
Contents
Postpartum thyroiditis
Postpartum thyroiditis is also known as autoimmune lymphocytic thyroiditis or inflammation of your thyroid gland that occurs in women within 12 months after the delivery of a baby (postpartum) without a history of thyroid disease prior to pregnancy 1, 2, 3, 4. Thyroiditis or inflammation of your thyroid gland can cause both thyrotoxicosis also known as overactive thyroid (high thyroid hormone levels in the blood) and hypothyroidism also known as underactive thyroid (low thyroid hormone levels in the blood). In postpartum thyroiditis, thyrotoxicosis (overactive thyroid or hyperthyroidism) occurs first followed by hypothyroidism (underactive thyroid). Your thyroid gland is an important organ of the endocrine system and is a butterfly-shaped gland with a right lobe and a left lobe located at the base of your neck just below the larynx (voice box). The thyroid gland usually cannot be felt through the skin. The thyroid produces thyroid hormone and calcitonin (control the amount of calcium in your blood) that help regulate many functions in your body including growth, heart rate, body temperature, and metabolism (the way every cell in the body uses energy).
The exact cause of postpartum thyroiditis is not known but it is believed to be an autoimmune disease (a disease in which your body’s immune system mistakenly attacks healthy cells in your thyroid) very similar to Hashimoto’s thyroiditis 2. As in Hashimoto’s thyroiditis, postpartum thyroiditis is associated with the presence of anti-thyroid antibodies (anti-thyroid peroxidase [TPOAb], anti-thyroglobulin [TgAb]). Women with positive antithyroid antibodies are at a much higher risk of developing postpartum thyroiditis than women who do not have have positive antibodies.
In the United Status, postpartum thyroiditis occurs in approximately 5% to 10% of women in the year after a birth, abortion or miscarriage. The incidence can be greater in certain high-risk populations. Women with type 1 diabetes or a history of thyroid problem are most likely to develop postpartum thyroiditis.
Postpartum thyroiditis occurs in any woman with 5:
- Autoimmune disorders (such as Type 1, or juvenile onset, Diabetes Mellitus)
- Positive anti-thyroid antibodies (risk correlates with antibody levels, the higher the antibody the higher the risk)
- History of previous thyroid dysfunction
- History of previous postpartum thyroiditis (20% of women will have recurrence of thyroiditis with additional pregnancies)
- Family history of thyroid dysfunction
- Chronic viral hepatitis
Postpartum thyroiditis usually unfolds in phases:
- Phase 1: The inflammation causes your thyroid to produce and release too many hormones (hyperthyroidism). This phase usually happens between 1 to 6 months after a pregnancy. It may last from one week up to three months.
- Phase 2: Your thyroid doesn’t produce or release enough hormones (hypothyroidism). This phase usually takes place 4 to 8 months after pregnancy. It can last as long as a year.
- Phase 3: Your thyroid usually returns to producing normal hormone levels.
Not everyone experiences all the phases in order, though. Some people skip over the hypothyroid phase. They have hyperthyroidism, and then their thyroid function returns to normal.
The classic description of postpartum thyroiditis includes thyrotoxicosis also known as overactive thyroid (high thyroid hormone levels in the blood) followed by hypothyroidism also known as underactive thyroid (low thyroid hormone levels in the blood). Not all women appear to go through both phases; approximately 1/3 of patients will manifest both, while 1/3 of patients will have only a overactive thyroid (thyrotoxic) or only a hypothyroid (underactive thyroid) phase.
The thyrotoxic (overactive thyroid) phase occurs 1 to 4 months after delivery of a child and lasts for 1 to 3 months. The thyrotoxic (overactive thyroid) phase is associated with symptoms including anxiety, insomnia, palpitations (fast heart rate), fatigue, weight loss, and irritability. Since these symptoms may often be attributed to changes after delivery and the stress of having a new baby, the thyrotoxic (overactive thyroid) phase of post-partum thyroiditis is often overlooked.
It is much more common for women to present during the hypothyroid (underactive thyroid) phase. This typically occurs 4 to 8 months after delivery of a baby and may last up to 9 to 12 months. Typical hypothyroid (underactive thyroid) symptoms include fatigue, weight gain, constipation, dry skin, depression and poor exercise tolerance. Most women will regain normal thyroid function within 12 to 18 months after the onset of symptoms. However, approximately 20% of those that go into a hypothyroid phase will remain hypothyroid. Women who remain hypothyroid will need hormone replacement therapy to make up for low thyroid hormone levels.
Postpartum thyroiditis treatment depends on the phase of thyroiditis and degree of symptoms that a patient has. Women presenting with thyrotoxicosis may be treated with beta blockers to decrease symptoms such as palpitations and tremors. As symptoms improve, the medication can be reduced and stopped since the thyrotoxic phase is transient. Antithyroid medications are not used for the thyrotoxic phase since the thyroid is not overactive.
The hypothyroid phase may be treated with thyroid hormone replacement. If the hypothyroidism is mild, and the patient has few, if any, symptoms, no therapy may be necessary. If thyroid hormone therapy is started, treatment should be continued for approximately 6 to 12 months and then reduced to see if thyroid hormone is required permanently.
Thyroid function in most of the cases with postpartum thyroiditis returns to a normal state within 12 to 18 months of the onset of the symptoms 1. However, some mothers do not recover from the hypothyroid phase, and they will develop permanent hypothyroidism 6.
How long does it take to recover from postpartum thyroiditis?
Postpartum thyroiditis usually lasts between a year and a year and a half. Usually, within 12 to 18 months from when you first notice symptoms, your thyroid will return to normal. At this point, you’ll no longer need medicine.
Is it safe to breastfeed while I’m taking beta-blockers or thyroid hormone?
Certain beta-blockers are safe to use while you’re breastfeeding because only a small amount shows up in breast milk. The lowest possible dose to relieve your symptoms is best. Only a small amount of thyroid hormone medicine reaches your baby through breast milk, so it’s safe to take while you’re breastfeeding.
Can I get pregnant again after postpartum thyroiditis?
Yes. Many women go on to have healthy pregnancies after postpartum thyroiditis. It’s important, though, that you tell your doctor that you’ve had postpartum thyroiditis if you’re planning a pregnancy in the future. Approximately 20% of women with a history of postpartum thyroiditis develop it during later pregnancies.
Your doctor can monitor your thyroid hormone levels to help guide you through a healthy pregnancy.
Thyroid gland
The thyroid gland is the largest adult gland to have a purely endocrine function, weighing about 25-30 g. The thyroid gland is a small butterfly shaped gland with 2 lobes, the right lobe and the left lobe joined by a narrow piece of the thyroid gland called the isthmus, that is located in front of your neck near the base of your throat, beneath the larynx (voice box or Adam’s apple). About 50% of thyroid glands have a small third lobe, called the pyramidal lobe. It extends superiorly from the isthmus. The thyroid gland makes and releases hormones. You can’t usually feel a thyroid gland that is normal.
