Contents
What is anabolic steroid
Anabolic steroids also known as “anabolic-androgenic steroids“, “steroids“, “androgens” or “performance and image enhancing drugs” are a group of man-made (synthetic) drugs with similar effects to the male sex hormone called testosterone 1, 2, 3, 4, 5. Common slang terms for anabolic steroids include ‘roids’, ‘gear’, ‘juice’, ‘Arnolds’, ‘pumpers’, ‘stackers’, ‘gym candy’, ‘weight trainers’ and ‘weight gainers’. Anabolic steroids help to rebuild tissues that have become weak because of serious injury or illness 6. Anabolic steroids are also used in sports to boost strength, build muscles, reduce fat, enhance sporting performance and speed up recovery from injury 7, 8, 9, 10, 11, 12. The use of anabolic steroids in sports is known as doping. Doping with anabolic steroids is banned by most sports leagues and groups. People who misuse anabolic steroids may include athletes, bodybuilders and people who feel they need to look muscular to feel good about themselves 13, 14, 15, 16, 17, 6, 18, 19, 20.
There are 2 types of anabolic steroids 1:
- 17 alpha alkyl derivatives: e.g., oxandrolone, oxymetholone, and fluoxymesterone;
- 17 beta ester derivatives: e.g., testosterone cypionate, testosterone enanthate, testosterone heptylate, testosterone propionate, nandrolone decanoate, nandrolone phenpropionate, and dromostanolone.
Commonly misused anabolic steroids
- Oral anabolic steroids
- Oxymetholone (Anadrol)
- Oxandrolone (Anavar)
- Oxymetholone
- Methandienone (Dianabol)
- Methandrostenolone
- Stanozolol (Winstrol)
- Testosterone undecanoate (Restandol)
- Injectable anabolic steroids
- Nandrolone decanoate (Deca-Durabolin)
- Nandrolone phenpropionate (Durabolin)
- Testosterone cypionate (Depo-Testosterone)
- Testosterone propionate (Agovirin)
- Testosterone phenylpropionate (Retandrol)
- Trenbolone also known as trienolone or trienbolone
- Boldenone undecylenate (Equipoise)
Some bodybuilders and athletes use anabolic steroids may take the steroids orally, inject them into muscles, or apply them to the skin as a gel or cream. These doses may be 10 to 100 times higher than doses prescribed by medical professionals to treat medical conditions. Some bodybuilders and athletes typically take two or more anabolic steroids at the same time in a cyclic manner known as “cycles” lasting from a few weeks to a few months, believing that this will improve their effectiveness and minimize the side effects 21, 22, 23, 12. All anabolic steroids are Drug Enforcement Administration (DEA) schedule 3 drugs 24, 25, 26. Using anabolic steroids this way, without a prescription from a doctor, is not legal or safe.
There are several substances that produce effects similar to those of anabolic steroids. These non-steroidal anabolics include human growth hormone (GH), clenbuterol, gonadotropins, and erythropoietin. Human chorionic gonadotropin (hCG) has luteinizing hormone (LH) activity that stimulates endogenous testosterone production in men, but not women 27. Exogenous human chorionic gonadotropin (hCG) is widely available, and effective when administered twice weekly as a subcutaneous injection. Human chorionic gonadotropin (hCG) is commonly (much more commonly than injectable recombinant luteinizing hormone (rLH)) used by athletes and members of the general public who want increased anabolic androgenic steroid effects on muscle mass and strength 28. Aromatase inhibitors (e.g., anastrozole, letrozole, exemestane) and selective estrogen receptor modulators such as clomiphene or raloxifene increase circulating luteinizing hormone (LH) that stimulates Leydig cells in the testis to synthesize testosterone 27. Finally, high dosages of testosterone precursors such dehydroepiandrosterone (DHEA) increase testosterone production and circulating testosterone concentrations.
Anabolic steroids should be not be confused with corticosteroids (e.g., cortisone, prednisone, prednisolone, methylprednisolone, dexamethasone, betamethasone and hydrocortisone) sometimes also referred to as ‘steroids’ that resemble the human adrenal hormone cortisol and have potent antiinflammatory and immunosuppressive properties 29. Corticosteroids or glucocorticoids antiinflammatory properties are used to reduce inflammation. This can ease symptoms of inflammatory conditions, such as rheumatoid arthritis, inflammatory bowel disease (IBD), asthma, allergies and skin rashes. Corticosteroids also suppress the immune system. This can help control conditions in which the immune system mistakenly attacks its own tissues. They also are used to prevent organ rejection in transplant recipients.
Anabolic steroids used by doctors for medical reasons 30:
- To help patients who have severe illness, injury, or chronic infection gain weight. Anabolic steroids also are used when patients fail to gain or maintain normal weight because of loss of muscle caused by diseases like cancer or HIV or unexplained medical reasons.
- As androgen replacement therapy for male hypogonadism
- To treat delayed puberty in boys.
- To treat certain types of anemia.
- To treat certain kinds of breast cancer in some women.
- To treat hereditary angioedema, which causes swelling of the face, arms, legs, throat, windpipe, bowels, or sexual organs.
- Other indications for the use of testosterone include primary testicular failure in patients with cryptorchidism, orchitis, testicular torsion, vanishing testis syndrome, previous history of orchiectomy, Klinefelter syndrome, chemotherapeutic agents, toxic damage from alcohol use, and heavy metals.
FDA-approved indications for the use of anabolic steroids are:
- primary hypogonadism,
- delayed puberty in boys (testosterone enanthate),
- hypogonadotropic hypogonadism (testosterone cypionate, enanthate, and undecanoate),
- gonadotropin and luteinizing hormone-releasing hormone deficiency,
- pituitary-hypothalamic axis dysfunction from various tumors, injury, and radiation.
Non-FDA-approved indications of androgenic steroids include:
- bone marrow stimulation in leukemia,
- aplastic anemia,
- kidney failure,
- growth failure,
- stimulation of appetite, and muscle mass in cancer
- acquired immunodeficiency syndrome.
Anabolic steroids may also be used for other conditions as determined by your doctor.
Anabolic steroids are available only with your doctor’s prescription.
A study completed by the National Drug and Alcohol Research Center found the following people use anabolic steroids 10:
- Competitive athletes – who are motivated by their desire to succeed.
- People concerned about their body image – recreational weight trainers and body builders and people working in the fashion and entertainment industries.
- Body building professionals – people involved in body building as a competitive sport.
- People who need muscle strength to do their job – bodyguards, security personal, construction workers, police and members of the armed services.
- Young men – who want to increase their athletic performance or who are striving to reach the same physical appearance that is often portrayed in the media.
Anabolic steroid users are sometimes used by athletes at all levels in sports such as bodybuilding, weightlifting, baseball, football, cycling, wrestling, and many others to improve their performance. Typically, it is males in their mid to late 30’s who use anabolic steroids non-medically the most 11. In 2022, an estimated 0.8% of 8th graders, 0.5% of 10th graders, and 1.3% of 12th graders reported misusing anabolic steroids in the past 12 months 31.
The misuse of anabolic steroids can cause long-term side effects. These can include heart and blood vessels complications, liver disease, reproductive organ damage and severe mood swings.
Many athletes take anabolic steroids at doses that are too high. These doses are much higher than those prescribed by doctors for medical reasons. Anabolic steroids have serious side effects too.
Anabolic steroids affect everyone differently. All people who use anabolic steroids might start to get 12, 32, 33:
- Severe acne leading to permanent scarring
- A higher risk of swollen or torn tendons, which attach muscle to bone.
- Liver tumors, liver cancer or other changes to the liver.
- Kidney damage.
- Higher levels of the “bad” cholesterol, called low-density lipoprotein (LDL) cholesterol.
- Lower levels of the “good” cholesterol, called high-density lipoprotein (HDL) cholesterol.
- High blood pressure (hypertension).
- Problems with the heart and blood flow including heart attack
- Water retention – leading to facial bloating.
- Issues with anger, violence or aggressive behavior often referred to as “roid rage”. In some individuals, anabolic steroid use can cause irritability and dramatic mood swings, increased feelings of hostility, impaired judgment, and increased levels of aggression.
- Mental health conditions, such as irritability and mood swings, aggression and violence and depression.
- A need for anabolic steroids that can’t be controlled.
- Diseases, such as HIV and AIDS or hepatitis, if using needles to give shots of the drugs. Users who inject anabolic steroids run the risk of contracting various infections due to non-sterile injection techniques, sharing of contaminated needles, and the use of steroid preparations manufactured in non-sterile environments. All these factors put users at risk for contracting viral infections such as HIV/AIDS or hepatitis B or C, and bacterial infections at the sight of injection. Users may also develop endocarditis, a bacterial infection that causes a potentially fatal inflammation of the heart lining.
- More frequent colds
- Increased sex drive (increased libido)
- Sleeping difficulties.
Young men are more likely than young women to use steroids to gain weight and muscle mass 34. Teens who take anabolic steroids might grow less than usual or stunted growth. Teens who take anabolic steroids also might raise their risk of health problems later in life. The risks of certain side effects are higher if steroids are injected by young men in their late teens/ early 20s, before they have stopped growing. For example 35, 36:
- Stunted growth
- Premature balding
- Acne scarring
- Stretch marks on chest and arms
- Prematurely-aged, ‘leathery’ skin
- Injuries from excessively intense gym workouts.
Anabolic steroids side effects in Men may include 12, 33:
- Baldness
- Breast growth (gynecomastia)
- Low sperm count or infertility. Not being able to get their partner pregnant.
- Shrinking of the testicles
- Learn from a doctor that their prostate gland has gotten bigger.
Anabolic steroids side effects in Women may include 12, 33:
- Get a deeper voice. Treatment may not be able to change it back.
- Notice that a part of their genitals called the clitoris has gotten bigger.
- Growth of body and facial hair.
- Lose the hair on the head. Treatment might not be able to bring the hair back.
- Stop getting periods (amenorrhea) or get them much less often than they used to (irregular menstrual cycle).
Pregnant women who use anabolic steroids are at risk of harming their unborn baby. To be safe, anabolic steroid use should be stopped at least 4 months before falling pregnant, as well as during pregnancy 37, 38.
Even though anabolic steroids don’t cause a high, anabolic steroids can cause psychological dependence and addiction with users can find themselves relying on anabolic steroids to build confidence and self-esteem 39, 40, 22. This reliance can make it difficult to stop using them in the longer term. Furthermore, the fear of losing muscle size or definition can lead to internal pressure to continue use 32.
When users stop taking anabolic steroids, they may experience withdrawal symptoms:
- Fatigue
- Restlessness
- Loss of appetite
- Sleep problems
- Decreased sex drive
- Steroid cravings
- Depression, which can sometimes be severe enough to lead one to commit suicide.
It can take up to four months to restore the body’s natural testosterone levels if taking high doses for an extended period of time 28.
