Contents
Methamphetamine
Methamphetamine also known as N-methylamphetamine, meth, crystal meth, crank, glass, ice, speed, uppers, Tina, Christine or Yaba is a is a highly addictive central nervous system (brain and spinal cord) stimulant that is mainly used as a recreational or performance-enhancing drug and less commonly as a second-line treatment for attention-deficit hyperactivity disorder (ADHD), narcolepsy and obesity 1, 2, 3, 4, 5. Methamphetamine has powerful addictive properties and, therefore, has devastating effects on health and other aspects of life of the people who abuse it 5. Due to methamphetamine’s high potential for abuse, methamphetamine is a Schedule 2 Drug under the Controlled Substances Act with prescription methamphetamine Desoxyn® can only be prescribed for attention deficit hyperactivity disorder (ADHD), extreme obesity, or narcolepsy 6, 7. Methamphetamine works in the treatment of attention-deficit hyperactivity disorder (ADHD) by increasing attention and decreasing restlessness in children and adults who are overactive, cannot concentrate for very long, or are easily distracted and impulsive. Methamphetamine (Desoxyn) is used as part of a total treatment program that also includes social, educational, and psychological treatment. Methamphetamine (Desoxyn) is also used for a limited period of time (a few weeks) along with a reduced calorie diet and an exercise plan for weight loss in obese people who are unable to lose weight through diet and exercise alone.
On the other hand, a strong form of methamphetamine is being illegally sold on the streets 8, 9, 3, 10, 11, 12. People can smoke methamphetamine or snort the powder up their nose. They can also inject methamphetamine into their bodies with a needle. People use the crystal version of methamphetamine by smoking it in a glass pipe. A dangerous form of methamphetamine ingestion called “parachuting,” in which drugs are wrapped in toilet paper or plastic wrap to delay absorption, is becoming more commonplace 13. Someone using methamphetamine may experience a temporary sense of heightened feeling of wellness (euphoria), alertness, and energy that is most often called a “rush”. This is because meth increases the amount of dopamine, a natural chemical, in your brain. Dopamine is involved in body movement, motivation, and reinforcing rewarding behaviors. Methamphetamine rapidly releases high levels of dopamine into reward areas of the brain, making people want to continue to use meth. Methamphetamine not only changes how your brain works, but also speeds up your body’s systems to dangerous, sometimes lethal levels by increasing blood pressure and heart and respiratory rates, sweating, restlessness, dry mouth, elevated body temperature, and large, wide pupils. People who repeatedly use meth may also experience anxiety, paranoia, aggression, hallucinations, and mood disturbances. Some people take methamphetamine again and again over a long period of time. This is because the high that people feel from taking methamphetamine doesn’t last long. This is called a binge. Using methamphetamine as a recreational or performance-enhancing drug can cause memory loss, aggression, psychotic behavior, damage to the cardiovascular system, malnutrition, and severe dental problems. Methamphetamine misuse has also been shown to contribute to increased transmission of infectious diseases, such as hepatitis and HIV/AIDS 14.
Over the past decade, all regions of the United States have experienced a significant increase in the number of people using methamphetamine and emergency department visits. According to data from the 2021 National Survey on Drug Use and Health, more than 16.8 million people aged 12 or older (6% of the population) used methamphetamine at least once during their lifetime 15. In 2021, an estimated 2.5 million people reported using methamphetamine in the past 12 months 15 and it remains one of the most commonly misused stimulant drugs in the world 16. In the US, methamphetamine abusers are predominantly white males in their 30s and 40s 2. More recently, methamphetamine abuse epidemic has been described in adolescents 2. Addiction to methamphetamine is one of the most difficult to cure as there is no agent that can prevent abstinence 17, 18. Methamphetamine abusers tend to be dishonest and mistrustful of health care professionals when describing their drug history with the majority of abusers continue to abuse methamphetamine until they run afoul of the legal system 13, 19, 20. The majority of methamphetamine abusers come from a subculture that is involved in the manufacture of the drug 21, 22, 23. In the United States, there were greater than 150,000 emergency department visits for toxicity from methamphetamine in 2011 based on data from the Substance Abuse and Mental Health Services Administration.
Methamphetamine short-term effects:
- Decreased appetite
- Nausea
- Psychosis
- Tachycardia
- Hypertension
- Increased body temperature
- Panic attack
- Mydriasis (dilation of pupils)
- Disturbed sleep patterns
- Violent, bizarre, and erratic behavior
- Hallucinations and irritability
- Seizures, convulsions, and death from high doses 24, 25, 26, 27
Methamphetamine long-term effects:
- Long-lasting damage to the blood vessel of the heart and brain
- Lung, liver, and kidney damage
- Hypertension that can lead to heart attacks, strokes, and death
- Severe tooth degeneration
- In cases where the drug was sniffed, destruction of soft tissues in the nose
- In cases where the drug was smoked, respiratory problems
- In cases where the drug was injected, infectious diseases, cellulitis, and abscesses
- Weight loss and malnutrition
- Disorientation, apathy, confusion, and exhaustion
- Delusions
- Delusional behavior
- Extreme paranoia
- Major mood swings
- Insomnia (severe inability to sleep)
- Severe psychological dependence
- Psychosis
- Depression
- Damage to the brain structure similar to Alzheimer disease, epilepsy, and stroke
- Missing and rotted teeth (called “meth mouth”)
- Repeated infections
- Severe weight loss
- Skin sores (abscesses or boils).
Prescription methamphetamine (Desoxyn) comes as a tablet to take by mouth. If your child is taking methamphetamine for ADHD, it is usually taken one or two times daily. If you are taking methamphetamine for weight management, it is usually taken 30 minutes before meal(s). Prescription methamphetamine (Desoxyn) may cause difficulty falling asleep or staying asleep if it is taken in the evening. Take methamphetamine at around the same time(s) every day. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take methamphetamine exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
If your child is taking prescription methamphetamine (Desoxyn) for ADHD, the doctor will probably start the child on a low dose and gradually increase the dose, not more often than once every week. The doctor may stop methamphetamine treatment from time to time to see if the medication is still needed. Follow these directions carefully.
If you are taking prescription methamphetamine (Desoxyn) to lose weight, the doctor will maintain you on the lowest dose possible. Tolerance to the weight loss effect may develop within a few weeks, making this medication less effective. When this occurs, the doctor may stop the medication.
Prescription methamphetamine (Desoxyn) helps to control ADHD but does not cure this condition. Continue to take prescription methamphetamine (Desoxyn) even if you feel well. Do not stop taking methamphetamine without talking to your doctor.
