
Contents
- Age related hypogonadism
- Age related hypogonadism causes
- Age related hypogonadism signs and symptoms
- Age related hypogonadism diagnosis
- Age related hypogonadism treatment
Age-related hypogonadism also called “age related low testosterone”, “age-associated testosterone decline” or “late-onset hypogonadism” is a male age-related decline in testosterone production giving rise to a spectrum of symptoms such as low sex drive (loss of libido), erectile dysfunction, loss of muscle mass, increased body fat, anemia (low red blood cells), reduced bone density (osteoporosis), depressed mood, decreased vitality, sweating, and hot flushes 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11. Some authors called it “a combined form of primary and secondary hypogonadism” 12, 13. Age-related hypogonadism can significantly impact the quality of life and organ function in older men 14.
Testosterone is the major male sex hormone and is produced by the male testes in men and to a lesser extent by the adrenal glands in both men and women. In men, testosterone is thought to regulate sex drive (libido), bone mass, fat distribution, promotes gains in muscle mass and strength when combined with resistance training, the production of red blood cells and controlling fertility and the development of sperm (spermatogenesis) 15, 16. Testosterone also plays an important part in the development of ‘male sex characteristics’ such as a deeper voice and certain patterns of muscle development and hair growth. Testosterone helps bring on the physical changes that turn a boy into a man. This time of life is called puberty. Adolescent boys with too little testosterone may not experience normal masculinization. For example, the genitals may not enlarge, facial and body hair may be scant and the voice may not deepen normally. In women or anyone with ovaries, testosterone impacts overall growth as well as development of muscle and reproductive tissue. Testosterone is produced in the Leydig cells in the testis in men and to a lesser extent by the adrenal glands in both men and women 17. In males, the normal range for early morning testosterone is between 300 ng/dL to 1000 ng/dL but may vary from laboratory to laboratory 18, 19, 20.
Blood levels of testosterone peak in 20 to 30 year-old males and then decline with age with average rate of decline of 1.6% per year 21, 22, 23, 24, 25, 26, 27. One study found that serum testosterone levels were below the normal range in 20% of men in their 60s and in close to 50% of men in their 80s 24. However, the prevalence of symptomatic low testosterone (hypogonadism) is estimated by some to be much lower in this population, at about 2% 28. Longitudinal studies demonstrated a gradual decline in total serum testosterone levels in men from the age of 40, with 20% and 30% of men meeting age-related hypogonadism criteria in their 60s and 70s 29, 30.
Testosterone in the blood can be either bound or free:
- Bound testosterone is attached to proteins such as sex-hormone-binding-globulin (SHBG) and albumin. Most testosterone (approximately 60–70%) is transported in the blood to target tissues bound to sex hormone-binding globulin (SHBG), which in men is also called testosterone-binding globulin. About 30–40% of testosterone is loosely bound to albumin. This majority supply of protein-bound testosterone acts as a surplus of testosterone hormone for the body 31.
- Free testosterone, the active form, is all the remaining testosterone that is not bound to other substances. The small amounts of free testosterone (approximately 0.5–2%) in the blood act at the level of the tissues, primarily the seminal vesicles, bone, muscle, and prostate gland 31.
Historically, only free testosterone was thought to be the biologically active component. However, testosterone is weakly bound to serum albumin and dissociates freely in the capillary bed, thereby becoming readily available for tissue uptake. All non-SHBG-bound testosterone is therefore considered bioavailable.
Low testosterone levels in men is defined as total testosterone < 350 ng/dL and free testosterone < 225 pmol/L and are associated with sexual dysfunction such as low sexual desire (low libido), erectile dysfunction (fewer or diminished spontaneous erections, decreased nocturnal penile tumescence), reduced skeletal muscle mass and strength, decreased bone mineral density, sparse beard growth, shrinking testes, increased cardiovascular risk and alterations of the glycometabolic profile 32, 18, 33, 34, 35. The European Urological Association recommends a total testosterone level < 300 ng/dL as the diagnosis of hypogonadism 36, the American Urological Association considers 3.5 ng/mL (12 nmol/L) total testosterone represents a reliable threshold to diagnose age-related hypogonadism 37, and the Endocrine Society recommends the reasonable cut-off of total testosterone in men as 264 ng/dL (9.2 nmol/L) 38. This variation total testosterone level diagnostic criteria underscores the lack of uniformity in defining age-related low testosterone across different medical governing bodies. Total testosterone 12 nmol/L (3.5 ng/mL) represents a reliable threshold to diagnose age-related hypogonadism 7. Calculated free-testosterone of < 220 pmol/L has been suggested as a possible cut-off to diagnose age-related hypogonadism 7.
The mainstay of age-related hypogonadism diagnosis includes signs and symptoms consistent with hypogonadism, coupled with biochemical evidence of low morning serum total testosterone levels on two or more occasions, measured with a reliable assay and in fasting conditions. Testosterone levels are also potentially influenced by food intake 39; therefore, serum total testosterone should be measured in fasting conditions in the morning (between 7AM and 11AM). A confirmatory measurement should always be undertaken in the case of a abnormal value, and before starting any testosterone therapy.
In clinical conditions that may interfere with sex hormone-binding globulin (SHBG) levels, evaluation of free testosterone should be considered to better estimate actual androgen levels. Unfortunately, despite free testosterone potential clinical value 40, no validated thresholds for free testosterone are available from clinical studies and this represents an area of uncertainty; however, data from the European Male Aging Study indicated that free testosterone levels < 220 pmol/L (6.4 ng/dL) increased the likelihood to correct identify hypogonadism as compared with total testosterone level alone, particularly when total testosterone levels are between 8.0 and 11 nmol per liter 41, 42, 28.
The incidence of low testosterone in the United States is reported to be approximately 20% in men older than 60 years of age with 30% in those older than 70 years of age and 50% in those older than 80 years 24, although the prevalence of syndromic low testosterone defined as at least 3 sexual symptoms with a total testosterone level < 320 ng/dL (<11.1 nmol/L) is lower 28.
However, uncertainty exists as to whether nonspecific signs and symptoms associated with age-related low testosterone, such as sexual dysfunction, decreases in energy and muscle mass, mood disturbances, changes in bone mineral density, cardiovascular disease, depression, decreased libido, erectile dysfunction, decreased volume of ejaculate, loss of body and facial hair, weakness, and mortality, are a consequence of age-related low testosterone or whether they are a result of other factors, such as chronic illnesses or concomitant medications 43, 44, 45, 46, 47. Given the high prevalence of low testosterone and more limited correlation of low testosterone with symptoms in aging men, it is uncertain to what extent does low testosterone represents a physiologic or pathologic event 22, 24. Furthermore, symptoms typically associated with low testosterone are less specific in older men and may be caused by other diseases or medical conditions. For example, erectile dysfunction can be the result of vascular insufficiency, neurologic impairment, psychogenic causes or substance use 48. Conditions such as diabetes and atherosclerosis are more common in older men, with up to 40% of men over 50 years of age having evidence of vascular insufficiency as the primary cause of their erectile dysfunction 49. Low libido similarly can result from psychiatric or medical conditions that are more common in older men 50.
The role of testosterone treatment in managing age-related low testosterone is controversial 51. The U.S. Food and Drug Administration (FDA) requires the pharmaceutical industry to label all testosterone medications to clearly state that their products are approved for use only in persons with low testosterone levels due to known causes and the FDA cautions about using testosterone products for low testosterone due to aging; requiring labeling change to inform of possible increased risk of heart attack and stroke with testosterone use 52, 44.
The American College of Physicians (ACP) recently issued new guidelines on prescribing supplemental testosterone for men with age-related low testosterone 51:
- The American College of Physicians suggests that clinicians discuss whether to initiate testosterone treatment in men with age-related low testosterone with sexual dysfunction who want to improve sexual function (conditional recommendation; low-certainty evidence). The discussion should include the potential benefits, harms, costs, and patient’s preferences.
- The American College of Physicians suggests that clinicians should reevaluate symptoms within 12 months and periodically thereafter. Clinicians should discontinue testosterone treatment in men with age-related low testosterone with sexual dysfunction in whom there is no improvement in sexual function (conditional recommendation; low-certainty evidence).
- The American College of Physicians suggests that clinicians consider intramuscular rather than transdermal formulations when initiating testosterone treatment to improve sexual function in men with age-related low testosterone, as costs are considerably lower for the intramuscular formulation and clinical effectiveness and harms are similar.
- The evidence shows that men with age-related low testosterone may experience slight improvements in sexual function by 35% and erectile dysfunction by 27% if prescribed supplemental testosterone.
- The evidence does not support prescribing testosterone for men with concerns about energy, vitality, physical function, or cognition.
- The new guidelines point out that treating with supplemental testosterone is not risk free. Potential risks include blood clots, stroke, sleep apnea, acne and possibly enlarged breasts (gynecomastia). Men with these or other conditions may be advised against using supplemental testosterone even for sexual dysfunction.
- If men are treated with supplemental testosterone for sexual dysfunction, the decision to continue to treat should be reevaluated after a year and then periodically after that. Treatment should be stopped if sexual dysfunction doesn’t improve, according to the new guidelines.
Data from meta-analyses have shown that testosterone replacement therapy is ineffective when baseline testosterone levels are > 3.5 ng/mL (>12 nmol/L). Positive outcomes are documented when testosterone levels are < 3.5 ng/mL (<12 nmol/L), being higher in symptomatic patients with more severe forms of hypogonadism (< 8 nmol/L). Hence, 3.5 ng/mL (12 nmol/L) should be considered as a possible threshold for starting testosterone therapy in the presence of hypogonadal symptoms 56, 57.
