Contents
What is acromegaly
Acromegaly is a rare but serious condition caused by too much growth hormone (GH) in the blood, causing body tissues and bones to grow more quickly.
Over time, the excess growth hormone (GH) leads to abnormally large hands and feet, and a wide range of other symptoms.
Acromegaly is usually diagnosed in adults aged 30 to 50 but can affect people of any age. When it develops before puberty, it’s known as “gigantism”.
Growth hormone (GH) is released into the bloodstream by the pituitary gland, located at the base of the brain. The blood carries growth hormone (GH) to other parts of the body where it has specific effects. In children, growth hormone (GH) stimulates growth and development. In adults, growth hormone (GH) affects energy levels, muscle strength, bone health, and one’s sense of well-being. Too much growth hormone (GH) in children is called gigantism and is extremely rare. Acromegaly in adults occurs mainly in middle-aged men and women. Acromegaly is a very rare condition. Each year, about three new cases of acromegaly occur for every million people.
Acromegaly is usually caused by a non-cancerous tumor in the pituitary gland called a pituitary adenoma. The tumor produces too much growth hormone (GH) and raises the level of growth hormone in the blood. When growth hormone (GH) is secreted into your bloodstream, it triggers your liver to produce a hormone called insulin-like growth factor-I (IGF-I). In turn, insulin-like growth factor-I (IGF-I) stimulates the growth of bones and other tissues. If your pituitary gland makes too much growth hormone (GH), excessive amounts of IGF-I can result. Too much insulin-like growth factor-I (IGF-I) can cause abnormal growth of your soft tissues and skeleton and other signs and symptoms characteristic of acromegaly and gigantism. Rarely, acromegaly is caused by hormone-producing tumors in other parts of the body.
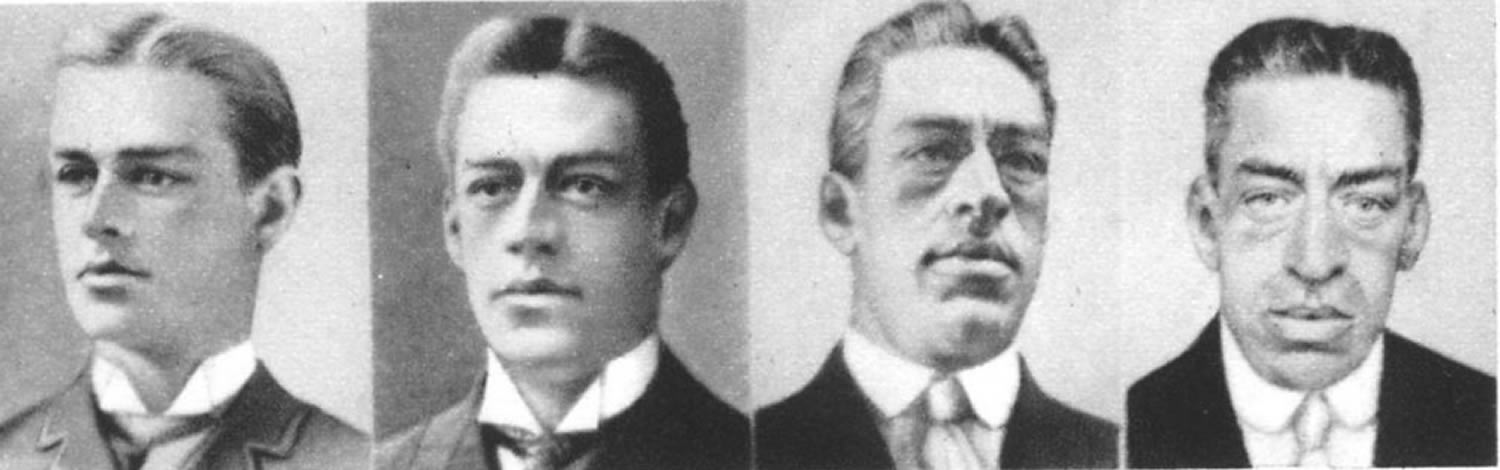
Because acromegaly is uncommon and physical changes occur gradually, the condition often isn’t recognized immediately: sometimes not for years. The earlier the tumor is detected, the sooner the treatment can occur, and the fewer long-term changes in appearance the individual will experience, which is why knowing the definition of acromegaly is important. Those who suspect they may be suffering from this pituitary condition should consult with a doctor as soon as possible.
