
Contents
What is narcolepsy
Narcolepsy is a lifelong sleep disorder that makes you feel overwhelmingly tired characterized by excessive daytime sleepiness and in severe cases, have sudden uncontrollable sleep attacks, cataplexy (sudden loss of muscle control), hypnagogic hallucinations (vivid perceptual experiences while falling asleep), sleep paralysis (a temporary inability to move or to speak that happens in the transition from sleeping to the waking state), and disturbed nocturnal sleep patterns 1. Narcolepsy doesn’t cause serious or long-term physical health problems, but it can have a significant impact on daily life and be difficult to cope with emotionally.
Narcolepsy can impact nearly every aspect of your life. Narcolepsy is dangerous because you can have excessive sleepiness or a sleep attack at any time of the day, in the middle of any activity including eating, walking or driving. Operating a vehicle with untreated narcolepsy can be very dangerous and some states even have laws against it.
Clinical features of narcolepsy usually begin in the teens or twenties, although diagnosis may be established years later. Onset after 50 years of age is unusual. The classic symptoms of narcolepsy are:
- excessive daytime sleepiness – feeling very drowsy throughout the day, and having difficulty concentrating and staying awake;
- cataplexy – temporary loss of muscle control resulting in weakness and possible collapse, often in response to emotions such as laughter and anger;
- hallucinations upon falling asleep (hypnagogic hallucinations) and/or upon awakening (hypnopompic hallucinations);
- sleep paralysis – a generalized temporary inability to move or speak when waking up or falling asleep;
- sleep attacks – falling asleep suddenly and without warning
Many people with narcolepsy do not know they have the sleep disorder. In general, narcolepsy affects 1 in 3,000 individuals 2. The overall prevalence of narcolepsy in the general population of the United States and Europe is about 0.05 percent 3. The prevalence varies worldwide from less than 0.02 percent of the population in Israel, to about 0.15 percent of the population in Japan 4. Narcolepsy may run in some families, but most cases are not genetic. The disorder is extremely rare in children. The cause of narcolepsy is still unknown, but recent research suggests that many people with narcolepsy with cataplexy have low levels of the neurotransmitter hypocretin, a chemical that regulates arousal, wakefulness and appetite.
Specific genetic factors are thought to contribute to narcolepsy. First-degree relatives of narcoleptic patients have a 20-40-fold increased risk of experiencing narcolepsy with cataplexy, indicating that it has a genetic component 5.
A number of studies have shown that narcolepsy has a negative social, psychological, economic, educational, and vocational effect on people with the condition, and a negative socioeconomic impact on their partner 6. As there is no known cure, current treatments for narcolepsy aim to improve symptoms 7.
Although the specific mechanisms of narcolepsy are not fully understood, recent studies demonstrate that narcolepsy with cataplexy is secondary to the loss of hypocretin neurons in the hypothalamus and is associated with human HLA DQB1*0602, and could be autoimmune 1. The prevalence of narcolepsy with cataplexy ranges between 25 and 50 per 100,000 people worldwide 8.
Narcolepsy affects both genders and typically begins between age 15 and 24, although it has been found in children as young as 5 years old. The age at onset varies from early childhood to mid-adulthood and has a bimodal distribution with an early peak of the disease at 14.7 years and a late peak at 35 years 9. Narcolepsy rarely develops after age 40.
According to the International Sleep Disorder Classification-3rd edition, narcolepsy can be divided into two groups:
- Narcolepsy Type I (narcolepsy with cataplexy)– a disorder diagnosed by excessive daytime sleepiness, with definite cataplexy and positive mean sleep latency result (the interval from the start of each test to the first epoch of sleep) of <8 minutes and ≥2 sleep-onset REM periods), or low CSF hypocretin-1 (<110pg/ml or 1</3 mean value of normal subjects with the same assay). This type of narcolepsy involves a combination of excessive daytime sleepiness and one or both of the following:
- Cataplexy is when you have attacks that cause a sudden loss of muscle tone while you are awake. It may lead to slurred speech and buckling knees, or in more severe cases complete paralysis. These events are usually triggered by strong emotions such as joy, surprise, laughter or anger.
- Low or absent CSF hypocretin-1 levels. Narcolepsy type 1 is caused by a deficiency of hypocretin (orexin). A patient with low hypocretin has narcolepsy type 1, even if they don’t exhibit cataplexy.
- Narcolepsy Type 2 (narcolepsy without cataplexy) – excessive daytime sleepiness and positive mean sleep latency in the absence of cataplexy 10. You may take a nap for a couple of hours and wake up feeling refreshed. But after a short time, you feel tired again. This type of narcolepsy occurs when you have continuous excessive sleepiness but no cataplexy. Narcolepsy without Cataplexy (Narcolepsy Type 2) is diagnosed when the patient presents with hypnagogic hallucinations and/or sleep-onset paralysis, and when polysomnography reveals the presence of sleep-onset REM periods (suggestive of narcolepsy) without conclusive evidence of cataplexy 11.This may either be due to the fact that cataplexy has not yet fully developed in these patients or that their narcoleptic symptoms differ etiologically 12. If cataplexy develops, the disorder should be reclassified as narcolepsy with cataplexy.
When you add up the hours of total sleep time, people with narcolepsy don’t necessarily sleep any more than people who don’t have the sleep disorder. This is especially true when you consider that many people with narcolepsy often have difficulty sleeping through the night because of unwanted awakenings.
