low thyroid hormone levels in the blood). Not all women appear to go through both phases; approximately 1/3 of patients will manifest both, while 1/3 of patients will have only a overactive thyroid (thyrotoxic) or only a hypothyroid (underactive thyroid) phase.
The thyrotoxic (overactive thyroid) phase occurs 1 to 4 months after delivery of a child and lasts for 1 to 3 months. The thyrotoxic (overactive thyroid) phase is associated with symptoms including anxiety, insomnia, palpitations (fast heart rate), fatigue, weight loss, and irritability. Since these symptoms may often be attributed to changes after delivery and the stress of having a new baby, the thyrotoxic (overactive thyroid) phase of post-partum thyroiditis is often overlooked.
It is much more common for women to present during the hypothyroid (underactive thyroid) phase. This typically occurs 4 to 8 months after delivery of a baby and may last up to 9 to 12 months. Typical hypothyroid (underactive thyroid) symptoms include fatigue, weight gain, constipation, dry skin, depression and poor exercise tolerance. Most women will regain normal thyroid function within 12 to 18 months after the onset of symptoms. However, approximately 20% of those that go into a hypothyroid phase will remain hypothyroid. Women who remain hypothyroid will need hormone replacement therapy to make up for low thyroid hormone levels.
Subacute postpartum thyroiditis diagnosis
If you have any signs or symptoms that suggest you might have thyroid dysfunction, your doctor will want to know your complete medical history. You will be asked questions about your possible risk factors, symptoms, and any other health problems or concerns. If someone in your family has had thyroid problem, it is important to tell your doctor, as you might be at high risk for this disease.
A blood test is usually enough to diagnose postpartum thyroiditis. It can also help exclude similar diagnoses, like Graves’ disease or Hashimoto’s thyroiditis.
Testing thyroid function
To determine if thyrotoxicosis (overactive thyroid) or hypothyroidism (underactive thyroid) is the cause of your symptoms, your doctor will order blood tests that may include the following:
- Thyroid stimulating hormone (TSH) test. Thyroid-stimulating hormone (TSH or thyrotropin) is produced by the pituitary gland. When the pituitary detects low thyroid hormones in the blood, it sends thyroid-stimulating hormone (TSH) to the thyroid to prompt an increase in thyroid hormone production. High TSH levels in the blood indicates hypothyroidism.
- Thyroxine (T4) tests. The main thyroid hormone is thyroxine (T4). A low blood level of thyroxine (T4) confirms the findings of a high TSH level and indicates the problem is within the thyroid itself.
- Thyroglobulin (Tg). Thyroglobulin (Tg) is a protein made by the thyroid gland. Thyroglobulin (Tg) plays a key role in helping the body create, store and release thyroid hormones. Thyroglobulin (Tg) may be present in the blood when the thyroid has been damaged. Some doctors may check thyroglobulin (Tg) levels when diagnosing hyperthyroidism and hypothyroidism, thyroid disorders that are not thyroid cancer. If you recently had surgery for thyroid cancer, your doctor may measure thyroglobulin (Tg) levels to determine whether your treatment successfully removed all of your thyroid cells, including noncancerous and cancerous cells. This postoperative evaluation of thyroglobulin (Tg) levels is usually ordered four to six weeks following surgery. The presence of detectable thyroglobulin (Tg), particularly a rising thyroglobulin level, may give an early warning of a recurrence of thyroid cancer.
Subacute postpartum thyroiditis antibodies
More than one disease process can lead to thyrotoxicosis (overactive thyroid) or hypothyroidism (underactive thyroid). To determine if postpartum thyroiditis is the cause of thyrotoxicosis (overactive thyroid) or hypothyroidism, your doctor will order an antibody test.
The intended purpose of an antibody is to flag disease-causing foreign agents that need to be destroyed by other actors in the immune system. In an autoimmune disorder, the immune system produces rogue antibodies that target healthy cells or proteins in the body.
Usually in postpartum thyroiditis, the immune system produces an antibody to thyroid peroxidase (TPOAb), a protein that plays an important part in thyroid hormone production.
Thyroid peroxidase antibodies (TPOAb)
Thyroid peroxidase antibodies (TPOAb) may be checked in patients with a high thyroid-stimulating hormone (TSH or thyrotropin) to help establish the underlying cause. Postpartum thyroiditis is an autoimmune disorder where your body’s immune system creates antibodies to thyroid peroxidase (thyroid peroxidase antibodies [TPOAb]) that attack your thyroid cells. Postpartum thyroiditis is also known as destructive thyroiditis with lymphocytic infiltration within the thyroid gland 36.