Figure 1. Testosterone
Figure 2. Anabolic steroids
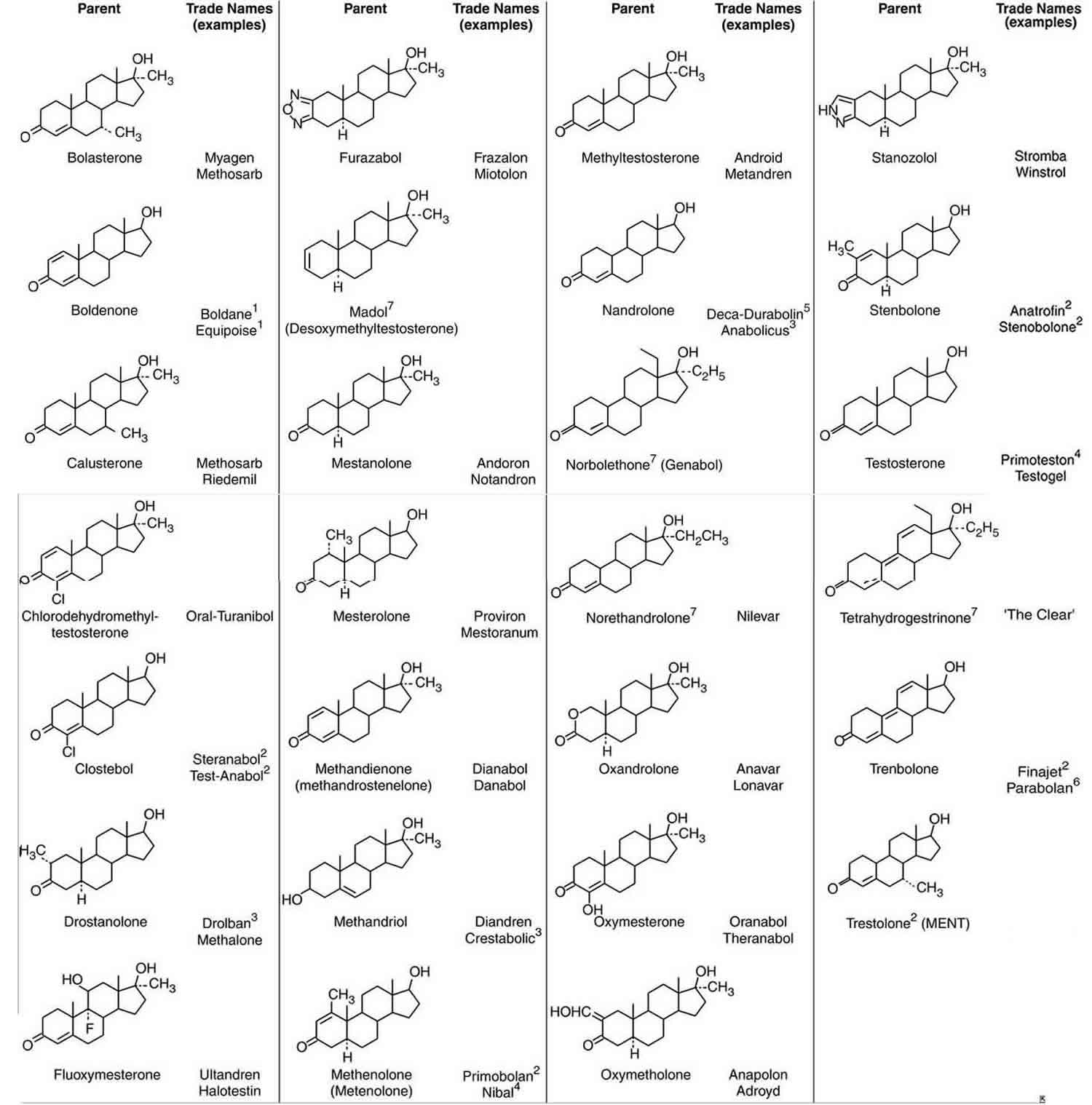
Footnotes: Structures of anabolic steroids with corresponding diagnostic metabolites and examples of registered trade names. Superscripts (1–6) refer to 17β-hydroxyl-esterified preparations: 1undecylenoate; 2acetate; 3propionate; 4heptanoate; 5decanoate; 6hexahydrobenzylcarbonate.
[Source 41 ]Are anabolic steroids addictive?
An undetermined percentage of anabolic steroid users may develop a anabolic steroid use disorder. Substance use disorders are defined by continued use despite adverse consequences; for anabolic steroid users, these may include physical or psychological problems such as breast growth (in men), sexual dysfunction, high blood pressure, excessive fats in the blood, heart disease, mood swings, severe irritability, or aggressiveness. Anabolic steroid users also may give up other important activities for fear that they will miss workouts, violate their dietary restrictions, or be prevented from using anabolic steroids. Anabolic steroid users also typically spend large amounts of time and money obtaining the drugs, and they may try to reduce or stop anabolic steroid use without success—possibly due to depression, anxiety about losing muscle mass, or and other unpleasant effects of withdrawal 42.
Withdrawal from anabolic steroids occurs when an individual develops dependence. A review of the research suggests that about 32 percent of people who misuse anabolic steroids become dependent 43. Symptoms of dependence can include tolerance, which is needing to take more steroids to achieve the same effects. Another indicator of dependence is withdrawal once anabolic steroid use stops 42. Withdrawal symptoms can include fatigue, restlessness, loss of appetite, insomnia, reduced sex drive, and steroid cravings 44. The most dangerous of the anabolic steroid withdrawal symptoms is depression, because it sometimes leads to suicide attempts 45.
What are anabolic steroids overdose effects?
Anabolic steroids are not associated with overdoses. The adverse effects a user would experience develop from the use of steroids over time.
How do anabolic steroids work?
Anabolic steroids work by imitating the properties of naturally occurring hormone similar to testosterone and can activate the body’s testosterone receptors. Once the testosterone receptors are stimulated, a domino effect of metabolic reactions takes place as the drug instructs the body to increase muscle tissue production.
Testosterone has two effects in your body:
- Anabolic effects – The anabolic actions cause the body to increase protein synthesis in skeletal muscles and various other tissues, facilitating muscle growth, speeding up recovery from injury, increasing bone density while stimulating the production of new red blood cells. The increased protein synthesis can result in an increased muscle size and strength as well as increased body weight 46, 26, 47, 48, 49, 50. For those sports that rely on body size or the generation of power and force by the muscle, the increase in muscle mass and strength often result in improvements in sport and athletic performance. Anabolic steroids also upregulate and increase the number of androgen receptors (ARs), thus enabling increased training intensity and indirectly contributing to increased muscle size and strength. Anabolic steroids also have a stimulatory effect on the brain through their diverse effects on various central nervous system neurotransmitters, blocking the effects of glucocorticoids, and stimulation of the growth hormone-insulin-like growth factor-1 axis.
- Androgenic effects also known as masculinizing effects – is responsible for the growth, development and maintaining male sex characteristics such as the penis, testicles, muscle mass, deep voice and facial hair 51, 52, 53.
Although testosterone is called a male sex hormone, it also occurs naturally in women, but in much smaller amounts. In men about 95% of the testosterone is synthesized from cholesterol in the Leydig cells in the testis. Testosterone can bind directly with the androgen receptor (AR). In target tissues where intracellular enzymes are present, the action of testosterone is mediated by metabolism. Testosterone is further metabolized by the enzyme 5α-reductase to dihydrotestosterone (DHT), which binds with greater affinity to the androgen receptor (AR) or by aromatase to estradiol (E2), which binds to the estrogen receptor (ER). The ovaries and the adrenal glands in both sexes produce very little testosterone, but secrete weaker androgens in particular, dehydroepiandrosterone (DHEA; and its sulpho-conjugate) and androstenedione are of physiological importance in the women, not least because they can undergo peripheral conversion to more potent androgens, for example to testosterone and dihydrotestosterone (DHT). Another weaker endogenous androgen, androstenediol, also binds to estrogen receptors (ER).
In reproductive target tissues, testosterone can be considered to be a prohormone, being readily converted by 5α-reductase to the more potent androgen dihydrotestosterone (DHT). In other tissues, such as fatty tissue and parts of the brain, testosterone is converted by aromatase to the estrogen, estradiol (E2). In bone, the mechanism of action of the anabolism of androgens has not been entirely elucidated but both a direct effect of testosterone and a mediated effect by aromatization to estradiol are important 54, 55. In the human skeletal muscle collected less than 12 hour post-mortem, 5α-reductase activity either type 1 or 2 is not detectable 56, so testosterone itself is chiefly binding to the androgen receptor (AR). Aromatase expression and activity is significant in human skeletal muscle 57 but whether the conversion of androgens to estrogens within this tissue is physiologically important for mediating some of the myotrophic effect of androgens is yet to be determined.
Figure 3. Testosterone biosynthetic pathways
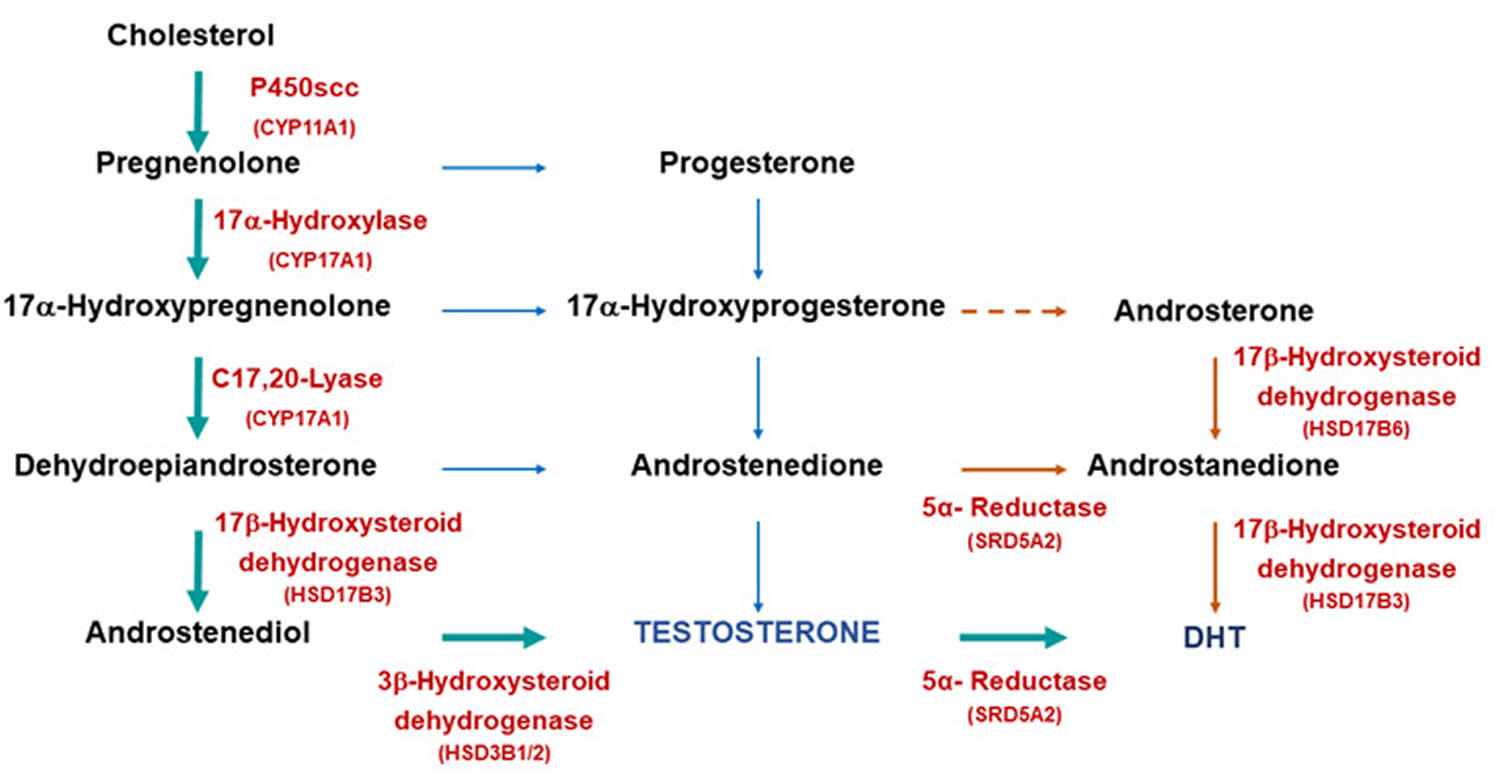
Footnotes: Biosynthetic pathways for testosterone and dihydrotestosterone (DHT) synthesis. The classic pathway show testosterone synthesized from cholesterol with further metabolism to dihydrotestosterone (DHT). The alternative or “backdoor” pathway shows DHT production without going through testosterone. Note only some of the enzymes are shown for clarity.