You should not receive testosterone therapy if you have:
- Prostate or breast cancer (or suspected)
- Enlarged prostate causing difficulty with urination
- Elevated prostate specific antigen (PSA) levels
- High number of red blood cells
- Untreated sleep apnea (obstructed breathing during sleep)
- Planning to have children
- Heart attack or stroke within the last 6 months
- Blood clots
Possible risks of testosterone treatment include:
- Decreased sperm production
- A high red blood cell count
- Acne
- An increase in prostate size
- Sleep apnea—the occasional stopping of breathing during sleep (rarely)
You should discuss with your doctor how to monitor for prostate cancer and other risks to your prostate. Men with known or suspected prostate or breast cancer should not receive testosterone therapy. You should also talk to your doctor about the risks of testosterone therapy if you have, or are at risk for, heart disease or stroke. In addition, if you are planning fertility, you should not use testosterone therapy.
Figure 1. Age-related hypogonadism diagnostic algorithm
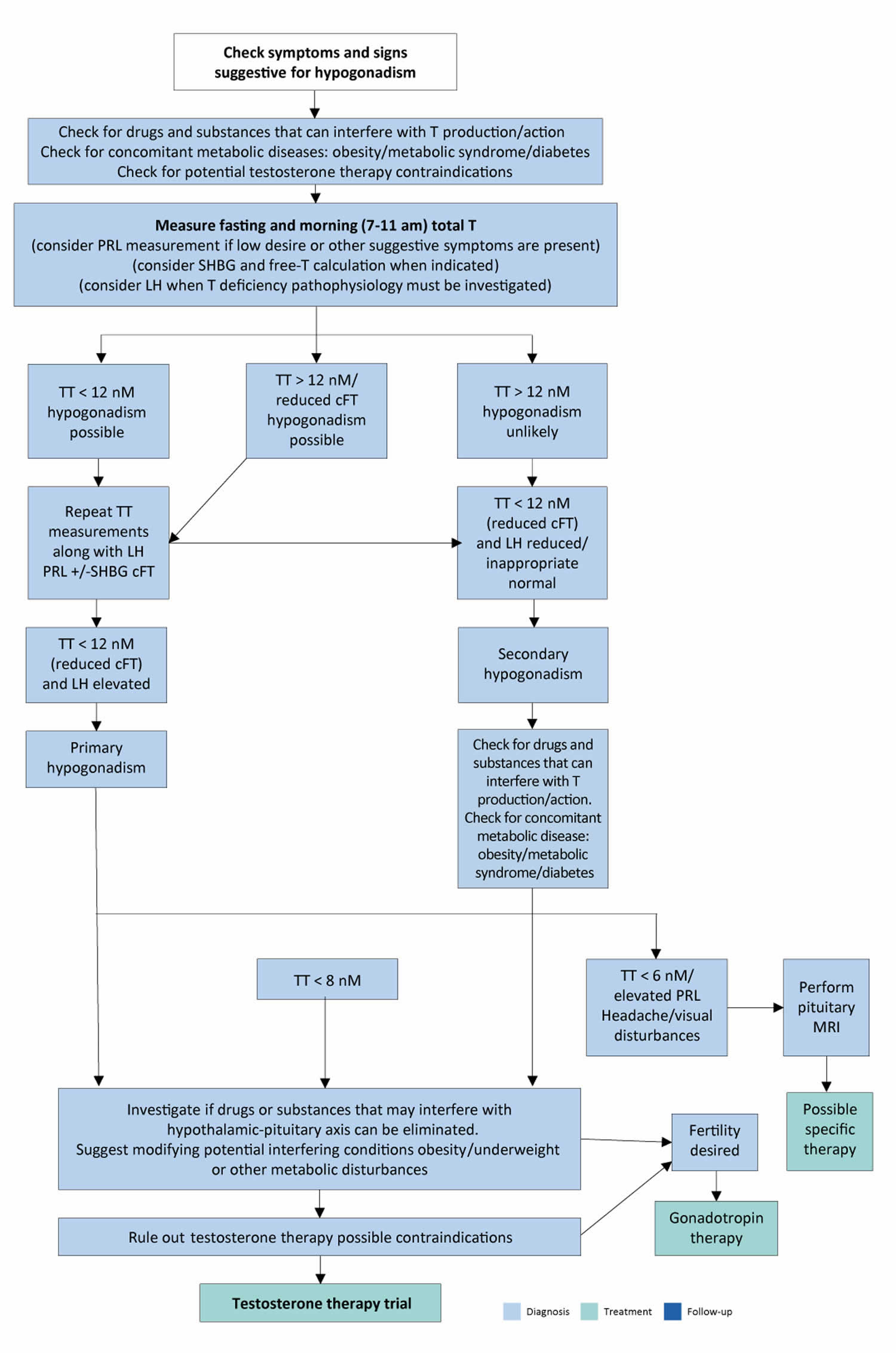
Abbreviations: TT = total testosterone; cFT = calculated free testosterone; PRL = prolactin; SHBG = sex hormone-binding globulin; LH = luteinising hormone; MRI = Magnetic resonance imaging.
[Source 7 ]As men age, there’s a slow, progressive decrease in testosterone or “T” production. Blood levels of testosterone peak in 20 to 30 year-old males and then decline with age with average rate of decline of 1.6% per year 21, 22, 23, 24, 25, 26, 27. One study found that serum testosterone levels were below the normal range in 20% of men in their 60s and in close to 50% of men in their 80s 24. However, the prevalence of symptomatic low testosterone (hypogonadism) is estimated by some to be much lower in this population, at about 2% 28. Longitudinal studies demonstrated a gradual decline in total serum testosterone levels in men from the age of 40, with 20% and 30% of men meeting age-related hypogonadism criteria in their 60s and 70s 29, 30.
Risk factors for hypogonadism include:
- HIV/AIDS. HIV/AIDS can cause low levels of testosterone by affecting the hypothalamus, the pituitary and the testes.
- Medications. The use of certain drugs, such as opiate pain medications and some hormones, can affect testosterone production.
- Previous chemotherapy or radiation therapy. Chemotherapy or radiation therapy for the treatment of cancer can interfere with testosterone and sperm production. The effects of both treatments often are temporary, but permanent infertility may occur. Although many men regain their fertility within a few months after treatment, preserving sperm before starting cancer therapy is an option for men.
- Obesity. Being significantly overweight at any age might be linked to hypogonadism.
- Undescended testicles (cryptorchidism). Before birth, the testicles develop inside the abdomen and normally move down into their permanent place in the scrotum. Sometimes one or both of the testicles aren’t descended at birth. This condition often corrects itself within the first few years of life without treatment. If not corrected in early childhood, it can lead to malfunction of the testicles and reduced production of testosterone.
- Mumps orchitis. A mumps infection involving the testicles that occurs during adolescence or adulthood can damage the testicles, affecting the function of the testicles and testosterone production.
- Hemochromatosis. Too much iron in the blood can cause testicular failure or pituitary gland dysfunction, affecting testosterone production.
Injury to the testicles. Because they’re outside the abdomen, the testicles are prone to injury. Damage to both testicles can cause hypogonadism. Damage to one testicle might not impair total testosterone production. - Malnutrition or nutritional deficiencies.
- Pituitary disorders. An abnormality in the pituitary gland can impair the release of hormones from the pituitary gland to the testicles, affecting normal testosterone production. A pituitary tumor or other type of brain tumor located near the pituitary gland may cause testosterone or other hormone deficiencies. Also, treatment for a brain tumor, such as surgery or radiation therapy, can affect the pituitary gland and cause hypogonadism.
- Inflammatory disease. Certain inflammatory diseases, such as sarcoidosis, histiocytosis and tuberculosis, involve the hypothalamus and pituitary gland and can affect testosterone production.
- Kallmann’s syndrome. This is an abnormal development of the area of the brain that controls the secretion of pituitary hormones (hypothalamus). This abnormality can also affect the ability to smell (anosmia) and cause red-green color blindness.
- Klinefelter syndrome. Klinefelter syndrome results from a congenital abnormality of the sex chromosomes, X and Y. A male normally has one X and one Y chromosome. In Klinefelter syndrome, two or more X chromosomes are present in addition to one Y chromosome. The Y chromosome contains the genetic material that determines the sex of a child and related development. The extra X chromosome that occurs in Klinefelter syndrome causes abnormal development of the testicles, which in turn results in underproduction of testosterone.
Hypogonadism can be inherited. If any of these risk factors are in your family health history, tell your doctor.
Sexual symptoms such as reduced sex drive or a drop in libido, erectile dysfunction and decreased spontaneous or morning erections are the most specific symptoms associated with age-related hypogonadism.
Early signs and symptoms of male hypogonadism might include:
- Decreased sex drive
- Reduced energy
- Depression
Over time, men with hypogonadism can develop:
- Erectile dysfunction (ED — inability to get or keep an erection) and loss of spontaneous erections
- Lowered sperm count and infertility (inability to have children)
- Decrease in hair growth on the face and body
- Decrease in muscle mass
- Development of breast tissue (gynecomastia) or breast tenderness
- Loss of bone mass (osteoporosis)
Severe hypogonadism can also cause mental and emotional changes. As testosterone decreases, some men have symptoms similar to those of menopause in women. These can include:
- Difficulty concentrating
- Increased irritability, and depressed mood
- Hot flashes (when testosterone levels are very low)
Over time, low testosterone may cause a man to lose body hair, muscle bulk, cause weak bones (osteoporosis), low red blood cells and smaller testes. Signs and symptoms (what you see and feel) vary from person to person.
| Sexual symptoms | Physical symptoms | Psychological symptoms | |
|---|---|---|---|
| More specific | Reduced libido Erectile dysfunction Decreased spontaneous/morning erections | Decreased vigorous activity Difficulty walking > 1 km Decreased bending | Low mood/mood deflection Decreased motivation Fatigue |
| Less specific | Reduced frequency of sexual intercourse Reduced frequency of masturbation Delayed ejaculation | Hot flushes Decreased energy Decreased physical strength/function/ activity | Concentration difficulties Sleep disturbances |
Diagnosis of age-related hypogonadism or low testosterone related to aging typically involves a medical history, a physical exam, and blood tests that measure testosterone levels. The blood for the test is usually drawn in the morning because testosterone levels fluctuate during the day but are highest in the morning. Testing may be done on two different days and in fasting conditions to confirm the hormone levels.
