Contents
What is Klinefelter syndrome
Klinefelter syndrome is a genetic condition that affects males physical, behavioral, and cognitive development and functioning. Klinefelter syndrome occurs if boys are born with an extra X chromosome. Boys and men with Klinefelter syndrome are still genetically male and often will not realize they have this extra X chromosome (47, XXY), but occasionally it can cause problems that may require treatment, problems such as a small penis, small testes and infertility. Klinefelter syndrome is quite common, affecting around 1 in every 500 to 1,000 newborn males.
Some people with features of Klinefelter syndrome have conditions known as “variants of Klinefelter syndrome” where there is more than one extra sex chromosome in each cell (48,XXXY, 48,XXYY and 49,XXXXY) 1. Most variants of Klinefelter syndrome are much rarer, occurring in 1 in 50,000 to 1 in 85,000 or fewer newborns 2.
Common physical features may include tall stature, reduced muscle tone, small testes (hypogonadism), delayed pubertal development and lack of secondary male sex characteristics such as decreased facial and body hair and increased breast growth (gynecomastia) in late puberty. Common cognitive and behavioral features may include speech and language delays, ADHD, and emotional and social functioning challenges. The features of Klinefelter syndrome (47, XXY) are typically associated with decreased testosterone level and elevated gonadotropin levels.
Klinefelter syndrome isn’t necessarily anything serious, but treatment can help reduce some of the symptoms if necessary.