Gigantism vs Acromegaly
Gigantism causes children to grow taller than average. This condition, which most often affects children, occurs due to a noncancerous tumor on the pituitary gland that creates too much growth hormone. Children with gigantism will grow unusually tall, and many will experience delayed puberty.
Unfortunately, diagnosing gigantism can be difficult for parents, because the condition does not cause many signs other than unusual height. If the family is an unusually tall family, this may simply be attributed to a growth spurt or the child’s genetic makeup.
Early diagnosis of gigantism is important for the child’s health and well-being. The condition is treatable by removing the tumor, but once the growth has occurred the child is not going to shrink back to an average height. For this reason, the earlier the condition is treated, the better the outcome is for the child.
The definition of acromegaly is a disease caused by noncancerous tumors in the pituitary gland that cause secretions of growth hormone. The difference between acromegaly and gigantism is that acromegaly occurs in adults, typically between the ages of 30 and 50.
Hypothalamus and Pituitary Gland
The pituitary gland is a pea-shaped structure that measures 1–1.5 cm (0.5 in.) in diameter and lies in the hypophyseal fossa of the sella turcica of the sphenoid bone (see Figure 1). The pituitary gland attaches to the hypothalamus by a stalk, the infundibulum and has two anatomically and functionally separate portions:
- the anterior pituitary and
- the posterior pituitary.
The anterior pituitary (anterior lobe), also called the adenohypophysis, accounts for about 75% of the total weight of the gland and is composed of epithelial tissue. The anterior pituitary consists of two parts in an adult: The pars distalis is the larger portion, and the pars tuberalis forms a sheath around the infundibulum.
The posterior pituitary (posterior lobe), also called the neurohypophysis, is composed of neural tissue. It also consists of two parts: the pars nervosa, the larger bulbar portion, and the infundibulum.
