Contents
What is acromioclavicular joint
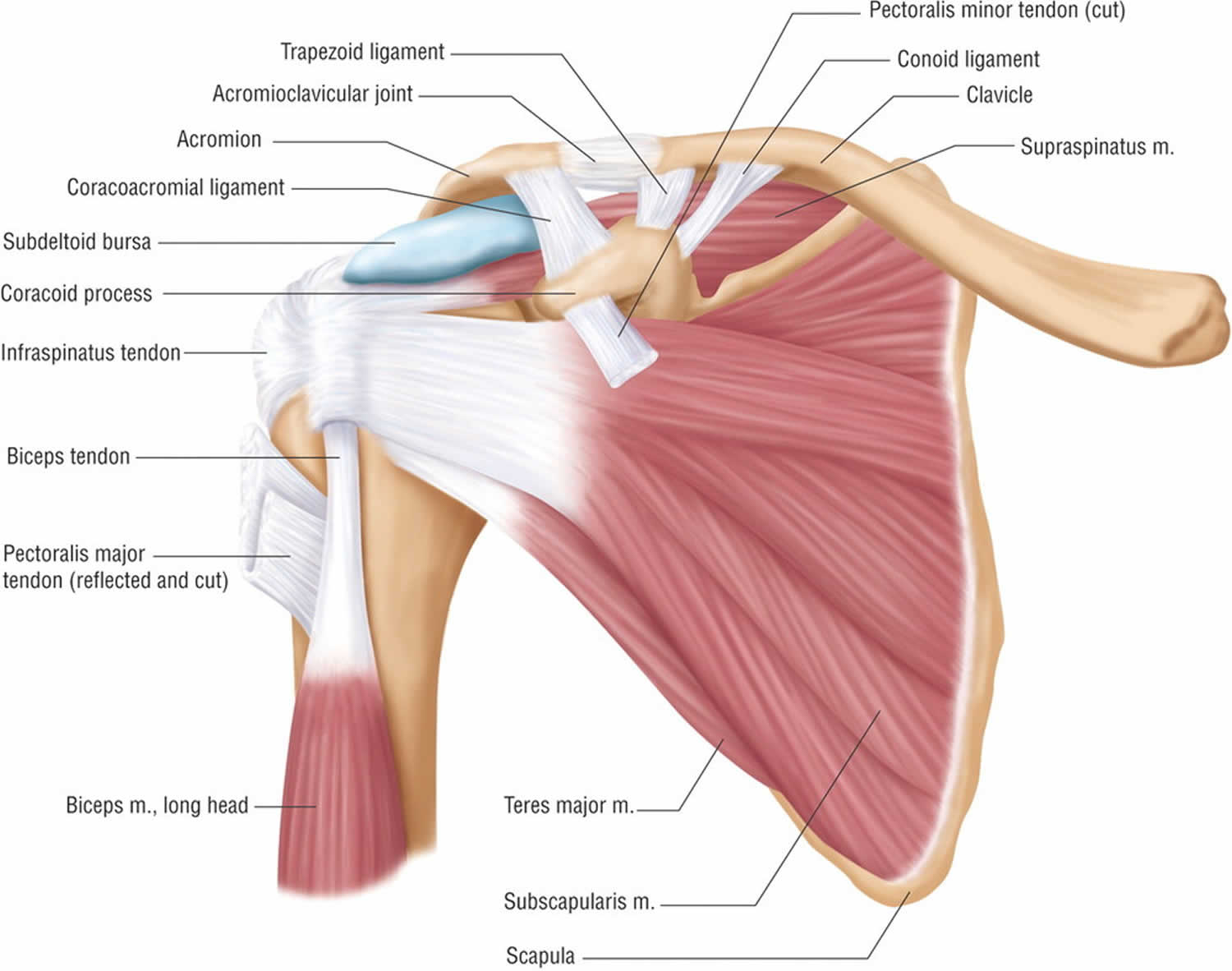
The acromioclavicular joint is a diarthrodial joint where the collarbone (clavicle) meets the highest point of the shoulder blade or scapula (acromion) 1. There is very little motion at the acromioclavicular joint. Rather, it is a strong junction between these two bones held together by very strong ligaments. Acromioclavicular joint can develop painful arthritis that is often associated with rotator cuff disease.
The acromioclavicular joint is surrounded by a capsule and lined by a synovial membrane. In between the osseous portions lies an intra-articular cartilaginous disk. Lastly, the articulating surfaces are lined with fibrocartilage, as opposed to hyaline cartilage.
Three main ligaments stabilize the acromioclavicular joint. The acromioclavicular ligament (acromioclavicular) has both superior, inferior, anterior, and posterior components. The superior and posterior ligaments are the strongest, and it mainly serves to provide horizontal stability. The coracoclavicular ligaments complex consists of the conoid and trapezoid ligaments. They insert on the posteromedial and anterolateral region of the undersurface of the distal clavicle, respectively. It mainly serves to provide vertical stability. The coracoacromial ligament is a strong triangular band that connects the coracoid process to the acromion and also provides vertical stability 2.
