
Contents
- What is acupuncture
- How does acupuncture work
- Who Provides Acupuncture Treatments ?
- Acupuncture therapy
- Acupuncture benefits
- Stroke Rehabilitation
- Period Pain
- Peripheral Joint Osteoarthritis
- Rheumatoid arthritis
- Fibromyalgia
- Neuropathic pain in adults
- Cancer pain in adults
- Shoulder pain
- Lateral elbow pain
- Low-Back Pain
- Neck Pain
- Headache
- Episodic migraine
- Attention Deficit Hyperactivity Disorder (ADHD) in children and adolescents
- Autism spectrum disorders (ASD)
- Induction of labour
- Pain management in labour
- Glaucoma
- Slowing the progression of myopia in children and adolescents
- Depression
- Epilepsy
- Acute hordeolum (Stye infection)
- Bell’s palsy
- Insomnia
- Restless legs syndrome
- Cocaine dependence
- Smoking cessation
- Uterine fibroids
- Endometriosis
- Polycystic ovarian syndrome
- Menopausal hot flushes
- Functional dyspepsia
- Irritable bowel syndrome
- Stress urinary incontinence in adults
- Schizophrenia
- Vascular dementia
- Acupuncture side effects
What is acupuncture
Acupuncture is a technique of insertion and manipulation of fine needles in specific points on the body to achieve therapeutic purposes 1. The acupuncture technique that has been most often studied scientifically involves penetrating the skin with thin, solid, metallic needles that are manipulated by the hands or by electrical stimulation.
Acupuncture has been practiced widely in China for more than 4000 years and is an integral part of traditional Chinese medicine. It was first described in the medical writings The Yellow Emperor’s Classic of Internal Medicine1 around 200 BC. As early as 5000 years ago, stones were sculpted and formed into crude needles to be used as medical instruments 2. In time, other materials, including bamboo, fish bones, bronze, gold, and silver, have been refined into acupuncture needles.
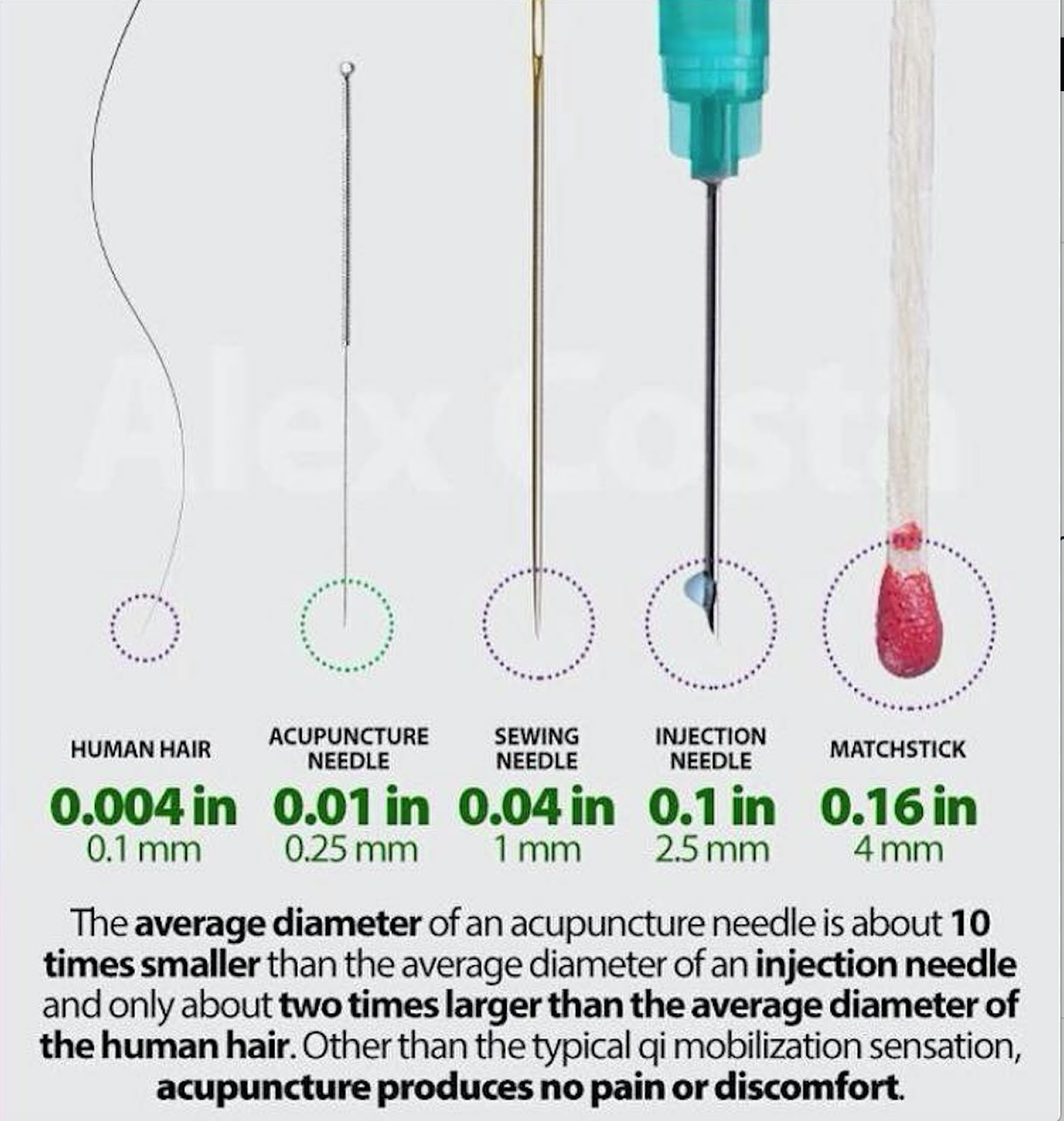
Modern acupuncture needles are thin and flexible and are made of solid surgical stainless steel. Unlike hypodermic needles, acupuncture needles are finely tapered, allowing them to slide smoothly into the skin (see Figure 1). Certain acupuncture needles are thinner than the average strand of human hair.
