
Contents
What to do for a bee sting
Bee stings are a common outdoor nuisance. In most cases, bee stings are just annoying, and home treatment is all that’s necessary to ease the pain of bee stings. But if you’re allergic to bee stings or you get stung numerous times, you may have a more-serious reaction that requires emergency treatment 1.
- Call your local emergency number and services if you’re having a serious reaction to a bee sting that suggests anaphylaxis, even if it’s just one or two signs or symptoms. If you were prescribed an emergency epinephrine autoinjector (EpiPen, Auvi-Q, others), use it right away as your doctor directed.
You can take several steps to avoid bee stings — as well as hornet and wasp stings — and find out how to treat them if you do get stung.
Symptoms of a Bee sting
Bee stings can produce different reactions, ranging from temporary pain and discomfort to a severe allergic reaction. Having one type of reaction doesn’t mean you’ll always have the same reaction every time you’re stung, or that the next reaction will necessarily be more severe.
Mild reaction
Most of the time, bee sting symptoms are minor and include:
- Instant, sharp burning pain at the sting site
- A red welt at the sting area
- Slight swelling around the sting area
In most people, the swelling and pain go away within a few hours.
Moderate reaction
Some people who get stung by a bee or other insect have a bit stronger reaction, with signs and symptoms such as:
- Extreme redness
- Swelling at the site of the sting that gradually enlarges over the next day or two
Moderate reactions tend to resolve over five to 10 days. Having a moderate reaction doesn’t mean you’ll have a severe allergic reaction the next time you’re stung. But some people develop similar moderate reactions each time they’re stung. If this happens to you, talk to your doctor about treatment and prevention, especially if the reaction becomes more severe each time.
Severe allergic reaction
A severe allergic reaction (anaphylaxis) to bee stings is potentially life-threatening and requires emergency treatment. A small percentage of people who are stung by a bee or other insect quickly develop anaphylaxis. Signs and symptoms of anaphylaxis include:
- Skin reactions, including hives and itching and flushed or pale skin
- Difficulty breathing
- Swelling of the throat and tongue
- A weak, rapid pulse
- Nausea, vomiting or diarrhea
- Dizziness or fainting
- Loss of consciousness
People who have a severe allergic reaction to a bee sting have a 30 to 60 percent chance of anaphylaxis the next time they’re stung. Talk to your doctor or an allergy specialist about prevention measures such as immunotherapy (“allergy shots”) to avoid a similar reaction in case you get stung again.
Multiple bee stings
Generally, insects such as bees and wasps aren’t aggressive and only sting in self-defense. In most cases, this results in one or perhaps a few stings. In some cases a person will disrupt a hive or swarm of bees and get multiple stings. Some types of bees — such as Africanized honeybees — are more likely than are other bees to swarm, stinging in a group.
If you get stung more than a dozen times, the accumulation of venom may induce a toxic reaction and make you feel quite sick. Signs and symptoms include:
- Nausea, vomiting or diarrhea
- Headache
- A feeling of spinning (vertigo)
- Convulsions
- Fever
- Dizziness or fainting
Multiple stings can be a medical emergency in children, older adults, and people who have heart or breathing problems.
When to see a doctor
In most cases, bee stings don’t require a visit to your doctor. In more-severe cases, you’ll need immediate care – call your local emergency number.
Causes of bee sting
To sting, a bee jabs a barbed stinger into the skin. Bee sting venom contains proteins that affect skin cells and the immune system, causing pain and swelling around the sting area. In people with a bee sting allergy, bee venom can trigger a more-serious immune system reaction.
Risk factors for bee sting
You’re at increased risk of bee stings if:
- You live in an area where bees are especially active or with beehives nearby
- Your work or hobbies require spending time outside
You’re more likely to have an allergic reaction to bee stings if you’ve had an allergic reaction to a bee sting in the past, even if it was minor.
Adults tend to have more-severe reactions than children do and are more likely to die of anaphylaxis than children are.