The presence of thyroid peroxidase antibodies (TPOAb) is also seen in other autoimmune thyroid diseases such as Graves disease and Hashimoto thyroiditis. The level of thyroid peroxidase antibodies (TPOAb) reflects the severity of the infiltration of lymphocytes within the thyroid gland. Thyroid peroxidase antibodies (TPOAb) are complement-fixing, which subsequently induce antibody-dependent cell-mediated cytotoxicity 43. Almost all patients with Hashimoto’s thyroiditis have high levels of thyroid peroxidase antibodies (TPOAb). If thyroid peroxidase antibodies (TPOAb) are negative, it means you may not have a thyroid disorder and that the high thyroid-stimulating hormone (TSH) may resolve spontaneously, or there is an underlying thyroid disorder caused by another factor (e.g. following a viral infection or due to prescribed medication).
It is normally only necessary to measure thyroid peroxidase antibodies (TPOAb) once when trying to establish the cause of the thyroid disorder. Thyroid peroxidase antibodies (TPOAb) are found in more than 90% of people with autoimmune hypothyroidism and also in about 10% of people without a thyroid disorder where they may be ‘markers’ of autoimmunity. This means they may be more likely to develop autoimmune disease in the future.
Thyroid stimulating antibodies (TRAb)
Thyroid stimulating antibodies (TRAb) also known as thyrotropin receptor antibodies (TRAb) bind to the receptors on thyroid cells normally activated by TSH. In Graves’ disease, an antibody called thyroid-stimulating immunoglobulin (TSI) binds to the TSH receptor and mimics the action of TSH. This causes constant stimulation of the thyroid gland, prompting it to release too much thyroid hormone.
Thyroglobulin antibodies (TgAb)
Thyroglobulin antibodies (TgAb) are directed against the thyroglobulin (Tg) molecule and are found in approximately 10% of the general population; they can be raised in people with Hashimoto’s thyroiditis.
Where thyroglobulin antibodies (TgAb) are present it can affect the accuracy of the measurement of thyroglobulin (Tg) and so additional means need to be used to monitor people who have had treatments for thyroid cancer. Thyroglobulin antibodies (TgAb) generally do not add anything to thyroid peroxidase antibody (TPOAb) results in the assessment of people with a raised TSH.
Subacute postpartum thyroiditis treatment
Subacute postpartum thyroiditis treatment depends on the phase of thyroiditis and degree of symptoms that you have. Treatment depends on whether you’re experiencing hyperthyroidism or hypothyroidism. Most women have mild symptoms and don’t need treatment unless symptoms worsen. Mothers presenting with thyrotoxicosis may be treated with beta blockers to decrease symptoms such as heart palpitations (feelings of having a fast-beating, fluttering or pounding heart) and tremors. As symptoms improve, the medication can be reduced and stopped since the thyrotoxic phase is temporary. Antithyroid medications are not used for the thyrotoxic phase since the thyroid is not overactive.
The hypothyroid phase may be treated with thyroid hormone replacement. If the hypothyroidism is mild, and the patient has few, if any, symptoms, no therapy may be necessary.
Hypothyroidism associated with postpartum thyroiditis is usually treated with a synthetic hormone called levothyroxine (Levoxyl, Synthroid, others). The synthetic hormone works like the thyroxine (T4) hormone naturally produced by your thyroid. The treatment goal is to restore and maintain adequate thyroxine (T4) hormone levels and improve symptoms of hypothyroidism. If thyroid hormone therapy is started, treatment should be continued for approximately 6 to 12 months and then reduced to see if thyroid hormone is required permanently. You’ll probably be able to taper off the medication as your thyroid returns to normal. Your doctor will monitor your thyroid levels during treatment every six to eight weeks 44.
Certain medications, supplements and foods may affect your ability to absorb levothyroxine (synthetic thyroxine). It may be necessary to take levothyroxine at least four hours before these substances. Talk to your doctor about any of the following:
- Soy products
- High-fiber foods
- Iron supplements, including multivitamins that contain iron
- Cholestyramine (Prevalite), a medication used to lower blood cholesterol levels
- Aluminum hydroxide, which is found in some antacids
- Sucralfate, an ulcer medication
- Calcium supplements.
Selenium supplementation has been explored for its possible anti-inflammatory effect in autoimmune thyroiditis 45. However, clinical trials of selenium supplementation in pregnancy have shown mixed results 46. Therefore, selenium supplementation for prevention or treatment of postpartum thyroiditis is currently not recommended 44.
Subacute postpartum thyroiditis prognosis
Subacute postpartum thyroiditis is usually temporary. Seventy to 80% of women eventually no longer need medication because their thyroid starts making hormones at normal levels again within 12 to 18 months. The other 20% to 30% cases with subacute postpartum thyroiditis stay in the hypothyroid state one year postpartum 40. Women who are positive for serum thyroid peroxidase antibodies (TPOAb) are at increased risk of developing permanent hypothyroidism after postpartum thyroiditis 47. They’ll need thyroid hormone replacement therapy long-term.
Postpartum hypothyroidism also makes you more likely to develop future thyroid issues, including hypothyroidism or an enlarged thyroid gland (goiter). Even if your thyroid returns to normal, your doctor will likely need to get regular TSH tests to monitor your thyroid hormone function.
