Contents
What is acoustic neuroma
Acoustic neuroma (also known as vestibular schwannoma, acoustic neurinoma, or acoustic neurilemoma) is a rare benign (non-cancerous), usually slow-growing tumor that develops from the balance and hearing nerves supplying the inner ear – the 8th cranial nerve (also known as the acoustic nerve or vestibulocochlear nerve) consists of the vestibular and cochlear divisions, which runs from the inner ear to the brain. Branches of the vestibular nerve directly influence your balance and branches of the cochlear division influence your hearing, and pressure from an acoustic neuroma can cause hearing loss, ringing in your ear and unsteadiness. The tumor comes from an overproduction of Schwann cells–the cells that normally wrap around nerve fibers like onion skin to help support and insulate nerves. Acoustic neuromas generally originate within the internal auditory canal and may cause bony erosion as they expand. A untreated acoustic neuroma tumor will protrude further into the brain and may eventually compromise other nerves and brainstem function. As the acoustic neuroma grows, it presses against the hearing and balance nerves (the 8th cranial nerve or vestibulocochlear nerve), usually causing unilateral (one-sided) or asymmetric hearing loss, tinnitus (ringing in the ear), and dizziness/loss of balance. As the tumor grows, it can interfere with the face sensation nerve (the 5th cranial nerve or the trigeminal nerve), causing facial numbness. Acoustic neuromas can also affect the facial nerve (the 7th cranial nerve for the muscles of the face) causing facial weakness or paralysis on the side of the tumor. If the tumor becomes large, it will eventually press against nearby brain structures (such as the brainstem and the cerebellum), becoming life-threatening. Acoustic neuromas do not spread (metastasize) to other parts of the body. The brain is not invaded by the acoustic tumor, but the tumor pushes on the brain as it enlarges.
Acoustic neuromas occur throughout the world. No ethnic groups are affected disproportionately. It is estimated that the instances of acoustic neuroma are between 1 to 3.5 in every 100,000 to 5 in every million people. Acoustic tumors constitute 6%-10% of all brain tumors and are found in roughly one of every 100,000 people per year in the United States. This translates to about 2,500-3,000 newly diagnosed acoustic tumors per year. Acoustic neuromas more common in men and between the ages of 30-60 years.
Acoustic neuromas are nearly always slow growing, do not spread, and are thought of as benign tumors. Often they have been there a long time by the time they are diagnosed. Acoustic neuromas are found most often in older people. Loss of hearing in one ear can be a sign of acoustic neuroma.
Rarely, acoustic neuromas are associated with a genetic condition called neurofibromatosis. People with neurofibromatosis are usually diagnosed at a much younger age and tumors might be on both sides of the brain (bilateral). Those affected might also develop another type of brain tumor called meningiomas.
Because the acoustic neuroma grows so slowly, the symptoms are easy to miss or misinterpret. The earliest and most common symptoms of an acoustic neuroma are a gradual reduction in hearing in one ear and tinnitus, a ringing or noisy sound in the ear.
Other possible symptoms of acoustic neuroma that may occur, depending on the extent of the tumor, include: dizziness, loss of balance or clumsiness facial paralysis, numbness or tingling, headache, a feeling of something clogging the ear, or mental confusion.
Most of these tumors grow slowly, taking years before they become large enough to cause symptoms. Once diagnosed, they must be treated or carefully observed; they do not resolve on their own.
Types of acoustic neuroma
- Unilateral (one side) occurs spontaneously without any evidence of family history, accounts for 95% of acoustic neuromas
- Bilateral (both sides) is most likely caused by a genetic condition called Neurofibromatosis Type 2 (NF2) which affects approximately 1 in every 40,000 people. Neurofibromatosis Type 2 will be suspected if a parent/sibling/child of the patient has Neurofibromatosis Type 2 and acoustic neuroma occurs before age 30 or if the patient has had a meningioma, glioma, or cataract.
Treatment will depend on the size of your tumor. The treatment options are observation (watchful waiting), surgical removal or radiation therapy. The choice of treatment may be based on tumor size, hearing in the ear at time of diagnosis, patient age and health, and patient preference.