Prevention of bee sting
The following tips can help reduce your risk of getting stung by bees:
- Take care when drinking sweet beverages outside. Wide, open cups may be your best option because you can see if a bee is in them. Inspect cans and straws before drinking from them.
- Tightly cover food containers and trash cans.
- Clear away garbage, fallen fruit, and dog or other animal feces (flies can attract wasps).
- Wear close-toed shoes when walking outside.
- Don’t wear bright colors or floral prints, which can attract bees.
- Don’t wear loose clothing, which can trap bees between the cloth and your skin.
- When driving, keep your windows rolled up.
- Be careful when mowing the lawn or trimming vegetation, activities that might arouse insects in a beehive or wasp nest.
- Have hives and nests near your home removed by a professional.
Know what to do when you’re exposed to bees:
- If a few bees are flying around you, stay calm and slowly walk away from the area. Swatting at an insect may cause it to sting.
- If a bee or wasp stings you, or many insects start to fly around, cover your mouth and nose and quickly leave the area. When a bee stings, it releases a chemical that attracts other bees. If you can, get into a building or closed vehicle.
Diagnosis of bee sting
If you’ve had a reaction to bee stings that suggests you might be allergic to bee venom, your doctor may suggest one or both of the following tests:
- Skin test. During skin testing, a small amount of allergen extract (in this case, bee venom) is injected into the skin of your arm or upper back. This test is safe and won’t cause any serious reactions. If you’re allergic to bee stings, you’ll develop a raised bump on your skin at the test site.
- Allergy blood test. A blood test can measure your immune system’s response to bee venom by measuring the amount of allergy-causing antibodies in your bloodstream. A blood sample is sent to a medical laboratory, where it can be tested for evidence of sensitivity to possible allergens.
Allergy skin tests and allergy blood tests are often used together to diagnose insect allergies. Your doctor may also want to test you for allergies to yellow jackets, hornets and wasps — which can cause allergic reactions similar to those of bee stings.
Treatment of bee sting
For ordinary bee stings that do not cause an allergic reaction, home treatment is enough. Multiple stings or an allergic reaction, on the other hand, can be a medical emergency that requires immediate treatment.
Emergency treatment for allergic reactions
- During an anaphylactic attack, an emergency medical team may perform cardiopulmonary resuscitation (CPR) if you stop breathing or your heart stops beating.
You may be given medications including:
- Epinephrine (adrenaline) to reduce your body’s allergic response
- Oxygen, to help you breathe
- Intravenous (IV) antihistamines and cortisone to reduce inflammation of your air passages and improve breathing
- A beta agonist (such as albuterol) to relieve breathing symptoms
Epinephrine autoinjector
If you’re allergic to bee stings, your doctor is likely to prescribe an emergency epinephrine autoinjector (EpiPen, Auvi-Q, others). You’ll need to have it with you at all times. An autoinjector is a combined syringe and concealed needle that injects a single dose of medication when pressed against your thigh. Always be sure to replace epinephrine by its expiration date.
Be sure you know how to use the autoinjector. Also, make sure the people closest to you know how to administer the drug — if they’re with you in an anaphylactic emergency, they could save your life. Medical personnel called in to respond to a severe anaphylactic reaction also may give you an epinephrine injection or another medication.
Consider wearing an alert bracelet that identifies your allergy to bee or other insect stings.
Allergy shots
Bee and other insect stings are a common cause of anaphylaxis. If you’ve had a serious reaction to a bee sting or multiple stings, your doctor likely will refer you to an allergist for allergy testing and consideration of allergy shots (immunotherapy). These shots, generally given regularly for a few years, can reduce or eliminate your allergic response to bee venom.
Home remedies for bee sting
If a bee stings you or your child, follow the suggestions below.
Treatment for minor reactions
- Remove the stinger as soon as you can, as it takes only seconds for all of the venom to enter your body. Get the stinger out any way you can, such as with your fingernails or a tweezer.
