
Contents
What is SIBO
SIBO or Small Intestinal Bacterial Overgrowth is defined as the presence of an abnormally high number of coliform bacteria in the small bowel 1.
Human gut harbor 1014 bacterial cells, which are 10 times higher than the number of cells in the human body 2. Gastrointestinal (GI) tract is considered as the most heavily colonized organ and more than 70% of microbes reside in colon 3. The human GI tract is inhabited by a vast number of microbial population including bacteria, fungi, and viruses 4. Bacteria contribute to the largest population of gut microbiota, consisting of 500 (using culture approaches) to 1,000 (by 16S rRNA gene sequencing) different bacterial species 5. The number of bacteria increases from stomach (101 to 103 bacteria/g) to the colon (1011 to 1012 bacteria/g) 3. The small intestine comprises mainly of Gram positive and aerobic bacteria and the large intestine contains predominantly Gram negative and anaerobic bacteria 6. Majority of bacteria residing in the colon are strictly anaerobes (95% of total) followed by facultative anaerobes and aerobes 5. More than 50 bacterial phyla have been identified in human gut 7. Major phyla residing in the gut are Bacteroidetes and Firmicutes, whilst Proteobacteria, Verrucomicrobia, Actino-bacteria, Fusobacteria, and Cyanobacteria are present in minor proportion 8.
Normal gut flora may provide several beneficial effects to the host. These include fermentation of un-digested dietary residue and endogenous mucus producing short chain fatty acids, which are nutrients to the colonic epithelial cells and conservation of energy, absorption of NaCl and water, particularly from the right colon, synthesis of vitamin K, control of epithelial cell proliferation, protection against pathogens by a barrier effect and training of the immune system 9. One study showed that small intestine of germ free animal has thin and irregular villi, reduced crypt size, increased number of Peyer’s patches, and infiltration of leukocytes in lamina propria 10. Alteration in the normal flora leads to disturbance in the intestinal homeostasis 11.
There are several intrinsic and extrinsic factors that prevent overgrowth of bacteria in the small intestine:
Intrinsic factors include 12, 13, 14:
- Secretion of gastric juice and bile, which have antibacterial effect;
- Peristaltic movement preventing adherence of bacteria into the intestinal mucosa;
- Normal gut defense including humoral and cellular mechanisms;
- Mucin production by intestinal mucosal epithelial cell inhibiting pathogenic bacteria;
- Gut antibacterial peptides such as defensins; and
- Ileocecal valve preventing retrograde translocation of bacteria from colon to the small intestine.
Extrinsic factors include 15:
- Diet and drugs modulating gut flora, such as pre and probiotics, gastric acid suppressants such as proton pump inhibitors (PPIs), H2 blockers, and antibiotics and drugs altering motility (prokinetics, anticholinergics, and opioids).
If, there is failure of any of the above-mentioned protective mechanisms, it may lead to development of SIBO (Figure 1).
Figure 1. Schematic diagram showing the frequency of small intestinal bacterial overgrowth (SIBO)
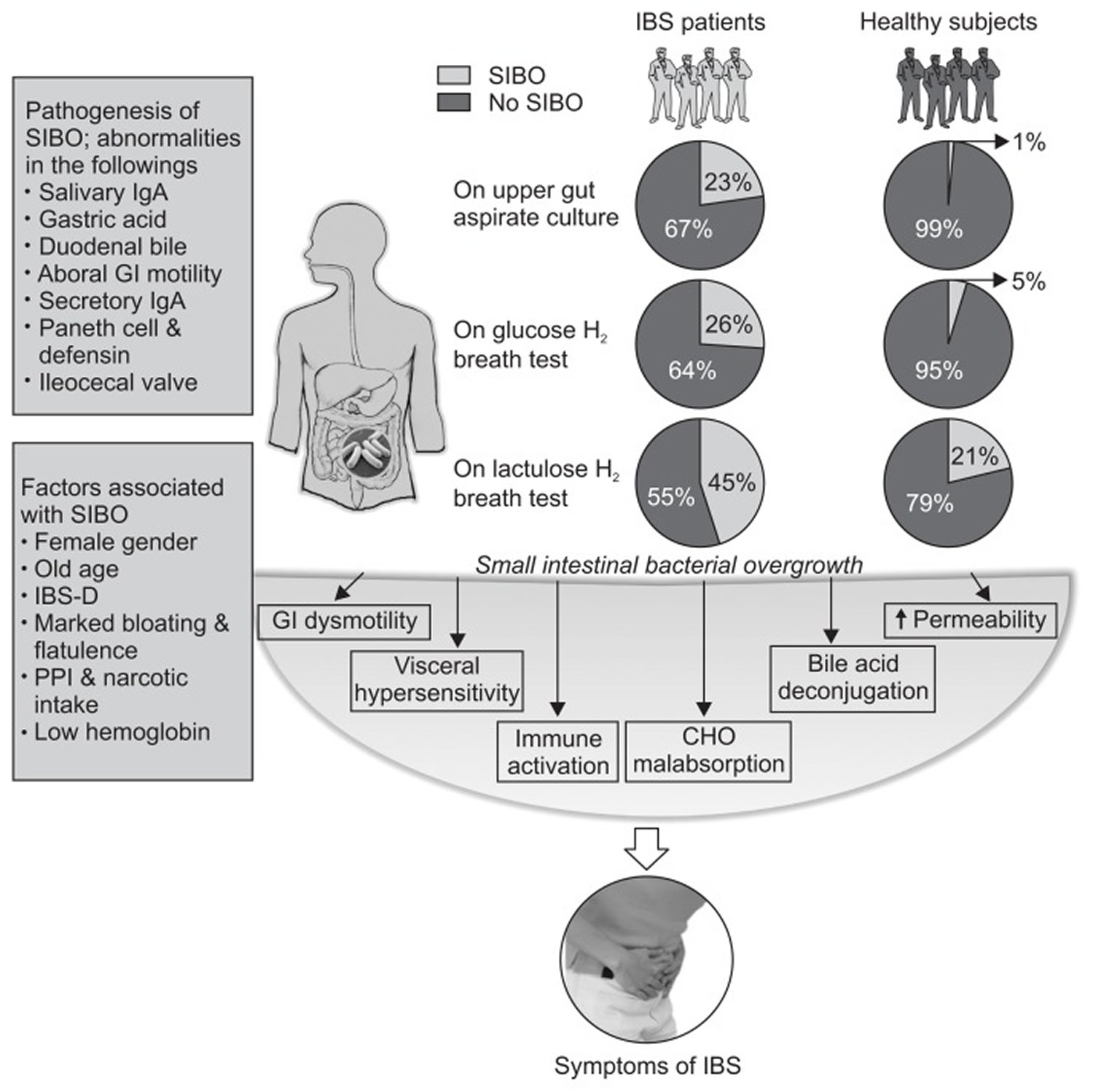
Note: Schematic diagram showing the frequency of small intestinal bacterial overgrowth (SIBO) using quantitative jejunal aspirate culture, glucose and lactulose hydrogen breath tests (GHBT and LHBT, respectively) among patients with irritable bowel syndrome (IBS), gut defense mechanisms that prevent the development of SIBO, factors associated with SIBO among patients with IBS, and mechanisms of IBS symptom development. As shown in the figure, the frequency of SIBO in IBS patients using LHBT (early-peak criteria) is higher than that by using upper gut aspirate culture and GHBT (LHBT [45%]; upper gut aspirate culture [23%] and GHBT [26%]). Moreover, SIBO is more frequent in healthy controls using LHBT due to false positive test results (LHBT [21%], upper gut aspirate culture [1%] and GHBT [5%]).
[Source 16]What Causes SIBO
Bacterial overgrowth occurs when intestinal stasis give the coliform bacteria the opportunity to proliferate locally. Mechanical stasis is an obvious cause of stasis in the gut and can be seen often in patients who have undergone previous gastrointestinal surgery. The classic of these is the surgical blind loop that allows for bacterial proliferation (see Table 1). Other prominent causes include diabetes, scleroderma, intestinal diverticulosis, afferent loop following a Billroth II gastrojenunostomy, and intestinal obstruction caused by strictures, adhesions, cancer and more recently irritable bowel syndrome (IBS). In addition, certain medications are associated with stasis and SIBO. For example, narcotics cause intestinal slowing and proton pump inhibitors (PPIs) reduce acid, which can lead to oral microbe penetration of the proximal gut [Lombardo et al. 2010; Compare et al. 2011; Hamvas, 2012].
Table 1. Causes of small intestinal bacterial overgrowth (SIBO)
| Causes | |
|---|---|
| Gastric achlorhydria | Due to long term use of a proton pump inhibitor 17 or autoimmune etiology (chronic atrophic gastritis) |
| Anatomic abnormality of the small intestine with stagnation | Afferent limb of Billroth II gastrojejunostomy, small intestine diverticula 18, obstruction, surgical blind loop, radiation enteritis |
| Small intestine motility disorder | Diabetic autonomic neuropathy, scleroderma, chronic intestinal pseudo-obstruction, small bowel diverticulosis, irritable bowel syndrome (IBS) 19 |
| Gastrocolic or coloenteric fistula | Crohn’s disease 20, malignancy, surgical resection |
| Miscellaneous | AIDS, chronic pancreatitis in 30–40% of cases 21, liver cirrhosis in up to 60% of patients, IgA deficiency, combined variable immunodeficiency, nonalchoholic steatohepatitis 22, fibromyalgia, celiac disease 23 |
Note: AIDS, acquired immunodeficiency syndrome; IgA, immunoglobulin A.
In evaluating the mechanism of diarrhea in bacterial overgrowth, it is essential to realize that it is multifactorial. Hypothetical mechanisms are the following:
- Bacteria digest carbohydrates, producing gas and osmotically active byproducts that promote osmotic diarrhea.