A third region of the pituitary gland called the pars intermedia atrophies during human fetal development and ceases to exist as a separate lobe in adults. However, some of its cells migrate into adjacent parts of the anterior pituitary, where they persist.
Anterior Pituitary
The anterior pituitary secretes hormones that regulate a wide range of bodily activities, from growth to reproduction.
Types of Anterior Pituitary Cells and Their Hormones
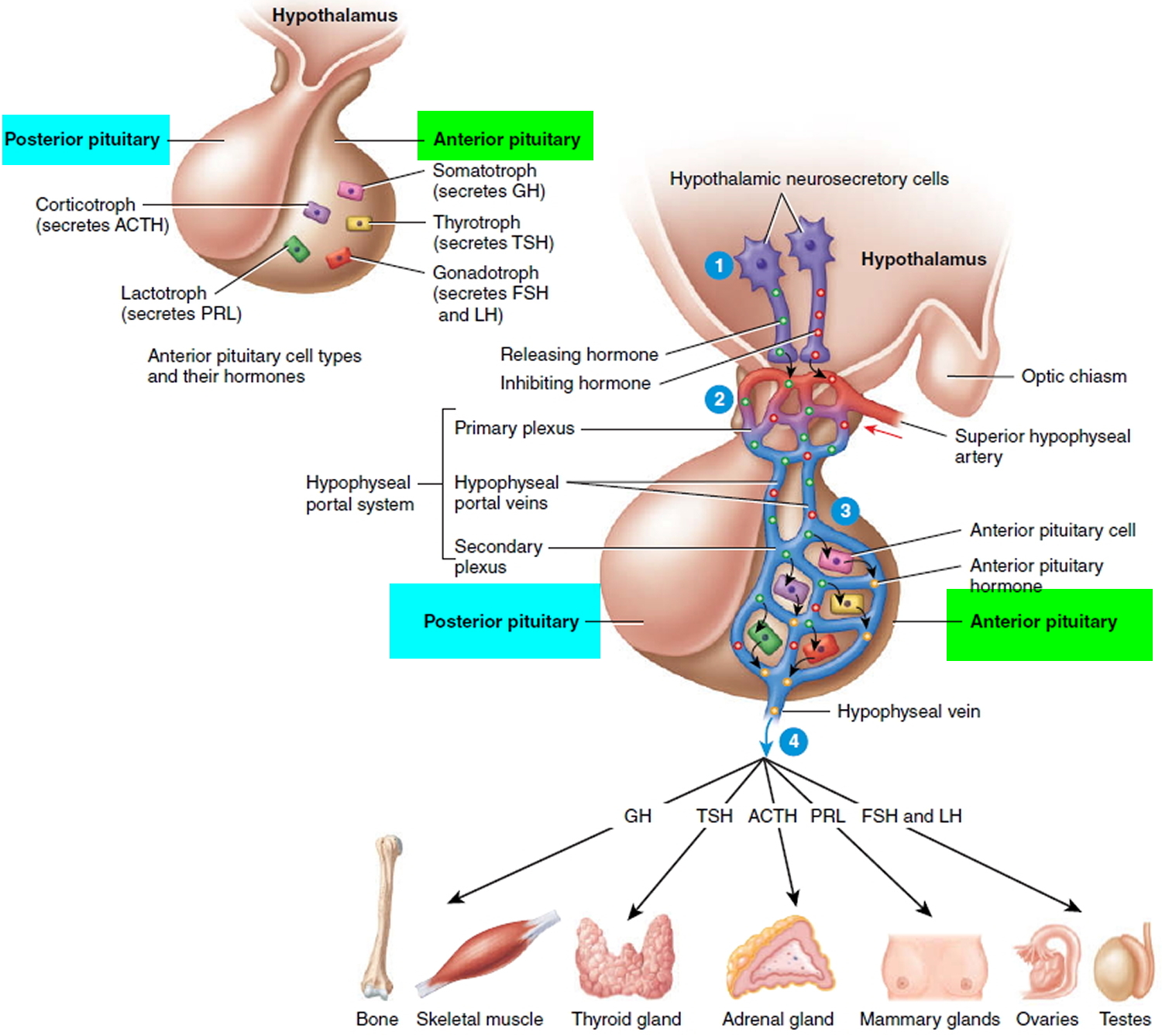
Five types of anterior pituitary cells—somatotrophs, thyrotrophs, gonadotrophs, lactotrophs, and corticotrophs—secrete seven hormones:
- 1. Somatotrophs secrete growth hormone (GH), also known as human growth hormone (hGH) or somatotropin. Growth hormone stimulates general body growth and regulates aspects of metabolism.
- 2. Thyrotrophs secrete thyroid-stimulating hormone (TSH), also known as thyrotropin. TSH controls the secretions and other activities of the thyroid gland.
- 3. Gonadotrophs secrete two gonadotropins: follicle-stimulating hormone (FSH) and luteinizing hormone (LH). FSH and LH both act on the gonads (testes and ovaries). In men, they stimulate the testes to produce sperm and to secrete testosterone. In women, they stimulate the ovaries to mature oocytes (eggs) and to secrete estrogens and progesterone.
- 4. Lactotrophs secrete prolactin (PRL), which initiates milk production in the mammary glands.
- 5. Corticotrophs secrete adrenocorticotropic hormone (ACTH), also known as corticotropin, which stimulates the adrenal cortex to secrete glucocorticoids such as cortisol. Some corticotrophs, remnants of the pars intermedia, also secrete melanocyte stimulating hormone (MSH).
Hypothalamic Control of the Anterior Pituitary
Release of anterior pituitary hormones is regulated in part by the hypothalamus. The hypothalamus secretes five releasing hormones, which stimulate secretion of anterior pituitary hormones:
- 1. Growth hormone-releasing hormone (GHRH), also known as somatocrinin, stimulates secretion of growth hormone.
- 2. Thyrotropin-releasing hormone (TRH) stimulates secretion of thyroid-stimulating hormone.
- 3. Corticotropin-releasing hormone (CRH) stimulates secretion of adrenocorticotropic hormone.