The thyroid gland has 2 main types of cells:
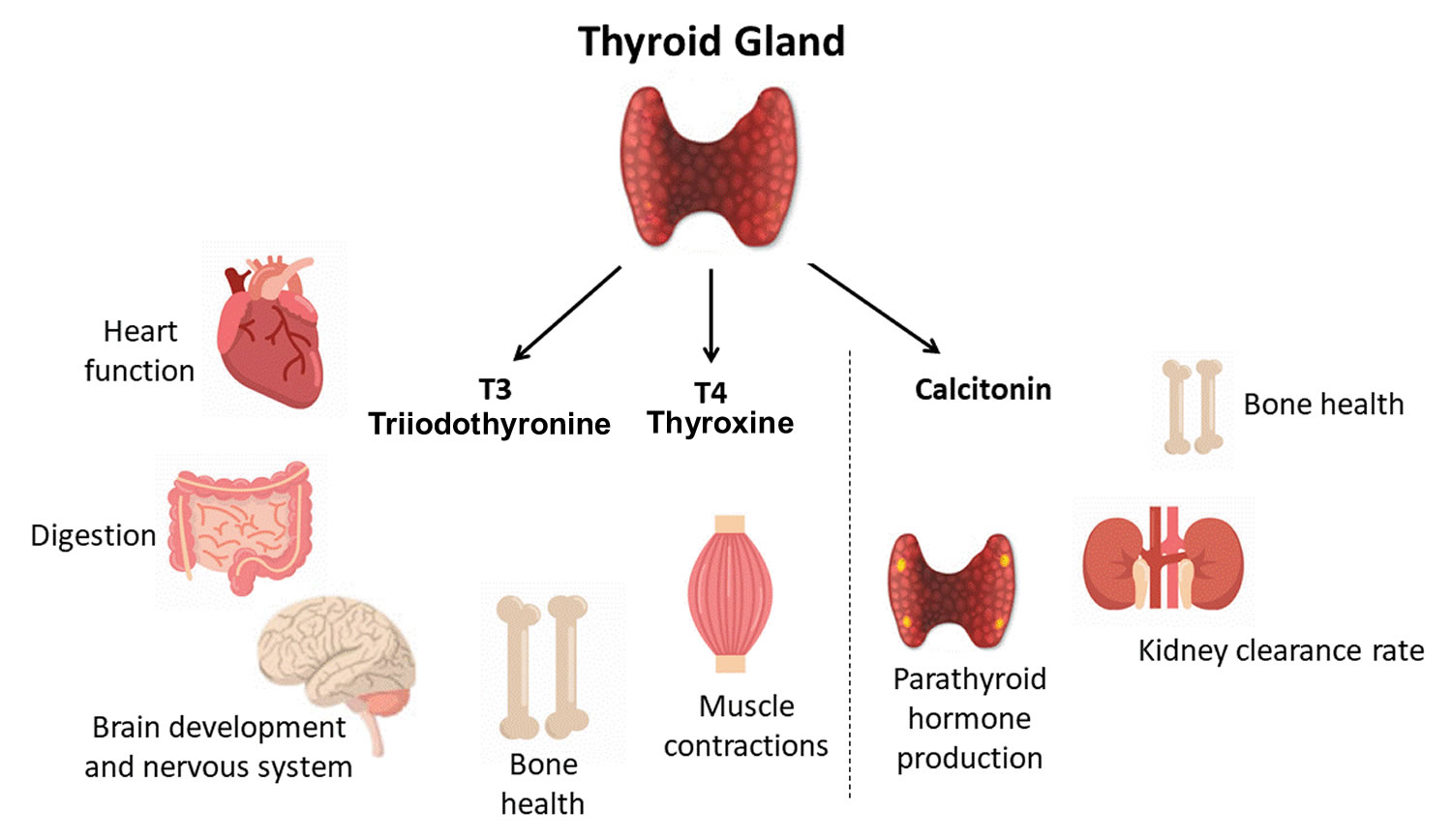
- Follicular cells use iodine from the blood to make thyroid hormones, which help regulate a person’s metabolism. Having too much thyroid hormone (hyperthyroidism) can cause a fast or irregular heartbeat, trouble sleeping, nervousness, hunger, weight loss, and a feeling of being too warm. Having too little thyroid hormone (hypothyroidism) causes a person to slow down, feel tired, and gain weight. The amount of thyroid hormone released by the thyroid gland is regulated by the pituitary gland at the base of the brain, which makes a substance called thyroid-stimulating hormone (TSH) (see Figure 5).
- C cells also called parafollicular cells at the periphery of the follicles that make calcitonin, a hormone that helps control how your body uses calcium. The parafollicular cells (C cells) respond to rising levels of blood calcium by secreting the hormone calcitonin. Calcitonin antagonizes (blocks) parathyroid hormone (PTH) and stimulates osteoblast activity, thus promoting calcium deposition and bone formation. It is important mainly in children, having relatively little effect in adults. Parathyroid hormone is made by parathyroid glands. These sit behind and are attached to the thyroid gland (see Figure 1).
Other, less common cells in the thyroid gland include immune system cells (lymphocytes) and supportive (stromal) cells.
Thyroid hormone is secreted or inhibited in response to fluctuations in metabolic rate. The brain monitors the body’s metabolic rate and stimulates thyroid hormone secretion through the action of thyrotropin-releasing hormone (TRH) and thyroid stimulating hormone (TSH) as depicted in figure 5.
The primary effect of thyroid hormone (TH) is to increase one’s metabolic rate. As a result, it raises oxygen consumption and has a calorigenic effect—it increases heat production. To ensure an adequate blood and oxygen supply to meet this increased metabolic demand, thyroid hormone also raises the breathing (respiratory) rate, heart rate, and strength of the heartbeat. It stimulates the appetite and accelerates the breakdown of carbohydrates, fats, and protein for fuel. Thyroid hormone also promotes alertness and quicker reflexes; growth hormone secretion; growth of the bones, skin, hair, nails, and teeth; and development of the fetal nervous system.
Figure 1. Thyroid gland location and parathyroid gland
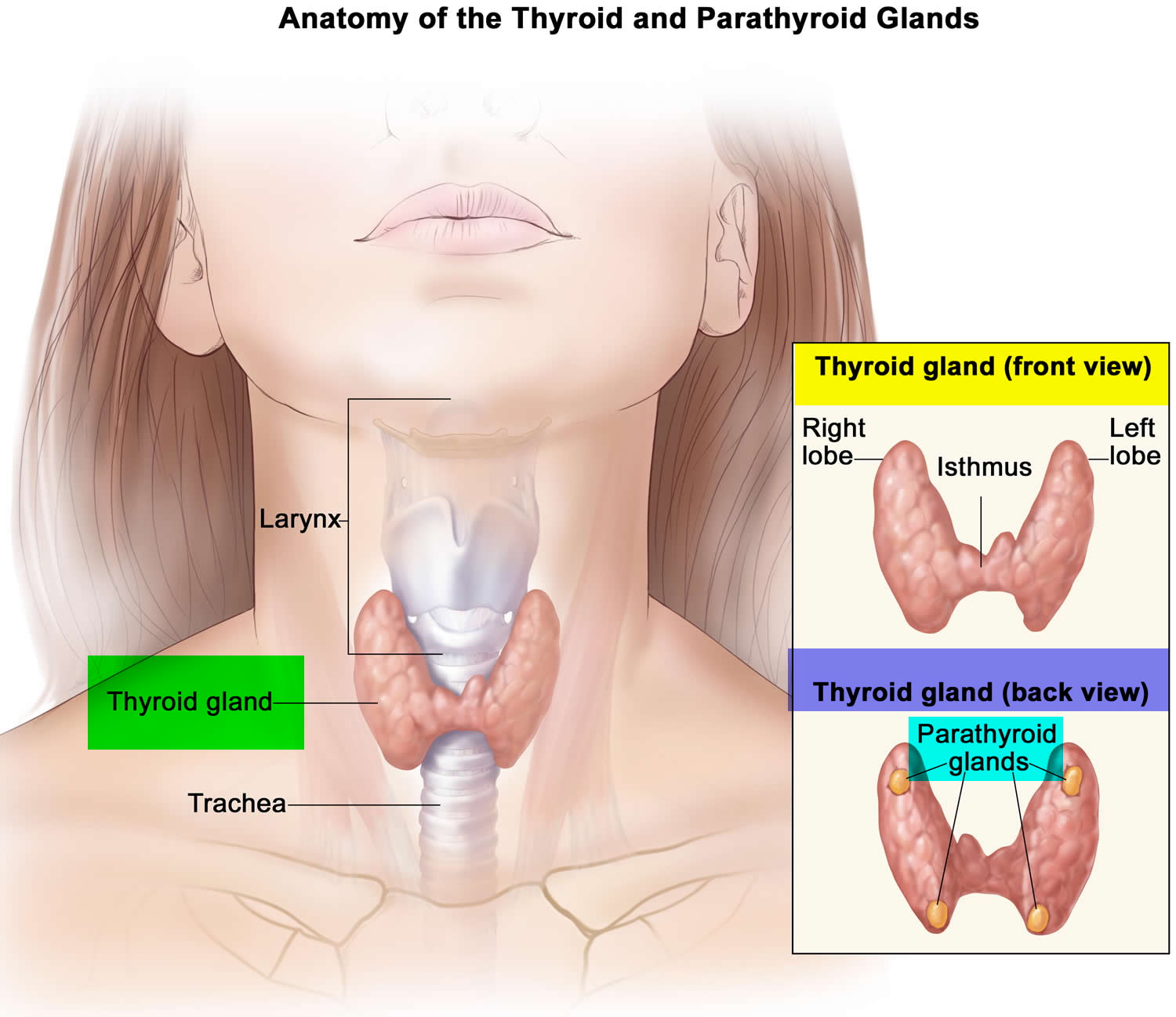
Footnotes: Anatomy of the thyroid and parathyroid glands. The thyroid gland lies at the base of the throat near the trachea. It is shaped like a butterfly, with the right lobe and left lobe connected by a thin piece of tissue called the isthmus. The parathyroid glands are four pea-sized organs found in the neck near the thyroid. The thyroid and parathyroid glands make hormones.