Medical History
Specific symptoms associated with hypogonadism, including age-related hypogonadism, are shown in Table 1. These symptoms are non-specific and need to be recorded and taken in context with the clinical and biochemical state. Several self-reported questionnaires or structural interviews have been developed for screening of hypogonadism. Although these case-history tools have demonstrated clinical utility in supporting the biochemical diagnosis of hypogonadism, or in the assessment of testosterone therapy outcomes, their specificity remains poor and they should not be used for a systematic screening of hypogonadal men 58. Headache and/or visual disturbance may indicate a pituitary-related disorder. History of surgical intervention for undescended testicle (cryptorchidism) or hypospadias (a condition in which the urethral opening of the penis is on the underside rather than at the tip) must be taken into account as possible signs of congenital defects. Chronic and systemic diseases or medical conditions must be comprehensively investigated in every patient. Use of drugs that potentially interfere with the hypothalamic-pituitary-gonadal axis (HPG axis) should be excluded. Acute diseases are associated with development of functional hypogonadism and determination of serum total testosterone levels should be avoided in these conditions; however, the role of testosterone in the case of acute illness remains to be clarified 59, 60, 61. Fertility issues should be always discussed.
Physical Examination
Since obesity is frequently associated with hypogonadism (mostly functional), the determination of body mass index (BMI) and the measurement of waist circumference are strongly recommended in all individuals. Testicular and penile size, as well as the presence of sexual secondary characteristics can provide useful information regarding overall androgen status. In addition, upper segment/lower segment ratio (n.v. > 0.92) and arm-span to height ratio (n.v. < 1.0) can be useful to identify a eunuchoid body shape, especially in subjects with pre-pubertal hypogonadism or delayed puberty. Finally, digital rectal examination (DRE) should be performed in all subjects to exclude prostate abnormalities before testosterone therapy (any type) or to support suspicion of hypogonadism (in case of reduced volume) 62.
Laboratory tests
Testosterone levels are produced in a circadian variation being highest in the morning and lowest at night, which may persist in ageing men 63, 64. Testosterone levels are also potentially influenced by food intake 39. Therefore, serum total testosterone should be measured in fasting conditions in the morning (between 7 a.m. and 11 a.m.). Testosterone levels can also be temporarily lower due to too much exercise, poor nutrition, severe illness, and with certain medications. A confirmatory measurement should always be undertaken in the case of a abnormal value, and before starting any testosterone therapy.
Liquid Chromatography-Tandem Mass Spectrometry (LC-MS/MS) represents the most accurate method for sex steroid evaluation; however, standardised automated platform immuno-assays for total testosterone assessment demonstrate a good correlation with Liquid Chromatography-Tandem Mass Spectrometry (LC-MS/MS) 65. Available immuno-assays are not able to provide an accurate estimation of free testosterone; therefore, direct free testosterone evaluation with these methods is not recommended and should be avoided 66. Equilibrium dialysis is the most accurate method for total testosterone measurement and free testosterone calculation 67. Alternatively, free testosterone can be derived from specific mathematical calculations using total testosterone as derived by common immunoassays and taking into account serum sex hormone binding globulin (SHBG) and albumin levels 68.
Low testosterone levels in men is defined as total testosterone < 350 ng/dL and free testosterone < 225 pmol/L and are associated with sexual dysfunction such as low sexual desire (low libido), erectile dysfunction (fewer or diminished spontaneous erections, decreased nocturnal penile tumescence), reduced skeletal muscle mass and strength, decreased bone mineral density, sparse beard growth, shrinking testes, increased cardiovascular risk and alterations of the glycometabolic profile 32, 18, 33, 34, 35. The European Urological Association recommends a total testosterone level < 300 ng/dL as the diagnosis of hypogonadism 36, the American Urological Association considers 3.5 ng/mL (12 nmol/L) total testosterone represents a reliable threshold to diagnose age-related hypogonadism 37, and the Endocrine Society recommends the reasonable cut-off of total testosterone in men as 264 ng/dL (9.2 nmol/L) 38. This variation total testosterone level diagnostic criteria underscores the lack of uniformity in defining age-related low testosterone across different medical governing bodies.
Data from meta-analyses have shown that testosterone therapy is ineffective when baseline levels are > 3.5 ng/mL (>12 nmol/L). Positive outcomes are documented when testosterone levels are <3.5 ng/mL (<12 nmol/L), being higher in symptomatic patients with more severe forms of hypogonadism (< 8 nmol/L). Hence, 3.5 ng/mL (12 nmol/L) should be considered as a possible threshold for starting testosterone therapy in the presence of hypogonadal symptoms 56, 57.
In clinical conditions that may interfere with sex-hormone-binding-globulin (SHBG) levels, evaluation of free testosterone should be considered to better estimate actual androgen levels. Unfortunately, despite free testosterone potential clinical value 40, no validated thresholds for free testosterone are available from clinical studies and this represents an area of uncertainty; however, data from the European Male Aging Study indicated that free testosterone levels < 220 pmol/L (6.4 ng/dL) increased the likelihood to correct identify hypogonadism as compared with total testosterone level alone, particularly when total testosterone levels are between 8.0 and 11 nmol per liter 41, 42, 28.
The determination of luteinizing hormone (LH) must be performed along with prolactin (PRL) when pathological total testosterone levels are detected, in order to correctly define the underlying conditions and exclude possible organic causes. Follicle-stimulating hormone (FSH) determination can further support the diagnosis of primary or secondary hypogonadism 9, 69. Due to prolactin (PRL) negative influence on libido, prolactin (PRL) can also be considered as first-line screening in patients with reduced sexual desire. In addition, contrast-enhanced pituitary magnetic resonance imaging (MRI) scanning, as well as other pituitary hormone evaluations, is required in the presence of specific symptoms such as visual disturbances, headache and when hyperprolactinemia is confirmed 70, 71. Limited evidence suggests also performing pituitary MRI in the case of severe hypogonadism (< 6 nmol/L, 1.75 ng/mL) with inadequate luteinizing hormone (LH) and follicle-stimulating hormone (FSH) levels 70, 71, 72.
Testosterone replacement therapy (TRT), a generally accepted method treating for age-related hypogonadism, can improve the symptoms of age-related hypogonadism and is most usually administered by injection, oral administration and transdermal administration 14. Many studies have reported the benefit of testosterone replacement therapy (TRT) for age-related hypogonadism 53. However, some studies revealed that symptoms related to age-related hypogonadism may not be correlated with serum total testosterone levels 54, 55.
The American College of Physicians (ACP) recently issued new guidelines on prescribing supplemental testosterone for men with age-related low testosterone 51:
- The American College of Physicians suggests that clinicians discuss whether to initiate testosterone treatment in men with age-related low testosterone with sexual dysfunction who want to improve sexual function (conditional recommendation; low-certainty evidence). The discussion should include the potential benefits, harms, costs, and patient’s preferences.
- The American College of Physicians suggests that clinicians should reevaluate symptoms within 12 months and periodically thereafter. Clinicians should discontinue testosterone treatment in men with age-related low testosterone with sexual dysfunction in whom there is no improvement in sexual function (conditional recommendation; low-certainty evidence).
- The American College of Physicians suggests that clinicians consider intramuscular rather than transdermal formulations when initiating testosterone treatment to improve sexual function in men with age-related low testosterone, as costs are considerably lower for the intramuscular formulation and clinical effectiveness and harms are similar.
- The evidence shows that men with age-related low testosterone may experience slight improvements in sexual function by 35% and erectile dysfunction by 27% if prescribed supplemental testosterone.
- The evidence does not support prescribing testosterone for men with concerns about energy, vitality, physical function, or cognition.
- The new guidelines point out that treating with supplemental testosterone is not risk free. Potential risks include blood clots, stroke, sleep apnea, acne and possibly enlarged breasts (gynecomastia). Men with these or other conditions may be advised against using supplemental testosterone even for sexual dysfunction.
- If men are treated with supplemental testosterone for sexual dysfunction, the decision to continue to treat should be reevaluated after a year and then periodically after that. Treatment should be stopped if sexual dysfunction doesn’t improve, according to the new guidelines.
Data from meta-analyses have shown that testosterone replacement therapy is ineffective when baseline testosterone levels are > 3.5 ng/mL (>12 nmol/L). Positive outcomes are documented when testosterone levels are < 3.5 ng/mL (<12 nmol/L), being higher in symptomatic patients with more severe forms of hypogonadism (< 8 nmol/L). Therefore, patients with symptomatic hypogonadism without specific contraindications where testosterone levels are less than 3.5 ng/mL (<12 nmol/L) should be considered for starting testosterone therapy 56, 57.
Testosterone replacement therapy
Several testosterone formulations are available. Direct comparisons among different testosterone products are still lacking. Patients who are considering testosterone therapy should be adequately informed about the possible risks and benefits of all available testosterone preparations. The final choice should be based on the clinical situation, testosterone formulation availability, and patient needs and expectations 73, 74.
One Food and Drug Administration-approved oral testosterone replacement preparation, testosterone undecanoate (Jatenzo), is absorbed by the lymph system. It might avoid the liver problems seen with other oral forms of testosterone.
Other preparations you might choose, depending on convenience, cost and your insurance coverage, include:
- Testosterone Gel. There are several gels and solutions available, with different ways of applying them. Depending on the brand, you rub the testosterone into your skin on your upper arm or shoulder (AndroGel, Testim, Vogelxo) or apply it to the front and inner thigh (Fortesta). Your body absorbs testosterone through your skin. Don’t shower or bathe for several hours after a gel application, to be sure it gets absorbed. Side effects include skin irritation and the possibility of transferring the medication to another person. Avoid skin-to-skin contact until the gel is completely dry, or cover the area after an application.
