
Contents
What is allergic sinusitis
Allergic fungal sinusitis is a benign noninvasive sinus disease related to a hypersensitivity reaction to fungal antigens. A wide variety of fungal agents has been implicated, with the vast majority belonging to the Dematiaceae family. Allergic fungal sinusitis should be suspected in any atopic patient with refractory nasal polyps.
Fungi are eukaryotic, filamentous and mostly spore-bearing heterotrophic organisms that depend on external nutrients and therefore live as saprophytes, parasites or symbionts of animals and plants under nearly all environmental conditions. The phenotype of molds ranges from a unicellular to a dimorphic or filamentous appearance. Out of over 100,000 fungal species reported, a few hundred occur as opportunists and about 100 are known to elicit mycoses in man and animals 1. More than 80 mold genera have been shown to induce type I allergies in susceptible persons, whereas allergenic proteins have been identified in 23 fungal genera.
The Bent and Kuhn diagnostic criteria 2 is the standard for diagnosis of the allergic fungal sinusitis disease, including the following major criteria:
- Characteristic computed tomography (CT) findings of chronic paranasal sinusitis,
- Nasal polyposis,
- Allergic mucin,
- Identification of fungi in the paranasal sinus contents without fungal invasion of the tissue and
- Type I allergy confirmed by history, positive skin tests or serology.
Fungal sinusitis is classically divided into non-invasive (fungal ball, allergic fungal sinusitis, saprophytic fungal growth) and invasive forms (acute invasive fungal sinusitis, chronic invasive fungal sinusitis, chronic granulomatous fungal sinusitis) (Table 1) 3. Invasive fungal sinusitis is a life-threatening entity involving fungal species such as Mucor and Aspergillus that, in the immunosuppressed host, become invasive, and extend beyond the bony boundaries of the sinuses and skull base 3. The morbidity and mortality associated with invasive fungal sinusitis are high, especially for acute invasive fungal sinusitis 4.
Table 1. Fungal sinusitis definitions/categories
| Subtype | Commonly affected sinuses | Immune system characterization | Common causative fungus | Histopathology | Classic Imaging Findings | Symptoms | Management | Outcome | |
|---|---|---|---|---|---|---|---|---|---|
| Non- Invasive | Fungal Ball | Maxillary and sphenoid sinus | Immuno-competent | Aspergillus species | Sinus contents: dense tangles of hyphae with calcification and oxalate crystals | CT: Single opacified sinus w/o erosion MRI: hypointense sinus content T1, T2 | Asymptomatic, Or symptomatic as nonspecific chronic rhinosinusitis | 1) Endoscopic debridement 2) Repeated topical irrigations | Excellent; rare local recurrence |
| Allergic Fungal Sinusitis | Bilateral sinuses affected, one side often more severe | Immuno-competent, Hx of allergic rhinosinusitis and/or asthma, Type 1 hypersensitivity to fungi | Aspergillus fumigatus, Dematiaceous species | Hyphae present but scarce, eosinophilic mucin without fungal invasion into sinus tissue; Charcot-Leyden crystals present | CT: hyperattenuated mucin with in sinuses, thinning of sinus walls MRI: T1 variable, T2 hypointense sinus content | Symptomatic as nonspecific chronic rhinosinusitis | 1) Endoscopic debridement 2) Repeated topical irrigation 3) Topical and/or oral steroids | Favorable, common loco-regional recurrence | |