If postpartum thyroiditis does not evolved into permanent hypothyroidism, it tends to recur 5. The recurrence risk of postpartum thyroiditis in a patient with the previous history of postpartum thyroiditis is reported at up to 70% 48, 49, 50.
Subacute thyroiditis causes
Subacute thyroiditis is an uncommon condition. It is thought to be the result of a viral infection. Subacute thyroiditis often occurs a few weeks after a viral infection of the ear, sinus, or throat, such as coxsackievirus 51, mumps virus 52, Epstein-Barr virus 53, cytomegalovirus 54, influenza virus 55, 56, 57, COVID-19 and adenovirus 22, 4, 16, 15, 23. Subacute thyroiditis occurs most often in middle-aged women with symptoms of a viral upper respiratory tract infection in the past month.
Initially, it was thought that subacute thyroiditis is common in summers 15, but other studies have shown it to be equally distributed throughout the season 9, 7.
Other causes of subacute thyroiditis, or at least conditions that have been associated with the disease, include the following 58:
- Radioiodine therapy for Graves disease can result in transient thyroidal inflammation, causing thyroiditis
- Subacute thyroiditis also has been described following external radiation to the neck
- Subacute thyroiditis has presented as a paraneoplastic manifestation of renal cell carcinoma
- An association between subacute thyroiditis and febrile neutrophilic dermatoses (Sweet syndrome) has been reported
- Concurrence of giant cell arteritis has been reported in patients with classic de Quervain thyroiditis
- Subacute thyroiditis has been described after bone marrow transplantation for chronic granulocytic leukemia
Subacute thyroiditis symptoms
The symptoms of subacute thyroiditis depend on the type of subacute thyroiditis you have and its phase. The most obvious symptom of subacute thyroiditis is pain in your neck caused by a swollen and inflamed thyroid gland. Sometimes, the pain can spread (radiate) to your jaw or ears. Your thyroid gland may be painful and swollen for weeks or, in rare cases, months. Some people with subacute thyroiditis have an enlarged thyroid gland (goiter).
Other symptoms include:
- Tenderness when gentle pressure is applied to the thyroid gland
- Difficulty or painful swallowing, hoarseness
- Fatigue, feeling weak
- Fever
The inflamed thyroid gland may release too much thyroid hormone, causing symptoms of hyperthyroidism, including:
- More frequent bowel movements
- Hair loss
- Heat intolerance
- Irregular (or very light) menstrual periods in women
- Mood changes
- Nervousness, shaking hands (tremors)
- Palpitations
- Sweating
- Weight loss, but with increased appetite
As the thyroid gland heals, it may release too little hormone, causing symptoms of hypothyroidism, including:
- Cold intolerance
- Constipation
- Fatigue
- Irregular (or heavy) menstrual periods in women
- Weight gain
- Dry skin
- Mood changes
Thyroid gland function often returns to normal over a few months. During this time you may need treatment for your underactive thyroid. In rare cases, hypothyroidism may be permanent.
Figure 7. Subacute thyroiditis time course
Symptoms of thyrotoxicosis
The thyrotoxic phase of subacute thyroiditis is usually short, lasting one to three months. If your thyroid cells are damaged quickly and there’s a leak of excess thyroid hormone, you might experience symptoms of hyperthyroidism (overactive thyroid), which include:
- Fast heart rate
- Increased appetite
- Unexplained weight loss
- Anxiety and nervousness
- Irritability
- Trouble sleeping
- Increased sweating and sensitivity to heat
- Tremors.
Symptoms of hypothyroidism
If your thyroid cells are damaged and thyroid hormone levels fall, you might experience the symptoms of hypothyroidism (underactive thyroid), which include:
- Fatigue
- Unexplained weight gain
- Constipation
- Depression
- Dry skin
- Increased sensitivity to cold
- Muscle weakness
- Decreased ability to concentrate and focus.
Subacute thyroiditis diagnosis
Your doctor will perform a physical exam, including assessing your thyroid, and ask you questions about your symptoms and medical history. If your doctor suspect you may have subacute thyroiditis, he/she will likely order any combination of the following tests to help diagnose it:
- Thyroid function tests: These are blood tests that measure the levels of thyroid-related hormones and thyroid hormones in your body, including:
- Thyroid-stimulating hormone (TSH)
- T3 (triiodothyronine)
- T4 (thyroxine)
- Thyroid stimulating hormone (TSH) comes from your pituitary gland and stimulates your thyroid gland to produce the hormones T4 (thyroxine) and T3 (triiodothyronine), which together are called thyroid hormones.
- Thyroglobulin (Tg). Thyroglobulin (Tg) is a protein made by the thyroid gland. Thyroglobulin (Tg) plays a key role in helping the body create, store and release thyroid hormones. Thyroglobulin (Tg) may be present in the blood when the thyroid has been damaged. Some doctors may check thyroglobulin (Tg) levels when diagnosing hyperthyroidism and hypothyroidism, thyroid disorders that are not thyroid cancer. If you recently had surgery for thyroid cancer, your doctor may measure thyroglobulin (Tg) levels to determine whether your treatment successfully removed all of your thyroid cells, including noncancerous and cancerous cells. This postoperative evaluation of thyroglobulin (Tg) levels is usually ordered four to six weeks following surgery. The presence of detectable thyroglobulin (Tg), particularly a rising thyroglobulin level, may give an early warning of a recurrence of thyroid cancer.