Figure 1. Comparison of acupuncture needles with a 20-gauge hypodermic needle. Matchstick shown for indication of needle sizes
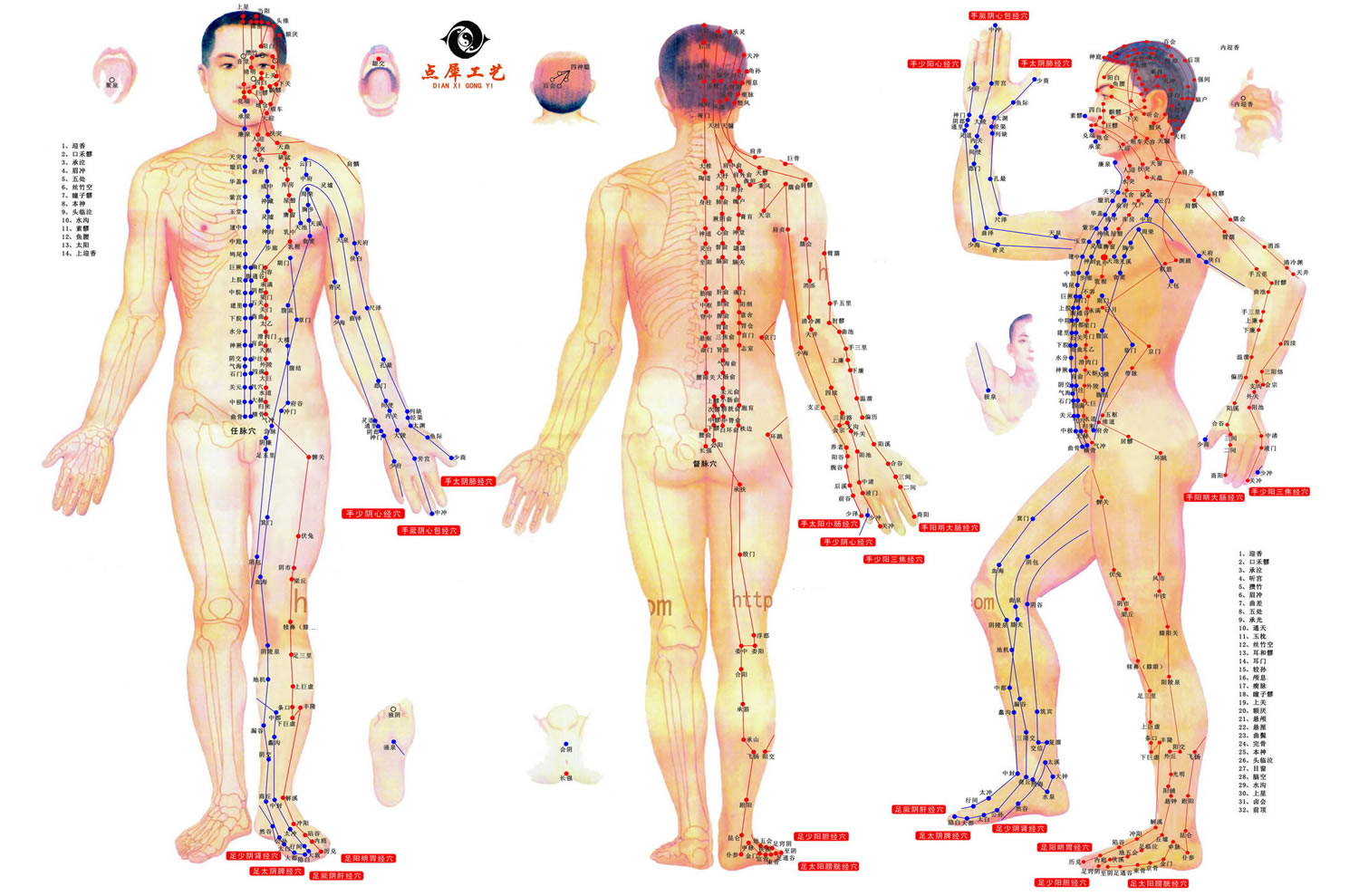
Acupuncture is based on the idea that living beings have an inner energy, known as Qi (pronounced chee), and it is the flow of this inner energy that sustains them. According to traditional Chinese medical philosophy, balanced Qi is vital to optimal health; illness and disease are caused by the imbalance or interruption in the flow of Qi. Although acupuncture was developed for prevention of illness, it is useful in managing disease symptoms by reintroducing balanced flow of Qi, its main focus. According to the philosophy of traditional acupuncture, energy circulates in ‘meridians’ located throughout the body. Pain or ill health happens when something occurs to cause this meridian energy circulation to be blocked. The way to restore health is to stimulate the appropriate combination of acupuncture points in the body by inserting very thin needles. Sometimes in painful conditions, electrical stimulation along with the needles is also used. According to acupuncture theory, one way you can tell that acupuncture is relieving pain is that you may feel numbness or tingling, called De Qi, where the needle is inserted.
Jesuit missionaries introduced acupuncture to Europe in the 17th century, when they returned from China. The Jesuits were active in disseminating the idea and practice of acupuncture throughout Europe. In addition, traveling physicians helped pioneer acupuncture use in Europe 3.
In the United States, acupuncture gained public and professional attention in 1971, when New York Times reporter James Reston wrote about his experience with acupuncture after an emergency appendectomy in China 4. The operation was a success, but Reston soon had a considerable amount of postoperative pain and bloating. To provide relief, Chinese physicians offered acupuncture as a therapeutic modality. Reston, impressed by the effectiveness of this “ancient” procedure, described the overall improvement of his symptoms with no recurrence afterward. Through his newspaper article, he exposed countless Americans to acupuncture for the first time.
Today millions of Americans use acupuncture each year, often for chronic pain, but there has been considerable controversy surrounding its value as a therapy and whether it is anything more than placebo. Research exploring a number of possible mechanisms for acupuncture’s pain-relieving effects is ongoing.
Research suggests that acupuncture can help manage certain pain conditions – may help ease types of pain that are often chronic such as low-back pain, neck pain, and osteoarthritis/knee pain, but evidence about its value for other health issues is uncertain.
Acupuncture also may help reduce the frequency of tension headaches and prevent migraine headaches. Therefore, acupuncture appears to be a reasonable option for people with chronic pain to consider. However, clinical practice guidelines are inconsistent in recommendations about acupuncture.
The effects of acupuncture on the brain and body and how best to measure them are only beginning to be understood. Current evidence suggests that many factors—like expectation and belief—that are unrelated to acupuncture needling may play important roles in the beneficial effects of acupuncture on pain.
How does acupuncture work
There are many theories that may explain how acupuncture works. Many studies in animals and humans have demonstrated that acupuncture can cause multiple biological responses, including circulatory and biochemical effects. These responses can occur locally or close to the site of application or at a distance. They are mediated mainly by sensory neurons to many structures within the central nervous system. This can lead to activation of pathways affecting various physiological systems in the brain as well as in the periphery 5. In summary, possible mechanisms of the effects of acupuncture on neurological conditions include stimulation of neuronal cell proliferation 6, facilitation of neural plasticity 7, reduction of the post-ischaemic inflammatory reaction 8 and prevention of neuronal apoptosis 9.
Figure 2. Acupuncture points
Gate Control Theory of Pain
This theory postulates that specific nerve fibers transmit a pain signal to the brain via the spinal cord, and input of other nerve fibers can inhibit the pain signal transmission 10. Acupuncture is thought to stimulate inhibitory nerve fibers for a short period, thus reducing transmission of the pain signal to the brain.
Endorphin Model
During the 1970s, researchers isolated endogenous endorphins in the central nervous system. Clinical studies reported that inserting acupuncture needles into specific acupuncture points triggered the production of endorphins in cerebrospinal fluid after patients underwent acupuncture treatments 11. The pain-alleviating effects of acupuncture were reduced when naloxone was used to pretreat the patient, which may indicate that acupuncture-induced analgesia may be partly mediated through endogenous opioids 12.
Recent research has found that traditional Chinese medicine acupuncture therapy has a direct effect in the up-regulation of μ-opioid receptor binding availability in the central nervous system compared with placebo (sham) acupuncture 13. This finding may help explain some of the analgesic effects seen with acupuncture therapy.
Neurotransmitter Model
Research in animals has found that acupuncture can modulate serotonin, norepinephrine, and neurons that transmit or secrete γ-aminobutyric acid 14. It is postulated that through the neurotransmitter model, acupuncture can be efficacious for treatment of depression, anxiety, and addiction.