| Saprophytic Fungal Growth | Non-specific | Immuno-competent | Aspergillus | N/A | N/A | Not symptomatic | None, removal during nasal endoscopy | Excellent | |
| Pre- Invasive | Pre-invasive Fungal Sinusitisa | Sphenoid | Immuno-compromised and immuno-competent | Culture negative | Submucosal presence of septated hyphae without angioinvasion | CT: sphenoid sinus opacity w/or w/o erosion MRI: variable in T1, T2 | - Fever - Headache - Visualloss | 1) Limited endoscopic debridement without serial re-inspection 2) Short term antifungal use possible | Favorable |
| Invasive | Acute Invasive Fungal Sinusitis | Non-specific; middle turbinate mucosa is frequently involved | Almost always immuno- compromised | Aspergillus, Rhizopus and Mucor species | Fungal hyphae in mucosa that invades blood vessels or bones with tissue necrosis and neutrophilic infiltration | CT: mucosal thickening, bone erosion, soft tissue infiltration MRI: variable on T1, T2; lack of mucosal enhancement with contrast | - Fever - Facial swelling - Nasal congestion - Diplopia - Decreased vision - Nasal discharge - Facial pain - Headache | 1) Aggressive surgical debridement 2) Immune restoration therapy 3) High dose antifungal therapy | High mortality, possibility of recurrence |
| Chronic Invasive Fungal Sinusitis | Ethmoid, sphenoid | Immuno-competent and immuno-compromised secondary to numerous causes of immune dysfunction | Aspergillus fumigatus, mucor | Presence of a dense fungal element, infiltration of mucosa and angioinvasion with a nonspecific inflammatory response, and necrosis of adjacent tissue | CT: hyperattenuating intranasal soft tissue mass ± calcification within ≥ one sinus and ± bone erosion or sinus expansion MRI: decreased signal on T1 and T2 | - Rhinosinusitis symptoms - Proptosis - Diplopia - Visualloss - Cranial nerve deficit - Cavernous sinus syndrome - Orbital apex syndrome | 1) Aggressive surgical debridement 2) Immune restoration therapy 3) Antifungal therapy | Moderate, variable | |
| Granulo-matous Invasive Fungal Sinusitis | Non-specific | Immuno-competent | Aspergillus flavus | Noncaseating granulomas with giant cells and plasma cells with surrounding vasculitis and perivascular fibrosis | Overlaps with imaging findings from chronic invasive fungal sinusitis (above) | - Enlarging mass in the sinonasal cavity - Proptosis | 1) ± antifungal therapy 2) ± surgical debridement | Uncertain |
It is believed that allergic fungal sinusitis is a type I-mediated allergic reaction. The majority are associated with the members of the ascomycota or the basidiomycota, and Calvatia, Coprinus, Ganoderma, Pleurotus and Psilocybe are the most prominent genera of the basidiomycota 6.
Allergic fungal sinusitis is considered as a special type of chronic rhinosinusitis and the primary treatment for Allergic fungal sinusitis is surgery. Functional endoscopic sinus surgery is the gold standard surgical treatment for chronic rhinosinusitis 7. Allergic fungal sinusitis constitutes 5%–7% of all cases of chronic rhinosinusitis that require surgery 8. Most series were from medical centers in the southern United States 9.
