Contents
What is agnosia
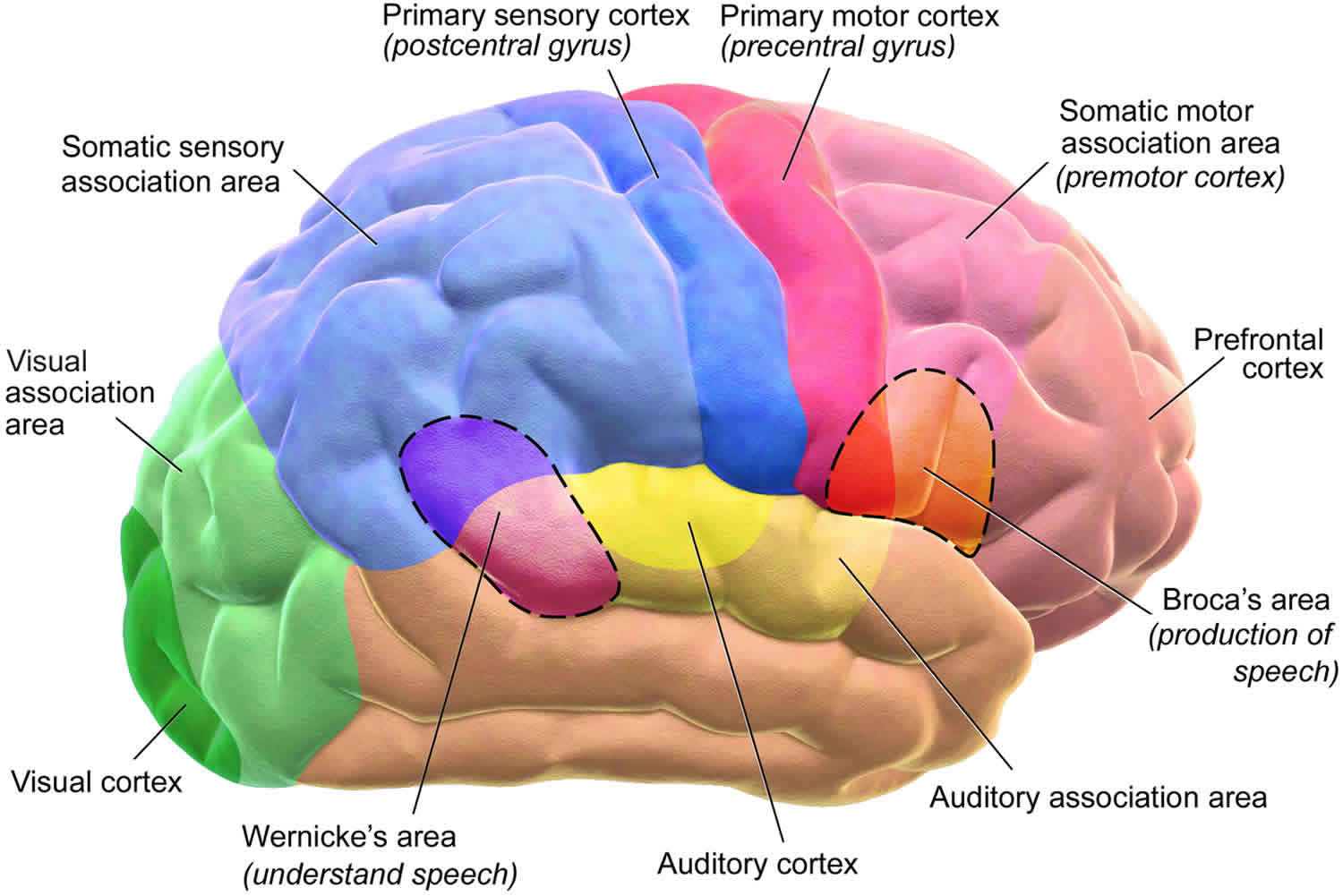
Agnosia is a rare disorder whereby a patient is unable to recognize and identify objects, persons, or sounds using one or more of the senses despite otherwise normally functioning senses 1. The deficit cannot be explained by memory, attention, language problems, or unfamiliarity to the stimuli. Agnosia symptoms may vary, according to the area of the brain that is affected. Agnosia can be limited to one sensory modality such as vision or hearing; for example, a person may have difficulty in recognizing an object as a cup or identifying a sound as a cough. Agnosia can result from strokes, traumatic brain injury, dementia, a tumor, developmental disorders, overexposure to environmental toxins (e.g., carbon monoxide poisoning), or other neurological conditions 2. Visual agnosia may also occur in association with other underlying disorders. Agnosia happens when there is brain damage along pathways that connect primary sensory processing areas. These areas typically include the posterior parietal cortex and occipitotemporal regions. Agnosia typically results from damage to specific brain areas in the occipital or parietal lobes of the brain. People with agnosia may retain their cognitive abilities in other areas 2.