Other Theories
Other theories postulate that acupuncture indirectly influences the autonomic system. Acupuncture treatment can affect respiration, heart rate, blood pressure, circulation, and immune function 15. Research indicates the increased electrical conductivity of tissues along acupuncture meridians 16. This result suggests that manipulation of the acupuncture meridians with needles may modulate the transmission of certain signals within the body. The current scientific theories provide a basis for stating that acupuncture has an effect on the nervous system, but its effects cannot be explained with a single mechanism.
Who Provides Acupuncture Treatments ?
Nonphysician, licensed acupuncturists provide most acupuncture treatments in the United States. Although formal training programs differ from state to state, the National Certification Commission for Acupuncture and Oriental Medicine has developed rigorous certification criteria and examination requirements for licensed acupuncturists. The licensing mandates of a state should be checked to ensure the qualifications of a practitioner before a patient begins acupuncture treatment by that practitioner.
If you decide to visit an acupuncturist, check his or her credentials. Most states require a license, certification, or registration to practice acupuncture; however, education and training standards and requirements for obtaining these vary from state to state. Although a license does not ensure quality of care, it does indicate that the practitioner meets certain standards regarding the knowledge and use of acupuncture. Most states require a diploma from the National Certification Commission for Acupuncture and Oriental Medicine for licensing.
With the growth of integrative medicine, more physicians are seeking formal training in medical acupuncture. Physicians trained in medical acupuncture may be desirable practitioners, especially in complex cases in which conventional allopathic therapies need to be considered in developing an integrative treatment plan. The American Academy of Medical Acupuncture is a physician resource for training and certification.
Ask the practitioner about the estimated number of treatments needed and how much each treatment will cost. Some insurance companies may cover the costs of acupuncture, while others may not.
- Don’t use acupuncture to postpone seeing a health care provider about a health problem. Help your health care providers give you better coordinated and safe care by telling them about all the health approaches you use. Give them a full picture of what you do to manage your health.
Acupuncture therapy
The Chinese people continue to use acupuncture as a primary healing modality for the prevention and treatment of most ailments. In the United States, physicians and patients most frequently request acupuncture as an adjuvant therapy for managing conditions associated with acute and chronic pain. These conditions range across different neurologic, musculoskeletal, and gastrointestinal symptoms (see Table 1). As acceptance of acupuncture increases within the medical community, the scope of acupuncture practice will likely broaden to mirror what is practiced worldwide to include non–pain-related conditions. These changing trends are likely to lead to additional research efforts focused on conditions in which a paucity of evidence for use exists.
Table 1. Traditional Uses of Acupuncture Therapy
| Indication | Example | Comments |
|---|---|---|
| Common | ||
| Neurologic | Migraine Tension headache | Evidence suggests acupuncture can be helpful for management of migraine and tension-type headaches |
| Musculoskeletal | Osteoarthritis (knee) Fibromyalgia Back pain Neck pain Postoperative pain | Evidence suggests acupuncture can be helpful for management of osteoarthritis of the knee, fibromyalgia, and back, neck, and postoperative pain |
| Gastrointestinal | Nausea and vomiting Constipation Postoperative ileus IBS | Evidence suggests acupuncture can be helpful for management of chemotherapy-induced nausea and postoperative nausea and vomiting Inconsistent evidence suggests efficacy of acupuncture for management of constipation, postoperative ileus, and IBS Further research may be helpful |
| Gynecologic/reproductive | Hot flashes Infertility PMS | Inconsistent evidence suggests efficacy of acupuncture for management of hot flashes, infertility, and PMS Further research may be helpful |
| Psychiatric/mood | Stress Anxiety Depression | Inconsistent evidence suggests efficacy of acupuncture for management of stress, anxiety, and depression Further research may be helpful |
| Addiction | Nicotine dependence Alcohol dependence | Inconsistent evidence to make recommendations about the value of acupuncture in treatment of nicotine and alcohol dependence Further research needed |
| Endocrine | Obesity | Inconsistent evidence to make recommendations about the value of acupuncture in treatment of obesity Further research needed |
| Less common | ||
| ENT | Allergic rhinitis Sinusitis | Inconsistent evidence to make recommendations about the value of acupuncture in treatment of allergic rhinitis and sinusitis Further research needed |
| Respiratory | Asthma COPD | Inconsistent evidence to make recommendations about the value of acupuncture in treatment of asthma and COPD Further research needed |
| Cardiovascular | Hypertension Angina | Inconsistent evidence to make recommendations about the value of acupuncture in treatment of hypertension and angina Further research needed |
| Sleep | Insomnia Enuresis | Inconsistent evidence to make recommendations about the value of acupuncture in treatment of insomnia and enuresis Further research needed |
Note: COPD = chronic obstructive pulmonary disease; ENT = ear, nose, throat; IBS = irritable bowel syndrome; PMS = premenstrual syndrome.
[Source 1]Acupuncture benefits
What Does the Evidence Show ?
Although acupuncture has been used for thousands of years in Asia, the research community has started studying it only in the past few decades. The nature of acupuncture therapy involves tailoring treatments to the individual patient, and thus research on acupuncture has been difficult because of variable treatment interventions, techniques, and study size. Meta-analysis studies of acupuncture are limited because of the heterogeneity of pooling acupuncture treatment data.
Stroke Rehabilitation
A 2016 Cochrane review 17 involving 31 trials with a total of 2257 participants in the subacute or chronic stages of stroke. Two trials compared real acupuncture plus baseline treatment with sham acupuncture plus baseline treatment. There was no evidence of differences in the changes of motor function and quality of life between real acupuncture and sham acupuncture for people with stroke in the convalescent stage. Twenty-nine trials compared acupuncture plus baseline treatment versus baseline treatment alone. Compared with no acupuncture, for people with stroke in the convalescent phase, acupuncture had beneficial effects on the improvement of dependency (activity of daily living). The review authors conclusion was that acupuncture may have beneficial effects on improving dependency, global neurological deficiency, and some specific neurological impairments for people with stroke in the convalescent stage, with no obvious serious adverse events 17. However, most included trials were of inadequate quality and size. There is, therefore, inadequate evidence to draw any conclusions about its routine use 17. Rigorously designed, randomized, multi-center, large sample trials of acupuncture for stroke are needed to further assess its effects.
Period Pain
Another good quality review conducted in 2016 18 included 42 randomized controlled trials (4640 women). Acupuncture or acupressure was compared with a sham/placebo group, medication, no treatment or other treatment. Many of the continuous data were not suitable for calculation of means, mainly due to evidence of skew. The finding of that good quality review was there is insufficient evidence to demonstrate whether or not acupuncture or acupressure are effective in treating primary dysmenorrhoea (period pain) and for most comparisons no data were available on adverse events 18. The quality of the evidence was low or very low for all comparisons. The main limitations were risk of bias, poor reporting, inconsistency and risk of publication bias.
Peripheral Joint Osteoarthritis
In 2010 a Cochrane Review 19 was conducted to assess the effects of acupuncture for treating peripheral joint osteoarthritis. Sixteen trials involving 3498 people were included. Twelve of the randomized controlled trials included only people with osteoarthritis of the knee, 3 only osteoarthritis of the hip, and 1 a mix of people with osteoarthritis of the hip and/or knee. In comparison with a sham control, acupuncture showed statistically significant, short-term improvements in osteoarthritis pain; however, these benefits are small, do not meet the review authors pre-defined thresholds for clinical relevance and are probably due at least partially to placebo effects from incomplete blinding 19. Waiting list-controlled trials of acupuncture for peripheral joint osteoarthritis suggest statistically significant and clinically relevant benefits, much of which may be due to expectation or placebo effects 19.