[Source 58 ]Figure 4. Enzymes involved in the biosynthesis of the adrenal steroid hormones and the gonadal steroid hormones
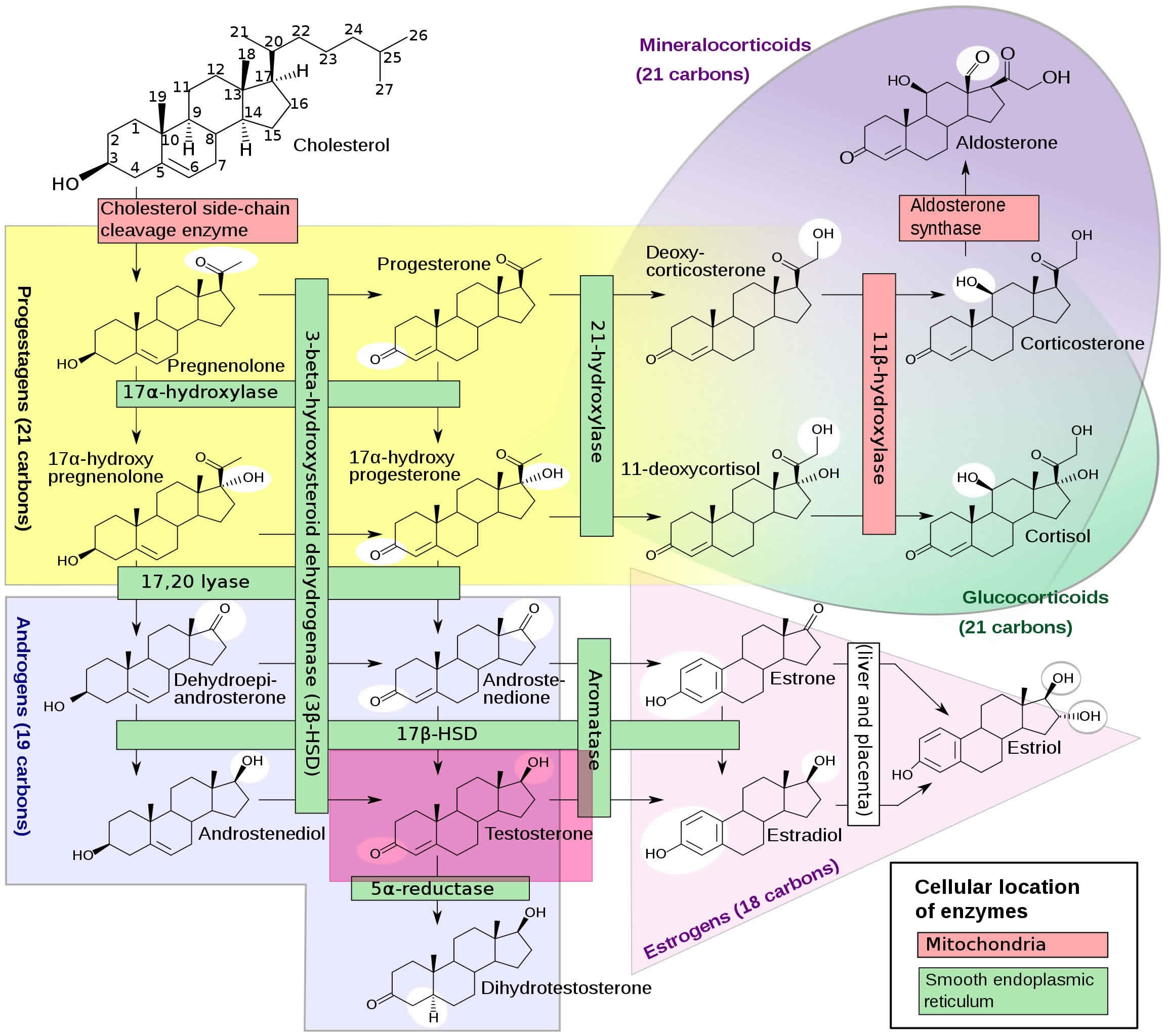
Footnotes: Figure 4 illustrates all of the enzymes involved in the biosynthesis of the adrenal steroid hormones, corticosterone, cortisol, and aldosterone; and the gonadal steroid hormones, progesterone, estradiol, and testosterone. Leydig cells in the testes function to turn cholesterol into testosterone 59. Luteinizing hormone (LH) regulates the initial step in this process. Two important intermediates in this process are dehydroepiandrosterone (DHEA) and androstenedione. Androstenedione is converted to testosterone by the enzyme 17-beta-hydroxysteroid dehydrogenase. At the cellular level, testosterone gets converted to dihydrotestosterone (DHT) by the enzyme 5-alpha-reductase. Dihydrotestosterone (DHT) is an androgen, which means it is a hormone that triggers the development of male characteristics 60. About 10% of the testosterone in the bodies of both men and women is converted into dihydrotestosterone (DHT) in adults, with a much higher amount in puberty. This may be why it is so closely related to the triggering of puberty. The dihydrotestosterone hormone (DHT) is much more powerful than testosterone. Dihydrotestosterone initiates the start of puberty in boys. It causes the genitals to develop and can cause the growth of pubic and body hair. It also causes the prostate to grow during puberty and may work together with testosterone to begin the expression of sexual desires and behavior. Women also have dihydrotestosterone (DHT), but its role in their bodies is not as well known. Some research has shown that it can lead to pubic hair growth after puberty in girls. It may also play a role in determining when puberty will start for a girl. Both men and women also produce weak acting androgens in the zona reticularis of the adrenal cortex. These weak-acting androgens are known as dehydroepiandrosterone (DHEA and androstenedione. They bind to testosterone receptors with weaker affinity but can also be converted to testosterone in the peripheral tissues if produced at high amounts 60.
Figure 5. Hypothalamic–pituitary–gonadal axis
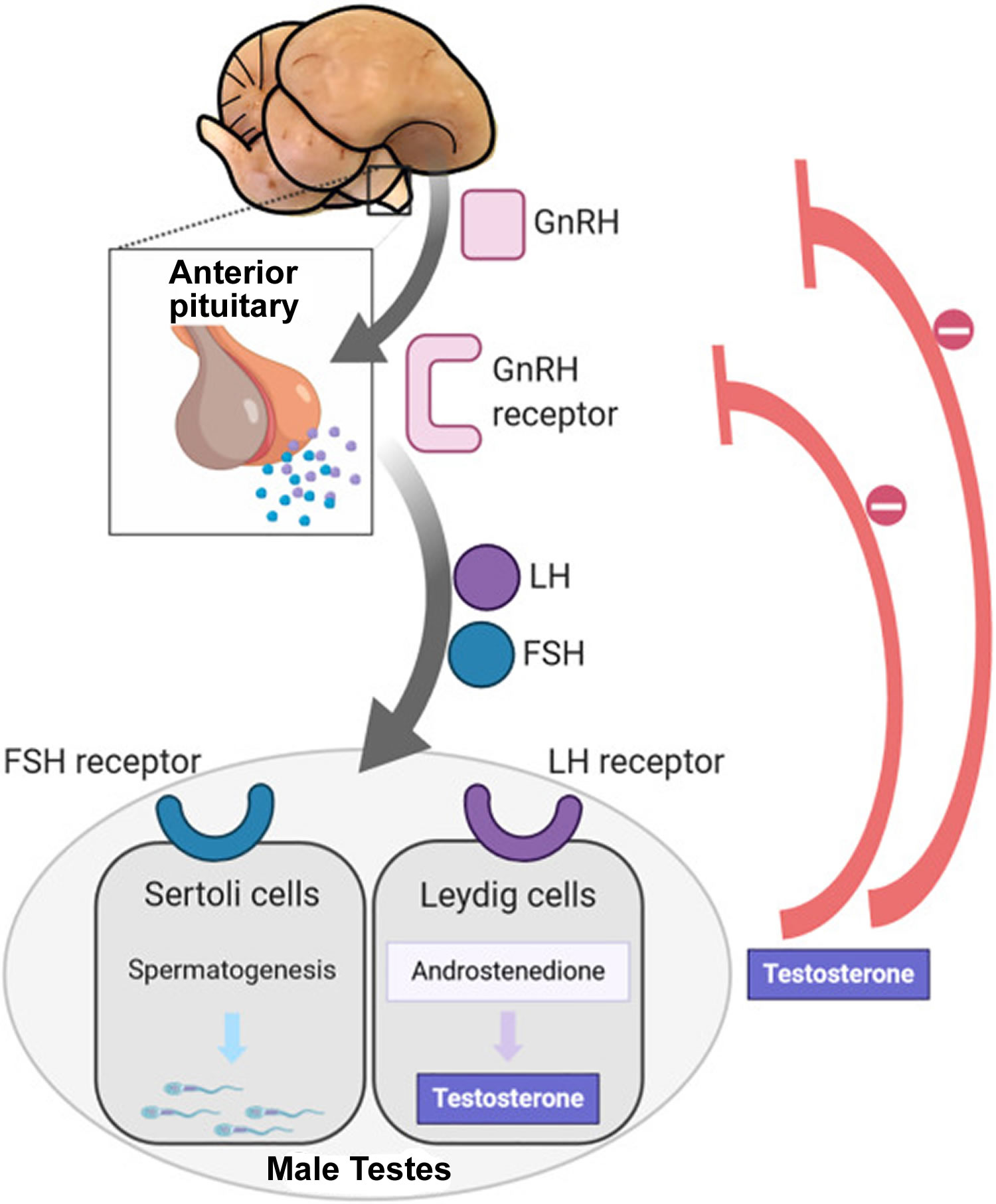
Footnotes: In puberty, the hypothalamic-pituitary-gonadal axis plays a major role in regulating testosterone levels and gonadal function. Gonadotropin-releasing hormone (GnRH) is secreted from the hypothalamus by GnRH-expressing neurons. The GnRH travels down the hypothalamohypophyseal portal system to the anterior pituitary, which secretes luteinizing hormone (LH) and follicle-stimulating hormone (FSH). LH and FSH are two gonadotropic hormones that travel through the blood and act on receptors in the gonads. The largest amounts of testosterone (>95%) are produced by the testes in men, while the adrenal glands account for most of the remainder. In the testes, testosterone is produced by the Leydig cells 61. The male testes also contain Sertoli cells, which require testosterone for spermatogenesis (sperm cell development). Luteinizing hormone (LH), in particular, acts on the Leydig cells to increase testosterone production. Testosterone limits its own secretion via negative feedback. High levels of testosterone in the blood feedback to the hypothalamus to suppress the secretion of GnRH and also feedback to the anterior pituitary, making it less responsive to GnRH stimuli 62. Throughout the reproductive life of males, the hypothalamus releases GnRH in pulses every 1 to 3 hours. Despite this pulsatile release, however, average plasma levels of FSH and LH remain fairly constant from the start of puberty, where levels spike, to the third decade of life, where levels peak and slowly begin to decline. Prior to puberty, testosterone levels are low, reflecting the low secretion of GnRH and gonadotropins. Changes in neuronal input to the hypothalamus and brain activity during puberty cause a dramatic rise in GnRH secretion.
How anabolic steroids affect your body
People who use anabolic steroids generally experience an increase in muscle strength very quickly 63, 64. This generally means that people are able to train more often and for longer periods of time, with improved recovery. This can often lead to rapid increases in lean muscle tissue. Fluid retention is also common and can lead to muscles looking soft or bloated.
The evidence around whether anabolic steroids can significantly improve athletic performance is limited 8. But generally speaking, there has been some research which has shown that people who use anabolic steroids will experience an increase in muscle strength 9. Bhasin et al. 50 demonstrated that 12 weeks of testosterone at a dosage of 10 to 12 times the normal daily production rate significantly increased strength in young trained men and that the effects of testosterone and exercise were additive. There is a dosage-dependent effect of anabolic steroids on muscle mass and strength 65, 66. The dose-response curve for anabolic steroids has not been clearly defined, but male athletes and body builders often use mega dosages 28. They also often use a variety of anabolic steroids simultaneously (“stacking”) or sequentially (“cyclically”) because of a belief that these regimens are safer 28. With the exception of a few elite female athletes and body builders, women seldom use supraphysiologic dosages of anabolic steroid. There are few data on the effects of exogenous androgen therapy in women, but modestly supraphysiologic dosages of testosterone appear to increase muscle mass and strength in women 67, 68.
Nandrolone decanoate and nandrolone phenpropionate are associated with the increased ratio of anabolic activity versus androgenic activity. Nandrolone decanoate is a slow-acting anabolic steroid designed for the sole purpose of increasing muscle mass. Nandrolone decanoate acts by promoting nitrogen retention in muscles, leading to an increase in muscle size, and providing joint pain relief by promoting collagen synthesis and enhancing bone mineralization. Nandrolone phenpropionate also causes an increase in muscle growth, stimulation of appetite, and an increase in the production of red blood cells.
Dromostanolone is a synthetic anabolic steroid with anti-estrogenic properties and is five times more potent than methyltestosterone, which is being used widely by bodybuilders to prepare for competition. It increases retention of nitrogen, phosphorus, and potassium, resulting in increased protein anabolism and a decrease in the catabolism of amino acids, leading to an increase in density and hardness of muscle.
How are anabolic steroids used?
Some anabolic steroids are taken orally, others are injected intramuscularly 69 and still others are provided in gels or creams that are applied to the skin 70. Many users start with the oral form and then progress to injectable forms, since the latter causes less liver damage 71. However, oral anabolic steroids clear more rapidly from the body, often making this the preferred route for users concerned with drug testing 72. Doses taken by people misusing anabolic steroids can be 10 to 100 times higher than the doses used to treat medical conditions 71.
Cycling
Anabolic steroids are often used in patterns called “cycling”. This involves taking multiple doses of steroids over a specific period of time, stopping for a period, and starting again.
Stacking
People who misuse anabolic steroids also typically “stack” the drugs, meaning that they take two or more different anabolic steroids, mix oral and/or injectable types, and sometimes even take compounds that are designed for veterinary use 73, 14. The belief is that different anabolic steroids interact to produce an effect on muscle size that is greater than the effects of each drug individually, a theory that has not been tested scientifically 71.