Is Klinefelter syndrome inherited?
Klinefelter syndrome (47, XXY) and variants of Klinefelter syndrome (48,XXXY, 48,XXYY and 49,XXXXY) are not inherited.
Klinefelter syndrome chromosomal changes usually occur as random events during the formation of reproductive cells (eggs and sperm) in a parent. An error in cell division called nondisjunction results in either the mother’s egg or the father’s sperm having the extra X chromosome (an equal chance of this happening in either). For example, an egg or sperm cell may gain one or more extra copies of the X chromosome as a result of nondisjunction. If one of these atypical reproductive cells contributes to the genetic makeup of a child, the child will have one or more extra X chromosomes in each of the body’s cells. This change in the egg or sperm seems to happen randomly. If you have a son with the condition, the chances of this happening again are very small. However, the risk of a woman having a son with Klinefelter syndrome may be slightly higher if the mother is over 35 years of age.
Figure 1. Klinefelter syndrome karyotype (47, XXY)
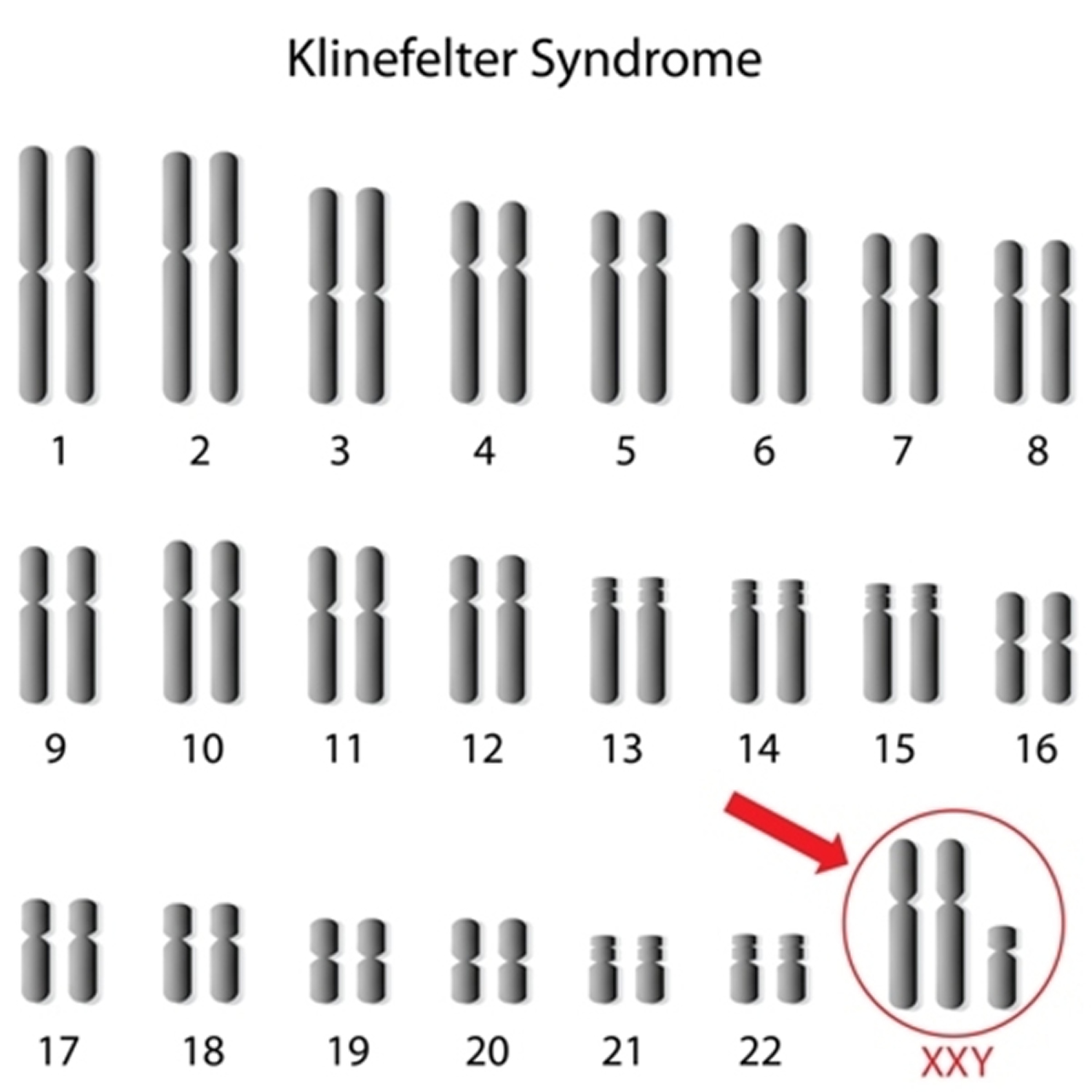
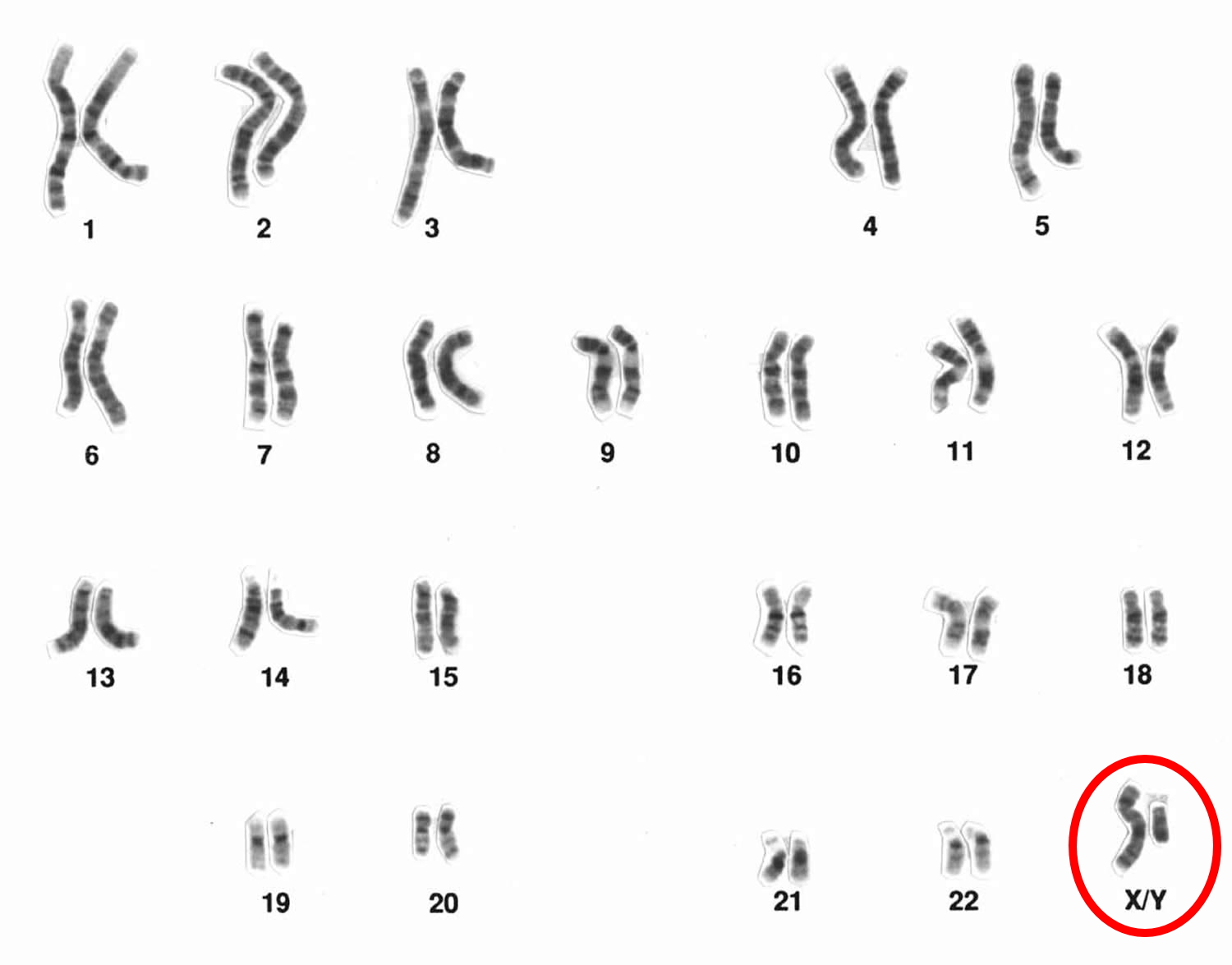
Figure 2. Normal males (boys & men) karyotype (46, XY)
Other names for Klinefelter syndrome
- Klinefelter’s syndrome
- XXY syndrome
- XXY trisomy
Klinefelter syndrome facts
Klinefelter syndrome was named after a physician, Dr. Harry Klinefelter, who published a report in 1942 about nine men with enlarged breast development, sparse facial and body hair, small testes, and an inability to produce sperm.