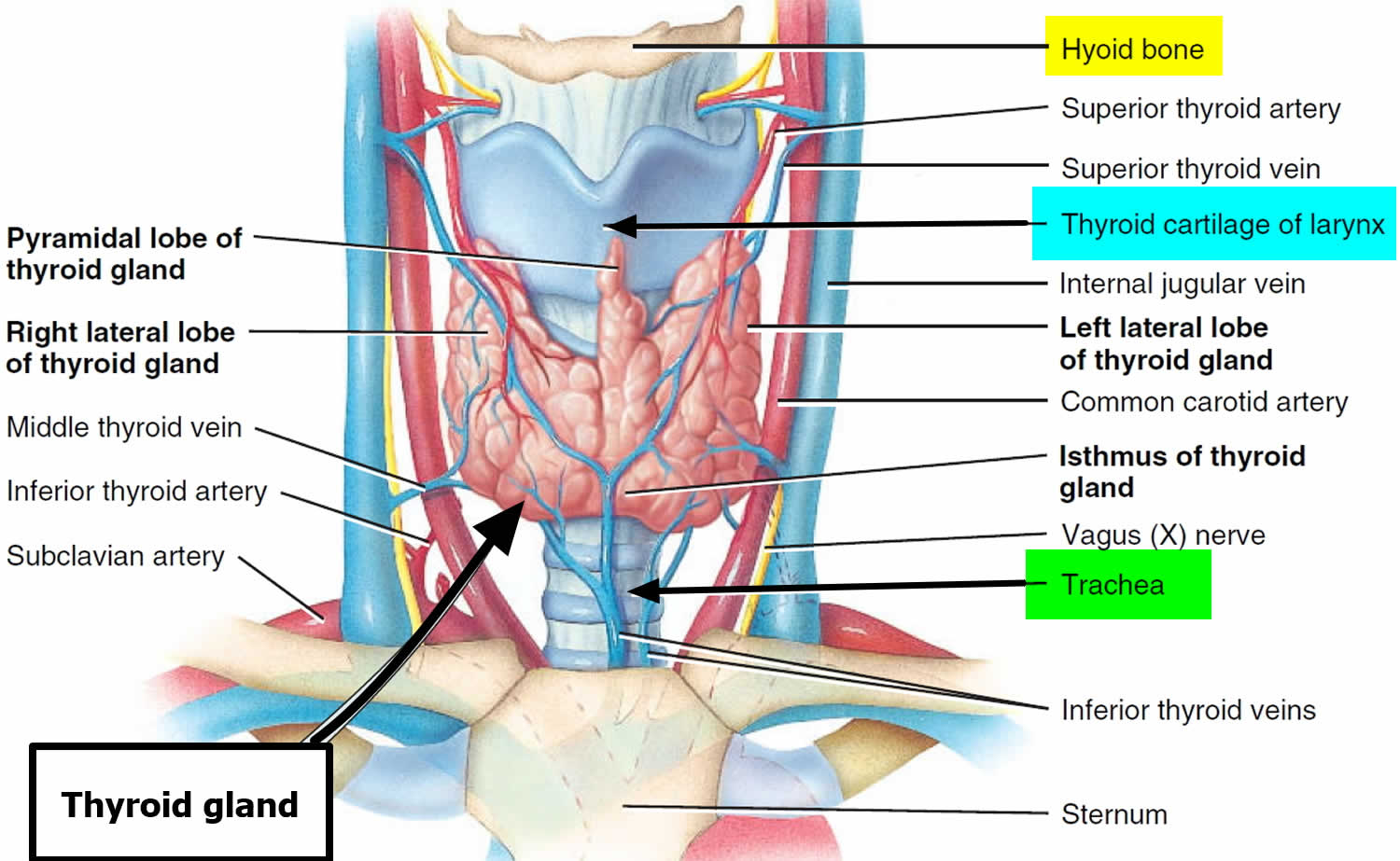
Figure 2. Thyroid gland location
Figure 3. Thyroid gland anatomy
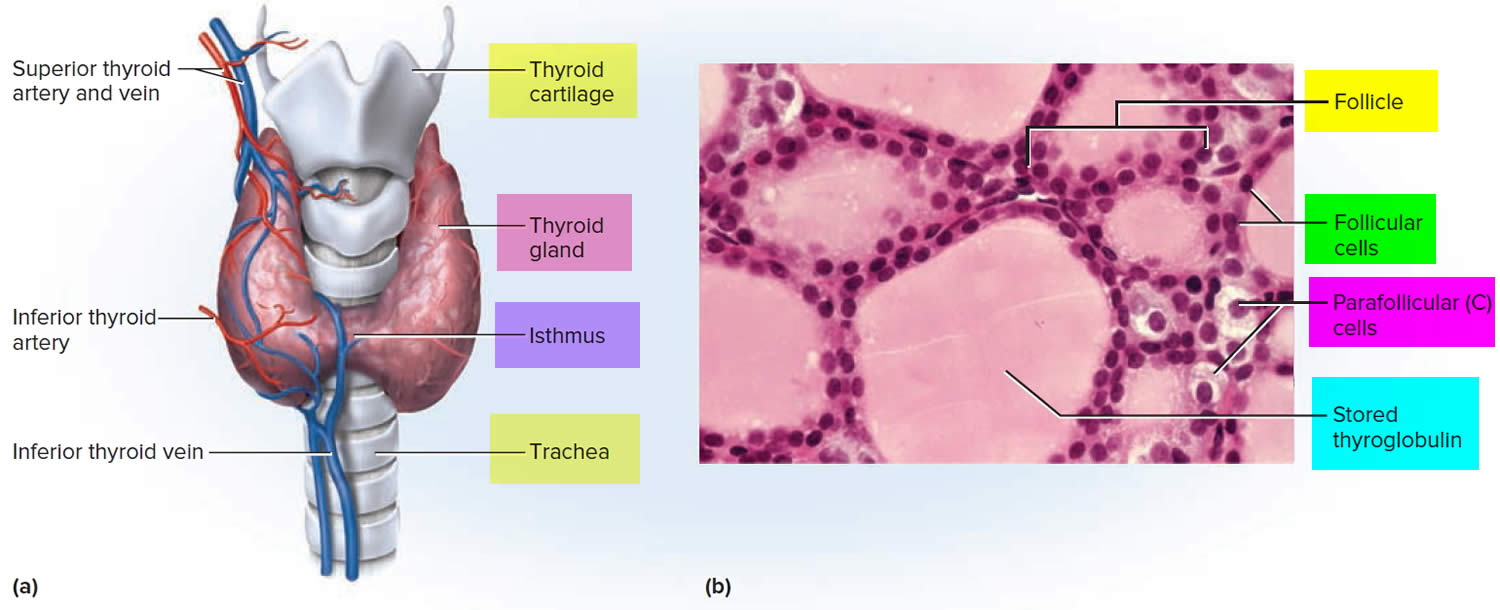
Footnote: (a) Gross anatomy, anterior view. (b) Histology, showing the saccular thyroid follicles (the source of thyroid hormone) and nests of C cells (the source of calcitonin).