Less than 1% of all neurological patients have agnosia. Visual agnosia is the most common and better-described type of agnosia 3.
Classically, there are 2 forms of agnosia: apperceptive and associative.
- Apperceptive agnosia is a failure in recognition due to deficits in early stages of perceptual processing.
- Associative agnosia is a failure in recognition despite no deficit in perception. Associative agnosia patients can typically draw, matc
Diagnosis is mainly clinical, based on clinical history and physical examination including a thorough neurologic exam, psychological exam, and certain standardized tests of brain function. Referrals to ophthalmology, speech pathology, audiology, psychiatry, and other professionals may be needed for detailed evaluation of sensory and neurobehavioral status. Once a tentative diagnosis of agnosia is made, a thorough neuropsychological examination is done to test intelligence, memory function, linguistic competence, and assess sensory-perceptual processing.
A variety of psychophysical tests can be conducted to pinpoint the nature of the visual process that is disrupted in an individual. Brain damage that causes visual agnosia may be identified through imaging techniques, including computed tomography (CT scan) and magnetic resonance imaging (MRI).
Agnosia can considerably limit the everyday functioning of the patients. It can also significantly affect the lives of family and caretakers. There is no direct cure.
Treatment of primary agnosia is symptomatic and supportive; when it is caused by an underlying disorder, treatment of the disorder may reduce symptoms and help prevent further brain damage 2. Rehabilitation with speech or occupational therapists can help patients learn to compensate for their deficits.
Agnosia prognosis depends on the nature and extent of damage and patient age. There is no specific treatment, but speech and occupational therapy may help patients compensate 1.
Agnosia types
Discrete brain lesions can cause different forms of agnosia, which may involve any sense. Typically, only one sense is affected:
- Hearing (auditory agnosia—the inability to identify objects through sound such as a ringing telephone)
- Taste (gustatory agnosia)
- Smell (olfactory agnosia)
- Touch (tactile agnosia)
- Sight (visual agnosia)
Other forms of agnosia involve very specific and complex processes within one sense.
Prosopagnosia is inability to identify well-known faces, including those of close friends, or to otherwise distinguish individual objects among a class of objects, despite the ability to identify generic facial features and objects. Prosopagnosia often accompanies damage to the inferotemporal lobe—often bilateral small lesions, especially in the fusiform gyrus.
Anosognosia is lack of awareness that a deficit exists or lack of insight into an existing deficit. It often accompanies damage to the right, nondominant parietal lobe (which is usually due to an acute stroke or traumatic brain injury). Patients with multiple impairments can be unaware of one impairment but fully aware of others. Patients with anosognosia may deny their motor deficit, insisting that nothing is wrong even when one side of their body is completely paralyzed. When shown the paralyzed body part, patients may deny that it is theirs.
In an often related phenomenon, patients ignore the paralyzed or desensitized body parts (hemi-inattention) or the space around them (hemineglect). Hemineglect most often involves the left side of the body.
Somatosensory agnosia can also result from lesions in the parietal lobe. Patients with somatosensory agnosia have difficulty identifying a familiar object (eg, key, safety pin) that is placed in the hand on the side of the body opposite the damage. However, when they look at the object, they immediately recognize and can identify it.
Occipitotemporal lesions may cause:
- An inability to recognize familiar places (environmental agnosia)
- Visual disturbances (visual agnosia)
- Color blindness (achromatopsia)
Right-sided temporal lesions may cause:
- An inability to interpret sounds (auditory agnosia)
- Impairment of music perception (amusia)
Visual agnosia
Visual agnosia refers to an impairment in recognizing visually presented objects, despite otherwise normal visual field, acuity, color vision, brightness discrimination, language, and memory. Patients can recognize objects using other sensory modalities. Sometimes impairment is worse for certain types of objects, so a variety of objects should be tested to diagnose precisely. Visual agnosia is the most common and better-understood agnosia.
Visual agnosia is further divided in 2 subtypes: apperceptive visual agnosia and associative visual agnosia 3.