- Testosterone Injection. Testosterone cypionate (Depo-Testosterone) and testosterone enanthate are given in a muscle or under the skin. Your symptoms might waver between doses depending on the frequency of injections. You or a family member can learn to give testosterone injections at home. If you’re uncomfortable giving yourself injections, member of your care team can give the injections.
- Testosterone undecanoate (Aveed) is given by deep intramuscular injection, typically every 10 weeks. It must be given at your provider’s office and can have serious side effects.
- Testosterone Patch. A patch containing testosterone (Androderm) is applied each night to your thighs or torso. A possible side effect is severe skin reaction.
- Testosterone Pellets (Testopel): Testosterone-containing pellets are surgically implanted under the skin every three to six months for consistent and long-term dosages. Side effects: pellet coming out through skin, site infection/ bleeding (rare), dose decreasing over time and hypogonadism symptoms possibly returning towards the end of dose period.
- Testosterone Gum and Cheek (buccal cavity). A small putty-like substance, gum-and-cheek testosterone replacement delivers testosterone through the natural depression above your top teeth where your gum meets your upper lip (buccal cavity). This product, taken three times a day, sticks to your gumline and allows testosterone to be absorbed into your bloodstream. It can cause gum irritation.
- Testosterone Nasal. This testosterone gel (Natesto) can be pumped into the nostrils. This option reduces the risk that medication will be transferred to another person through skin contact. Nasal-delivered testosterone must be applied twice in each nostril, three times daily, which might be more inconvenient than other delivery methods.
Testosterone Oral formulations
An oral formulation has been available in oleic acid since the 1970s, and has been recently reformulated in a mixture of castor oil and propylene glycol laureate (testosterone undecanoate [TU] caps), to allow the drug to be maintained at room temperature without degradation 73, 74. The main limitation is related to poor bioavailability, which is strongly dependent on dietary fat content 73, 74. The US Food and Drug Administration (FDA) approved a new formulation of oral testosterone undecanoate in a liquid-filled soft gel capsule, which improved oral availability 75. Available evidence showed that testosterone undecanoate capsule formulations can reach steady 24-hour average serum testosterone levels in more than 80% of hypogonadal men, thus resulting in a significant improvement of all sexual function domains at all time points when compared to baseline along with an excellent safety profile 75. More recently, the FDA has approved a new oral formulation which contains as carriers Vitamin E, phytosterol esters, polyoxyl 40 hydrogenated castor oil and propylene glycol monolaurate 75. For all new oral testosterone undecanoate formulations a mild increase in arterial blood pressure has been reported. Hence, the FDA has required a black box warning that these drugs can induce a blood pressure increase 75.
Mesterolone is a 5α-dihydrotestosterone (DHT) derivate available for oral administration. Along with DHT, mesterolone cannot be converted to estrogens and can only be used for a limited period and for specific indications, such as the presence of painful gynecomastia. However, the lack of a full spectrum of testosterone bioactivity strongly limits its long-term use 73.
Testosterone Injectable formulations
Injectable testosterone preparations can be classified according to their half-lives. Testosterone propionate is a short-term ester formulation requiring multiple fractionated doses (usually 50-100 mg, every two to three days), thus representing a major limitation for its use 73, 74. Cypionate and enanthate-testosterone esters are short-term formulations, requiring administration every two to four weeks. A formulation containing mixed testosterone esters (testosterone undecanoate, isocaproate, phenyl propionate, propionate) which has the benefit of a steady release of testosterone into the circulation, is available in some countries. The use of these older formulations is associated with wide fluctuations in plasma testosterone concentrations and is often reported as unpleasant by patients potentially resulting in adverse effects, such as polycythaemia 73, 74, 76. A longer-lasting testosterone undecanoate injectable formulation is widely available 73, 74, with a good safety/benefit profile allowing the maintenance of normal stable testosterone levels at a dose of 1,000 mg initially every twelve weeks, following a six-week loading dose, but can be adjusted to a frequency of ten to fourteen weeks dependent on the trough (pre-injection level) after three to five injections to maintain levels in the therapeutic range (usually > 12 and < 18 nmol/L) 73, 74, 77.
Testosterone Transdermal preparations
Among the available transdermal formulations, testosterone gels represent the most frequently used preparations. The testosterone gel is quickly absorbed by the stratum corneum, creating a reservoir within the subcutaneous tissues from where testosterone is continuously delivered for 24 hours, after a single daily application. These formulations have been shown to normalise serum testosterone levels with an excellent safety profile 73, 74, 77. The introduction of specific devices and skin enhancers has resulted in better skin penetration of the drugs, thus reducing potential adverse effects. Local skin adverse effects are limited when compared to those with traditional testosterone patches, but they potentially allow transference of testosterone during close contact with the skin surface. The risk can be reduced by wearing clothing or by applying the gel on skin surfaces not usually touched (e.g., the inner thigh surface) 73, 74. To reduce the total amount of gel applied and residual quantities remaining on the skin, new formulations of testosterone gel have been introduced with a testosterone concentration of 1.62-2% 73, 74. Another transdermal testosterone formulation includes a topical, alcohol-based testosterone (2%) solution, which must be applied to the underarm once daily, using a metered dose applicator 73, 74. Testosterone levels should be monitored to optimize the testosterone dose. Blood collection is best taken two to four hours after gel application to use the peak level of testosterone absorbed as a reference for adequate therapeutic levels. Levels of testosterone after application can vary and a repeat measurement may be indicated especially as sometimes, inadvertently, the skin over the venipuncture site can be contaminated by the gel, leading to falsely elevated results.
In some European countries, dihydrotestosterone (DHT) is available as a hydroalcoholic 2.5% gel. It is rapidly absorbed, reaching a steady state in two to three days 73, 74. Similar to that reported for mesterolone, dihydrotestosterone (DHT) is not aromatised but can be useful for treating particular conditions, such as gynecomastia and microphallus 73, 74.
Testosterone Transmucosal formulations
A testosterone buccal system is still available in several countries. It consists of a sustained-release muco-adhesive buccal-testosterone-tablet requiring twice-daily application to the upper gums. The tablet does not dissolve completely in the mouth and must be removed after twelve hours. This formulation has been proven to restore testosterone levels within the physiological range with minimal or transient local problems, including gum oedema, blistering and gingivitis 73, 74.
A gel for intranasal administration is available in some countries, including the USA and Canada. It requires administration two or three times daily using a specific metered-dose pump. The application is rapid, non-invasive, and convenient, and avoids secondary transference observed with other topical products 73, 74. Preliminary results suggest that intranasal testosterone is associated with lower suppression of gonadotropin levels and with a lower risk of hematocrit increases 78.
Testosterone Subdermal depots
The implantation of testosterone pellets, available in a limited number of countries, represents the longest available testosterone formulation lasting from four to seven months. The procedure is invasive and may be unattractive to patients 73, 74.
Testosterone therapy side effects
Testosterone therapy carries various risks, including:
- Increased production of red blood cells
- Acne
- Enlarged breasts
- Sleep disturbances
- Prostate enlargement
- Limited sperm production
Testosterone therapy contraindications
Main contraindications of testosterone therapy:
- Absolute contraindications
- Locally advanced or metastatic prostate cancer
- Male breast cancer
- Men with an active desire to have children
- Hematocrit ≥ 54%
- Uncontrolled or poorly controlled congestive heart failure
- Relative contraindication
- International Prostate Symptom Score (IPSS) > 19
- Baseline hematocrit 48-50%
- Familial history of venous thromboembolism
Absolute contraindications to testosterone replacement therapy are untreated breast and prostate cancer. Similarly, conditions such as cardiovascular diseases as well as uncontrolled or poorly controlled congestive heart failure should be considered when prescribing testosterone therapy 79. Severe lower urinary tract symptoms (LUTS) [International Prostate Symptom Score (IPSS) score > 19] represent a relative contraindication, as there is insufficient data on the long-term effects of testosterone therapy in these patients 66. A positive family history for venous thromboembolism requires further analysis to exclude a condition of undiagnosed thrombophilia-hypofibrinolysis 80. These patients need to be carefully counseled prior to testosterone therapy initiation. An elevated hematocrit (HCT) level is the most common adverse effect of testosterone therapy. Stimulation of erythropoiesis is a normal biological action that enhances the delivery of oxygen to testosterone-sensitive tissues (e.g., striated, smooth and cardiac muscle). Any elevation of hematocrit (HCT) above the normal range for hematocrit usually becomes evident between three and twelve months after testosterone therapy initiation. However, polycythemia can also occur after any subsequent increase in testosterone dose, switching from topical to parenteral administration and, development of comorbidity, which can be linked to an increase in hematocrit (e.g., respiratory or haematological diseases).
A hematocrit (HCT) > 54% should require testosterone therapy withdrawal, reduction in dose, change of formulation and venesection depending on the clinical situation to avoid any potential cardiovascular complications. Lower baseline hematocrit (HCT) (48-50%) should be carefully evaluated before testosterone therapy initiation, to avoid pathological increases during treatment, especially in high-risk men such as those with Chronic Obstructive Pulmonary Disease (COPD) or Obstructive Sleep Apnea (OSA). Accordingly, the Framingham Heart Study showed that hematocrit (HCT) > 48% represented a condition associated with increased risk of coronary artery disease (coronary heart disease) and mortality and was associated with cardiovascular disorders 81. Testosterone therapy suppresses gonadotropin (luteinizing hormone [LH] and follicle-stimulating hormone [FSH]) and endogenous testosterone secretion as well as spermatogenesis 82. Therefore, testosterone therapy is contraindicated in individuals who desire fertility 83. Secondary hypogonadism is characterised by low or inappropriately normal gonadotropin levels; therefore, the rationale is to substitute the gonadotropin deficiency with simultaneously luteinizing hormone (LH) and follicle-stimulating hormone (FSH) analogues, if fertility is desired 84.