- Bacteria and fatty acid byproducts injure the mucosa and contribute to diarrhea.
- Mucosal injuries create lactase deficiencies.
- Bacterial deconjugation of bile salts interferes with fat absorption and the absorption of fat-soluble vitamins.
Most of these have not been determined by modern scientific method. However, the cause of SIBO also needs to be considered. For example, bowel obstruction or adhesions can cause bloating or distension in addition to SIBO.
SIBO Symptoms
Although the symptoms of bacterial overgrowth are well known (Table 2), there are few studies that aim to scientifically characterize the symptoms. Since SIBO can be due to a number of local and systemic disorders, the symptoms of SIBO are distorted by symptoms of the underlying condition (scleroderma is a good example). The clinical manifestations of SIBO depend upon the severity of disease. While one would assume that the greater the quantity of bacteria, the greater the symptom, this has not been well studied. In Billroth II subjects, where coliform counts are ≥1 × 105cfu/ml these patients often develop significant malabsorption as well as the typical symptoms of bloating. It is not clear if the malabsorption is due to the nature of the surgery, the level of bacteria or other consequences. However, it is now believed that most patients with bacterial overgrowth do not have clinical malnutrition caused by malabsorption. In these cases the typical symptoms are nonspecific, and include distention, flatulence and diarrhea. Only rare instances (mostly associated with jejunoileal bypass surgery or short bowel syndrome) result in vitamin and mineral deficiencies, including the fat-soluble vitamins A or D, vitamin B12 and iron.
Recently, data are accumulating to suggest that the most common association with SIBO is IBS and bacterial overgrowth may be part of the pathogenesis of this condition 24. In addition, SIBO has been reported with rosacea, a dermatological skin condition affecting the face 25. d-lactic acidosis is a severe complication of patients with short bowel syndrome (with intact large bowel). It is caused by an excessive overgrowth of lactobacilli. In clinically expressed cases, symptoms comprise characteristic neurologic abnormalities including confusion, cerebellar ataxia, slurred speech and loss of memory, and patients may exhibit some degree of altered mental status 26.
Table 2. SIBO (small intestinal bacterial overgrowth) symptoms and signs
| Nonspecific symptoms | Bloating, flatulence, abdominal discomfort, diarrhea, abdominal pain |
| Signs of malabsorption in extreme cases | Weight loss, steatorrhea, malnutrition, arthralgia |
| Clinical associations | Irritable bowel syndrome 27 |
| Rosacea 25 | |
| Restless leg syndrome 28 | |
| Deficiency syndromes | Macrocytic anemia (due to vitamin B12 deficiency) |
| Microcytic anemia due to bleeding from ulcers in stagnant intestinal loops 29 | |
| Tetany in hypocalcaemia induced by vitamin D deficiency | |
| Metabolic bone disease 30 | |
| Polyneuropathy due to vitamin B12 deficiency | |
| Other | d-Lactic acidosis- in patients with short bowel syndrome 31 |
SIBO Diagnostic Test
Though quantitative culture of the upper gut aspirate has traditionally been used as the gold standard for the diagnosis SIBO, its limitations include difficulty and invasiveness, cost, contamination by oropharyngeal flora, and inability to culture as high as 70% bacteria colonizing the gut 32. Moreover, distribution of bacterial overgrowth may be patchy and upper gut aspirate may not be able to detect bacterial overgrowth in distal gut 33. The anaerobic bacteria may not grow if air is used during endoscopy; hence, either nitrogen or carbon dioxide is better for this purpose. Hence, search for other less invasive and patient-friendly methods for diagnosis of SIBO continues.
In an attempt to overcome some of the limitations of the traditional culture-based method for diagnosis of SIBO, a novel technology, called culturomics, has been developed recently 34. Culturomics confer a new platform for identification of large number of bacterial colonies as well as noncultivable species in a short time duration using matrix-assisted laser desorption ionization time-of-flight (MALDI-TOF) 35. In a recent study, using 212 different culture conditions, 340 different bacterial, 5 fungal species and one virus were identified, including 31 new species using culturomics (MALDI-TOF) technique 36. Thus, culturomic approaches are feasible, rapid, cost-effective and reproducible for the study of gut microbiota 35. However, studies on SIBO using culturomics method are lacking. Moreover, use of effective culture conditions and sequencing methods may make it rarely usable for routine clinical application.
SIBO Breath Test
Breath tests are popular, noninvasive and patient-friendly methods used increasingly for diagnosis of SIBO 37. Diagnostic role of hydrogen breath tests depends on the type of the substrates used; for example, lactose and fructose hydrogen breath tests are useful for carbohydrate malabsorption; on the other hand, GHBT (glucose hydrogen breath test) and lactulose hydrogen breath tests (LHBT) are useful for diagnosis of SIBO, the former being more specific. Therefore, choice of the substrate while performing hydrogen breath test is important as only specific substrate diagnoses SIBO and others test for carbohydrate malabsorption 37.
Hydrogen and methane gases are produced by the gut flora from the ingested substrates, particularly the colonic flora in patients with carbohydrate malabsorption and from small bowel bacteria in patients with SIBO 38. Eighty percent of the gases like hydrogen and methane are eliminated with the flatus and the remaining 20% are absorbed and exhaled by lung, which can be measured in breath 39. In GHBT (glucose hydrogen breath test), rise in hydrogen by 12 parts per million (ppm) above basal following administration of 50 to 100 g glucose due to bacterial fermentation of the substrate in small intestine is diagnostic of SIBO 37. A recent study showed that measuring methane does not increase the yield of hydrogen breath test to diagnose SIBO 40. In presence of SIBO, two peaks may be seen during LHBT (lactulose hydrogen breath test): the first one due to bacterial fermentation of lactulose in small bowel and the second one after lactulose reaches colon 40. Since number of bacteria in colon is higher than that in the small bowel even in patients with SIBO, a rise in breath hydrogen more than 20 ppm above basal is expected from colonic fermentation of the lactulose 41. Though GHBT (glucose hydrogen breath test) is highly specific (78% to 97%) 42, it is quite insensitive (15.7% to 62%) 43. In contrast, conventional double-peak criteria on LHBT (lactulose hydrogen breath test) lack sensitivity (31% to 68%) and the recently proposed early-peak criterion (rise in breath hydrogen within 90 minutes by 20 ppm above basal following lactulose ingestion) often gives false positive result with specificity of 65% to 97.9% 44. This is the reason for overestimation of frequency SIBO (as high as 78%) in the initial studies from United States 41. In fact, the early-peak criterion on LHBT (lactulose hydrogen breath test), which was used in the initial studies on SIBO in patients with IBS, presumed that normal mouth to cecum transit time is more than 90 minutes in spite of the observation that it may be shorter 37. A study that combined radio-nuclide gut transit and LHBT (lactulose hydrogen breath test) revealed that in most patients in whom a peak in hydrogen was seen on LHBT, radio-nuclide already arrived in cecum 45. Other methods for diagnosis of SIBO include CO2 breath tests (14C or 13C D-xylose, 13C glucose and 13C cholylglycine hydrolase) 46, 47.
Though hydrogen breath tests are quite popular for the diagnosis of SIBO, these are not free from limitations. In patients with distal SIBO, GHBT (glucose hydrogen breath test) may be falsely negative as glucose gets completely absorbed in the proximal small bowel and hence, may not reach the site of SIBO. In patients with fast gut transit, early peak criteria proposed by Pimentel et al. 41 often give false positive results. Fast gut transit is not uncommon, particularly in Asia. In a study, median orocecal transit time in healthy subjects was 65 minutes (range, 40 to 110 minutes) 48. A Taiwanese study revealed that average orocecal transit time was 85±37 minutes 49. Hence, it is important to realize that there is need to search for a noninvasive yet sensitive and specific method for diagnosis of SIBO.
Sibo treatment
Treatment for SIBO is complex and must be individualized. The three main components in treating patients with SIBO are:
- Treat the underlying disease or condition.
- Eradicate overgrowth
- Address associated nutritional deficiencies.
It is important to address all causes, symptoms and complications associated with SIBO. Where physical causes are responsible, the best way to treat bacterial overgrowth is to correct the anatomic defect that has potentiated the overgrowth (e.g. adhesions, bowel obstruction, strictures). In other cases, treatment for bacterial overgrowth includes eliminating drugs that reduce intestinal motility or reduce gastric acidity. Dietary manipulation may also assist in the treatment of SIBO 50.
There are several approaches to treat SIBO among patients with IBS that include antibiotics, probiotics and prokinetics. Dietary manipulation has potential influence on the gut microbiota that may relieve some of the symptoms of SIBO. Recently, utility of therapeutic manipulation of gut flora using antibiotic and probiotic to treat IBS is being increasingly recognized and hence, worth reviewing.
1. SIBO Antibiotics
While choosing antibiotics, one should consider whether its antibacterial spectrum is broad including aerobes and anaerobes and absorption is poor reducing systemic side effects. Though in the past, tetracycline, doxycycline, co-trimoxazole, fluoroquinolones have all been used in the treatment of SIBO 51, 52, in most of the recent studies among patients with IBS, rifaximin has been the preferred antibiotic (Table 3) 53, 54.