- 4. Prolactin-releasing hormone (PRH) stimulates secretion of prolactin.
- 5. Gonadotropin-releasing hormone (GnRH) stimulates secretion of FSH and LH.
The hypothalamus also produces two inhibiting hormones, which suppress secretion of anterior pituitary hormones:
- 1. Growth hormone-inhibiting hormone (GHIH), also known as somatostatin, suppresses secretion of growth hormone.
2. Prolactin-inhibiting hormone (PIH), which is dopamine, suppresses secretion of prolactin.
Figure 1. Pituitary gland and hypothalamus
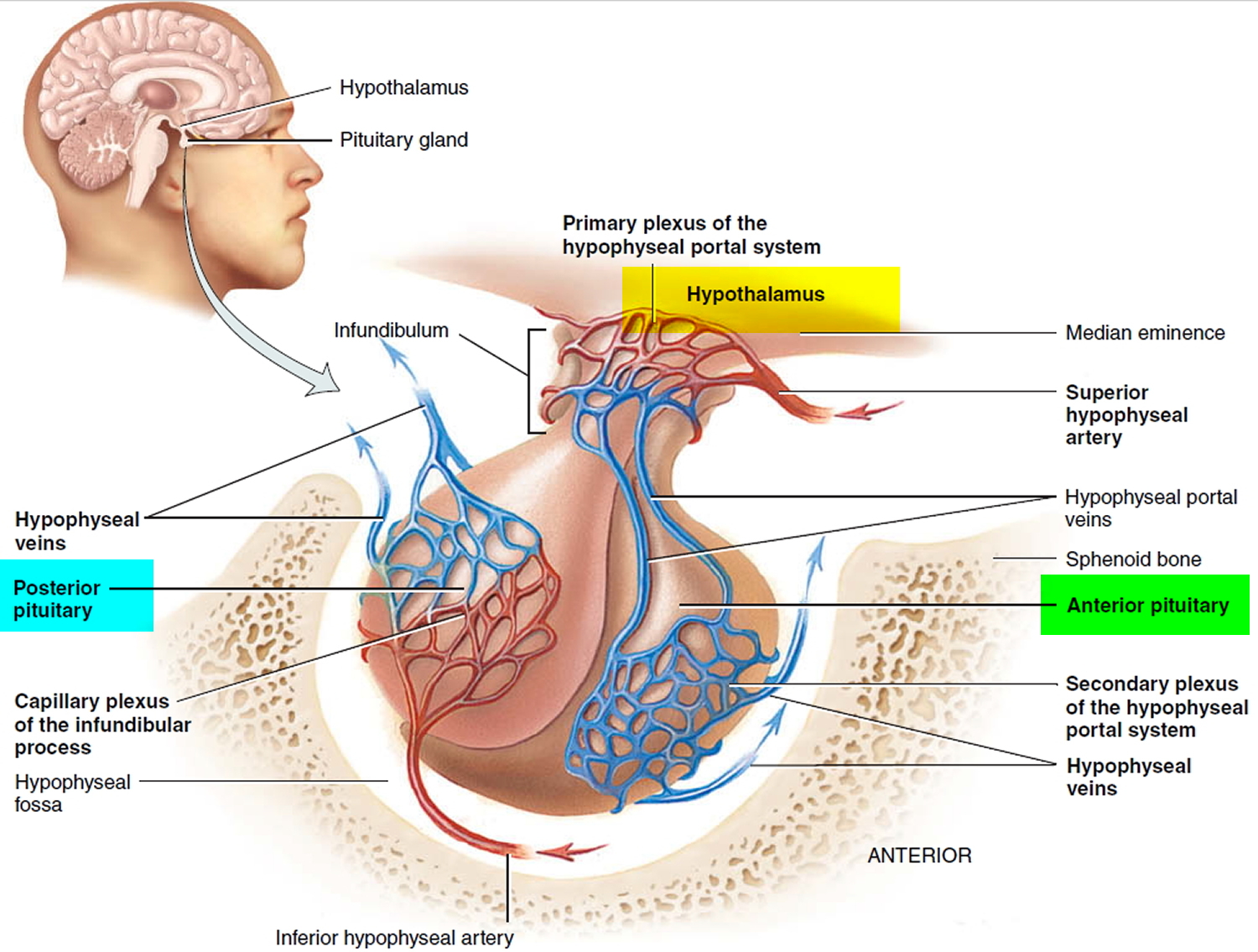
Figure 2. Hypothalamic Control of Pituitary Gland
Complications of acromegaly
If you do not get treatment, you may be at risk of developing:
- type 2 diabetes
- high blood pressure (hypertension)
- heart disease, particularly enlargement of the heart (cardiomyopathy)
- disease of the heart muscle (cardiomyopathy)
- osteoarthritis
- bowel polyps, which can potentially turn into bowel cancer if left untreated
- goiter
- precancerous growths (polyps) on the lining of your colon
- sleep apnea, a condition in which breathing repeatedly stops and starts during sleep
- Carpal tunnel syndrome
- reduced secretion of other pituitary hormones (hypopituitarism)
- uterine fibroids, benign tumors in the uterus
- spinal cord compression
- vision loss
Because of the risk of bowel polyps, a colonoscopy might be recommended for anyone diagnosed with acromegaly, and regular colonoscopy screening may be necessary.