Klinefelter syndrome is quite common, affecting around 1 in every 500 to 1,000 newborn males. Klinefelter syndrome and its variants are not inherited. It is estimated that 3,000 affected boys are born each year in the United States. Researchers suspect that Klinefelter syndrome is under diagnosed because the condition may not be identified in people with mild signs and symptoms. Additionally, the features of Klinefelter syndrome vary and overlap significantly with those of other conditions.
Affected males typically have small testes that do not produce as much testosterone as usual. Testosterone is the hormone that directs male sexual development before birth and during puberty. A shortage of testosterone can lead to delayed or incomplete puberty, breast enlargement (gynecomastia), reduced facial and body hair, and an inability to have biological children (infertility). Some affected males also have genital differences including undescended testes (cryptorchidism), the opening of the urethra on the underside of the penis (hypospadias), or an unusually small penis (micropenis).
Older children and adults with Klinefelter syndrome tend to be taller than their peers. Compared with unaffected men, adults with Klinefelter syndrome have an increased risk of developing breast cancer and a chronic inflammatory disease called systemic lupus erythematosus (SLE). Their chance of developing these disorders is similar to that of women in the general population.
Children with Klinefelter syndrome may have learning disabilities and delayed speech and language development. They tend to be quiet, sensitive, and unassertive, but personality characteristics vary among affected individuals.
Klinefelter syndrome characteristics
Klinefelter syndrome doesn’t usually cause any obvious symptoms early in childhood, and even the later symptoms may be difficult to spot.
Many boys and men don’t realize they have Klinefelter syndrome. In many cases, it’s only detected if a man with Klinefelter syndrome undergoes fertility tests.
No one can predict for certain what effect the extra X chromosome will have on an individual. Personalities in this group are as varied as in the general population. In addition, the spectrum of manifestations is wide.
However, the following characteristics are said to occur more often in children with Klinefelter syndrome (47,XXY). Keep in mind that a child may have only one or two features, while others may have more:
- Delayed speech
- Gross and fine motor delays
- Sensory integration difficulties, which may include sensitivity to things like sounds, touch, or movement
- Mild hypotonia or low muscle tone
- ADHD
- Auditory processing problems
- Language-based learning disabilities, including reading and written language difficulties
- Social skill deficits
- Anxiety
- Depression
- Gynecomastia or swelling of breast tissue during puberty
Possible features, which aren’t always present, may include:
- in babies and toddlers – learning to sit up, crawl, walk and talk later than usual, being weaker, quieter and more passive than usual
- in childhood – shyness and low self-confidence, problems with reading, writing, spelling and paying attention, mild dyslexia and/or dyspraxia, low energy levels, difficulty socializing or expressing feelings
- in teenagers – growing taller than expected for the family (with long arms and legs), broad hips, poor muscle tone and slower than usual muscle growth, reduced facial and body hair that starts growing later than usual, a small penis and testicles, enlarged breasts (gynecomastia)
- in adulthood – inability to have children naturally (infertility) and a low sex drive, in addition to the physical characteristics mentioned above.
Some people with features of Klinefelter syndrome have more than one extra X chromosome in each cell (such as 48,XXXY or 49,XXXXY). In these cases, known as “variants of Klinefelter syndrome”, the signs and symptoms can be more severe and may include:
- Intellectual disability
- Distinctive facial features
- Skeletal abnormalities
- Poor coordination
- Severe speech difficulties
- Behavioral problems
- Heart defects
- Teeth problems.
Klinefelter syndrome complications
Most boys and men with Klinefelter syndrome will not be significantly affected and can live normal, healthy lives.
Infertility tends to be the main problem, although there are treatments that can help.
However, men with Klinefelter syndrome are at a slightly increased risk of developing other health problems, including:
- Type 2 diabetes
- Weak and fragile bones (osteoporosis)
- Cardiovascular disease and blood clots
- Autoimmune disorders (where the immune system mistakenly attacks the body), such as lupus, thyroiditis
- An underactive thyroid gland (hypothyroidism)
- Anxiety, learning difficulties and depression – although intelligence is usually unaffected
- Dental problems that make dental cavities more likely
- Male breast cancer – although this is very rare
A number of complications caused by Klinefelter syndrome are related to low testosterone (hypogonadism). Testosterone replacement therapy reduces the risk of certain health problems, especially when therapy is started at the beginning of puberty.