Best estimate of what happens to people with osteoarthritis who have acupuncture 19:
Pain after 8 weeks:
- People who had acupuncture rated their pain to be improved by about 4 points on a scale of 0 to 20.
- People who received sham acupuncture rated their pain to be improved by about 3 points on a scale of 0 to 20.
- People who received acupuncture had a 1 point greater improvement on a scale of 0-20. (5% absolute improvement).
Pain after 26 weeks:
- People who had acupuncture rated their pain to be improved by slightly more than 3 points on a scale of 0 to 20.
- People who received sham acupuncture rated their pain to be improved by slightly less than 3 points on a scale of 0 to 20.
- People who received acupuncture had under a 1 point greater improvement on a scale of 0-20. (2% absolute improvement).
Physical function after 8 weeks :
- People who had acupuncture rated their function to be improved by about 11 points on a scale of 0 to 68.
- People who received sham acupuncture rated their function to be improved by about 8 points on a scale of 0 to 68.
- People who received acupuncture had about a 3 point greater improvement on a scale of 0-68. (4% absolute improvement)
Physical function after 26 weeks :
- People who had acupuncture rated their function to be improved by about 11 points on a scale of 0 to 68.
- People who received sham acupuncture rated their function to be improved by about 10 points on a scale of 0 to 68.
- People who received acupuncture had about a 1 point greater improvement on a scale of 0-68. (2% absolute improvement).
Rheumatoid arthritis
A good quality systematic review 20 was conducted to evaluate the effects of acupuncture or electro-acupuncture on the objective and subjective measures of disease activity in patients with rheumatoid arthritis. Although the results of the study on electro-acupuncture show that electro-acupuncture may be beneficial to reduce symptomatic knee pain in patients with rheumatoid arthritis 24 hours and 4 months post treatment, the reviewers concluded that the poor quality of the trial, including the small sample size preclude its recommendation. The reviewers further conclude that acupuncture has no effect on ESR, CRP, pain, patient’s global assessment, number of swollen joints, number of tender joints, general health, disease activity and reduction of analgesics 20. These conclusions are limited by methodological considerations such as the type of acupuncture (acupuncture vs electroacupuncture), the site of intervention, the low number of clinical trials and the small sample size of the included studies.
Fibromyalgia
One in five fibromyalgia sufferers use acupuncture treatment within two years of diagnosis. In 2013 a Cochrane Review 21 was conducted to examine the benefits and safety of acupuncture treatment for fibromyalgia. Nine trials (395 participants) were included. All studies except one were at low risk of selection bias; five were at risk of selective reporting bias (favoring either treatment group); two were subject to attrition bias (favoring acupuncture); three were subject to performance bias (favoring acupuncture) and one to detection bias (favoring acupuncture). Three studies utilized electro-acupuncture with the remainder using manual acupuncture without electrical stimulation. All studies used ‘formula acupuncture’ except for one, which used trigger points.
There was low to moderate-level evidence that compared with no treatment and standard therapy, acupuncture improves pain and stiffness in people with fibromyalgia 21. There is moderate-level evidence that the effect of acupuncture does not differ from sham acupuncture in reducing pain or fatigue, or improving sleep or global well-being. Electro-acupuncture is probably better than manual acupuncture for pain and stiffness reduction and improvement of global well-being, sleep and fatigue. The effect lasts up to one month, but is not maintained at six months follow-up. Manual acupuncture probably does not improve pain or physical functioning. Acupuncture appears safe. People with fibromyalgia may consider using electro-acupuncture alone or with exercise and medication. The small sample size, scarcity of studies for each comparison, lack of an ideal sham acupuncture weaken the level of evidence and its clinical implications. Larger studies are warranted.
Neuropathic pain in adults
Neuropathic pain may be caused by nerve damage, and is often followed by changes to the central nervous system. Due to the limited data available, there is insufficient evidence to support or refute the use of acupuncture for neuropathic pain in general, or for any specific neuropathic pain condition when compared with sham acupuncture or other active therapies 22. Five studies are still ongoing and seven studies are awaiting classification due to the unclear treatment duration, and the results of these studies may influence the current findings.
Cancer pain in adults
Forty per cent of individuals with early or intermediate stage cancer and 90% with advanced cancer have moderate to severe pain and up to 70% of patients with cancer pain do not receive adequate pain relief. Five randomized controlled trials with 285 participants were included in this review 23. All studies had a high risk of bias from inadequate sample size and a low risk of bias associated with random sequence generation. Only three studies had low risk of bias associated with incomplete outcome data, while two studies had low risk of bias associated with allocation concealment and one study had low risk of bias associated with inadequate blinding. In conclusion, there is insufficient evidence to judge whether acupuncture is effective in treating cancer pain in adults.
Shoulder pain
In 2005 a well conducted review 24 was done to determine the efficacy and safety of acupuncture in the treatment of adults with shoulder pain. Nine trials of varying methodological quality met the inclusion criteria. For all trials there was poor description of interventions. Varying placebos were used in the different trials. There was no significant difference in short-term improvement associated with acupuncture when compared to placebo. In conclusion, due to a small number of clinical and methodologically diverse trials, little can be concluded from this review. There is little evidence to support or refute the use of acupuncture for shoulder pain although there may be short-term benefit with respect to pain and function. There is a need for further well designed clinical trials.
Lateral elbow pain
There is insufficient evidence to either support or refute the use of acupuncture (either needle or laser) in the treatment of lateral elbow pain. This review 25 has demonstrated needle acupuncture to be of short term benefit with respect to pain, but this finding is based on the results of 2 small trials, the results of which were not able to be combined in meta-analysis. No benefit lasting more than 24 hours following treatment has been demonstrated. No trial assessed or commented on potential adverse effect. Further trials, utilizing appropriate methods and adequate sample sizes, are needed before conclusions can be drawn regarding the effect of acupuncture on tennis elbow.
Low-Back Pain
- A 2012 analysis of data on participants in acupuncture studies looked at back and neck pain together and found that actual acupuncture was more helpful than either no acupuncture or simulated acupuncture.
- A 2010 review by the Agency for Healthcare Research and Quality found that acupuncture relieved low-back pain immediately after treatment but not over longer periods of time.
- A 2008 systematic review of studies on acupuncture for low-back pain found strong evidence that combining acupuncture with usual care helps more than usual care alone. The same review also found strong evidence that there is no difference between the effects of actual and simulated acupuncture in people with low-back pain.
Clinical practice guidelines issued by the American Pain Society and the American College of Physicians in 2007 recommend acupuncture as one of several nondrug approaches physicians should consider when patients with chronic low-back pain do not respond to self-care (practices that people can do by themselves, such as remaining active, applying heat, and taking pain-relieving medications). - Clinical practice guidelines issued by the American Pain Society and the American College of Physicians in 2007 recommend acupuncture as one of several nondrug approaches physicians should consider when patients with chronic low-back pain do not respond to self-care (practices that people can do by themselves, such as remaining active, applying heat, and taking pain-relieving medications).
Neck Pain
- A 2009 analysis found that actual acupuncture was more helpful for neck pain than simulated acupuncture, but the analysis was based on a small amount of evidence (only three studies with small study populations).
- A large German study with more than 14,000 participants evaluated adding acupuncture to usual care for neck pain. The researchers found that participants reported greater pain relief than those who didn’t receive it; the researchers didn’t test actual acupuncture against simulated acupuncture.