Figure 1. Methamphetamine
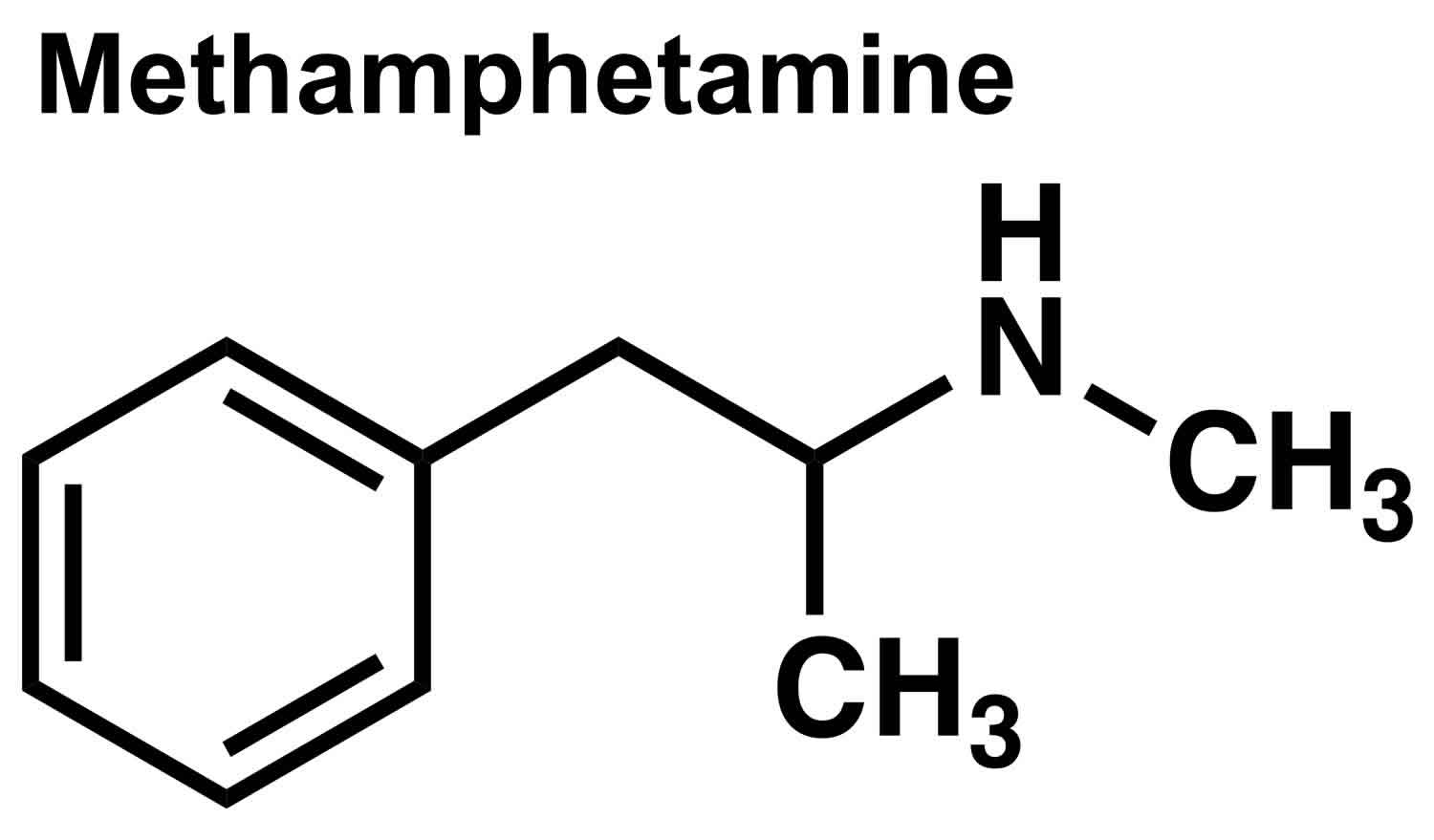
Figure 2. Amphetamine
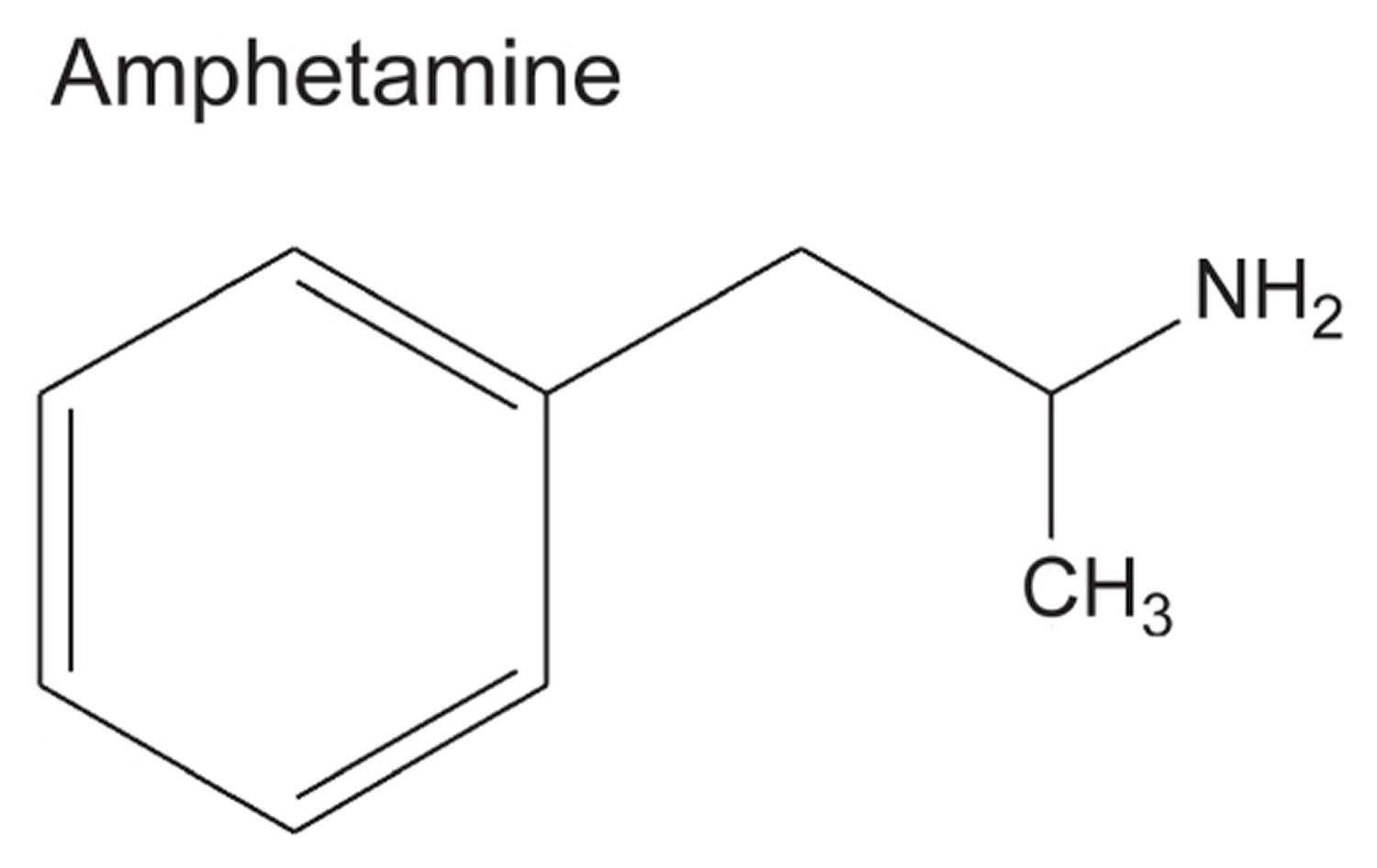
Footnotes: Comparison of chemical structures of methamphetamine and amphetamine. Methamphetamine differs from its metabolite amphetamine by the presence of a methyl group. Both produce the same stimulant behavioural effects and are used clinically for the treatment of attention-deficit hyperactivity disorder (ADHD).
[Source 28 ]Methamphetamine can be habit-forming. Do not take a larger dose, take it more often, or take it for a longer time than prescribed by your doctor. Methamphetamine should only be taken for a short period (e.g., a few weeks) when used for weight loss. However, if you take too much methamphetamine you may find that the medication no longer controls your symptoms, you may feel a need to take large amounts of the medication, and you may experience symptoms such as rash, difficulty falling asleep or staying asleep, irritability, hyperactivity, and unusual changes in your personality or behavior. Overusing methamphetamine may also cause serious heart problems or sudden death.
Tell your doctor if you or anyone in your family drinks or has ever drunk large amounts of alcohol, uses or has ever used street drugs, or has overused prescription medications. Your doctor will probably not prescribe methamphetamine for you.
Do not stop taking methamphetamine without talking to your doctor, especially if you have overused the medication. Your doctor will probably decrease your dose gradually and monitor you carefully during this time. You may experience depression and extreme tiredness if you suddenly stop taking methamphetamine after overusing it.
Do not sell, give away, or let anyone else take your medication. Selling or giving away methamphetamine is against the law and may harm others. Store methamphetamine in a safe place so that no one else can take it accidentally or on purpose. Keep track of how many tablets are left so you will know if any are missing.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with methamphetamine and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions. You can also visit the manufacturer’s website to obtain the Medication Guide.
Can I become addicted to methamphetamine?