- Wash the sting area with soap and water.
- Apply a cold compress.
Treatment for moderate reactions
The following steps may help ease the swelling and itching often associated with large local reactions:
- Remove the stinger as soon as you can.
- Wash the affected area with soap and water.
- Apply a cold compress.
- Take an over-the-counter pain reliever as needed. You might try ibuprofen (Motrin IB, Children’s Motrin, others) to help ease discomfort.
- If the sting is on an arm or leg, elevate it.
- Apply hydrocortisone cream or calamine lotion to ease redness, itching or swelling.
- If itching or swelling is bothersome, take an oral antihistamine that contains diphenhydramine (Benadryl) or chlorpheniramine (Chlor-Trimeton).
- Avoid scratching the sting area. This will worsen itching and swelling and increase your risk of infection.
What is Anaphylaxis ?
Anaphylaxis is a life-threatening, systemic hypersensitivity reaction that may be caused by both immunological and nonimmunological mechanisms. Most reactions are immunoglobulin (IgE) mediated 2. It is the most severe form of allergic reaction and is almost always unexpected 3. Delay in clinical diagnosis and treatment may result in death by airway obstruction or vascular collapse 2. The incidence of anaphylaxis in the United States is 49.8 cases per 100,000 person-years 3. Lifetime prevalence is 0.05 to 2 percent, with a mortality rate of 1 percent 4. Compared with that of the general population, the risk of anaphylaxis is doubled in patients with mild asthma and tripled in those with severe disease 5. The true prevalence and mortality rates may be higher because of the unexpected nature of the disease, the lack of reliable confirmatory testing, confusion over the clinical definition, and underreporting by physicians 6. Patients may arrive at a physician’s office remote from an event or with active symptoms, or they may develop anaphylaxis after administration of common treatments used in the clinic. Patients need to be prepared to recognize and quickly treat anaphylaxis to prevent potentially catastrophic outcomes 7.
Triggers and Causes of Anaphylaxis
Anaphylaxis is a systemic response to a specific allergen, usually occurring within one hour of exposure. The most common triggers are food, insect stings, and medications (Table 1) 7. Food-related reactions are most common in children up to four years of age, and medication reactions are most common in patients older than 55 years 3.
Table 1. Possible Triggers of Anaphylaxis
| Allergy testing and allergy-specific immunotherapy |
| Animal dander |
| Foods |
| Egg, fish, food additives, milk, peanuts, sesame, shellfish, tree nuts |
| Idiopathic anaphylaxis (always a diagnosis of exclusion; consider unrecognized allergen or mastocytosis) |
| Insect venom |
| Stinging insects from the Hymenoptera order (e.g., bee, wasp, fire ants) |
| Latex and other occupational allergens |
| Medications |
| Allopurinol (Zyloprim), angiotensin-converting enzyme inhibitors, antibiotics (beta-lactams most common), aspirin, biologic modifiers (e.g., interferon), nonsteroidal anti-inflammatory drugs, opioids |
| Physical factors (very rare) |
| Cold, heat, exercise, sunlight |
| Radiocontrast media |
Most cases of anaphylaxis are immunoglobulin E (IgE)–mediated. Antibodies exposed to a particular allergen attach to mast cells and basophils, resulting in their activation and degranulation. A variety of chemical mediators are released including histamine, heparin, tryptase, kallikrein, platelet-activating factor, bradykinin, tumor necrosis factor, nitrous oxide, and several types of interleukins 7, 6.
Historically, anaphylaxis-type reactions triggered by the direct activation of the mast cell (e.g., radiocontrast media reactions) were referred to as anaphylactoid reactions. Currently, immune and nonimmune anaphylaxis are the preferred terms to differentiate between IgE-mediated reactions and direct activation reactions. This distinction matters little in the acute clinical setting, because the treatment is the same for both types of reactions. However, the difference is important when deciding on prevention strategies, such as immunomodulation therapy 7, 6.