Some people assume that because they are consistently tired during the day, that they may have narcolepsy. Other sleep disorders that cause daytime sleepiness are often mistaken for narcolepsy. These include sleep apnea, circadian rhythm sleep disorders and restless legs syndrome. Medical conditions, mental health disorders and use of certain medications or substances can also cause symptoms similar to narcolepsy.
Impact of narcolepsy on sleep
The total time someone with narcolepsy spends sleeping isn’t necessarily different from that of people who do not have the condition. However, narcolepsy can significantly affect sleep cycles and decrease the quality of sleep.
Sleep consists of cycles of different brain activity known as non-rapid eye movement (NREM) and rapid eye movement (REM). During REM sleep, brain activity increases and dreaming may occur.
Normal sleep consists of three stages of NREM sleep at first, followed by a short period of REM sleep, with NREM and REM sleep then alternating throughout the night. During the latter part of the night, REM sleep is more prominent.
If you have narcolepsy, this pattern is much more fragmented and you may wake several times during the night. You may also experience REM sleep much earlier than normal after falling asleep, and may experience effects of REM sleep, such as dreaming and paralysis, while you’re still conscious.
Do I have narcolepsy ?
Narcolepsy – Self-Tests
- Have you had the sudden urge to sleep during the day even though you’re getting enough sleep at night?
- Have you fallen asleep while working, eating or speaking with someone?
- Have you felt alert after a brief nap but then the alertness quickly changes to sleepiness?
If you answer yes to any of these questions, there is a chance that you have narcolepsy. Since narcolepsy is not a common sleep problem, many primary care physicians have difficulty diagnosing the sleep disorder. A board-certified sleep medicine physician can help make the proper diagnosis. Schedule an appointment with a sleep medicine physician. He or she will perform a combination of the tests to help determine if you have narcolepsy.
Normal sleep pattern vs. narcolepsy
The normal process of falling asleep begins with a phase called non-rapid eye movement (NREM) sleep. During this phase, your brain waves slow considerably. After an hour or so of NREM sleep, your brain activity changes, and REM sleep begins. Most dreaming occurs during REM sleep.
In narcolepsy, however, you may suddenly enter into REM sleep without first experiencing NREM sleep, both at night and during the day. Some of the characteristics of REM sleep, such as cataplexy, sleep paralysis and hallucinations, occur during wakefulness or drowsiness in people with narcolepsy.
Narcolepsy complications
Public misunderstanding of the condition
Narcolepsy may cause serious problems for you professionally and personally. Others might see you as lazy or lethargic. Your performance may suffer at school or work.
Interference with intimate relationships
Extreme sleepiness may cause low sex drive or impotence, and people with narcolepsy may even fall asleep while having sex. Intense feelings, such as anger or joy, can trigger some signs of narcolepsy such as cataplexy, causing affected people to withdraw from emotional interactions.
Physical harm
Sleep attacks may result in physical harm to people with narcolepsy. You’re at increased risk of a car accident if you have an attack while driving. Your risk of cuts and burns is greater if you fall asleep while preparing food.
Obesity
People with narcolepsy are more likely to be overweight. The weight gain may be related to medications, inactivity, binge eating, hypocretin deficiency or a combination of factors.
Narcolepsy causes
Many cases of narcolepsy are caused by a lack of the brain chemical hypocretin (also known as orexin), which regulates wakefulness and Rapid Eye Movement (REM) sleep 13.
Hypocretin levels are particularly low in those who experience cataplexy. Exactly what causes the loss of hypocretin-producing cells in the brain isn’t known, but experts suspect it’s due to an autoimmune reaction. In 2010 scientists in Switzerland discovered that some people with narcolepsy produce antibodies against a protein called trib 2. Trib 2 is produced by an area of the brain that also produces hypocretin. This results in a lack of hypocretin, which means the brain is less able to regulate sleep cycles. Current evidence demonstrates the loss of some or all of the almost 100,000 hypocretin-containing hypothalamic neurons in patients who have narcolepsy with cataplexy 14, 15, 16, 17, 2. These research results may help explain the cause of narcolepsy in many cases, but it doesn’t explain why some people with the condition still produce near-normal levels of hypocretin.
This hypocretin deficiency is thought to result from the immune system mistakenly attacking parts of the brain cells that produce hypocretin or the receptors that allow it to work. However, a lack of hypocretin doesn’t explain all cases of narcolepsy, and the exact cause of the problem is often unclear.
Things that have been suggested as possible triggers of narcolepsy include:
- hormonal changes, which can occur during puberty or the menopause
- major psychological stress
- an infection, such as swine flu, or the medication used to vaccinate against it (Pandermix)
Immune system problem
Normally, antibodies are released by the body to destroy disease-carrying organisms and toxins. When antibodies mistakenly attack healthy cells and tissue, it’s known as an autoimmune response.
In 2010 scientists in Switzerland discovered that some people with narcolepsy produce antibodies against a protein called trib 2.
Trib 2 is produced by an area of the brain that also produces hypocretin. This results in a lack of hypocretin, which means the brain is less able to regulate sleep cycles.
These research results may help explain the cause of narcolepsy in many cases, but it doesn’t explain why some people with the condition still produce near-normal levels of hypocretin.
Possible triggers
A number of factors may increase a person’s risk of narcolepsy or cause an autoimmune problem, including:
- an inherited genetic fault. In some cases, genetics may play a role.
- hormonal changes, including those that occur during puberty or the menopause
- major psychological stress
- a sudden change in sleep patterns
- an infection, such as swine flu or a streptococcal infection
- having the flu vaccine Pandemrix
Research is yet to confirm whether all of these play a role in narcolepsy.