Early treatment of acromegaly can prevent these complications from developing or becoming worse. If untreated, acromegaly and its complications can lead to premature death.
Acromegaly causes
In adults, a tumor is the most common cause of too much growth hormone production:
- Pituitary tumors. Most cases of acromegaly are caused by a noncancerous (benign) tumor (adenoma) of the pituitary gland. The tumor secretes excessive amounts of growth hormone, causing many of the signs and symptoms of acromegaly. Some of the symptoms of acromegaly, such as headaches and impaired vision, are due to the tumor mass pressing on nearby brain tissues.
- Nonpituitary tumors. In a few people with acromegaly, tumors in other parts of the body, such as the lungs, pancreas or adrenal glands, cause the disorder. Sometimes, these tumors actually secrete growth hormone. In other cases, the tumors produce a hormone called growth hormone-releasing hormone (GH-RH), which stimulates the pituitary gland to make more growth hormone.
Acromegaly happens because your pituitary gland (a pea-sized gland just below the brain) produces too much growth hormone.
This is usually caused by a non-cancerous tumor in the pituitary gland called an adenoma.
Most of the symptoms of acromegaly are due to the excess of growth hormone itself, but some come from the tumor pressing on nearby tissues. For example, you may get headaches and vision problems if a tumor pushes against the nearby nerves.
Acromegaly does sometimes run in families, but most of the time it’s not inherited. Adenomas usually spontaneously develop because of a genetic change in a cell of the pituitary gland. This change causes uncontrolled growth of the affected cells, creating the tumor.
In rare cases, acromegaly is caused by a tumor in another part of the body, such as the lungs, pancreas or another part of the brain. It may also be linked to some genetic conditions.
Acromegaly symptoms
Acromegaly can cause a wide range of symptoms, which tend to develop very slowly over time.
Early symptoms include:
- swollen hands and feet – you may notice a change in your ring or shoe size
- tiredness and difficulty sleeping, and sometimes sleep apnea (breathing repeatedly stops and starts during sleep)
- gradual changes in your facial features, such as your brow, lower jaw and nose getting larger, or your teeth becoming more widely spaced
- numbness and weakness in your hands, caused by a compressed nerve (Carpal tunnel syndrome)
- high blood glucose (sugar)
- coarse, oily, thickened skin
- excessive sweating and body odor
- small outgrowths of skin tissue (skin tags)
- fatigue and muscle weakness
- deepened, husky voice due to enlarged vocal cords and sinuses
- enlarged tongue
Children and teenagers will be abnormally tall.
As time goes on, common symptoms include:
- abnormally large hands and feet
- large, prominent facial features (such as the nose and lips) and an enlarged tongue
- skin changes – such as thick, coarse, oily skin; skin tags; or sweating too much
- deepening of the voice, as a result of enlarged sinuses and vocal cords
- joint pain
- tiredness and weakness
- headaches
- blurred or reduced vision
- loss of sex drive
- abnormal periods (in women) and erection problems (in men)
- heart failure or enlarged heart
- high blood pressure (hypertension)
- arthritis
- goiter (enlarged thyroid gland)
- enlarged liver, heart, kidneys, spleen and other organs
- increased chest size (barrel chest)
Symptoms often become more noticeable as you get older.