Figure 1. Acromioclavicular joint
Acromioclavicular joint injury
Injuries to the acromioclavicular joint are common. They can present as sprains or dislocations. However, sprains are more common. The most common etiology is direct trauma to the acromioclavicular joint or lateral trauma providing an axial load on the joint space. This can occur from motor vehicle accidents, sports or accidental trauma. Falling on the outstretched hand or elbow can also cause acromioclavicular joint injuries. acromioclavicular joint injuries account for over 40% of all shoulder injuries. Note that acromioclavicular dislocations are different from “shoulder dislocation,” which refers to the dislocation of the glenohumeral joint 3.
Patients will generally present reporting pain over the acromioclavicular joint and a mechanism consistent with that injury. They will describe pain over the joint, possibly radiating to the shoulder or neck and made worse with movement or use of the arm. On exam, the provider may observe swelling, bruising, or deformity. There may be tenderness to palpation over the area. There may be limited active or passive range of motion of the shoulder or neck. The examiner should assess for anterior-posterior or superior-inferior mobility and laxity. In dislocations, the deformities may be obvious. It is important to evaluate the entire clavicle and shoulder for additional injuries in addition to performing a full neurovascular examination.
A special test may assist in the evaluation of a suspected acromioclavicular joint injury. Pain with any of these test may suggest acromioclavicular pathology. The adduction or cross-arm test has the patient either actively or passively adduct their arm across the body in the axial plane. Pain at the acromioclavicular joint is a positive test, and it has the greatest sensitivity for acromioclavicular joint pathology. In performing the shear test, the examiner applies an external force to the acromioclavicular joint by simultaneously pushing the scapula from a posterior direction and the clavicle from an anterior direction. In the one-handed shear test, also known as Paxinos test, the examiners place their thumb on the posterior acromion and fingers on the mid-clavicle. The examiner then tries to squeeze the thumb and fingers together.
Radiographic evaluation of the acromioclavicular joint is standard for suspected acromioclavicular-joint injury or undifferentiated shoulder pain in the setting of trauma. Standard AP, lateral, and axillary radiographs should be obtained. If the diagnosis is uncertain, the Zanca view is the most accurate view for examining the acromioclavicular joint. This is an antero-posterior view with the beam directed at the acromioclavicular joint with 10 degrees of cephalic tilt. In grade 1 acromioclavicular joint sprain, which is most common, radiographs will be normal. Disruption of the joint will be seen in grade 2 through 6. If there is continued uncertainty, ultrasound or MRI may be utilized to provide additional diagnostic information.
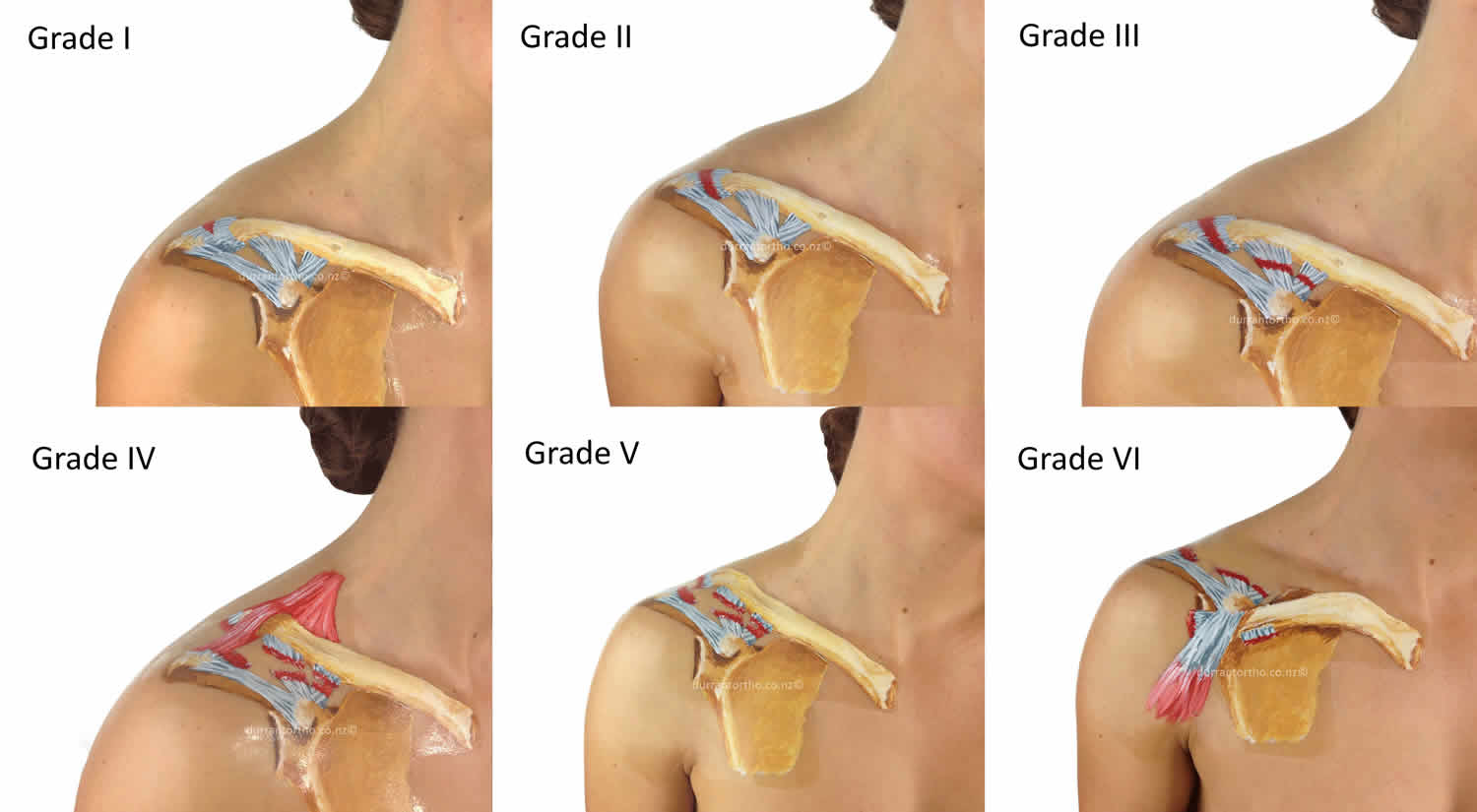