Treatment of infertility due to hypogonadism
If a pituitary problem is the cause of low testosterone, pituitary hormones can be given to stimulate sperm production and restore fertility. A pituitary tumor may require surgical removal, medication, radiation or the replacement of other hormones. Gonadotropin therapy should be considered the standard treatment in men with secondary hypogonadism who desire to have children 73, 85. Recombinant human chorionic gonadotropin (rhCG) and recombinant luteinizing hormone (rLH) formulations offer comparable effects to urinary-derived preparations 85. According to a meta-analysis of the available evidence, hCG should be administered with follicle-stimulating hormone (FSH) since combined therapy results in better outcomes 7. Similar to recombinant hCG, recombinant follicle-stimulating hormone (rFSH) offers comparable effects to urinary-derived preparations 77.
Anti-oestrogens, including selective estrogen receptor modulators (SERMs) and aromatase inhibitors (AI) have been suggested as off-label treatments to restore testosterone levels and fertility in men with functional secondary hypogonadism or idiopathic infertility 7. They work by preventing down-regulation of the hypothalamic-pituitary-gonadal (HPG) axis by estrogens and for this reason are particularly useful in men with obesity and metabolic disorders 86, 87. In the latter case, the hypothesis is that the excess of fatty tissue leads to increased aromatase activity and estrogens levels resulting in impairment of the hypothalamic-pituitary-gonadal (HPG) axis 88. Due to their presumed mechanism of action, they require an intact HPG axis and cannot work in primary hypogonadism or secondary hypogonadism due to organic damage of the HPG axis. Both types of selective estrogen receptor modulators (SERMs), which bind estrogen receptors (ERs) with an agonist or antagonist effect depending upon the target tissue, and aromatase inhibitors, which prevent androgens from being converted into estrogens by aromatase, have been used in clinical practice 73, 85. The evidence published so far is poor; all these products are off-label treatments and selective estrogen receptor modulators (SERMs), due to their agonistic effect on venous vessels, could predispose men to the development of venous thromboembolism 73, 85. In this context patients should be warned of the potential increased risk of venous thromboembolism, although data are lacking. Long-term use of these agents can lead to reduced bone density and the development of osteoporosis, potentially increasing fracture risk 7.
There’s often no effective treatment to restore fertility in men with primary hypogonadism, but assisted reproductive technology may be helpful. This technology covers a variety of techniques designed to help couples who have been unable to conceive.
Monitoring Testosterone Replacement Therapy
Testosterone therapy alleviates symptoms and signs of hypogonadism in men in a specific time-dependent manner 7. The results of testosterone clinical trials showed that testosterone therapy improved sexual symptoms as early as 3 months after initiation 89, 80, 90. Table 2 summarises the clinical and biochemical parameters that should be monitored during testosterone therapy. The first evaluation should be planned after 3 months of testosterone treatment. Further evaluation may be scheduled at 6 months or 12 months, according to patient characteristics, as well as results of biochemical testing. Patients at high risk of developing elevated hematocrit should be evaluated every 3 months during the first year of testosterone therapy and at least every 6 months thereafter. Accordingly, current guidelines suggest that hematocrit should be maintained below 45% in patients with polycythemia vera to avoid thromboembolism risk 91. Similarly, data derived using a multi-institutional database including a large cohort of hypogonadal (total testosterone < 12 nmol/L) men who received testosterone therapy and subsequently did (n=5,887) or did not (n=4,2784) develop polycythemia (hematocrit > 52%) showed that men who had an increased hematocrit had a higher risk of major adverse cardiovascular events or venous thromboembolism mostly during the first year of therapy 92. The risk was even higher when a hematocrit threshold of 54% was considered whilst no risk was observed when a hematocrit 50% threshold was applied 92.
Testosterone Trials were designed to maintain the serum testosterone concentration within the normal range for young men (280–873 ng/dL or 9.6-30 nmol/L) 89. This approach resulted in a good benefit/risk ratio. A similar approach could be considered during follow-up. The correct timing for the evaluation of testosterone levels varies according to the type of testosterone preparation used. Testosterone is involved in the regulation of erythropoiesis 76 and prostate growth 62, hence measuring serum PSA and hematocrit should be mandatory before and during testosterone therapy. However, it is important to recognize that the risk of prostate cancer in men aged < 40 years is low. Similarly, the mortality risk for prostate cancer in men aged > 70 years has not been considered high enough to warrant monitoring in the general population 93. Therefore, any screening for prostate cancer through the determination of PSA and digital rectal exam (DRE) in men aged < 40 or > 70 years during testosterone therapy should be discussed with the patients.
Baseline and annual metabolic profile evaluation may be a reasonable consideration, particularly in the management of functional hypogonadism. Testosterone therapy may be beneficial for hypogonadal men with low or moderate fracture risk 94. Therefore, dual energy X-ray absorptiometry (DEXA) bone scan may also be considered at baseline and 18-24 months following testosterone therapy, particularly in patients with more severe hypogonadism 94.
Digital rectal examination (DRE) may detect prostate abnormalities that can be present even in men with normal PSA values. Hence, digital rectal exam (DRE) is mandatory in all men at baseline and is recommended to be performed at least annually during testosterone therapy, as long as there is no significant increase in PSA velocity.
The decision to stop testosterone therapy or to perform a prostate biopsy due to PSA increase or prostate abnormalities should be based on local prostate cancer guidelines. There is a large consensus that any increase of hematocrit > 54% during testosterone therapy requires testosterone withdrawal and phlebotomy to avoid potential adverse effects including venous-thromboembolism and cardiovascular disease, especially in high-risk individuals 7. In patients with lower risk of relevant clinical complications, the situation can be alternatively managed by reducing testosterone dose and switching formulation along with venesection 7. A positive family history of venous-thromboembolism should be carefully investigated and the patient counseled about testosterone therapy to avoid/prevent thrombophilia-hypofibrinolysis 80. Finally, caution should be exercised in men with pre-existing cardiovascular disease or at higher risk of cardiovascular disease 79.
Table 2. Clinical and biochemical parameters to be checked during testosterone therapy
| Parameters | Year 1 of treatment | After year 1 of treatment | ||||
|---|---|---|---|---|---|---|
| Baseline | 3 months | 6 months | 12 months | Annually | 18-24 months | |
| Clinical | ||||||
| Symptoms | X | X | X | X | X | |
| Body Mass Index | X | X | X | |||
| Waist circumference | X | X | X | X | ||
| Digital rectal examination | X | X | X | |||
| Blood pressure | X | X | X | X | ||
| Biochemistry | ||||||
| PSA (ng/mL) | X | X | X2 | X | X | |
| Hematocrit (%) | X | X | X1,2 | X | X | |
| Testosterone | X | X | X | X | ||
| Lipid and glycaemic profile | X | X | X | |||
| Instrumental | ||||||
| DEXA | X | X | ||||
Footnotes: 1) Population with polycythemia vera or at high risk of secondary polycythemia (e.g., sleep apnea, morbidobesity, heavy smokers, chronic obstructive pulmonary disease); 2) Prostate cancer survivors.