- Apperceptive visual agnosia refers to an abnormality in visual perception and discriminative process, despite the absence of elementary visual deficits. These people are unable to recognize objects, draw, or copy a figure. They cannot perceive correct forms of the object, although knowledge of the object is intact. Apperceptive visual agnosia is typically associated with lesions to the parietal, occipital cortex
- Associative visual agnosia refers to difficulty with understanding the meaning of what they are seeing. They can draw or copy but do not know what they have drawn. They correctly perceive the form and know the object when tested with verbal or tactile information, but cannot identify the object. They are unable to link the fully perceived visual stimulus to prior experience to help them recognize the stimulus. Associative visual agnosia is usually associated with damage to the bilateral inferior occipitotemporal cortex.
Types of visual agnosia
- Prosopagnosia is the inability to recognize familiar faces. Patients can often identify other aspects like gender, hair, emotions. Prosopagnosia results from damage to fusiform face area (located in the inferior temporal cortex in fusiform gyrus). People with apperceptive prosopagnosia cannot perceive facial expression and cues but can recognize non-facial clues like hair and clothing. Associative prosopagnosia patients can derive some facial information like gender and age. Mr. P in Oliver Sack’s book The Man Who Mistook His Wife for a Hat presents a classic case of prosopagnosia.
- Simultanagnosia is the inability to recognize and sort out objects when they appear together, but they can recognize them when they appear alone. Patients are unable to perceive the overall meaning of a picture or multiple things together, although they can describe isolated elements. Two forms of simultagnosia have been described.
- Dorsal simultagnosia: Patients cannot see more than one object at a time. For example, when presented with a picture with table, chair and flower vase, they may report only one thing at a time. When their attention is diverted to the other thing, they can then identify only that thing; other things disappear to them. They often have difficulty reading as it involves viewing more than one word at a time. They often bump into objects that are close together. Dorsal simultagnosia is typically associated with lesions in the bilateral occipitotemporal cortex.
- Ventral simultagnosia: These individuals also cannot identify more than one object or complex objects at one time, although they can see more than one object at a time. They are unable to perceive the whole picture as one and derive a meaning out of it. For example, in a night sky picture with stars and full moon, they may identify moon as a ball, unable to derive the meaning of the whole picture. Ventral Simultagnosia is associated with lesions in the left inferior occipital area.
- Color agnosia is the inability to identify and distinguish colors, despite intact basic color vision and brightness discrimination mechanisms. It is very difficult to diagnose this type of agnosia as colors can only be appreciated visually. Usually, these patients have a lesion in the left occipitotemporal region of the brain.
- Topographical agnosia is the inability to orient to surroundings because of inability to interpret the spatial information. These patients have a good memory of the layout and specifics of the places well known to them, but they are unable to navigate their way through. They are unable to use the visual cues to guide them in the right direction. Associated with a lesion in the right posterior cingulate area of the brain.
- Finger agnosia is a difficulty in naming and differentiating among the fingers of either hand as well the hand of others. It does not refer to the inability to identify a finger as a finger, as the name may suggest. It is a part of the constellation of symptoms often referred to as Gerstmann syndrome which includes acalculia, agraphia, finger agnosia, and left-right disorientation.
- Akinetopsia refers to the inability to perceive motion.
- Agnostic alexia refers to the inability to recognize words visually (they can still write and talk without difficulty).
Auditory Agnosia
Auditory agnosia is an inability to recognize sounds despite intact hearing. Auditory agnosias are typically associated with right side temporal lesions.
Types of Auditory Agnosia
- Phonagnosia is the inability to recognize familiar voices. They can recognize words spoken by others. It is caused by damage to certain parts of sound association region.
- Verbal auditory agnosia or pure word deafness is the inability to comprehend spoken words but can read, write, and speak in a relatively normal manner.
- Nonverbal auditory agnosia is the inability to comprehend nonverbal sounds and noises, with sparing of speech comprehension.
- Amusia is the inability to recognize the music. They are unable to comprehend that certain types of sounds represent music and therefore cannot distinguish music from other sounds.
Tactile Agnosia
Tactile agnosia refers to the inability to recognize objects by touch. They can name objects by sight.
- Amorphognosia is the inability to identify the size and shape of objects by touch, for example, a triangle or square.
- Anosognosia is the inability to identify distinctive qualities like texture and weight, for example, a piece of wood, cotton or metal.
- Tactile asymbolia is impaired recognition by touch in the absence of amorphognosia and ahylognosia.