Table 3. Clinical Trials of Antibiotics among Patients with Small Intestinal Bacterial Overgrowth and IBS
| Study no. | Antibiotics (dosage) | Duration, day | Study subject | Clinical outcome | Reference |
|---|---|---|---|---|---|
| 1 | Rifaximin (1,600 mg/day) vs rifaximin (1,200 mg/day) | 7 | 80 Patients with SIBO | Rate of normalization of GHBT was greater with higher dose of rifaximin than lower dose (80% vs 58%, p<0.05). | Scarpellini et al.55 |
| 2 | Rifaximin (group 1, 600; group 2, 800; group 3, 1,200 mg/day) | 7 | 90 Patients with SIBO and 30 patients in each group | Rate of normalization of GHBT was higher in group 3 than group 1 and 2 (60% vs 17%, p<0.001; 60% vs 27%, p<0.01). | Lauritano et al.56 |
| 3 | Neomycin (n=55) or placebo (n=56) | 7 | 111 Patients with IBS | Neomycin reduced the symptoms of IBS more often than placebo (35% vs 11%, p<0.05) and normalized lactulose hydrogen breath test result. | Pimentel et al.57 |
| 4 | Ciprofloxacin (500 mg, twice daily) | 10 | 7 Patients with SIBO | Ciprofloxacin decreased viable bacterial counts in five patients (71%), while four (57%) still fulfilled criteria for SIBO. Three patients (43%) reported at least 25% improvement in IBS symptoms. | Posserud et al.58 |
| 5 | Norfloxacin (800 mg/day) or placebo | 10 | 80 IBS patients | Norfloxacin significantly reduced the symptom scores among patients with SIBO than without but not with placebo at 1 month. Symptoms resolved to turn Rome III negative more often in SIBO patients receiving norfloxacin than placebo at 1 month (7/8, 87.5 vs 0/7, p=0.004). | Ghoshal et al.54 |
Note: SIBO, small intestinal bacterial overgrowth; GHBT, glucose hydrogen breath test; IBS, irritable bowel syndrome.
Rifaximin is a semi-synthetic, nonabsorbable antimicrobial agent that acts against Gram positive and Gram negative aerobic and anaerobic bacteria 55. Pimentel et al. 57 reported two identically designed, large, multicenter, double blind, placebo-controlled trials (TARGET 1 and TARGET 2) among patients with nonconstipating IBS (n=1,260) diagnosed by Rome II criteria. IBS subjects receiving rifaximin at a dose of 550 mg three times daily for 14 days reported adequate relief in global IBS symptoms as compared to identical placebo (TARGET 1: 40.8% vs 31.2% and TARGET 2: 40.6% vs 32.2%) 57. Moreover, rifaximin was more effective in relieving abdominal bloating than placebo (TARGET 1: 39.5% vs 28.7% and TARGET 2: 41.0% vs 31.9%) 57. The improvement in symptoms of IBS (like abdominal pain, loose or watery stool) persisted for a duration of 10 weeks after the end of 2-week treatment 57.
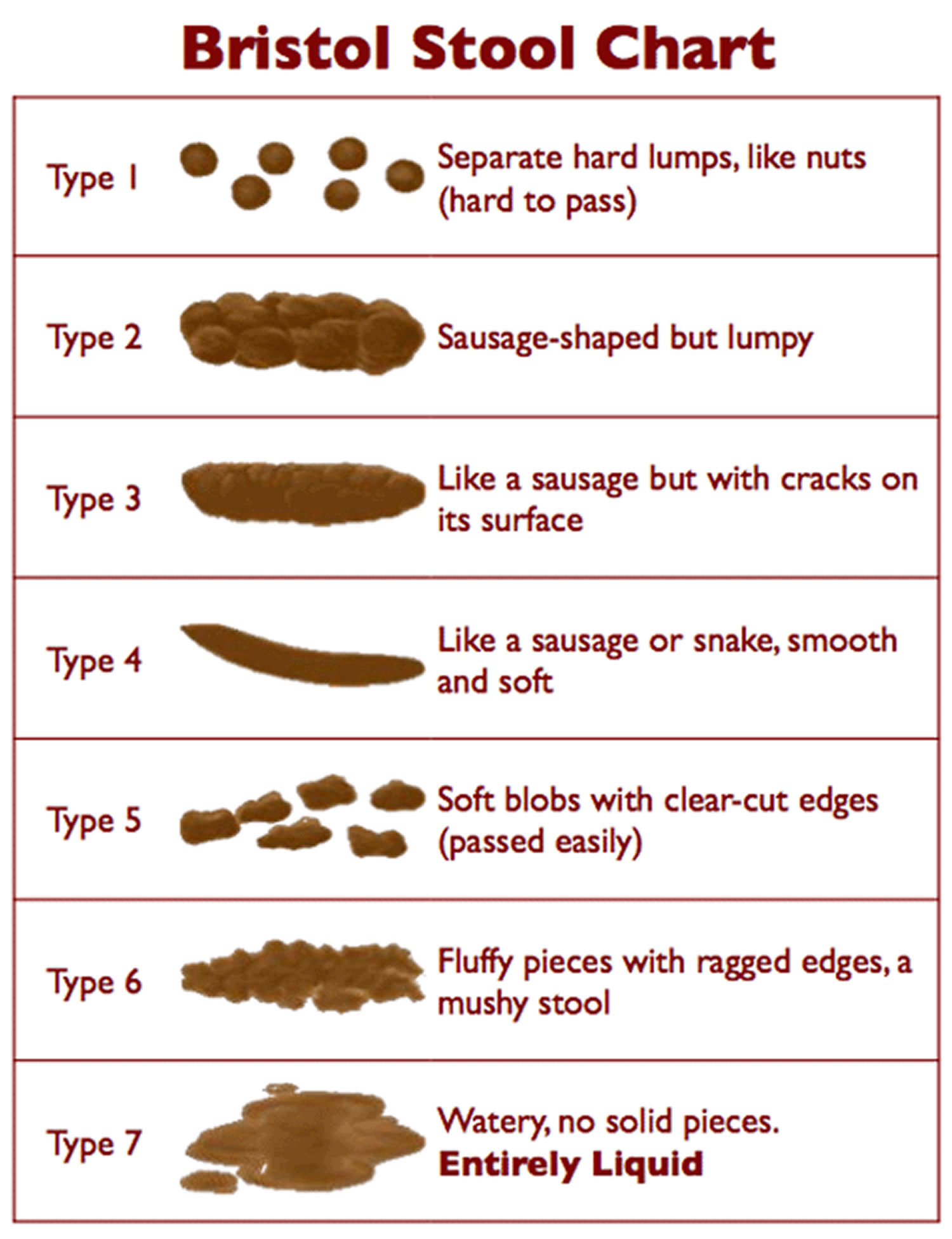
Recently, TARGET 3 study has been completed to evaluate the efficacy and safety of retreatment with rifaximin among 636 patients with IBS-Diarrhea, who had responded to rifaximin previously but developed recurrent IBS symptoms over a duration of 18 weeks follow-up 59. The end-point of TARGET 3 study was different from the TARGET 1 and TARGET 2 studies according to the guidelines proposed by Food and Drug Administration (FDA). TARGET 3 study included those IBS subjects who reported improvement in symptoms during at least 2 of the first 4 weeks in abdominal pain (≥30% decrease from baseline in mean weekly pain score) and stool consistency (≥50% decrease from baseline in the number of days per week with bowel movements complying with type 6 or 7 on the Bristol stool form scale [see Figure 2 Bristol Stool Chart]) 60. Retreatment with rifaximin showed 33% response rate as compared to 25% in placebo group, consistent with FDA guidelines for clinical assessment of IBS drugs 60.
There are seven types of stools (feces) according to the Bristol Stool Chart. The Bristol Stool Chart or Bristol Stool Scale is a medical aid designed to classify feces into seven groups.
The type of stool or feces depends on the time it spends in the colon. After you pass feces, what you see in the toilet bowl is basically the result of your diet, fluids, medications and lifestyle. You can use the Bristol Stool Chart to check what your stools are telling you.
The Bristol Stool Chart shows seven categories of stool. Every person will have different bowel habits, but the important thing is that your stools are soft and easy to pass – like types 3 and 4 below.
- Type 1–2 indicate constipation
- Type 3–4 are ideal stools as they are easier to pass, and
- Type 5–7 may indicate diarrhea and urgency.
Figure 2. Bristol Stool Chart
[Source 61]
In a study of open level antibiotic treatment, bacterial overgrowth was eradicated in 25 out of 47 patients and symptoms of IBS like diarrhea and abdominal pain were improved 41. Moreover, 48% of the subjects were found negative for Rome I criteria 41. In another study, of the 10 patients with SIBO treated with norfloxacin, amoxicillin-clavulanic acid and Saccharomyces boulardii over a period of 7 days 62, norfloxacin and amoxicillin-clavulanic acid significantly improved the mean daily stool frequency, but not S. boulardii 62. Recently, a proof of the concept study suggested that the lower response rate of 40% among patients treated with antibiotic in TARGET I and II studies might be related to the fact that patients were not selected based on the presence or absence of SIBO. In this study, 7 of 8 (87.5%) of 15 patients with SIBO treated with norfloxacin became Rome III negative at 1 month as compared to none of those treated with placebo. Interestingly, in this study, of 40 patients treated with norfloxacin, 15 (37.5%) responded showing that when not selected according to presence of SIBO, response rate was somewhat similar to the frequency of improvement as reported in TARGET I and II study 54.
In a recent meta-analysis, efficiency of rifaximin (two studies) in eradicating SIBO was 64.1% as compared to 41% with other systemic antibiotics (metronidazole or tetracycline) 63. Another meta-analysis of eight studies showed that overall normalization rate of breath test with rifaximin was 49.5% 64. Antibiotics like metronidazole, neomycin and ciprofloxacin (four studies) showed higher response rate than placebo in normalizing breath tests with an odds ratio of 2.55 (95% CI) 64. Thus, evidence from above studies suggests that antibiotics can be given in IBS patients with suspected SIBO.