Pandemrix vaccine
Recent research has shown an association between the use of the flu vaccine, Pandemrix, which was used during the swine flu epidemic of 2009-10, and narcolepsy in children.
However, the risk is very small. Researchers estimate the chance of developing narcolepsy after receiving a dose of the vaccine is around 1 in 52,000 in the UK.
As a result of the findings, Pandemrix is no longer given to people under the age of 20.
Swine flu and H1N1 vaccine
Research indicates a possible association with exposure to the H1N1 virus (swine flu) and a certain form of H1N1 vaccine that’s currently administered in Europe. It’s not yet known if the virus directly triggers narcolepsy or whether exposure to the virus increases the likelihood that someone will have narcolepsy.
Secondary narcolepsy
Narcolepsy can sometimes occur as a result of an underlying condition that damages the areas of the brain that produce hypocretin.
For example, narcolepsy can sometimes develop after:
- a head injury
- a brain tumor
- multiple sclerosis (MS)
- encephalitis
Narcolepsy caused by an identifiable underlying condition is known as secondary narcolepsy.
Narcolepsy signs and symptoms
Symptoms of narcolepsy usually begin between the ages of 15 to 25, but it is possible start experiencing symptoms at a much younger or older age. Not everyone with narcolepsy experiences the same symptoms. Some experience them regularly, while others are less frequently affected.
Symptoms may develop slowly over a number of years, or suddenly over the course of a few weeks.
Narcolepsy is usually a long-term (chronic) condition, although some of the symptoms may improve as you get older.
You may experience the following:
Excessive daytime sleepiness
The primary symptom of narcolepsy is excessive daytime sleepiness. You may feel tired during the day even though you had a full night’s sleep. This sleepiness is difficult to prevent and may vary over the course of the day. After a brief nap, you may feel alert, but the sleepiness will return after an hour or two.
This can have a significant impact on everyday life. Feeling drowsy throughout the day and struggling to stay awake makes it difficult to concentrate at work or school. People with narcolepsy may be misjudged as being lazy or rude.
Sleep attacks
Sleep attacks – falling asleep suddenly and without warning – are also common in people with narcolepsy. They may occur at any time.
The length of time a sleep attack lasts will vary from person to person. Some people will only have “microsleeps” lasting a few seconds, whereas others may fall asleep for several minutes.
If narcolepsy isn’t well controlled, sleep attacks may happen several times a day.
Hallucinations
Some patients with narcolepsy have vivid hallucinations at sleep onset. These hypnagogic hallucinations are usually visions that someone or something is present in your bedroom. It can feel very real, and trigger feelings of fear or dread. Other common visions may include being caught in a fire or flying through the air. These experiences are mainly visual, though they may also involve your senses of sound, touch, taste and smell.
Sleep paralysis
You might lose the ability to move or speak and feel paralyzed when you are falling asleep or waking up. This usually lasts a few seconds or minutes. This can be frightening, but it is not associated with an inability to breathe. Sleep paralysis can sometimes be paired with hallucinations, which are especially upsetting.
Disturbed nighttime sleep
About half of people with narcolepsy have problems sleeping through the night. You may wake up frequently and have difficulty falling back to sleep.
Memory problems
You may have trouble remembering things that people tell you because you were not fully awake at the time. Memory lapses also happen when sleepiness sets in as you are doing activities that do not require much thought.
Sudden loss in muscle tone (cataplexy)
This only occurs if you have narcolepsy with cataplexy (sudden, temporary muscle weakness or loss of muscular control). Cataplexy attacks are usually triggered by an emotion, such as excitement, laughter, anger or surprise. Attacks can last from a few seconds to several minutes. This can happen when you are surprised, elated or even intimate with a partner. You may slur your speech or lose control of your limbs, or you may become completely paralyzed.
Typical symptoms of cataplexy are:
- the jaw dropping
- the head slumping down
- legs collapsing uncontrollably
- slurred speech
- double vision or finding it difficult to focus
Some people with narcolepsy have cataplexy attacks once or twice a year, while others experience them several times a day. In an attempt to avoid attacks, some people may become emotionally withdrawn and socially isolated.
Narcolepsy with cataplexy is frequently linked to increased weight, sometimes obesity. It is possible to have narcolepsy along with another sleep disorder, such as sleep apnea or REM sleep behavior disorder.
Other symptoms
As well as the symptoms described above, narcolepsy can cause a number of other symptoms, including:
- headaches
- restless sleep – for example, having hot flushes, waking up frequently, having vivid nightmares, or physically acting out dreams
- automatic behavior – continuing with an activity without having any recollection of it afterwards
- depression
Narcolepsy diagnosis
Narcolepsy can usually be diagnosed by observing how you sleep and ruling out other conditions.
Your doctor will take a close look at your medical and family history. They will ask about your sleeping habits and any other symptoms you are experiencing.
If you think you may have narcolepsy, you should see your doctor. Before your appointment, it may be useful to record your symptoms in a diary or complete an Epworth sleepiness questionnaire (see Figure 1 below).
Although some patients present with the symptom of daytime sleepiness, most are far sleepier than they realize. Questionnaires such as the Stanford Sleepiness Scale and the Epworth Sleepiness Scale (Figure 1) are validated, patient-completed assessments of daytime sleepiness that can be used as screening tests. A test score in excess of 12 on the Epworth Sleepiness Scale or a patient history of falling asleep while driving are clear indications that further evaluation and work-up are required.