Agnosia causes
Primary visual agnosia occurs as a result of damage to the brain. Symptoms develop due to the inability to retrieve information from those damaged areas that are associated with visual memory. Lesions may occur as a result of traumatic brain injury, stroke, tumor, or overexposure to dangerous environmental toxins (e.g., carbon monoxide poisoning). In some cases, the cause of the brain damage may not be known. Symptoms may vary, according to the area of the brain that is affected.
Visual agnosia may also occur in association with other underlying disorders (secondary visual agnosia) such as Alzheimer’s disease, agenesis of the corpus callosum, mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes (MELAS), and other diseases that result in progressive dementia. Disorders that may precede the development of primary visual agnosia (and may be useful in identifying an underlying cause of some forms of this disorder) include Alzheimer’s disease, Pick’s disease, and a rare disorder called Balint’s syndrome.
Is there a known genetic cause for agnosia?
Agnosia has been found to have many causes. For several types of agnosia, including prosopagnosia (an inability to recognize faces) and color agnosia, articles in the medical literature describe families in which multiple relatives have similar symptoms 4, 5, 6. The authors of these articles suggest this is evidence of a genetic factor contributing to agnosia in these families 4, 5, 6. However, a specific gene has not yet been found to cause agnosia.
Agnosia symptoms
People with primary visual agnosia may have one or several impairments in visual recognition without impairment of intelligence, motivation, and/or attention. Vision is almost always intact and the mind is clear. Some affected individuals do not have the ability to recognize familiar objects. They can see objects, but are unable to identify them by sight. However, objects may be identified by touch, sound, and/or smell. For example, affected individuals may not be able to identify a set of keys by sight, but can identify them upon holding them in their hands.
Some researchers separate visual agnosia into two broad categories: apperceptive agnosia and associative agnosia. Apperceptive agnosia refers to individuals who cannot properly process what they see, meaning they have difficult identifying shapes or differentiating between different objects (visual stimuli). Affected individuals may not be able to recognize that pictures of the same object from different angles are of the same object. Affected individuals may be unable to copy (e.g., draw a picture) of an object. Associative agnosia refers to people who cannot match an object with their memory. They can accurately describe an object and even draw a picture of the object, but are unable to state what the object is or is used for. However, if told verbally what the object is, an affected individual will be able to describe what it is used for.
In some cases, individuals with primary visual agnosia cannot identify familiar people (prosopagnosia). They can see the person clearly and can describe the person (e.g., hair and eye color), but cannot identify the person by name. People with prosopagnosia may identify people by touch, smell, speech, or the way that they walk (gait). In some rare cases, affected individuals cannot recognize their own face.
Some people have a form of primary visual agnosia associated with the loss of the ability to identify their surroundings (loss of environmental familiarity agnosia). Symptoms include the inability to recognize familiar places or buildings. Affected individuals may be able to describe a familiar environment from memory and point to it on a map.
Simultanagnosia is a characterized by the inability to read and the inability to view one’s surroundings as a whole. The affected individual can see parts of the surrounding scene, but not the whole. There is an inability to comprehend more than one part of a visual scene at a time or to coordinate the parts.
In rare cases, people with primary visual agnosia may not be able to recognize or point to various parts of the body (autotopagnosia). Symptoms may also include loss of the ability to distinguish left from right.
Agnosia diagnosis
Diagnosis is mainly clinical, based on clinical history and physical examination including a thorough neurologic exam, psychological exam, and certain standardized tests of brain function. It is important to make sure that the abnormality cannot be explained in another way, for example, genuine unfamiliarity with the stimuli, poor instructions, overlooked disease like neuropathy and cataracts, or other neurologic conditions like dyspraxia or dysphasia.
Various standardized tests are available to test for memory and cognition (MMSE, Montreal Cognitive assessment, ADAS-cog) and aphasia (Boston naming test, western aphasia battery).
Diagnosis is supplemented by neuroimaging tests such as head CT and brain MRI to look for etiology. More testing may be needed based on clinical judgment and suspected etiology. Auditory or visual evoked potentials may be used to determine whether a deficit exists in the sensory projection area as opposed to primary sensory or association cortex.
Careful patient history is very important in cases of suspected agnosia. Clues to diagnosis and cause often involve a detailed interview with the patient, family members, and caregivers. It is harder to diagnose when the patient lacks the insight of his or her deficits. History will reveal clues pointing to the type of agnosia. For example, a patient with visual agnosia will specify problems in day-to-day life, for example, getting dressed or inability to differentiate fork and a knife because of inability to recognize certain types of objects visually. Patients with topographical agnosia will present with getting often lost, findings directions. Patients with akinetopsia often bump in things, get confused how things got moved around, have difficulty in crossing roads and driving and are accident prone. Patients with simultagnosia will often have trouble reading and writing and interpreting multiple things at a time.