Figure 1. Vestibulocochlear nerve (Cranial nerve 8)

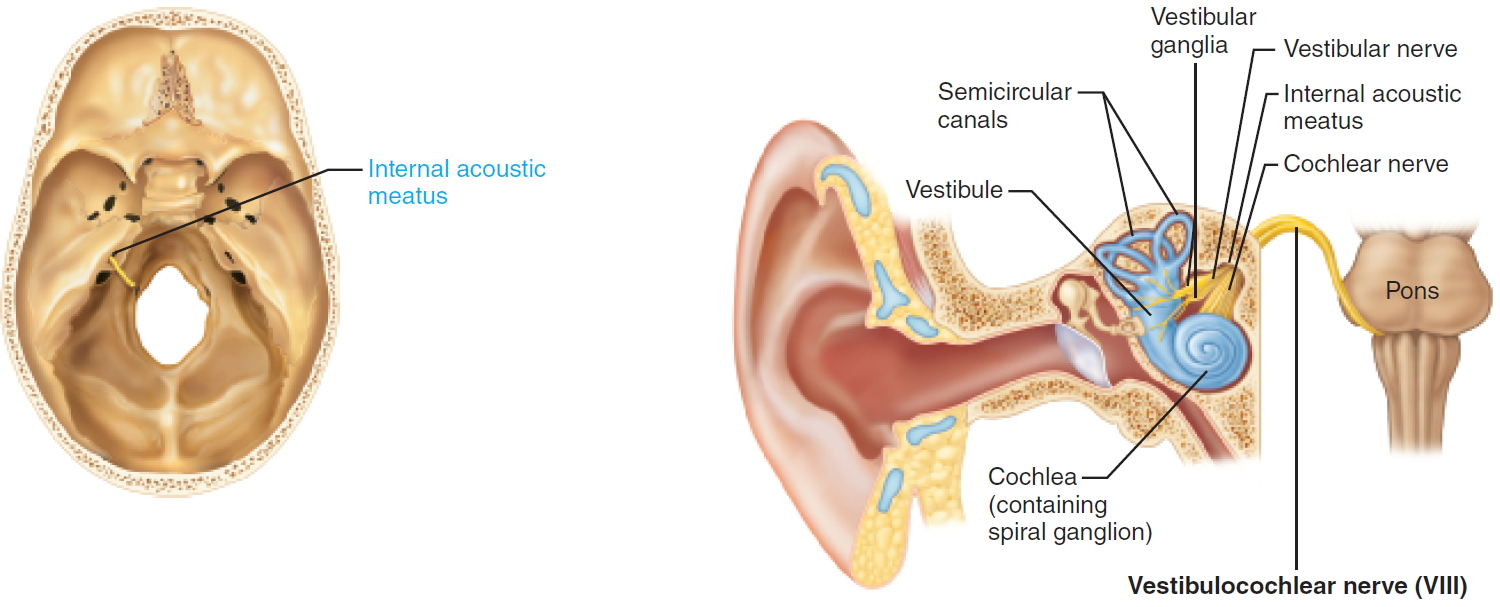 Note: The normal anatomy of the ear. The outer ear funnels sound to the eardrum, which vibrates three tiny bones called ossicles (malleus, incus and stapes). The spiral-shaped cochlea is filled with liquid, which moves in response to vibrations. As the fluid moves, thousands of hair cells are stimulated, sending signals along the cochlear nerve (responsible for hearing) to the brain. Attached to the cochlea are three semicircular canals positioned at right angles to each other. The three canals are able to sense head position and posture. Electrical signals from the semicircular canals are carried to the brain by the superior and inferior vestibular nerves (responsible for balance). The cochlear and vestibular nerves form a bundle inside the bony internal auditory canal. Inside the canal, the vestibulocochlear nerve lies next to the facial nerve (responsible for facial movement).
Note: The normal anatomy of the ear. The outer ear funnels sound to the eardrum, which vibrates three tiny bones called ossicles (malleus, incus and stapes). The spiral-shaped cochlea is filled with liquid, which moves in response