The optimal medical therapy for allergic fungal sinusitis has not been determined 7. Systemic steroids are the mainstay of therapy in allergic bronchopulmonary aspergillosis. However, steroids have multiple side effects and their use is controversial. It has been suggested that patients with recurrent allergic fungal sinusitis should have receive systemic corticosteroids after extensive debridement of all affected sinuses. After 2 weeks this is gradually reduced to alternate day therapy at lower doses 10. The eventual aim is for maintenance inhaled corticosteroid therapy. Topical intranasal steroid sprays have minimal side effects and are used routinely in the postoperative management of allergic fungal sinusitis. However, the duration and effectiveness of steroid sprays in allergic fungal sinusitis has not been proven scientifically. The role of antifungal therapy in treatment of allergic fungal sinusitis is unclear. Since allergic fungal sinusitis is thought to be an allergic disease caused by an extrinsic fungal antigen rather than a true infection, systemic antifungals should be ineffective. Topic antifungal agent irrigation may reduce the fungal load and hence decrease antigenic stimuli.
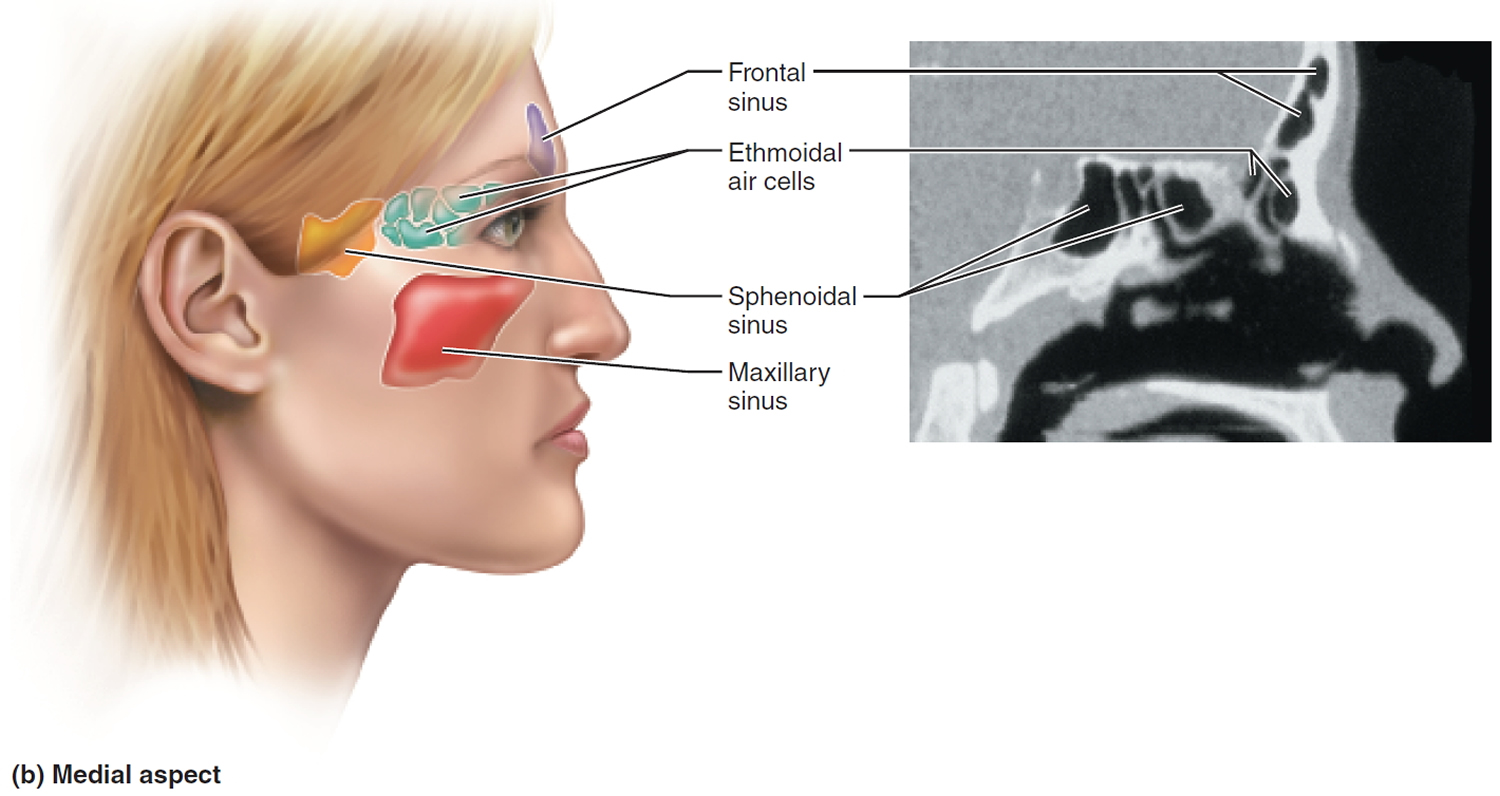
The sinuses
The paranasal sinuses are spaces in the bones of the skull which are mainly full of air. The paranasal sinuses include:
- the sphenoid sinus – in the centre of the head;
- the maxillary sinuses – situated in the cheekbones;
- the frontal sinuses – above the eyes; and
- the ethmoidal sinuses – on either side of the nose.
The lining of the sinuses produces clear fluid – mucus – which cleans them. This fluid passes through narrow drainage passages into the back of the nose and throat, from where it is swallowed. This happens continually, although we are usually unaware of it.
Because the drainage holes from the sinuses are narrow, they block up easily. So any excess mucus production can cause a blockage, and pressure builds up in the sinuses.
The 2 main causes of excess mucus production are:
- Infection; and
- Allergy.
Figure 1. Paranasal sinuses

Allergic fungal sinusitis symptoms
Individuals with allergic fungal sinusitis experience symptoms typical of chronic sinusitis (chronic rhinosinusitis), including nasal congestion, facial pain/pressure, nasal discharge, and diminished olfaction. From an epidemiological perspective, allergic fungal sinusitis patients are younger, more likely to be male subjects, and more likely to be black American than other patients with chronic sinusitis (chronic rhinosinusitis) and nasal polyps 11. An estimated 5–10% of chronic sinusitis (chronic rhinosinusitis) patients requiring surgery have allergic fungal sinusitis 12, although a distinct geographic variation exists with cases concentrated in warm, humid climates such as the southeastern United States and India 13. Patients typically have an intact immune system and often have a history of atopy, including allergic rhinitis and/or asthma.