2. SIBO Probiotics
Probiotics are live microorganisms, which, when administered in sufficient quantities may alleviate symptoms of IBS than placebo as shown by several clinical trials 11. Probiotics may work by suppressing proinflammatory cytokines, modulating gut microbiota, sustaining the integrity of intestinal epithelium and altering the visceral hypersensitivity and brain function 65, 66. Randomized controlled trials of probiotics among patients with SIBO are scanty. An old randomized controlled cross-over study only on 10 patients with SIBO showed that though norfloxacin and amoxicillin-clavulanic acid were effective in improving mean daily stool frequency and breath hydrogen, S. boulardii administered for one week was ineffective 62. Another study, however, showed that administration of high doses of S. boulardii for one month reduced abdominal pain, bloating, flatulence among pediatric patients with short bowel syndrome (SBS) and led to some change in bacterial flora in the stool samples suggesting that S. boulardii may impact the gut microbiota in patients with short bowel syndrome (SBS) 67. Furthermore, probiotics may enhance the efficiency of antibiotics. One study showed that treatment with rifaximin along with probiotic (Lactobacillus casei) improved the symptoms of SIBO more effectively than antibiotic followed by prebiotic (short chain fructo-oligosaccharide) 68. Some studies recommended that treatment with rifaximin along with probiotics as a standard therapy for management of SIBO 68. Use of multispecies probiotics had shown several benefits in reliving symptoms of IBS 69. A randomized controlled trial of VSL#3 (twice daily for 8 weeks) in patients with IBS-DIARRHEA showed that abdominal bloating was significantly reduced as compared to placebo but not other parameters such as bowel dysfunction, colonic transit time, abdominal pain, flatulence or urgency 69, 70. More studies, however, are needed to evaluate efficacy of probiotics among patients with IBS in relation to presence of SIBO.
3. SIBO Prokinetics
Since IBS is associated with alteration and gut motility, and SIBO is associated with motility disorders, prokinetics are expected to be beneficial in patients with SIBO. In an earlier study, Pimentel et al. 71 showed that IBS patients with SIBO had lower frequency of migratory motor complex. Hence, it is expected that prokinetic drugs that improve small bowel motility might be useful in preventing SIBO following its successful treatment. The same group of authors showed that tegaserod, a serotonin receptor agonist, prevents the recurrence of IBS symptoms after antibiotic treatment compared to another prokinetic, erythromycin (a motilin agonist) 72.
4. SIBO Natural Treatment
Dietary manipulation may help patients with IBS in general and those with SIBO in particular. In patients with SIBO, bacteria in the small bowel may ferment carbohydrates such as lactose, fructose and also the dietary Fermentable Oligosaccharides, Disaccharides, Monosaccharides And Polyols (FODMAPs), which forms gas resulting in flatulence, abdominal bloating and pain. Hence, restriction of these dietary components may improve these symptoms.136 Moreover, some preliminary data suggest that manipulation of the diet may alter gut microbiota. In a study, human fecal microbiota was transplanted into germ free mice that were fed low fat diet and plant polysaccharides. Subsequently, feeding Western diet resulted in change in composition of gut microbiota leading to increased number of Firmicutes, Clostridium species, Eubacterium, Enterococcus and decreased number of Bacteroides. Moreover, diet rich in complex carbohydrates favors growth of less pathogenic bacteria (Mycobacterium avium subspecies paratuberculosis and Enterobacteriaceae) than diet rich in fat or protein. Vegetarian diets, rich in fiber, lead to higher production of short chain fatty acids, which inhibit potentially invasive bacteria like E. coli and other members of Enterobacteriaceae. In a recent study, we found that vegetarianism was a risk factor for IBS on univariate and multivariate analysis. More studies are needed to evaluate effect of dietary manipulation on gut microbiota including SIBO.
Researchers suggest that the small intestine does not absorb FODMAPs very well. They increase the amount of fluid in the bowel. They also create more gas. That’s because bacteria in the colon they are easily fermented by colonic bacteria. The increased fluid and gas in the bowel leads to bloating and changes in the speed with which food is digested. This results in gas, pain and diarrhea. Eating less of these types of carbohydrates should decrease these symptoms.
Figure 3. Foods that may trigger IBS symptoms
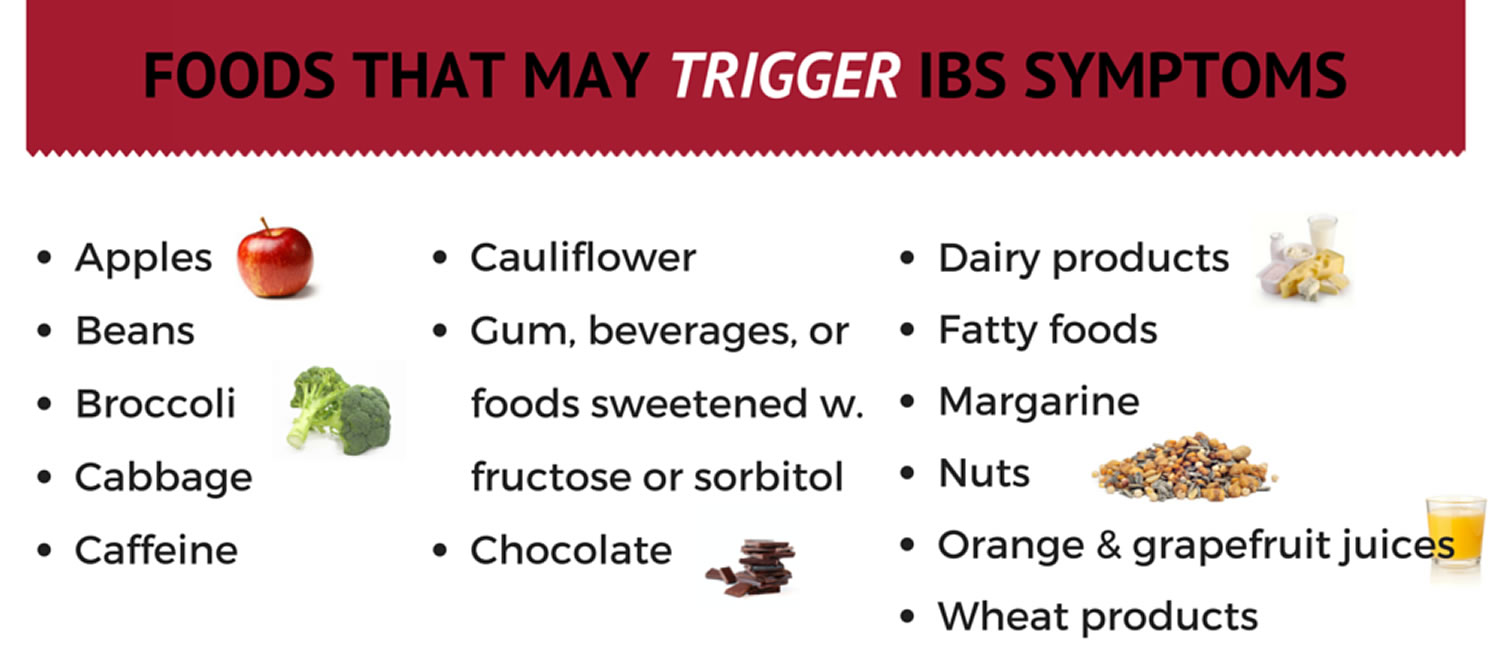
So far, studies have shown that a low FODMAP diet has a beneficial effect in a majority of patients with Irritable Bowel Syndrome (IBS) symptoms 73. One study even found that 76% of Irritable Bowel Syndrome (IBS) patients following the diet reported improvement with their symptoms. Probiotics also have great potential in the management of Irritable Bowel Syndrome (IBS); however, it is still unclear which strains and doses are the most beneficial. Further research is needed on the effect of different fibers or combinations of fibers, in Irritable Bowel Syndrome (IBS).
SIBO Diet
FODMAP stands for Fermentable, Oligo-, Di-, Mono-saccharides And Polyols. FODMAPs are short-chain carbohydrates (sugars) that are highly fermentable (to ferment, is to go through a chemical change that results in alcohol) and poorly absorbed during digestion 74. The acronym FODMAPs was created to describe poorly absorbed, short-chain carbohydrates that can lead to excessive fluid and gas accumulation, resulting in bloating, abdominal pain, and distention (Figure 4).
The Low FODMAP diet was developed by researchers at Monash University more than five years ago, in Australia, by Susan Shepherd and Peter Gibson. This diet eliminates certain foods to improve the symptoms of functional gut disorders (FGD). Irritable bowel syndrome (IBS), a type of FGD, may be helped by this diet. IBS is the most commonly diagnosed gastrointestinal condition and over half of patients with IBS associate a trigger in their symptoms with eating a meal 75. The Monash team, led by Professor Peter Gibson, provided the first evidence that a Low FODMAP diet improves IBS symptoms. Irritable bowel syndrome (IBS) is a common functional gastrointestinal disorder affecting one in seven Australian adults and approximately 35 million Americans are impacted by IBS including many in Europe and many in Asian countries. IBS is characterised by chronic and relapsing symptoms; lower abdominal pain and discomfort, bloating, wind, distension and altered bowel habit (ranging from diarrhoea to constipation) but with no abnormal pathology. The diagnosis of IBS should be made by a medical practitioner.
FODMAPs are found in a wide variety of foods, including those containing lactose, fructose in excess of glucose, fructans, galacto-oligosaccharides, and polyols (sorbitol, mannitol, xylitol, and maltitol). All FODMAPs have poor absorption and rapid fermentation, and they are comprised of small, osmotically active molecules. FODMAPs are poorly absorbed for a number of reasons, including the absence of luminal enzymes capable of hydrolyzing the glycosidic bonds contained in carbohydrates, the absence or low activity of brush border enzymes (eg, lactase), or the presence of low-capacity epithelial transporters (fructose, glucose transporter 2 [GLUT-2], and glucose transporter 5 [GLUT-5]). Fructose, which is an important FODMAP in the Western diet, is absorbed across villous epithelium through low-capacity, carrier-mediated diffusion involving GLUT-5. The absorption of free fructose is markedly enhanced in the presence of glucose via GLUT-2. Therefore, if fructose is present in excess of glucose, the risk of fructose malabsorption is increased. In addition, some molecules, such as polyols, are too large for simple diffusion. The fermentation rate is determined by the chain length of the carbohydrate 76.