Acromioclavicular joint injuries follow a Rockwood classification system of type I to type VI 4 (see Figure 2 below):
- Type I – Trauma to the joint ligaments but no severe tearing or fracture. It is commonly referred to as a sprain (acromioclavicular ligament sprain; coracoclavicular ligament intact; no radiographic abnormalities). Most doctors treat this type of injury with anti-inflammatory drugs, pain medication and the placement of the arm in a sling or an immobilizer.
- Type II – Complete tearing of the acromioclavicular ligament, as well as a sprain or partial tear of the coracoclavicular ligaments. Clavicle elevated but not superior to the border of the acromion or there is a less than 25% increase in the coracoclavicular interspace. This often causes a noticeable bump on the shoulder which is permanent. Severe pain and loss of movement are common. Treatment is typically an arm sling, bed rest, ice and heat therapy, and anti-inflammatory drugs. Most people recover full motion of the shoulder and arm within 6 to 8 weeks, often with the assistance of physiotherapy.
- Type III – Both acromioclavicular and coracoclavicular ligaments are torn. Clavicle is elevated above the border of the acromion or there is a 25% to 100% increase in the coracoclavicular interspace. A significant bump, resulting in some shoulder deformity, is formed by the end of the clavicle. This bump, caused by the clavicle’s dislocation, is permanent. The clavicle can be moved in and out of place on the shoulder. It may take as long as 12 weeks for the injury to heal and in some cases even longer for shoulder strength and range of motion to feel normal. Physiotherapy can be beneficial.
- Type IV – Acromioclavicular and coracoclavicular ligaments are torn; posterior displacement of the distal clavicle into the trapezius. An unusual injury where the clavicle is pushed behind the acromioclavicular joint.
- Type V – Acromioclavicular and coracoclavicular ligaments are torn; superior displacement of the distal clavicle by more than 25 mm. An exaggerated Type III injury in which the muscle above the acromioclavicular joint is punctured by the end of the clavicle causing a significant bump over the injury.
- Type VI – Exceedingly rare. Acromioclavicular and coracoclavicular ligaments are torn; inferolateral displacement in a subacromial or subcoracoid displacement behind the coracobrachialis or biceps tendon. The clavicle is pushed downwards, and becomes lodged below the corocoid (part of the scapula).
The prognosis of acromioclavicular joints dislocations is generally favorable. Grade I and II sprains are self-limited and are managed with conservative therapy including a brief period of rest, sling, ice, anti-inflammatory medications, physical therapy, and a graded return to activity. Treatment for grade III dislocations is controversial and is determined based on the occupation of the patient, their goals, and the consulting orthopedic surgeon. Grade IV to VI are rare, but require surgical correction due to the risk of comorbid injuries. Surgically managed injuries have a longer recovery and higher risk of complications.