Pyramiding
Another common mode of anabolic steroid misuse is referred to as “pyramiding”, which typically involves taking anabolic steroid in a cycle of six to 12 weeks, tapering gradually rather than starting and finishing a cycle abruptly. At the beginning of a cycle, the person starts with low doses of the anabolic steroid being stacked and then slowly increases the doses. In the second half of the cycle, the doses are slowly decreased to zero. This is sometimes followed by a second cycle in which the person continues to train but without anabolic steroid. Steroid users believe that pyramiding allows the body time to adjust to the high doses, and the drug-free cycle allows the body’s hormonal system time to recuperate 74.
Plateauing
A technique called “plateauing” may also be used, whereby anabolic steroids are staggered, overlapped, or substituted with another type of anabolic steroid to avoid developing tolerance 71. As with stacking, the effects of pyramiding, cycling, and plateauing have not been substantiated scientifically.
Anabolic steroids administration
Anabolic steroids administration can be via oral pills, injections, creams or topical gels, and skin patches.
- Testosterone cypionate is given as 50 to 400 mg intramuscularly once to 4 times a month for primary hypogonadism and hypogonadotropic hypogonadism.
- Testosterone undecanoate dosing starts as an initial dose of 750 mg, then 750 mg given four weeks after the first dose, and 750 mg subsequently, given at ten weeks intervals between each dose.
- Testosterone gel is given as 11 mg 3 times daily, with a total dose of 33 mg daily.
- Transdermal testosterone is applied as 50 mg applied once daily in the morning to the upper limb, shoulder, or abdomen with a maximum dose of 100 mg per day.
- Another testosterone gel is given in the dose of 40 mg once a day every morning with a maximum dose of 70 milligrams per day.
Medications Not Approved by FDA for Medical Use
- Nandrolone decanoate dosing is 100 mg per week for comfort and relief of joint pain and in the dose range of 200 mg to 400 mg per week to increase growth and performance. It is ideally used for about ten to twelve weeks to get the desired results in athletes, powerlifters, and bodybuilders.
- Dromostanolone is available as 200 to 400 mg weekly, which bodybuilders use to enhance their athletic performance. Because of its short half-life, dromostanolone injections are administered every 3 to 4 days.
Anabolic steroids contraindications
Testosterone cypionate is contraindicated in the presence of severe kidneyl, heart and liver disease, men with breast cancer and prostate cancer, venous thromboembolism, pregnant women, or women who may become pregnant breastfeeding women, hypersensitivity to any component of the formulation. The Endocrinology Society suggests that it may be judicious to avoid treatment with testosterone in men who have a history of heart attack (myocardial infarction) and stroke in the last six months 75, 76.
Contraindications to testosterone replacement therapy include 77:
- History of breast cancer
- Prostate cancer
- Uncontrolled heart failure
- Myocardial infarction or cerebrovascular accident within the past 6 months
- Untreated obstructive sleep apnea
- Hematocrit over 48%
- Men planning fertility
- A palpable undiagnosed prostate nodule
- An elevated PSA above 4 ng/mL
- An elevated PSA level above 3vng/mL in high-risk patients including African Americans and men with a first-degree relative with prostate cancer.
Anabolic steroids side effects
The side effects of anabolic steroid use can differ from person to person. In the worst case, long-term heavy anabolic steroid use can lead to heart attack, stroke and death 78, especially among men aged in their early 30s who combine anabolic steroids with stimulant drugs, such as speed and ecstasy 12, 79, 80.
All people who use anabolic steroids might start to get 12, 32, 33:
- Severe acne leading to permanent scarring
- A higher risk of swollen or torn tendons, which attach muscle to bone.
- Liver tumors, liver cancer or other changes to the liver.
- Kidney damage.
- Higher levels of the “bad” cholesterol, called low-density lipoprotein (LDL) cholesterol.
- Lower levels of the “good” cholesterol, called high-density lipoprotein (HDL) cholesterol.
- High blood pressure (hypertension).
- Problems with the heart and blood flow including heart attack
- Water retention – leading to facial bloating.
- Issues with anger, violence or aggressive behavior often referred to as “roid rage”. In some individuals, anabolic steroid use can cause irritability and dramatic mood swings, increased feelings of hostility, impaired judgment, and increased levels of aggression.
- Mental health conditions, such as irritability and mood swings, aggression and violence and depression.
- A need for anabolic steroids that can’t be controlled.
- Diseases, such as HIV and AIDS or hepatitis, if using needles to give shots of the drugs. Users who inject anabolic steroids run the risk of contracting various infections due to non-sterile injection techniques, sharing of contaminated needles, and the use of steroid preparations manufactured in non-sterile environments. All these factors put users at risk for contracting viral infections such as HIV/AIDS or hepatitis B or C, and bacterial infections at the sight of injection. Users may also develop endocarditis, a bacterial infection that causes a potentially fatal inflammation of the heart lining.
- More frequent colds
- Increased sex drive (increased libido)
- Sleeping difficulties.
Long-term effects of regular anabolic steroids use may eventually cause:
- Liver disease (peliosis hepatis and liver tumors)
- Damage to the gonads (testicles or ovaries)
- Kidney, prostate or testicular cancer
- Malfunctions of the kidneys, liver or heart
- High blood pressure (hypertension)
- High blood cholesterol levels
- Depression
- Cardiovascular complications (blood clots, heart attacks, stroke and artery damage)
- Tendon and ligament damage or injuries that can’t keep up with the increased muscle strength
- ‘Roid rage’, which is characterized by uncontrollable outbursts of psychotic aggression
- Paranoia and mood swings, including deep depression
- Delusional feelings of being superhuman or invincible
- Trembling and muscle tremors
- Severe acne, which can cause scarring
- Nerve damage from needle use – this may lead to conditions such as sciatica
- Unsafe needle use can increased the risk of contracting infactions such as hepatitis B and hepatitis C, HIV/AIDS and tetanus.
Most data on the long-term effects of anabolic steroids in humans come from case reports rather than formal epidemiological studies. Serious and life-threatening adverse effects may be underreported, especially since they may occur many years later. One review found 19 deaths in published case reports related to anabolic steroid use between 1990 and 2012; however, many steroid users also used other drugs, making it difficult to show that the anabolic steroid use caused these deaths 81. One animal study found that exposing male mice for one fifth of their lifespan to anabolic steroid doses comparable to those taken by human athletes caused a high frequency of early deaths 82.
Young men are more likely than young women to use steroids to gain weight and muscle mass 34. Teens who take anabolic steroids might grow less than usual or stunted growth. Teens who take anabolic steroids also might raise their risk of health problems later in life. The risks of certain side effects are higher if steroids are injected by young men in their late teens/ early 20s, before they have stopped growing. For example 35, 36:
- Stunted growth
- Premature balding
- Acne scarring
- Stretch marks on chest and arms
- Prematurely-aged, ‘leathery’ skin
- Injuries from excessively intense gym workouts.
Anabolic steroids side effects in Men may include 12, 33:
- Baldness
- Breast growth (gynecomastia)
- Low sperm count or infertility. Not being able to get their partner pregnant.
- Shrinking of the testicles
- Learn from a doctor that their prostate gland has gotten bigger.
Anabolic steroids side effects in Women may include 12, 33:
- Get a deeper voice. Treatment may not be able to change it back.
- Notice that a part of their genitals called the clitoris has gotten bigger.
- Growth of body and facial hair.
- Lose the hair on the head. Treatment might not be able to bring the hair back.
- Stop getting periods (amenorrhea) or get them much less often than they used to (irregular menstrual cycle).
Pregnant women who use anabolic steroids are at risk of harming their unborn baby. To be safe, anabolic steroid use should be stopped at least 4 months before falling pregnant, as well as during pregnancy 37, 38.
Anabolic steroids and mental health. Research demonstrates a relationship between people who use anabolic steroids and increased mental health issues. Anabolic steroid users are more likely than non-users to report anxiety, and some users have been known to develop hypomania, manic or psychotic symptoms during exposure to anabolic steroids 83, 84. Many users have also reported major depressive symptoms and sleep disorders – particularly during periods of abstinence after intense use 83, 84.
Even though anabolic steroids don’t cause a high, anabolic steroids can cause psychological dependence and addiction with users can find themselves relying on anabolic steroids to build confidence and self-esteem 39, 40, 22. This reliance can make it difficult to stop using them in the longer term. Furthermore, the fear of losing muscle size or definition can lead to internal pressure to continue use 32.
When users stop taking anabolic steroids, they may experience withdrawal symptoms:
- Fatigue
- Restlessness
- Loss of appetite
- Sleep problems
- Decreased sex drive
- Steroid cravings
- Depression, which can sometimes be severe enough to lead one to commit suicide.
It can take up to four months to restore the body’s natural testosterone levels if taking high anabolic steroids doses for an extended period of time 28.
Hormonal side effects
Anabolic steroids use suppresses secretion of gonadotropins from the pituitary and thus suppresses your body’s testosterone production 85, shrinking of the testicles (testicular atrophy) 86, 87 and the production of sperm (spermatogenesis) in men and estrogen and progestogen production and ovulation in women 88, 89, 90, 85, 91, 92, 93, 86, 94, 95, 96. Many men who take anabolic steroids are infertile during the time of anabolic steroid use. Because chronic anabolic steroid use suppresses spermatogenesis (sperm production), the testes shrink. Many men who use anabolic steroids will also take human chorionic gonadotropin (hCG) to prevent testicular shrinkage. Many men who use anabolic steroids report decreased libido or erectile function. This sexual dysfunction might be due to lack of estrogen effect on the brain. In normal men, testosterone is aromatized to estradiol, and estradiol effects on the brain are important for normal libido and overall sexual function. Many anabolic steroid compounds are not aromatizable. In addition to absence of monthly menstrual periods (amenorrhea) or irregular and infrequent menstrual periods (oligomenorrhea) and anovulatory infertility, women often develop enlarged clitoris (clitoromegaly) with chronic high-dosage anabolic steroid use 92, 93.
Irreversible changes include male-pattern baldness and breast development (gynecomastia) in men 96, 97. Anabolic steroids may also act upon the hormone system to increase the risk of testicular cancer, especially when steroids are used in combination with insulin-like growth factor 98.
In females, anabolic steroids cause masculinization or the abnormal development of male sexual characteristics in a female. Specifically, breast size and body fat decrease, the skin becomes coarse, and the voice deepens 99. Women may experience excessive growth of body hair (hirsutism) but lose scalp hair 100. With continued administration of anabolic steroids, some of these effects become irreversible. It is commonly believed that anabolic steroids will produce irreversible enlargement of the clitoris in females, although there are no studies on this 101.
Cardiovascular disease
Anabolic steroids have been associated with a variety of adverse cardiovascular effects, including dyslipidemia, high blood pressure, increased atherosclerosis, left ventricular hypertrophy, decreased function of the heart’s ventricles, abnormal heart remodeling and scarring, arrhythmia, and thrombophilia (increased tendency of blood to clot) 102, 103, 43, 104, 105 and cardiovascular diseases such as heart attacks, artery damage, and strokes even in athletes younger than 30 106, 107, 108, 109. Of these potential adverse effects, the strongest data relate to hyperlipidemia. Anabolic steroids have consistently been associated with low serum high-density lipoprotein (HDL) cholesterol (“good” cholesterol) and increasing the level of low-density lipoprotein (LDL) (“bad” cholesterol) concentrations in men and women 109, 65; orally ingested alkylated anabolic steroids may cause profound suppression of serum HDL cholesterol (“good” cholesterol). High LDL (“abd” cholesterol) and low HDL (“good” cholesterol) levels increase the risk of atherosclerosis, a condition in which fatty substances are deposited inside arteries and disrupt blood flow. If blood is prevented from reaching the heart or brain, the result can be a heart attack or stroke, respectively. Anabolic steroids also increase the risk that blood clots will form in blood vessels, potentially disrupting blood flow and damaging the heart muscle, so that it does not pump blood effectively 110.
Infections
Many people who inject anabolic steroids may use nonsterile injection techniques or share contaminated needles with other users. This puts these steroid users at risk for acquiring life threatening viral infections, such as HIV and hepatitis B and C 111. In addition, animal models indicate that anabolic steroids suppress the immune system, which could worsen infections 112.
Liver diseases
Anabolic steroid misuse has been associated with liver damage 113, 114, liver tumor 108, 115, 116 and a rare condition called peliosis hepatis, in which blood-filled cysts form in the liver 117. The cysts can rupture, causing internal bleeding and even death in rare cases 118.
Anabolic steroids can also produce jaundice, or yellowing of the skin or eyes, as a result of damage to the liver 119, 120.