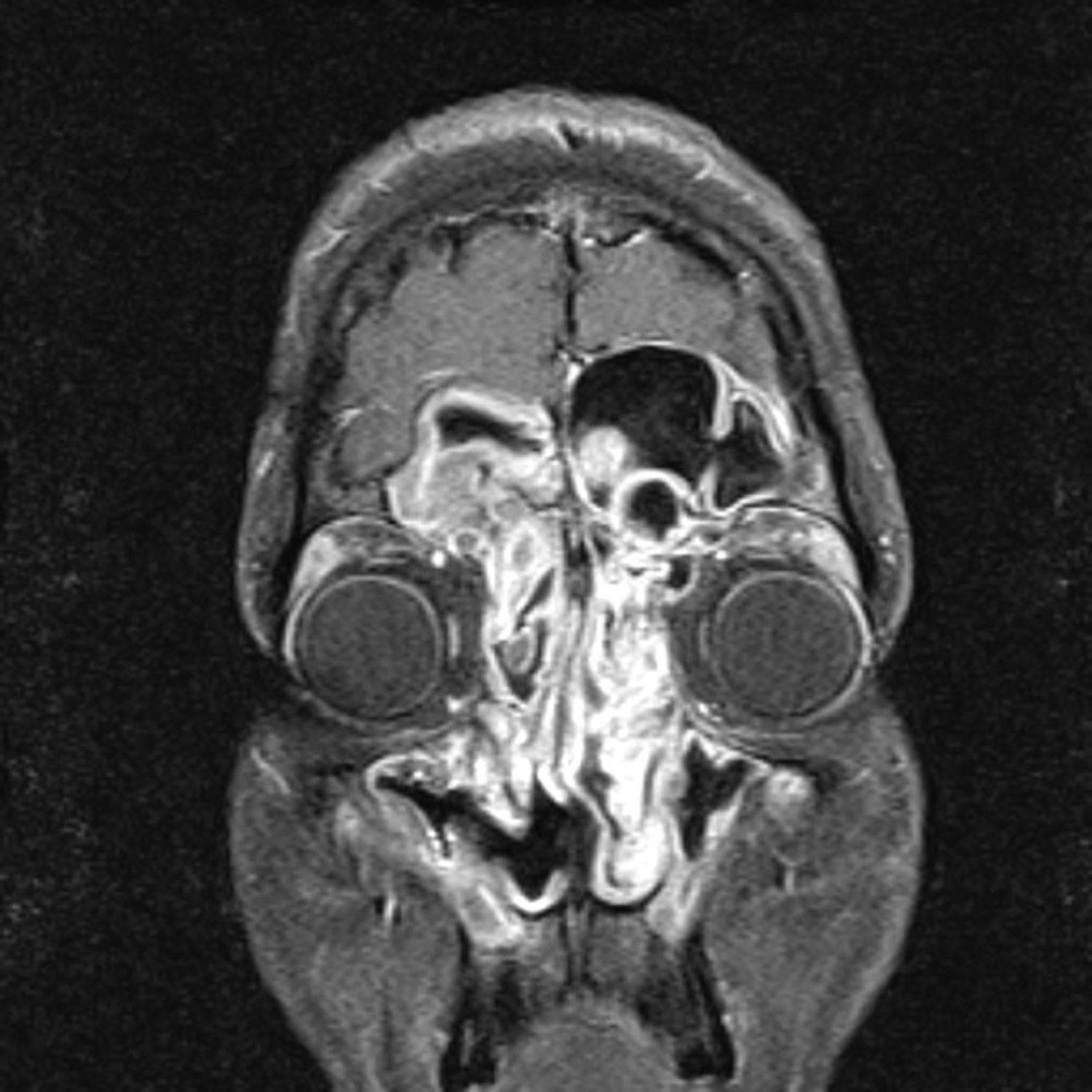
A diagnosis of allergic fungal sinusitis is often suspected based on radiographic characteristics 14. Hyperattenuated mucin is often visible within the sinus lumen on CT scan and in many cases there has been progressive expansion and thinning of sinus walls. In select cases, bone can be completely eroded such that sinus mucosa is in direct apposition with underlying dura 15. Multiple sinuses are typically affected in a bilateral fashion, although radiographic findings are often more severe on one side than the other. T1-weighted MRI may show mixed signal intensities, whereas T2-weighted images are frequently hypointense and may also show flow voids from either concentrated metals within fungal hyphae or low free-water content (Figure 2).
Figure 2. Allergic fungal sinusitis. T1-weighted MRI with contrast shows enhancing mucosa characteristic of polyps in the ethmoid, frontal, and maxillary sinuses
Allergic fungal sinusitis diagnosis
The Bent and Kuhn criteria for allergic fungal sinusitis consist of the following 16:
- Nasal polyposis,
- Fungi on staining,
- Eosinophilic mucin without fungal invasion into sinus tissue,
- Type I hypersensitivity to fungi, and
- Characteristic radiological findings with soft tissue differential densities on CT scanning.
When using these criteria, several caveats should be considered. Patients who have undergone prior sinus surgery may only show generalized mucosal edema as opposed to frank polyps. The presence of fungi on staining can also be problematic, because fungal elements may be sparse and histopathologists may not routinely use fungal stains. The use of type 1 hypersensitivity, either via skin-prick or radioallergosorbent testing (RAST – a blood test using radioimmunoassay test to detect specific IgE antibodies, to determine the substances a subject is allergic to), is a fundamental criterion of the aforementioned classification system. However, studies often report disparities between the fungal species cultured from patients and fungal-specific sensitivities on allergy testing 17.