The most common complications from acromioclavicular joint injuries is residual pain, affecting 30% to 50% of individuals. Primary or secondary osteoarthritis are commonly seen in the acromioclavicular joint. Incidence of acromioclavicular joint osteoarthritis increases with age. It can be through overuse, chronic degeneration, or through prior trauma (secondary osteoarthritis). This leads to narrowing of the articular disc and degeneration of the cartilage. Osteoarthritis may lead to osteophytic lesions and subacromial impingement and compression of nearby structures 5.
Acromioclavicular joint separation
The most common cause for acromioclavicular joint separation is from a fall directly onto your shoulder. The fall injures the ligaments that surround and stabilize the acromioclavicular joint (see Figure 1 above).
If the force is severe enough, the ligaments attaching to the underside of the clavicle are torn. This causes the separation of the collarbone and the shoulder blade (scapula). The shoulder blade (scapula) actually moves downward from the weight of the arm. This creates a bump or bulge above the shoulder.
The acromioclavicular joint separation injury can range from a mild sprain without a bump to a complete disruption with a very large bump. Good pain-free function often returns even with a very large bump. The greater the deformity, the longer it takes for pain-free function to return.
- A mild acromioclavicular joint separation involves a sprain of the acromioclavicular ligament that does not move the collarbone and looks normal on X-rays.
- A more serious injury tears the acromioclavicular ligament and sprains or slightly tears the coracoclavicular ligament, putting the collarbone out of alignment to some extent with a smaller bump.
- The most severe shoulder separation completely tears both the acromioclavicular and coracoclavicular ligaments and puts the acromioclavicular joint noticeably out of position, with a larger bump.
Acromioclavicular joint injuries follow a Rockwood classification system of type I to type VI 4. Acromioclavicular joint separation are graded according to the severity of the injury and the position of the displaced bones and are graded from Type I to VI 6:
- Type I – Trauma to the joint ligaments but no severe tearing or fracture. It is commonly referred to as a sprain (acromioclavicular ligament sprain; coracoclavicular ligament intact; no radiographic abnormalities). Most doctors treat this type of injury with anti-inflammatory drugs, pain medication and the placement of the arm in a sling or an immobilizer.
- Type II – Complete tearing of the acromioclavicular ligament, as well as a sprain or partial tear of the coracoclavicular ligaments. Clavicle elevated but not superior to the border of the acromion or there is a less than 25% increase in the coracoclavicular interspace. This often causes a noticeable bump on the shoulder which is permanent. Severe pain and loss of movement are common. Treatment is typically an arm sling, bed rest, ice and heat therapy, and anti-inflammatory drugs. Most people recover full motion of the shoulder and arm within 6 to 8 weeks, often with the assistance of physiotherapy.
- Type III – Both acromioclavicular and coracoclavicular ligaments are torn. Clavicle is elevated above the border of the acromion or there is a 25% to 100% increase in the coracoclavicular interspace. A significant bump, resulting in some shoulder deformity, is formed by the end of the clavicle. This bump, caused by the clavicle’s dislocation, is permanent. The clavicle can be moved in and out of place on the shoulder. It may take as long as 12 weeks for the injury to heal and in some cases even longer for shoulder strength and range of motion to feel normal. Physiotherapy can be beneficial.
- Type IV – Acromioclavicular and coracoclavicular ligaments are torn; posterior displacement of the distal clavicle into the trapezius. An unusual injury where the clavicle is pushed behind the acromioclavicular joint.
- Type V – Acromioclavicular and coracoclavicular ligaments are torn; superior displacement of the distal clavicle by more than 25 mm. An exaggerated Type III injury in which the muscle above the acromioclavicular joint is punctured by the end of the clavicle causing a significant bump over the injury.
- Type VI – Exceedingly rare. Acromioclavicular and coracoclavicular ligaments are torn; inferolateral displacement in a subacromial or subcoracoid displacement behind the coracobrachialis or biceps tendon. The clavicle is pushed downwards, and becomes lodged below the corocoid (part of the scapula).
The acromioclavicular joint separation injury is easy to identify when it causes deformity. When there is less deformity, the location of pain and x-rays help the doctor make the diagnosis. Sometimes having the patient hold a weight in the hand can increase the deformity, which makes the acromioclavicular joint separation injury more obvious on x-rays.
The prognosis for acromioclavicular joint injuries is generally favorable. Most injuries are non-operative, and individuals typically regain functional motion by 6 weeks and return to normal activity by 12 weeks. Surgically managed injuries have a longer recovery time including immobilization for 6 weeks and a gradual return to full activity around 6 months 7.
Figure 2. Acromioclavicular joint separation
Is a acromioclavicular joint separation the same as a shoulder dislocation?
No. These two injuries are commonly confused, but they are very different conditions. The shoulder joint is located at the junction of three different bones: the clavicle, the scapula, and the humerus. In a acromioclavicular joint separation, the junction of the clavicle and scapula is disrupted. In a shoulder dislocation, the humerus (arm bone) is displaced from the socket. Not only are the injuries different in anatomical terms, but the implications for treatment, recovery, and complications are also different.