to vibrations. As the fluid moves, thousands of hair cells are stimulated, sending signals along the cochlear nerve (responsible for hearing) to the brain. Attached to the cochlea are three semicircular canals positioned at right angles to each other. The three canals are able to sense head position and posture. Electrical signals from the semicircular canals are carried to the brain by the superior and inferior vestibular nerves (responsible for balance). The cochlear and vestibular nerves form a bundle inside the bony internal auditory canal. Inside the canal, the vestibulocochlear nerve lies next to the facial nerve (responsible for facial movement).Figure 2. General structure of a neuron
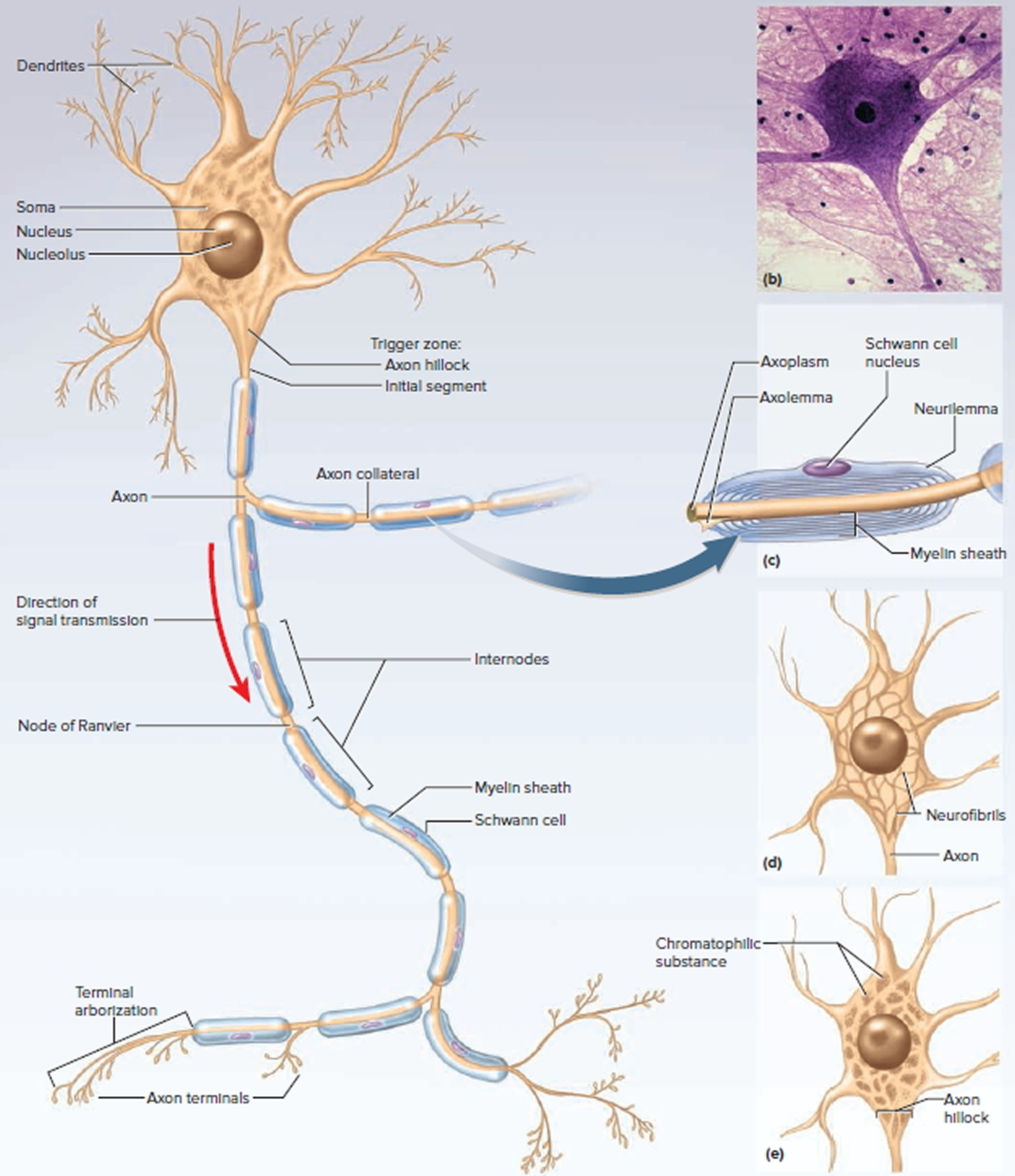
Figure 3. Schwann cell and myelination
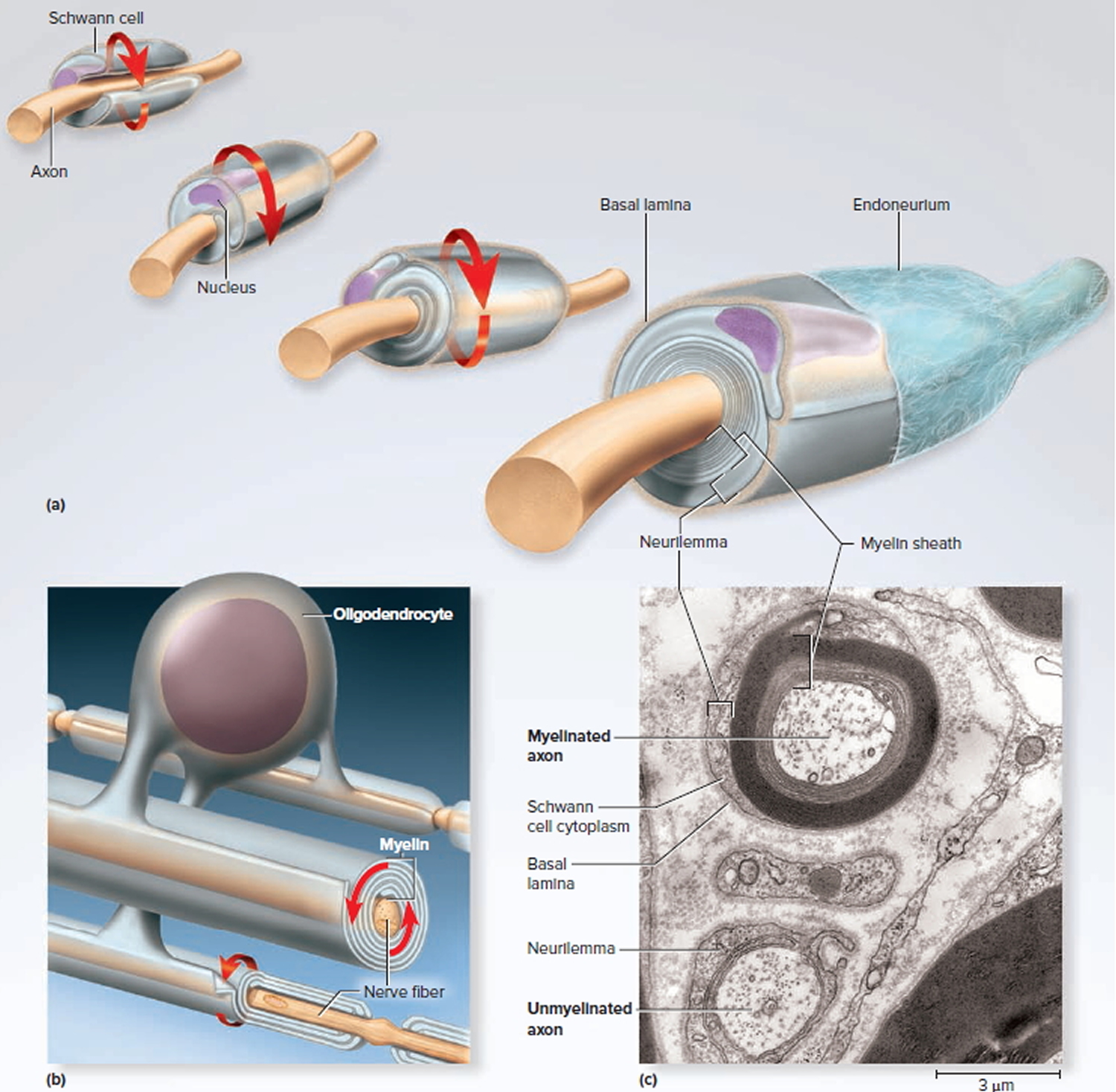
Note: (a) A Schwann cell of the peripheral nervous system, wrapping repeatedly around an axon to form the multilayered myelin sheath.
The myelin spirals outward away from the axon as it is laid down.
(b) An oligodendrocyte of the central nervous system (brain and spinal cord) wrapping around the axons of multiple neurons. Here, the myelin spirals inward toward the axon as it is laid down.