What does the thyroid gland do?
Formation, storage, and release of thyroid hormones
The thyroid gland is the only endocrine gland that stores its secretory product in large quantities—normally about a 100-day supply. Synthesis and secretion of triiodothyronine (T3) and thyroxine or tetraiodothyronine (T4) occurs as follows:
- Iodide trapping. Thyroid follicular cells trap iodide ions (I −) by actively transporting them from the blood into the cytosol. As a result, the thyroid gland normally contains most of the iodide in the body.
- Synthesis of thyroglobulin. While the follicular cells are trapping I −, they are also synthesizing thyroglobulin (TGB), a large glycoprotein that is produced in the rough endoplasmic reticulum, modified in the Golgi complex, and packaged into secretory vesicles. The vesicles then undergo exocytosis, which releases thyroglobulin into the lumen of the follicle.
- Oxidation of iodide. Some of the amino acids in thyroglobulin are tyrosines that will become iodinated. However, negatively charged iodide (I −) ions cannot bind to tyrosine until they undergo oxidation (removal of electrons) to iodine: I −→ I. As the iodide ions are being oxidized, they pass through the membrane into the lumen of the follicle.
- Iodination of tyrosine. As iodine atoms (I) form, they react with tyrosines that are part of thyroglobulin molecules. Binding of one iodine atom yields monoiodotyrosine (T1), and a second iodination produces diiodotyrosine (T2). The thyroglobulin with attached iodine atoms, a sticky material that accumulates and is stored in the lumen of the thyroid follicle, is termed colloid.
- Coupling of monoiodotyrosine (T1) and diiodotyrosine (T2). During the last step in the synthesis of thyroid hormone, two diiodotyrosine (T2) molecules join to form thyroxine (T4) or one T1 and one T2 join to form triiodothyronine (T3).
- Pinocytosis and digestion of colloid. Droplets of colloid reenter follicular cells by pinocytosis and merge with lysosomes. Digestive enzymes in the lysosomes break down thyroglobulin, cleaving off molecules of triiodothyronine (T3) and thyroxine (T4).
- Secretion of thyroid hormones. Because T3 and T4 are lipid soluble, they diffuse through the plasma membrane into interstitial fluid and then into the blood. T4 normally is secreted in greater quantity than T3, but T3 is several times more potent. Moreover, after T4 enters a body cell, most of it is converted to T3 by removal of one iodine.
- Transport thyroid hormones in the blood. More than 99% of both the T3 and the T4 combine with transport proteins in the blood, mainly thyroxine binding globulin (TBG).
Figure 4. Thyroid hormones
Actions of thyroid hormones
Because most body cells have receptors for thyroid hormones, triiodothyronine (T3) and thyroxine (T4) affect tissues throughout the body. Thyroid hormones act on their target cells mainly by inducing gene transcription and protein synthesis. The newly formed proteins in turn carry out the cellular response.
Functions of thyroid hormones include the following:
- Increase basal metabolic rate. Thyroid hormones raise the basal metabolic rate (BMR), the rate of energy expenditure under standard or basal conditions (awake, at rest, and fasting). When basal metabolic rate increases, cellular metabolism of carbohydrates, lipids, and proteins increases. Thyroid hormones increase BMR in several ways: (1) They stimulate synthesis of additional Na+/K+ ATPases, which use large amounts of ATP to continually eject sodium ions (Na+) from cytosol into extracellular fluid and potassium ions (K+) from extracellular fluid into cytosol; (2) they increase the concentrations of enzymes involved in cellular respiration, which increases the breakdown of organic fuels and ATP production; and (3) they increase the number and activity of mitochondria in cells, which also increases ATP production. As cells produce and use more ATP, basal metabolic rate increases, more heat is given off and body temperature rises, a phenomenon called the calorigenic effect. In this way, thyroid hormones play an important role in the maintenance of normal body temperature. Normal mammals can survive in freezing temperatures, but those whose thyroid glands have been removed cannot.
- Enhance actions of catechlolamines. Thyroid hormones have permissive effects on the catecholamines (epinephrine and norepinephrine) because they up-regulate β-adrenergic receptors. Catecholamines bind to β-adrenergic receptors, promoting sympathetic responses. Therefore, symptoms of excess levels of thyroid hormone include increased heart rate, more forceful heartbeats, and increased blood pressure.
- Regulate development and growth of nervous tissue and bones. Thyroid hormones are necessary for the development of the nervous system: They promote synapse formation, myelin production, and growth of dendrites. Thyroid hormones are also required for growth of the skeletal system: They promote formation of ossification centers in developing bones, synthesis of many bone proteins, and secretion of growth hormone (GH) and insulin-like growth factors (IGFs). Deficiency of thyroid hormones during fetal development, infancy, or childhood causes severe mental retardation and stunted bone growth.
Control of thyroid hormone secretion
Thyrotropin-releasing hormone (TRH) from the hypothalamus and thyroid-stimulating hormone (TSH) from the anterior pituitary stimulate secretion of thyroid hormones, as shown in Figure 5:
- Low blood levels of T3 and T4 or low metabolic rate stimulate the hypothalamus to secrete thyrotropin-releasing hormone (TRH).
- Thyrotropin-releasing hormone (TRH) enters the hypothalamic–hypophyseal portal system and flows to the anterior pituitary, where it stimulates thyrotrophs to secrete thyroid stimulating hormone (TSH).
- Thyroid stimulating hormone (TSH) stimulates virtually all aspects of thyroid follicular cell activity, including iodide trapping, hormone synthesis and secretion, and growth of the follicular cells.
- The thyroid follicular cells release T3 and T4 into the blood until the metabolic rate returns to normal.
- An elevated level of T3 inhibits release of TRH and TSH (negative feedback inhibition).
Conditions that increase ATP demand—a cold environment, hypoglycemia, high altitude, and pregnancy—increase the secretion of the thyroid hormones.