Acromioclavicular joint separation treatment
Nonsurgical treatment
Nonsurgical treatments for acromioclavicular joint separation, such as a sling, cold packs, and medications can often help manage the pain. Rarely, a doctor may use more complicated supports to help lessen acromioclavicular joint motion and pain.
- Icing the Injury – The inflammation from a separated shoulder can be controlled with ice placed on the joint every four hours for a period of 15 minutes. Icing can be done for the first several days until the swelling around the joint has subsided.
- Rest – In the acute stage, together with a protective sling and ice, rest can help to reduce the pain and swelling. Resting the joint will help minimize painful symptoms and allow healing to begin.
- Physiotherapy – A rehabilitation program will aim to restore the normal motion and strength to the shoulder. This will begin as soon as tolerated. Returning to sporting activities can occur within 2 to 12 weeks depending on the grade of separation.
- Anti-inflammatory Medications – These medications may assist with the reduction of swelling and pain within the affected shoulder.
Most people return to near full function with this injury, even if there is a persistent, significant deformity/bump. Some people have continued pain in the area of the acromioclavicular joint, even with only a mild deformity. This may be due to:
- Abnormal contact between the bone ends when the joint is in motion
- Development of acromioclavicular joint arthritis
- Injury to a disk-like piece of cushioning cartilage that is often found between the bone ends of this joint
It is often worthwhile to wait and see if reasonable function returns without surgical treatment. Most patients, even with very severe acromioclavicular joint injuries, are often managed effectively without surgery.
Surgical treatment
Surgery can be considered if acromioclavicular joint pain persists or the deformity is severe. A surgeon might recommend trimming back the end of the collarbone (clavicle) so that it does not rub against the shoulder blade bone (acromion).
Where there is significant deformity, reconstructing the ligaments that attach to the underside of the collarbone is helpful. This type of surgery works well even if it is done long after the problem started. These operations can be done arthroscopically or open, with a plate or without. Sometimes, if a plate is used to assist with the surgery, it is usually removed after healing of the shoulder separation.