You usually do not get addicted to prescription methamphetamine when you take them at the right dosage to treat your health condition. In low to moderate doses, methamphetamine can elevate mood, increase alertness, concentration and energy in fatigued individuals, reduce appetite, and promote weight loss.
However, methamphetamine is very addictive and you can become addicted to methamphetamine. Over time, methamphetamine can change the way your brain works. If you stop using methamphetamine, you can start to feel really sick. This makes it hard to stop. This is called addiction.
Anyone can become addicted to methamphetamine. There is no way to predict who is likely to become addicted. The right treatment can help someone who is addicted feel better and stop using methamphetamine, but treatment is hard work and it can take many years to recover from addiction. The best approach is to never start using methamphetamine in the first place.
Does methamphetamine cause brain damage?
Through imaging studies, a variety of structural changes have been found in the brain of some methamphetamine users 29. However, the data are still too preliminary to answer the question of whether a specific pattern of brain abnormality is characteristic of chronic methamphetamine exposure.
Data from animals show that a high dose of methamphetamine damages striatal dopamine nerve terminals 30 and it is reasonable to expect from the experimental findings that such damage would also occur in people exposed to some dose of the drug 31, 32. The consistent findings from animals have raised the public health concern that chronic methamphetamine exposure might damage nigrostriatal dopamine neurons to the extent that Parkinsonism would develop in later life. However, there is no evidence for dopamine nerve terminal damage in humans who take therapeutic doses of amphetamines (e.g., for attention-deficit hyperactivity disorder), although this possibility has been raised as a specific concern 32. In contrast, some recreational methamphetamine users show modestly decreased levels of the dopamine transporter, a marker of dopamine nerve terminals, in the striatum 31. Whether this represents actual loss of dopamine nerve terminals or has clinical consequences continues to be debated.
Methamphetamine mechanism of action
Methamphetamine was first discovered in 1893 from two chemical subgroups: dextromethamphetamine and levomethamphetamine 1. The term methamphetamine refers to an equal mixture of dextromethamphetamine and levomethamphetamine in their pure amine forms. Methamphetamine was initially developed from its parent drug amphetamine as a nasal decongestant and bronchial inhaler. Like amphetamine, methamphetamine causes increased activity and talkativeness, decreased appetite, and a pleasurable sense of well-being or euphoria. Methamphetamine is highly lipid-soluble, which helps it to be transferred relatively fast across the blood-brain barrier and has an immediate effect on the central nervous system (brain and spinal cord) 7, 33.
Methamphetamine is in a class of medications called central nervous system (brain and spinal cord) stimulants. Methamphetamine promotes the release of monoamine neurotransmitters dopamine, serotonin, and norepinephrine within central nervous system and peripheral nerve endings 34. Methamphetamine also blocks re-uptake of dopamine similar to cocaine, and it may act as a false neurotransmitter. This explains methamphetamine’s euphoric effects in the central nervous system and sympathomimetic effects such as tachycardia and hypertension 35.
Methamphetamine causes the levels of monoamines to be increased by 1:
- Discharging the monoamines out of their storage and freeing them into the synaptic space by making reversal action of the dopamine transporters
- Obstructing the reuptake of monoamines by preventing the activity of transporters of monoamine 36
- Methamphetamine can increase the expression of CRE-Luc by G-protein–coupled trace amine-associated receptor 1 (TAAR1) in transfected cells. Methamphetamine interacts with G protein–coupled trace amine-associated receptor 1 (TAAR1), which triggers a definite inhibition in dopamine uptake dependent on TAAR1 in transfected cells. Methamphetamine has a similar effect on brain striatal synaptosomes 36, 37
- Reducing the dopamine transporters expressions at the cell surface
- The proliferation of the cytosolic levels of monoamines by inhibiting the monoamine oxidase activity
- Enhancing the expression and activity of the dopamine-synthesizing enzyme tyrosine hydroxylase 38.
For oral administration, peak methamphetamine concentrations are seen in 2-4 hours; snorting, smoking, and injecting peak methamphetamine concentrations occur within minutes 2. Methamphetamine elimination half-life ranges from 6-15 hours. Methamphetamine is broken down via the cytochrome P450 complex to active amphetamine, and p-OH-amphetamine and norephedrine, which are both inactive. The rate of methamphetamine excretion into the urine is enhanced as pH falls. Urine toxicology screening may be positive up to 4 days after use 2.
People who use methamphetamine feel an acute, powerful short rush for about 5 to 30 minutes, which varies based on different routes of use. Methamphetamine also causes an enhanced energy level, decreases appetite, and creates euphoria for a range of 6 to 12 hours.
Methamphetamine uses
Methamphetamine has been classified by the U.S. Drug Enforcement Administration as a Schedule 2 stimulant, which makes it legally available only through a nonrefillable prescription. Methamphetamine (Desoxyn) is medically approved in the United States FDA for the treatment of attention deficit hyperactivity disorder (ADHD) in children and adults who are overactive, cannot concentrate for very long, or are easily distracted and impulsive and and for the short-term treatment of obesity 39, but these uses are limited and it is rarely prescribed; also, the prescribed methamphetamine doses are far lower than those typically misused 28, 40. The FDA also indicates that the limited therapeutic usefulness of methamphetamine should be weighed against the inherent risks associated with its use. To avoid toxicity and risk of side effects, FDA guidelines recommend an initial dose of methamphetamine at doses 5–10 mg/day for ADHD in adults and children over six years of age, and may be increased at weekly intervals of 5 mg, up to 25 mg/day, until optimum clinical response is found; the usual effective dose is around 20–25 mg/day. Methamphetamine is sometimes prescribed off label for narcolepsy and idiopathic hypersomnia 41, 42,
The typical acute behavioural effects of methamphetamine include feelings of alertness, wakefulness, energy, well-being, euphoria (at high doses) and suppression of appetite. Methamphetamine also activates the cardiovascular system by increasing heart rate and blood pressure and, for this reason, methamphetamine can cause death at high doses 43.
In the brain, a primary action of methamphetamine is to elevate the levels of extracellular monoamine neurotransmitters (dopamine, serotonin, norepinephrine) by promoting their release from the nerve endings 44. Methamphetamine also blocks re-uptake of dopamine similar to cocaine, and it may act as a false neurotransmitter. This explains methamphetamine’s euphoric effects in the central nervous system and sympathomimetic effects such as tachycardia and hypertension 35.
Contraindications to methamphetamine use
Contraindications to methamphetamine use 1:
- Having thoughts of suicide
- Tourette syndrome
- Hyperthyroidism
- Bipolar disorder
- Psychotic disorder
- Drug abuse
- Behaving with excessive cheerfulness or activity
- Chronic muscle twitches or movements
- Aggressive behavior
- Increased ophthalmic pressure
- Hypertension
- History of a heart attack
- Coronary artery disease
- Cardiomyopathy
- Arrhythmia
- Chronic heart failure
- Stroke
- Atherosclerosis
- Numbness
- Prickling
- Tingling of fingers and toes
- Seizures
- Loss of appetite
- Weight loss
- Breastfeeding mothers
- Increased cardiovascular event risk
- Structural disorder of the heart
- Chronic kidney disease stage 4 (severe) or 5 (failure)
- Kidney disease with a likely reduction in kidney function
- Allergic reaction to sympathomimetic agents or amphetamine analogs.
Is methamphetamine safe?
The consequences of methamphetamine misuse are terrible for the individual psychologically, medically, and socially 14. Using methamphetamine can cause memory loss, aggression, psychotic behavior, damage to the heart and blood vessels, malnutrition, and severe dental problems. Methamphetamine misuse has also been shown to contribute to increased transmission of infectious diseases, such as hepatitis and HIV/AIDS 14.
Taking small amounts of methamphetamine can cause harmful health effects, including 45, 46, 47, 48, 49, 50, 51:
- Increased blood pressure (hypertension) and body temperature (hyperthermia)
- Faster breathing
- Rapid or irregular heartbeat (arrhythmias)
- Loss of appetite, disturbed sleep patterns, or nausea
- Erratic, aggressive, irritable, or violent behavior.