Why is early diagnosis of Klinefelter syndrome important?
Klinefelter syndrome (47,XXY) is a leading cause of male infertility and testosterone deficiency, yet the vast majority of Klinefelter syndrome individuals will
reach adulthood without diagnosis.
Early diagnosis means:
- Developmental delays can be addressed sooner
- Appropriate educational interventions can be determined
- Hormone replacement can be timed appropriately
- Having greater knowledge and understanding of one’s condition
- Gaining better health management throughout life
Are males with Klinefelter syndrome more prone to weight gain?
Recent research has shown that males with Klinefelter syndrome have increased body fat and reduced muscle mass. However at this time, the cause of the increased body fat, especially in the abdominal (stomach) area, is not known. Some medical researchers believe it may be caused by the hormone imbalance due to hypogonadism. Others believe the increased body fat may be caused by genetic factors due to having an extra X chromosome since the body fat begins to appear in childhood before the hormones of puberty would play a role. Still other medical researchers believe it is a combination of both testosterone levels and genetic factors. In a recent study of males with Klinefelter syndrome, testosterone therapy only partly corrected the unfavorable muscle/fat ratio, however some researches believe this may have been because the testosterone doses were too low. In addition, males with Klinefelter syndrome also have lower aerobic capacity (ability of lungs and heart to get oxygen to the muscles during exercise) and reduced muscle strength in both biceps and quadriceps muscles. This may decrease the amount of exercise a male with Klinefelter syndrome can do, which might increase the risk of weight gain. At present, no studies have studied the effects of testosterone treatment on muscle strength or other measures of physical fitness in males with Klinefelter syndrome.
Men with Klinefelter syndrome, especially those with increased weight in their abdominal area, are at an increased risk for type 2 diabetes and metabolic syndrome. Therefore if you are having difficulty losing weight, you should make certain your doctor is screening you for these conditions.
Boys with Klinefelter syndrome are known to have an increased risk for psychosocial problems. While large studies of boys with Klinefelter syndrome are uncommon (only 10% of affected males are diagnosed during childhood), the time around puberty (peripubertal time) is presumed to be a susceptible time for the emergence of physical and psychosocial health issues
Poor outcomes have been reported on measures of well-being, body image, self-esteem, mental health, social support, and general health for males with Klinefelter syndrome compared with the general male population. Studies have suggested that the majority of youth with Klinefelter syndrome report poor quality of life, with a risk for depression and/or suicidality. One study found that 68.8% of the affected males studied had clinically significant levels of depressive symptoms. Little is understood about the underlying cause, manifestations, and consequences of depression in affected males. However, depression is a leading cause of disability in adolescents and adults in the general population.
Research has also raised concerns that there is an increased risk for psychiatric disorders besides depression, including anxiety, schizophrenia, and other psychotic disorders.
For those who are diagnosed with Klinefelter syndrome, attention to self-esteem, self-concept, depression risk, and quality of life are important aspects of health care. Early neurocognitive and behavioral interventions for children who have psychosocial vulnerabilities are recommended.
Are men with Klinefelter syndrome able to have children?
The vast majority of people with Klinefelter syndrome are azoospermic (have no sperm present in the ejaculate). However, motile sperms in the ejaculate and even spontaneous pregnancies resulting from fathers with Klinefelter syndrome have been described, although such cases are rare. In general, people with mosaic Klinefelter syndrome (those that also have a 46,XY/47,XXY cell line) are less severely affected so the chance of finding sperm in the ejaculate is significantly higher than in non-mosaic cases (47,XXY). In the past, the use of donor semen or adoption were the only possible ways of having a child. However, in recent years, testicular sperm extraction followed by intracytoplasmic sperm injection (ICSI) have helped more than 100 people with Klinefelter syndrome became biological parents.
People with Klinefelter syndrome should not automatically assume they are infertile without thorough testing.
Are the children of a person with Klinefelter syndrome at increased risk to have the same condition or another chromosome abnormality?
Studies of ejaculated or testicular mature sperm in people with Klinefelter syndrome have shown varying amounts of normal sperm. It has been proposed that adults with Klinefelter syndrome have a substantially higher proportion of sperm with an abnormal number of chromosomes than those without Klinefelter syndrome, giving these people a theoretically increased risk of fathering a child with conditions such as Klinefelter syndrome or 47 XXX syndrome. It has also been proposed that affected people may have an increased risk for sperm with an extra copy of chromosome 13, 18, or 21 3.