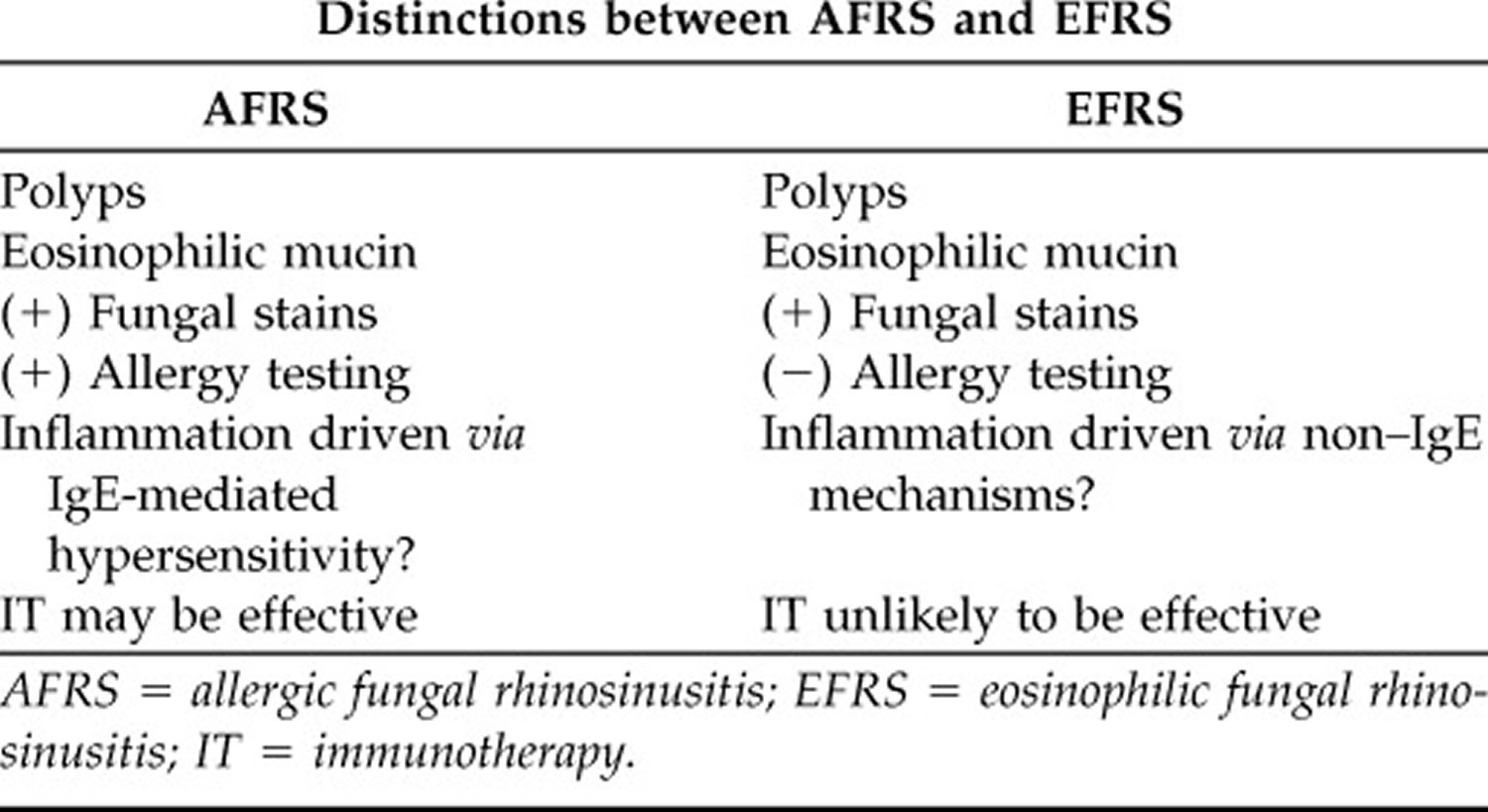
The International Society for Human and Animal Mycology Working Group spent much time considering the pathophysiological basis of allergic fungal sinusitis and similar conditions 18. What is clear from prior research is that a subtype of chronic rhinosinusitis with nasal polyps patients has eosinophilic mucin evident on histopathology. In those chronic rhinosinusitis with nasal polyps patients with eosinophilic mucin, some will have detectable fungal hyphae within the mucin and some will not (Table 2). Those with fungal hyphae on staining would be classified as allergic fungal sinusitis if they also show type 1 hypersensitivity to fungi. Those chronic rhinosinusitis with nasal polyps patients with eosinophilic mucin and detectable fungal hyphae, but absence of type 1 responses, would be classified as eosinophilic fungal rhinosinusitis (EFRS). From a mechanistic standpoint, allergic fungal sinusitis and eosinophilic fungal rhinosinusitis (EFRS) differ based on whether sinonasal inflammation is associated with an IgE-mediated process or not. From a clinical management standpoint, this distinction only matters insomuch as immunotherapy (subcutaneous or sublingual) could be considered in allergic fungal sinusitis whereas it would not be indicated in eosinophilic fungal rhinosinusitis 19. Apart from immunotherapy, the clinical management of allergic fungal sinusitis and eosinophilic fungal rhinosinusitis would be indistinguishable at this point in time.