Referral to a sleep clinic is indicated if narcolepsy is suspected. The typical sequence of testing for suspected narcolepsy is one to two weeks of a sleep log or actigraphy to document sleep duration, followed by polysomnography to evaluate for other sleep disorders and document adequate sleep time, and concluding the next day with a multiple sleep latency test. The multiple sleep latency test is a daytime nap test to objectively assess for sleepiness and for onset of rapid eye movement (REM) sleep during naps. The combination of a mean sleep latency of less than eight minutes plus at least two naps with early onset REM sleep supports a diagnosis of narcolepsy 18.
Figure 1. Epworth Sleepiness Scale Questionnaire
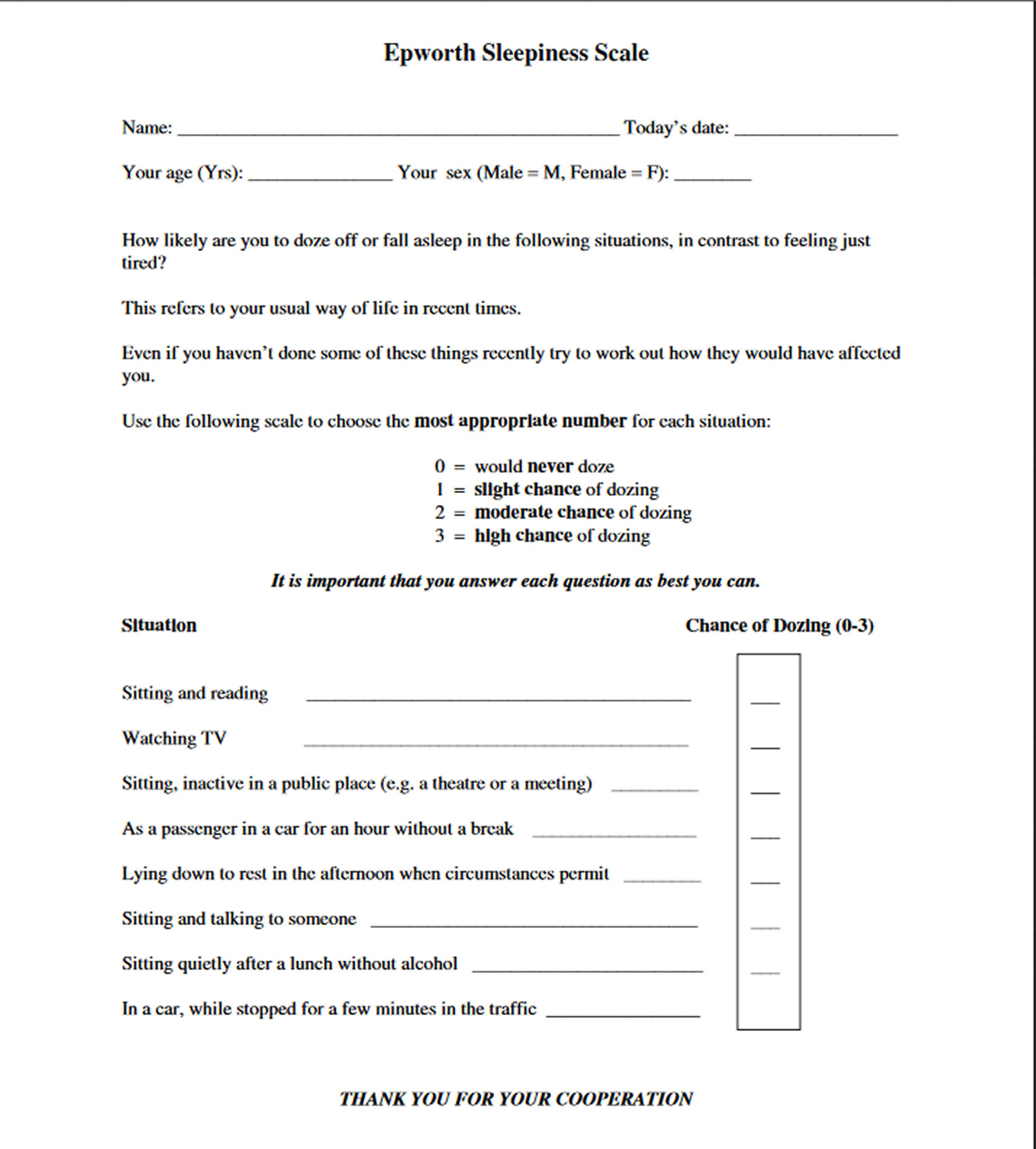
How to score the Epworth Sleepiness Scale
All Epworth Sleepiness Scale item-scores are intended to be integers (0-3). However, some people cannot decide on one number and report half-values. It is recommended that these scores be taken at face value. If, after adding them up, the total Epworth Sleepiness Scale score includes a half, it should be rounded up to the next whole number. If one or more item-scores are missing, that Epworth Sleepiness Scale is invalid because it is not feasible to interpolate missing item-scores. The Epworth Sleepiness Scale score (the sum of 8 item-scores) is the only number required under most circumstances.
- If total score less than 8 – indicates reported normal daytime alertness
- 8 to 11 – indicates mild sleepiness
- 12 to 15 – indicates moderate sleepiness
- 16 to 24 – indicates severe sleepiness
Narcolepsy test
Formal diagnosis may require staying overnight at a sleep center, where you undergo an in-depth analysis of your sleep by sleep specialists. Methods of diagnosing narcolepsy and determining its severity include:
- Sleep history. Your doctor will ask you for a detailed sleep history. A part of the history involves filling out the Epworth Sleepiness Scale, which uses a series of short questions to gauge your degree of sleepiness. For instance, you indicate on a numbered scale how likely it is that you would doze off in certain situations, such as sitting down after lunch.