Headache
- A 2012 analysis of data on individual participants in acupuncture studies looked at migraine and tension headaches. The analysis showed that actual acupuncture was more effective than either no acupuncture or simulated acupuncture in reducing headache frequency or severity.
- A 2009 systematic review of studies concluded that actual acupuncture, compared with simulated acupuncture or pain-relieving drugs, helped people with tension-type headaches. A 2008 systematic review of studies suggested that actual acupuncture has a very slight advantage over simulated acupuncture in reducing tension-type headache intensity and the number of headache days per month.
- A 2009 systematic review found that adding acupuncture to basic care for migraines helped to reduce migraine frequency. However, in studies that compared actual acupuncture with simulated acupuncture, researchers found that the differences between the two treatments may have been due to chance.
Episodic migraine
In a Cochrane Review 26, twenty-two trials involving 4985 participants, acupuncture was associated with a moderate reduction of headache frequency over no acupuncture after treatment. The available evidence suggests that adding acupuncture to symptomatic treatment of attacks reduces the frequency of headaches. The updated evidence 26 also suggests that there is an effect over sham, but this effect is small. The available trials also suggest that acupuncture may be at least similarly effective as treatment with prophylactic drugs. Acupuncture can be considered a treatment option for patients willing to undergo this treatment. As for other migraine treatments, long-term studies, more than one year in duration, are lacking.
Attention Deficit Hyperactivity Disorder (ADHD) in children and adolescents
Attention Deficit Hyperactivity Disorder (ADHD) is a common childhood psychiatric disorder with features of inattention, hyperactivity and impulsivity.
A comprehensive search showed that there is no evidence base of randomized or quasi-randomized controlled trials to support the use of acupuncture as a treatment for ADHD in children and adolescents. Due to the lack of trials, we cannot reach any conclusions about the efficacy and safety of acupuncture for ADHD in children and adolescents. This excellent quality review 27 highlights the need for further research in this area in the form of high quality, large scale, randomized controlled trials.
Autism spectrum disorders (ASD)
Autism spectrum disorders (ASD) are lifelong disorders of development. People with ASD have particular difficulties with social interaction and communication and they lack flexibility in their thinking and behavior. No cure is currently available but interventions may improve symptoms.
Current evidence does not support the use of acupuncture for treatment of ASD 28 high quality trials of larger size and longer follow-up are needed.
Induction of labour
Induction of labour is offered to pregnant women when it is thought the outcome will be better for the mother or her baby if the pregnancy does not continue and the baby is born. Common reasons for induction include the pregnancy going beyond the due date, pre-term or pre-labour rupture of the membranes, and concerns about the health of the mother or baby such as pre-eclampsia or poor growth of the baby.
Overall, there was no clear benefit from acupuncture or acupressure in reducing caesarean section rate 29. The quality of the evidence varied between low to high. Few trials reported on neonatal morbidity or maternal mortality outcomes. Acupuncture showed some benefit in improving cervical maturity, however, more well-designed trials are needed. Future trials could include clinically relevant safety outcomes.
Pain management in labour
Many women would like to avoid pharmacological or invasive methods of pain management in labour and this may contribute towards the popularity of complementary methods of pain management. A systematic review was done in 2011 using 13 trials with data reporting on 1986 women 30. Nine trials reported on acupuncture and four trials reported on acupressure. Less intense pain was found from acupuncture compared with no intervention. Pain intensity was reduced in the acupressure group compared with a placebo control. In conclusion, acupuncture and acupressure may have a role with reducing pain, increasing satisfaction with pain management and reduced use of pharmacological management 30. However, there is a need for further research.
Glaucoma
In 2013 Cochrane Review 31 to assess the effectiveness and safety of acupuncture in people with glaucoma. The review found that it is impossible to draw reliable conclusions from available data to support the use of acupuncture for the treatment of glaucoma. Because of ethical considerations, randomized controlled trials comparing acupuncture alone with standard glaucoma treatment or placebo are unlikely to be justified in countries where the standard of care has already been established 31. Because most glaucoma patients currently cared for by ophthalmologists do not use nontraditional therapy, clinical practice decisions will have to be based on physician judgments and patient preferences, given this lack of data in the literature. Inclusion of the seven Chinese trials in future updates of this review may change their conclusions.
Slowing the progression of myopia in children and adolescents
Myopia (near-sightedness or short-sightedness) is one of the three commonly detected refractive (focusing) errors. Two trials are included in this review 32 but no conclusions can be drawn for the benefit of co-acupressure for slowing progress of myopia in children. Further evidence in the form of randomized controlled trials are needed before any recommendations can be made for the use of acupuncture treatment in clinical use. These trials should compare acupuncture to placebo and have large sample sizes. Other types of acupuncture (such as auricular acupuncture) should be explored further as well as compliance with treatment for at least six months or longer. Axial length elongation of the eye should be investigated for at least one year. The potential to reduce/eliminate pain from acupuncture experienced by children should also be reviewed.
Depression
A good quality review 33 examined the effectiveness and adverse effects of acupuncture in the treatment for depression. The review found there was a high risk of bias in the majority of trials. There was insufficient evidence of a consistent beneficial effect from acupuncture compared with a wait list control or sham acupuncture control. The reviewers found insufficient evidence to recommend the use of acupuncture for people with depression 33. The results are limited by the high risk of bias in the majority of trials meeting inclusion criteria.
Epilepsy
A Cochrane Review was conducted in 2014 34 to determine the effectiveness and safety of acupuncture in people with epilepsy. There were 17 randomized controlled trials with 1538 participants that had a wide age range and were suffering mainly from generalized epilepsy. The duration of treatment varied from 7.5 weeks to 1 year. All included trials had a high risk of bias with short follow-up. Compared with Chinese herbs, needle acupuncture plus Chinese herbs was not effective in achieving at least 50% reduction in seizure frequency (80% in control group versus 90% in intervention group. Based on those small, heterogeneous and high risk of biased evidence, the use of acupuncture for treating epilepsy cannot be supported.
Acute hordeolum (Stye infection)
Hordeolum is an acute, purulent inflammation of the eyelid margin usually caused by obstructed orifices of the sebaceous glands of the eyelid. The condition, which affects sebaceous glands internally or externally, is common. A Cochrane Review 35 was conducted to investigate the effectiveness and safety of acupuncture to treat acute hordeolum compared with no treatment, sham acupuncture, or other active treatment. There was low-certainty evidence suggesting that acupuncture with or without conventional treatments may provide short-term benefits for treating acute hordeolum when compared with conventional treatments alone. The certainty of the evidence was low to very low mainly due to small sample sizes, inadequate allocation concealment, lack of masking of the outcome assessors, inadequate or unclear randomization method, and a high or unreported number of dropouts. All randomized controlled trials were conducted in China, which may limit their generalizability to non-Chinese populations.
Because no randomized controlled trials included a valid sham acupuncture control, we cannot rule out a potential expectation/placebo effect associated with acupuncture. As resolution is based on clinical observation, the outcome could be influenced by the observer’s knowledge of the assigned treatment. Adverse effects of acupuncture were reported sparsely in the included randomized controlled trials and, when reported, were rare. Randomized controlled trials with better methodology, longer follow-up, and which are conducted among other populations are warranted to provide more general evidence regarding the benefit of acupuncture to treat acute hordeolum.
