Contents
Peliosis hepatis
Peliosis hepatis also called “peliosis hepatitis” is rare benign blood vessel condition characterized by multiple, randomly distributed, blood-filled and cyst-like cavities throughout the liver 1, 2, 3, 4, 5. These blood-filled cavities communicate with the hepatic sinusoids and are associated with rupture of the reticulin framework 3. The size of the cystic lesions may vary from 1 millimeter to several centimeters 6. The cystic lesions are often irregularly shaped and in many cases are incompletely lined with endothelium 7. Peliosis hepatis has been described as typically involving the entire liver 6.
Peliosis mostly exists without symptoms (asymptomatic) being incidentally found on imaging or during an autopsy 8. However, with the progress of modern medical imaging technologies such as ultrasound, magnetic resonance imaging (MRI), FDG-PET (fluorodeoxyglucose positron emission tomography) or computed tomography (CT) scan, peliosis hepatis is now more frequently encountered in clinical practice 9. Despite these various medical imaging modalities, imaging may be inadequate for establishing a clear diagnosis of peliosis 10, 11.
Peliosis hepatis can occur at any age. Although a fetal form exists, peliosis hepatis usually develops in adults without regard to sex 6.
The cause of peliosis hepatis can be related to drugs including anabolic steroids, oral contraceptives, corticosteroids, tamoxifen, diethylstilbestrol, azathioprine, 6-thioguanine, 6-mercaptopurine, and methotrexate; toxins such as polyvinyl chloride, arsenic, and thorium oxide; chronic wasting diseases (e.g., tuberculosis, leprosy, and various cancers, particularly hepatocellular carcinoma); liver and kidney transplantation; and Bartonella henselae and Bartonella quintana infection in AIDS so-called bacillary peliosis 12, 13, 14, 15, 6. In addition, several other conditions are described as associated with peliosis hepatis, including sprue (a disorder in which the intestines are unable to absorb nutrients from food), diabetes mellitus, necrotizing vasculitis, and blood disorders including multiple myeloma, aplastic anemia, Hodgkin disease, and myelofibrosis 6. Moreover, peliosis hepatis may develop after kidney or heart transplantation. In 20 to 50% of patients, no associated condition is identified 6.
Peliosis hepatis is very difficult to diagnose. The diagnosis of peliosis hepatis is often missed or delayed because it is usually asymptomatic, and its radiologic appearance closely resembles a benign and malignant/pre-malignant lesions or multiple abscesses 16, 17. Radiological imaging shows a broad spectrum of appearances because of its dependence on the blood supply to the lesions. Laparoscopy is a useful examination to sporadically detect dark-blue or dark-red patchy patterns on the liver surface, which is a characteristic finding of peliosis hepatis 18. Pathological findings are considered the gold standard for the diagnosis of peliosis hepatis, being histologically characterized by blood-filled cavities. However, a case has been reported in which repeated biopsies were required to diagnose peliosis hepatis 19.
The correct diagnosis of peliosis hepatis is important because withdrawal of the offending drug or toxin can resolve the disease and prevent serious complications such as hepatic failure or death related to intraabdominal hemorrhage 6. Because of peliosis hepatis potential complications, surgical resection of the involved liver parenchyma should always be considered. In HIV-related peliosis hepatis caused by Bartonella henselae, clinical improvement has been documented with the use of antibiotics (i.e., erythromycin).