- Sleep records. You may be asked to keep a detailed diary of your sleep pattern for a week or two, so your doctor can compare how your sleep pattern and alertness are related. Often, in addition to this sleep log, the doctor will ask you to wear an actigraph. This device has the look and feel of a wristwatch. It measures periods of activity and rest and provides an indirect measure of how and when you sleep.
- Polysomnography. This test measures a variety of signals during sleep using electrodes placed on your scalp. For this test, you must spend a night at a medical facility. The test measures the electrical activity of your brain (electroencephalogram) and heart (electrocardiogram) and the movement of your muscles (electromyogram) and eyes (electro-oculogram). It also monitors your breathing.
- Multiple sleep latency test. Also known as a daytime nap study, the Multiple Sleep Latency Test measures your daytime sleepiness by measuring how quickly you fall asleep in a quiet environment during the day. The test requires you to attempt to take multiple naps in a sleep lab at set times throughout the day. It is used to see how quickly you fall asleep in quiet daytime situations. For each nap trial you are asked to lie quietly in bed in a dark room and try to go to sleep. Most people with narcolepsy fall asleep in an average of three minutes during the multiple sleep latency test. The Multiple Sleep Latency Test is a full-day test that consists of five scheduled naps separated by two-hour breaks. During each nap trial, you will lie quietly in bed and try to go to sleep. Once the lights go off, the test will measure how long it takes for you to fall asleep. You will be awakened after sleeping 15 minutes. If you do not fall asleep within 20 minutes, the nap trial will end. Each nap will be taken in a dark and quiet sleep environment that is intended for your comfort and to isolate any external factors that may affect your ability to fall asleep. A series of sensors will measure whether you are asleep. The sensors also determine your sleep stage. People who have narcolepsy fall asleep easily and enter into rapid eye movement (REM) sleep quickly.
- You may also have a blood test to find out whether you have a genetic marker known as HLA DQB *0602, which is associated with narcolepsy. A positive result supports a diagnosis, but doesn’t make it 100% certain – 30% of people without narcolepsy also have the genetic marker.
- Measuring hypocretin (orexin) levels. Many cases of narcolepsy are linked to a deficiency in the sleep-regulating brain chemical hypocretin, also known as orexin. Recent research has shown that measuring the level of hypocretin in your cerebrospinal fluid, which surrounds the brain and spinal cord, can be useful in diagnosing narcolepsy. To measure your level of hypocretin, a sample of cerebrospinal fluid is removed using a needle during a procedure called a lumbar puncture. This test is increasingly being used by sleep disorder specialists to help make a diagnosis.
These tests can also help doctors rule out other possible causes of your signs and symptoms. Other sleep disorders, such as sleep apnea, can cause excessive daytime sleepiness.
Polysomnography
Polysomnography is an investigation of your sleep carried out at a specialist sleep center. The study usually involves staying overnight at the sleep centre so your sleeping patterns can be analysed.
During the night, several different parts of your body will be carefully monitored using electrodes and bands that are placed on the surface of your body while you sleep. Sensors will also be placed on your legs and an oxygen sensor is attached to your finger.
A number of different tests will be carried out during polysomnography, including:
- electroencephalography (EEG) – which monitors brain waves
- electrooculography – which monitors eye movements
- electromyography (EMG) – which monitors muscle tone
- recordings of movements in your chest and abdomen
- recordings of airflow through your mouth and nose
- pulse oximetry – which measures your heart rate and blood oxygen levels
- electrocardiography (ECG) – which monitors your heart
Sound recording and video equipment may also be used to record sound and images.
After you have slept, a specialist will analyze your test results to determine whether you have normal brain wave activity, breathing patterns, and muscle and eye movement.
Figure 2. Polysomnography recordings of the characteristics of sleep onset in a normal subject vs. a patient with narcolepsy.