(c) A myelinated axon (top) and unmyelinated axon (bottom).
Figure 4. Acoustic neuroma
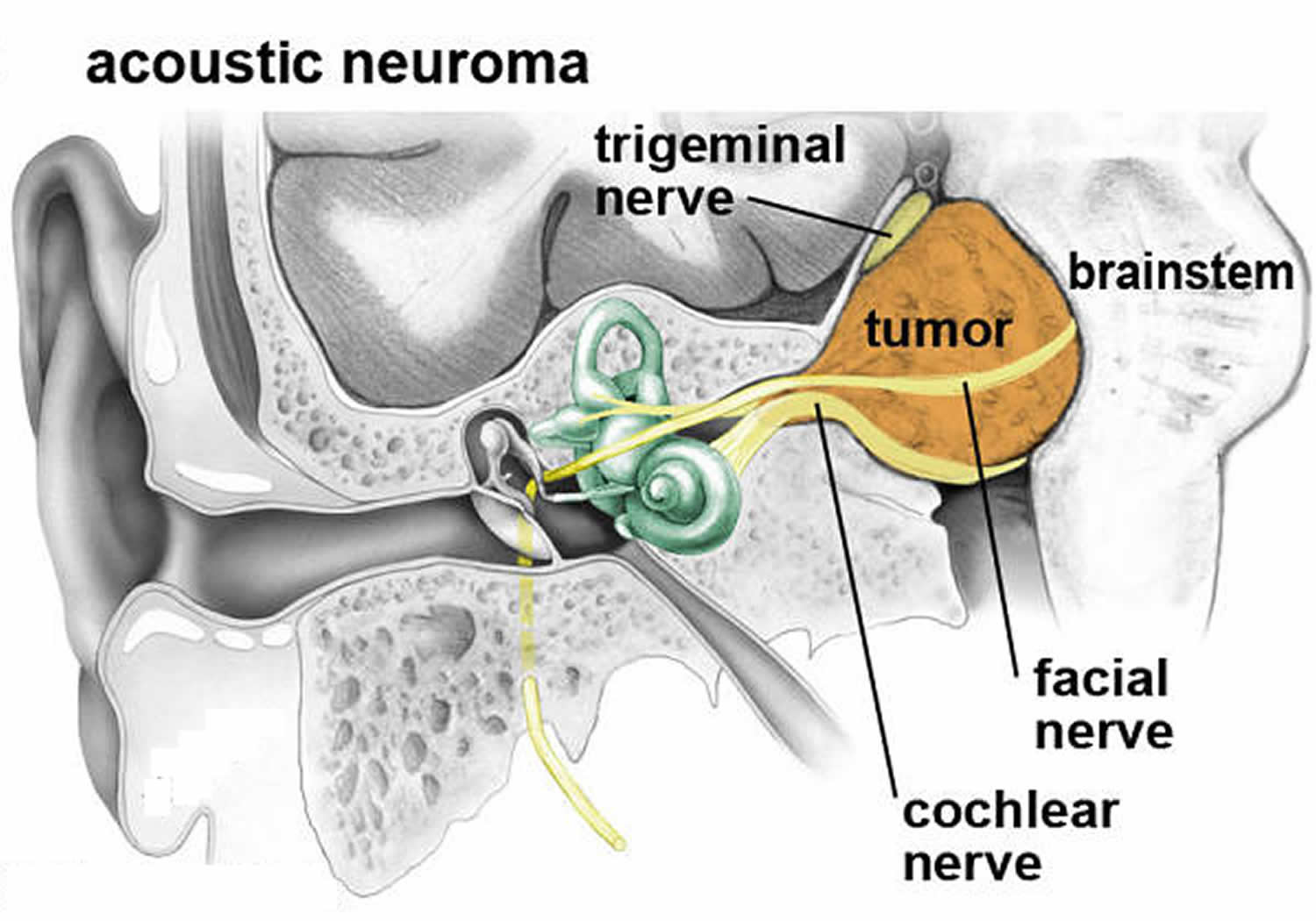 Note: An acoustic neuroma expands out of the internal auditory canal displacing the cochlear, facial and trigeminal nerves located in the cerebellopontine angle. Eventually the tumor can compress the brainstem.