- Thyroid ultrasound: Providers often use ultrasound to evaluate the anatomy of your thyroid gland. It can show a nodule (a growth) in your thyroid gland, a change in blood flow to your thyroid and the density of the gland.
- Thyroid antibody tests: These are blood tests that measure thyroid antibodies that include antithyroid (microsomal) antibodies (TPO) or thyroid receptor stimulating antibodies (TRAb). These antibodies could signal that you have a type of thyroiditis caused by autoimmune disease. Positive antithyroglobulin antibodies are less often associated with autoimmune thyroid disease.
- Erythrocyte sedimentation rate (ESR or sed rate): This is a blood test that helps detect inflammation in your body. The ESR is high in subacute thyroiditis.
- C-reactive protein (CRP): C-reactive protein (CRP) test that measures the level of c-reactive protein (CRP) in your blood. CRP increases when there’s inflammation in your body, and it’s usually significantly elevated in acute infectious thyroiditis.
- Radioactive iodine uptake (RAIU) test: Radioactive iodine uptake (RAIU) test measures the amount of radioactive iodine (taken by mouth) that your thyroid gland absorbs. The amount is always low in the thyrotoxic phase of thyroiditis.
The commonest lab abnormalities in subacute thyroiditis are elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), T3, and T4, thyroglobulin (Tg) and low thyroid-stimulating hormone (TSH) 1. Serum thyroglobulin (TG) elevation may persist for well over a year after the initial diagnosis, indicating that disordered follicular architecture, low-grade inflammation, or both can persist for a relatively long period. Thyroglobulin (TG) in patients with subacute thyroiditis is heterogeneous with respect to sedimentation properties and structural integrity. The presence of serum thyroglobulin (TG) with hormone residue is a common and distinctive feature of subacute thyroiditis.
Additional findings
Serum alkaline phosphatase (ALP) levels may be elevated in as many as 60% of patients; less commonly, other liver function test results may be elevated. Mild increases in pancreatic enzymes have also been reported 60.
Serum IL-6 levels are increased, probably reflecting ongoing inflammation. While other parameters, such as ESR and CRP, decrease during corticosteroid therapy, IL-6 levels continue to increase (up to 17 days in some patients). This probably reflects dissociation between persistent release of IL-6 from the damaged thyroid cells and immediate inhibition of secondary inflammatory reactions by corticosteroids.
A Japanese study 8 derived from a medical records review of 852 patients with subacute thyroiditis found that most of the laboratory test–based indications for thyrotoxicosis and thyroiditis-associated inflammation peaked within a week after the onset of subacute thyroiditis.
Subacute thyroiditis differential diagnoses
Conditions to consider in the differential diagnosis of subacute thyroiditis include the following:
- Acute hemorrhage into a thyroid cyst, nodule, or neoplasm
- Infectious thyroiditis
- Radiation-induced thyroiditis
- Trauma- or palpation-induced thyroiditis
- Riedel or fibroid thyroiditis
- Graves thyrotoxicosis
- Toxic thyroid adenoma
- Toxic multinodular goiter
- Acute suppurative thyroiditis
The last disorder in the above list, acute suppurative thyroiditis, is most commonly caused by a bacterial infection of the thyroid via the conduit of a congenital pyriform sinus fistula. This pain and swelling in the early stages can be confused with subacute thyroiditis. A study by Masuoka et al 61 of 60 patients with acute suppurative thyroiditis found that careful imaging can provide clues to an early diagnosis of this condition, which can develop into a life-threatening endocrine emergency.
Subacute thyroiditis treatment
Subacute thyroiditis treatment depends on the type and the symptoms. Subacute thyroiditis treatment goal is to reduce thyroid pain and treat hyperthyroidism (overactive thyroid), if it occurs. Medicines such as aspirin or ibuprofen are used to control thyroid pain in mild cases. Patients with mild to moderate thyroid pain are generally treated with rest and aspirin usually taken every 4 to 6 hours as needed to treat thyroid pain, naproxen 500 to 1000 mg twice a day, or ibuprofen 400 to 800 mg orally every 8 hours 3. The median time from start of therapy to complete alleviation of pain is five weeks 7. If no improvement occurs within 1 week, oral corticosteroids (Prednisone) may be given in a dosage of 40 to 60 mg daily tapered to complete discontinuation over four to six weeks. Usually, symptoms improve in 2 to 3 days with non-steroidal anti-inflammatory drugs (NSAIDs); prednisone should be initiated if no improvement is noted. Steroids should provide pain relief in 1 to 2 days. The typical steroid course can be two months, occasionally longer. The persistence of pain beyond two days should need a further workup for other causes of thyroid pain 3. Once thyroid pain is improved, an attempt should be made to use the lowest possible dose, and dosing can be titrated by decreasing 5 to 10 mg every week 3. Recurrent pain should require up-titration of prednisone dose. Unfortunately, prednisone has no role in preventing thyroid dysfunction 28.