Musculoskeletal system side effects
Rising levels of testosterone and other sex hormones normally trigger the growth spurt that occurs during puberty and adolescence. These rising levels of testosterone also provide the signals to stop growth 121. When a child or adolescent takes anabolic steroids, the resulting artificially high sex hormone levels can prematurely signal the bones to stop growing 122.
Evidence suggests that weightlifters who misuse anabolic steroids have stiffer tendons, which could lead to an increased risk for tendon injury 123.
Skin problems
Anabolic steroid misuse can cause acne, hair loss on the head, cysts, and oily hair and skin 124, 125, 126, 100. Users who inject anabolic steroids may also develop pain and abscess formation at injection sites 127.
Aggression
Case reports and small studies indicate that anabolic steroids increase irritability and aggression 128, although findings may be confounded by personality traits that are overrepresented in steroid users (i.e., antisocial, borderline, and histrionic personality disorder) and use of other drugs 129, 130. People who misuse anabolic steroids report more anger than nonusers, as well as more fights, verbal aggression, and violence toward their significant others, sometimes called “roid rage” 131, 132. One study suggests that the mood and behavioral effects seen during anabolic steroid misuse may result from secondary hormonal changes 128.
Scientists have attempted to test the association between anabolic steroids and aggression by administering high steroid doses or placebo for days or weeks to human volunteers and then assessing behavioral symptoms. In one such study, researchers found that testosterone over a six week period was associated with increased aggression, as assessed by a questionnaire and computer-based model of aggressive behavior 133. In addition, high steroid doses produced greater feelings of irritability and aggression than placebo 134, although the effects appear to be highly variable across individuals 135 and other studies have not shown that effect 136. One possible explanation, according to the researchers, is that some but not all anabolic steroids increase irritability and aggression.
Psychiatric disorders
Anabolic steroid users are more likely than nonusers to report anxiety 137, 138. Moderate to high doses of anabolic steroids are also associated with major mood disorders such as mania, hypomania, and major depression 138, 139. In one study, manic symptoms were not uniform across individuals, with most showing little psychological change, whereas a few demonstrated prominent effects 135.
Other Drug Use
Anabolic steroid users are more likely to use drugs such as marijuana, prescription opioids, cocaine, or heroin 138, 139. In a study of men admitted to treatment for opioid use disorders, 25 percent reported prior use of anabolic steroids. Some described first learning about opioids from friends at the gym, and that they first purchased opioids from the same person who had sold them the anabolic steroids 140. In a study of anabolic steroid users dependent upon the injectable opioid analgesic nalbuphine, most reported that they began using nalbuphine to treat pain from weightlifting injuries. They also described widespread use of nalbuphine in their gyms 141.
Research also indicates that some users might turn to other drugs to alleviate some of the negative effects of anabolic steroids. For example, a study of 227 men admitted in 1999 to a private treatment center for addiction to heroin or other opioids found that 9.3 percent had previously misused anabolic steroids 142. Of these, most reported using opioids to counteract insomnia, irritability, depression, and withdrawal from anabolic steroids 142.
Anabolic steroid risks in teens
Unlike most illicit drug use, misuse of anabolic steroids most commonly begins in young adulthood rather than adolescence. But anabolic steroid use in teens is of concern, especially since the hormonal systems they interact with play a critical role in brain development during these years 143, 144, 145, 146, 147. In adolescent rats, exposure to anabolic steroids increased neuronal spine densities in the hippocampus and amygdala—brain regions involved in learning and emotions (e.g., aggression), respectively. Four weeks after withdrawal, these increases in neuronal spine densities returned to normal in the amygdala, but not in the hippocampus. This suggests that pubertal steroid exposure could produce long-lasting structural changes in certain brain regions 148.
Teens who use anabolic steroids may also be at increased risk for some cognitive side effects compared with adults. For example, males who begin using anabolic steroids during the teen years show increased impulsivity and decreased attention, compared to men who began using steroids in their adult years 149. In adolescent rats, anabolic steroid exposure is associated with electrolytic imbalances, hyperactivity, anxiety, and increased sympathetic autonomic modulation (e.g., fight or flight response) during adulthood, even when steroid use was discontinued during adolescence 150. In addition, adolescent male hamsters given anabolic steroids show increased aggression, even after steroid use is discontinued. These aggressive effects are paralleled by changes in levels of serotonin and androgen receptors in the rodent brain 151, 152, 153.
Anabolic steroids monitoring
Before initiating treatment with testosterone, diagnosis of hypogonadism require confirmation by measuring early morning testosterone levels on two separate days. Lipid profile, liver function tests, hemoglobin, hematocrit, prostate-specific antigen (PSA), and prostate exam in patients older than 40 years of age are necessary before initiating treatment.
During treatment with anabolic steroids, clinicians should obtain the patient’s lipid profile, liver function tests, hemoglobin, and hematocrit at 3 to 6 months, then every year. Women treated with testosterone for breast cancer require monitoring for signs of virilization. Patients on testosterone should be monitored for their response to treatment and adverse effects three to six months after initiation of therapy and then every year, especially for cardiac adverse events.
Men greater than 40 years of age with baseline prostate-specific antigen (PSA) more than 0.6 ng/mL should have their PSA levels measured and a prostate examination at 3 to 6 months. Treatment should be withheld in men with a palpable prostate nodule or prostate-specific antigen more than 4 ng/mL and in patients at high risk of prostate malignancy with prostate-specific antigen more than 3 ng/mL.
Testosterone level should be measured midway between injections in testosterone enanthate and testosterone cypionate, and dose and frequency adjustments should be implemented to keep testosterone concentration between 400 ng/dL and 700 ng/dL. Serum testosterone level should be measured two to eight hours after application and after fourteen days of starting the therapy or with dose titration in patients using a topical solution of testosterone.
Total serum testosterone should be measured periodically, starting from the first month after initiating therapy in patients using nasal testosterone gel, and treatment should terminate if total testosterone exceeds 1050 ng/dL. Serum testosterone level should be measured approximately 14 days after initiation of therapy, in the morning, before application of transdermal testosterone, at the end of the dosing interval in testosterone pellets, and 4 to 12 weeks after initiation of treatment and before the morning dose in patients using a buccal form of testosterone 154, 155.
Table 1. Cutoff values of testosterone for low testosterone (testosterone deficiency) diagnosis
| Cutoff Values | Year of Release and Update | |
|---|---|---|
| Expert opinion | Total testosterone or free testosterone below the lower limits of normal | Before Official Guideline |
| International Society for the Study of the Aging Male (ISSAM) | Total testosterone < 231 ng/dL (8 nmol/L) Total testosterone: 231–346 ng/dL (8–12 nmol/L) or free testosterone < 52 pg/mL | 2005 |
| Total testosterone < 230 ng/dL (8 nmol/L) total testosterone: 230–350 ng/dL (8–12 nmol/L) or free testosterone < 52 pg/mL, sex-hormone-binding-globulin (SHBG) | 2008 | |
| Total testosterone < 350 ng/dL (12 nmol/L) or free testosterone < 65 pg/mL | 2015 | |
| Endocrine Society | Total testosterone < 300 ng/dL or free testosterone < 5 ng/dL | 2006 |
| Total testosterone < 280–300 ng/dL or free testosterone < 5–9 ng/dL | 2010 | |
| Total testosterone < 300 ng/dL or free testosterone < 5 ng/dL | 2018 | |
| International Society for Sexual Medicine (ISSM) | Total testosterone < 350 ng/dL (12 nmol/L) | International Consultation for Sexual Medicine (ICSM) 2015 |
| American Urological Association (AUA) | Total testosterone < 300 ng/dL | 2018 |
Table 2. Clinical and biochemical parameters to be checked during testosterone therapy
| Parameters | Year 1 of treatment | After year 1 of treatment | ||||
|---|---|---|---|---|---|---|
| Baseline | 3 months | 6 months | 12 months | Annually | 18-24 months | |
| Clinical | ||||||
| Symptoms | X | X | X | X | X | |
| Body Mass Index | X | X | X | |||
| Waist circumference | X | X | X | X | ||
| Digital rectal examination | X | X | X | |||
| Blood pressure | X | X | X | X | ||
| Biochemistry | ||||||
| PSA (ng/mL) | X | X | X2 | X | X | |
| Hematocrit (%) | X | X | X1,2 | X | X | |
| Testosterone | X | X | X | X | ||
| Lipid and glycaemic profile | X | X | X | |||
| Instrumental | ||||||
| DEXA | X | X | ||||
Footnotes: 1) Population with polycythemia vera or at high risk of secondary polycythemia (e.g., sleep apnea, morbidobesity, heavy smokers, chronic obstructive pulmonary disease); 2) Prostate cancer survivors.
[Source 157 ]- Ganesan K, Rahman S, Zito PM. Anabolic Steroids. [Updated 2023 May 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482418[↩][↩]
- Anna L Goldman, Harrison G Pope, Shalender Bhasin, The Health Threat Posed by the Hidden Epidemic of Anabolic Steroid Use and Body Image Disorders Among Young Men, The Journal of Clinical Endocrinology & Metabolism, Volume 104, Issue 4, April 2019, Pages 1069–1074, https://doi.org/10.1210/jc.2018-01706[↩]
- Rashid H, Ormerod S, Day E. Anabolic androgenic steroids: what the psychiatrist needs to know. Adv Psychiatr Treat. 2007;13(3):203-211[↩]
- Bradley D Anawalt, Diagnosis and Management of Anabolic Androgenic Steroid Use, The Journal of Clinical Endocrinology & Metabolism, Volume 104, Issue 7, July 2019, Pages 2490–2500, https://doi.org/10.1210/jc.2018-01882[↩]
- Larance B, Degenhardt L, Copeland J, Dillon P. Injecting risk behaviour and related harm among men who use performance- and image-enhancing drugs. Drug Alcohol Rev. 2008 Nov;27(6):679-86. doi: 10.1080/09595230802392568[↩]