Preimplantation genetic diagnosis is generally offered to people Klinefelter syndrome who have undergo successful testicular sperm extraction and intracytoplasmic sperm injection (ICSI). This technique allows for identifying chromosomally abnormal embryos in order to avoid transferring them into the uterus 3.
People interested in learning more about genetic risks and reproductive options should speak with a genetics professional.
Genetics professional online directories are provided by:
- American College of Medical Genetics: https://www.acmg.net/ACMG/Find_Genetic_Services/ACMG/ISGweb/FindaGeneticService.aspx?hkey=720856ab-a827-42fb-a788-b618b15079f9
- National Society of Genetic Counselors: https://www.findageneticcounselor.com/
Klinefelter syndrome prognosis
Babies with the 47, XXY form of Klinefelter differ little from healthy children. The results of one study on non-mosaic XXY infants younger than 2 years indicated that most XXY babies had normal external genitalia and facial features with height and weight in the normal range. Genetic testing had been performed due to a delay in walking and/or speech. Early diagnosis of Klinefelter syndrome is shown to be important to monitor potential developmental problems.
Boys with the 47, XXY karyotype may struggle through adolescence with academics, various frustrations, and, in a few instances, serious emotional or behavioral difficulties. However, most move toward full independence from their families as they enter adulthood. Some have completed graduate education and have a normal level of functioning. Lifespan is not affected by Klinefelter syndrome.
Klinefelter syndrome causes
What causes Klinefelter syndrome
Klinefelter syndrome is a condition related to the sex chromosomes (X and Y chromosomes). Klinefelter syndrome is caused by an additional X chromosome. People typically have two sex chromosomes in each cell: females have two X chromosomes (46,XX), and males have one X and one Y chromosome (46,XY). Most often, Klinefelter syndrome results from the presence of one extra copy of the X chromosome in each cell (47,XXY). Extra copies of genes on the X chromosome interfere with male sexual development, often preventing the testes from functioning normally and reducing the levels of testosterone. Most people with an extra X chromosome have the features described above, although some have few or no associated signs and symptoms.
Some people with features of Klinefelter syndrome have more than one extra sex chromosome in each cell (for example, 48,XXXY or 49,XXXXY). These conditions, which are often called variants of Klinefelter syndrome, tend to cause more severe signs and symptoms than classic Klinefelter syndrome. In addition to affecting male sexual development, variants of Klinefelter syndrome are associated with intellectual disability, distinctive facial features, skeletal abnormalities, poor coordination, and severe problems with speech. As the number of extra sex chromosomes increases, so does the risk of these health problems.
Some people with features of Klinefelter syndrome have the extra X chromosome in only some of their cells; in these individuals, the condition is described as mosaic Klinefelter syndrome (46,XY/47,XXY). Individuals with mosaic Klinefelter syndrome may have milder signs and symptoms, depending on how many cells have an additional X chromosome 4. Approximately 15-20% of cases of Klinefelter syndrome are mosaic 5. The true prevalence is suspected to be greater as there could be cases missed given the varying levels of mosaicism that can be found in different tissues and the potential for males with mosaic Klinefelter syndrome to have more mild symptoms and miss diagnosis 6.
Klinefelter syndrome and its variants are not inherited; these chromosomal changes usually occur as random events during the formation of reproductive cells (eggs and sperm) in a parent. An error in cell division called nondisjunction results in a reproductive cell with an abnormal number of chromosomes. For example, an egg or sperm cell may gain one or more extra copies of the X chromosome as a result of nondisjunction. If one of these atypical reproductive cells contributes to the genetic makeup of a child, the child will have one or more extra X chromosomes in each of the body’s cells. The cause of nondisjunction is unknown. Nondisjunction seems to be a chance event. Nothing that a person does or doesn’t do during their reproductive years can cause these chromosomal changes. We do know that nondisjunction occurs more frequently in the eggs of women as they get older 7.
Mosaic 46,XY/47,XXY is also not inherited. It occurs as a random event during cell division early in fetal development. As a result, some of the body’s cells have one X chromosome and one Y chromosome (46,XY), and other cells have an extra copy of the X chromosome (47,XXY).
Klinefelter syndrome chromosome
Humans have 46 chromosomes, including two sex chromosomes that determine a person’s sex. Females have two X sex chromosomes (XX). Males have an X and a Y sex chromosome (XY).
Chromosomes are packages of genes found in every cell in your body. Two types of chromosome, called the sex chromosomes, determine the genetic sex of a baby. These are named either X or Y.
Usually, a female baby has two X chromosomes (XX) and a male has one X and one Y (XY). But in Klinefelter syndrome, a boy is born with an extra copy of the X chromosome (XXY).
The X chromosome is not a “female” chromosome and is present in everyone. The presence of a Y chromosome denotes male sex.
Klinefelter syndrome can be caused by:
- One extra copy of the X chromosome in each cell (XXY), the most common cause
- An extra X chromosome in some of the cells (mosaic Klinefelter syndrome), with fewer symptoms
- More than one extra copy of the X chromosome, which is rare and results in a severe form
Extra copies of genes on the X chromosome can interfere with male sexual development and fertility.