Bell’s palsy
Bell’s palsy or idiopathic facial palsy is an acute facial paralysis due to inflammation of the facial nerve. A number of studies published in China have suggested acupuncture is beneficial for facial palsy. A quality review 36 was conducted to examine the efficacy of acupuncture in hastening recovery and reducing long-term morbidity from Bell’s palsy. The quality of the included trials was inadequate to allow any conclusion about the efficacy of acupuncture. More research with high quality trials is needed.
Insomnia
A 2012 Cochrane Review 37 involving thirty-three trials were included to determine the efficacy and safety of acupuncture for insomnia. They recruited 2293 participants with insomnia, aged 15 to 98 years, some with medical conditions contributing to insomnia (stroke, end-stage renal disease, perimenopause, pregnancy, psychiatric diseases). They evaluated needle acupuncture, electro-acupuncture, acupressure or magnetic acupressure. Due to poor methodological quality, high levels of heterogeneity and publication bias, the current evidence is not sufficiently rigorous to support or refute acupuncture for treating insomnia. Larger high-quality clinical trials are required.
Restless legs syndrome
Restless legs syndrome is a sensorimotor movement disorder characterized by uncomfortable sensations in the legs and an urge to move them. The syndrome is very common and its lifestyle impacts justify a search for more effective and acceptable interventions. There is insufficient evidence to support the use of acupuncture for the symptomatic treatment of restless legs syndrome 38.
Cocaine dependence
More than 400 substance abuse clinics in the USA and Europe offer a treatment for cocaine dependence called auricular acupuncture. In this treatment, needles are usually inserted into five specific points in the ear, but some clinics use only four or three of the points. In this Cochrane review 39 the authors set out to discover whether auricular acupuncture is effective in treating cocaine dependence and whether the number of points used makes a difference. There is currently no evidence that auricular acupuncture is effective for the treatment of cocaine dependence 39. The evidence is not of high quality and is inconclusive. Further randomized trials of auricular acupuncture may be justified.
Smoking cessation
Although pooled estimates suggest possible short-term effects there is no consistent, bias-free evidence that acupuncture, acupressure, or laser therapy have a sustained benefit on smoking cessation for six months or more 40. However, lack of evidence and methodological problems mean that no firm conclusions can be drawn. Electrostimulation is not effective for smoking cessation. Well-designed research into acupuncture, acupressure and laser stimulation is justified since these are popular interventions and safe when correctly applied, though these interventions alone are likely to be less effective than evidence-based interventions.
Uterine fibroids
Uterine fibroids are benign growths within the uterine muscle and are present in 30% of women during their reproductive years. To assess the benefits and harms of acupuncture in women with uterine fibroids, as systematic review 41 was done. No randomized double-blind controlled trials met the inclusion criteria. The effectiveness of acupuncture for the management of uterine fibroids remains uncertain. More evidence is required to establish the efficacy and safety of acupuncture for uterine fibroids. There is a continued need for well designed randomized controlled trials with long term follow up.
Endometriosis
Endometriosis is a gynaecological disease that causes chronic pelvic pain, most notably painful menstruation, as the most common complaint.
The evidence to support the effectiveness of acupuncture for pain in endometriosis is limited, based on the results of only a single study that was included in this review 42. This review examined the effectiveness of acupuncture for reducing pain in endometriosis; however only one study met our inclusion criteria. The data from the included study, involving 67 women, indicated that ear acupuncture is more effective compared to Chinese herbal medicine for reducing menstrual pain. The study did not report whether participants suffered any side effects from their treatments. Larger, well-designed studies comparing acupuncture with conventional therapies are necessary to confirm these results.
Polycystic ovarian syndrome
Polycystic ovarian syndrome (PCOS) is where women have small cysts on their ovaries (organs that produce eggs) and is characterised by the clinical signs of infrequent or very light menstruation (periods), failure to conceive (become pregnant) and excessive hair growth. Thus far, only a limited number of randomized controlled trials have been reported. At present, there is insufficient evidence to support the use of acupuncture for treatment of ovulation disorders in women with PCOS 43.
Menopausal hot flushes
Hot flushes are the most common menopausal vasomotor symptom. Hormone therapy has frequently been recommended for relief of hot flushes, but concerns about the health risks of hormone therapy have encouraged women to seek alternative treatments.A Cochrane Review found insufficient evidence to determine whether acupuncture is effective for controlling menopausal vasomotor symptoms 44. When we compared acupuncture with sham acupuncture, there was no evidence of a significant difference in their effect on menopausal vasomotor symptoms. When we compared acupuncture with no treatment there appeared to be a benefit from acupuncture, but acupuncture appeared to be less effective than hormone therapy. These findings should be treated with great caution as the evidence was low or very low quality and the studies comparing acupuncture versus no treatment or hormone therapy were not controlled with sham acupuncture or placebo hormone therapy. Data on adverse effects were lacking.
Functional dyspepsia
A Cochrane Review 45 was done in 2014 to to assess the efficacy and safety of manual acupuncture and electroacupuncture in the treatment of functional dyspepsia. However, all the evidence was of low or very low quality. The body of evidence identified cannot yet permit a robust conclusion regarding the efficacy and safety of acupuncture for functional dyspepsia. It remains unknown whether manual acupuncture or electro-acupuncture is more effective or safer than other treatments for patients with functional dyspepsia.
Irritable bowel syndrome
Sham-controlled randomized controlled trials have found no benefits of acupuncture relative to a credible sham acupuncture control for IBS symptom severity or IBS-related quality of life 46. In comparative effectiveness Chinese trials, patients reported greater benefits from acupuncture than from two antispasmodic drugs (pinaverium bromide and trimebutine maleate), both of which have been shown to provide a modest benefit for IBS. Future trials may help clarify whether or not these reportedly greater benefits of acupuncture relative to pharmacological therapies are due entirely to patients’ preferences for acupuncture or greater expectations of improvement on acupuncture relative to drug therapy.
Stress urinary incontinence in adults
Stress urinary incontinence is a common disease among older people, especially women. The symptoms are leakage of urine when the person coughs, laughs or exercises. It affects social, psychological, physical and financial aspects of life.
The effect of acupuncture for stress urinary incontinence for adults is uncertain. There is not enough evidence to determine whether acupuncture is more effective than drug treatment 47.
Schizophrenia
A 2014 Cochrane Review 48 found limited evidence suggesting that acupuncture may have some antipsychotic effects as measured on global and mental state with few adverse effects. Better designed large studies are needed to fully and fairly test the effects of acupuncture for people with schizophrenia.
Vascular dementia
The effectiveness of acupuncture for vascular dementia is uncertain 49. More evidence is required to show that vascular dementia can be treated effectively by acupuncture. There are no randomized controlled trials and high quality trials are few. Randomized double-blind placebo-controlled trials are urgently needed.
Acupuncture side effects
Acupuncture is generally considered safe when performed by an experienced, well-trained practitioner using sterile needles. Improperly performed acupuncture can cause serious side effects.
The U.S. Food and Drug Administration (FDA) regulates acupuncture needles as medical devices for use by licensed practitioners and requires that needles be manufactured and labeled according to certain standards. For example, the FDA requires that needles be sterile, nontoxic, and labeled for single use by qualified practitioners only.