For example, oligosaccharides are rapidly fermented, compared to polysaccharides. Fermentation results in the production of carbon dioxide, hydrogen, and/or methane gas. Finally, small, osmotically active molecules draw more water and other liquid into the small bowel. Given these properties, a diet low in FODMAPs has become a potential therapy for IBS patients.
When FODMAPs reach the colon (large intestine), bacteria ferment these sugars, turning them into gas and chemicals. This stretches the walls of the colon, causing abdominal bloating, distension, and pain or cramping in many people. Other symptoms, such as diarrhea, constipation, and nausea, are also common side effects of FODMAP carbohydrates. Not everyone has the same reaction to FODMAPs. Ethnicity, genetics, and environmental factors (such as an individual’s microbiome, motility, immune system, and sensory system) may play a part in your body’s ability to tolerate these carbohydrates.
Figure 4. FODMAPs in your gut
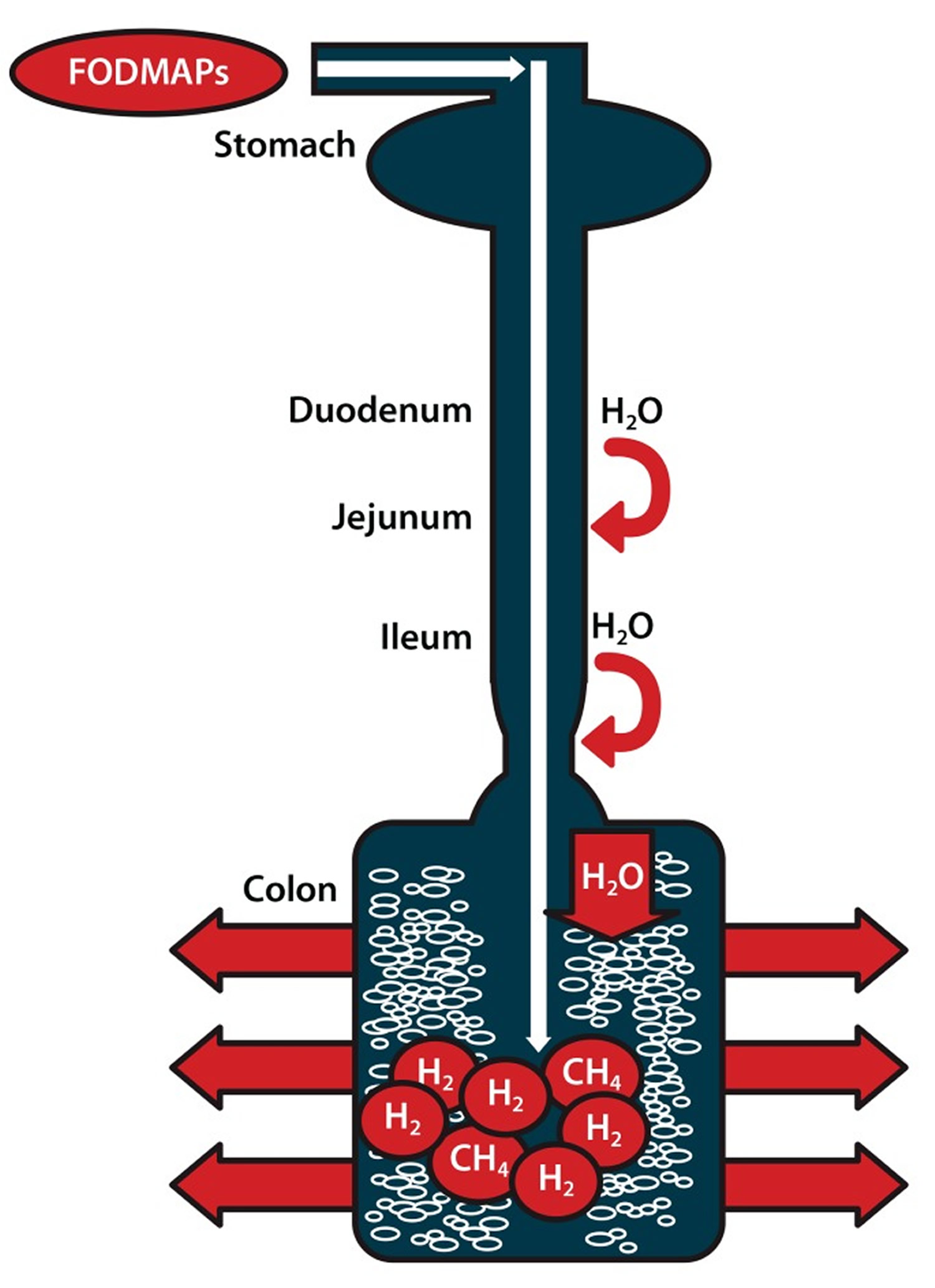
Note: Ingested fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) are poorly absorbed in the small intestine. Their small molecular size results in an osmotic effect, drawing water (H20) through to the large intestine. FODMAPs are then fermented by colonic microflora, producing hydrogen (H2) and/or methane gas (CH4). The increase in fluid and gas leads to diarrhea, bloating, flatulence, abdominal pain, and distension.
[Source 77]When is a SIBO diet recommended ?
Despite limited data, implementation of a low-FODMAP diet should be considered in patients with IBS, particularly those in whom food is a trigger for symptoms.
Eliminating or restricting FODMAPs from the diet may greatly improve symptoms of functional gut disorders (FGD). In Australia, a Low-FODMAP diet is the main treatment for irritable bowel syndrome (IBS). It was adopted by their National Therapeutic Guidelines. The Low-FODMAP diet can be adjusted to meet personal food and lifestyle preferences. Following a personally developed Low-FODMAP plan does not cure IBS, but it may lead to drug-free management of symptoms and better quality of life. As with any diet, it is important to discuss with your doctor and working with a gastrointestinal trained dietician is also useful.
A number of studies suggest that limiting FODMAPs in the diet leads to improved symptoms in one-half to two-thirds of patients who follow this diet. Many patients see improvement in 1-2 weeks, though some may need to wait up to 4 weeks. Bloating and abdominal pain are the most likely symptoms to improve. Diarrhea is more likely to improve than constipation. If there is no improvement after 4 weeks, it is likely not worth continuing this diet.
A Low-FODMAP diet is not recommended for people without gastrointestinal symptoms. Also, if your IBS symptoms improve on the Low-FODMAP diet, you should eventually re-introduce FODMAPs, one at a time, to identify foods that trigger symptoms and those that do not. This will allow a more diverse diet. Keeping a personal food diary may help simplify this process
Implementation of a low-FODMAP diet is best done with the help of a dietician during a one-to-one consultation so that the dietician can understand the patient’s symptoms; this process also ensures that any diet modifications are individualized and still provide a balanced diet. A diet history should be taken to determine the composition of FODMAPs in an individuals diet. Education can then be tailored appropriately rather than focusing on FODMAPs that may never be consumed. Lists of food substitutions can help patients understand what they can and cannot eat (Table 4) 78. For good symptom control, individuals should restrict their total FODMAP load for 6-8 weeks. After this time, the diet may be modified to be less restrictive based on symptom response.
However, there are also several limitations to low-FODMAP diets. Most foods do not list their FODMAP content. In addition, the cutoff levels for FODMAP content are not clearly defined. When this diet was first examined, cutoff values were proposed based on foods that patients identified to be triggers for their symptoms. Foods and beverages with the following amounts of FODMAPs were considered to have risk for inducing symptoms: more than 0.5 g of fructose in excess of glucose per 100 g, more than 3 g of fructose in an average serving quantity regardless of glucose amount, and more than 0.2 g of fructans per serving 78. Although a low-FODMAP diet has been shown to be helpful in patients with IBS or other functional bowel disorders, further randomized controlled trials should be conducted.