Table 2. Clinical features of AFRS (Allergic Fungal Rhinosinusitis) and EFRS (Eosinophilic Fungal Rhinosinusitis)
Allergic fungal sinusitis treatment
Surgical Therapy
Most clinical series describe surgical therapy to remove polyps, open sinus ostia, and clear eosinophilic fungal mucin, followed by aggressive medical therapies. From the literature it appears that surgery in combination with other medical treatments leads to improved outcomes. A retrospective review reported that incomplete removal of all fungal and eosinophilic mucin contributed to disease recurrence and the need for revision surgery 21. Champagne et al. 22 showed improvements in quality of life and endoscopy scores in all patient groups at 12 months follow-up. In this series, all patients were treated post-operatively with saline irrigations, topical nasal steroid spray, oral antibiotics and a 1-month oral steroid taper. Their maintenance treatment consisted of topical nasal steroid spray, nasal saline, montelukast, budesonide irrigations, and month-long bursts of oral steroids for exacerbations. Thus, it is difficult to isolate the impact of surgery alone from the rest of a comprehensive regimen. Overall, recurrence rates after surgery have been reported from 10 to 100% 23.
Medical Therapy
Most reports on treatment options for allergic fungal sinusitis are combined into larger series addressing chronic rhinosinusitis with nasal polyps patients and it is therefore difficult to discern if there are varying effects in the allergic fungal sinusitis population as opposed to the entire chronic rhinosinusitis with nasal polyps population. In general, medical therapies have been divided into oral and topical steroids, oral and topical antifungals, leukotriene antagonists, and immunotherapy. In all but the mildest cases of allergic fungal sinusitis, it is felt that medical therapy alone without surgical intervention is not effective in the long term; thus, most efficacy studies examining medical treatments have been performed postoperatively.
Oral and Topical Anti-Inflammatory Medications
Oral steroid studies specific to allergic fungal sinusitis patients have generally been conducted in the postoperative setting where benefit has been established. In a prospective, randomized double-blinded, placebo-controlled trial in allergic fungal sinusitis patients examining the effectiveness of postoperative oral steroids, as well as the side effects of such treatments, patients received oral prednisolone (50 mg daily × 6 weeks, and then additional 6-week taper) or placebo for 2 weeks after surgery 24. All patients received fluticasone nasal spray and oral itraconazole for 12 weeks. At 12-week follow-up, symptoms and endoscopy were improved in the oral steroid group. All 12 patients in the steroid group suffered from weight gain, 5 developed Cushingoid features, 2 developed acne, and 1 developed steroid-induced diabetes mellitus. At 18 months of follow-up, patients who stopped all treatment, including topical steroids, developed recurrent disease. It is unclear if postoperative oral steroids for 12 weeks had an impact at 18 months. A number of other non–placebo-controlled case series have been reported with highly variable dosing protocols and durations but generally reporting a positive effect when using postoperative oral steroids 25. It does not appear that prospective studies on the effects of topical steroids alone have been conducted in the allergic fungal sinusitis population; however, the majority of studies include topical steroid medications as an integral component of a comprehensive treatment regimen. No controlled studies of leukotriene antagonists have been performed in allergic fungal sinusitis patients. Leukotriene antagonists are sometimes included in a comprehensive medical regimen and thus individual efficacy apart from other medications is difficult to discern. One case report of improvement on leukotriene antagonist therapy has been reported 26.
Oral or Topical Antifungal Therapy
Limited non–placebo-controlled case series have reported benefits of oral antifungal therapies in patients with allergic fungal sinusitis. Chan et al. 27 reported outcomes of 32 patients with allergic fungal sinusitis treated with 100 mg of itraconazole three times daily for 1 month, followed by 100 mg twice daily for 2 months. Nasal endoscopy findings improved in 37.5% and symptom scores improved in 56%.
Seiberling and Wormald 28 reported a retrospective case series of 23 patients with disease classified as either allergic fungal sinusitis or eosinophilic fungal rhinosinusitis. Patients refractory to other treatments were dosed with oral itraconazole twice daily for 6 months. After treatment, 69.6% were felt to have a favorable response in clinical symptoms or endoscopy based on chart review, although it is unclear what constituted a favorable response because no objective criteria were described. Elevated liver function studies were noted in 17–19% of patients. Several randomized controlled trials of topical antifungal therapies have failed to show a benefit in chronic rhinosinusitis with nasal polyps patients, although few have specifically evaluated the allergic fungal sinusitis population 29.