Symptoms saused by hypopituitarism:
- Menstrual disorders (irregular bleeding; absence of periods)
- Lower sexual desire
- Tiredness
Symptoms caused by tumor volume:
- Headaches
- Vision problems (tunnel vision; vision loss)
Diagnosing acromegaly
Because the symptoms of acromegaly often develop gradually over several years, you may not get a diagnosis straight away. Your doctor may ask you to bring in photographs of yourself that span the past few years to look for the tell-tale gradual changes.
Blood tests
If your doctor suspects you have acromegaly, you will need to have a blood test to measure your growth hormone levels.
To make sure the blood test gives an accurate result, you may be asked to drink a sugary solution before having a series of blood samples taken. For people without acromegaly, drinking the solution should stop growth hormone being released. In people with acromegaly, the level of growth hormone in the blood will remain high. This is called a glucose tolerance test.
Your doctor will also measure the level of another hormone, called insulin-like growth factor 1 (IGF-1). A higher level of IGF-1 is a very accurate indication that you might have acromegaly. High IGF-1 levels can mean that your levels of growth hormone are also high.
Another way to diagnose acromegaly is with an oral glucose tolerance test. In this test, growth hormone levels in the blood are measured after you drink sugar water. Normally, the sugar water will make the pituitary gland stop producing growth hormone and blood levels drop. However, a growth hormone-producing pituitary tumor will not stop making growth hormone, so the levels of growth hormone in the blood will not change.
Brain scans
If your blood tests show a high level of growth hormone and IGF-1, you might have an MRI scan of your brain. This will show where the adenoma is in your pituitary gland and how big it is. If you can’t have an MRI scan, a CT scan can be carried out, but this is less accurate.
Acromegaly treatment
Acromegaly requires expert care. Too much growth hormone and IGF-1 in the blood lower both your quality of life and how long you might live. The main goal of treatment is to lower growth hormone and IGF-1 levels to normal. Treatment may be surgery, pituitary irradiation (radiation therapy on the pituitary gland), medication, or a combination of these options.
The type of treatment offered for acromegaly depends on the symptoms you have. Usually the goal is to:
- reduce growth hormone production to normal levels
- relieve the pressure a tumour may be putting on surrounding tissues
- treat any hormone deficiencies
- improve your symptoms
Most people with acromegaly will have a pituitary tumor that needs to be surgically removed. Medication or radiotherapy may sometimes be needed after, or instead of, surgery.
Surgery
Surgery is effective in most people and can completely cure acromegaly. But sometimes the tumor is too large to be removed entirely, and you may need another operation or further treatment with medication or radiotherapy.
Under general anesthetic, the surgeon will make a small cut inside your nose or behind your upper lip to access the pituitary gland.
A long, thin, flexible tube with a light and video camera at one end, called an endoscope, is fed into the opening so your doctor can see the tumor. Surgical instruments are passed through the same opening and used to remove the tumor.
Removing the tumor should instantly lower your levels of growth hormone and relieve pressure on the surrounding tissue. Often, facial features start to return to normal and swelling improves within a few days.