Note: An acoustic neuroma expands out of the internal auditory canal displacing the cochlear, facial and trigeminal nerves located in the cerebellopontine angle. Eventually the tumor can compress the brainstem.Figure 5. Acoustic neuroma
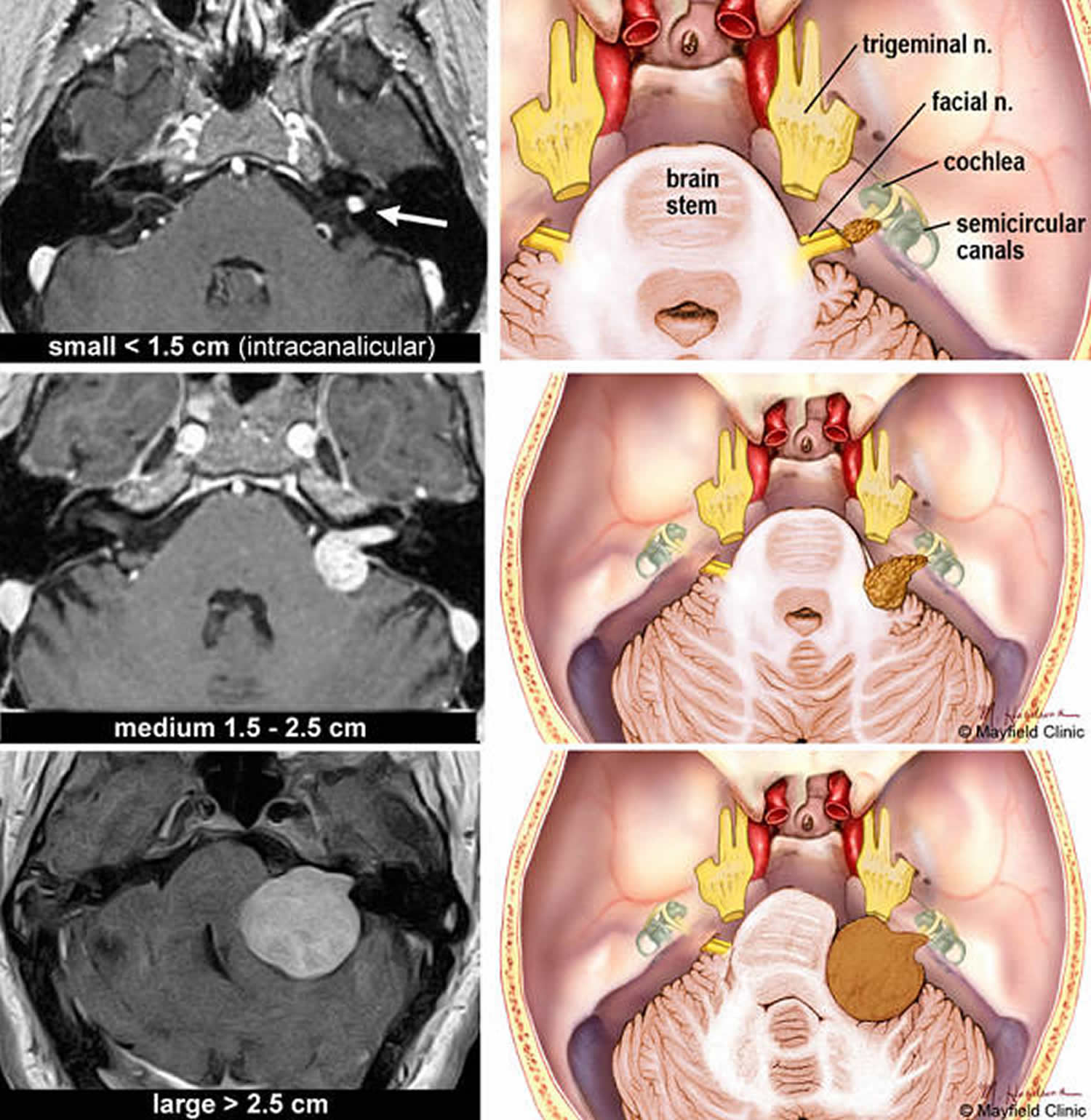
Note: Acoustic neuromas are classified according to their size. MRI scans and correlative illustrations of small (intracanalicular), medium and large acoustic neuromas.
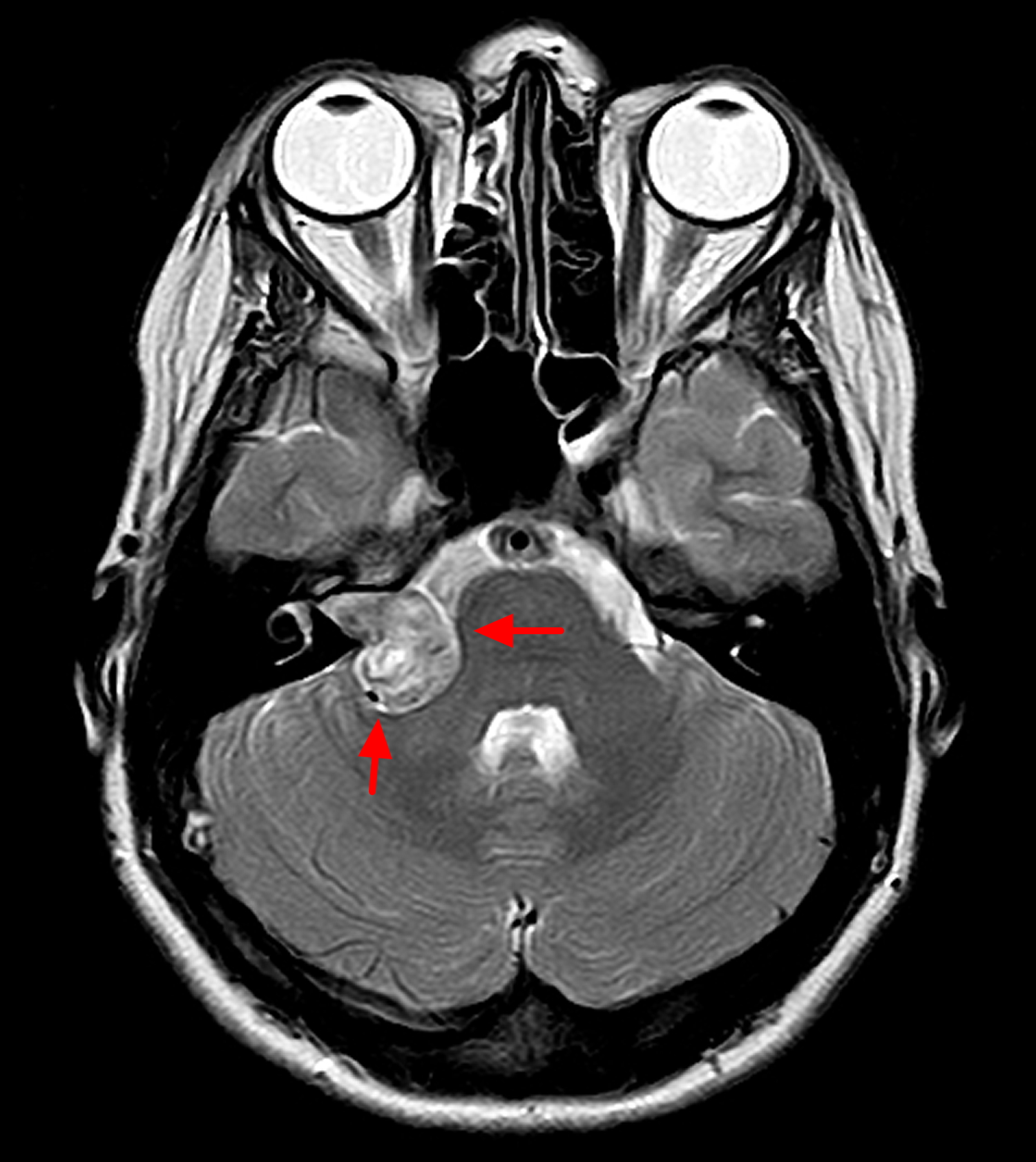
Figure 6. Acoustic neuroma MRI
Acoustic neuroma causes
The cause of acoustic neuromas appears to be or a spontaneous mutation (alteration in genetic material) or a malfunctioning gene on chromosome 22 1. Normally, this gene produces a tumor suppressor protein that helps control the growth of Schwann cells covering the nerves.