The use of methamphetamine can cause physical and psychological dependence and increased tolerance. Because of the rapid development of tolerance, methamphetamine users frequently need to increase methamphetamine dose to get to the satisfying “high”, which can be very dangerous because the administration of too much methamphetamine also increases the risk of an overdose 52. Based on the reports from 2011, more than 102,000 emergency department visits in the United States were related to methamphetamine use, with over 50% of users also using a combination of other drugs such as alcohol and marijuana, thus producing a synergistic effect.
Chronic methamphetamine use can lead to many damaging, long-term health effects, even when people stop taking meth, including 53:
- Intracranial hemorrhage
- Ischemic stroke
- Heart attack
- Irregular or stopped heartbeat
- Permanent damage to the heart (heart failure) and brain
- High blood pressure leading to heart attacks, strokes, and death 53
- Liver, kidney, and lung damage
- Difficulty breathing
- Anxiety, confusion, and insomnia
- Extreme paranoia, hallucinations, major mood swings, delusions, delusional behavior or violent behavior (psychotic symptoms can sometimes last for months or years after meth use)
- Intense itching, causing skin sores from scratching
- Premature osteoporosis
- Insomnia (severe inability to sleep)
- Severe dental problems with missing and rotted teeth called “meth mouth”
- Repeated infections
- Kidney damage and possibly kidney failure
- Seizures
- Severe weight loss
- Skin sores (abscesses or boils)
- Coma or unresponsiveness (in extreme cases).
The last stage of methamphetamine misuse happens when the person who inappropriately uses methamphetamine becomes paranoid and irritable because of a lack of sleep for about 3 to 15 days. This behavior is called “tweaking” and the person with this behavior is known as the “tweaker” 1. Usually, “tweakers” continue to require more methamphetamine to get to the original high 54. However, this “high” is difficult to achieve, which causes frustration and irritability, and unsteady behavior in the methamphetamine user. Because “tweakers” are unpredictable, they can behave violently, can get involved in domestic arguments, spur-of-the-moment offenses, and become a danger to others or themselves 55. A “tweaker” can behave normally and have clear eyes, concise speech, and brisk movements; however, careful observation will indicate that the person’s eye movement is much faster than normal (up to 10 times). They have a minor quiver voice and jerky movements. Some tweakers minimize or cover these physical symptoms by using a depressant like alcohol or opioids; however, the use of a depressant by the tweaker increases his or her negative feelings of paranoia, irritability, and frustration significantly. Other people around methamphetamine users should use extreme caution because of their unpredictable behaviors 56.
Chronic methamphetamine users also usually show poor personal hygiene and sores on their bodies from picking at “crank bugs”, unhealthy complexion, pallor, and tactile hallucinations that often occur in “tweakers”. Methamphetamine users may develop cracked teeth because of extreme clenching of their jaw when they are high on methamphetamine.
Methamphetamine special precautions
It is very important that your doctor check your or your child’s progress at regular visits to make sure methamphetamine is working properly. Blood tests may be needed to check for unwanted side effects.
Before taking methamphetamine prescribed by your doctor:
- Tell your doctor and pharmacist if you are allergic to methamphetamine, other stimulant medications such as amphetamine, benzphetamine, dextroamphetamine (Dexedrine, in Adderall), lisdexamfetamine (Vyvanse), any other medications, or any of the ingredients in methamphetamine tablets. Ask your pharmacist for a list of the ingredients.
- Tell your doctor or pharmacist if you are taking the following medications or have stopped taking them in the past two weeks: monoamine oxidase (MAO) inhibitors including isocarboxazid (Marplan), linezolid (Zyvox), methylene blue, phenelzine (Nardil), selegiline (Eldepryl, Emsam, Zelapar), or tranylcypromine (Parnate). If you stop taking methamphetamine, you should wait at least 14 days before you start to take an MAO inhibitor.
- Some medications should not be taken with methamphetamine. Other medications may cause dosing changes or extra monitoring when taken with methamphetamine. Make sure you have discussed any medications you are currently taking or plan to take before taking methamphetamine with your doctor and pharmacist. Before starting, stopping, or changing any medications while taking methamphetamine, please get the advice of your doctor or pharmacist.
- The following nonprescription or herbal products may interact with methamphetamine: sodium bicarbonate (Arm and Hammer Baking Soda, Soda Mint); sodium phosphate; St. John’s wort; tryptophan; nutritional supplements including glutamic acid (L-glutamine). Be sure to let your doctor and pharmacist know that you are taking these medications before you start taking methamphetamine. Do not start any of these medications while taking methamphetamine without discussing with your healthcare provider.
- Tell your doctor if you have glaucoma (increased pressure in the eye that may cause vision loss), hypertension (high blood pressure), hyperthyroidism (condition in which there is too much thyroid hormone in the body), feelings of anxiety, tension, or agitation, or heart or blood vessel disease. Your doctor will probably tell you not to take methamphetamine.
- Tell your doctor if anyone in your family has or has ever had an irregular heartbeat or has died suddenly. Also tell your doctor if you have recently had a heart attack, and if you have or have ever had a heart defect, an irregular heartbeat, or other heart problems. Your doctor will examine you to see if your heart and blood vessels are healthy. Your doctor will probably tell you not to take methamphetamine if you have a heart condition or if there is a high risk that you may develop a heart condition.
- Tell your doctor if you or anyone in your family has or has ever had depression, bipolar disorder (mood that changes from depressed to abnormally excited), or mania (frenzied, abnormally excited mood), facial or motor tics (repeated uncontrollable movements), verbal tics (repetition of sounds or words that is hard to control) or Tourette’s syndrome (a condition characterized by the need to perform repeated motions or to repeat sounds or words), or has thought about or attempted suicide. Also tell your doctor if you have or have ever had mental illness, seizures, diabetes, or an abnormal electroencephalogram (EEG; test that measures electrical activity in the brain). If your child is taking methamphetamine to treat ADHD, tell your child’s doctor if your child has recently experienced unusual stress.
- Tell your doctor if you are pregnant, plan to become pregnant, or are breastfeeding. If you become pregnant while taking methamphetamine, call your doctor. Do not breastfeed while taking methamphetamine.
- You should know that methamphetamine may make you drowsy. Do not drive a car or operate machinery until you know how this medication affects you.
- You should know that methamphetamine should be used as part of a total treatment program for ADHD, which may include counseling and special education. Make sure to follow all of your doctor’s and/or therapist’s instructions.
- You should know that methamphetamine may cause sudden death in children and teenagers, especially children and teenagers who have heart defects or serious heart problems. This medication also may cause sudden death, heart attack, or stroke in adults, especially adults with heart defects or serious heart problems. Call your or your child’s doctor right away if you or
- Your child has any signs of heart problems while taking this medication including: chest pain, shortness of breath, or fainting.
Do not use methamphetamine if you are using or have used an MAO inhibitor (MAOI), including isocarboxazid (Marplan), linezolid (Zyvox), phenelzine (Nardil), selegiline (Eldepryl), tranylcypromine (Parnate), within the past 14 days.
You or your child will also need to have your blood pressure and heart rate measured before starting methamphetamine and while you are using it. If you notice any change in your blood pressure, call your doctor right away. If you have questions about this, talk to your doctor.
Methamphetamine may cause serious heart or blood vessel problems. This may be more likely to occur in patients who have a family history of heart disease. Check with your doctor right away if you have chest pain, trouble breathing, or fainting while taking methamphetamine.
Tell your doctor right away if you or your family notice any unusual changes in behavior, such as an increase in aggression, hostility, agitation, irritability, or suicidal thinking or behavior. Also tell your doctor if you or your child see, hear, or feel things that are not there, or have any unusual thoughts, especially if they are new or getting worse quickly.
If you have been using methamphetamine for a long time and you think you may have become mentally or physically dependent on it, check with your doctor. Some signs of dependence may be:
- A strong desire or need to continue taking the medicine.
- A need to increase the dose to receive the same effects.