Figure 5. Control of thyroid hormone secretion
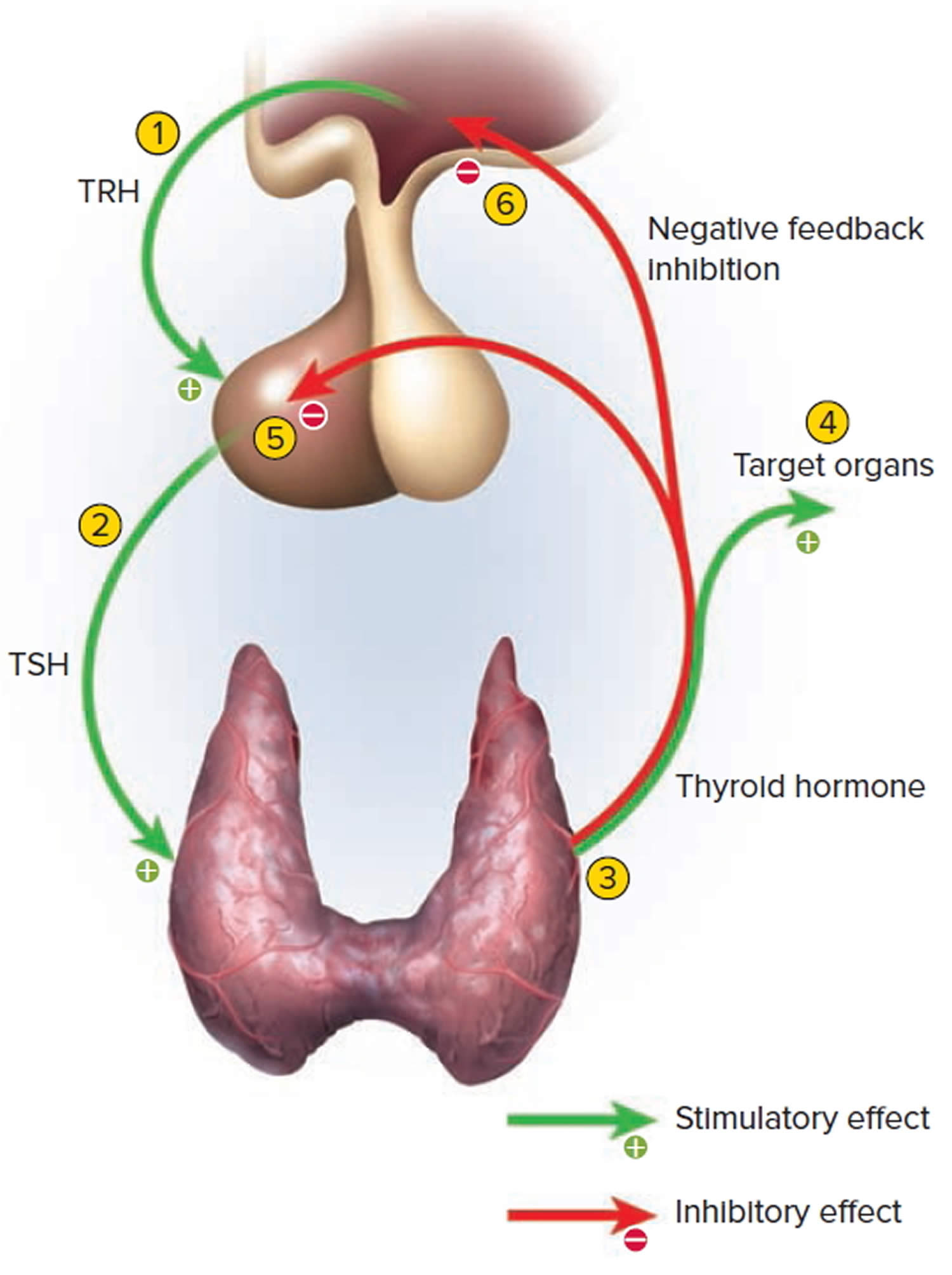
Footnote: Negative Feedback Inhibition of the Anterior Pituitary Gland by the Thyroid Gland
Control of calcium balance
The hormone produced by the parafollicular cells of the thyroid gland is calcitonin. Calcitonin can decrease the level of calcium in the blood by inhibiting the action of osteoclasts, the cells that break down bone extracellular matrix. The secretion of calcitonin is controlled by a negative feedback system (see Figure 7).
Calcitonin is produced by C cells (clear cells) of the thyroid gland. It is secreted when the blood calcium concentration rises too high, and it lowers the concentration by two principal mechanisms:
- Osteoclast inhibition. Within 15 minutes after it is secreted, calcitonin reduces osteoclast activity by as much as 70%, so osteoclasts liberate less calcium from the skeleton.
- Osteoblast stimulation. Within an hour, calcitonin increases the number and activity of osteoblasts, which deposit calcium into the skeleton.
Calcitonin plays an important role in children but has only a weak effect in most adults. The osteoclasts of children are highly active in skeletal remodeling and release 5 g or more of calcium into the blood each day. By inhibiting this activity, calcitonin can significantly lower the blood calcium level in children. In adults, however, the osteoclasts release only about 0.8 g of calcium per day. Calcitonin cannot change adult blood calcium very much by suppressing this lesser contribution. Calcitonin deficiency is not known to cause any adult disease. Calcitonin may, however, inhibit bone loss in pregnant and lactating women. Miacalcin, a calcitonin extract derived from salmon that is 10 times more potent than human calcitonin, is prescribed to treat osteoporosis.
Figure 6. Hormonal control of calcium balance
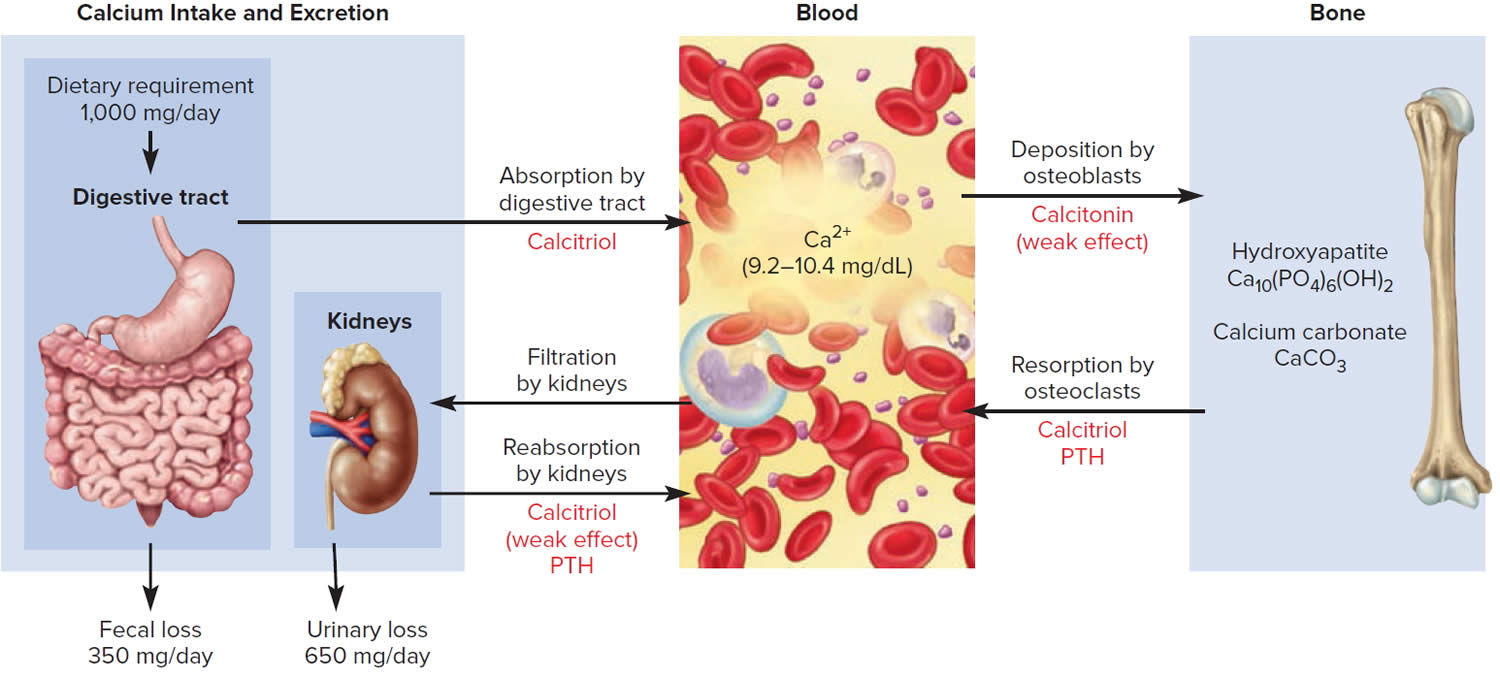
Footnote: The central panel represents the blood reservoir of calcium and shows its normal (safe) range. Calcitriol and Parathyroid Hormone (PTH) regulate calcium exchanges between the blood and the small intestine and kidneys (left). Calcitonin, calcitriol, and Parathyroid Hormone (PTH) regulate calcium exchanges between blood and bone (right).