Signs and symptoms of anaphylaxis
Signs and symptoms usually develop within five to 30 minutes of exposure to the offending allergen, but may not develop for several hours. A biphasic reaction is a second acute anaphylactic reaction occurring hours after the first response and without further exposure to the allergen 8. One to 20 percent of patients with anaphylaxis experience biphasic reactions, which usually occur within eight hours of the initial reaction, but may occur as late as 24 to 72 hours after exposure 9.
Typical reactions with skin manifestations (urticaria) plus cardiovascular or respiratory involvement are easily diagnosed. However, some reactions are atypical and recognised only when the diagnosis is considered because of the context. A sudden onset of symptoms affecting two or more organ systems or just hypotension on its own, even without skin involvement, should trigger consideration of the diagnosis in the right context, ie. recent exposure to a potential allergen or stimulant. Hypotension may be absolute (systolic <90 mmHg) or relative – defined as a greater than 30% drop from baseline/normal for that patient 10.
Anaphylaxis must be considered as a possible cause in any case of acute respiratory distress, bronchospasm, hypotension and/or cardiac arrest. Some real-life examples of difficult to diagnose anaphylaxis are provided in Table 2. A common theme in these examples is the subtlety or absence of skin features. Some other pointers to consider are:
Table 2. Signs and symptoms of Anaphylaxis by Body System
| Dermatologic/mucosal |
| Eyes: periorbital swelling/erythema, injected conjunctiva, tears |
| Oral mucosa: angioedema of the tongue and lips |
| Skin: urticarial rash, pruritus or flushing, morbilliform rash, piloerection, angioedema |
| Respiratory |
| Lower airway: bronchospasm with wheezing or cough, chest tightness, tachypnea, decreased peak expiratory flow, cyanosis, respiratory collapse/arrest |
| Upper airway: sensation of throat constriction; dry cough; difficulty breathing, swallowing, speaking; changes in voice; stridor; cyanosis; respiratory collapse/arrest |
| Cardiovascular |
| Early: tachycardia, diaphoresis, delayed capillary refill, hypotension |
| Late: bradycardia, shock, T-wave inversion and ST depression in multiple leads, cyanosis, cardiac arrest |
| Gastrointestinal |
| Nausea, vomiting, diarrhea, abdominal cramps |
| Neurologic |
| Throbbing headache, dizziness, lightheadedness, confusion, tunnel vision, loss of consciousness |
| General |
| Anxiety, feeling of impending doom, metallic taste, paresthesia in extremities, malaise, weakness |
| In children: sudden behavior changes, irritability, cessation of play |
Note: Manifestations are listed in order of clinical importance/frequency.
[Source 11]Skin involvement, predominantly urticaria and angioedema, occurs in 90 percent of episodes. Respiratory manifestations are present in 70 percent of episodes, primarily with signs and symptoms of upper airway obstruction. Lower airway obstruction may occur, especially in patients with a history of asthma. Cardiovascular involvement, which could lead to life-threatening hypotension, occurs in 45 percent of patients. Gastrointestinal and neurologic involvement occur 45 and 15 percent of the time, respectively.
In 2004, the Second Symposium on the Definition and Management of Anaphylaxis developed clinical criteria for diagnosing anaphylaxis in the acute setting (Table 3) 12. The presence of one of three criteria predicts diagnosis of anaphylaxis 95 percent of the time 4. The clinical history is the most important tool to determine whether a patient has had an anaphylactic reaction and the cause of the episode 2.