What makes this gene malfunction isn’t clear, and in most cases of acoustic neuroma, there is no identifiable cause. This faulty gene is also inherited in neurofibromatosis type 2, a rare disorder that usually involves the growth of tumors on balance nerves on both sides of your head (bilateral vestibular schwannomas).
Risk factors for acoustic neuroma
Neurofibromatosis type 2
The only confirmed risk factor for acoustic neuroma is having a parent with the rare genetic disorder neurofibromatosis type 2. But neurofibromatosis type 2 only accounts for about 5 percent of acoustic neuroma cases.
Neurofibromatosis type 2 (NF2) is a genetic disorder that is inherited in an autosomal dominant pattern, meaning that the mutation can be passed on by just one parent (dominant gene). Each child of an affected parent has a 50-50 chance of inheriting it. Neurofibromatosis type 2, occurs with a frequency of 1 in 30,000 to 1 in 50,000 births.
A hallmark characteristic of neurofibromatosis type 2 is the development of noncancerous acoustic neuromas on both sides of your head, as well as on other nerves. This creates the perplexing problem of the possibility of complete deafness if the tumors are left to grow unchecked. Preventing or treating the complete deafness that may befall individuals with neurofibromatosis type 2 requires complex decision making. The trend at most academic U.S. medical centers is to recommend treatment for the smallest tumor which has the best chance of preserving hearing. If this goal is successful, then treatment can also be offered for the remaining tumor. If hearing is not preserved at the initial treatment, then usually the second tumor, in the only-hearing ear, is just observed. If it shows continued growth and becomes life-threatening, or if the hearing is lost over time as the tumor grows, then treatment is undertaken. This strategy has the highest chance of preserving hearing for the longest time possible.
There are now several options to try to rehabilitate deafness in neurofibromatosis type 2 patients. Implanting the hearing part of the brainstem (auditory brainstem implant) can help restore some sound perception to these patients. Also cochlear implants can be used if the cochlear nerve is preserved following surgery. Radiosurgery may be an option although stereotactic radiosurgery may not have the effect on the neurofibromatosis type 2 patient as in patients with unilateral sporadic acoustic neuroma tumors.There are some centers using radiation therapy for neurofibromatosis type 2 with mixed results. The risk of malignant transformation after radiation is higher in this group. Recent studies have shown that these individuals may have more tumors that are resistant to radiation, due to the cell type. These cases should be handled in centers with very experienced skull base teams.
Acoustic neuroma prognosis
Acoustic neuromas are not malignant and do not spread to other parts of the body. The average growth rate of an acoustic neuroma is approximately 1.5 millimeters per year. Several studies have demonstrated that as many as 50% of tumors show little to no growth over long periods of time (5 to 10 years). No known environmental or dietary factors are known to influence the growth rate of acoustic neuromas.
However, some untreated neuromas can grow very aggressively and cause severe and permanent damage to nerves, ear and brain tissue. Hearing loss and balance problems related to the tumor may remain, even after treatment by surgery or radiation. If an acoustic neuroma is diagnosed early, when the tumour is small, treatment is more likely to preserve hearing.
Acoustic neuroma complications
An acoustic neuroma may cause a variety of permanent complications, including:
- Hearing loss
- Facial numbness and weakness
- Difficulties with balance
- Ringing in the ear
Large tumors may press on your brainstem, preventing the normal flow of fluid between your brain and spinal cord (cerebrospinal fluid). In this case, fluid can build up in your head (hydrocephalus), increasing the pressure inside your skull.
Some symptoms of an acoustic neuroma can be difficult to live with and may affect your quality of life. For example, hearing impairment may have an impact on your job and communication may be more difficult. Severe dizziness and loss of balance may also affect your job and limit the activities you can do.
Speak to your doctor or specialist if your acoustic neuroma is being monitored but you feel the symptoms are significantly affecting your daily life. There may be ways of easing your symptoms, such as using a hearing aid or painkilling medication, or you may need treatment to remove the tumor.
Recurrence
Occasionally, acoustic neuromas return after being removed. The tumors reoccur in less than five in every 100 people who have surgery to remove them.