Thyroid antibodies
Antibodies are proteins produced by your immune system in response to invasion by foreign proteins (antigens) — such as bacteria, fungi, parasites, viruses and toxins — and remove them from your body. Antibodies help protect you from viruses and bacteria. Thyroid antibodies develop when your immune system mistakenly attacks your thyroid cells, tissues or proteins. This leads to thyroid inflammation (thyroiditis), thyroid tissue damage and/or disruption of thyroid function. These antibodies attacking your body are also known as autoantibodies or antithyroid antibodies. These autoantibodies or antithyroid antibodies cause autoimmune thyroid disorders (a disease in which your body’s immune system mistakenly attacks healthy cells in your thyroid), such as Graves’ disease and Hashimoto’s thyroiditis.
If your initial thyroid test results show signs of a thyroid problem, and if there is a suspicion of autoimmune thyroid disease, your doctor may order one or more thyroid antibody tests (see Table 1). Antibody tests are used to confirm the diagnosis of autoimmune thyroid diseases. Some people will test positive for more than one type of thyroid antibody.
In people with subclinical thyroid disease, the presence of antibodies can indicate the person may go on to develop full-blown thyroid disease in the future, but that treatment is not yet required. Positive antibodies can also be present in people without thyroid disease.
Understanding the underlying cause of thyroid dysfunction can help your doctor plan the best course of treatment.
Table 1. Thyroid antibodies
| Antibodies | What do they indicate? |
|---|---|
| Thyroid peroxidase antibodies (TPOAb) | Raised in Hashimoto’s thyroiditis (or autoimmune thyroiditis) and sometimes raised in Graves’ disease |
| Thyroglobulin antibodies (Tg Ab) – antibodies directed against the thyroglobulin (a protein present in the thyroid gland), from which thyroid hormones are produced | May be measured as part of the monitoring of people previously treated for thyroid cancer. Also sometimes raised in Hashimoto’s thyroiditis |
| Thyroid stimulating hormone receptor antibodies (TRAb). TRAb is potentially stimulatory and blocking to the thyroid gland. | Raised in Graves’ disease |
| Thyroid Stimulating Immunoglobulin (TSI) antibody specific to Graves’ disease. It is a stimulatory antibody and the one that causes an overactive thyroid gland. | May be raised in Graves’ disease. This is not routinely tested and used mainly as a research tool. |
Footnote: Thyroid antibody tests are used to diagnose autoimmune thyroid disease. Thyroid antibody tests may also be used to determine whether your mild hypothyroidism (underactive thyroid) is likely to get worse over time, to evaluate the risk to the fetus in pregnant individuals with thyroid disease, to estimate the risk of relapse after treatment for Graves’ disease and to monitor if you have been previously treated for thyroid cancer 7.
[Source 8 ]Postpartum thyroiditis causes
Postpartum thyroiditis is an autoimmune disorder where your body’s immune system creates antibodies to thyroid peroxidase (thyroid peroxidase antibodies [TPOAb]) that attack your thyroid cells as if they were bacteria, viruses or some other foreign body. It is not known why certain people make anti-thyroid antibodies, although this tends to run in families. Scientists are still researching what causes the antibodies to attack after a pregnancy. A popular theory is that you’re more likely to get diagnosed if you had an underlying autoimmune condition (that you didn’t know about) before pregnancy. An autoimmune condition happens when antibodies attack healthy cells and tissue.
Postpartum thyroiditis is also known as autoimmune lymphocytic thyroiditis with lymphocytic infiltration within the thyroid gland 1. Histological features of postpartum thyroiditis are similar to Hashimoto thyroiditis, and both are associated with HLA-D and HLA-B haplotypes 1. These findings indicate the importance of inherited risk factors 9, 10.
The presence of thyroid peroxidase antibodies (TPOAb) is also seen in other autoimmune thyroid diseases such as Graves disease and Hashimoto thyroiditis. The level of thyroid peroxidase antibodies (TPOAb) reflects the severity of the infiltration of lymphocytes within the thyroid gland. Thyroid peroxidase antibodies (TPOAb) are complement-fixing, which subsequently induce antibody-dependent cell-mediated cytotoxicity 11.
You’re more likely to develop postpartum thyroiditis if you 5:
- Have had postpartum thyroiditis before (20% of women will have recurrence of thyroiditis with additional pregnancies).
- Have type 1 diabetes (a type of autoimmune condition).
- Have a personal or family history of thyroid disease.
- Had anti-thyroid antibodies before you were pregnant (you may not have known because you didn’t notice symptoms).
- Chronic viral hepatitis.
Postpartum thyroiditis pathophysiology
The inflammatory process in postpartum thyroiditis initiates with the presence of thyroid antibodies (thyroid peroxidase antibodies [TPOAb] and thyroglobulin antibodies [TgAb]), activation of the complement cascade, increased levels of IgG1, lymphocyte abnormalities, increased activity of NK cells, and specific HLA haplotypes 1. The inflammatory process activates the proteolysis of the thyroglobulin within the thyroid follicles. The result is the destruction of the thyroid follicles and releasing significant amounts of thyroxine (T4) and triiodothyronine (T3) into the blood and subsequently hyperthyroid state 1. This hyperthyroid state is transient and lasts until all thyroglobulin storages released into circulation and no more thyroglobulin left within the follicles. During the hyperthyroid state, the synthesis of new hormones becomes shutdown because excessive T4/T3 in circulation causes downregulation of TSH secretion. Synthesis of thyroid hormones will be resumed once all inflammatory process subsides 1.
Postpartum thyroiditis symptoms
Postpartum thyroiditis usually unfolds in phases:
- Phase 1: The inflammation causes your thyroid to produce and release too many hormones (hyperthyroidism). This phase usually happens between one to six months after a pregnancy. It may last from one week up to three months.
- Most people don’t notice symptoms in the first phase, hyperthyroidism. If you do experience symptoms, they usually involve body functions (like metabolism) being “hyper” or sped up. They may include:
- Anxiety
- Hair loss
- Unexplained weight loss
- Rapid heart rate (tachycardia)
- Hypersensitivity to heat.
- Most people don’t notice symptoms in the first phase, hyperthyroidism. If you do experience symptoms, they usually involve body functions (like metabolism) being “hyper” or sped up. They may include:
- Phase 2: Your thyroid doesn’t produce or release enough hormones (hypothyroidism). This phase usually takes place four to eight months after pregnancy. It can last as long as a year.
- It isn’t until the second phase, hypothyroidism, that most people notice symptoms. Symptoms of hypothyroidism usually involve body functions (like metabolism) slowing down. They may include:
- Fatigue
- Weight gain
- Depression
- Dry skin
- Constipation
- Muscle pain
- Not having enough breast (chest) milk come in
- Hypersensitivity to cold.