[Source 7 ]- Snyder PJ. Symptoms of late-onset hypogonadism in men. Endocrinol Metab Clin North Am (2022) 51(4):755–60. https://doi.org/10.1016/j.ecl.2022.04.001[↩]
- Nieschlag, E. (2020), Late-onset hypogonadism: a concept comes of age. Andrologia, 8: 1506-1511. https://doi.org/10.1111/andr.12719[↩]
- Ferrini RL, Barrett-Connor E. Sex hormones and age: a cross-sectional study of testosterone and estradiol and their bioavailable fractions in community-dwelling men. Am J Epidemiol. 1998;147(8):750–754. doi: 10.1093/oxfordjournals.aje.a009519[↩]
- Mohr BA, Guay AT, O’Donnell AB, McKinlay JB. Normal, bound and nonbound testosterone levels in normally ageing men: results from the Massachusetts male ageing study. Clin Endocrinol (Oxf) 2005;62(1):64–73. doi: 10.1111/j.1365-2265.2004.02174.x[↩]
- Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. Baltimore longitudinal study of aging. J Clin Endocrinol Metab. 2001;86(2):724–731. doi: 10.1210/jcem.86.2.7219[↩]
- Wu FC, Tajar A, Pye SR, Silman AJ, Finn JD, O’Neill TW, et al. Hypothalamic-pituitary-testicular axis disruptions in older men are differentially linked to age and modifiable risk factors: the European male aging study. J Clin Endocrinol Metab. 2008;93(7):2737–2745. doi: 10.1210/jc.2007-1972[↩]
- MALE HYPOGONADISM. https://uroweb.org/guidelines/sexual-and-reproductive-health/chapter/male-hypogonadism[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Shiozawa K, Maeda M, Ho HJ, Katsurai T, Howlader MZH, Horiuchi K, Sugita Y, Ohsaki Y, Agista AZ, Goto T, Komai M, Shirakawa H. Biotin Enhances Testosterone Production in Mice and Their Testis-Derived Cells. Nutrients. 2022 Nov 10;14(22):4761. doi: 10.3390/nu14224761[↩]
- Isidori AM, Aversa A, Calogero A, Ferlin A, Francavilla S, Lanfranco F, Pivonello R, Rochira V, Corona G, Maggi M. Adult- and late-onset male hypogonadism: the clinical practice guidelines of the Italian Society of Andrology and Sexual Medicine (SIAMS) and the Italian Society of Endocrinology (SIE). J Endocrinol Invest. 2022 Dec;45(12):2385-2403. doi: 10.1007/s40618-022-01859-7[↩][↩]
- Corona G, Maseroli E, Rastrelli G, Francomano D, Aversa A, Hackett GI, Ferri S, Sforza A, Maggi M. Is late-onset hypogonadotropic hypogonadism a specific age-dependent disease, or merely an epiphenomenon caused by accumulating disease-burden? Minerva Endocrinol. 2016 Jun;41(2):196-210. https://www.minervamedica.it/en/journals/minerva-endocrinology/article.php?cod=R07Y2016N02A0196[↩]
- Wu FC, Tajar A, Pye SR, Silman AJ, Finn JD, O’Neill TW, et al.. Hypothalamic-pituitary-testicular axis disruptions in older men are differentially linked to age and modifiable risk factors: the European Male aging study. J Clin Endocrinol Metab (2008) 93(7):2737–45. doi: 10.1210/jc.2007-1972[↩]
- Zitzmann M, Nieschlag E. Der Altershypogonadismus des Mannes. Rationale Diagnostik und Therapie [Hypogonadism in the elderly man. Reliable diagnosis and therapy]. Internist (Berl). 2003 Oct;44(10):1313-21. German. doi: 10.1007/s00108-003-1044-z[↩]
- Morales A, Lunenfeld B; International Society for the Study of the Aging Male. Investigation, treatment and monitoring of late-onset hypogonadism in males. Official recommendations of ISSAM. International Society for the Study of the Aging Male. Aging Male. 2002 Jun;5(2):74-86.[↩]
- Xu Z, Chen X, Zhou H, Ren C, Wang Q, Pan Y, Liu L, Liu X. An updated systematic review and meta-analysis of the effects of testosterone replacement therapy on erectile function and prostate. Front Endocrinol (Lausanne). 2024 Jan 26;15:1335146. doi: 10.3389/fendo.2024.1335146[↩][↩][↩]
- Nassar GN, Leslie SW. Physiology, Testosterone. [Updated 2023 Jan 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526128[↩]
- Kelly DM, Jones TH. Testosterone: a metabolic hormone in health and disease. J Endocrinol (2013) 217(3):R25–45. doi: 10.1530/JOE-12-0455[↩]
- McEwan IJ, Brinkmann AO. Androgen Physiology: Receptor and Metabolic Disorders. [Updated 2021 Jul 2]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279028[↩]
- Sizar O, Leslie SW, Pico J. Androgen Replacement. [Updated 2023 Nov 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534853[↩][↩][↩]
- Vermeulen A, Kaufman JM. Diagnosis of hypogonadism in the aging male. Aging Male. 2002 Sep;5(3):170-6. Erratum in: Aging Male. 2002 Dec;5(4):iv.[↩]
- Vermeulen A. Hormonal cut-offs of partial androgen deficiency: a survey of androgen assays. J Endocrinol Invest. 2005;28(3 Suppl):28-31.[↩]
- Tajar A, Forti G, O’Neill TW, Lee DM, Silman AJ, Finn JD, Bartfai G, Boonen S, Casanueva FF, Giwercman A, Han TS, Kula K, Labrie F, Lean ME, Pendleton N, Punab M, Vanderschueren D, Huhtaniemi IT, Wu FC; EMAS Group. Characteristics of secondary, primary, and compensated hypogonadism in aging men: evidence from the European Male Ageing Study. J Clin Endocrinol Metab. 2010 Apr;95(4):1810-8. doi: 10.1210/jc.2009-1796[↩][↩]
- Feldman HA, Longcope C, Derby CA, Johannes CB, Araujo AB, Coviello AD, Bremner WJ, McKinlay JB. Age trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts male aging study. J Clin Endocrinol Metab. 2002 Feb;87(2):589-98. doi: 10.1210/jcem.87.2.8201[↩][↩][↩]
- Nieschlag E, Swerdloff R, Behre HM, Gooren LJ, Kaufman JM, Legros JJ, Lunenfeld B, Morley JE, Schulman C, Wang C, Weidner W, Wu FC. Investigation, treatment and monitoring of late-onset hypogonadism in males: ISA, ISSAM, and EAU recommendations. Int J Androl. 2005 Jun;28(3):125-7. doi: 10.1111/j.1365-2605.2005.00553.x[↩][↩]
- Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR; Baltimore Longitudinal Study of Aging. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. Baltimore Longitudinal Study of Aging. J Clin Endocrinol Metab. 2001 Feb;86(2):724-31. doi: 10.1210/jcem.86.2.7219[↩][↩][↩][↩][↩][↩]
- Stanworth RD, Jones TH. Testosterone for the aging male; current evidence and recommended practice. Clin Interv Aging. 2008;3(1):25-44. doi: 10.2147/cia.s190[↩][↩]
- Iwamoto T., Yanase T., Koh E., Horie H., Baba K., Namiki M., Nawata H. Reference ranges of total serum and free testosterone in Japanese male adults. Nihon Hinyokika Gakkai Zasshi. 2004;95:751–760. doi: 10.5980/jpnjurol1989.95.751[↩][↩]
- Wu FC, Tajar A, Pye SR, Silman AJ, Finn JD, O’Neill TW, Bartfai G, Casanueva F, Forti G, Giwercman A, Huhtaniemi IT, Kula K, Punab M, Boonen S, Vanderschueren D; European Male Aging Study Group. Hypothalamic-pituitary-testicular axis disruptions in older men are differentially linked to age and modifiable risk factors: the European Male Aging Study. J Clin Endocrinol Metab. 2008 Jul;93(7):2737-45. doi: 10.1210/jc.2007-1972[↩][↩]
- Wu FC, Tajar A, Beynon JM, Pye SR, Silman AJ, Finn JD, O’Neill TW, Bartfai G, Casanueva FF, Forti G, Giwercman A, Han TS, Kula K, Lean ME, Pendleton N, Punab M, Boonen S, Vanderschueren D, Labrie F, Huhtaniemi IT; EMAS Group. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med. 2010 Jul 8;363(2):123-35. doi: 10.1056/NEJMoa0911101[↩][↩][↩][↩][↩]
- Feldman HA, Longcope C, Derby CA, Johannes CB, Araujo AB, Coviello AD, et al.. Age trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts male aging study. J Clin Endocrinol Metab (2002) 87(2):589–98. doi: 10.1210/jcem.87.2.8201[↩][↩]
- Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR, Baltimore Longitudinal Study of Aging . Longitudinal effects of aging on serum total and free testosterone levels in healthy men. Baltimore Longitudinal Study of Aging. J Clin Endocrinol Metab (2001) 86(2):724–31. doi: 10.1210/jcem.86.2.7219[↩][↩]
- Winter, A. G., Zhao, F., & Lee, R. K. (2014). Androgen deficiency and metabolic syndrome in men. Translational andrology and urology, 3(1), 50–58. https://doi.org/10.3978/j.issn.2223-4683.2014.01.04[↩][↩]
- Abbasi A.A., Drinka P.J., Mattson D.E., Rudman D. Low circulating levels of insulin-like growth factors and testosterone in chronically institutionalized elderly men. J. Am. Geriatr. Soc. 1993;41:975–982. doi: 10.1111/j.1532-5415.1993.tb06764.x[↩][↩]
- Spaziani M, Mileno B, Rossi F, Granato S, Tahani N, Anzuini A, Lenzi A, Radicioni AF. Endocrine and metabolic evaluation of classic Klinefelter syndrome and high-grade aneuploidies of sexual chromosomes with male phenotype: are they different clinical conditions? Eur J Endocrinol. 2018 Apr;178(4):343-352. doi: 10.1530/EJE-17-0902[↩][↩]
- Bozzola M, Bozzola E, Montalbano C, Stamati FA, Ferrara P, Villani A. Delayed puberty versus hypogonadism: a challenge for the pediatrician. Ann Pediatr Endocrinol Metab. 2018 Jun;23(2):57-61. doi: 10.6065/apem.2018.23.2.57[↩][↩]