- Wade N. Anabolic Steroids: Doctors Denounce Them, but Athletes Aren’t Listening. Science. 1972 Jun 30;176(4042):1399-403. doi: 10.1126/science.176.4042.1399[↩][↩]
- Kouri EM, Pope HG Jr, Katz DL, Oliva P. Fat-free mass index in users and nonusers of anabolic-androgenic steroids. Clin J Sport Med. 1995 Oct;5(4):223-8. doi: 10.1097/00042752-199510000-00003[↩]
- Andrews MA, Magee CD, Combest TM, Allard RJ, Douglas KM. Physical Effects of Anabolic-androgenic Steroids in Healthy Exercising Adults: A Systematic Review and Meta-analysis. Curr Sports Med Rep. 2018 Jul;17(7):232-241. doi: 10.1249/JSR.0000000000000500[↩][↩]
- Fomiati R, Moore D, Latham JR, Fraser S, Lenton E, Seear K, et al. Understanding performance and image-enhancing drug injecting to improve health and minimise hepatitis C transmission: Findings and recommendations from a national qualitative project. Melbourne: The Australian Research Centre in Sex, Health and Society, La Trobe University; 2019.[↩][↩]
- Larance B, Degenhardt L, Dillon P, Copeland J. Rapid assessment of performance and image enhancing drugs (PIEDs) in New South Wales: Feasibility study 2005. Sydney: National Drug and Alcohol Research Centre; 2005.[↩][↩]
- Heard S, Iversen J, Geddes L, L M. Australian NSP Survey National Data Report 2014-2018. Sydney: The Kirby Institute; 2019.[↩][↩]
- Brands B, Sproule B, Marshman J. Drugs and Drug Abuse. 3 ed. Toronto: Addiction Research Foundation; 1998.[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Casaburi R, Storer T, Bhasin S. Androgen effects on body composition and muscle performance. In: Bhasin S, Gabelnick HL, Spieler JM, Swerdloff RS, Wang C, eds. Pharmacology, biology, and clinical applications of androgens: current status and future prospects. New York: Wiley-Liss, 1996:283-8.[↩]
- Wilson JD. Androgen abuse by athletes. Endocr Rev. 1988 May;9(2):181-99. doi: 10.1210/edrv-9-2-181[↩][↩]
- Strauss RH, Yesalis CE. Anabolic steroids in the athlete. Annu Rev Med. 1991;42:449-57. doi: 10.1146/annurev.me.42.020191.002313[↩]
- Haupt HA, Rovere GD. Anabolic steroids: a review of the literature. Am J Sports Med. 1984 Nov-Dec;12(6):469-84. doi: 10.1177/036354658401200613[↩]
- Elashoff JD, Jacknow AD, Shain SG, Braunstein GD. Effects of anabolic-androgenic steroids on muscular strength. Ann Intern Med. 1991 Sep 1;115(5):387-93. doi: 10.7326/0003-4819-115-5-387[↩]
- Cowart V. Steroids in Sports: After Four Decades, Time to Return These Genies to Bottle? JAMA. 1987;257(4):421–427. doi:10.1001/jama.1987.03390040031003[↩]
- Buckley WE, Yesalis CE, Friedl KE, Anderson WA, Streit AL, Wright JE. Estimated Prevalence of Anabolic Steroid Use Among Male High School Seniors. JAMA. 1988;260(23):3441–3445. doi:10.1001/jama.1988.03410230059028[↩]
- American College of Sports Medicine position stand on the use of anabolic-androgenic steroids in sports. Med Sci Sports Exerc. 1987 Oct;19(5):534-9.[↩]
- Llewellyn W. Molecular Nutrition. 9th Edition Jupiter; Florida: 2009. Anabolics.[↩]
- Pope HG, Brower KJ. Anabolic-Androgenic Steroid-Related Disorders. In: Sadock B, Sadock V, editors. Comprehensive Textbook of Psychiatry. Ninth Edition Lippincott Williams & Wilkins; Philadelphia, PA: 2009. pp. 1419–1431.[↩][↩][↩]
- Pope HG Jr, Katz DL. Affective and psychotic symptoms associated with anabolic steroid use. Am J Psychiatry. 1988 Apr;145(4):487-90. doi: 10.1176/ajp.145.4.487[↩]
- Lusetti M, Licata M, Silingardi E, Bonsignore A, Palmiere C. Appearance/Image- and Performance-Enhancing Drug Users: A Forensic Approach. Am J Forensic Med Pathol. 2018 Dec;39(4):325-329. doi: 10.1097/PAF.0000000000000424[↩]
- Jones IA, Togashi R, Hatch GFR 3rd, Weber AE, Vangsness CT Jr. Anabolic steroids and tendons: A review of their mechanical, structural, and biologic effects. J Orthop Res. 2018 Nov;36(11):2830-2841. doi: 10.1002/jor.24116[↩]
- Armstrong JM, Avant RA, Charchenko CM, Westerman ME, Ziegelmann MJ, Miest TS, Trost LW. Impact of anabolic androgenic steroids on sexual function. Transl Androl Urol. 2018 Jun;7(3):483-489. doi: 10.21037/tau.2018.04.23[↩][↩]
- Handelsman DJ. Clinical review: The rationale for banning human chorionic gonadotropin and estrogen blockers in sport. J Clin Endocrinol Metab. 2006 May;91(5):1646-53. doi: 10.1210/jc.2005-2569[↩][↩]
- Anawalt BD. Diagnosis and Management of Anabolic Androgenic Steroid Use. J Clin Endocrinol Metab. 2019 Jul 1;104(7):2490-2500. doi: 10.1210/jc.2018-01882[↩][↩][↩][↩][↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Corticosteroids. [Updated 2021 May 7]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548400[↩]
- Pinsky MR, Hellstrom WJ. Hypogonadism, ADAM, and hormone replacement. Ther Adv Urol. 2010 Jun;2(3):99-104. doi: 10.1177/1756287210369805[↩]
- Miech, R. A., Johnston, L. D., Patrick, M. E., & O’Malley, P. M. (2024). Monitoring the Future national survey results on drug use, 1975–2023: Overview and detailed results for secondary school students. Monitoring the Future Monograph Series. Ann Arbor, MI: Institute for Social Research, University of Michigan.[↩]
- Hartgens F, Kuipers H. Effects of androgenic-anabolic steroids in athletes. Sports Med. 2004;34(8):513-54. doi: 10.2165/00007256-200434080-00003[↩][↩][↩][↩]
- Performance and Image Enhancing Drugs: Factsheet. https://positivechoices.org.au/teachers/performance-and-image-enhancing-drugs-factsheet[↩][↩][↩][↩][↩][↩]
- Harris MA, Dunn M, Alwyn T. A qualitative exploration of the motivations underlying anabolic-androgenic steroid use from adolescence into adulthood. Health Psychology Report. 2016;4[↩][↩]
- Larance B, Jacka, B. Performance and Image Enhancing Drugs: Factsheet: Positive Choices; 2017[↩][↩]
- Parkinson AB, Evans NA. Anabolic androgenic steroids: a survey of 500 users. Med Sci Sports Exerc. 2006 Apr;38(4):644-51. doi: 10.1249/01.mss.0000210194.56834.5d[↩][↩]
- Shahidi NT. A review of the chemistry, biological action, and clinical applications of anabolic-androgenic steroids. Clin Ther. 2001 Sep;23(9):1355-90. doi: 10.1016/s0149-2918(01)80114-4[↩][↩]
- Cardoso RC, Padmanabhan V. Prenatal Steroids and Metabolic Dysfunction: Lessons from Sheep. Annu Rev Anim Biosci. 2019 Feb 15;7:337-360. doi: 10.1146/annurev-animal-020518-115154[↩][↩]
- Kanayama G, Hudson JI, Pope HG Jr. Long-term psychiatric and medical consequences of anabolic-androgenic steroid abuse: a looming public health concern? Drug Alcohol Depend. 2008 Nov 1;98(1-2):1-12. doi: 10.1016/j.drugalcdep.2008.05.004[↩][↩]
- Kanayama G, Brower KJ, Wood RI, Hudson JI, Pope HG Jr. Treatment of anabolic-androgenic steroid dependence: Emerging evidence and its implications. Drug Alcohol Depend. 2010 Jun 1;109(1-3):6-13. doi: 10.1016/j.drugalcdep.2010.01.011[↩][↩]
- Kicman AT. Pharmacology of anabolic steroids. Br J Pharmacol. 2008 Jun;154(3):502-21. doi: 10.1038/bjp.2008.165[↩]
- Kanayama G, Brower KJ, Wood RI, Hudson JI, Pope HG. Issues for DSM-V: clarifying the diagnostic criteria for anabolic-androgenic steroid dependence. Am J Psychiatry. 2009;166(6):642-645. doi:10.1176/appi.ajp.2009.08111699[↩][↩]
- Pope HG, Kanayama G, Athey A, Ryan E, Hudson JI, Baggish A. The lifetime prevalence of anabolic-androgenic steroid use and dependence in Americans: current best estimates. Am J Addict Am Acad Psychiatr Alcohol Addict. 2014;23(4):371-377. doi:10.1111/j.1521-0391.2013.12118.x[↩][↩]
- Brower KJ, Blow FC, Young JP, Hill EM. Symptoms and correlates of anabolic-androgenic steroid dependence. Br J Addict. 1991 Jun;86(6):759-68. doi: 10.1111/j.1360-0443.1991.tb03101.x[↩]
- Malone DA Jr, Dimeff RJ, Lombardo JA, Sample RH. Psychiatric effects and psychoactive substance use in anabolic-androgenic steroid users. Clin J Sport Med. 1995;5(1):25-31. doi: 10.1097/00042752-199501000-00005[↩]
- ACSM’s Introduction to Exercise Science, Third Edition. https://www.acsm.org/education-resources/books/introduction-exercise-science[↩]
- Melo Junior AF, Dalpiaz PLM, Sousa GJ, Oliveira PWC, Birocale AM, Andrade TU, Abreu GR, Bissoli NS. Nandrolone alter left ventricular contractility and promotes remodelling involving calcium-handling proteins and renin-angiotensin system in male SHR. Life Sci. 2018 Sep 1;208:239-245. doi: 10.1016/j.lfs.2018.07.041[↩]
- Zhou S, Glowacki J. Dehydroepiandrosterone and Bone. Vitam Horm. 2018;108:251-271. doi: 10.1016/bs.vh.2018.01.005[↩]
- Bhasin S, Woodhouse L, Storer TW. Proof of the effect of testosterone on skeletal muscle. J Endocrinol. 2001 Jul;170(1):27-38. doi: 10.1677/joe.0.1700027[↩]
- Bhasin S, Storer TW, Berman N, Callegari C, Clevenger B, Phillips J, Bunnell TJ, Tricker R, Shirazi A, Casaburi R. The effects of supraphysiologic doses of testosterone on muscle size and strength in normal men. N Engl J Med. 1996 Jul 4;335(1):1-7. doi: 10.1056/NEJM199607043350101[↩][↩]
- FOSS GL, SIMPSON SL. Oral methyltestosterone and jaundice. Br Med J. 1959 Jan 31;1(5117):259-63. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1992426/pdf/brmedj02956-0023.pdf[↩]
- Liu P, Handelsman D. Androgen therapy in non-gonadal disease. Testosterone: Action, Deficiency and Substitution, 3rd ed Springer-Verlag, Berlin: 2004. pp. 445-95.[↩]
- Orr R, Fiatarone Singh M. The anabolic androgenic steroid oxandrolone in the treatment of wasting and catabolic disorders: review of efficacy and safety. Drugs. 2004;64(7):725-50. doi: 10.2165/00003495-200464070-00004[↩]
- Zitzmann M, Nieschlag E.Androgens and bone metabolism Testosterone 2004Cambridge University Press: UK; 233–254.In: Nieschlag E, Behre HM (eds).3rd edn.[↩]
- Orwoll ES. Androgens as anabolic agents for bone. Trends Endocrinol Metab. 1996 Apr;7(3):77-84. doi: 10.1016/1043-2760(96)00024-0[↩]
- Thigpen AE, Silver RI, Guileyardo JM, Casey ML, McConnell JD, Russell DW. Tissue distribution and ontogeny of steroid 5 alpha-reductase isozyme expression. J Clin Invest. 1993 Aug;92(2):903-10. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC294929/pdf/jcinvest00029-0377.pdf[↩]
- Larionov AA, Vasyliev DA, Mason JI, Howie AF, Berstein LM, Miller WR. Aromatase in skeletal muscle. J Steroid Biochem Mol Biol. 2003 Mar;84(4):485-92. doi: 10.1016/s0960-0760(03)00059-1[↩]
- McEwan IJ, Brinkmann AO. Androgen Physiology: Receptor and Metabolic Disorders. [Updated 2021 Jul 2]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279028[↩]
- Nassar GN, Leslie SW. Physiology, Testosterone. [Updated 2022 Jan 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526128[↩]
- Clark BJ, Prough RA, Klinge CM. Mechanisms of Action of Dehydroepiandrosterone. Vitam Horm. 2018;108:29-73. doi: 10.1016/bs.vh.2018.02.003[↩][↩]
- Saez, J. M., Forest, M. G., Morera, A. M., & Bertrand, J. (1972). Metabolic clearance rate and blood production rate of testosterone and dihydrotestosterone in normal subjects, during pregnancy, and in hyperthyroidism. The Journal of clinical investigation, 51(5), 1226–1234. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC292254/pdf/jcinvest00201-0192.pdf[↩]