- It isn’t until the second phase, hypothyroidism, that most people notice symptoms. Symptoms of hypothyroidism usually involve body functions (like metabolism) slowing down. They may include:
- Phase 3: Your thyroid usually returns to producing normal hormone levels.
Not everyone experiences all the phases in order, though. Some people skip over the hypothyroid phase. They have hyperthyroidism, and then their thyroid function returns to normal.
The classic description of postpartum thyroiditis includes thyrotoxicosis also known as overactive thyroid (high thyroid hormone levels in the blood) followed by hypothyroidism also known as underactive thyroid (low thyroid hormone levels in the blood). Not all women appear to go through both phases; approximately 1/3 of patients will manifest both, while 1/3 of patients will have only a overactive thyroid (thyrotoxic) or only a hypothyroid (underactive thyroid) phase.
The thyrotoxic (overactive thyroid) phase occurs 1 to 4 months after delivery of a child and lasts for 1 to 3 months. The thyrotoxic (overactive thyroid) phase is associated with symptoms including anxiety, insomnia, palpitations (fast heart rate), fatigue, weight loss, and irritability. Since these symptoms may often be attributed to changes after delivery and the stress of having a new baby, the thyrotoxic (overactive thyroid) phase of post-partum thyroiditis is often overlooked.
It is much more common for women to present during the hypothyroid (underactive thyroid) phase. This typically occurs 4 to 8 months after delivery of a baby and may last up to 9 to 12 months. Typical hypothyroid (underactive thyroid) symptoms include fatigue, weight gain, constipation, dry skin, depression and poor exercise tolerance. Most women will regain normal thyroid function within 12 to 18 months after the onset of symptoms. However, approximately 20% of those that go into a hypothyroid phase will remain hypothyroid. Women who remain hypothyroid will need hormone replacement therapy to make up for low thyroid hormone levels.
Postpartum thyroiditis diagnosis
If you have any signs or symptoms that suggest you might have thyroid dysfunction, your doctor will want to know your complete medical history. You will be asked questions about your possible risk factors, symptoms, and any other health problems or concerns. If someone in your family has had thyroid problem, it is important to tell your doctor, as you might be at high risk for this disease.
A blood test is usually enough to diagnose postpartum thyroiditis. It can also help exclude similar diagnoses, like Graves’ disease or Hashimoto’s thyroiditis.
Testing thyroid function
To determine if thyrotoxicosis (overactive thyroid) or hypothyroidism (underactive thyroid) is the cause of your symptoms, your doctor will order blood tests that may include the following:
- Thyroid stimulating hormone (TSH) test. Thyroid-stimulating hormone (TSH or thyrotropin) is produced by the pituitary gland. When the pituitary detects low thyroid hormones in the blood, it sends thyroid-stimulating hormone (TSH) to the thyroid to prompt an increase in thyroid hormone production. High TSH levels in the blood indicates hypothyroidism.
- Thyroxine (T4) tests. The main thyroid hormone is thyroxine (T4). A low blood level of thyroxine (T4) confirms the findings of a high TSH level and indicates the problem is within the thyroid itself.
- Thyroglobulin (Tg). Thyroglobulin (Tg) is a protein made by the thyroid gland. Thyroglobulin (Tg) plays a key role in helping the body create, store and release thyroid hormones. Thyroglobulin (Tg) may be present in the blood when the thyroid has been damaged. Some doctors may check thyroglobulin (Tg) levels when diagnosing hyperthyroidism and hypothyroidism, thyroid disorders that are not thyroid cancer. If you recently had surgery for thyroid cancer, your doctor may measure thyroglobulin (Tg) levels to determine whether your treatment successfully removed all of your thyroid cells, including noncancerous and cancerous cells. This postoperative evaluation of thyroglobulin (Tg) levels is usually ordered four to six weeks following surgery. The presence of detectable thyroglobulin (Tg), particularly a rising thyroglobulin level, may give an early warning of a recurrence of thyroid cancer.
Postpartum thyroiditis antibodies
More than one disease process can lead to thyrotoxicosis (overactive thyroid) or hypothyroidism (underactive thyroid). To determine if postpartum thyroiditis is the cause of thyrotoxicosis (overactive thyroid) or hypothyroidism, your doctor will order an antibody test.
The intended purpose of an antibody is to flag disease-causing foreign agents that need to be destroyed by other actors in the immune system. In an autoimmune disorder, the immune system produces rogue antibodies that target healthy cells or proteins in the body.
Usually in postpartum thyroiditis, the immune system produces an antibody to thyroid peroxidase (TPOAb), a protein that plays an important part in thyroid hormone production.
Thyroid peroxidase antibodies (TPOAb)
Thyroid peroxidase antibodies (TPOAb) may be checked in patients with a high thyroid-stimulating hormone (TSH or thyrotropin) to help establish the underlying cause. Postpartum thyroiditis is an autoimmune disorder where your body’s immune system creates antibodies to thyroid peroxidase (thyroid peroxidase antibodies [TPOAb]) that attack your thyroid cells. Postpartum thyroiditis is also known as destructive thyroiditis with lymphocytic infiltration within the thyroid gland 1.
The presence of thyroid peroxidase antibodies (TPOAb) is also seen in other autoimmune thyroid diseases such as Graves disease and Hashimoto thyroiditis. The level of thyroid peroxidase antibodies (TPOAb) reflects the severity of the infiltration of lymphocytes within the thyroid gland. Thyroid peroxidase antibodies (TPOAb) are complement-fixing, which subsequently induce antibody-dependent cell-mediated cytotoxicity 11. Almost all patients with Hashimoto’s thyroiditis have high levels of thyroid peroxidase antibodies (TPOAb). If thyroid peroxidase antibodies (TPOAb) are negative, it means you may not have a thyroid disorder and that the high thyroid-stimulating hormone (TSH) may resolve spontaneously, or there is an underlying thyroid disorder caused by another factor (e.g. following a viral infection or due to prescribed medication).
It is normally only necessary to measure thyroid peroxidase antibodies (TPOAb) once when trying to establish the cause of the thyroid disorder. Thyroid peroxidase antibodies (TPOAb) are found in more than 90% of people with autoimmune hypothyroidism and also in about 10% of people without a thyroid disorder where they may be ‘markers’ of autoimmunity. This means they may be more likely to develop autoimmune disease in the future.
Thyroid stimulating antibodies (TRAb)
Thyroid stimulating antibodies (TRAb) also known as thyrotropin receptor antibodies (TRAb) bind to the receptors on thyroid cells normally activated by TSH. In Graves’ disease, an antibody called thyroid-stimulating immunoglobulin (TSI) binds to the TSH receptor and mimics the action of TSH. This causes constant stimulation of the thyroid gland, prompting it to release too much thyroid hormone.
Thyroglobulin antibodies (TgAb)
Thyroglobulin antibodies (TgAb) are directed against the thyroglobulin (Tg) molecule and are found in approximately 10% of the general population; they can be raised in people with Hashimoto’s thyroiditis.
Where thyroglobulin antibodies (TgAb) are present it can affect the accuracy of the measurement of thyroglobulin (Tg) and so additional means need to be used to monitor people who have had treatments for thyroid cancer. Thyroglobulin antibodies (TgAb) generally do not add anything to thyroid peroxidase antibody (TPOAb) results in the assessment of people with a raised TSH.
Postpartum thyroiditis differential diagnosis
Postpartum thyroiditis differential diagnosis may include:
- Graves disease
- Hashimoto thyroiditis
- Postpartum mood disorder
Postpartum thyroiditis treatment
Postpartum thyroiditis treatment depends on the phase of thyroiditis and degree of symptoms that you have. Treatment depends on whether you’re experiencing hyperthyroidism or hypothyroidism. Most women have mild symptoms and don’t need treatment unless symptoms worsen. Mothers presenting with thyrotoxicosis may be treated with beta blockers to decrease symptoms such as heart palpitations (feelings of having a fast-beating, fluttering or pounding heart) and tremors. As symptoms improve, the medication can be reduced and stopped since the thyrotoxic phase is temporary. Antithyroid medications are not used for the thyrotoxic phase since the thyroid is not overactive.