Figure 3. Endoscopic transnasal transsphenoidal surgery
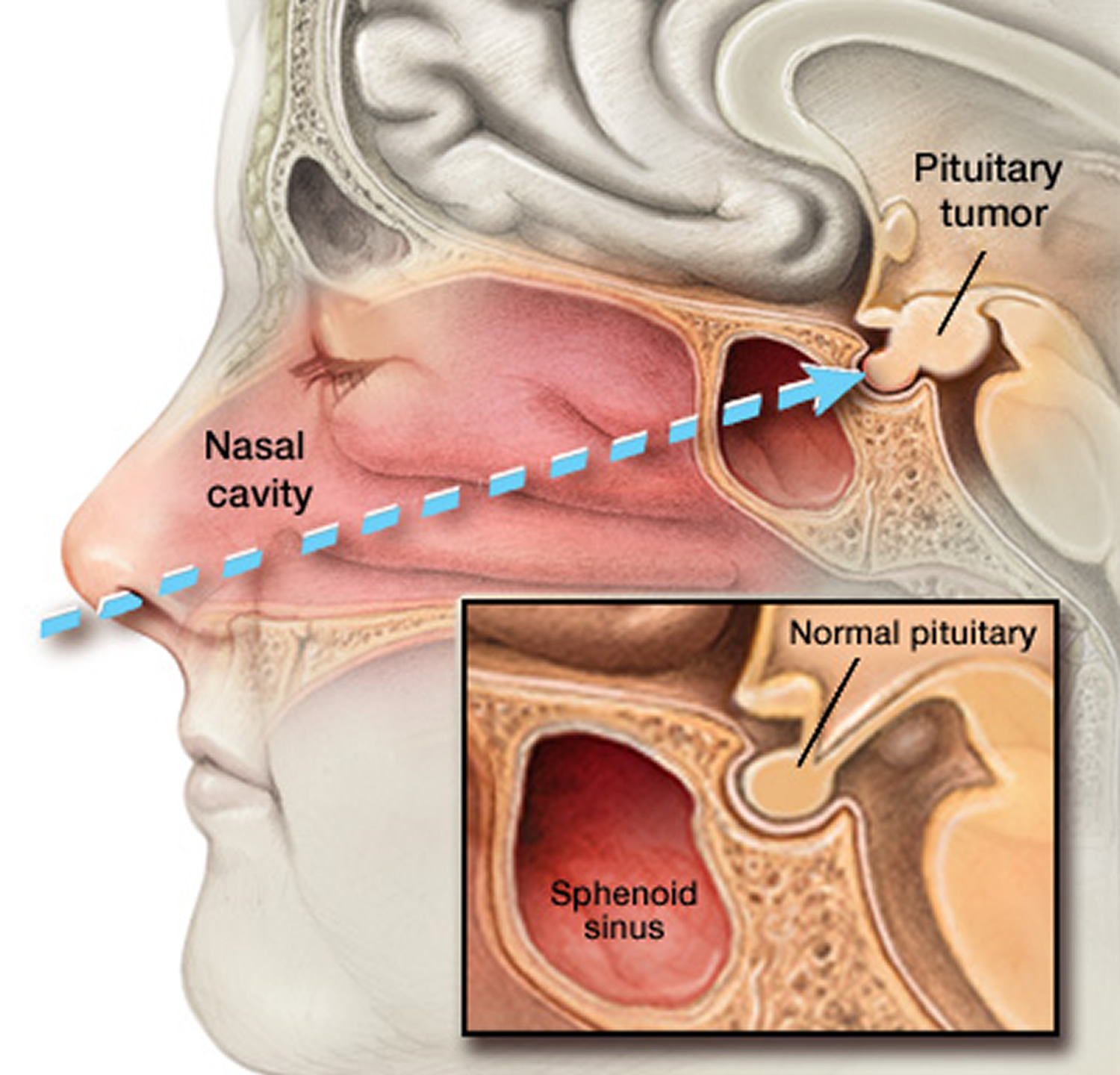
Note: In transnasal transsphenoidal endoscopic surgery, a surgical instrument is placed through the nostril and alongside the nasal septum to access a pituitary tumor.
With surgery, there is risk of:
- causing damage to healthy parts of your pituitary gland
- leakage of the fluid that surrounds and protects your brain
- meningitis – although this is rare
Your surgeon will discuss these risks with you and answer any questions you have.
Medication
If your levels of growth hormone are still higher than normal after surgery, or surgery wasn’t possible, you may be prescribed medication.
- Somatostatin analogues. The drugs octreotide (Sandostatin) and lanreotide (Somatuline Depot) are synthetic versions of the brain hormone somatostatin. They can interfere with the excessive secretion of GH by the pituitary gland, and thus can produce rapid declines in GH levels. When starting octreotide treatment, you initially inject yourself with a short-acting preparation under your skin (subcutaneously) three times a day to determine if you have any side effects from the medication and if it’s effective. Then, if it’s tolerated and effective, you can take a long-acting form that requires an injection into the muscles of your buttocks (gluteal muscles) by a health care professional, administered once a month. Lanreotide is administered as a subcutaneous injection once a month.