Symptoms of an overactive thyroid are treated with a class of medicines called beta-blockers to decrease palpitations (fast heart rate) and tremors. As your symptoms improve, your doctor will taper off the medication since the thyrotoxic phase is temporary. Exercise caution with the initial dose of propranolol; patients may become hypotensive, because they are often dehydrated from a decrease in the oral intake of fluids and increased perspiration from thyrotoxicosis. Beta-1 selective agents (metoprolol or atenolol) have more convenient dosing and are better tolerated.
If your thyroid becomes underactive during the recovery phase, thyroid hormone replacement may be needed. Hypothyroidism associated with subacute thyroiditis is treated with a synthetic hormone called levothyroxine (Levoxyl, Synthroid, others). The synthetic hormone works like the T-4 hormone naturally produced by your thyroid. The treatment goal is to restore and maintain adequate T-4 hormone levels and improve symptoms of hypothyroidism. Levothyroxine should be discontinued, and thyroid function tests should be done in 1 month to ensure hypothyroidism is transient. Some patients may need treatment with levothyroxine for a long time.
If your hypothyroidism is mild and you have few, if any, symptoms, then no medication may be necessary.
Diet
Avoiding high-dose iodine supplements, such as those found in seaweed tablets, during and after an episode of subacute thyroiditis is important 62. Inflammation appears to prevent the thyroid from escaping the iodine-induced Wolff-Chaikoff suppression of thyroid hormone synthesis. Consequently, patients are likely to become hypothyroid when ingesting large amounts of iodine 62.
Monitoring
Patients should be seen every 4 weeks for reassurance and for measurement of thyroid hormone levels. Occasionally, patients have relapses of the thyrotoxic phase and experience persistent symptoms. Monitor for the subsequent hypothyroid phase and treat with levothyroxine if patients are symptomatic 63.
Subacute granulomatous thyroiditis
Patients usually recover completely from subacute granulomatous thyroiditis. The episodes rarely recur. Generally, patients are not prone to other thyroid disease and do not need long-term follow-up.
Subacute lymphocytic and subacute postpartum thyroiditis
These conditions are sometimes associated with chronic thyroiditis. Postpartum thyroiditis usually recurs after each pregnancy. Patients should be observed routinely every 6-12 months for the development of goiter or hypothyroidism from chronic thyroiditis.
Subacute thyroiditis prognosis
The prognosis (outlook) for subacute thyroiditis is generally good. Subacute thyroiditis should improve on its own. People who develop subacute thyroiditis usually have symptoms for one to three months, but complete recovery of thyroid function can take up to 12 to 18 months. These people have about a 5% chance of developing permanent hypothyroidism. Long-term or severe complications do not often occur. Approximately 5-10% of patients have permanent thyroid dysfunction, usually hypothyroidism, after an episode of subacute thyroiditis 26. Permanent goiter and thyroid dysfunction occur most frequently after postpartum thyroiditis.
Full thyroid function recovery from postpartum and silent (painless) thyroiditis also takes about 12 to 18 months. People with these conditions have about a 20% chance of developing permanent hypothyroidism.
Subacute thyroiditis is not infectious. People cannot catch it from you. It is not inherited within families like some thyroid conditions.
- Majety P, Hennessey JV. Acute and Subacute, and Riedel’s Thyroiditis. [Updated 2022 Jul 25]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK285553[↩][↩]
- Subacute Thyroiditis. https://emedicine.medscape.com/article/125648-overview[↩][↩][↩][↩][↩][↩][↩]