Figure 1. Peliosis hepatis
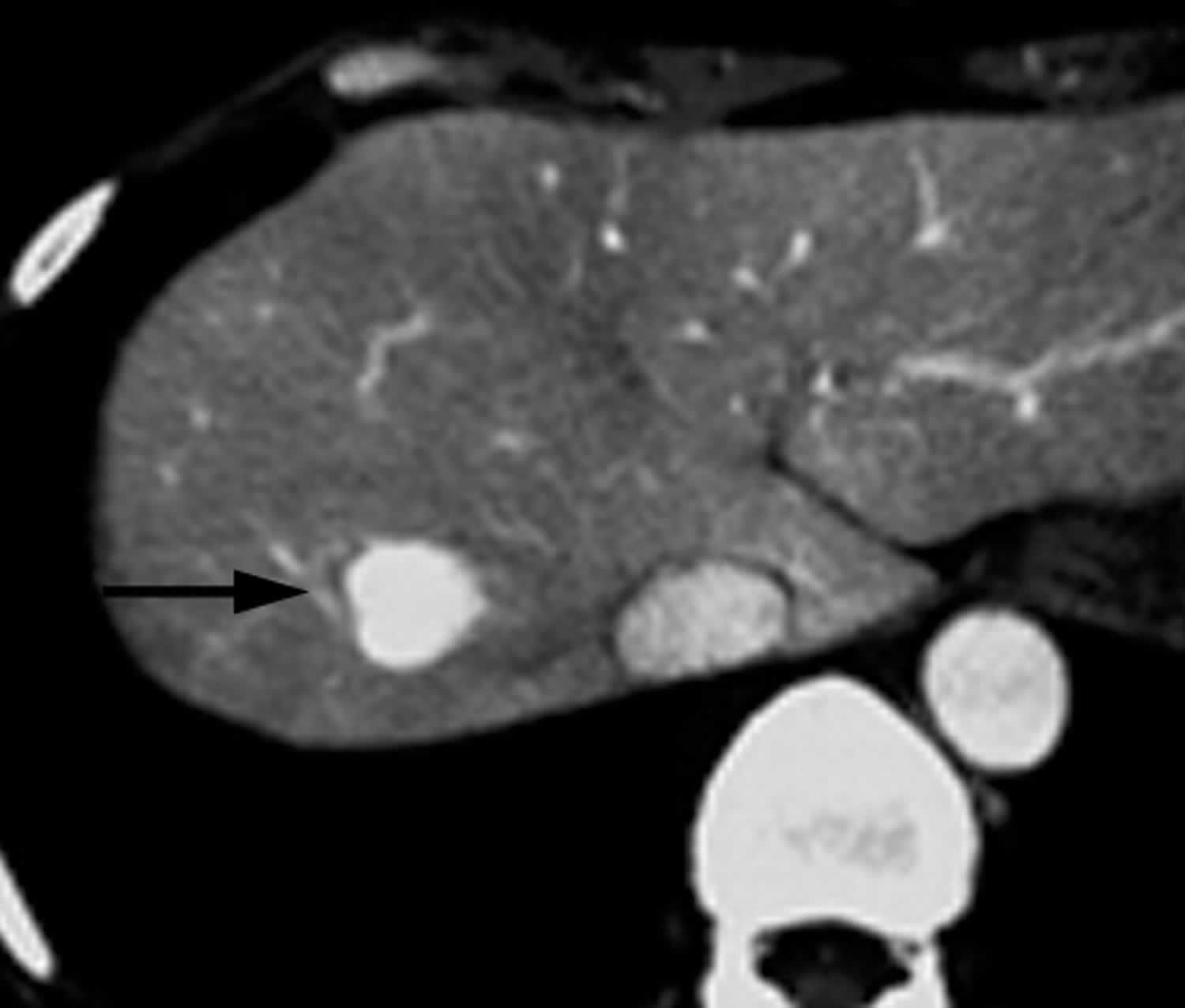
Footnotes: 51-year-old woman with history of benign ovarian tumor and incidentally discovered hepatic mass. On contrast-enhanced CT during hepatic arterial phase, lesion (arrow) shows marked homogeneous contrast enhancement.
[Source 6 ]Peliosis hepatis cause
The cause of peliosis hepatis can be related to drugs including anabolic steroids, oral contraceptives, corticosteroids, tamoxifen, diethylstilbestrol, azathioprine, 6-thioguanine, 6-mercaptopurine, and methotrexate; toxins such as polyvinyl chloride, arsenic, and thorium oxide; chronic wasting diseases (e.g., tuberculosis, leprosy); cancers, particularly hepatocellular carcinoma; liver and kidney transplantation; and Bartonella henselae and Bartonella quintana infection in AIDS so-called bacillary peliosis 12, 13, 14, 15, 6. In addition, several other conditions are described as associated with peliosis hepatis, including sprue (a disorder in which the intestines are unable to absorb nutrients from food), diabetes mellitus, alcoholic liver disease, necrotizing vasculitis, and blood disorders including multiple myeloma, aplastic anemia, Hodgkin disease, and myelofibrosis 20, 21, 14, 6. Moreover, peliosis hepatis may develop after kidney or heart transplantation. In 20 to 50% of patients, no associated condition is identified 6.