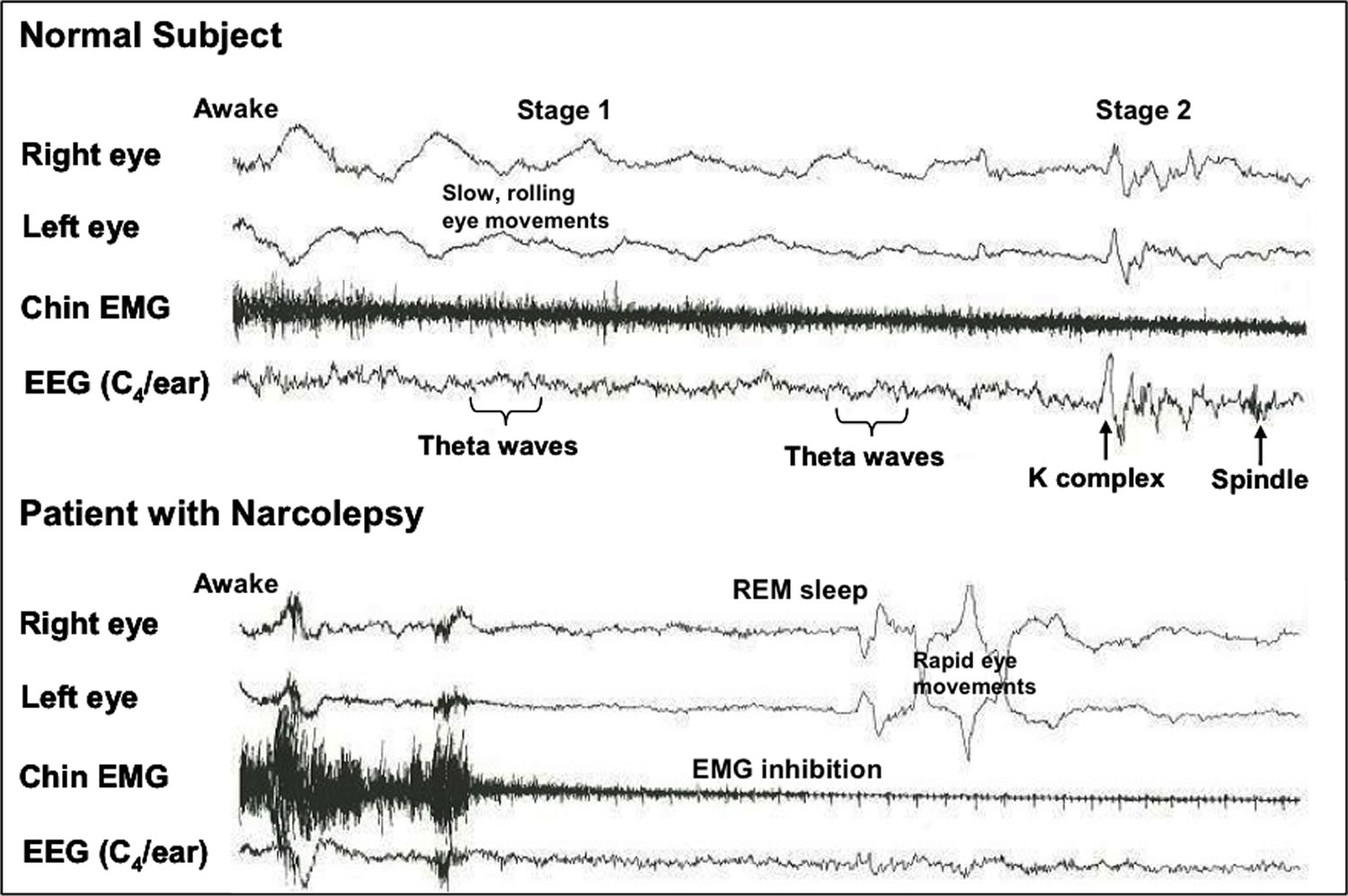
Note: Sleep onset in a normal subject and in a patient with narcolepsy. Note how the normal subject goes from awake to stage 1 (slow eye movements, gradual reduction of chin EMG, theta waves in the EEG) and then to stage 2 (K complexes and sleep spindle). The patient with narcolepsy changes immediately from wakefulness to REM sleep (rapid eye movements, sudden decrease in chin EMG and sawtooth waves in the EEG) 19.
Narcolepsy treatment
There is no cure for narcolepsy, but medications and lifestyle modifications can help you manage the symptoms.
Narcolepsy medications
Central nervous system stimulants are the main treatments used for excessive daytime sleepiness in narcolepsy, and these stimulants include Amphetamine, Methylphenidate, Modafinil, Dextroamphetamine and Armodafinil. (It should be noted that the FDA issued an alert in 2007 for Modafinil, citing severe adverse skin reactions). Another drug used to treat narcolepsy is Atomoxetine, an NRI (Norepinephrine Reuptake Inhibitor) and non-stimulant, which has no recreational effects or addiction liability.
Successful treatment depends on developing an acceptable balance between the stimulants’ wake-promoting effects and their side-effects (e.g., anxiety, tremors, and anorexia). Modafinil or its R-enantiomer, armodafinil (both wakefulness-promoting agents) is currently the initial treatment of choice due to its proven efficacy, favorable side effect profile, and low potential for abuse 20. Armodafinil maintains higher plasma concentrations later in the day, which may result in improved wakefulness 21.
If treatment with modafinil or armodafinil is unsuccessful, stimulants such as methylphenidate or dextroamphetamine may be prescribed, often in their extended-release formulations 22.
Sodium Oxybate (Xyrem®), or SGH (Sodium Gamma Hydroxybutyrate) is another approved treatment option for narcolepsy. This treatment can be used for excessive daytime sleepiness and cataplexy associated with narcolepsy. It is a strong sleep-inducing agent and can be used if cataplexy remains despite therapy with stimulants. Sodium oxybate’s common side effects include dizziness, headache, nausea, vomiting, confusion, and urinary incontinence. Long-term treatment efficacy with no evidence of tolerance to cataplectic effects has been demonstrated 23.
Specific serotonin reuptake inhibitors (SSRIs) (e.g., fluoxetine and paroxetine) and tricyclic antidepressants (e.g., clomipramine and imipramine) are often used to treat narcolepsy, in addition to other drugs that suppress REM sleep. An antidepressant known to block the reuptake of norepinephrine and serotonin, known as Venlafaxine, has also shown some usefulness in managing the symptoms of cataplexy; however, sleep disruption is just one of its notable side-effects. They may also decrease hypnagogic hallucinations and sleep paralysis 24. However, they have not been approved by the Food and Drug Administration for this indication. As a class, specific serotonin reuptake inhibitors are less effective anti-cataplectics than tricyclic antidepressants, but are safer and better tolerated 24.