Table 3. Clinical Criteria for Diagnosing Anaphylaxis
| Anaphylaxis is highly likely when any one of the following three sets of criteria is fulfilled: |
|---|
| 1. Acute onset of an illness (minutes to several hours) with involvement of the skin, mucosal tissue, or both (e.g., generalized hives; pruritus or flushing; swollen lips, tongue, or uvula), and at least one of the following: |
| Respiratory compromise (e.g., dyspnea, wheeze-bronchospasm, stridor, reduced peak expiratory flow, hypoxemia) |
| Reduced blood pressure or associated symptoms of end-organ dysfunction (e.g., hypotonia [collapse], syncope, incontinence) |
| 2. Two or more of the following that occur rapidly (minutes to several hours) after exposure to a likely allergen for that patient: |
| Involvement of the skin, mucosal tissue, or both (e.g., generalized hives; pruritus or flushing; swollen lips, tongue, or uvula) |
| Respiratory compromise (e.g., dyspnea, wheeze-bronchospasm, stridor, reduced peak expiratory flow, hypoxemia) |
| Reduced blood pressure or associated symptoms (e.g., hypotonia [collapse], syncope, incontinence) |
| Persistent gastrointestinal symptoms (e.g., abdominal cramps, vomiting) |
| 3. Reduced blood pressure that occurs rapidly (minutes to several hours) after exposure to a known allergen for that patient. |
| Infants and children: low systolic blood pressure (age-specific)* or a more than 30 percent decrease in systolic blood pressure |
| Adults: systolic blood pressure of less than 90 mm Hg or a more than 30 percent decrease from that person’s baseline |
*—Defined as less than 70 mm Hg in children one month to one year of age; less than 70 mm Hg + (2 × age) in children one to 10 years of age; and less than 90 mm Hg in those 11 to 17 years of age.
[Source 13]Management of Acute Anaphylaxis
In the management of anaphylaxis, administering intramuscular epinephrine and ensuring proper oxygenation and effective circulation are key.3 A suggested protocol is listed in Table 4. Performing a primary survey and providing supportive care for the patient’s airway, breathing, and circulation (with administration of epinephrine) are the critical initial steps. Patients should have easy access to commercially made, nonexpired epinephrine autoinjectors, which are preferred for delivering this therapy.
Table 4. Initial management of anaphylaxis
| 1. Stop exposure to allergen (if possible), assess severity and treat |