- Plant TM, Marshall GR. The functional significance of FSH in spermatogenesis and the control of its secretion in male primates. Endocr Rev. 2001 Dec;22(6):764-86. doi: 10.1210/edrv.22.6.0446[↩]
- Kanayama G, Pope HG Jr. History and epidemiology of anabolic androgens in athletes and non-athletes. Mol Cell Endocrinol. 2018 Mar 15;464:4-13. doi: 10.1016/j.mce.2017.02.039[↩]
- Hakansson A, Mickelsson K, Wallin C, Berglund M. Anabolic androgenic steroids in the general population: user characteristics and associations with substance use. Eur Addict Res. 2012;18(2):83-90. doi: 10.1159/000333037[↩]
- Bhasin S, Woodhouse L, Casaburi R, Singh AB, Bhasin D, Berman N, Chen X, Yarasheski KE, Magliano L, Dzekov C, Dzekov J, Bross R, Phillips J, Sinha-Hikim I, Shen R, Storer TW. Testosterone dose-response relationships in healthy young men. Am J Physiol Endocrinol Metab. 2001 Dec;281(6):E1172-81. doi: 10.1152/ajpendo.2001.281.6.E1172[↩][↩]
- Bhasin S, Woodhouse L, Casaburi R, Singh AB, Mac RP, Lee M, Yarasheski KE, Sinha-Hikim I, Dzekov C, Dzekov J, Magliano L, Storer TW. Older men are as responsive as young men to the anabolic effects of graded doses of testosterone on the skeletal muscle. J Clin Endocrinol Metab. 2005 Feb;90(2):678-88. doi: 10.1210/jc.2004-1184[↩]
- Huang G, Basaria S, Travison TG, Ho MH, Davda M, Mazer NA, Miciek R, Knapp PE, Zhang A, Collins L, Ursino M, Appleman E, Dzekov C, Stroh H, Ouellette M, Rundell T, Baby M, Bhatia NN, Khorram O, Friedman T, Storer TW, Bhasin S. Testosterone dose-response relationships in hysterectomized women with or without oophorectomy: effects on sexual function, body composition, muscle performance and physical function in a randomized trial. Menopause. 2014 Jun;21(6):612-23. doi: 10.1097/GME.0000000000000093[↩]
- Huang G, Basaria S. Do anabolic-androgenic steroids have performance-enhancing effects in female athletes? Mol Cell Endocrinol. 2018 Mar 15;464:56-64. doi: 10.1016/j.mce.2017.07.010[↩]
- American Academy of Pediatrics. Adolescents and anabolic steroids: a subject review. American Academy of Pediatrics. Committee on Sports Medicine and Fitness. Pediatrics. 1997;99(6):904-908.[↩]
- Testosterone Topical. https://medlineplus.gov/druginfo/meds/a605020.html[↩]
- Trenton AJ, Currier GW. Behavioural manifestations of anabolic steroid use. CNS Drugs. 2005;19(7):571-95. doi: 10.2165/00023210-200519070-00002[↩][↩][↩][↩]
- Adolescents and anabolic steroids: a subject review. American Academy of Pediatrics. Committee on Sports Medicine and Fitness. Pediatrics. 1997 Jun;99(6):904-8.[↩]
- Evans NA. Gym and tonic: a profile of 100 male steroid users. Br J Sports Med. 1997 Mar;31(1):54-8. doi: 10.1136/bjsm.31.1.54[↩]
- Rashid H, Ormerod S, Day E. Anabolic androgenic steroids: what the psychiatrist needs to know. Adv Psychiatr Treat. 2007;13(3):203-211.[↩]
- Garner O, Iardino A, Ramirez A, Yakoby M. Cardiomyopathy induced by anabolic-androgenic steroid abuse. BMJ Case Rep. 2018 Jul 23;2018:bcr2017223891. doi: 10.1136/bcr-2017-223891[↩]
- Costanzo PR, Pacenza NA, Aszpis SM, Suárez SM, Pragier UM, Usher JGS, Vásquez Cayoja M, Iturrieta S, Gottlieb SE, Rey RA, Knoblovits P. Clinical and Etiological Aspects of Gynecomastia in Adult Males: A Multicenter Study. Biomed Res Int. 2018 May 29;2018:8364824. doi: 10.1155/2018/8364824[↩]
- Bhasin S, Brito JP, Cunningham GR, Hayes FJ, Hodis HN, Matsumoto AM, Snyder PJ, Swerdloff RS, Wu FC, Yialamas MA. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2018 May 01;103(5):1715-1744[↩]
- Angell P, Chester N, Green D, Somauroo J, Whyte G, George K. Anabolic steroids and cardiovascular risk. Sports Med. 2012 Feb 1;42(2):119-34. doi: 10.2165/11598060-000000000-00000[↩]
- Darke S, Torok M, Duflou J. Sudden or unnatural deaths involving anabolic-androgenic steroids. J Forensic Sci. 2014 Jul;59(4):1025-8. doi: 10.1111/1556-4029.12424[↩]
- Baggish AL, Weiner RB, Kanayama G, Hudson JI, Picard MH, Hutter AM Jr, Pope HG Jr. Long-term anabolic-androgenic steroid use is associated with left ventricular dysfunction. Circ Heart Fail. 2010 Jul;3(4):472-6. doi: 10.1161/CIRCHEARTFAILURE.109.931063[↩]
- Frati P, Busardò FP, Cipolloni L, Dominicis ED, Fineschi V. Anabolic Androgenic Steroid (AAS) related deaths: autoptic, histopathological and toxicological findings. Curr Neuropharmacol. 2015 Jan;13(1):146-59. doi: 10.2174/1570159X13666141210225414[↩]
- Bronson FH, Matherne CM. Exposure to anabolic-androgenic steroids shortens life span of male mice. Med Sci Sports Exerc. 1997 May;29(5):615-9. doi: 10.1097/00005768-199705000-00005[↩]
- Ip EJ, Lu DH, Barnett MJ, Tenerowicz MJ, Vo JC, Perry PJ. Psychological and physical impact of anabolic-androgenic steroid dependence. Pharmacotherapy. 2012 Oct;32(10):910-9. doi: 10.1002/j.1875-9114.2012.01123[↩][↩]
- Havnes IA, Jørstad ML, Wisløff C. Anabolic-androgenic steroid users receiving health-related information; health problems, motivations to quit and treatment desires. Subst Abuse Treat Prev Policy. 2019 May 16;14(1):20. doi: 10.1186/s13011-019-0206-5[↩][↩]
- Christou MA, Christou PA, Markozannes G, Tsatsoulis A, Mastorakos G, Tigas S. Effects of Anabolic Androgenic Steroids on the Reproductive System of Athletes and Recreational Users: A Systematic Review and Meta-Analysis. Sports Med. 2017 Sep;47(9):1869-1883. doi: 10.1007/s40279-017-0709-z[↩][↩]
- Bonetti A, Tirelli F, Catapano A, Dazzi D, Dei Cas A, Solito F, Ceda G, Reverberi C, Monica C, Pipitone S, Elia G, Spattini M, Magnati G. Side effects of anabolic androgenic steroids abuse. Int J Sports Med. 2008 Aug;29(8):679-87. doi: 10.1055/s-2007-965808[↩][↩]
- Schürmeyer T, Knuth UA, Belkien L, Nieschlag E. Reversible azoospermia induced by the anabolic steroid 19-nortestosterone. Lancet. 1984 Feb 25;1(8374):417-20. doi: 10.1016/s0140-6736(84)91752-5[↩]
- Pope HG Jr, Wood RI, Rogol A, Nyberg F, Bowers L, Bhasin S. Adverse health consequences of performance-enhancing drugs: an Endocrine Society scientific statement. Endocr Rev. 2014 Jun;35(3):341-75. doi: 10.1210/er.2013-1058[↩]
- Kanayama G, Hudson JI, DeLuca J, Isaacs S, Baggish A, Weiner R, Bhasin S, Pope HG Jr. Prolonged hypogonadism in males following withdrawal from anabolic-androgenic steroids: an under-recognized problem. Addiction. 2015 May;110(5):823-31. doi: 10.1111/add.12850[↩]
- Rasmussen JJ, Selmer C, Østergren PB, Pedersen KB, Schou M, Gustafsson F, Faber J, Juul A, Kistorp C. Former Abusers of Anabolic Androgenic Steroids Exhibit Decreased Testosterone Levels and Hypogonadal Symptoms Years after Cessation: A Case-Control Study. PLoS One. 2016 Aug 17;11(8):e0161208. doi: 10.1371/journal.pone.0161208[↩]
- Rahnema CD, Lipshultz LI, Crosnoe LE, Kovac JR, Kim ED. Anabolic steroid-induced hypogonadism: diagnosis and treatment. Fertil Steril. 2014 May;101(5):1271-9. doi: 10.1016/j.fertnstert.2014.02.002[↩]
- Ip EJ, Barnett MJ, Tenerowicz MJ, Kim JA, Wei H, Perry PJ. Women and anabolic steroids: an analysis of a dozen users. Clin J Sport Med. 2010 Nov;20(6):475-81. doi: 10.1097/JSM.0b013e3181fb5370[↩][↩]
- Gruber AJ, Pope HG Jr. Psychiatric and medical effects of anabolic-androgenic steroid use in women. Psychother Psychosom. 2000;69(1):19-26. doi: 10.1159/000012362[↩][↩]
- Liu PY, Swerdloff RS, Christenson PD, Handelsman DJ, Wang C; Hormonal Male Contraception Summit Group. Rate, extent, and modifiers of spermatogenic recovery after hormonal male contraception: an integrated analysis. Lancet. 2006 Apr 29;367(9520):1412-20. doi: 10.1016/S0140-6736(06)68614-5[↩]
- Torres-Calleja J, González-Unzaga M, DeCelis-Carrillo R, Calzada-Sánchez L, Pedrón N. Effect of androgenic anabolic steroids on sperm quality and serum hormone levels in adult male bodybuilders. Life Sci. 2001 Mar 2;68(15):1769-74. doi: 10.1016/s0024-3205(01)00972-9[↩]
- Calzada L, Torres-Calleja J, Martinez JM, Pedrón N. Measurement of androgen and estrogen receptors in breast tissue from subjects with anabolic steroid-dependent gynecomastia. Life Sci. 2001 Aug 17;69(13):1465-9. doi: 10.1016/s0024-3205(01)01227-9[↩][↩]
- Orlandi MA, Venegoni E, Pagani C. Gynecomastia in two young men with histories of prolonged use of anabolic androgenic steroids. J Ultrasound. 2010 Jun;13(2):46-8. doi: 10.1016/j.jus.2010.07.006[↩]
- Chimento A, Sirianni R, Zolea F, et al. Nandrolone and stanozolol induce Leydig cell tumor proliferation through an estrogen-dependent mechanism involving IGF-I system. J Cell Physiol. 2012;227(5):2079-2088. doi:10.1002/jcp.22936[↩]
- Baker J. A report on alterations to the speaking and singing voices of four women following hormonal therapy with virilizing agents. J Voice. 1999 Dec;13(4):496-507. doi: 10.1016/s0892-1997(99)80005-8[↩]
- Scott MJ 3rd, Scott AM. Effects of anabolic-androgenic steroids on the pilosebaceous unit. Cutis. 1992 Aug;50(2):113-6.[↩][↩]
- Nieschlag E, Vorona E. MECHANISMS IN ENDOCRINOLOGY: Medical consequences of doping with anabolic androgenic steroids: effects on reproductive functions. Eur J Endocrinol Eur Fed Endocr Soc. 2015;173(2):R47-58. doi:10.1530/EJE-15-0080[↩]
- Pope HG Jr, Wood RI, Rogol A, Nyberg F, Bowers L, Bhasin S. Adverse health consequences of performance-enhancing drugs: an Endocrine Society scientific statement. Endocr Rev. 2014 Jun;35(3):341-75. doi: 10.1210/er.2013-105[↩]
- Baggish AL, Weiner RB, Kanayama G, Hudson JI, Lu MT, Hoffmann U, Pope HG Jr. Cardiovascular Toxicity of Illicit Anabolic-Androgenic Steroid Use. Circulation. 2017 May 23;135(21):1991-2002. doi: 10.1161/CIRCULATIONAHA.116.026945[↩]
- Urhausen A, Albers T, Kindermann W. Are the cardiac effects of anabolic steroid abuse in strength athletes reversible? Heart. 2004 May;90(5):496-501. doi: 10.1136/hrt.2003.015719[↩]
- Vanberg P, Atar D. Androgenic anabolic steroid abuse and the cardiovascular system. Handb Exp Pharmacol. 2010;(195):411-457. doi:10.1007/978-3-540-79088-4_18[↩]
- Baggish AL, Weiner RB, Kanayama G, et al. Cardiovascular Toxicity of Illicit Anabolic-Androgenic Steroid Use. Circulation. 2017;135(21):1991-2002. doi:10.1161/CIRCULATIONAHA.116.026945[↩]
- El Scheich T, Weber A-A, Klee D, Schweiger D, Mayatepek E, Karenfort M. Adolescent ischemic stroke associated with anabolic steroid and cannabis abuse. J Pediatr Endocrinol Metab JPEM. 2013;26(1-2):161-165. doi:10.1515/jpem-2012-0057[↩]
- Santamarina RD, Besocke AG, Romano LM, Ioli PL, Gonorazky SE. Ischemic stroke related to anabolic abuse. Clin Neuropharmacol. 2008;31(2):80-85. doi:10.1097/WNF.0b013e3180ed4485[↩][↩]
- Palatini P, Giada F, Garavelli G, Sinisi F, Mario L, Michieletto M, Baldo-Enzi G. Cardiovascular effects of anabolic steroids in weight-trained subjects. J Clin Pharmacol. 1996 Dec;36(12):1132-40. doi: 10.1002/j.1552-4604.1996.tb04167.x[↩][↩]