Whether treated conservatively or with surgery, the shoulder will require rehabilitation to restore and rebuild motion, strength, and flexibility.
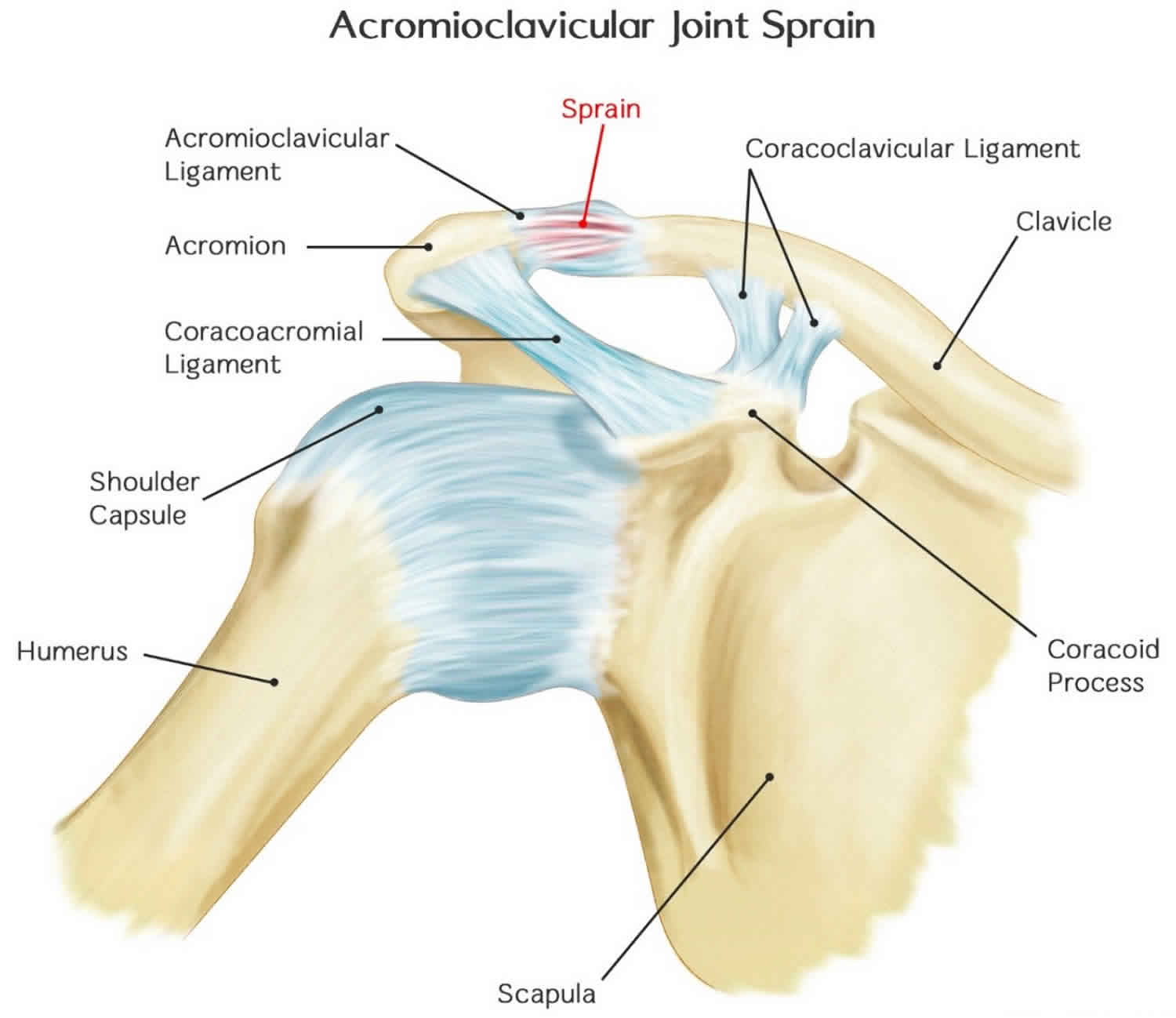
Acromioclavicular joint sprain
Acromioclavicular joint sprain is injury to the ligaments which hold the acromioclavicular joint together at the top of the shoulder.
At first, treatment of both acromioclavicular joint sprains and strains usually involves resting the injured area, icing it, wearing a bandage or device that compresses the area, and medicines. Later treatment might include exercise and physical therapy.
Figure 3. Acromioclavicular joint sprain
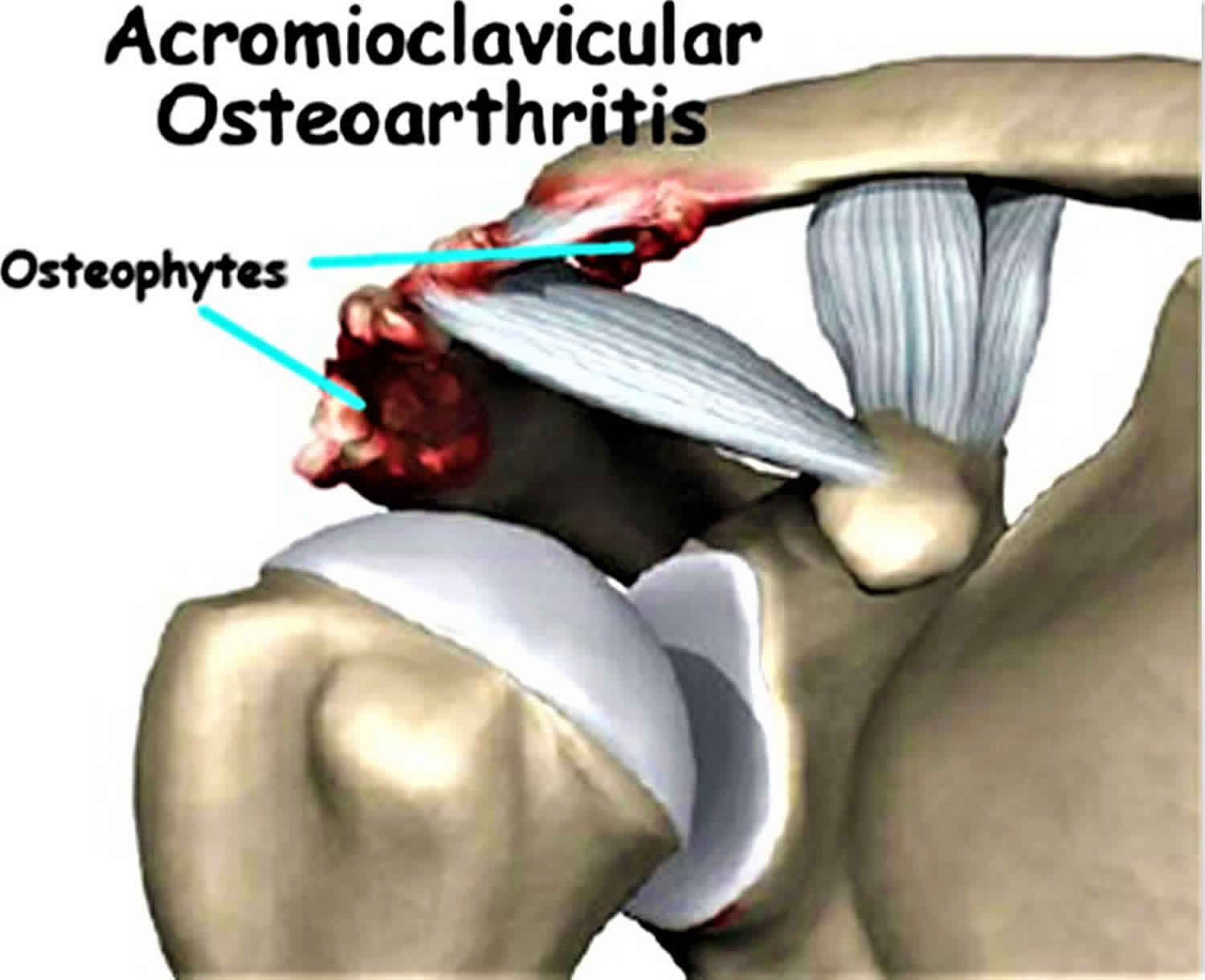
Acromioclavicular joint osteoarthritis
Acromioclavicular joint osteoarthritis is one of the most common causes of shoulder pain originating from the acromioclavicular joint 8. Acromioclavicular joint osteoarthritis is a frequent finding in patients older than 50 years of age 9. A study demonstrated 54–57% of elderly patients have radiographic evidence of degenerative arthritis of the acromioclavicular joint 10. Evaluation of MRIs among asymptomatic subjects demonstrated the prevalence of acromioclavicular joint osteoarthritis to be between 48% and 82% 11. Non-steroidal anti-inflammatory drugs (NSAIDS) and corticosteroid injections have shown to improve pain and function temporarily, causing patients to seek surgical treatment 8. One study found injection provided on an average 20 days of pain relief, with 18 of the 27 patients (67%) seeking surgical treatment following injections 12. A variety of surgical treatments exist, ranging from open distal clavicle resection to direct and indirect arthroscopic surgical resection.
Figure 4. Acromioclavicular joint osteoarthritis
Acromioclavicular joint osteoarthritis treatment
Non-surgical treatments
Initial treatment of acromioclavicular joint arthritis is non-operative and includes activity modification, physical therapy, non-steriodal anti-inflammatory medications (NSAIDs), and local acromioclavicular joint injection of anesthetics or corticosteroids 13. Activity modification includes avoidance of repetitive motions causing the pain, such as push-ups, dips, flies, and bench press exercises 14. Physical therapy would include exercises to maintain active range of motion and increase muscle strength for scapular stabilization 13. However, physical therapy is not as effective for acromioclavicular joint arthritis as it is for rotator cuff disease 15.