- Hauser LJ, Jensen EL, Mirsky DM, Chan KH. Pediatric anosmia: A case series. Int J Pediatr Otorhinolaryngol. 2018 Jul;110:135-139. doi: 10.1016/j.ijporl.2018.05.011[↩][↩]
- Salonia A, Bettocchi C, Boeri L, Capogrosso P, Carvalho J, Cilesiz NC, et al.. EAU working group on male sexual and reproductive health. European association of urology guidelines on sexual and reproductive health-2021 update: male sexual dysfunction. Eur Urol (2021) 80(3):333–57. doi: 10.1016/j.eururo.2021.06.007[↩][↩]
- Mulhall JP, Trost LW, Brannigan RE, Kurtz EG, Redmon JB, Chiles KA, et al.. Evaluation and management of testosterone deficiency: AUA guideline. J Urol (2018) 200(2):423–32. doi: 10.1016/j.juro.2018.03.115[↩][↩]
- Bhasin S, Brito JP, Cunningham GR, Hayes FJ, Hodis HN, Matsumoto AM, et al.. Testosterone therapy in men with hypogonadism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab (2018) 103(5):1715–44. doi: 10.1210/jc.2018-00229[↩][↩]
- Gagliano-Jucá T, Li Z, Pencina KM, Beleva YM, Carlson OD, Egan JM, Basaria S. Oral glucose load and mixed meal feeding lowers testosterone levels in healthy eugonadal men. Endocrine. 2019 Jan;63(1):149-156. doi: 10.1007/s12020-018-1741-y[↩][↩]
- Boeri L, Capogrosso P, Ventimiglia E, Cazzaniga W, Pederzoli F, Moretti D, Dehò F, Montanari E, Montorsi F, Salonia A. Does Calculated Free Testosterone Overcome Total Testosterone in Protecting From Sexual Symptom Impairment? Findings of a Cross-Sectional Study. J Sex Med. 2017 Dec;14(12):1549-1557. doi: 10.1016/j.jsxm.2017.10.070[↩][↩]
- Rastrelli G, O’Neill TW, Ahern T, Bártfai G, Casanueva FF, Forti G, Keevil B, Giwercman A, Han TS, Slowikowska-Hilczer J, Lean MEJ, Pendleton N, Punab M, Antonio L, Tournoy J, Vanderschueren D, Maggi M, Huhtaniemi IT, Wu FCW; EMAS study group. Symptomatic androgen deficiency develops only when both total and free testosterone decline in obese men who may have incident biochemical secondary hypogonadism: Prospective results from the EMAS. Clin Endocrinol (Oxf). 2018 Oct;89(4):459-469. https://eprints.gla.ac.uk/163468/7/163468.pdf[↩][↩]
- Antonio L, Wu FC, O’Neill TW, Pye SR, Ahern TB, Laurent MR, Huhtaniemi IT, Lean ME, Keevil BG, Rastrelli G, Forti G, Bartfai G, Casanueva FF, Kula K, Punab M, Giwercman A, Claessens F, Decallonne B, Vanderschueren D; European Male Ageing Study Study Group. Low Free Testosterone Is Associated with Hypogonadal Signs and Symptoms in Men with Normal Total Testosterone. J Clin Endocrinol Metab. 2016 Jul;101(7):2647-57. doi: 10.1210/jc.2015-4106[↩][↩]
- Bassil N, Morley JE. Late-life onset hypogonadism: a review. Clin Geriatr Med. 2010 May;26(2):197-222. doi: 10.1016/j.cger.2010.02.003[↩]
- Nguyen CP, Hirsch MS, Moeny D, Kaul S, Mohamoud M, Joffe HV. Testosterone and “Age-Related Hypogonadism”–FDA Concerns. N Engl J Med. 2015 Aug 20;373(8):689-91. doi: 10.1056/NEJMp1506632[↩][↩]
- Maggi M, Schulman C, Quinton R, Langham S, Uhl-Hochgraeber K. The burden of testosterone deficiency syndrome in adult men: economic and quality-of-life impact. J Sex Med. 2007 Jul;4(4 Pt 1):1056-69. doi: 10.1111/j.1743-6109.2007.00531.x[↩]
- Mulligan T, Frick MF, Zuraw QC, Stemhagen A, McWhirter C. Prevalence of hypogonadism in males aged at least 45 years: the HIM study. Int J Clin Pract. 2006 Jul;60(7):762-9. doi: 10.1111/j.1742-1241.2006.00992.x[↩]
- Petak SM, Nankin HR, Spark RF, Swerdloff RS, Rodriguez-Rigau LJ; American Association of Clinical Endocrinologists. American Association of Clinical Endocrinologists Medical Guidelines for clinical practice for the evaluation and treatment of hypogonadism in adult male patients–2002 update. Endocr Pract. 2002 Nov-Dec;8(6):440-56. Erratum in: Endocr Pract. 2008 Sep;14(6):802-3. Petak, Steven M [added]; Nankin, Howard R [added]; Spark, Richard F [added]; Swerdloff, Ronald S [added]; Rodriguez-Rigau, Luis J [added].[↩]
- McVary KT. Clinical practice. Erectile dysfunction. N Engl J Med. 2007 Dec 13;357(24):2472-81. doi: 10.1056/NEJMcp067261[↩]
- Kaiser FE, Viosca SP, Morley JE, Mooradian AD, Davis SS, Korenman SG. Impotence and aging: clinical and hormonal factors. J Am Geriatr Soc. 1988 Jun;36(6):511-9. doi: 10.1111/j.1532-5415.1988.tb04021.x[↩]
- Meuleman EJ, van Lankveld JJ. Hypoactive sexual desire disorder: an underestimated condition in men. BJU Int. 2005 Feb;95(3):291-6. doi: 10.1111/j.1464-410X.2005.05285.x[↩]
- Amir Qaseem, Carrie A. Horwitch, Sandeep Vijan, et al; for the Clinical Guidelines Committee of the American College of Physicians. Testosterone Treatment in Adult Men With Age-Related Low Testosterone: A Clinical Guideline From the American College of Physicians. Ann Intern Med.2020;172:126-133. doi:10.7326/M19-0882[↩][↩][↩]
- FDA cautions about using testosterone products for low testosterone due to aging; requires labeling change to inform of possible increased risk of heart attack and stroke with use. https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-cautions-about-using-testosterone-products-low-testosterone-due[↩]
- Hisanori Taniguchi, Seiji Shimada, Hidefumi Kinoshita; Testosterone Therapy for Late-Onset Hypogonadism Improves Erectile Function: A Systematic Review and Meta-Analysis. Urol Int 1 June 2022; 106 (6): 539–552. https://doi.org/10.1159/000520135[↩][↩]
- Kang S, Park HJ, Park NC. Serum total testosterone level and identification of late-onset hypogonadism: a communitybased study. Korean J Urol (2013) 54:619–23. doi: 10.4111/kju.2013.54.9.619[↩][↩]
- Lin YC, Hwang TI, Chiang HS, Yang CR, Wu HC, Wu TL, et al.. Correlations of androgen deficiency with clinical symptoms in Taiwanese males. Int J Impot Res (2006) 18:343–7. doi: 10.1038/sj.ijir.3901417[↩][↩]
- Corona G, Giagulli VA, Maseroli E, Vignozzi L, Aversa A, Zitzmann M, Saad F, Mannucci E, Maggi M. THERAPY OF ENDOCRINE DISEASE: Testosterone supplementation and body composition: results from a meta-analysis study. Eur J Endocrinol. 2016 Mar;174(3):R99-116. doi: 10.1530/EJE-15-0262[↩][↩][↩]
- Corona G, Rastrelli G, Morgentaler A, Sforza A, Mannucci E, Maggi M. Meta-analysis of Results of Testosterone Therapy on Sexual Function Based on International Index of Erectile Function Scores. Eur Urol. 2017 Dec;72(6):1000-1011. doi: 10.1016/j.eururo.2017.03.032[↩][↩][↩]
- Millar AC, Lau ANC, Tomlinson G, Kraguljac A, Simel DL, Detsky AS, Lipscombe LL. Predicting low testosterone in aging men: a systematic review. CMAJ. 2016 Sep 20;188(13):E321-E330. doi: 10.1503/cmaj.150262[↩]
- Rastrelli G, Di Stasi V, Inglese F, Beccaria M, Garuti M, Di Costanzo D, Spreafico F, Greco GF, Cervi G, Pecoriello A, Magini A, Todisco T, Cipriani S, Maseroli E, Corona G, Salonia A, Lenzi A, Maggi M, De Donno G, Vignozzi L. Low testosterone levels predict clinical adverse outcomes in SARS-CoV-2 pneumonia patients. Andrology. 2021 Jan;9(1):88-98. doi: 10.1111/andr.12821[↩]
- Salonia A, Pontillo M, Capogrosso P, Gregori S, Tassara M, Boeri L, Carenzi C, Abbate C, Cignoli D, Ferrara AM, Cazzaniga W, Rowe I, Ramirez GA, Tresoldi C, Mushtaq J, Locatelli M, Santoleri L, Castagna A, Zangrillo A, De Cobelli F, Tresoldi M, Landoni G, Rovere-Querini P, Ciceri F, Montorsi F. Severely low testosterone in males with COVID-19: A case-control study. Andrology. 2021 Jul;9(4):1043-1052. doi: 10.1111/andr.12993[↩]
- Corona G, Vena W, Pizzocaro A, Pallotti F, Paoli D, Rastrelli G, Baldi E, Cilloni N, Gacci M, Semeraro F, Salonia A, Minhas S, Pivonello R, Sforza A, Vignozzi L, Isidori AM, Lenzi A, Maggi M, Lombardo F. Andrological effects of SARS-Cov-2 infection: a systematic review and meta-analysis. J Endocrinol Invest. 2022 Dec;45(12):2207-2219. doi: 10.1007/s40618-022-01801-x[↩]
- Rastrelli G, Vignozzi L, Corona G, Maggi M. Testosterone and Benign Prostatic Hyperplasia. Sex Med Rev. 2019 Apr;7(2):259-271. doi: 10.1016/j.sxmr.2018.10.006[↩][↩]
- Guay A, Miller MG, McWhirter CL. Does early morning versus late morning draw time influence apparent testosterone concentration in men aged > or =45 years? Data from the Hypogonadism In Males study. Int J Impot Res. 2008 Mar-Apr;20(2):162-7. doi: 10.1038/sj.ijir.3901580[↩]
- Travison TG, Vesper HW, Orwoll E, Wu F, Kaufman JM, Wang Y, Lapauw B, Fiers T, Matsumoto AM, Bhasin S. Harmonized Reference Ranges for Circulating Testosterone Levels in Men of Four Cohort Studies in the United States and Europe. J Clin Endocrinol Metab. 2017 Apr 1;102(4):1161-1173. doi: 10.1210/jc.2016-2935[↩]