It’s likely that you’ll need to have magnetic resonance imaging (MRI) scans over a number of years, regardless of which treatment you have.
Hydrocephalus
One of the most serious complications of acoustic neuroma is a condition called hydrocephalus.
Hydrocephalus occurs when an acoustic neuroma is very large and presses on your brainstem (the lowest part of the brain that connects to the spinal cord).
This prevents the cerebrospinal fluid (CSF) from flowing between your brain and spinal cord. The blockage can cause pressure to build up inside your skull, which in turn puts pressure on the delicate tissues in your brain.
Hydrocephalus can be treated by draining away the excess CSF. It’s important that it’s treated quickly because in severe cases it can cause brain damage. In rare cases, hydrocephalus can be fatal.
Acoustic neuroma symptoms
Usually acoustic neuromas (acoustic neuromas) grow very slowly and the signs and symptoms of acoustic neuroma are often subtle and may take many years to develop. This means there may not be any symptoms in the early stages when the tumor is small.
Many people say they notice some loss of hearing and tinnitus, or ringing in the ears. Usually one ear is affected, but both ears can be involved if the person has neurofibromatosis type 2. Pressure from the tumor on adjacent nerves controlling facial muscles and sensation (facial and trigeminal nerves), nearby blood vessels, or brain structures may also cause problems.
Whether or not there are any other symptoms can depend on the size of the tumor and how hard it presses on the eighth cranial nerve. Some people with an acoustic neuroma get:
- Hearing loss, usually gradual — although in some cases sudden — and occurring on only one side or more pronounced on one side
- Ringing (tinnitus) in the affected ear
- Dizziness or vertigo, which is a feeling that the space around you is spinning
- Loss of balance
- Headache
- Facial numbness or tingling.
In rare cases, an acoustic neuroma may grow large enough to compress the brainstem and become life-threatening.
Acoustic neuroma diagnosis
Acoustic neuroma is often difficult to diagnose in the early stages because signs and symptoms may be subtle and develop gradually over time. Common symptoms such as hearing loss are also associated with many other middle and inner ear problems.
After asking questions about your symptoms, your doctor will conduct an ear exam. Your doctor may order the following tests:
- Hearing test (audiometry). In this test, conducted by a hearing specialist (audiologist), you hear sounds directed to one ear at a time. The audiologist presents a range of sounds of various tones and asks you to indicate each time you hear the sound. Each tone is repeated at faint levels to find out when you can barely hear. The audiologist may also present various words to determine your hearing ability.
- Imaging. Magnetic resonance imaging (MRI) is the preferred imaging test to confirm the presence of acoustic neuroma and can detect tumors as small as 1 to 2 millimeters in diameter. If MRI is unavailable or you can’t tolerate an MRI scan, computerized tomography (CT) may be used, but it may miss very small tumors.
Acoustic neuroma treatment
Your acoustic neuroma treatment may vary, depending on the size and growth of the acoustic neuroma, your overall health, and if you’re experiencing symptoms. To treat acoustic neuroma, your doctor may suggest one or more of three potential treatment methods: monitoring, surgery or radiation therapy.
The options for treatment include:
- no treatment – just monitoring the tumor growth and related symptoms
- surgery – to cut out the tumor
- stereotactic treatment – this procedure sends focused radiation to the tumor to stop it from growing.
Which treatment you have depends on the size and location or the tumor, your symptoms, your age and general health, and what you want.
Even though acoustic neuromas are not cancerous, they can cause serious, permanent damage to nerves. If you have any of the symptoms listed above, see your doctor as soon as possible.
Monitoring
If you have an acoustic neuroma that’s very small or growing very slowly, you may not need to have any immediate treatment. Instead, your condition will be carefully monitored.
Research suggests that up to three-quarters of acoustic neuromas don’t appear to be growing, so monitoring the tumor is all that’s needed.
Simply monitoring an acoustic neuroma is often the best option because the risks associated with surgery or radiosurgery (see below) outweigh the risk of the tumor having an adverse effect on your health.
Your doctor may recommend that you have regular imaging and hearing tests, usually every six to 12 months, to determine whether the tumor is growing and how quickly.
To help monitor your condition, you’ll need to have regular magnetic resonance imaging (MRI) scans (where a magnetic field and radio waves are used to create an image of the inside of your body). The MRI scan will be used to check the size and growth of your acoustic neuroma.
Other treatments may be considered if the tumor shows any signs of growing or if there’s a risk of it significantly affecting your health.
You may need to have an MRI scan every one to two years, although this will depend on your general health and the size of your tumor.
Acoustic neuroma surgery
You may need surgery to remove an acoustic neuroma. Your surgeon may use one of several techniques for removing an acoustic neuroma, depending on the size of your tumor, hearing status and other factors.
The goal of surgery is to remove the tumor, preserve the facial nerve to prevent facial paralysis and preserve hearing when possible.
Surgery for an acoustic neuroma is performed under general anesthesia and involves removing the tumor through the inner ear or through a window in your skull.
The entire tumor may not be able to be completely removed in certain cases. For example, if the tumor is too close to important parts of the brain or the facial nerve.
Sometimes, surgical removal of the tumor may worsen symptoms if the hearing, balance or facial nerves are damaged during the operation.
Complications may include:
- Leakage of cerebrospinal fluid (CSF) through the wound
- Hearing loss
- Facial weakness
- Facial numbness
- Ringing in the ear
- Balance problems
- Persistent headache
- Infection of the cerebrospinal fluid (meningitis)
- Stroke or brain bleeding
Microsurgery
Microsurgery can be used to remove an acoustic neuroma. The surgery will be carried out under general anesthetic and the acoustic neuroma will be removed through an incision made in your skull.