Subcutaneous Immunotherapy
A large, retrospective series reported that compliance with immunotherapy for all fungal and nonfungal antigens was beneficial in preventing recurrence of disease. A 3- to 4-year course of subcutaneous immunotherapy showed benefit 12–26 months after discontinuation 30 and prolonged courses of systemic steroids were not used in these patients 31. However, a subsequent study by the same group on a smaller subset of patients with longer-term follow-up ranging from 46 to 138 months failed to indicate any benefit of subcutaneous immunotherapy, with 60% of subcutaneous immunotherapy patients having normal mucosa or only mild edema on endoscopy, and 100% of non-subcutaneous immunotherapy patients had normal mucosa or mild edema 32. This study was not randomized and obviously has the potential for bias in selecting treatment arms. Fortunately, reports of both high-dose and low-dose subcutaneous immunotherapy have all established safety 33.
- De Hoog GS, Guarro J, Gene J, Figueras MJ: Atlas of Clinical Fungi, ed 2. Utrecht, Centraalbureau voor Schimmelcultures, 2000.[↩]
- Bent J.P., 3rd, Kuhn F.A. Diagnosis of allergic fungal sinusitis. Otolaryngol Head Neck Surg. 1994;111:580–588. https://www.ncbi.nlm.nih.gov/pubmed/7970796[↩]
- Deshazo R.D. Syndromes of invasive fungal sinusitis. Med Mycol. 2009;47:S309–S314. https://www.ncbi.nlm.nih.gov/pubmed/18654920[↩][↩]
- Soler Z.M., Schlosser R.J. The role of fungi in diseases of the nose and sinuses. Am J Rhinol Allergy. 2012;26:351–358. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3904040/[↩]
- Paknezhad H, Borchard NA, Charville GW, et al. Evidence for a “preinvasive” variant of fungal sinusitis: Tissue invasion without angioinvasion. World Journal of Otorhinolaryngology – Head and Neck Surgery. 2017;3(1):37-43. doi:10.1016/j.wjorl.2017.01.003. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5683596/[↩]
- Simon-Nobbe B., Denk U., Pöll V., Rid R., Breitenbach M. The spectrum of fungal allergy. Int Arch Allergy Immunol. 2008;145:58–86. https://www.karger.com/Article/FullText/107578[↩]
- Liu X, Zou H, Chen Q-J, Lu C-M. Allergic fungal sinusitis caused by Schizophyllum commune. World Journal of Otorhinolaryngology – Head and Neck Surgery. 2017;3(1):59-63. doi:10.1016/j.wjorl.2017.02.009. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5683597/[↩][↩]
- Kupferberg S.B., Bent J.P. Allergic fungal sinusitis in the pediatric population. Arch Otolaryngol Head Neck Surg. 1996;122:1381–1384. https://www.ncbi.nlm.nih.gov/pubmed/8956755[↩]
- Manning S.C., Merkel M., Kriesel K., Vuitch F., Marple B. Computed tomography and magnetic resonance diagnosis of allergic fungal sinusitis. Laryngoscope. 1997;107:170–176. https://www.ncbi.nlm.nih.gov/pubmed/9023239[↩]
- Allphin A.L., Strauss M., Abdul-Karim F.W. Allergic fungal sinusitis: problems in diagnosis and treatment. Laryngoscope. 1991;101:815–820. https://www.ncbi.nlm.nih.gov/pubmed/1865728[↩]
- Wise SK, Ghegan MD, Gorham E, Schlosser RJ. Socioeconomic factors in the diagnosis of allergic fungal rhinosinusitis. Otolaryngol Head Neck Surg 138:38–42, 2008. https://www.ncbi.nlm.nih.gov/pubmed/18164991[↩]
- Schubert MS. Allergic fungal sinusitis: Pathophysiology, diagnosis, and management. Med Mycol 47:S324–S330, 2009. https://www.ncbi.nlm.nih.gov/pubmed/19330659[↩]
- Ferguson BJ, Barnes L, Bernstein JM, et al. Geographic variation in allergic fungal rhinosinusitis. Otolaryngol Clin North Am 33:441–449, 2000. https://www.ncbi.nlm.nih.gov/pubmed/10736417[↩]
- Aribandi M, McCoy VA, Bazan C. Imaging features of invasive and noninvasive fungal sinusitis: A review. Radiographics 27:1283–1296, 2007. https://www.ncbi.nlm.nih.gov/pubmed/17848691[↩]