Acupuncture in the developed parts of the world involves single-use, disposable needles packaged and sealed by the manufacturer in sterile conditions. Although case reports have highlighted major adverse events, such as organ puncture, infections, and bleeding complications, more recent, larger cohort studies using universal precautions have not found a significant complication rate. In a 2001 study of more than 34,000 acupuncture treatments in the United Kingdom, no serious adverse events (e.g, hospitalization, permanent disability, or death) were reported in relation to acupuncture therapy, and the rate of underlying minor adverse events (e.g, nausea, fainting, prolonged aggravation of existing symptoms, and psychological or emotional reaction) was reported to be between 0 and 1.1 per 10,000 treatments 50. Acupuncture involves puncturing the skin, and therefore slight bruising, bleeding, or soreness at the acupuncture site may occur because of needle penetration through capillaries. More serious adverse effects, such as a vasovagal response with a decrease in blood pressure and syncope, have been reported. Infections may occur at the needle site from the use of nonsterile needles. When herbs are burned too close to the skin, burn injuries can result around the needle site.
Acupuncture is generally considered safe for persons with bleeding disorders or taking anticoagulants. However, it is important for the patient to advise the practitioner of these facts so the practitioner can use vigilance in selecting insertion points. Acupuncture during pregnancy is a matter of continued debate. Certain acupuncture points are contraindicated because they may induce uterine contractions and premature labor.
- Chon TY, Lee MC. Acupuncture. Mayo Clinic Proceedings. 2013;88(10):1141–1146. http://www.mayoclinicproceedings.org/article/S0025-6196(13)00513-2/fulltext[↩][↩]
- Kee, C.P. Acupuncture: an ancient Chinese art of healing. Singapore Med J. 1963; 3: 151–157. https://www.ncbi.nlm.nih.gov/pubmed/14104633[↩]
- Hsu, E. Outline of the history of acupuncture in Europe. J Chin Med. 1989; 29: 28–32[↩]
- Reston, J. Now, about my operation in Peking; now, let me tell you about my appendectomy in Peking. New York Times. July 26, 1971; : 1[↩]
- Wang ZY. Compared analyses among Chinese medicinal herbs, acupuncture and combination of them in the treatment of hemiplegia in stroke patients [中药、针刺、针药并举对脑卒中偏瘫康复的疗效对比分析]. Modern Rehabilitation 2001;5(6):130. [↩]
- Cheng H, Yu J, Jiang Z. Acupuncture improves cognitive deficits and regulates the brain cell proliferation of SAMP8 mice. Neuroscience Letters 2008;432:111-6.[↩]
- Ren L, Zhang WA, Fang NY. The influence of electro-acupuncture on neural plasticity in acute cerebral infarction. Neurological Research 2008;30:985-9.[↩]
- Liu Z, Fang JQ, Zeng C. Development of studies on the underlying mechanism of acupuncture intervention in reducing post-ischemic inflammatory reaction and the related new research thought. Zhen Ci Yan Jiu 2009;34:61-6.[↩]
- Zhang HZ, Zhang LX, She YF. Effect of electroacupuncture on apoptosis of hippocampus tissue in mice with vascular dementia. Zhen Ci Yan Jiu 2008;33:377-81.[↩]
- Melzack, R. and Wall, P.D. Pain mechanisms: a new theory. Science. 1965; 150: 971–979[↩]
- Napadow, V., Ahn, A., Longhurst, J. et al. The status and future of acupuncture mechanism research. J Altern Complement Med. 2008; 14: 861–869. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3155097/[↩]
- Eriksson, S.V., Lundeberg, T., and Lundeberg, S. Interaction of diazepam and naloxone on acupuncture induced pain relief. Am J Chin Med. 1991; 19: 1–7. http://www.worldscientific.com/doi/abs/10.1142/S0192415X91000028[↩]
- Harris, R.E., Zubieta, J.K., Scott, D.J., Napadow, V., Gracely, R.H., and Clauw, D.J. Traditional Chinese acupuncture and placebo (sham) acupuncture are differentiated by their effects on mu-opioid receptors (MORs). Neuroimage. 2009; 47: 1077–1085. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2757074/[↩]
- Yoshimoto, K., Fukuda, F., Hori, M. et al. Acupuncture stimulates the release of serotonin, but not dopamine, in the rat nucleus accumbens. Tohoku J Exp Med. 2006; 208: 321–326. https://www.jstage.jst.go.jp/article/tjem/208/4/208_4_321/_pdf/-char/en[↩]
- Andersson, S. and Lundeberg, T. Acupuncture: from empiricism to science: functional background to acupuncture effects in pain and disease. Med Hypotheses. 1995; 45: 271–281. https://www.ncbi.nlm.nih.gov/pubmed/8569551[↩]
- Becker, R.O., Reichmanis, M., Marino, A.A., and Spadaro, J.A. Electrophysiological correlates of acupuncture points and meridians. Psychoenergetic Systems. 1976; 1: 105–112[↩]
- Yang A, Wu HM, Tang JL, Xu L, Yang M, Liu GJ. Acupuncture for stroke rehabilitation. Cochrane Database of Systematic Reviews 2016, Issue 8. Art. No.: CD004131. DOI: 10.1002/14651858.CD004131.pub3. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD004131.pub3/full[↩][↩][↩]
- Smith CA, Armour M, Zhu X, Li X, Lu ZY, Song J. Acupuncture for dysmenorrhoea. Cochrane Database of Systematic Reviews 2016, Issue 4. Art. No.: CD007854. DOI: 10.1002/14651858.CD007854.pub3. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007854.pub3/full[↩][↩]
- Manheimer E, Cheng K, Linde K, Lao L, Yoo J, Wieland S, van der Windt DAWM, Berman BM, Bouter LM. Acupuncture for peripheral joint osteoarthritis. Cochrane Database of Systematic Reviews 2010, Issue 1. Art. No.: CD001977. DOI: 10.1002/14651858.CD001977.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD001977.pub2/full[↩][↩][↩][↩]
- Casimiro L, Barnsley L, Brosseau L, Milne S, Welch V, Tugwell P, Wells GA. Acupuncture and electroacupuncture for the treatment of rheumatoid arthritis. Cochrane Database of Systematic Reviews 2005, Issue 4. Art. No.: CD003788. DOI: 10.1002/14651858.CD003788.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003788.pub2/full[↩][↩]
- Deare JC, Zheng Z, Xue CCL, Liu JP, Shang J, Scott SW, Littlejohn G. Acupuncture for treating fibromyalgia. Cochrane Database of Systematic Reviews 2013, Issue 5. Art. No.: CD007070. DOI: 10.1002/14651858.CD007070.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007070.pub2/full[↩][↩]
- Ju ZY, Wang K, Cui HS, Yao Y, Liu SM, Zhou J, Chen TY, Xia J. Acupuncture for neuropathic pain in adults. Cochrane Database of Systematic Reviews 2017, Issue 12. Art. No.: CD012057. DOI: 10.1002/14651858.CD012057.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD012057.pub2/full[↩]
- Paley CA, Johnson MI, Tashani OA, Bagnall AM. Acupuncture for cancer pain in adults. Cochrane Database of Systematic Reviews 2015, Issue 10. Art. No.: CD007753. DOI: 10.1002/14651858.CD007753.pub3. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007753.pub3/full[↩]
- Green S, Buchbinder R, Hetrick SE. Acupuncture for shoulder pain. Cochrane Database of Systematic Reviews 2005, Issue 2. Art. No.: CD005319. DOI: 10.1002/14651858.CD005319. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD006030.pub3/full[↩]