Medications for narcolepsy include:
- Stimulants. Drugs that stimulate the central nervous system are the primary treatment to help people with narcolepsy stay awake during the day. Doctors often try modafinil (Provigil) or armodafinil (Nuvigil) first for narcolepsy because it isn’t as addictive as older stimulants and doesn’t produce the highs and lows often associated with older stimulants. Side effects of modafinil are uncommon, but they may include headache, nausea or dry mouth. Some people need treatment with methylphenidate (Aptensio XR, Concerta, Ritalin) or various amphetamines. These medications are very effective but may sometimes cause side effects such as nervousness and heart palpitations and can be addictive.
- Selective serotonin reuptake inhibitors (SSRIs) or serotonin and norepinephrine reuptake inhibitors (SNRIs). Doctors often prescribe these medications, which suppress REM sleep, to help alleviate the symptoms of cataplexy, hypnagogic hallucinations and sleep paralysis. They include fluoxetine (Prozac, Sarafem, Selfemra) and venlafaxine (Effexor XR). Side effects can include weight gain, sexual dysfunction and digestive problems.
Tricyclic antidepressants. These older antidepressants, such as protriptyline (Vivactil), imipramine (Tofranil) and clomipramine (Anafranil), are effective for cataplexy, but many people complain of side effects, such as dry mouth and lightheadedness. - Sodium oxybate (Xyrem). This medication is highly effective for both daytime sleepiness and cataplexy. Sodium oxybate helps to improve nighttime sleep, which is often poor in narcolepsy. In high doses it may also help control daytime sleepiness. It must be taken in two doses because of its short half-life, one at bedtime and one up to four hours later. Xyrem can have side effects, such as nausea, bed-wetting and worsening of sleepwalking. Taking sodium oxybate together with other sleeping medications, narcotic pain relievers or alcohol can lead to difficulty breathing, coma and death.
If you have other health problems, such as high blood pressure or diabetes, ask your doctor how the medications you take for your other conditions may interact with those taken for narcolepsy.
Certain over-the-counter drugs, such as allergy and cold medications, can cause drowsiness. If you have narcolepsy, your doctor will likely recommend that you avoid taking these medications.
Emerging treatments being investigated for narcolepsy include hypocretin replacement, hypocretin gene therapy and immunotherapy, but further research is needed before any may be available in clinical practice.
Lifestyle and home remedies
Lifestyle modifications are important in managing the symptoms of narcolepsy. You may benefit from these steps:
- Stick to a strict bedtime routine. Go to sleep and wake up at the same time every day, including weekends.
- Take frequent, brief naps. Schedule short naps at regular intervals during the day. Naps of 20 minutes at strategic times during the day may be refreshing and reduce sleepiness for one to three hours. Some people may need longer naps.
- Avoid nicotine and alcohol. Using these substances, especially at night, can worsen your signs and symptoms.
- Avoiding caffeine (found in coffee, tea and some fizzy drinks) and smoking before going to bed
- Get regular exercise. Moderate, regular exercise at least four to five hours before bedtime may help you feel more awake during the day and sleep better at night.
- Relaxing before going to bed – have a warm bath, for example.
- Keeping your bedroom at a comfortable temperature, quiet and free from distractions.
- Not exercising too close to bedtime – leave at least two hours between finishing exercise and going to bed.
- Not eating large, heavy meals before going to bed.
- Some over-the-counter medications, such as cold and allergy medicines, can cause drowsiness as a side effect.
You should avoid taking these types of medicines during the day if you have narcolepsy as they may make your daytime drowsiness worse.
Speak to your doctor or pharmacist if you’re unsure about which medicines cause drowsiness. They may be able to recommend non-drowsy alternatives
Coping and support
Dealing with narcolepsy can be challenging. Making adjustments in your daily schedule may help. Consider these tips:
- Talk about it. Tell your employer or teachers about your condition and work with them to find ways to accommodate your needs. This may include taking naps during the day, breaking up monotonous tasks, recording meetings or classes, standing during meetings or lectures, and taking brisk walks at various times throughout the day. The Americans With Disabilities Act prohibits discrimination against workers with narcolepsy and requires employers to provide reasonable accommodation to qualified employees.
Talking to others
As well as being a difficult condition to live with, narcolepsy can be difficult for others to understand.
Some of the symptoms, such as sudden loss of muscle control (cataplexy), can also be frightening for people who are unaware of the condition. You may find it useful to talk to your friends and family about your condition.
Inform your child’s teachers if your child is diagnosed with narcolepsy. It’s important that teachers are aware of your child’s diagnosis so they don’t mistake their behaviour for laziness or staying up too late at night.
If you’re diagnosed with narcolepsy there’s no reason why you shouldn’t be able to work, as long as your employer is aware of your diagnosis and they agree to an approach that accommodates your sleep disorder, such as flexible working hours or allowing you to take planned naps. Some careers, however, won’t be suitable for you.
Your doctor or specialist may be able to arrange for you to speak to a social worker if they think it may help.
A social worker can offer counseling and support, including advice about careers, any adjustments that can be made at school or work, and any financial or relationship problems you may be having.
- Be safe. If you must drive a long distance, work with your doctor to establish a medication schedule that ensures the greatest likelihood of wakefulness during your drive. Stop for naps and exercise breaks whenever you feel drowsy. Don’t drive if you feel your sleepiness is not well-controlled.
Support groups and counseling can help you and your loved ones cope with narcolepsy. Ask your doctor to help you locate a group or qualified counselor in your area.