Table 4. Foods High in Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAPs) and Suitable Alternatives
| FODMAP | Foods high in FODMAPs | Suitable alternatives low in FODMAPs |
|---|---|---|
| Excess fructose | Fruits: apple, clingstone peach, mango, nashi pear, pear, sugar snap pea, tinned fruit in natural juice, watermelon | Fruits: banana, blueberry, cantaloupe, carambola, durian, grape, grapefruit, honeydew melon, kiwi, lemon, lime, orange, passion fruit, pawpaw, raspberry, strawberry, tangelo |
| Honey sweeteners: fructose, high-fructose corn syrup | Honey substitutes: golden syrup, maple syrup | |
| Large total fructose dose: concentrated fruit sources, large servings of fruit, dried fruit, fruit juice | Sweeteners: any sweeteners except polyols | |
| Lactose | Milk: regular and low-fat cow, goat, and sheep milk; ice cream | Milk: lactose-free milk, rice milk Ice cream substitutes: gelato, sorbet |
| Yogurts: regular and low-fat yogurts | Yogurts: lactose-free yogurts | |
| Cheeses: soft and fresh cheeses | Cheeses: hard cheeses | |
| Oligosaccharides (fructans and/or galactans) | Vegetables: artichoke, asparagus, beetroot, broccoli, Brussels sprout, cabbage, fennel, garlic, leek, okra, onion, pea, shallot | Vegetables: bamboo shoot, bok choy, capsicum, carrot, celery, chives, choko, choy sum, corn, eggplant, green bean, lettuce, parsnip, pumpkin, silverbeet, spring onion (green part only) |
| Cereals: rye and wheat cereals when eaten in large amounts (eg, biscuit, bread, couscous, cracker, pasta) | Onion/garlic substitutes: garlic-infused oil | |
| Legumes: baked bean, chickpea, lentil, red kidney bean | Cereals: gluten-free and spelt bread/cereal products | |
| Fruits: custard apple, persimmon, rambutan, watermelon, white peach | Fruit: tomato | |
| Polyols | Fruits: apple, apricot, avocado, cherry, longon, lychee, nashi pear, nectarine, peach, pear, plum, prune, watermelon | Fruits: banana, blueberry, cantaloupe, carambola, durian, grape, grapefruit, honeydew melon, kiwi, lemon, lime, orange, passion fruit, pawpaw, raspberry |
| Vegetables: cauliflower, mushroom, snow pea | ||
| Sweeteners: isomalt, maltitol, mannitol, sorbitol, xylitol, and other sweeteners ending in “-ol” | Sweeteners: glucose, sugar (sucrose), other artificial sweeteners not ending in “-ol” |
SIBO Food List
Table 5. FODMAP Food List
Food | Avoid | Suitable |
| Lactose | Dairy whey and high-lactose containing milks such as cow, goat, sheep, chocolate, buttermilk, and condensed milk, and whipped cream. Ice cream, cow’s milk-based yogurt, brie, cottage cheese, ricotta, and sour cream. | Gelato or sorbet (though watch fructose content) and lactose-free yogurts. Aged hard cheeses tend to be easier to tolerate. Cheddar, Colby, parmesan, and mozzarella. Greek yogurt. Limit: Butter, margarine, sour cream, half and half, cream cheese, Swiss cheese, goat cheese, feta cheese, cheddar, parmesan, and mozzarella contain lactose, although at lower amounts. |
| Non-Dairy Milk Alternatives | Soy milk contains galactans and should be avoided as well, coconut milk, soy products, hummus, beans, and lentils. | Lactose- free or lactaid milk, rice milk, almond milk, almond butter, and cashew milk. |
| Fructose / Sweeteners | Honey, agave, apples, cherries, dates, guava, honeydew melon, lychee, mandarin oranges, mangoes, peaches, pears, persimmons, star fruit, canned fruit in natural juices, dried fruits and less ripe fruits, corn syrup, high fructose sweeteners, coconut milk, fruit pastes (i.e. chutney, plum sauce, barbeque sauce, ketchup), rosé wine, port, and sherry | Maple syrup, jams, marmalades, vegemite, table sugar, bananas, blackberries, blueberries, boysenberries, cranberries, grapefruit, kiwis, kumquats, lemons, limes, passion fruit, raspberries, and strawberries. Limit: grapes, oranges, papaya, pineapple, and watermelon. |
| Fructans | ||
| Starches | Bread, pasta, semolina, flour tortillas, wheat-based bread and breadcrumbs. Wheat-based cereals, crackers, cookies, cakes, pasta, and pastries. Beer. | Corn breads, gluten- free breads, pastas, cereals, as well as corn flakes, oatmeal, potato-based breads, rice-based noodles and breads, and wheat-free rye bread. |
| Fruit | Grapes, mangoes, peaches, persimmon, pineapple, watermelon, and bananas. | Grapefruit, lemons, limes, papaya, raspberries, strawberries, and blueberries. |
| Vegetables | Artichokes, asparagus, beets, broccoli, Brussel sprouts, cabbage, chicory, garlic, leeks, lettuce, okra, onions, radicchio, scallions, shallots, snow peas, and zucchini. | Bean sprouts, bell peppers, bok choy, carrots, celery, chives, cucumber, eggplant, potatoes, pumpkin, radishes, spinach, tomatoes, turnips, winter squash, and garlic-infused oil. |
| Galactans | Plant based proteins such as beans, black-eyed peas, chick peas, kidney beans, lentils, lima beans, pinto beans, soy products, broccoli, Brussel sprouts, cabbage, green beans, and yellow beans. | Eggs, nuts, quinoa, seeds, bean sprouts, bell peppers, bok choy, carrots, celery, chives, cucumbers, eggplant, potatoes, pumpkin, radish, spinach, and tomatoes. |
| Artificial Sweeteners | Sorbitol, mannitol, isomaltose, malitol, xylitol, polydextrose, hydrogenated starch | Aspartame, sucralose, saccharin. Commonly found in various gum and candy as well. |
| Polyols | ||
| Fruit | Apples, apricots, avocados, cherries, lychee, nectarines, peaches, pears, plums, and watermelon. | Bananas, blueberries, grapefruit, kiwi, lemons, limes, passion fruit, raspberries, cantaloupe, honeydew, and strawberries |
| Vegetables | Artichoke, asparagus, brussel sprouts, cabbage, cauliflower, green beans mushrooms, snow peas sprouts, and summer squash. | Bean sprouts, bell peppers, bok choy, carrots, celery, chives, cucumbers, eggplant, kale, lettuce, potatoes, pumpkin, radishes, spinach, tomatoes, winter squash, yams, and zucchini. |
Eat Less Of These Foods
Lactose
- Cow’s milk, yogurt, pudding, custard, ice cream, cottage cheese, ricotta cheese and mascarpone
Fructose
- Fruits, such as apples, pears, peaches, cherries, mangoes, pears and watermelon
- Sweeteners, such as honey and agave nectar
- Products with high fructose corn syrup
Fructans
- Vegetables, such as artichokes, asparagus, Brussels sprouts, broccoli, beetroot, garlic and onions
- Grains such as wheat and rye
- Added fiber, such as inulin
Oligosaccharides (fructans and/or galactans)
- Chickpeas, lentils, kidney beans and soy products
- Vegetables, such as broccoli
Polyols
- Fruits, such as apples, apricots, blackberries, cherries, nectarines, pears, peaches, plums and watermelon
- Vegetables, such as cauliflower, mushrooms and snow peas
- Sweeteners, such as sorbitol, mannitol, xylitol, maltitol and isomalt found in sugar-free gum and mints, and cough medicines and drops
Eat More Of These Foods
- Dairy: Lactose-free milk, rice milk, almond milk, coconut milk, lactose-free yogurt; hard cheeses such as feta and brie
- Fruit: Bananas, blueberries, cantaloupe, grapefruit, honeydew, kiwi, lemon, lime, oranges and strawberries
- Vegetables: Bamboo shoots, bean sprouts, bok choy, carrots, chives, cucumbers, eggplant, ginger, lettuce, olives, parsnips, potatoes, spring onions and turnips
- Protein: Beef, pork, chicken, fish, eggs and tofu
- Nuts/seeds (limit to 10-15 each): Almonds, macadamia, peanuts, pine nuts and walnuts
- Grain: Oat, oat bran, rice bran, gluten-free pasta, such as rice, corn, quinoa, white rice, corn flour and quinoa
The idea behind the low FODMAPs diet is to only limit the problematic foods in a category — not all of them. (After all, they do have health benefits.) You may tolerate some foods better than others.
Meet with a registered dietician if you are considering this diet. It’s important to make sure your eating plan is safe and healthy. He or she will have you eliminate FODMAPs from your diet. Then you gradually add the carbohydrates back in one at a time and monitor your symptoms. A food diary and symptom chart may be helpful tools.
- Sachdev AH, Pimentel M. Gastrointestinal bacterial overgrowth: pathogenesis and clinical significance. Therapeutic Advances in Chronic Disease. 2013;4(5):223-231. doi:10.1177/2040622313496126. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3752184/[↩][↩][↩]
- Gerritsen J, Smidt H, Rijkers GT, de Vos WM. Intestinal microbiota in human health and disease: the impact of probiotics. Genes & Nutrition. 2011;6(3):209-240. doi:10.1007/s12263-011-0229-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3145058/[↩]
- Sekirov I, Russell SL, Antunes LC, Finlay BB. Gut microbiota in health and disease. Physiol Rev. 2010;90:859–904. doi: 10.1152/physrev.00045.2009. http://physrev.physiology.org/content/90/3/859.long[↩][↩]
- Ghoshal UC, Park H, Gwee KA. Bugs and irritable bowel syndrome: the good, the bad and the ugly. J Gastroenterol Hepatol. 2010;25:244–251. doi: 10.1111/j.1440-1746.2009.06133.x. https://www.ncbi.nlm.nih.gov/pubmed/20074148[↩]