- Wise SK, Rogers GA, Ghegan MD, et al. Radiologic staging systems for allergic fungal rhinosinusitis (AFRS). Otolaryngol Head Neck Surg 140:735–740, 2009. https://www.ncbi.nlm.nih.gov/pubmed/19393421[↩]
- Bent JP, Kuhn FA. Diagnosis of allergic fungal rhinosinusitis. Otolaryngol Head Neck Surg 111:580–588, 1994. https://www.ncbi.nlm.nih.gov/pubmed/7970796[↩]
- Pant H, Schembri MA, Wormald PJ, Macardle PJ. IgE-mediated fungal allergy in allergic fungal sinusitis. Laryngoscope 119:1046–1052, 2009. https://www.ncbi.nlm.nih.gov/pubmed/19358255[↩]
- Chakrabarti A, Denning DW, Ferguson BJ, et al. Fungal rhinosinusitis: A categorization and definitional schema addressing current controversies. Laryngoscope 119:1809–1818, 2009. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2741302[↩]
- Mabry RL, Mabry CS. Allergic fungal sinusitis: The role of immunotherapy. Otolaryngol Clin North Am 33:433–440, 2000. https://www.ncbi.nlm.nih.gov/pubmed/10736416[↩]
- Soler ZM, Schlosser RJ. The role of fungi in diseases of the nose and sinuses. American Journal of Rhinology & Allergy. 2012;26(5):351-358. doi:10.2500/ajra.2012.26.3807. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3904040/[↩]
- Marple BL, Mabry RL. Allergic fungal sinusitis: Learning from our failures. Am J Rhinol 14:223–226, 2000. https://www.ncbi.nlm.nih.gov/pubmed/10979494[↩]
- Champagne JP, Antisdel JL, Woodard TD, Kountakis SE. Epidemiologic factors affect surgical outcomes in allergic fungal sinusitis. Laryngoscope 120:2322–2324, 2010. https://www.ncbi.nlm.nih.gov/pubmed/20938955[↩]
- Marple BF. Allergic fungal rhinosinusitis: Current theories and management strategies. Laryngoscope 111:1006–1019, 2001. https://www.ncbi.nlm.nih.gov/pubmed/11404613[↩]
- Rupa V, Jacob M, Mathews MS, Seshadr MS. A prospective, randomised, placebo-controlled trial of postoperative oral steroid in allergic fungal sinusitis. Eur Arch Otorhinolaryngol 267:233–238, 2010. https://www.ncbi.nlm.nih.gov/pubmed/19714349[↩]
- Kinsella JB, Bradfield JJ, Gourley WK, et al. Allergic fungal sinusitis. Clin Otolaryngol Allied Sci 21:389–392, 1996. https://www.ncbi.nlm.nih.gov/pubmed/8932939[↩]
- Schubert MS. Antileukotriene therapy for allergic fungal sinusitis. J Allergy Clin Immunol 108:466–467, 2001. https://www.ncbi.nlm.nih.gov/pubmed/11544470[↩]
- Chan KO, Genoway KA, Javer AR. Effectiveness of itraconazole in the management of refractory allergic fungal rhinosinusitis. J Otolaryngol Head Heck Surg 37:870–874, 2008. https://www.ncbi.nlm.nih.gov/pubmed/19128719[↩]
- Sieberling K, Wormald PJ. The role of itraconazole in recalcitrant fungal sinusitis. Am J Rhinol Allergy 23:303–306, 2009. https://www.ncbi.nlm.nih.gov/pubmed/19490806[↩]
- Ebbens FA, Georgalas C, Luiten S, et al. The effect of topical amphotericin B on inflammatory markers in patients with chronic rhinosinusitis: A multicenter randomized controlled study. Laryngoscope 119:401–408, 2009. https://www.ncbi.nlm.nih.gov/pubmed/19160404[↩]
- Mabry RL, Marple BF, Folker RJ, Mabry CS. Immunotherapy for allergic fungal sinusitis: Three years’ experience. Otolaryngol Head Neck Surg 119:648–651, 1998. https://www.ncbi.nlm.nih.gov/pubmed/9852541[↩]
- Folker RJ, Marple BF, Mabry RL, Mabry CS. Treatment of allergic fungal sinusitis: A comparison trial of postoperative immunotherapy with specific fungal allergens. Laryngoscope 108:1623–1627, 1998. https://www.ncbi.nlm.nih.gov/pubmed/9818816[↩]
- Marple B, Newcomer M, Schwade N, Mabry R. Natural history of allergic fungal rhinosinusitis: A 4- to 10-year follow-up. Otolaryngol Head Neck Surg 127:361–366, 2002. https://www.ncbi.nlm.nih.gov/pubmed/12447228[↩]
- Greenhaw B, deShazo RD, Arnold J, Wright L. Fungal immunotherapy in patients with allergic fungal sinusitis. Ann Allergy Asthma Immunol 107:432–436, 2011. https://www.ncbi.nlm.nih.gov/pubmed/22018615[↩]





{kind=link}