Corticosteroid injection into the acromioclavicular joint is warranted following previous failed trials of NSAIDs and activity modification, and also if a diagnostic local anesthetic injection provides relief. The acromioclavicular joint can be located by first palpating the soft spot where the clavicle and spine of the scapula meet and then moving slightly anterior 15. The skin is anesthetized and the needle is inserted into the joint-space using a superior approach and moved inferiorly until a decrease in resistance is felt as the needle enters the capsule [14]. Injections of 0.25–0.5 mL of betamethasone sodium phosphate and acetate or 0.25–0.5 mL methylprednisolone, 40 mg/mL are recommended 14. Limits of two to four injections per year with a total of twenty 14 are recommended, as excessive corticosteroid administration may cause subcutaneous fat atrophy and dermal thinning 16.
In some cases the pain relief afforded by corticosteroid injection may be short in duration. Jacob and Sallay 17 followed 31 patients diagnosed with acromioclavicular joint arthropathy and concluded acromioclavicular joint corticosteroid injection offered short-term pain relief but did not alter natural disease progression. The 31 patients received 1 mL of Celestone/Soluspan or dexamethasone and 2 mL of lidocaine injections. Of the 31 patients four were excluded from the study as they were lost to follow-up. The mean duration of improvement was 20 days, as reported by patients, with a range of 2 h to 3 months. Of the 27 patients 18 underwent distal clavicle resection at an average of 4 months postinjection. Only five of the remaining nine patients were considered to have had long-term therapeutic benefit from the injections. Of the 31 patients with acromioclavicular joint arthropathy who received corticosteroid injection, 93% reported improvement in pain and function, 81% failed to obtain long-term results, and 67% underwent distal clavicle resection. Though osteoarthritis is considered a non-inflammatory process, recent evidence demonstrates a likely inflammatory component 14 which suggests corticosteroids should play a role in treatment.
Surgical treatments
Surgical treatment options become apparent once all non-invasive treatment modalities have failed to provide adequate pain relief and persistent symptoms continue to interfere with activities of daily living 13. At least 6 months of conservative treatment should be attempted before surgery 14. Variables such as patient occupation, age, degree of activity limitation, shoulder dominance, and patient goals should be considered by both patient and physician before a decision concerning surgical treatment is made 18.