- Withdrawal effects after stopping the medicine such as mental depression, nausea or vomiting, stomach cramps or pain, trembling, or unusual tiredness or weakness.
Symptoms of methamphetamine overdose include:
- Agitation, aggressive, blurred vision, change in consciousness, chest pain or discomfort, confusion, dark urine, diarrhea, dizziness, faintness, or lightheadedness when getting up suddenly from a lying or sitting position, fast, pounding, or irregular heartbeat or pulse, fever, headache, inability to speak, loss of consciousness, muscle pains, stiffness, cramps, or spasms, nausea, nervousness, pain or discomfort in the arms, jaw, back, or neck, pale, clammy skin, palpitations, panic state, pounding in the ears, restlessness, seeing, hearing, or feeling things that are not there, seizures, shakiness in legs, arms, hands, feet, shivering, slow or fast heartbeat, slurred speech, sweating, talking or acting with excitement you cannot control, temporary blindness, thirst, trembling or shaking of hands or feet, overactive reflexes, rapid breathing, unusual tiredness or weakness, vomiting, or weakness in the arm or leg on one side of the body, sudden and severe.
- Call your doctor right away if you notice these symptoms.
Methamphetamine may cause some people to feel a false sense of wellbeing or to become dizzy, lightheaded, or less alert than they are normally. It may also cause blurred vision or other vision problems. Make sure you know how you react to methamphetamine before you drive, use machines, or do anything else that could be dangerous if you are dizzy or not alert.
Methamphetamine may cause slow growth. If your child is using methamphetamine, the doctor will need to keep track of your child’s height and weight.
Methamphetamine may cause Raynaud’s phenomenon, which is a problem with blood circulation in the fingers or toes. Tell your doctor if you have tingling or pain, a cold feeling, paleness, or skin color changes in the fingers or toes, especially when exposed to cold. Call your doctor right away if you have unexplained sores or ulcers on your fingers or toes.
Check with your doctor right away if you have anxiety, restlessness, a fast heartbeat, fever, sweating, muscle spasms, twitching, nausea, vomiting, diarrhea, or see or hear things that are not there. These may be symptoms of a serious condition called serotonin syndrome. Your risk may be higher if you also take certain other medicines that affect serotonin levels in your body.
Before you have any medical tests, tell the medical doctor in charge that you are taking methamphetamine. The results of some tests may be affected by methamphetamine.
Do not take other medicines unless they have been discussed with your doctor. This includes prescription or nonprescription (over-the-counter [OTC]) medicines, herbal or vitamin supplements, and medicine for appetite control, asthma, colds, cough, hayfever, or sinus problems.
Medical problems
The presence of other medical problems may affect the use of methamphetamine. Make sure you tell your doctor if you have any other medical problems, especially:
- Agitation, severe or
- Arteriosclerosis (hardening of the arteries), severe or
- Drug abuse, history of or
- Glaucoma or
- Heart attack, recent or
- Heart failure or
- Hypertension (high blood pressure), severe or
- Hyperthyroidism (overactive thyroid) or
- Stroke, history of—Should not be used in patients with these conditions.
- Alcohol abuse, history of—Use with caution. Dependence may be more likely to develop.
- Bipolar disorder (manic-depressive illness), history of or
- Depression, or a family history of or
- Heart or blood vessel disease (eg, cardiomyopathy, coronary artery disease) or
- Heart rhythm problem (eg, ventricular arrhythmia), or family history of or
- Hypertension (high blood pressure), mild or
- Psychosis (mental illness), history of or
- Raynaud’s phenomenon (blood vessel disease) or
- Seizures, history of or
- Tachycardia (rapid heart rate) or
- Tourette syndrome, or family history of—Use with caution. May make these conditions worse.
Drug interactions
Although certain medicines should not be used together at all, in other cases two different medicines may be used together even if an interaction might occur. In these cases, your doctor may want to change the dose, or other precautions may be necessary. When you are taking methamphetamine, it is especially important that your doctor know if you are taking any of the medicines listed below. The following interactions have been selected on the basis of their potential significance and are not necessarily all-inclusive.
Using methamphetamine with any of the following medicines is not recommended. Your doctor may decide not to treat you with this medication or change some of the other medicines you take.
- Furazolidone
- Iproniazid
- Isocarboxazid
- Linezolid
- Methylene Blue
- Moclobemide
- Nialamide
- Ozanimod
- Phenelzine
- Procarbazine
- Rasagiline
- Safinamide
- Selegiline
- Sibutramine
- Tranylcypromine.
Methamphetamine dosage
The dose of methamphetamine will be different for different patients. Follow your doctor’s orders or the directions on the label. The following information includes only the average doses of methamphetamine. If your dose is different, do not change it unless your doctor tells you to do so.
The amount of medicine that you take depends on the strength of the medicine. Also, the number of doses you take each day, the time allowed between doses, and the length of time you take the medicine depend on the medical problem for which you are using the medicine.
Methamphetamine oral dosage form (tablets)
- For attention deficit hyperactivity disorder (ADHD):
- Adults and children 6 years of age and older: At first, 5 milligrams (5 mg) 1 or 2 times a day. Your doctor may adjust your dose as needed. However, the dose is usually not more than 25 mg per day.
- Children younger than 6 years of age: Use and dose must be determined by your doctor.
Missed dose
If you miss a dose of methamphetamine, take it as soon as possible. However, if it is almost time for your next dose, skip the missed dose and go back to your regular dosing schedule. Do not double doses.
Methamphetamine side effects
Along with its needed effects, methamphetamine may cause some unwanted effects. Although not all of these side effects may occur, if they do occur they may need medical attention.
See your doctor if any of these symptoms are severe or do not go away:
- restlessness
- upset stomach
- constipation
- dry mouth
- unpleasant taste
- headache
- weight loss
- loss of appetite
- itching
- changes in sex drive or ability
- difficulty falling asleep or staying asleep
Some methamphetamine side effects can be serious. If you experience any of these symptoms or those listed in the IMPORTANT WARNING section above, stop taking methamphetamine and see your doctor immediately or get emergency medical treatment:
- fast or pounding heartbeat
- uncontrollable shaking of a part of your body
- excessive tiredness
- slow or difficult speech
- seizures
- motor or verbal tics
- believing things that are not true
- feeling unusually suspicious of others
- hallucinating (seeing things or hearing voices that do not exist)
- agitation, hallucinations (seeing things or hearing voices that do not exist), fever, sweating, confusion, fast heartbeat, shivering, severe muscle stiffness or twitching, loss of coordination, nausea, vomiting, or diarrhea
- mania (frenzied or abnormally excited mood)
- aggressive or hostile behavior
- changes in vision or blurred vision
- paleness or blue color of fingers or toes
- pain, burning, or tingling in the hands or feet
- unexplained wounds appearing on fingers or toes.
Incidence not known:
- bad, unusual, or unpleasant (after) taste
- change in taste
- constipation
- decreased interest in sexual intercourse
- dry mouth
- hives or welts, itching, or skin rash
- inability to have or keep an erection
- indigestion
- loss in sexual ability, desire, drive, or performance
- passing of gas
- redness of the skin
- weight loss
Methamphetamine may slow children’s growth or weight gain. Your child’s doctor will watch his or her growth carefully. Talk to your child’s doctor if you have concerns about your child’s growth or weight gain while he or she is taking this medication. Talk to your child’s doctor about the risks of giving methamphetamine to your child.
If you take a large amount of methamphetamine, you will be at higher risk for more dangerous side effects, including:
- Agitation
- Chest pain
- Coma or unresponsiveness (in extreme cases)
- Heart attack
- Irregular or stopped heartbeat
- Difficulty breathing
- Very high body temperature
- Kidney damage and possibly kidney failure
- Paranoia
- Seizures
- Severe stomach pain
- Stroke
Long-term use of methamphetamine can lead to significant psychological problems, including:
- Delusions
- Delusional behavior
- Extreme paranoia
- Major mood swings
- Insomnia (severe inability to sleep)
Other long-term use of methamphetamine symptoms may include:
- Missing and rotted teeth called “meth mouth”
- Repeated infections
- Severe weight loss
- Skin sores (abscesses or boils)
The length of time methamphetamines stay active can be much longer than for cocaine and other stimulants. Some paranoid delusions can last for 15 hours.