If the patient is hypotensive:
|
| 2. If there is inadequate response, an immediate lifethreatening situation or deterioration |
|
| 3. Disposition |
| All patients should be transferred by ambulance to an emergency department with monitoring and resuscitation capability for a minimum 4–6 hours observation |
Figure 1. Provides step-by-step instructions on how to use the current Epipen
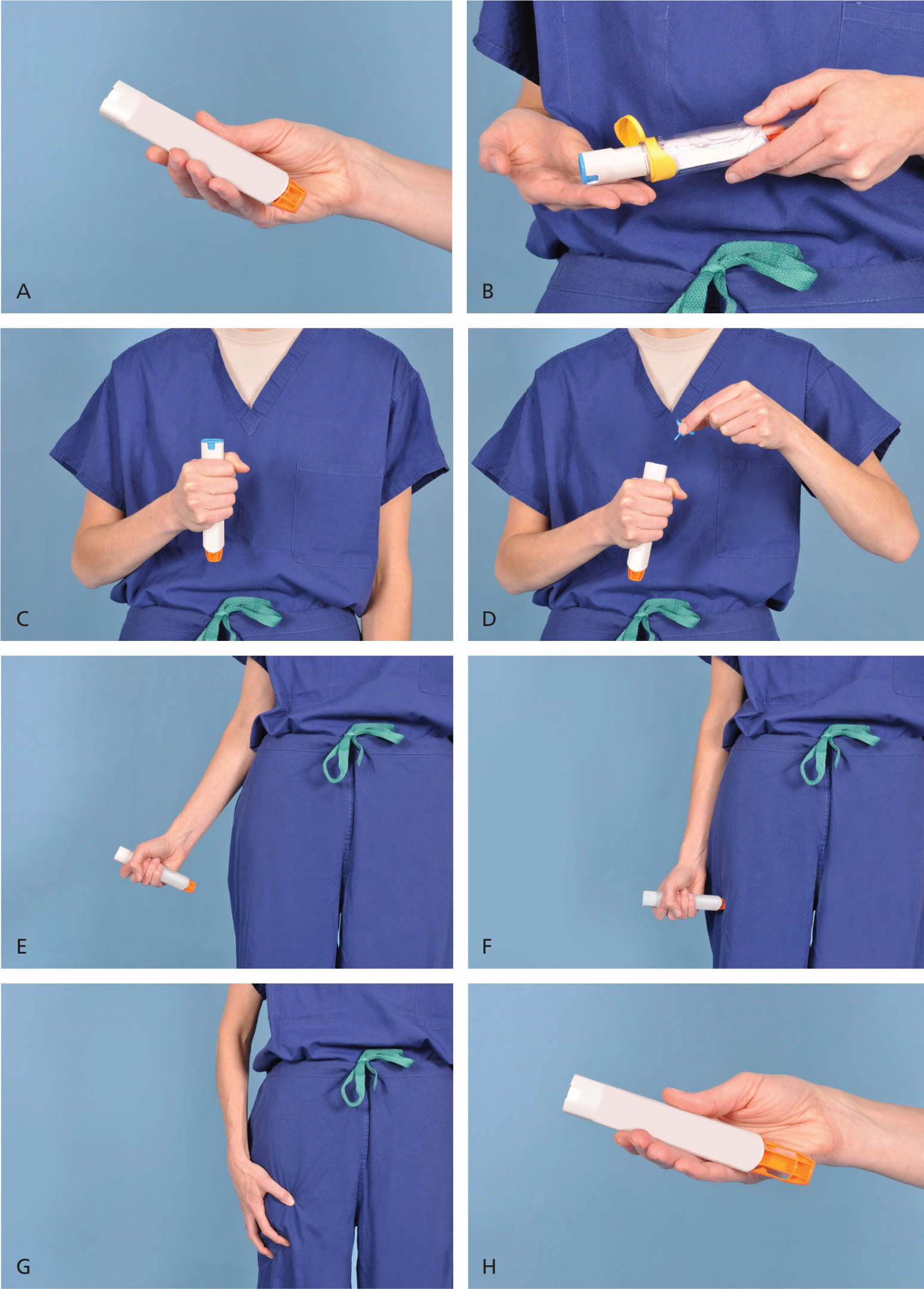
Figure 1. How To Use Epipen
Demonstration of appropriate deployment of the (A) Epipen (released in 2008). For demonstration purposes, a trainer device is being used instead of a live device; however, the coloring of key components is the same as the actual adult device. (B) Open the yellow cap of the carrying case and remove the device from its storage tube (the Epipen Jr. has a green cap). (C) Grasp and form a fist around the unit with the orange tip facing down. (D) With the other hand, remove the blue safety release. (E) Aim the orange tip toward the outer thigh. (F) Swing the arm and jab the device firmly into the outer thigh, at a 90-degree angle, until the device clicks. The needle will deploy at this time into thigh (the autoinjector is designed to work through clothing). Hold the device firmly against the thigh for 10 seconds, so the entire dose will be delivered. (G) Remove the device from the thigh and massage the injection area for 10 seconds. (H) The safety feature of the device, extension of the orange tip that locks into place, will completely cover the needle immediately after use. The used device should be taken to the hospital emergency department with the patient for disposal.
Laboratory Testing for Anaphylaxis
Anaphylaxis is a clinical diagnosis. The value of confirmatory blood testing is limited 14. Two tests that have been evaluated for use in the acute setting are serum histamine and tryptase levels; elevations from baseline levels may be helpful in confirming anaphylaxis 14. Histamine levels must be obtained within one hour of symptom onset, and samples require special handling because histamine breaks down with any movement. Tryptase levels do not increase until 30 minutes after the onset of symptoms and peak at one to two hours; therefore, serial levels are sampled on presentation, one to two hours after presentation, and 24 hours after presentation to assess for a return to baseline 14.