Klinefelter syndrome signs and symptoms
At birth, most neonates with Klinefelter syndrome (47, XXY) have no dysmorphic or unusual features. Most individuals with Klinefelter syndrome are identified though prenatal diagnosis or when the child does not progress through puberty completely or adequately.
- Infants and young children with Klinefelter syndrome are sometimes initially identified because of an abnormality in the location of the urinary opening in the penis (hypospadias), small penis or testes, or developmental delay (e.g. speech delay).
- Signs and symptoms may include:
- Weak muscles
- Slow motor development — taking longer than average to sit up, crawl and walk
- Delay in speaking
- Quiet, docile personality
- Problems at birth, such as testicles that haven’t descended into the scrotum
- Signs and symptoms may include:
- Older children and teenagers are sometimes diagnosed with Klinefelter syndrome if secondary sexual characteristics do not develop completely, puberty is delayed, testes are small, or breast development may occur. Many males with Klinefelter syndrome are not identified until they have infertility problems as adults.
- Signs and symptoms may include:
- Taller than average stature
- Longer legs, shorter torso and broader hips compared with other boys
- Absent, delayed or incomplete puberty
- After puberty, less muscle and less facial and body hair compared with other teens
- Small, firm testicles
- Small penis
- Enlarged breast tissue (gynecomastia)
- Weak bones
- Low energy levels
- Tendency to be shy and sensitive
- Difficulty expressing thoughts and feelings or socializing
- Problems with reading, writing, spelling or math
- Signs and symptoms may include:
- Men with Klinefelter syndrome may have a relatively increased risk to develop breast cancer. Most males with Klinefelter syndrome have normal intelligence but there is an increased risk of language based learning disorders, dyslexia, and social and executive functioning challenges.
- Signs and symptoms may include:
- Low sperm count or no sperm
- Small testicles and penis
- Low sex drive
- Taller than average height
- Weak bones
- Decreased facial and body hair
- Less muscular than normal
- Enlarged breast tissue
- Increased belly fat
- Signs and symptoms may include:
- Often, boys and men with Klinefelter syndrome will present with verbal communication delays due to language based learning disorders and subtle motor planning deficits. Research has shown, however, that nonverbal capacities in males with Klinefelter syndrome, such as perceptual reasoning and receptive language skills, may be intact or even advanced. Thus, nonverbal IQ is often higher than verbal IQ on neurodevelopmental testing.
- Socially, males with Klinefelter syndrome may have difficulty perceiving social cues and regulating their emotions in stressful situations. They may exhibit autistic traits.
Men with Klinefelter syndrome may have an increased risk for endocrine conditions such as diabetes mellitus, hypothyroidism and hypoparathyroidism and autoimmune diseases such as systemic lupus erythematosus (SLE), Sjogren syndrome and rheumatoid arthritis.
Klinefelter syndrome diagnosis
See your doctor if you have concerns about your son’s development or you notice any troubling symptoms of Klinefelter syndrome in yourself or your son.
Your doctor will likely do a thorough physical exam and ask detailed questions about symptoms and health. This may include examining the genital area and chest, performing tests to check reflexes, and assessing development and functioning.
Your doctor may suspect Klinefelter syndrome after a physical examination and they may suggest sending off a sample of blood to check reproductive hormone levels.
The main tests used to diagnose Klinefelter syndrome are:
- Hormone testing. Blood or urine samples can reveal abnormal hormone levels that are a sign of Klinefelter syndrome.
- Chromosome analysis. Also called karyotype analysis, this test is used to confirm a diagnosis of Klinefelter syndrome. A blood sample is sent to the lab to check the shape and number of chromosomes.
The diagnosis can be confirmed by checking a sample of blood for the presence of the extra X chromosome.
A small percentage of males with Klinefelter syndrome are diagnosed before birth. This might be identified after a pregnant woman has a procedure to examine fetal cells drawn from the amniotic fluid (amniocentesis) or placenta for another reason, such as being older than age 35 or having a family history of genetic conditions.
Klinefelter syndrome treatment
There’s no cure for Klinefelter syndrome, but some of the problems associated with the condition can be treated if necessary.
If you or your son is diagnosed with Klinefelter syndrome, your health care team may include a doctor who specializes in diagnosing and treating disorders involving the body’s glands and hormones (endocrinologist), a speech therapist, a pediatrician, a physical therapist, a genetic counselor, a reproductive medicine or infertility specialist, and a counselor or psychologist.
Although there’s no way to repair the sex chromosome changes due to Klinefelter syndrome, treatments can help minimize its effects. The earlier a diagnosis is made and treatment is started, the greater the benefits. But it’s never too late to get help.