Distal clavicle excision, which prevents abutment of the distal clavicle against the medial acromion 19, is the mainstay of surgical treatment for acromioclavicular joint arthritis 13. Various surgical techniques, such as an open approach or direct and indirect arthroscopic approaches, are available. The open technique frequently utilizes a 3- to 5-cm transverse or perpendicular saber skin incision with division of the deltotrapezial fascia. An oscillating saw is used to excise a 1- to 2-cm portion of the distal clavicle 13.
- Wong M, Kiel J. Anatomy, Shoulder and Upper Limb, Acromioclavicular Joint. [Updated 2018 Dec 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499858[↩]
- Gottschalk HP, Browne RH, Starr AJ. Shoulder girdle: patterns of trauma and associated injuries. J Orthop Trauma. 2011 May;25(5):266-71[↩]
- Wurm M, Beirer M, Biberthaler P, Kirchhoff C. [Clavicular fractures : Diagnostics, management and treatment]. Unfallchirurg. 2018 Dec;121(12):983-998[↩]
- Kiel J, Kaiser K. Acromioclavicular Joint Injury. [Updated 2018 Dec 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK493188[↩][↩]
- Doyscher R, Kraus K, Finke B, Scheibel M. [Acute and overuse injuries of the shoulder in sports]. Orthopade. 2014 Mar;43(3):202-8[↩]
- Granville-Chapman J, Torrance E, Rashid A, Funk L. The Rockwood classification in acute acromioclavicular joint injury does not correlate with symptoms. J Orthop Surg (Hong Kong). 2018 May-Aug;26(2):2309499018777886[↩]
- Stein T, Müller D, Blank M, Reinig Y, Saier T, Hoffmann R, Welsch F, Schweigkofler U. Stabilization of Acute High-Grade Acromioclavicular Joint Separation: A Prospective Assessment of the Clavicular Hook Plate Versus the Double Double-Button Suture Procedure. Am J Sports Med. 2018 Sep;46(11):2725-2734[↩]
- Docimo S, Kornitsky D, Futterman B, Elkowitz DE. Surgical treatment for acromioclavicular joint osteoarthritis: patient selection, surgical options, complications, and outcome. Curr Rev Musculoskelet Med. 2008;1(2):154–160. doi:10.1007/s12178-008-9024-5 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2684214/[↩][↩]
- Petersson CJ. Degeneration of the acromioclavicular joint: a morphological study. Acta Orthop Scand. 1983;54:434–8.[↩]
- Horvath F, Kery L. Degenerative deformations of the acromioclavicular joint in the elderly. Arch Gerontol Geriatr. 1984;3:259–65. doi: 10.1016/0167-4943(84)90027-X[↩]
- Stein BE, Wiater JM, Pfaff HC, Bigliani LU, Levine WN. Detection of acriomioclavicular joint pathology in asymptomatic shoulders with magnetic resonance imaging. J Shoulder Elbow Surg. 2001;10:204–8. doi: 10.1067/mse.2001.113498[↩]
- Jacob AK, Sallay PI. Therapeutic efficacy of corticosteroid injections in the acromioclavicular joint. Biomed Sci Instrum. 1997;34:380–5.[↩]
- Rabalais RD, McCarty E. Surgical treatment of symptomatic acromioclavicular joint problems. Clin Orthop Relat Res. 2006;455:30–7. doi: 10.1097/BLO.0b013e31802f5450[↩][↩][↩][↩][↩]
- Buttaci CJ, Stitik TP, Yonclas PP, Foye PM. Osteoarthritis of the acromioclavicular joint: a review of anatomy, biomechanics, diagnosis, and treatment. Am J Phys Med Rehabil. 2004;83(10):791–7. doi: 10.1097/01.PHM.0000140804.46346.93[↩][↩][↩][↩][↩]
- Codsi MJ (2007) The painful shoulder: when to inject and when to refer. 74(7):473–4, 477–8, 480–2, 485–8.[↩][↩]
- Lemos MJ, Tolo ET. Complications of the treatment of the acromioclavicular and sternoclavicular joint injuries, including instability. Clin Sports Med. 2003;22:371–85. doi: 10.1016/S0278-5919(02)00102-3[↩]
- Jacob AK, Sallay PI. Therapeutic efficacy of corticosteroid injections in the acromioclavicular joint. Biomed Sci Instrum. 1997;34:380–5[↩]
- Shaffer BS. Painful conditions of the acromioclavicular joint. J Am Acad Orthop Surg. 1999;7:176–88[↩]
- Nuber GW, Bowen MK. Arthroscopic treatment of acromioclavicular joint injuries and results. Clin Sports Med. 2003;22:301–17. doi: 10.1016/S0278-5919(03)00014-0[↩]





{kind=link}