Allergen skin testing and in vitro assay for serum IgE of specific allergens do not reliably predict who will develop anaphylaxis. Allergen testing identifies sensitivity to an allergen, but not whether the patient will have a systemic reaction. Testing is more helpful after an episode of anaphylaxis to identify which allergen most likely caused the reaction and to promote future avoidance.
Postacute care
Referral to a clinical immunologist or allergist can assist with investigation and implementation of a comprehensive management plan. The use of subcutaneous immunotherapy with the relevant insect venom(s) is useful for stinging insect allergy18,19 and in special cases of medicine allergy, medicine desensitisation can also be employed if there is no alternative class of drug that can be used. Patients who experience an initial attack that is severe or refractory to treatment and those with comorbidities may benefit the most from referral.
- Bee sting. https://www.mayoclinic.org/diseases-conditions/bee-stings/symptoms-causes/syc-20353869[↩]
- Joint Task Force on Practice Parameters; American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma, and Immunology; Joint Council on Allergy, Asthma and Immunology. The diagnosis and management of anaphylaxis: an updated practice parameter [published correction appears in J Allergy Clin Immunol. 2008;122(1):68]. J Allergy Clin Immunol. 2005;115(3 suppl 2):S483–S523.[↩][↩][↩]
- Tang ML, Osborne N, Allen K. Epidemiology of anaphylaxis. Curr Opin Allergy Clin Immunol. 2009;9(4):351–356.[↩][↩][↩]
- Kemp SF. Navigating the updated anaphylaxis parameters. Allergy Asthma Clin Immunol. 2007;3(2):40–49.[↩][↩]
- González-Pérez A, Aponte Z, Vidaurre CF, Rodríguez LA. Anaphylaxis epidemiology in patients with and patients without asthma: a United Kingdom database review. J Allergy Clin Immunol. 2010;125(5):1098–1104.[↩]
- Simons FE. Anaphylaxis [published correction appears in J Allergy Clin Immunol. 2010;126(4):885]. J Allergy Clin Immunol. 2010;125(2 suppl 2):S161–S181.[↩][↩][↩][↩]
- Ben-Shoshan M, Clark AE. Anaphylaxis: past, present and future. Allergy. 2011;66(1):1–14.[↩][↩][↩][↩][↩]
- Kemp SF. The post-anaphylaxis dilemma: how long is long enough to observe a patient after resolution of symptoms? Curr Allergy Asthma Rep. 2008;8(1):45–48.[↩]
- Oswalt ML, Kemp SF. Anaphylaxis: office management and prevention Immunol Allergy Clin North Am. 2007;27(2):177–191vi.[↩]
- Sampson HA. Anaphylaxis and emergency treatment. Pediatrics. 2003;111(6 pt 3):1601–1608.[↩]
- Anaphylaxis: Recognition and Management. Am Fam Physician. 2011 Nov 15;84(10):1111-1118. http://www.aafp.org/afp/2011/1115/p1111.html[↩]
- Sampson HA, Muñoz-Furlong A, Campbell RL, et al. Second Symposium on the Definition and Management of Anaphylaxis: summary report—second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network Symposium. Ann Emerg Med. 2006;47(4):373–380.[↩]
- Sampson HA, Muñoz-Furlong A, Campbell RL, et al. Second Symposium on the Definition and Management of Anaphylaxis: summary report—second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network Symposium. Ann Emerg Med. 2006;47(4):374.[↩]
- Stone SF, Cotterell C, Isbister GK, Holdgate A, Brown SG; Emergency Department Anaphylaxis Investigators. Elevated serum cytokines during human anaphylaxis: identification of potential mediators of acute allergic reactions J Allergy Clin Immunol. 2009;124(4):786–792e4.[↩][↩][↩]





{kind=link}