Treatment for Klinefelter syndrome may include:
- Testosterone replacement therapy. Starting at the time of the usual onset of puberty, testosterone replacement can be given to help stimulate changes that normally occur at puberty, such as developing a deeper voice, growing facial and body hair, and increasing muscle mass and penis size. Testosterone therapy can also improve bone density and reduce the risk of fractures. It will not result in testicle enlargement or improve infertility.
- Breast tissue removal. In males who develop enlarged breasts, excess breast tissue can be removed by a plastic surgeon, leaving a more normal-looking chest.
- Speech and physical therapy. These treatments can help boys with Klinefelter syndrome overcome problems with speech, language and muscle weakness. Physiotherapy to help build muscle and increase strength. Occupational therapy to help with any co-ordination problems associated with dyspraxia. Speech and language therapy during childhood to help with speech development.
- Educational evaluation and support. Some boys with Klinefelter syndrome have trouble learning and socializing and can benefit from extra assistance. Talk to your child’s teacher, school counselor or school nurse about what kind of support might help.
- Fertility treatment. Most men with Klinefelter syndrome are unable to father children because few or no sperm are produced in the testicles. For some men with minimal sperm production, a procedure called intracytoplasmic sperm injection (ICSI) may help. During ICSI, sperm is removed from the testicle with a biopsy needle and injected directly into the egg (fertilize the egg) in the laboratory.
- Psychological counseling. Having Klinefelter syndrome can be a challenge, especially during puberty and young adulthood. For men with the condition, coping with infertility can be difficult. A family therapist, counselor or psychologist can help work through the emotional issues.
Testosterone replacement therapy
Testosterone replacement therapy involves taking medication containing testosterone. It can be taken in the form of gels or tablets in teenagers, or given as gel or injections in adult men.
Testosterone replacement therapy may be considered once puberty begins and may help with the development of a deep voice, facial and body hair, an increase in muscle mass, reduction in body fat, and improvement in energy. You should see a specialist in children’s hormones (a pediatric endocrinologist) at this time.
Long-term treatment during adulthood may also help with several other problems associated with Klinefelter syndrome – including osteoporosis, low mood, reduced sex drive, low self-esteem and low energy levels – although it can’t reverse infertility.
How long is testosterone replacement therapy typically used in people with Klinefelter syndrome?
About half of people with a Klinefelter syndrome (47, XXY chromosome) finding have low testosterone levels, which can typically be raised by taking supplemental testosterone. However, not all males with a Klinefelter syndrome (47, XXY chromosome) finding benefit from testosterone therapy. Furthermore, although the majority of people with a 47, XXY chromosome finding and/or Klinefelter syndrome grow up to identify as males, some develop atypical gender identities. For these people, supplemental testosterone may not be appropriate. Gender identity should be discussed with health care specialists before starting treatment.
In most cases, testosterone replacement therapy (sometimes referred to as androgen therapy), is started at puberty (around age 12 for males). The dose is gradually increased until it is enough to maintain age-appropriate serum concentrations of testosterone, estradiol, follicle-stimulating hormone (FSH), and luteinizing hormone (LH). Regular testosterone injections can promote strength and facial hair growth; build a more muscular body type; increase sexual desire; enlarge the testes; improve mood, self-image, and behavior; and protect against early osteoporosis.
Limited information about the treatment of adults with Klinefelter syndrome is available; however, research has shown that continued testosterone injections, even if begun in adulthood, can be beneficial to those seeking treatment and may continue to help with hypogonadism, low libido (sex drive), and psychosocial issues. People with Klinefelter syndrome should consult their physicians regarding their personal course of treatment and to discuss the risks and benefits of testosterone replacement therapy.
Coping and support
Treatment, health education and social support can greatly benefit individuals with Klinefelter syndrome.
Boys with Klinefelter syndrome
If you have a son with Klinefelter syndrome, you can help promote healthy mental, physical, emotional and social development.
- Learn about Klinefelter syndrome. Then you can provide accurate information, support and encouragement.
- Monitor your son’s development carefully. Seek help for problems you notice, such as trouble with speech or language.
- Keep regular follow-up appointments with medical professionals. This may help prevent future problems.
- Encourage participation in sports and physical activities. These activities will help build muscle strength and motor skills.
- Encourage social opportunities and participation in group activities. These activities can help develop social skills.
- Work closely with your son’s school. Teachers, school counselors and administrators who understand your son’s needs can make a big difference.
- Learn what support is available. For example, ask about special education services, if needed.
- Connect with other parents. Klinefelter syndrome is a common condition, and you — and your son — aren’t alone. Ask your doctor about internet resources and support groups that may help answer questions and ease concerns.
Men with Klinefelter syndrome
If you have Klinefelter syndrome, you may benefit from these self-care measures:
- Work closely with your doctor. Appropriate treatment can help you maintain your physical and mental health and prevent problems later in life, such as osteoporosis.