Methamphetamine may cause other side effects. See your doctor if you have any unusual problems while taking methamphetamine.
Methamphetamine overdose
Methamphetamine overdose may be acute (sudden) or chronic (long-term).
- An acute methamphetamine overdose occurs when someone takes this drug by accident or on purpose and has side effects. These side effects can be life threatening.
- A chronic methamphetamine overdose refers to the health effects in someone who uses methamphetamine on a regular basis.
Symptoms of acute methamphetamine overdose may include the following:
- aggressive behavior
- agitation
- angry
- blurred vision
- coma (loss of consciousness for a period of time)
- change in consciousness
- chest pain or discomfort
- confusion
- dark urine
- depression
- diarrhea
- dizziness, faintness, or lightheadedness when getting up suddenly from a lying or sitting position
- fainting
- fast breathing
- fast, slow, or irregular heartbeat
- fever
- hallucinations (seeing things or hearing voices that do not exist)
- headache
- inability to speak
- irregular heartbeat
- loss of consciousness
- muscle cramps, spasms, pain, or stiffness
- nausea
- nervousness
- overactive reflexes
- pain or discomfort in the arms, jaw, back, or neck
- pale, clammy skin
- palpitations
- panic
- pounding in the ears
- restlessness
- seeing, hearing, or feeling things that are not there
- seizures
- shivering
- slow or fast heartbeat
- slurred speech
- stomach cramps
- sweating
- talking or acting with excitement you cannot control
- temporary blindness
- thirst
- tiredness
- tremor
- trouble breathing
- unusual tiredness or weakness
- uncontrollable shaking of a part of your body
- vomiting
- weakness in the arm or leg on one side of the body, sudden and severe.
A large methamphetamine overdose can cause death. Knowing the physical and behavioral symptoms of the methamphetamine overdose and diagnosis of the overdose is essential for saving the patient’s life 57.
If you believe someone has taken methamphetamine and they are having bad symptoms, get them medical help right away. Take extreme caution around them, especially if they appear to be extremely agitated or paranoid.
If they are having a seizure, gently hold the back of their head to prevent injury. If possible, turn their head or body to the side in case they vomit. DO NOT try to stop their arms and legs from shaking, or put anything in their mouth.
Emergency room treatment
The emergency room doctor will measure and monitor the person’s vital signs, including temperature, pulse, breathing rate, and blood pressure. Symptoms will be treated as appropriate. The person may receive:
- Activated charcoal and laxative, if the drug was recently taken by mouth.
- Blood and urine tests.
- Breathing support, including oxygen. If needed, the person may be placed on a breathing machine with a tube through the mouth into the throat.
- Chest x-ray if the person had vomiting or abnormal breathing.
- CT (computerized tomography) scan of the head, if head injury is suspected.
- ECG (electrocardiogram, or heart tracing).
- Intravenous fluids (through a vein) medicines to treat symptoms such as pain, anxiety, agitation, nausea, seizures, and high blood pressure.
- Poison and drug (toxicology) screening.
- Other medicines or treatments for heart, brain, muscle, and kidney complications.
Benzodiazepines represent first-line treatment for methamphetamine overdose but frequently require repeated and escalated dosing to achieve the effect 2. However, some methamphetamine users may be resistant to benzodiazepine treatment 2. Antipsychotics, such as haloperidol and olanzapine, are also useful in the management of agitation 2. Combination treatment with benzodiazepines and antipsychotics has been shown to be more efficacious than monotherapy 58. Diphenhydramine is often added to enhance sedation and as prophylaxis against dystonia and akathisia. A common example of this is the “B-52” with its combination of haloperidol (5 mg), diphenhydramine (50 mg), and lorazepam (2 mg) 59, 60.
For tachycardia and hypertension that does not respond to sedation, the combined beta/alpha-blocker labetalol is preferred based on a systematic review from 2015 61. For tachycardia without hypertension, the beta 1-blocker metoprolol is preferred. Both labetalol and metoprolol have the added advantage of being lipophilic, with CNS penetration and antagonism of excess monoamines causing agitation. Despite the unfortunate persistence of dogma carried over from a small number (n=7) of cocaine cases, there have been no cases of “unopposed alpha stimulation” reported with beta-blocker use and treatment of methamphetamine overdose 2. For severe hypertension without tachycardia, nitroprusside is recommended as it is easily titrated to effect and has a half-life of minutes. Administration of copious intravenous crystalloids is also recommended to enhance urinary elimination and prevent acute renal failure 2. Calcium channel blockers may be used but do not directly treat the hyperadrenergic state induced by methamphetamine, and their reduction of tachycardia and blood pressure is much less predictable than beta-blockers 2.
There are no FDA-approved medications for stimulant use disorder but a recent study found the combination of injectable naltrexone and oral bupropion was safe and effective in treating adults with moderate or severe methamphetamine use disorder 62.
Methamphetamine overdose prognosis
A large methamphetamine overdose can cause death. Deaths from methamphetamine overdose are common and include arrhythmias, intracranial hemorrhage, and cardiogenic shock. The use of methamphetamine during pregnancy has also been linked to preterm birth and intrauterine growth restriction. How well a person does depends on the amount of methamphetamine they took and how quickly they were treated. The faster a person gets medical help, the better the chance for recovery.
Psychosis and paranoia may last up to 1 year, even with aggressive medical treatment. Memory loss and difficulty sleeping may be permanent. Skin changes and tooth loss are permanent unless the person has cosmetic surgery or dentistry to correct the problems. Further disability may occur if the person had a heart attack or a stroke. These can happen if the drug caused very high blood pressure and body temperatures. Infections and other complications in organs such as the heart, brain, kidneys, liver, and spine, may occur as a result of injection. There may be permanent damage to the organs even if the person receives treatment. The antibiotics used to treat these infections may also result in complications.
The long-term outlook of methamphetamine abuse depends on what organs are affected. Permanent damage may occur, which may cause:
- Seizures, stroke, and paralysis
- Chronic anxiety and psychosis (severe mental disorders)
- Decreased mental functioning
- Heart problems
- Kidney failure that requires dialysis (kidney machine)
- Destruction of muscles, which can lead to amputation.