- Green S, Buchbinder R, Barnsley L, Hall S, White M, Smidt N, Assendelft WJJ. Acupuncture for lateral elbow pain. Cochrane Database of Systematic Reviews 2002, Issue 1. Art. No.: CD003527. DOI: 10.1002/14651858.CD003527. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003527/full[↩]
- Linde K, Allais G, Brinkhaus B, Fei Y, Mehring M, Vertosick EA, Vickers A, White AR. Acupuncture for the prevention of episodic migraine. Cochrane Database of Systematic Reviews 2016, Issue 6. Art. No.: CD001218. DOI: 10.1002/14651858.CD001218.pub3. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD001218.pub3/full[↩][↩]
- Li S, Yu B, Zhou D, He C, Kang L, Wang X, Jiang S, Chen X. Acupuncture for Attention Deficit Hyperactivity Disorder (ADHD) in children and adolescents. Cochrane Database of Systematic Reviews 2011, Issue 4. Art. No.: CD007839. DOI: 10.1002/14651858.CD007839.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007839.pub2/full[↩]
- Cheuk DKL, Wong V, Chen WX. Acupuncture for autism spectrum disorders (ASD). Cochrane Database of Systematic Reviews 2011, Issue 9. Art. No.: CD007849. DOI: 10.1002/14651858.CD007849.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007849.pub2/full[↩]
- Smith CA, Armour M, Dahlen HG. Acupuncture or acupressure for induction of labour. Cochrane Database of Systematic Reviews 2017, Issue 10. Art. No.: CD002962. DOI: 10.1002/14651858.CD002962.pub4. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD002962.pub4/full[↩]
- Smith CA, Collins CT, Crowther CA, Levett KM. Acupuncture or acupressure for pain management in labour. Cochrane Database of Systematic Reviews 2011, Issue 7. Art. No.: CD009232. DOI: 10.1002/14651858.CD009232. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD009232/full[↩][↩]
- Law SK, Li T. Acupuncture for glaucoma. Cochrane Database of Systematic Reviews 2013, Issue 5. Art. No.: CD006030. DOI: 10.1002/14651858.CD006030.pub3. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD006030.pub3/full[↩][↩]
- Wei ML, Liu JP, Li N, Liu M. Acupuncture for slowing the progression of myopia in children and adolescents. Cochrane Database of Systematic Reviews 2011, Issue 9. Art. No.: CD007842. DOI: 10.1002/14651858.CD007842.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007842.pub2/full[↩]
- Smith CA, Hay PPJ, MacPherson H. Acupuncture for depression. Cochrane Database of Systematic Reviews 2010, Issue 1. Art. No.: CD004046. DOI: 10.1002/14651858.CD004046.pub3. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD004046.pub3/full[↩][↩]
- Cheuk DKL, Wong V. Acupuncture for epilepsy. Cochrane Database of Systematic Reviews 2014, Issue 5. Art. No.: CD005062. DOI: 10.1002/14651858.CD005062.pub4. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD005062.pub4/full[↩]
- Cheng K, Law A, Guo M, Wieland LS, Shen X, Lao L. Acupuncture for acute hordeolum. Cochrane Database of Systematic Reviews 2017, Issue 2. Art. No.: CD011075. DOI: 10.1002/14651858.CD011075.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD011075.pub2/full[↩]
- Chen N, Zhou M, He L, Zhou D, Li N. Acupuncture for Bell’s palsy. Cochrane Database of Systematic Reviews 2010, Issue 8. Art. No.: CD002914. DOI: 10.1002/14651858.CD002914.pub5. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD002914.pub5/full[↩]
- Cheuk DKL, Yeung WF, Chung KF, Wong V. Acupuncture for insomnia. Cochrane Database of Systematic Reviews 2012, Issue 9. Art. No.: CD005472. DOI: 10.1002/14651858.CD005472.pub3. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD005472.pub3/full[↩]
- Cui Y, Wang Y, Liu Z. Acupuncture for restless legs syndrome. Cochrane Database of Systematic Reviews 2008, Issue 4. Art. No.: CD006457. DOI: 10.1002/14651858.CD006457.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD006457.pub2/full[↩]
- Gates S, Smith LA, Foxcroft D. Auricular acupuncture for cocaine dependence. Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD005192. DOI: 10.1002/14651858.CD005192.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD005192.pub2/full[↩][↩]
- White AR, Rampes H, Liu JP, Stead LF, Campbell J. Acupuncture and related interventions for smoking cessation. Cochrane Database of Systematic Reviews 2014, Issue 1. Art. No.: CD000009. DOI: 10.1002/14651858.CD000009.pub4. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000009.pub4/full[↩]
- Zhang Y, Peng W, Clarke J, Zhishun L. Acupuncture for uterine fibroids. Cochrane Database of Systematic Reviews 2010, Issue 1. Art. No.: CD007221. DOI: 10.1002/14651858.CD007221.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007221.pub2/full[↩]
- Zhu X, Hamilton KD, McNicol ED. Acupuncture for pain in endometriosis. Cochrane Database of Systematic Reviews 2011, Issue 9. Art. No.: CD007864. DOI: 10.1002/14651858.CD007864.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007864.pub2/full[↩]
- Lim CED, Ng RWC, Xu K, Cheng NCL, Xue CCL, Liu JP, Chen N. Acupuncture for polycystic ovarian syndrome. Cochrane Database of Systematic Reviews 2016, Issue 5. Art. No.: CD007689. DOI: 10.1002/14651858.CD007689.pub3. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007689.pub3/full[↩]
- Dodin S, Blanchet C, Marc I, Ernst E, Wu T, Vaillancourt C, Paquette J, Maunsell E. Acupuncture for menopausal hot flushes. Cochrane Database of Systematic Reviews 2013, Issue 7. Art. No.: CD007410. DOI: 10.1002/14651858.CD007410.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007410.pub2/full[↩]
- Lan L, Zeng F, Liu GJ, Ying L, Wu X, Liu M, Liang FR. Acupuncture for functional dyspepsia. Cochrane Database of Systematic Reviews 2014, Issue 10. Art. No.: CD008487. DOI: 10.1002/14651858.CD008487.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD008487.pub2/full[↩]
- Manheimer E, Cheng K, Wieland LS, Min LS, Shen X, Berman BM, Lao L. Acupuncture for treatment of irritable bowel syndrome. Cochrane Database of Systematic Reviews 2012, Issue 5. Art. No.: CD005111. DOI: 10.1002/14651858.CD005111.pub3. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD005111.pub3/full[↩]
- Wang Y, Zhishun L, Peng W, Zhao J, Liu B. Acupuncture for stress urinary incontinence in adults. Cochrane Database of Systematic Reviews 2013, Issue 7. Art. No.: CD009408. DOI: 10.1002/14651858.CD009408.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD009408.pub2/full[↩]
- Shen X, Xia J, Adams CE. Acupuncture for schizophrenia. Cochrane Database of Systematic Reviews 2014, Issue 10. Art. No.: CD005475. DOI: 10.1002/14651858.CD005475.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD005475.pub2/full[↩]
- Peng W, Wang Y, Zhang Y, Liang CM. Acupuncture for vascular dementia. Cochrane Database of Systematic Reviews 2007, Issue 2. Art. No.: CD004987. DOI: 10.1002/14651858.CD004987.pub2. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD004987.pub2/full[↩]
- MacPherson, H., Thomas, K., Walters, S., and Fitter, M. The York acupuncture safety study: prospective survey of 34000 treatments by traditional acupuncturists. BMJ. 2001; 323: 486–487. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC48134/[↩]





{kind=link}