Other important points to elicit in history can confirm that other sensory modalities, memory, and cognition are not affected.
Initial assessment involves asking patients to identify common objects through sight, touch, and smell. A thorough physical examination is done to detect for any primary deficits in individual senses (visual fields, acuity, reading, drawing, hearing tests, among others) or in the ability to communicate that may interfere with identifying the objects (memory, cognition, attention, aphasia).
An important aspect of diagnosing agnosia is ruling out alternative explanations. Recognition disturbance can occur in many other neurological conditions, but agnosia can be diagnosed only in the absence of aphasia, generalized dementia, delirium, or any deficit that may impair some or all of the information-processing steps involved in object recognition.
It is very important to rule out genuine unfamiliarity with stimuli. It is important to consider cultural and life experience and other factors that may lead to unfamiliarity. Testing of common objects and constructing a balanced set of items that are determined individually should be done.
For example, to assess for visual agnosia, show the patient several familiar items like keys, a pen, and a banana and ask to name them. Differentiating visual agnosia and aphasia is important. For prosopagnosia, show the patient pictures of famous people, their family members, and themselves. For color agnosia, show solid color cards and ask them to name the colors. For simultagnosia, present pictures with several objects or people and ask them to identify what they see. For tactile agnosia, make sure patient is unable to see, then put common things in each hand one by one and ask the patient to identify by touch alone. Inability to correctly identify at least 50% of stimuli tested will suggest the diagnosis of agnosia.
Agnosia treatment
Agnosia treatment is generally symptomatic and supportive. The primary cause of the agnosia should be determined in order to treat other problems that may contribute to or result in agnosia. When possible, the cause of agnosia is treated (e.g., surgery and/or antibiotics for cerebral abscess, surgery and/or radiation for brain tumor).
Agnosia is managed supportively. Rehabilitation, speech, and occupational therapy play an important role in the treatment of agnosia and mainly focus on teaching patients to use the intact sensory modalities to compensate. Restorative training has limited utility. Interventions tend to focus on helping these patients and their family and caregivers cope and adapt to the condition, and furthermore, to help patients function independently within their context. Counseling of family members and helping them with behavioral changes is equally important.
Rehabilitation approaches need to be individualized and should focus on the specific deficit by developing compensatory strategies.
Alternative Cues and Strategies
Some general strategies that can be used are alternative cues, for example, teaching people with prosopagnosia learn to identify any facial scars or hairstyles. For patients with visual agnosia, teaching alternative strategies like learning to identify everything by touch; in patients with prosopagnosia, teaching voice recognition for people; and teaching patients with auditory agnosia to lip read and write everything.
Organizational Strategies
- Provide a predictable environment and consistency in performing a task, for example, placing things in the same place every day. Routines help develop consistency in performing a task.
- Declutter, for example, things patients use every day should be kept out in one place. This may help patients with visual agnosia.
- Label everything
Agnosia prognosis
Recovery from agnosia may be influenced by the:
- Type, size, and location of lesions
- Degree of impairment
- Patient age
- Effectiveness of therapy
Few patients with agnosia regain their sensory function. If the cause is self-limited or reversible, most recovery occurs within the first 3 months, but recovery may continue to a variable degree up to a year.
- Agnosia. https://www.merckmanuals.com/professional/neurologic-disorders/function-and-dysfunction-of-the-cerebral-lobes/agnosia[↩][↩]
- Agnosia Information Page. https://www.ninds.nih.gov/Disorders/All-Disorders/Agnosia-Information-Page[↩][↩][↩]
- Kumar A, Wroten M. Agnosia. [Updated 2019 Jan 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK493156[↩][↩]
- Mitchell KJ. Curiouser and curiouser: genetic disorders of cortical specialization. Current Opinion in Genetics &Development. 2011; 21(3):271-277. http://www.ncbi.nlm.nih.gov/pubmed/21296568[↩][↩]
- Duchaine B, Germine L, Nakayama K. Family resemblance: ten family members with prosopagnosia and within-class object agnosia. Cognitive Neuropsychology. 2007; 24(4):419-430. http://www.ncbi.nlm.nih.gov/pubmed/18416499[↩][↩]
- Nijboer TC, van Zandvoort MJ, de Haan EH. A familial factor in the development of colour agnosia. Neuropsychologia. 2007; 45(8):1961-1965. http://www.ncbi.nlm.nih.gov/pubmed/17337019[↩][↩]




{kind=link}