- Lagier J-C, Million M, Hugon P, Armougom F, Raoult D. Human Gut Microbiota: Repertoire and Variations. Frontiers in Cellular and Infection Microbiology. 2012;2:136. doi:10.3389/fcimb.2012.00136. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3487222/[↩][↩]
- Nigam D. Microbial interactions with humans and animals. Int J Microbiol Allied Sci. 2015;2:1–17.[↩]
- Eckburg PB, Bik EM, Bernstein CN, et al. Diversity of the Human Intestinal Microbial Flora. Science (New York, NY). 2005;308(5728):1635-1638. doi:10.1126/science.1110591. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1395357/[↩]
- Schloss PD, Handelsman J. Status of the Microbial Census. Microbiology and Molecular Biology Reviews. 2004;68(4):686-691. doi:10.1128/MMBR.68.4.686-691.2004. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC539005/[↩]
- Goulet O, Joly F. Intestinal microbiota in short bowel syndrome. Gastroenterol Clin Biol. 2010;34(Suppl 1):S37–S43. doi: 10.1016/S0399-8320(10)70019-1. https://www.ncbi.nlm.nih.gov/pubmed/20889003[↩]
- Bures J, Cyrany J, Kohoutova D, et al. Small intestinal bacterial overgrowth syndrome. World Journal of Gastroenterology : WJG. 2010;16(24):2978-2990. doi:10.3748/wjg.v16.i24.2978. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2890937/[↩]
- Ghoshal UC, Shukla R, Ghoshal U, Gwee K-A, Ng SC, Quigley EMM. The Gut Microbiota and Irritable Bowel Syndrome: Friend or Foe? International Journal of Inflammation. 2012;2012:151085. doi:10.1155/2012/151085. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3346986/[↩][↩]
- Gabrielli M, D’Angelo G, Di Rienzo T, Scarpellini E, Ojetti V. Diagnosis of small intestinal bacterial overgrowth in the clinical practice. Eur Rev Med Pharmacol Sci. 2013;17(Suppl 2):30–35. https://www.ncbi.nlm.nih.gov/pubmed/24443065[↩]
- Hao WL, Lee YK. Microflora of the gastrointestinal tract: a review. Methods Mol Biol. 2004;268:491–502. https://www.ncbi.nlm.nih.gov/pubmed/15156063[↩]
- Riordan SM, McIver CJ, Wakefield D, Duncombe VM, Thomas MC, Bolin TD. Small intestinal mucosal immunity and morphometry in luminal overgrowth of indigenous gut flora. Am J Gastroenterol. 2001;96:494–500. doi: 10.1111/j.1572-0241.2001.03533.x. https://www.ncbi.nlm.nih.gov/pubmed/11232696[↩]
- Ziegler TR, Cole CR. Small bowel bacterial overgrowth in adults: a potential contributor to intestinal failure. Curr Gastroenterol Rep. 2007;9:463–467. doi: 10.1007/s11894-007-0060-x. https://www.ncbi.nlm.nih.gov/pubmed/18377796[↩]
- Ghoshal UC, Shukla R, Ghoshal U. Small Intestinal Bacterial Overgrowth and Irritable Bowel Syndrome: A Bridge between Functional Organic Dichotomy. Gut and Liver. 2017;11(2):196-208. doi:10.5009/gnl16126. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5347643/[↩]
- Hamvas J. (2012) [Proton-pump inhibitor therapy and small bowel bacterial contamination]. Orv Hetil 153: 1287–1293. https://www.ncbi.nlm.nih.gov/pubmed/22890175[↩]
- Krishnamurthy S., Kelly M., Rohrmann C., Schuffler M. (1983) Jejunal diverticulosis. A heterogenous disorder caused by a variety of abnormalities of smooth muscle or myenteric plexus. Gastroenterology 85: 538–547. https://www.ncbi.nlm.nih.gov/pubmed/6409704[↩]
- Pimentel M., Chow E., Lin H. (2000) Eradication of small intestinal bacterial overgrowth reduces symptoms of irritable bowel syndrome. Am J Gastroenterol 95: 3503–3506. https://www.ncbi.nlm.nih.gov/pubmed/11151884[↩]
- Funayama Y., Sasaki I., Naito H., Fukushima K., Shibata C., Masuko T., et al. (1999) Monitoring and antibacterial treatment for postoperative bacterial overgrowth in Crohn’s disease. Dis Colon Rectum 42: 1072–1077. https://www.ncbi.nlm.nih.gov/pubmed/10458133[↩]
- Trespi E., Ferrieri A. (1999) Intestinal bacterial overgrowth during chronic pancreatitis. Curr Med Res Opin 15: 47–52. https://www.ncbi.nlm.nih.gov/pubmed/10216811[↩]
- Compare D., Coccoli P., Rocco A., Nardone O., De Maria S., Carteni M., et al. (2012) Gut–liver axis: the impact of gut microbiota on non alcoholic fatty liver disease. Nutr Metab Cardiovasc Dis 22: 471–476. https://www.ncbi.nlm.nih.gov/pubmed/22546554[↩]
- Krauss N., Schuppan D. (2006) Monitoring nonresponsive patients who have celiac disease. Gastrointest Endosc Clin N Am 16: 317–327. https://www.ncbi.nlm.nih.gov/pubmed/16644460[↩]
- Rifaximin treatment for symptoms of irritable bowel syndrome. Fumi AL, Trexler K. Ann Pharmacother. 2008 Mar; 42(3):408-12. https://www.ncbi.nlm.nih.gov/pubmed/18303148/[↩]
- Parodi A., Paolino S., Greco A., Drago F., Mansi C., Rebora A., et al. (2008) Small intestinal bacterial overgrowth in rosacea: clinical effectiveness of its eradication. Clin Gastroenterol Hepatol 6: 759–764. https://www.ncbi.nlm.nih.gov/pubmed/18456568[↩][↩]
- Small intestinal bacterial overgrowth syndrome. Bures J, Cyrany J, Kohoutova D, Förstl M, Rejchrt S, Kvetina J, Vorisek V, Kopacova M. World J Gastroenterol. 2010 Jun 28; 16(24):2978-90. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2890937/[↩]
- Simrén M, Barbara G, Flint HJ, et al. Intestinal microbiota in functional bowel disorders: a Rome foundation report. Gut. 2013;62(1):159-176. doi:10.1136/gutjnl-2012-302167. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3551212/[↩]
- Weinstock L., Walters A. (2011) Restless legs syndrome is associated with irritable bowel syndrome and small intestinal bacterial overgrowth. Sleep Med 12: 610–613. https://www.ncbi.nlm.nih.gov/pubmed/21570907[↩]
- Giannella R., Toskes P. (1976) Gastrointestinal bleeding and iron absorption in the experimental blind loop syndrome. Am J Clin Nutr 29: 754–757. https://www.ncbi.nlm.nih.gov/pubmed/1084685[↩]
- Di Stefano M., Veneto G., Malservisi S., Corazza G. (2001) Small intestine bacterial overgrowth and metabolic bone disease. Dig Dis Sci 46: 1077–1082. https://www.ncbi.nlm.nih.gov/pubmed/11341652[↩]
- Bongaerts G., Tolboom J., Naber A., Sperl W., Severijnen R., Bakkeren J., et al. (1997) Role of bacteria in the pathogenesis of short bowel syndrome-associated d-lactic acidemia. Microb Pathog 22: 285–293. https://www.ncbi.nlm.nih.gov/pubmed/9160298[↩]
- Ghoshal UC, Ghoshal U, Das K, Misra A. Utility of hydrogen breath tests in diagnosis of small intestinal bacterial overgrowth in malabsorption syndrome and its relationship with orocecal transit time. Indian J Gastroenterol. 2006;25:6–10. https://www.ncbi.nlm.nih.gov/pubmed/16567886[↩]
- Britton E, McLaughlin JT. Ageing and the gut. Proc Nutr Soc. 2013;72:173–177. doi: 10.1017/S0029665112002807. https://www.ncbi.nlm.nih.gov/pubmed/23146206[↩]
- Lagier JC, Million M, Hugon P, Armougom F, Raoult D. Human gut microbiota: repertoire and variations. Front Cell Infect Microbiol. 2012;2:136. doi: 10.3389/fcimb.2012.00136. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3487222/[↩]
- Lagier JC, Armougom F, Million M, et al. Microbial culturomics: paradigm shift in the human gut microbiome study. Clin Microbiol Infect. 2012;18:1185–1193. doi: 10.1111/1469-0691.12023. https://www.ncbi.nlm.nih.gov/pubmed/23033984[↩][↩]
- Kokcha S, Mishra AK, Lagier J-C, et al. Non contiguous-finished genome sequence and description of Bacillus timonensis sp. nov. Standards in Genomic Sciences. 2012;6(3):346-355. doi:10.4056/sigs.2776064. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3558959/[↩]
- Ghoshal UC. How to Interpret Hydrogen Breath Tests. Journal of Neurogastroenterology and Motility. 2011;17(3):312-317. doi:10.5056/jnm.2011.17.3.312. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3155069/[↩][↩][↩][↩]
- Nucera G, Gabrielli M, Lupascu A, et al. Abnormal breath tests to lactose, fructose and sorbitol in irritable bowel syndrome may be explained by small intestinal bacterial overgrowth. Aliment Pharmacol Ther. 2005;21:1391–1395. doi: 10.1111/j.1365-2036.2005.02493.x. https://www.ncbi.nlm.nih.gov/pubmed/15932370[↩]
- Abraczinskas D, Goldfinger SE. Intestinal gas and bloating. Up-ToDate Online. 2010:18.[↩]
- Ghoshal UC, Srivastava D, Ghoshal U, Misra A. Breath tests in the diagnosis of small intestinal bacterial overgrowth in patients with irritable bowel syndrome in comparison with quantitative upper gut aspirate culture. Eur J Gastroenterol Hepatol. 2014;26:753–760. doi: 10.1097/MEG.0000000000000122. https://www.ncbi.nlm.nih.gov/pubmed/24849768[↩][↩]
- Pimentel M, Chow EJ, Lin HC. Eradication of small intestinal bacterial overgrowth reduces symptoms of irritable bowel syndrome. Am J Gastroenterol. 2000;95:3503–3506. doi: 10.1111/j.1572-0241.2000.03368.x. https://www.ncbi.nlm.nih.gov/pubmed/11151884[↩][↩][↩][↩][↩]
- Shah ED, Basseri RJ, Chong K, Pimentel M. Abnormal breath testing in IBS: a meta-analysis. Dig Dis Sci. 2010;55:2441–2449. doi: 10.1007/s10620-010-1276-4. https://www.ncbi.nlm.nih.gov/pubmed/20467896[↩]