The hypothyroid phase may be treated with thyroid hormone replacement. If the hypothyroidism is mild, and the patient has few, if any, symptoms, no therapy may be necessary.
Hypothyroidism associated with postpartum thyroiditis is usually treated with a synthetic hormone called levothyroxine (Levoxyl, Synthroid, others). The synthetic hormone works like the thyroxine (T4) hormone naturally produced by your thyroid. The treatment goal is to restore and maintain adequate thyroxine (T4) hormone levels and improve symptoms of hypothyroidism. If thyroid hormone therapy is started, treatment should be continued for approximately 6 to 12 months and then reduced to see if thyroid hormone is required permanently. You’ll probably be able to taper off the medication as your thyroid returns to normal. Your doctor will monitor your thyroid levels during treatment every six to eight weeks 12.
Certain medications, supplements and foods may affect your ability to absorb levothyroxine (synthetic thyroxine). It may be necessary to take levothyroxine at least four hours before these substances. Talk to your doctor about any of the following:
- Soy products
- High-fiber foods
- Iron supplements, including multivitamins that contain iron
- Cholestyramine (Prevalite), a medication used to lower blood cholesterol levels
- Aluminum hydroxide, which is found in some antacids
- Sucralfate, an ulcer medication
- Calcium supplements.
Selenium supplementation has been explored for its possible anti-inflammatory effect in autoimmune thyroiditis 13. However, clinical trials of selenium supplementation in pregnancy have shown mixed results 14. Therefore, selenium supplementation for prevention or treatment of postpartum thyroiditis is currently not recommended 12.
Postpartum thyroiditis prognosis
Postpartum thyroiditis is usually temporary. Seventy to 80% of women eventually no longer need medication because their thyroid starts making hormones at normal levels again within 12 to 18 months. The other 20% to 30% cases with postpartum thyroiditis stay in the hypothyroid state one year postpartum 6. Women who are positive for serum thyroid peroxidase antibodies (TPOAb) are at increased risk of developing permanent hypothyroidism after postpartum thyroiditis 15. They’ll need thyroid hormone replacement therapy long-term.
Postpartum hypothyroidism also makes you more likely to develop future thyroid issues, including hypothyroidism or an enlarged thyroid gland (goiter). Even if your thyroid returns to normal, your doctor will likely need to get regular TSH tests to monitor your thyroid hormone function.
If postpartum thyroiditis does not evolved into permanent hypothyroidism, it tends to recur 3. The recurrence risk of postpartum thyroiditis in a patient with the previous history of postpartum thyroiditis is reported at up to 70% 16, 17, 18.
- Naji Rad S, Deluxe L. Postpartum Thyroiditis. [Updated 2023 Jun 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557646[↩][↩][↩][↩][↩][↩][↩][↩]
- Epp R, Malcolm J, Jolin-Dahel K, Clermont M, Keely E. Postpartum thyroiditis. BMJ. 2021 Mar 3;372:n495. https://www.bmj.com/content/372/bmj.n495.long[↩][↩]
- Stagnaro-Green A. Approach to the patient with postpartum thyroiditis. J Clin Endocrinol Metab. 2012 Feb;97(2):334-42. doi: 10.1210/jc.2011-2576[↩][↩]
- Benvenga S, Di Bari F, Vita R, et al. Relatively high rate of postpartum thyroiditis in the Straits of Messina area. Predictivity of both postpartum thyroiditis and permanent hypothyroidism by performing, in the first trimester of gestation, thyroid ultrasonography and measurement of serum thyroperoxidase and thyroglobulin autoantibodies. J Clin Transl Endocrinol. 2018 Nov 23;15:12-18. doi: 10.1016/j.jcte.2018.11.004. Erratum in: J Clin Transl Endocrinol. 2020 Dec 17;23:100246[↩]
- Leslie De Groot, Marcos Abalovich, Erik K, et al. Management of Thyroid Dysfunction during Pregnancy and Postpartum: An Endocrine Society Clinical Practice Guideline, The Journal of Clinical Endocrinology & Metabolism, Volume 97, Issue 8, 1 August 2012, Pages 2543–2565, https://doi.org/10.1210/jc.2011-2803[↩][↩]
- Stagnaro-Green A. Clinical review 152: Postpartum thyroiditis. J Clin Endocrinol Metab. 2002 Sep;87(9):4042-7. doi: 10.1210/jc.2002-020524[↩][↩]
- Thyroid Antibodies Test. https://www.testing.com/tests/thyroid-antibodies[↩]
- Thyroid antibodies explained. https://www.btf-thyroid.org/thyroid-antibodies-explained[↩]
- LiVolsi VA. Postpartum thyroiditis. The pathology slowly unravels. Am J Clin Pathol. 1993 Sep;100(3):193-5. doi: 10.1093/ajcp/100.3.193[↩]
- Kologlu M, Fung H, Darke C, Richards CJ, Hall R, McGregor AM. Postpartum thyroid dysfunction and HLA status. Eur J Clin Invest. 1990 Feb;20(1):56-60. doi: 10.1111/j.1365-2362.1990.tb01791.x[↩]
- Prummel MF, Wiersinga WM. Thyroid peroxidase autoantibodies in euthyroid subjects. Best Pract Res Clin Endocrinol Metab. 2005 Mar;19(1):1-15. doi: 10.1016/j.beem.2004.11.003[↩][↩]
- Alexander EK, Pearce EN, Brent GA, Brown RS, Chen H, Dosiou C, Grobman WA, Laurberg P, Lazarus JH, Mandel SJ, Peeters RP, Sullivan S. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid. 2017 Mar;27(3):315-389. doi: 10.1089/thy.2016.0457. Erratum in: Thyroid. 2017 Sep;27(9):1212.[↩][↩]
- De Leo S, Pearce EN. Autoimmune thyroid disease during pregnancy. Lancet Diabetes Endocrinol. 2018 Jul;6(7):575-586. doi: 10.1016/S2213-8587(17)30402-3[↩]
- Hubalewska-Dydejczyk A, Duntas L, Gilis-Januszewska A. Pregnancy, thyroid, and the potential use of selenium. Hormones (Athens). 2020 Mar;19(1):47-53. doi: 10.1007/s42000-019-00144-2[↩]
- Premawardhana LD, Parkes AB, Ammari F, John R, Darke C, Adams H, Lazarus JH. Postpartum thyroiditis and long-term thyroid status: prognostic influence of thyroid peroxidase antibodies and ultrasound echogenicity. J Clin Endocrinol Metab. 2000 Jan;85(1):71-5. doi: 10.1210/jcem.85.1.6227[↩]
- Pearce EN Management of thyrotoxicosis: preconception, pregnancy, and the postpartum period. Endocr Pract. 2019 Jan;25(1):62-68. doi: 10.4158/EP-2018-0356[↩]
- Stagnaro-Green A. Postpartum thyroiditis. Best Pract Res Clin Endocrinol Metab. 2004 Jun;18(2):303-16. doi: 10.1016/j.beem.2004.03.008[↩]
- Nicholson WK, Robinson KA, Smallridge RC, Ladenson PW, Powe NR. Prevalence of postpartum thyroid dysfunction: a quantitative review. Thyroid. 2006 Jun;16(6):573-82. doi: 10.1089/thy.2006.16.573[↩]





{kind=link}