- Tabassom A, Chippa V, Edens MA. De Quervain Thyroiditis. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526066[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Dayan CM, Daniels GH. Chronic autoimmune thyroiditis. N Engl J Med. 1996 Jul 11;335(2):99-107. doi: 10.1056/NEJM199607113350206[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Stagnaro-Green A. Approach to the patient with postpartum thyroiditis. J Clin Endocrinol Metab. 2012 Feb;97(2):334-42. doi: 10.1210/jc.2011-2576[↩][↩][↩]
- De Groot L, Abalovich M, Alexander EK, Amino N, Barbour L, Cobin RH, Eastman CJ, Lazarus JH, Luton D, Mandel SJ, Mestman J, Rovet J, Sullivan S. Management of thyroid dysfunction during pregnancy and postpartum: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012 Aug;97(8):2543-65. doi: 10.1210/jc.2011-2803. Erratum in: J Clin Endocrinol Metab. 2021 May 13;106(6):e2461. doi: 10.1210/clinem/dgab252[↩]
- Fatourechi V, Aniszewski JP, Fatourechi GZ, Atkinson EJ, Jacobsen SJ. Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study. J Clin Endocrinol Metab. 2003 May;88(5):2100-5. doi: 10.1210/jc.2002-021799[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Nishihara E, Ohye H, Amino N, Takata K, Arishima T, Kudo T, Ito M, Kubota S, Fukata S, Miyauchi A. Clinical characteristics of 852 patients with subacute thyroiditis before treatment. Intern Med. 2008;47(8):725-9. doi: 10.2169/internalmedicine.47.0740[↩][↩]
- Benbassat CA, Olchovsky D, Tsvetov G, Shimon I. Subacute thyroiditis: clinical characteristics and treatment outcome in fifty-six consecutive patients diagnosed between 1999 and 2005. J Endocrinol Invest. 2007 Sep;30(8):631-5. doi: 10.1007/BF03347442[↩][↩]
- Bindra A, Braunstein GD. Thyroiditis. Am Fam Physician. 2006 May 15;73(10):1769-76. https://www.aafp.org/pubs/afp/issues/2006/0515/p1769.html[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Mundy-Baird G, Kyriacou A, Syed AA. De Quervain subacute thyroiditis. CMAJ. 2021 Jul 5;193(26):E1007. doi: 10.1503/cmaj.202787[↩]
- Szabo SM, Allen DB. Thyroiditis. Differentiation of acute suppurative and subacute. Case report and review of the literature. Clin Pediatr (Phila). 1989 Apr;28(4):171-4. doi: 10.1177/000992288902800403[↩]
- Volpé R. The management of subacute (DeQuervain’s) thyroiditis. Thyroid. 1993 Fall;3(3):253-5. doi: 10.1089/thy.1993.3.253[↩]
- Ogawa E, Katsushima Y, Fujiwara I, Iinuma K. Subacute thyroiditis in children: patient report and review of the literature. J Pediatr Endocrinol Metab. 2003 Jul-Aug;16(6):897-900. doi: 10.1515/jpem.2003.16.6.897[↩]
- Martino E, Buratti L, Bartalena L, Mariotti S, Cupini C, Aghini-Lombardi F, Pinchera A. High prevalence of subacute thyroiditis during summer season in Italy. J Endocrinol Invest. 1987 Jun;10(3):321-3. doi: 10.1007/BF03348138[↩][↩][↩][↩][↩]
- Michas G, Alevetsovitis G, Andrikou I, Tsimiklis S, Vryonis E. De Quervain thyroiditis in the course of H1N1 influenza infection. Hippokratia. 2014 Jan;18(1):86-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4103053[↩][↩][↩]
- Muller I, Cannavaro D, Dazzi D, Covelli D, Mantovani G, Muscatello A, Ferrante E, Orsi E, Resi V, Longari V, Cuzzocrea M, Bandera A, Lazzaroni E, Dolci A, Ceriotti F, Re TE, Gori A, Arosio M, Salvi M. SARS-CoV-2-related atypical thyroiditis. Lancet Diabetes Endocrinol. 2020 Sep;8(9):739-741. doi: 10.1016/S2213-8587(20)30266-7[↩]
- Sakiyama R. Thyroiditis: a clinical review. Am Fam Physician. 1993 Sep 15;48(4):615-21.[↩][↩]
- Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med. 2003 Jun 26;348(26):2646-55. doi: 10.1056/NEJMra021194. Erratum in: N Engl J Med. 2003 Aug 7;349(6):620.[↩][↩]
- Schubert MF, Kountz DS. Thyroiditis. A disease with many faces. Postgrad Med. 1995 Aug;98(2):101-3, 107-8, 112.[↩][↩][↩][↩][↩][↩][↩]
- Ross DS, Burch HB, Cooper DS, Greenlee MC, Laurberg P, Maia AL, Rivkees SA, Samuels M, Sosa JA, Stan MN, Walter MA. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid. 2016 Oct;26(10):1343-1421. doi: 10.1089/thy.2016.0229. Erratum in: Thyroid. 2017 Nov;27(11):1462. doi: 10.1089/thy.2016.0229.correx[↩]
- Farwell AP, Braverman LE. Inflammatory thyroid disorders. Otolaryngol Clin North Am. 1996 Aug;29(4):541-56. https://doi.org/10.1016/S0030-6665(02)00133-0[↩][↩][↩][↩][↩]