- Simrén M, Stotzer P. Use and abuse of hydrogen breath tests. Gut. 2006;55(3):297-303. doi:10.1136/gut.2005.075127. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1856094/[↩]
- Ojetti V, Di Rienzo TA, D’Angelo G, et al. Early peak of hydrogen during lactose breath test predicts intestinal motility. Open J Gastroenterol. 2014;4:40–44. doi: 10.4236/ojgas.2014.41007.[↩]
- Yu D, Cheeseman F, Vanner S. Combined oro-caecal scintigraphy and lactulose hydrogen breath testing demonstrate that breath testing detects oro-caecal transit, not small intestinal bacterial overgrowth in patients with IBS. Gut. 2011;60:334–340. doi: 10.1136/gut.2009.205476. https://www.ncbi.nlm.nih.gov/pubmed/21112950[↩]
- Santavirta J. Lactulose hydrogen and [14C]xylose breath tests in patients with ileoanal anastomosis. Int J Colorectal Dis. 1991;6:208–211. doi: 10.1007/BF00341392. https://www.ncbi.nlm.nih.gov/pubmed/1770288[↩]
- Banik GD, Maity A, Som S, et al. Diagnosis of small intestinal bacterial overgrowth in irritable bowel syndrome patients using high-precision stable 13 CO 2/12 CO 2 isotope ratios in exhaled breath. J Anal At Spectrom. 2014;29:1918–1924. doi: 10.1039/C4JA00186A.[↩]
- Ghoshal UC, Ghoshal U, Ayyagari A, et al. Tropical sprue is associated with contamination of small bowel with aerobic bacteria and reversible prolongation of orocecal transit time. J Gastroenterol Hepatol. 2003;18:540–547. doi: 10.1046/j.1440-1746.2003.03006.x. https://www.ncbi.nlm.nih.gov/pubmed/12702046[↩]
- Lu CL, Chen CY, Chang FY, Lee SD. Characteristics of small bowel motility in patients with irritable bowel syndrome and normal humans: an Oriental study. Clin Sci (Lond) 1998;95:165–169. doi: 10.1042/cs0950165. https://www.ncbi.nlm.nih.gov/pubmed/9680498[↩]
- Vanderhoof J., Young R., Murray N., Kaufman S. (1998) Treatment strategies for small bowel bacterial overgrowth in short bowel syndrome. J Pediatr Gastroenterol Nutr 27: 155–160. https://www.ncbi.nlm.nih.gov/pubmed/9702645[↩]
- Di Stefano M, Miceli E, Missanelli A, Corazza GR. Treatment of small intestine bacterial overgrowth. Eur Rev Med Pharmacol Sci. 2005;9:217–222. https://www.ncbi.nlm.nih.gov/pubmed/16128041[↩]
- Quigley EM, Quera R. Small intestinal bacterial overgrowth: roles of antibiotics, prebiotics, and probiotics. Gastroenterology. 2006;130(2 Suppl1):S78–S90. doi: 10.1053/j.gastro.2005.11.046. https://www.ncbi.nlm.nih.gov/pubmed/16473077[↩]
- Chedid V, Dhalla S, Clarke JO, et al. Herbal Therapy Is Equivalent to Rifaximin for the Treatment of Small Intestinal Bacterial Overgrowth. Global Advances in Health and Medicine. 2014;3(3):16-24. doi:10.7453/gahmj.2014.019. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4030608/[↩]
- Ghoshal UC, Srivastava D, Misra A, Ghoshal U. A proof-of-concept study showing antibiotics to be more effective in irritable bowel syndrome with than without small-intestinal bacterial overgrowth: a randomized, double-blind, placebo-controlled trial. Eur J Gastroenterol Hepatol. 2016;28:281–289. doi: 10.1097/MEG.0000000000000557. https://www.ncbi.nlm.nih.gov/pubmed/26731696[↩][↩][↩]
- Scarpellini E, Gabrielli M, Lauritano CE, et al. High dosage rifaximin for the treatment of small intestinal bacterial overgrowth. Aliment Pharmacol Ther. 2007;25:781–786. doi: 10.1111/j.1365-2036.2007.03259.x. https://www.ncbi.nlm.nih.gov/pubmed/17373916[↩][↩]
- Lauritano EC, Gabrielli M, Lupascu A, et al. Rifaximin dose-finding study for the treatment of small intestinal bacterial overgrowth. Aliment Pharmacol Ther. 2005;22:31–35. doi: 10.1111/j.1365-2036.2005.02516.x. https://www.ncbi.nlm.nih.gov/pubmed/15963077[↩]
- Pimentel M, Chow EJ, Lin HC. Normalization of lactulose breath testing correlates with symptom improvement in irritable bowel syndrome: a double-blind, randomized, placebo-controlled study. Am J Gastroenterol. 2003;98:412–419. https://www.ncbi.nlm.nih.gov/pubmed/12591062[↩][↩][↩][↩][↩]
- Posserud I, Stotzer P, Björnsson ES, Abrahamsson H, Simrén M. Small intestinal bacterial overgrowth in patients with irritable bowel syndrome. Gut. 2007;56(6):802-808. doi:10.1136/gut.2006.108712. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1954873/[↩]
- Lacy BE, Chey WD, Lembo AJ. New and Emerging Treatment Options for Irritable Bowel Syndrome. Gastroenterology & Hepatology. 2015;11(4 Suppl 2):1-19. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4612133/[↩]
- Weinberg DS, Smalley W, Heidelbaugh JJ, Sultan S American Gastroenterological Association. American Gastroenterological Association Institute Guideline on the pharmacological management of irritable bowel syndrome. Gastroenterology. 2014;147:1146–1148. doi: 10.1053/j.gastro.2014.09.001. https://www.ncbi.nlm.nih.gov/pubmed/25224526[↩][↩]
- Heaton, K W & Lewis, S J 1997, ‘Stool form scale as a useful guide to intestinal transit time’. Scandinavian Journal of Gastroenterology, vol.32, no.9, pp.920 – 924.[↩]
- Attar A, Flourié B, Rambaud JC, Franchisseur C, Ruszniewski P, Bouhnik Y. Antibiotic efficacy in small intestinal bacterial overgrowth-related chronic diarrhea: a crossover, randomized trial. Gastroenterology. 1999;117:794–797. doi: 10.1016/S0016-5085(99)70336-7. https://www.ncbi.nlm.nih.gov/pubmed/10500060[↩][↩][↩]
- Gatta L, Scarpignato C. Mo2055 Rifaximin for treatment of small intestine bacterial overgrowth (SIBO): a systematic review and meta-analysis. Gastroenterology. 2013;144(5 Suppl 1):S729. doi: 10.1016/S0016-5085(13)62707-9.[↩]
- Shah SC, Day LW, Somsouk M, Sewell JL. Meta-analysis: antibiotic therapy for small intestinal bacterial overgrowth. Alimentary pharmacology & therapeutics. 2013;38(8):10.1111/apt.12479. doi:10.1111/apt.12479. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3819138/[↩][↩]
- Lee BJ, Bak YT. Irritable bowel syndrome, gut microbiota and probiotics. J Neurogastroenterol Motil. 2011;17:252–266. doi: 10.5056/jnm.2011.17.3.252. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3155061/[↩]
- Thijssen AY, Jonkers D, Clemens CH, Masclee A. Effect of probiotic treatment on visceral hypersensitivity in irritable bowel syndrome. Gastroenterology. 2011;140(5 Suppl 1):S852.[↩]
- Lyszkowska M, Popinska K, Idzik M, Ksiazyk P. Probiotics in children with gut failure. J Pediatr Gastroenterol Nutr. 2008;46:543.[↩]
- Rosania R, Giorgio F, Principi M, et al. Effect of probiotic or prebiotic supplementation on antibiotic therapy in the small intestinal bacterial overgrowth: a comparative evaluation. Curr Clin Pharmacol. 2013;8:169–172. doi: 10.2174/15748847113089990048. https://www.ncbi.nlm.nih.gov/pubmed/23244247[↩][↩]
- Kim HJ, Camilleri M, McKinzie S, et al. A randomized controlled trial of a probiotic, VSL#3, on gut transit and symptoms in diarrhoea-predominant irritable bowel syndrome. Aliment Pharmacol Ther. 2003;17:895–904. doi: 10.1046/j.1365-2036.2003.01543.x. https://www.ncbi.nlm.nih.gov/pubmed/12656692[↩][↩]
- Kim HJ, Vazquez Roque MI, Camilleri M, et al. A randomized controlled trial of a probiotic combination VSL# 3 and placebo in irritable bowel syndrome with bloating. Neurogastroenterol Motil. 2005;17:687–696. doi: 10.1111/j.1365-2982.2005.00695.x. https://www.ncbi.nlm.nih.gov/pubmed/16185307[↩]
- Pimentel M, Soffer EE, Chow EJ, Kong Y, Lin HC. Lower frequency of MMC is found in IBS subjects with abnormal lactulose breath test, suggesting bacterial overgrowth. Dig Dis Sci. 2002;47:2639–2643. doi: 10.1023/A:1021039032413. https://www.ncbi.nlm.nih.gov/pubmed/12498278[↩]
- Pimentel M, Morales W, Lezcano S, Sun-Chuan D, Low K, Yang J. Low-Dose Nocturnal Tegaserod or Erythromycin Delays Symptom Recurrence After Treatment of Irritable Bowel Syndrome Based on Presumed Bacterial Overgrowth. Gastroenterology & Hepatology. 2009;5(6):435-442. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2886395/[↩]
- Irritable bowel syndrome and diet: where are we in 2018 ? Current Opinion in Clinical Nutrition & Metabolic Care: November 2017 – Volume 20 – Issue 6 – p 456–463. http://journals.lww.com/co-clinicalnutrition/Abstract/2017/11000/Irritable_bowel_syndrome_and_diet___where_are_we.6.aspx[↩]
- Low-FODMAP Diet. American College of Gastroenterology. http://patients.gi.org/topics/low-fodmap-diet/[↩]
- Low FODMAP diet for Irritable Bowel Syndrome. Monash University. https://www.monash.edu/medicine/ccs/gastroenterology/fodmap[↩]
- Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. Gibson PR, Shepherd SJ. J Gastroenterol Hepatol. 2010 Feb; 25(2):252-8. https://www.ncbi.nlm.nih.gov/pubmed/20136989/[↩]
- Magge S, Lembo A. Low-FODMAP Diet for Treatment of Irritable Bowel Syndrome. Gastroenterology & Hepatology. 2012;8(11):739-745. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3966170/[↩]
- Gibson PR, Barrett JS. Clinical ramifications of malabsorption of fructose and other short-chain carbohydrates. Practical Gastroenterology. 2007;31:51–65.[↩][↩][↩]





{kind=link}