- Linton MRF, Yancey PG, Davies SS, et al. The Role of Lipids and Lipoproteins in Atherosclerosis. [Updated 2019 Jan 3]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK343489[↩]
- Ip EJ, Yadao MA, Shah BM, Lau B. Infectious disease, injection practices, and risky sexual behavior among anabolic steroid users. AIDS Care. 2016;28(3):294-299. doi:10.1080/09540121.2015.1090539[↩]
- Hughes TK, Fulep E, Juelich T, Smith EM, Stanton GJ. Modulation of immune responses by anabolic androgenic steroids. Int J Immunopharmacol. 1995 Nov;17(11):857-63. doi: 10.1016/0192-0561(95)00078-x[↩]
- Robles-Diaz M, Gonzalez-Jimenez A, Medina-Caliz I, et al. Distinct phenotype of hepatotoxicity associated with illicit use of anabolic androgenic steroids. Aliment Pharmacol Ther. 2015;41(1):116-125. doi:10.1111/apt.13023[↩]
- Schwingel PA, Cotrim HP, Santos CR dos, et al. Recreational Anabolic-Androgenic Steroid Use Associated With Liver Injuries Among Brazilian Young Men. Subst Use Misuse. 2015;50(11):1490-1498. doi:10.3109/10826084.2015.1018550[↩]
- Kosaka A, Takahashi H, Yajima Y, Tanaka M, Okamura K, Mizumoto R, Katsuta K. Hepatocellular carcinoma associated with anabolic steroid therapy: report of a case and review of the Japanese literature. J Gastroenterol. 1996 Jun;31(3):450-4. doi: 10.1007/BF02355039[↩]
- Socas L, Zumbado M, Pérez-Luzardo O, et al. Hepatocellular adenomas associated with anabolic androgenic steroid abuse in bodybuilders: a report of two cases and a review of the literature. Br J Sports Med. 2005;39(5):e27. doi:10.1136/bjsm.2004.013599[↩]
- Wakabayashi T, Onda H, Tada T, Iijima M, Itoh Y. High incidence of peliosis hepatis in autopsy cases of aplastic anemia with special reference to anabolic steroid therapy. Acta Pathol Jpn. 1984 Sep;34(5):1079-86. doi: 10.1111/j.1440-1827.1984.tb07637.x[↩]
- Hansma P, Diaz FJ, Njiwaji C. Fatal Liver Cyst Rupture Due to Anabolic Steroid Use: A Case Presentation. Am J Forensic Med Pathol. 2016;37(1):21-22. doi:10.1097/PAF.0000000000000218[↩]
- Cabb E, Baltar S, Powers DW, Mohan K, Martinez A, Pitts E. The Diagnosis and Manifestations of Liver Injury Secondary to Off-Label Androgenic Anabolic Steroid Use. Case Rep Gastroenterol. 2016;10(2):499-505. doi:10.1159/000448883[↩]
- Yoshida EM, Erb SR, Scudamore CH, Owen DA. Severe cholestasis and jaundice secondary to an esterified testosterone, a non-C17 alkylated anabolic steroid. J Clin Gastroenterol. 1994 Apr;18(3):268-70. doi: 10.1097/00004836-199404000-00036[↩]
- Zemel BS, Katz SH. The contribution of adrenal and gonadal androgens to the growth in height of adolescent males. Am J Phys Anthropol. 1986;71(4):459-466. doi:10.1002/ajpa.1330710409[↩]
- BIERICH JR. Effects and side effects of anabolic steroids in children. Acta Endocrinol Suppl (Copenh). 1961;39(Suppl 63):89-110. doi: 10.1530/acta.0.039s089[↩]
- Seynnes OR, Kamandulis S, Kairaitis R, et al. Effect of androgenic-anabolic steroids and heavy strength training on patellar tendon morphological and mechanical properties. J Appl Physiol Bethesda Md 1985. 2013;115(1):84-89. doi:10.1152/japplphysiol.01417.2012[↩]
- Kraus SL, Emmert S, Schön MP, Haenssle HA. The dark side of beauty: acne fulminans induced by anabolic steroids in a male bodybuilder. Arch Dermatol. 2012;148(10):1210-1212. doi:10.1001/archdermatol.2012.855[↩]
- Melnik B, Jansen T, Grabbe S. Abuse of anabolic-androgenic steroids and bodybuilding acne: an underestimated health problem. J Dtsch Dermatol Ges J Ger Soc Dermatol JDDG. 2007;5(2):110-117. doi:10.1111/j.1610-0387.2007.06176.x[↩]
- Voelcker V, Sticherling M, Bauerschmitz J. Severe ulcerated “bodybuilding acne” caused by anabolic steroid use and exacerbated by isotretinoin. Int Wound J. 2010;7(3):199-201. doi:10.1111/j.1742-481X.2010.00676.x[↩]
- Rich JD, Dickinson BP, Flanigan TP, Valone SE. Abscess related to anabolic-androgenic steroid injection. Med Sci Sports Exerc. 1999 Feb;31(2):207-9. doi: 10.1097/00005768-199902000-00001[↩]
- Daly RC, Su TP, Schmidt PJ, Pagliaro M, Pickar D, Rubinow DR. Neuroendocrine and behavioral effects of high-dose anabolic steroid administration in male normal volunteers. Psychoneuroendocrinology. 2003 Apr;28(3):317-31. doi: 10.1016/s0306-4530(02)00025-2[↩][↩]
- Perry PJ, Kutscher EC, Lund BC, Yates WR, Holman TL, Demers L. Measures of aggression and mood changes in male weightlifters with and without androgenic anabolic steroid use. J Forensic Sci. 2003 May;48(3):646-51.[↩]
- Lundholm L, Frisell T, Lichtenstein P, Långström N. Anabolic androgenic steroids and violent offending: confounding by polysubstance abuse among 10,365 general population men. Addict Abingdon Engl. 2015;110(1):100-108. doi:10.1111/add.12715[↩]
- Burnett KF, Kleiman ME. Psychological characteristics of adolescent steroid users. Adolescence. 1994 Spring;29(113):81-9.[↩]
- Choi PY, Pope HG Jr. Violence toward women and illicit androgenic-anabolic steroid use. Ann Clin Psychiatry. 1994 Mar;6(1):21-5. doi: 10.3109/10401239409148835[↩]
- Kouri EM, Lukas SE, Pope HG Jr, Oliva PS. Increased aggressive responding in male volunteers following the administration of gradually increasing doses of testosterone cypionate. Drug Alcohol Depend. 1995 Nov;40(1):73-9. doi: 10.1016/0376-8716(95)01192-7[↩]
- Bahrke MS, Yesalis CE 3rd, Wright JE. Psychological and behavioural effects of endogenous testosterone and anabolic-androgenic steroids. An update. Sports Med. 1996 Dec;22(6):367-90. doi: 10.2165/00007256-199622060-00005[↩]
- Pope HG Jr, Kouri EM, Hudson JI. Effects of supraphysiologic doses of testosterone on mood and aggression in normal men: a randomized controlled trial. Arch Gen Psychiatry. 2000 Feb;57(2):133-40; discussion 155-6. doi: 10.1001/archpsyc.57.2.133[↩][↩]
- Tricker R, Casaburi R, Storer TW, et al. The effects of supraphysiological doses of testosterone on angry behavior in healthy eugonadal men–a clinical research center study. J Clin Endocrinol Metab. 1996;81(10):3754-3758. doi:10.1210/jcem.81.10.8855834[↩]
- Eklöf A-C, Thurelius A-M, Garle M, Rane A, Sjöqvist F. The anti-doping hot-line, a means to capture the abuse of doping agents in the Swedish society and a new service function in clinical pharmacology. Eur J Clin Pharmacol. 2003;59(8-9):571-577. doi:10.1007/s00228-003-0633-z[↩]
- Ip EJ, Lu DH, Barnett MJ, Tenerowicz MJ, Vo JC, Perry PJ. Psychological and physical impact of anabolic-androgenic steroid dependence. Pharmacotherapy. 2012;32(10):910-919. doi:10.1002/j.1875-9114.2012.01123[↩][↩][↩]
- Pope HG Jr, Katz DL. Psychiatric and medical effects of anabolic-androgenic steroid use. A controlled study of 160 athletes. Arch Gen Psychiatry. 1994 May;51(5):375-82. doi: 10.1001/archpsyc.1994.03950050035004[↩][↩]
- Kanayama G, Cohane GH, Weiss RD, Pope HG. Past anabolic-androgenic steroid use among men admitted for substance abuse treatment: an underrecognized problem? J Clin Psychiatry. 2003 Feb;64(2):156-60. doi: 10.4088/jcp.v64n0208[↩]
- Wines JD Jr, Gruber AJ, Pope HG Jr, Lukas SE. Nalbuphine hydrochloride dependence in anabolic steroid users. Am J Addict. 1999 Spring;8(2):161-4. doi: 10.1080/105504999305965[↩]
- Arvary D, Pope HG. Anabolic-androgenic steroids as a gateway to opioid dependence. N Engl J Med. 2000;342(20):1532. doi:10.1056/NEJM200005183422018[↩][↩]
- Keenan BS, Richards GE, Ponder SW, Dallas JS, Nagamani M, Smith ER. Androgen-stimulated pubertal growth: the effects of testosterone and dihydrotestosterone on growth hormone and insulin-like growth factor-I in the treatment of short stature and delayed puberty. J Clin Endocrinol Metab. 1993;76(4):996-1001. doi:10.1210/jcem.76.4.8473416[↩]
- Morris JA, Jordan CL, Breedlove SM. Sexual differentiation of the vertebrate nervous system. Nat Neurosci. 2004;7(10):1034-1039. doi:10.1038/nn1325[↩]
- Romeo RD, Richardson HN, Sisk CL. Puberty and the maturation of the male brain and sexual behavior: recasting a behavioral potential. Neurosci Biobehav Rev. 2002 May;26(3):381-91. doi: 10.1016/s0149-7634(02)00009-x[↩]
- Schulz KM, Molenda-Figueira HA, Sisk CL. Back to the future: The organizational-activational hypothesis adapted to puberty and adolescence. Horm Behav. 2009;55(5):597-604. doi:10.1016/j.yhbeh.2009.03.010[↩]
- Zehr JL, Nichols LR, Schulz KM, Sisk CL. Adolescent development of neuron structure in dentate gyrus granule cells of male Syrian hamsters. Dev Neurobiol. 2008;68(14):1517-1526. doi:10.1002/dneu.20675[↩]
- Cunningham RL, Claiborne BJ, McGinnis MY. Pubertal exposure to anabolic androgenic steroids increases spine densities on neurons in the limbic system of male rats. Neuroscience. 2007;150(3):609-615. doi:10.1016/j.neuroscience.2007.09.038[↩]
- Hildebrandt T, Langenbucher JW, Flores A, Harty S, Berlin HA, Berlin H. The influence of age of onset and acute anabolic steroid exposure on cognitive performance, impulsivity, and aggression in men. Psychol Addict Behav J Soc Psychol Addict Behav. 2014;28(4):1096-1104. doi:10.1037/a0036482[↩]
- Olivares EL, Silveira ALB, Fonseca FV, et al. Administration of an anabolic steroid during the adolescent phase changes the behavior, cardiac autonomic balance and fluid intake in male adult rats. Physiol Behav. 2014;126:15-24. doi:10.1016/j.physbeh.2013.12.006[↩]
- Grimes JM, Melloni RH. Prolonged alterations in the serotonin neural system following the cessation of adolescent anabolic-androgenic steroid exposure in hamsters (Mesocricetus auratus). Behav Neurosci. 2006;120(6):1242-1251. doi:10.1037/0735-7044.120.6.1242[↩]
- Ricci LA, Rasakham K, Grimes JM, Melloni RH. Serotonin-1A receptor activity and expression modulate adolescent anabolic/androgenic steroid-induced aggression in hamsters. Pharmacol Biochem Behav. 2006;85(1):1-11. doi:10.1016/j.pbb.2006.06.022[↩]
- Menard CS, Harlan RE. Up-regulation of androgen receptor immunoreactivity in the rat brain by androgenic-anabolic steroids. Brain Res. 1993 Sep 17;622(1-2):226-36. doi: 10.1016/0006-8993(93)90823-6[↩]
- Moretti S, Lega F, Rigoni L, Saluti G, Giusepponi D, Gioiello A, Manuali E, Rossi R, Galarini R. Multiclass screening method to detect more than fifty banned substances in bovine bile and urine. Anal Chim Acta. 2018 Nov 22;1032:56-67. doi: 10.1016/j.aca.2018.06.037[↩]
- Dahmani H, Louati K, Hajri A, Bahri S, Safta F. Development of an extraction method for anabolic androgenic steroids in dietary supplements and analysis by gas chromatography-mass spectrometry: Application for doping-control. Steroids. 2018 Oct;138:134-160. doi: 10.1016/j.steroids.2018.08.001[↩]
- Park, H. J., Ahn, S. T., & Moon, D. G. (2019). Evolution of Guidelines for Testosterone Replacement Therapy. Journal of clinical medicine, 8(3), 410. https://doi.org/10.3390/jcm8030410[↩]
- MALE HYPOGONADISM. https://uroweb.org/guidelines/sexual-and-reproductive-health/chapter/male-hypogonadism[↩]





{kind=link}