- Meftah E, Rahmati R, Zari Meidani F, Khodadadi S, Chitzan-Zadeh K, Esfahanian F, Afshar S. Subacute thyroiditis following COVID-19: A systematic review. Front Endocrinol (Lausanne). 2023 Apr 5;14:1126637. doi: 10.3389/fendo.2023.1126637[↩][↩]
- Subacute Thyroiditis. https://emedicine.medscape.com/article/125648-overview#a4[↩][↩][↩][↩][↩]
- Sherman SI, Ladenson PW. Subacute thyroiditis causing thyroid storm. Thyroid. 2007 Mar;17(3):283. doi: 10.1089/thy.2007.0070[↩]
- Subacute Thyroiditis Prognosis. https://emedicine.medscape.com/article/125648-overview#a7[↩][↩][↩][↩]
- Kubota S, Nishihara E, Kudo T, Ito M, Amino N, Miyauchi A. Initial treatment with 15 mg of prednisolone daily is sufficient for most patients with subacute thyroiditis in Japan. Thyroid. 2013 Mar;23(3):269-72. doi: 10.1089/thy.2012.0459[↩]
- Ohsako N, Tamai H, Sudo T, Mukuta T, Tanaka H, Kuma K, Kimura A, Sasazuki T. Clinical characteristics of subacute thyroiditis classified according to human leukocyte antigen typing. J Clin Endocrinol Metab. 1995 Dec;80(12):3653-6. doi: 10.1210/jcem.80.12.8530615[↩][↩]
- Slatosky J, Shipton B, Wahba H. Thyroiditis: differential diagnosis and management. Am Fam Physician. 2000 Feb 15;61(4):1047-52, 1054. Erratum in: Am Fam Physician 2000 Jul 15;62(2):318. https://www.aafp.org/pubs/afp/issues/2000/0215/p1047.html[↩][↩]
- Alper AT, Hasdemir H, Akyol A, Cakmak N. Incessant ventricular tachycardia due to subacute thyroiditis. Int J Cardiol. 2007 Mar 2;116(1):e22-4. doi: 10.1016/j.ijcard.2006.08.068[↩]
- Salih AM, Kakamad FH, Rawezh QS, Masrur SA, Shvan HM, Hawbash MR, Lhun TH. Subacute thyroiditis causing thyrotoxic crisis; a case report with literature review. Int J Surg Case Rep. 2017;33:112-114. doi: 10.1016/j.ijscr.2017.02.041[↩]
- Volpé R. Is silent thyroiditis an autoimmune disease? Arch Intern Med. 1988 Sep;148(9):1907-8. doi: 10.1001/archinte.1988.00380090009003[↩]
- Woolf PD. Transient painless thyroiditis with hyperthyroidism: a variant of lymphocytic thyroiditis? Endocr Rev. 1980 Fall;1(4):411-20. doi: 10.1210/edrv-1-4-411[↩][↩]
- Muller AF, Drexhage HA, Berghout A. Postpartum thyroiditis and autoimmune thyroiditis in women of childbearing age: recent insights and consequences for antenatal and postnatal care. Endocr Rev. 2001 Oct;22(5):605-30. doi: 10.1210/edrv.22.5.0441[↩]
- Nishimaki M, Isozaki O, Yoshihara A, Okubo Y, Takano K. Clinical characteristics of frequently recurring painless thyroiditis: contributions of higher thyroid hormone levels, younger onset, male gender, presence of thyroid autoantibody and absence of goiter to repeated recurrence. Endocr J. 2009;56(3):391-7. doi: 10.1507/endocrj.k08e-055[↩]
- Naji Rad S, Deluxe L. Postpartum Thyroiditis. [Updated 2023 Jun 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557646[↩][↩][↩][↩][↩]
- Epp R, Malcolm J, Jolin-Dahel K, Clermont M, Keely E. Postpartum thyroiditis. BMJ. 2021 Mar 3;372:n495. https://www.bmj.com/content/372/bmj.n495.long[↩][↩]
- Benvenga S, Di Bari F, Vita R, et al. Relatively high rate of postpartum thyroiditis in the Straits of Messina area. Predictivity of both postpartum thyroiditis and permanent hypothyroidism by performing, in the first trimester of gestation, thyroid ultrasonography and measurement of serum thyroperoxidase and thyroglobulin autoantibodies. J Clin Transl Endocrinol. 2018 Nov 23;15:12-18. doi: 10.1016/j.jcte.2018.11.004. Erratum in: J Clin Transl Endocrinol. 2020 Dec 17;23:100246[↩]
- Leslie De Groot, Marcos Abalovich, Erik K, et al. Management of Thyroid Dysfunction during Pregnancy and Postpartum: An Endocrine Society Clinical Practice Guideline, The Journal of Clinical Endocrinology & Metabolism, Volume 97, Issue 8, 1 August 2012, Pages 2543–2565, https://doi.org/10.1210/jc.2011-2803[↩][↩]
- Stagnaro-Green A. Clinical review 152: Postpartum thyroiditis. J Clin Endocrinol Metab. 2002 Sep;87(9):4042-7. doi: 10.1210/jc.2002-020524[↩][↩]
- LiVolsi VA. Postpartum thyroiditis. The pathology slowly unravels. Am J Clin Pathol. 1993 Sep;100(3):193-5. doi: 10.1093/ajcp/100.3.193[↩]