Small acoustic neuromas can usually be completely removed. If you have a large tumor, a small part will occasionally be left behind to minimize the risk of damaging the facial nerve, which runs next to the acoustic nerve.
If a small part of the tumor remains, it can either be monitored with MRI scans or effectively treated using radiosurgery (see below).
- Hearing loss
After surgery to remove an acoustic neuroma, hearing in the ear affected by the tumor is almost always lost.
You may wish to discuss the possibility of having a ‘bone anchored hearing aid’ with your ENT (ear, nose and throat) surgeon, which will help divert sound from your affected ear to your good ear.
- Facial nerve damage
Surgery can occasionally damage the facial nerve (7th cranial nerve). This is because the acoustic nerve is very close to the facial nerve and large tumors are often stuck to it. Your surgeon will try not to damage your facial nerve and with large tumors will sometimes leave a small part of the tumor on the facial nerve to try to preserve it.
If your facial nerve is damaged during surgery you may find that:
- your face droops on one side (facial palsy)
- you drool saliva on the weak side of your face
- you have difficulty closing your eye on the weak side of your face
- your speech is less clear
These symptoms may improve within six to 12 months of having surgery and be helped with physiotherapy. However, it’s important to be aware that some damage to your facial nerve may be permanent.
Facial nerve damage can also affect your eyes. For example, you may find it difficult to blink or close your eye completely on the side that was operated on. As a result, your eye may dry out and you may need to use artificial tears (eye lubricant).
In cases where the tumor is small, less than one in every 100 people’s facial nerve will be badly affected after treatment.
For large tumors, around three in 10 people will have permanent, severe facial nerve weakness after surgery if a complete tumor removal is attempted. This falls to around one person in over 100 if a small part of the tumor is left on the facial nerve to preserve it.
Any minor post-surgery facial nerve weakness is likely to be temporary, although it may take several months to recover.
Recovery from surgery
Following surgery, you’ll usually need to spend up to a week in hospital to recuperate.
You should be able to return to work after about two months. The length of time it takes you to recover may depend on the size and position of the tumor that was removed. The healthcare professionals treating you will be able to advise you further.
If your acoustic neuroma was completely removed, you won’t usually need further treatment. However, you’ll continue to be monitored with MRI scans.
Radiation therapy
Stereotactic radiosurgery
Stereotactic radiosurgery delivers a very focused and precise dose of radiation to your acoustic neuroma. Stereotactic means locating a point (in this case the position of the tumor in your brain) using three-dimensional co-ordinates.
During stereotactic radiosurgery, the maximum amount of radiation will be aimed at your tumor without the surrounding tissue being exposed. It may be given as a single dose or delivered over several sessions. It doesn’t get rid of your tumor but aims to stop it growing further. It can only be used on small tumors or the remains of a tumor after surgery on large tumors. It’s not usually used for large tumors.
Stereotactic radiosurgery is carried out under local anesthetic, which means you’ll be conscious throughout the procedure but your scalp will be numbed. A lightweight metal frame is usually attached to the scalp and a series of scans will accurately pinpoint the position of the tumor. It can then be treated using a precise beam of radiation.
The goal of stereotactic radiosurgery is to stop the growth of a tumor, preserve the facial nerve’s function and possibly preserve hearing.
Immediate side effects of stereotactic radiosurgery are rare, and you’ll usually only need to take a couple of days off work to have the treatment. Risks of radiosurgery include hearing loss, ringing in the ear, facial weakness, facial numbness, balance problems and treatment failure (continued tumor growth).
It may take weeks, months or years before the effects of radiosurgery become evident. Your doctor will monitor your progress with follow-up imaging studies and hearing tests.
- Nerve damage
In some cases, stereotactic radiosurgery can cause nerve damage, although it may not be apparent until several weeks or months after treatment.
Symptoms of nerve damage can include:
- facial numbness (loss of feeling)
- facial paralysis (an inability to move part of your face)
- hearing loss
Facial paralysis affects around one in every 100 people who has stereotactic radiosurgery. It’s estimated that just under a third of people may experience hearing loss after stereotactic radiosurgery.
Stereotactic radiotherapy
Fractionated stereotactic radiotherapy (SRT) delivers a small dose of radiation to the tumor over several sessions in an effort to curb the growth of the tumor without damaging surrounding brain tissue.
Proton beam therapy
This type of radiation therapy uses high-energy beams of positively charged particles called protons that are delivered to the affected area in targeted doses to treat tumors and minimize radiation exposure to the surrounding area.
Coping and support
Dealing with the possibility of hearing loss and facial paralysis and deciding which treatment would be best for you can be quite stressful. Here are some suggestions you may find helpful:
- Educate yourself about acoustic neuroma. The more you know, the better prepared you’ll be to make good choices about treatment. Besides talking to your doctor and your audiologist, you may want to talk to a counselor or social worker. Or you may find it helpful to talk to other people who’ve had an acoustic neuroma and learn more about their experiences during and after treatment.
- Maintain a strong support system. Family and friends can help you as you go through this difficult time. Sometimes, though, you may find the concern and understanding of other people with acoustic neuroma especially comforting.
Your doctor or a social worker may be able to put you in uch with a support group. Or you may find an in-person or online support group through the Acoustic Neuroma Association (https://www.anausa.org/).
- Irving RM, Harada T, Moffat DA, Hardy DG, Whittaker JL, Xuereb JH, Maher ER. Somatic neurofibromatosis type 2 gene mutations and growth characteristics in vestibular schwannoma. Am J Otol. 1997 Nov; 18(6): 754-60[↩]





{kind=link}