- Yasaei R, Saadabadi A. Methamphetamine. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535356[↩][↩][↩][↩][↩]
- Richards JR, Laurin EG. Methamphetamine Toxicity. [Updated 2023 Jun 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430895[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- McKetin R, Sutherland R, Peacock A, Farrell M, Degenhardt L. Patterns of smoking and injecting methamphetamine and their association with health and social outcomes. Drug Alcohol Rev. 2021 Nov;40(7):1256-1265. doi: 10.1111/dar.13364[↩][↩]
- Jones CM, Houry D, Han B, Baldwin G, Vivolo-Kantor A, Compton WM. Methamphetamine use in the United States: epidemiological update and implications for prevention, treatment, and harm reduction. Ann N Y Acad Sci. 2022 Feb;1508(1):3-22. doi: 10.1111/nyas.14688[↩]
- Moszczynska A, Callan SP. Molecular, Behavioral, and Physiological Consequences of Methamphetamine Neurotoxicity: Implications for Treatment. J Pharmacol Exp Ther. 2017 Sep;362(3):474-488. doi: 10.1124/jpet.116.238501[↩][↩]
- Radfar SR, Rawson RA. Current research on methamphetamine: epidemiology, medical and psychiatric effects, treatment, and harm reduction efforts. Addict Health. 2014 Summer-Autumn;6(3-4):146-54. https://pmc.ncbi.nlm.nih.gov/articles/PMC4354220[↩]
- Cisneros IE, Ghorpade A. Methamphetamine and HIV-1-induced neurotoxicity: role of trace amine associated receptor 1 cAMP signaling in astrocytes. Neuropharmacology. 2014 Oct;85:499-507. doi: 10.1016/j.neuropharm.2014.06.011[↩][↩]
- World Drug Report 2016. (United Nations publication, Sales No. E.16.XI.7).[↩]
- World Drug Report 2019. (United Nations publication, Sales No. E.19.XI.8).[↩]
- United Nations Office on Drugs and Crime . World Drug Report 2017. New York: United Nations, 2017:13–20.[↩]
- Degenhardt L, Baxter AJ, Lee YY, Hall W, Sara GE, Johns N, Flaxman A, Whiteford HA, Vos T. The global epidemiology and burden of psychostimulant dependence: findings from the Global Burden of Disease Study 2010. Drug Alcohol Depend. 2014 Apr 1;137:36-47. doi: 10.1016/j.drugalcdep.2013.12.025[↩]
- Farrell M, Martin NK, Stockings E, Bórquez A, Cepeda JA, Degenhardt L, Ali R, Tran LT, Rehm J, Torrens M, Shoptaw S, McKetin R. Responding to global stimulant use: challenges and opportunities. Lancet. 2019 Nov 2;394(10209):1652-1667. doi: 10.1016/S0140-6736(19)32230-5[↩]
- Turner C, Chandrakumar D, Rowe C, Santos GM, Riley ED, Coffin PO. Cross-sectional cause of death comparisons for stimulant and opioid mortality in San Francisco, 2005-2015. Drug Alcohol Depend. 2018 Apr 1;185:305-312. doi: 10.1016/j.drugalcdep.2017.12.030[↩][↩]
- NIDA. 2023, February 24. Overview. Retrieved from https://nida.nih.gov/publications/research-reports/methamphetamine/overview[↩][↩][↩]
- 2021 NSDUH Annual National Report. https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report[↩][↩]
- Chomchai C, Chomchai S. Global patterns of methamphetamine use. Curr Opin Psychiatry. 2015 Jul;28(4):269-74. doi: 10.1097/YCO.0000000000000168[↩]
- Carfora A, Cassandro P, Feola A, La Sala F, Petrella R, Borriello R. Ethical Implications in Vaccine Pharmacotherapy for Treatment and Prevention of Drug of Abuse Dependence. J Bioeth Inq. 2018 Mar;15(1):45-55. doi: 10.1007/s11673-017-9834-5[↩]
- Matsumoto RR, Seminerio MJ, Turner RC, Robson MJ, Nguyen L, Miller DB, O’Callaghan JP. Methamphetamine-induced toxicity: an updated review on issues related to hyperthermia. Pharmacol Ther. 2014 Oct;144(1):28-40. doi: 10.1016/j.pharmthera.2014.05.001[↩]
- Liakoni E, Dolder PC, Rentsch K, Liechti ME. Acute health problems due to recreational drug use in patients presenting to an urban emergency department in Switzerland. Swiss Med Wkly. 2015 Jul 28;145:w14166. doi: 10.4414/smw.2015.14166[↩]
- Karila L, Megarbane B, Cottencin O, Lejoyeux M. Synthetic cathinones: a new public health problem. Curr Neuropharmacol. 2015 Jan;13(1):12-20. doi: 10.2174/1570159X13666141210224137[↩]
- Lappin JM, Darke S, Farrell M. Stroke and methamphetamine use in young adults: a review. J Neurol Neurosurg Psychiatry. 2017 Dec;88(12):1079-1091. doi: 10.1136/jnnp-2017-316071[↩]
- Roohbakhsh A, Shirani K, Karimi G. Methamphetamine-induced toxicity: The role of autophagy? Chem Biol Interact. 2016 Dec 25;260:163-167. doi: 10.1016/j.cbi.2016.10.012[↩]
- Uhlmann S, DeBeck K, Simo A, Kerr T, Montaner JS, Wood E. Health and social harms associated with crystal methamphetamine use among street-involved youth in a Canadian setting. Am J Addict. 2014 Jul-Aug;23(4):393-8. doi: 10.1111/j.1521-0391.2014.12123.x[↩]
- Hedegaard H, Minino AM & Warner M. 2020. Drug overdose deaths in the United States, 1999–2019. NCHS Data Brief, no 394. https://www.cdc.gov/nchs/data/databriefs/db394-H.pdf[↩]
- Mattson CL, Tanz LJ, Quinn K, Kariisa M, Patel P, Davis NL. Trends and Geographic Patterns in Drug and Synthetic Opioid Overdose Deaths – United States, 2013-2019. MMWR Morb Mortal Wkly Rep. 2021 Feb 12;70(6):202-207. doi: 10.15585/mmwr.mm7006a4[↩]
- Hedegaard H, Miniño AM, Warner M. Co-involvement of opioids in drug overdose deaths involving cocaine and psychostimulants. NCHS Data Brief, no 406. Hyattsville, MD: National Center for Health Statistics. 2021. DOI: https://doi.org/10.15620/cdc:103966[↩]
- Han B, Cotto J, Etz K, Einstein EB, Compton WM, Volkow ND. Methamphetamine Overdose Deaths in the US by Sex and Race and Ethnicity. JAMA Psychiatry. 2021 May 1;78(5):564-567. doi: 10.1001/jamapsychiatry.2020.4321[↩]
- Kish SJ. Pharmacologic mechanisms of crystal meth. CMAJ. 2008 Jun 17;178(13):1679-82. doi: 10.1503/cmaj.071675[↩][↩]
- Chang L, Alicata D, Ernst T, Volkow N. Structural and metabolic brain changes in the striatum associated with methamphetamine abuse. Addiction. 2007 Apr;102 Suppl 1:16-32. doi: 10.1111/j.1360-0443.2006.01782.x[↩]
- Ricaurte GA, Seiden LS, Schuster CR. Further evidence that amphetamines produce long-lasting dopamine neurochemical deficits by destroying dopamine nerve fibers. Brain Res. 1984 Jun 15;303(2):359-64. doi: 10.1016/0006-8993(84)91221-6[↩]
- Moszczynska A, Fitzmaurice P, Ang L, Kalasinsky KS, Schmunk GA, Peretti FJ, Aiken SS, Wickham DJ, Kish SJ. Why is parkinsonism not a feature of human methamphetamine users? Brain. 2004 Feb;127(Pt 2):363-70. doi: 10.1093/brain/awh046[↩][↩]
- Ricaurte GA, Mechan AO, Yuan J, Hatzidimitriou G, Xie T, Mayne AH, McCann UD. Amphetamine treatment similar to that used in the treatment of adult attention-deficit/hyperactivity disorder damages dopaminergic nerve endings in the striatum of adult nonhuman primates. J Pharmacol Exp Ther. 2005 Oct;315(1):91-8. doi: 10.1124/jpet.105.087916[↩][↩]
- Kalasinsky KS, Bosy TZ, Schmunk GA, Reiber G, Anthony RM, Furukawa Y, Guttman M, Kish SJ. Regional distribution of methamphetamine in autopsied brain of chronic human methamphetamine users. Forensic Sci Int. 2001 Feb 15;116(2-3):163-9. doi: 10.1016/s0379-0738(00)00368-6[↩]