- Kologlu M, Fung H, Darke C, Richards CJ, Hall R, McGregor AM. Postpartum thyroid dysfunction and HLA status. Eur J Clin Invest. 1990 Feb;20(1):56-60. doi: 10.1111/j.1365-2362.1990.tb01791.x[↩]
- Prummel MF, Wiersinga WM. Thyroid peroxidase autoantibodies in euthyroid subjects. Best Pract Res Clin Endocrinol Metab. 2005 Mar;19(1):1-15. doi: 10.1016/j.beem.2004.11.003[↩][↩]
- Alexander EK, Pearce EN, Brent GA, Brown RS, Chen H, Dosiou C, Grobman WA, Laurberg P, Lazarus JH, Mandel SJ, Peeters RP, Sullivan S. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid. 2017 Mar;27(3):315-389. doi: 10.1089/thy.2016.0457. Erratum in: Thyroid. 2017 Sep;27(9):1212.[↩][↩]
- De Leo S, Pearce EN. Autoimmune thyroid disease during pregnancy. Lancet Diabetes Endocrinol. 2018 Jul;6(7):575-586. doi: 10.1016/S2213-8587(17)30402-3[↩]
- Hubalewska-Dydejczyk A, Duntas L, Gilis-Januszewska A. Pregnancy, thyroid, and the potential use of selenium. Hormones (Athens). 2020 Mar;19(1):47-53. doi: 10.1007/s42000-019-00144-2[↩]
- Premawardhana LD, Parkes AB, Ammari F, John R, Darke C, Adams H, Lazarus JH. Postpartum thyroiditis and long-term thyroid status: prognostic influence of thyroid peroxidase antibodies and ultrasound echogenicity. J Clin Endocrinol Metab. 2000 Jan;85(1):71-5. doi: 10.1210/jcem.85.1.6227[↩]
- Pearce EN Management of thyrotoxicosis: preconception, pregnancy, and the postpartum period. Endocr Pract. 2019 Jan;25(1):62-68. doi: 10.4158/EP-2018-0356[↩]
- Stagnaro-Green A. Postpartum thyroiditis. Best Pract Res Clin Endocrinol Metab. 2004 Jun;18(2):303-16. doi: 10.1016/j.beem.2004.03.008[↩]
- Nicholson WK, Robinson KA, Smallridge RC, Ladenson PW, Powe NR. Prevalence of postpartum thyroid dysfunction: a quantitative review. Thyroid. 2006 Jun;16(6):573-82. doi: 10.1089/thy.2006.16.573[↩]
- Volpé R, Row VV, Ezrin C. Circulating viral and thyroid antibodies in subacute thyroiditis. J Clin Endocrinol Metab. 1967 Sep;27(9):1275-84. doi: 10.1210/jcem-27-9-1275[↩]
- EYLAN E, ZMUCKY R, SHEBA C. Mumps virus and subacute thyroiditis; evidence of a causal association. Lancet. 1957 May 25;272(6978):1062-3. doi: 10.1016/s0140-6736(57)91438-1[↩]
- Volta C, Carano N, Street ME, Bernasconi S. Atypical subacute thyroiditis caused by Epstein-Barr virus infection in a three-year-old girl. Thyroid. 2005 Oct;15(10):1189-91. doi: 10.1089/thy.2005.15.1189[↩]
- Al Maawali A, Al Yaarubi S, Al Futaisi A. An infant with cytomegalovirus-induced subacute thyroiditis. J Pediatr Endocrinol Metab. 2008 Feb;21(2):191-3. doi: 10.1515/jpem.2008.21.2.191[↩]
- Dimos G, Pappas G, Akritidis N. Subacute thyroiditis in the course of novel H1N1 influenza infection. Endocrine. 2010 Jun;37(3):440-1. doi: 10.1007/s12020-010-9327-3[↩]
- Yasuji I. Subacute thyroiditis in a patient with juvenile idiopathic arthritis undergoing etanercept treatment: a case report and review of the literature. Mod Rheumatol. 2013 Mar;23(2):397-400. doi: 10.1007/s10165-012-0670-5[↩]
- Desailloud R, Hober D. Viruses and thyroiditis: an update. Virol J. 2009 Jan 12;6:5. doi: 10.1186/1743-422X-6-5[↩]
- Subacute Thyroiditis Etiology. https://emedicine.medscape.com/article/125648-overview#a5[↩]
- Hennessey Jv. Subacute Thyroiditis. [Updated 2018 Jun 12]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279084[↩]
- Salvi A, Spandrio S, Tosoni M, Rossi M, Balestrieri GP, Candrina R. Liver enzyme abnormalities in subacute thyroiditis. Recenti Prog Med. 1990 Nov;81(11):686-8.[↩]
- Masuoka H, Miyauchi A, Tomoda C, Inoue H, Takamura Y, Ito Y, Kobayashi K, Miya A. Imaging studies in sixty patients with acute suppurative thyroiditis. Thyroid. 2011 Oct;21(10):1075-80. doi: 10.1089/thy.2010.0366[↩]
- Subacute Thyroiditis Treatment & Management. https://emedicine.medscape.com/article/125648-treatment[↩][↩]
- Weihl AC, Daniels GH, Ridgway EC, Maloof F. Thyroid function tests during the early phase of subacute thyroiditis. J Clin Endocrinol Metab. 1977 Jun;44(6):1107-14. doi: 10.1210/jcem-44-6-1107[↩]





{kind=link}