- Investigate your options for planning a family. You and your partner may want to talk to a doctor or other health professional about your options.
- Talk with others who have the condition. There are a number of resources that provide information about Klinefelter syndrome and can offer the perspectives of other men and their partners who cope with the condition. Many men also find it helpful to join a support group.
More information and support
If you or your son has been diagnosed with Klinefelter syndrome, you might find it useful to find out more about it and get in touch with others affected by it.
The following websites may be able to help:
- Association for X and Y Chromosome Variations (AXYS): https://genetic.org/
- American Association for Klinefelter Syndrome Information and Support: http://www.aaksis.org/
Mental health therapists or counselors, including psychologists and psychiatrists, can help males with Klinefelter syndrome find ways to cope with feelings of sadness, depression, self-doubt, and low self-esteem. These professionals can also help families deal with the emotions of having a son with Klinefelter syndrome.
People who are concerned about their child’s behaviors should seek appropriate care:
- Talk to the child’s doctor, school nurse, or another health care provider and seek further information about the behaviors or symptoms that are causing worry
- Ask the child’s primary care physician or other health care provider for a referral to a specialist with experience in child emotional and/or behavioral problems
Suicide warning signs
- Talking about suicide – Any talk about suicide, dying, or self-harm, such as “I wish I hadn’t been born,” “If I see you again…” and “I’d be better off dead.”
- Seeking out lethal means – Seeking access to guns, pills, knives, or other objects that could be used in a suicide attempt.
- Preoccupation with death – Unusual focus on death, dying, or violence. Writing poems or stories about death.
- No hope for the future – Feelings of helplessness, hopelessness, and being trapped (“There’s no way out”). Belief that things will never get better or change.
- Self-loathing, self-hatred – Feelings of worthlessness, guilt, shame, and self-hatred. Feeling like a burden (“Everyone would be better off without me”).
- Getting affairs in order – Making out a will. Giving away prized possessions. Making arrangements for family members.
- Saying goodbye – Unusual or unexpected visits or calls to family and friends. Saying goodbye to people as if they won’t be seen again.
- Withdrawing from others – Withdrawing from friends and family. Increasing social isolation. Desire to be left alone.
- Self-destructive behavior – Increased alcohol or drug use, reckless driving, unsafe sex. Taking unnecessary risks as if they have a “death wish.”
- Sudden sense of calm – A sudden sense of calm and happiness after being extremely depressed can mean that the person has made a decision to attempt suicide.
Many professional associations have listings of mental health providers, including:
- American Psychiatric Association: http://finder.psychiatry.org/
- American Psychological Association: https://locator.apa.org/
- Association for Behavioral and Cognitive Therapies: http://www.findcbt.org/xFAT/
Seek immediate assistance if you think your child is in danger of harming themselves or others. You can call a crisis line:
If you think you may attempt suicide, get help now:
- Call your local emergency number immediately.
- Call a suicide hotline number.
- In the U.S., call the National Suicide Prevention Lifeline (https://suicidepreventionlifeline.org/) at 1-800-273-8255. Use that same number and press “1” to reach the Veterans Crisis Line. Or call the National Hopeline Network at 1-800-784-2433
- In the UK and Ireland – call the Samaritans at 116-123
- In Australia – call Lifeline Australia at 13-11-14
- In other countries – Visit International Association for Suicide Prevention at http://www.iasp.info/resources/Crisis_Centres or Suicide.org to find a helpline in your country at http://www.suicide.org/international-suicide-hotlines.html.
These free helplines are there to help when you’re feeling down or desperate.
They’re open 24 hours a day, every day.
- Learning About Klinefelter Syndrome. https://www.genome.gov/19519068/[↩]
- Klinefelter syndrome. Genetics Home Reference (GHR). https://ghr.nlm.nih.gov/condition/klinefelter-syndrome[↩]
- Aksglaede L, Juul A. Therapy of endocrine disease: Testicular function and fertility in men with Klinefelter syndrome: a review. Eur J Endocrinol. March 15, 2013; 168(4):R67-76.[↩][↩]
- Klinefelter syndrome. Genetics Home Reference. https://ghr.nlm.nih.gov/condition/klinefelter-syndrome[↩]
- Chembolli Lakshmi, Selvaraj Swarnalakshimi. Acne in Klinefelter Syndrome-46XY/47XXY Mosaicism?. Indian J Dermatol.. 2015; 60(5):494-496. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4601420/[↩]
- Samplaski MK, Lo KC, Grober ED, Millar A, Dimitromanolakis A, Jarvi KA. Phenotypic differences in mosaic Klinefelter patients as compared with non-mosaic Klinefelter patients. Fertil Steril. April 2014; 101(4):950-5. https://www.ncbi.nlm.nih.gov/pubmed/24502895[↩]
- NONDISJUNCTION. http://www.omim.org/entry/158250[↩]





{kind=link}