- Der-Ghazarian TS, Charmchi D, Noudali SN, Scott SN, Holter MC, Newbern JM, Neisewander JL. Neural Circuits Associated with 5-HT1B Receptor Agonist Inhibition of Methamphetamine Seeking in the Conditioned Place Preference Model. ACS Chem Neurosci. 2019 Jul 17;10(7):3271-3283. doi: 10.1021/acschemneuro.8b00709[↩]
- Fleckenstein AE, Volz TJ, Riddle EL, Gibb JW, Hanson GR. New insights into the mechanism of action of amphetamines. Annu Rev Pharmacol Toxicol. 2007;47:681-98. doi: 10.1146/annurev.pharmtox.47.120505.105140[↩][↩]
- Miner NB, Phillips TJ, Janowsky A. The Role of Biogenic Amine Transporters in Trace Amine-Associated Receptor 1 Regulation of Methamphetamine-Induced Neurotoxicity. J Pharmacol Exp Ther. 2019 Oct;371(1):36-44. doi: 10.1124/jpet.119.258970[↩][↩]
- Shi X, Swanson TL, Miner NB, Eshleman AJ, Janowsky A. Activation of Trace Amine-Associated Receptor 1 Stimulates an Antiapoptotic Signal Cascade via Extracellular Signal-Regulated Kinase 1/2. Mol Pharmacol. 2019 Oct;96(4):493-504. doi: 10.1124/mol.119.116798[↩]
- Huang WS, Chen GJ, Tsai TH, Cheng CY, Shiue CY, Ma KH, Yeh SH. In vivo long-lasting alterations of central serotonin transporter activity and associated dopamine synthesis after acute repeated administration of methamphetamine. EJNMMI Res. 2019 Sep 18;9(1):92. doi: 10.1186/s13550-019-0557-y[↩]
- Index to Drug-Specific Information. https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/index-drug-specific-information[↩]
- DESOXYN- methamphetamine hydrochloride tablet. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=81bfc45f-c345-47d0-9fc9-77abe553b541[↩]
- Mitler MM, Hajdukovic R, Erman MK. Treatment of narcolepsy with methamphetamine. Sleep. 1993 Jun;16(4):306-17. https://pmc.ncbi.nlm.nih.gov/articles/PMC2267865[↩]
- Morgenthaler TI, Kapur VK, Brown T, Swick TJ, Alessi C, Aurora RN, Boehlecke B, Chesson AL Jr, Friedman L, Maganti R, Owens J, Pancer J, Zak R; Standards of Practice Committee of the American Academy of Sleep Medicine. Practice parameters for the treatment of narcolepsy and other hypersomnias of central origin. Sleep. 2007 Dec;30(12):1705-11. doi: 10.1093/sleep/30.12.1705. Erratum in: Sleep. 2008 Feb 1;31(2):table of contents.[↩]
- Karch SB. Karchs Pathology of Drug Abuse. 3rd ed. Boca Raton (FL): CRC Press; 2001.[↩]
- Rothman RB, Baumann MH. Monoamine transporters and psychostimulant drugs. Eur J Pharmacol. 2003 Oct 31;479(1-3):23-40. doi: 10.1016/j.ejphar.2003.08.054[↩]
- Pareek T, Platt DM, Rüedi-Bettschen D. Daily, limited access to methamphetamine self-administration during pregnancy leads to increased methamphetamine sensitivity in adult offspring. Dev Psychobiol. 2023 Jan;65(1):e22350 https://pmc.ncbi.nlm.nih.gov/articles/PMC10038219[↩]
- Rawson RA, Washton A, Domier CP, Reiber C. Drugs and sexual effects: role of drug type and gender. J Subst Abuse Treat. 2002 Mar;22(2):103-8. doi: 10.1016/s0740-5472(01)00215-x[↩]
- Kalechstein AD, Newton TF, Green M. Methamphetamine dependence is associated with neurocognitive impairment in the initial phases of abstinence. J Neuropsychiatry Clin Neurosci. 2003 Spring;15(2):215-20. doi: 10.1176/jnp.15.2.215[↩]
- Rawson RA, Gonzales R, Obert JL, McCann MJ, Brethen P. Methamphetamine use among treatment-seeking adolescents in Southern California: participant characteristics and treatment response. J Subst Abuse Treat. 2005 Sep;29(2):67-74. doi: 10.1016/j.jsat.2005.04.001[↩]
- Arria AM, Derauf C, Lagasse LL, Grant P, Shah R, Smith L, Haning W, Huestis M, Strauss A, Della Grotta S, Liu J, Lester B. Methamphetamine and other substance use during pregnancy: preliminary estimates from the Infant Development, Environment, and Lifestyle (IDEAL) study. Matern Child Health J. 2006 May;10(3):293-302. doi: 10.1007/s10995-005-0052-0[↩]
- Zapata LB, Hillis SD, Marchbanks PA, Curtis KM, Lowry R. Methamphetamine use is independently associated with recent risky sexual behaviors and adolescent pregnancy. J Sch Health. 2008 Dec;78(12):641-8. doi: 10.1111/j.1746-1561.2008.00360.x[↩]
- Albertson TE, Derlet RW, Van Hoozen BE. Methamphetamine and the expanding complications of amphetamines. West J Med. 1999 Apr;170(4):214-9. https://pmc.ncbi.nlm.nih.gov/articles/instance/1305551/pdf/westjmed00319-0028.pdf[↩]
- Nie L, Zhaom Z, Wen X, Luo W, Ju T, Ren A, Wu B, London ED, Li J. Factors affecting the occurrence of psychotic symptoms in chronic methamphetamine users. J Addict Dis. 2018 Jul-Dec;37(3-4):202-210. doi: 10.1080/10550887.2019.1661752[↩]
- Krasnova IN, Cadet JL. Methamphetamine toxicity and messengers of death. Brain Res Rev. 2009 May;60(2):379-407. doi: 10.1016/j.brainresrev.2009.03.002[↩][↩]
- Hauw F, Meppiel E, Steichen O, Conan PL, Capron J, de Broucker T. Isolated persistent acute global amnesia after acute abuse of 3,4-methylenedioxy-methamphetamine (MDMA). J Neurol Sci. 2018 Mar 15;386:36-38. doi: 10.1016/j.jns.2018.01.005[↩]
- Hoffman WF, Jacobs MB, Dennis LE, McCready HD, Hickok AW, Smith SB, Kohno M. Psychopathy and Corticostriatal Connectivity: The Link to Criminal Behavior in Methamphetamine Dependence. Front Psychiatry. 2020 Feb 28;11:90. doi: 10.3389/fpsyt.2020.00090[↩]
- Kaushal N, Matsumoto RR. Role of sigma receptors in methamphetamine-induced neurotoxicity. Curr Neuropharmacol. 2011 Mar;9(1):54-7. doi: 10.2174/157015911795016930[↩]
- Weng TI, Chen LY, Chen JY, Chen PS, Hwa HL, Fang CC. Characteristics of analytically confirmed illicit substance-using patients in the Emergency Department. J Formos Med Assoc. 2020 Dec;119(12):1827-1834. doi: 10.1016/j.jfma.2020.01.005[↩]
- Zun LS. Evidence-Based Review of Pharmacotherapy for Acute Agitation. Part 1: Onset of Efficacy. J Emerg Med. 2018 Mar;54(3):364-374. doi: 10.1016/j.jemermed.2017.10.011[↩]
- Yang X, Wang Y, Li Q, Zhong Y, Chen L, Du Y, He J, Liao L, Xiong K, Yi CX, Yan J. The Main Molecular Mechanisms Underlying Methamphetamine- Induced Neurotoxicity and Implications for Pharmacological Treatment. Front Mol Neurosci. 2018 Jun 4;11:186. doi: 10.3389/fnmol.2018.00186[↩]
- Schuring CA, Dodge DL, Whitcomb TJ, Wall GC, Smith HL, Hicklin GA. Overdoses and Substance Toxicity in Patients Admitted to Intensive Care Units in a Midwestern U.S. City. J Trauma Nurs. 2018 Mar/Apr;25(2):87-91. doi: 10.1097/JTN.0000000000000349[↩]
- Richards JR, Albertson TE, Derlet RW, Lange RA, Olson KR, Horowitz BZ. Treatment of toxicity from amphetamines, related derivatives, and analogues: a systematic clinical review. Drug Alcohol Depend. 2015 May 1;150:1-13. doi: 10.1016/j.drugalcdep.2015.01.040[↩]
- Trivedi MH, Walker R, Ling W, Dela Cruz A, Sharma G, Carmody T, Ghitza UE, Wahle A, Kim M, Shores-Wilson K, Sparenborg S, Coffin P, Schmitz J, Wiest K, Bart G, Sonne SC, Wakhlu S, Rush AJ, Nunes EV, Shoptaw S. Bupropion and Naltrexone in Methamphetamine Use Disorder. N Engl J Med. 2021 Jan 14;384(2):140-153. doi: 10.1056/NEJMoa2020214[↩]




{kind=link}