Narcolepsy in Special Groups
School-Aged Children
Children who have narcolepsy may have trouble studying, focusing, and remembering things. To help your child in school:
- Talk with your child’s teachers and school officials about your child’s narcolepsy and the best ways to meet his or her needs. For example, your child may need to take naps or walks during the day or tape the teacher’s lessons.
- Talk with the school nurse about your child’s narcolepsy and medicines. Together you can work out a place to keep the medicines and a schedule for taking them at school.
Pregnant Women
If you’re pregnant or planning a pregnancy, ask your doctor whether you should continue taking your narcolepsy medicines. Certain medicines may interfere with your pregnancy.
- De la Herrán-Arita AK, García-García F. Narcolepsy as an immune-mediated disease. Sleep Disorders 2014. https://www.hindawi.com/journals/sd/2014/792687/[↩][↩]
- Leschziner, G, Narcolepsy: a Clinical Review, Pract Neurol 2014; 0:1–9. doi:10.1136/practneurol-2014-000837.[↩][↩]
- Malik S, Boeve BF, Krahn LE, Silber MH. Narcolepsy associated with other central nervous system disorders. Neurology. 2001;57:539-541.[↩]
- Martinez-Rodriguez JE, Lin L, Iranzo A, et al. Decreased hypocretin-1 (Orexin-A) levels in the cerebrospinal fluid of patients with myotonic dystrophy and excessive daytime sleepiness. Sleep. 2003;26:287-290.[↩]
- Mignot E. Genetic and familial aspects of narcolepsy. Neurology. 1998;50:S16-22.[↩]
- Jennum P, Ibsen R, Petersen ER, Knudsen S, Kjellberg J. Health, social, and economic consequences of narcolepsy: a controlled national study evaluating the societal effect on patients and their partners. Sleep Medicine 2012;13(8):1086-93. https://www.ncbi.nlm.nih.gov/pubmed/22841027[↩]
- Ahmed I, Thorpy M. Clinical features, diagnosis and treatment of narcolepsy. Clinics in Chest Medicine 2010;31(2):371-81. https://www.ncbi.nlm.nih.gov/pubmed/20488294[↩]
- Longstreth WT Jr, Koepsell TD, Ton TG, Hendrickson AF, van Belle G. The epidemiology of narcolepsy. Sleep 2007;30(1):13-26. https://www.ncbi.nlm.nih.gov/pubmed/17310860[↩]
- Dauvilliers Y, Montplaisir J, Molinari N, Carlander B, Ondze B, Besset A, et al. Age at onset of narcolepsy in two large populations of patients in France and Quebec. Neurology 2001;57(11):2029-33. https://www.ncbi.nlm.nih.gov/pubmed/11739821[↩]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders. 3rd Edition. American Academy of Sleep Medicine, 2014.[↩]
- American Academy of Sleep Medicine (AASM), The International Classification of Sleep Disorders: Diagnostic and Coding Manual (3rd edition): ISCD-3, Darien, IL: AASM, 2014.[↩]
- Yoss RE, Daly DD. Criteria for the diagnosis of the narcoleptic syndrome. Mayo Clin Proc. 1957;32:320-328.[↩]
- S. Nishino, B. Ripley, S. Overeem, G. J. Lammers, and E. Mignot, “Hypocretin (orexin) deficiency in human narcolepsy,” The Lancet, vol. 355, no. 9197, pp. 39–40, 2000.[↩]
- Nishino S, Ripley B, Overeem S, et al. Hypocretin (orexin) deficiency in human narcolepsy (letter). Lancet. 2000;355:39-40.[↩]
- Mignot E, Lammers GJ, Ripley B, et al. The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias. Arch Neurol. 2002;59:1553-1562.[↩]
- Thannickal TC, Moore RV, Nienhuis R, et al. Reduced number of hypocretin neurons in human narcolepsy. Neuron. 2000;27:469-474.[↩]
- Hungs M, Lin L, Okun M, Mignot E. Polymorphisms in the vicinity of the hypocretin/orexin are not associated with human narcolepsy. Neurology. 2001;57:1893-1895.[↩]
- The International Classification of Sleep Disorders: Diagnostic and Coding Manual. 2nd ed. Westchester, Ill.: American Academy of Sleep Medicine; 2005.[↩]
- Mignot E, “Narcolepsy: Pharmacology, Pathophysiology, and Genetics,” In Kryger M, Roth T, Dement W (ed.), Principles and Practice of Sleep Medicine (5th Edition), St. Louis: Elsevier Saunders, 2011, pages 938-956.[↩]
- US Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil as a treatment for excessive daytime somnolence in narcolepsy. Neurology. 2000;54:1166-1175.[↩]
- National Sleep Foundation, “Sleep Related Problems: Narcolepsy and Sleep,” Arlington, VA: NSF, no date. Online at: http://sleepfoundation.org/sleep-topics/sleep-related-problems.[↩]
- Silber MH, Krahn LE, Morgenthaler TJ. Sleep Medicine in Clinical Practice. London, England: Taylor and Francis; 2004.[↩]
- US Xyrem Multicenter Study Group. A randomized, double blind, placebo-controlled multicenter trial comparing the effects of three doses of orally administered sodium oxybate with placebo for the treatment of narcolepsy. Sleep. 2002;25:42-49.[↩]
- Guilleminault C and M Fromherz, “Narcolepsy: Diagnosis and Management,” In Kryger M, Roth T, Dement W (ed.), Principles and Practice of Sleep Medicine (5th Edition), St. Louis: Elsevier Saunders, 2011, pages 957-968.[↩][↩]





{kind=link}