- Dopamine agonists. The medications cabergoline and bromocriptine (Parlodel) are taken as pills. In some people, these drugs can lower levels of GH and IGF-I. The tumor may decrease in size in some people taking a dopamine agonist or somatostatin analogues. Some people may develop compulsive behaviors, such as gambling, while taking these medications.
- Growth hormone antagonist. The medication pegvisomant (Somavert), a growth hormone antagonist, acts to block the effect of GH on body tissues. Pegvisomant may be particularly helpful for people who haven’t had good success with other forms of treatment. You administer this medication yourself daily by subcutaneous injection. This medication can normalize IGF-I levels and relieve symptoms in most people with acromegaly, but doesn’t lower GH levels or reduce the tumor size.
Three different types of medicine are used:
- A monthly injection of either octreotide, lanreotide or pasireotide: this slows down the release of growth hormone and can sometimes also shrink tumours.
- A daily pegvisomant injection: this blocks the effects of growth hormone and can significantly improve symptoms.
- Bromocriptine or cabergoline tablets: these can stop growth hormone being produced, but they only work in a small proportion of people.
Each of these medications has different advantages and disadvantages. Speak to your doctor about the options available to you, and the benefits and risks of each.
Radiotherapy
If surgery isn’t possible, not all of the tumor could be removed or medication hasn’t worked, then you may be offered radiotherapy.
This can eventually reduce your growth hormone levels, but it may not have a noticeable effect for several years and you may need to take medication in the meantime.
Three main types of radiotherapy are used to treat acromegaly:
- Stereotactic radiotherapy: Also known as Gamma Knife radiosurgery, stereotactic radiosurgery can deliver a high dose of radiation to the tumor cells in a single dose while limiting the amount of radiation to the normal surrounding tissues. A high-dose beam of radiation aimed very precisely at your adenoma. You will need to wear a rigid head frame or a plastic mask to hold your head still during the treatment. This can usually be done in one session. This type of radiation may bring growth hormone levels back to normal within three to five years.
- Conventional radiotherapy: this also uses a beam of radiation to target the adenoma, but it is wider and less precise than the one used in stereotactic radiotherapy. This means this treatment can damage your surrounding pituitary gland and brain tissue, so it’s given in small doses over four to six weeks to give your tissues time to heal between treatments. You may not realize the full effect of conventional radiation therapy for 10 or more years after treatment.
- Proton beam therapy. Proton beam therapy delivers a targeted, high dose of radiation to the tumor, sparing radiation exposure to normal tissues. Proton beam therapy is provided in fractions over time, but treatment times are generally less than conventional radiation.
Stereotactic radiotherapy is more commonly used to treat adenomas because it minimises the risk of damage to nearby healthy tissue.
However, stereotactic radiosurgery is available at only a few U.S. medical centers and is not recommended for all people undergoing radiation for acromegaly. Your doctor will determine which type of radiation therapy is right for you based on:
- The size and location of your remaining tumor cells
- Your levels of insulin-like growth factor-I (IGF-I)
Even after initial treatment, acromegaly requires periodic monitoring by your doctor to make sure that your pituitary gland is functioning properly. This follow-up care may last for the rest of your life.
Radiotherapy can have a number of side effects. It will often cause a gradual drop in the levels of other hormones produced by your pituitary gland, so you’ll usually need hormone replacement therapy for the rest of your life. It may also have an effect on your fertility.
Your doctor will be able to talk to you about these risks and other possible side effects.
Follow-up
Treatment is often effective at stopping the excessive production of growth hormone and improving the symptoms of acromegaly.
After treatment, you’ll need regular follow-up appointments with your specialist for the rest of your life. These will be used to monitor how well your pituitary gland is working, check you’re on the correct hormone replacement treatment and make sure the condition does not return.





{kind=link}