- Huhtaniemi IT, Tajar A, Lee DM, O’Neill TW, Finn JD, Bartfai G, Boonen S, Casanueva FF, Giwercman A, Han TS, Kula K, Labrie F, Lean ME, Pendleton N, Punab M, Silman AJ, Vanderschueren D, Forti G, Wu FC; EMAS Group. Comparison of serum testosterone and estradiol measurements in 3174 European men using platform immunoassay and mass spectrometry; relevance for the diagnostics in aging men. Eur J Endocrinol. 2012 Jun;166(6):983-91. doi: 10.1530/EJE-11-1051[↩]
- Rosner W, Vesper H; Endocrine Society; American Association for Clinical Chemistry; American Association of Clinical Endocrinologists; Androgen Excess/PCOS Society; American Society for Bone and Mineral Research; American Society for Reproductive Medicine; American Urological Association; Association of Public Health Laboratories; Endocrine Society; Laboratory Corporation of America; North American Menopause Society; Pediatric Endocrine Society. Toward excellence in testosterone testing: a consensus statement. J Clin Endocrinol Metab. 2010 Oct;95(10):4542-8. doi: 10.1210/jc.2010-1314[↩][↩]
- Fiers T, Wu F, Moghetti P, Vanderschueren D, Lapauw B, Kaufman JM. Reassessing Free-Testosterone Calculation by Liquid Chromatography-Tandem Mass Spectrometry Direct Equilibrium Dialysis. J Clin Endocrinol Metab. 2018 Jun 1;103(6):2167-2174. doi: 10.1210/jc.2017-02360[↩]
- Vermeulen A, Verdonck L, Kaufman JM. A critical evaluation of simple methods for the estimation of free testosterone in serum. J Clin Endocrinol Metab. 1999 Oct;84(10):3666-72. doi: 10.1210/jcem.84.10.6079[↩]
- Ferlin A, Calogero AE, Krausz C, Lombardo F, Paoli D, Rago R, Scarica C, Simoni M, Foresta C, Rochira V, Sbardella E, Francavilla S, Corona G. Management of male factor infertility: position statement from the Italian Society of Andrology and Sexual Medicine (SIAMS) : Endorsing Organization: Italian Society of Embryology, Reproduction, and Research (SIERR). J Endocrinol Invest. 2022 May;45(5):1085-1113. doi: 10.1007/s40618-022-01741-6[↩]
- Dalvi M, Walker BR, Strachan MW, Zammitt NN, Gibb FW. The prevalence of structural pituitary abnormalities by MRI scanning in men presenting with isolated hypogonadotrophic hypogonadism. Clin Endocrinol (Oxf). 2016 Jun;84(6):858-61. doi: 10.1111/cen.13015[↩][↩]
- Molitch ME. Diagnosis and Treatment of Pituitary Adenomas: A Review. JAMA. 2017 Feb 7;317(5):516-524. doi: 10.1001/jama.2016.19699[↩][↩]
- Cipriani S, Todisco T, Ghiandai N, Vignozzi L, Corona G, Maggi M, Rastrelli G. Biochemical predictors of structural hypothalamus-pituitary abnormalities detected by magnetic resonance imaging in men with secondary hypogonadism. J Endocrinol Invest. 2021 Dec;44(12):2785-2797. doi: 10.1007/s40618-021-01586-5[↩]
- Rastrelli G, Vignozzi L, Corona G, Maggi M. Pharmacotherapy of male hypogonadism. Curr Opin Pharmacol. 2023 Feb;68:102323. doi: 10.1016/j.coph.2022.102323[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Rastrelli G, Maggi M, Corona G. Pharmacological management of late-onset hypogonadism. Expert Rev Clin Pharmacol. 2018 Apr;11(4):439-458. doi: 10.1080/17512433.2018[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Miller JA, Nguyen TT, Loeb C, Khera M, Yafi FA. Oral testosterone therapy: past, present, and future. Sex Med Rev. 2023 Apr 3;11(2):124-138. doi: 10.1093/sxmrev/qead003[↩][↩][↩][↩]
- Ohlander SJ, Varghese B, Pastuszak AW. Erythrocytosis Following Testosterone Therapy. Sex Med Rev. 2018 Jan;6(1):77-85. doi: 10.1016/j.sxmr.2017.04.001[↩][↩]
- Rastrelli G, Corona G, Mannucci E, Maggi M. Factors affecting spermatogenesis upon gonadotropin-replacement therapy: a meta-analytic study. Andrology. 2014 Nov;2(6):794-808. doi: 10.1111/andr.262[↩][↩][↩]
- Rogol AD, Tkachenko N, Bryson N. Natesto™ , a novel testosterone nasal gel, normalizes androgen levels in hypogonadal men. Andrology. 2016 Jan;4(1):46-54. doi: 10.1111/andr.12137. Epub 2015 Dec 22. Erratum in: Andrology. 2017 Jul;5(4):844. doi: 10.1111/andr.12402[↩]
- Lincoff AM, Bhasin S, Flevaris P, Mitchell LM, Basaria S, Boden WE, Cunningham GR, Granger CB, Khera M, Thompson IM Jr, Wang Q, Wolski K, Davey D, Kalahasti V, Khan N, Miller MG, Snabes MC, Chan A, Dubcenco E, Li X, Yi T, Huang B, Pencina KM, Travison TG, Nissen SE; TRAVERSE Study Investigators. Cardiovascular Safety of Testosterone-Replacement Therapy. N Engl J Med. 2023 Jul 13;389(2):107-117. doi: 10.1056/NEJMoa2215025[↩][↩]
- Corona G, Dicuio M, Rastrelli G, Maseroli E, Lotti F, Sforza A, Maggi M. Testosterone treatment and cardiovascular and venous thromboembolism risk: what is ‘new’? J Investig Med. 2017 Aug;65(6):964-973. doi: 10.1136/jim-2017-000411[↩][↩][↩]
- Gagnon DR, Zhang TJ, Brand FN, Kannel WB. Hematocrit and the risk of cardiovascular disease–the Framingham study: a 34-year follow-up. Am Heart J. 1994 Mar;127(3):674-82. doi: 10.1016/0002-8703(94)90679-3[↩]
- Corona G, Rastrelli G, Marchiani S, Filippi S, Morelli A, Sarchielli E, Sforza A, Vignozzi L, Maggi M. Consequences of Anabolic-Androgenic Steroid Abuse in Males; Sexual and Reproductive Perspective. World J Mens Health. 2022 Apr;40(2):165-178. doi: 10.5534/wjmh.210021[↩]
- Colpi GM, Francavilla S, Haidl G, Link K, Behre HM, Goulis DG, Krausz C, Giwercman A. European Academy of Andrology guideline Management of oligo-astheno-teratozoospermia. Andrology. 2018 Jul;6(4):513-524. doi: 10.1111/andr.12502[↩]
- Corona G, Rastrelli G, Maggi M. The pharmacotherapy of male hypogonadism besides androgens. Expert Opin Pharmacother. 2015 Feb;16(3):369-87. doi: 10.1517/14656566.2015.993607. Epub 2014 Dec 19. Erratum in: Expert Opin Pharmacother. 2015 Apr;16(6):941. doi: 10.1517/14656566.2015.1027864. Ratrelli, Giulia [corrected to Rastrelli, Giulia].[↩]
- Rastrelli G, Maggi M, Corona G. Pharmacological management of late-onset hypogonadism. Expert Rev Clin Pharmacol. 2018 Apr;11(4):439-458. doi: 10.1080/17512433.2018.1445969[↩][↩][↩][↩]
- Corona G, Rastrelli G, Morelli A, Sarchielli E, Cipriani S, Vignozzi L, Maggi M. Treatment of Functional Hypogonadism Besides Pharmacological Substitution. World J Mens Health. 2020 Jul;38(3):256-270. doi: 10.5534/wjmh.190061[↩]
- Awouters M, Vanderschueren D, Antonio L. Aromatase inhibitors and selective estrogen receptor modulators: Unconventional therapies for functional hypogonadism? Andrology. 2020 Nov;8(6):1590-1597. doi: 10.1111/andr.12725[↩]
- Grossmann M. Hypogonadism and male obesity: Focus on unresolved questions. Clin Endocrinol (Oxf). 2018 Jul;89(1):11-21. doi: 10.1111/cen.13723[↩]
- Snyder PJ, Bhasin S, Cunningham GR, Matsumoto AM, Stephens-Shields AJ, Cauley JA, Gill TM, Barrett-Connor E, Swerdloff RS, Wang C, Ensrud KE, Lewis CE, Farrar JT, Cella D, Rosen RC, Pahor M, Crandall JP, Molitch ME, Resnick SM, Budoff M, Mohler ER 3rd, Wenger NK, Cohen HJ, Schrier S, Keaveny TM, Kopperdahl D, Lee D, Cifelli D, Ellenberg SS. Lessons From the Testosterone Trials. Endocr Rev. 2018 Jun 1;39(3):369-386. doi: 10.1210/er.2017-00234[↩][↩]
- Isidori AM, Buvat J, Corona G, Goldstein I, Jannini EA, Lenzi A, Porst H, Salonia A, Traish AM, Maggi M. A critical analysis of the role of testosterone in erectile function: from pathophysiology to treatment-a systematic review. Eur Urol. 2014 Jan;65(1):99-112. doi: 10.1016/j.eururo.2013.08.048[↩]
- Barbui T, Tefferi A, Vannucchi AM, Passamonti F, Silver RT, Hoffman R, Verstovsek S, Mesa R, Kiladjian JJ, Hehlmann R, Reiter A, Cervantes F, Harrison C, Mc Mullin MF, Hasselbalch HC, Koschmieder S, Marchetti M, Bacigalupo A, Finazzi G, Kroeger N, Griesshammer M, Birgegard G, Barosi G. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018 May;32(5):1057-1069. doi: 10.1038/s41375-018-0077-1[↩]
- Ory J, Nackeeran S, Balaji NC, Hare JM, Ramasamy AR. Secondary Polycythemia in Men Receiving Testosterone Therapy Increases Risk of Major Adverse Cardiovascular Events and Venous Thromboembolism in the First Year of Therapy. J Urol. 2022 Jun;207(6):1295-1301. doi: 10.1097/JU.0000000000002437[↩][↩]
- Mottet N, De Santis M, Briers E, Bourke L, Gillessen S, Grummet JP, Lam TB, van der Poel HG, Rouvière O, van den Bergh RCN, Cornford P. Updated Guidelines for Metastatic Hormone-sensitive Prostate Cancer: Abiraterone Acetate Combined with Castration Is Another Standard. Eur Urol. 2018 Mar;73(3):316-321. doi: 10.1016/j.eururo.2017.09.029[↩]
- Rochira V, Antonio L, Vanderschueren D. EAA clinical guideline on management of bone health in the andrological outpatient clinic. Andrology. 2018 Mar;6(2):272-285. doi: 10.1111/andr.12470[↩][↩]





{kind=link}