Peliosis hepatis causes 22:
- Idiopathic: 20 to 50% of cases
- Toxins
- arsenic
- polyvinyl chloride (PVC)
- thorium oxide
- Drugs
- anabolic steroids
- azathioprine
- corticosteroids
- diethylstilbestrol (DES)
- immunoglobulin therapy
- methotrexate
- oral contraceptives
- tamoxifen
- 6-thioguanine (6-TG)
- 6-mercaptopurine (6-MP)
- Chronic illness
- malignancy, particularly hepatocellular carcinoma
- tuberculosis (TB)
- leprosy
- celiac sprue
- diabetes mellitus
- necrotizing vasculitis
- hematologic disorders: Hodgkin disease, multiple myeloma
- Infection in AIDS
- bacillary peliosis caused by Bartonella henselae, Bartonella quintana and Rochalimaea henselae
- Kidney or heart transplantation
Peliosis hepatis pathophysiology
Peliosis hepatis pathogenesis remains poorly understood, with various investigators proposing that the primary event could be obstruction of hepatic outflow at the sinusoidal level, direct breakdown of sinusoidal borders, dilatation of the central vein of the hepatic lobule, or hepatocellular necrosis leading to cavity formation 4. Lastly, post-sinusoidal obstruction from several conditions such as malignant invasion, autoimmune inflammation, and drug injury is also hypothesized to be an alternate mechanism in the formation of peliosis hepatis 23.
The anatomy of the sinusoidal capillaries is different than other capillary beds within the body. The fenestrations which are present within the liver allow for passes and filtration of larger molecules such as albumin 23. Epithelial damage can result from smoking, which can disrupt the architecture through the formation of free radicals. This damage, in turn, impairs vasodilation by inhibiting nitric oxide formation, which allows for normal physiologic relaxation of the arteries 23. Additionally, inflammation, whether it be autoimmune, direct trauma through surgical instrumentation, medication-induced, or invasion by malignancy, can result in the recruitment of inflammatory cytokines and cells, sometimes resulting in further epithelial damage 23. An alternate mechanism may be the depletion of glutathione, a critical regulatory molecule that assists in many biochemical detoxification reactions, which may disrupt the integrity of the epithelial wall and allow toxic metabolites to build up. However, through signal proteins such as vascular endothelial growth factor and others, re-endothelization can occur; thus, that is why using the absence of epithelial lining on imaging studies is not adequate to diagnose patients with peliosis hepatis, though it can raise the concern for it 24, 25.
Histologically, hepatic peliosis is characterized by multiple mottled blood-filled cyst-like spaces within the liver with associated sinusoidal dilatation 26, 27. These vary in size from <1 mm to several centimeters in diameter.
Macroscopically, the liver appears dark or even purple, and usually, the entire liver is involved to a greater or lesser degree. Focal lesions may demonstrate central areas of hemorrhage.
Peliosis hepatis symptoms
Peliosis hepatis varies from minimal asymptomatic lesions that is diagnosed incidentally on imaging or during an autopsy to massive lesions that may present with cholestasis, hepatic failure, or spontaneous rupture requiring liver transplantation 16, 28. In some instances, enlarged liver (hepatomegaly), ascites (accumulation of fluid in the peritoneal cavity), portal hypertension, cholestasis, and hepatic failure may be present 6. Severe abdominal pain may result from rupture and intraperitoneal hemorrhage 6. In the case of bacillary peliosis, enlarged lymph node (lymphadenopathy) with Bartonella henselae and neurologic symptoms with Bartonella quintana are typical findings.
Peliosis hepatis complications
Peliosis hepatis complications may include:
- hepatic failure
- portal hypertension
- rupture and hemorrhage
There is no current consensus on whether patients with asymptomatic peliosis hepatis warrant routine imaging studies to monitor disease burden or progression. However, some experts believe annual or more frequent evaluation with ultrasound is adequate 29.
Although the incidence of intraperitoneal and intrahepatic hemorrhage do not seem to be common complications, the risk does exist 23. Thus surgical resection appears to assist in the avoidance of such complications, especially if imaging studies have demonstrated worsening of the cavitary lesions 30.
Peliosis hepatis diagnosis
Peliosis hepatis is very difficult to diagnose. The diagnosis of peliosis hepatis is often missed or delayed because it is usually asymptomatic, and its radiologic appearance closely resembles a benign and malignant/pre-malignant lesions or multiple abscesses 16, 17. Radiological imaging shows a broad spectrum of appearances because of its dependence on the blood supply to the lesions. In reality, the imaging findings of peliosis hepatis vary depending on the pathologic patterns of disease, various stages of the blood component of the lesions, and concomitant hepatic steatosis 31.
Laparoscopy is a useful examination to sporadically detect dark-blue or dark-red patchy patterns on the liver surface, which is a characteristic finding of peliosis hepatis 18. Pathological findings are considered the gold standard for the diagnosis of peliosis hepatis, being histologically characterized by blood-filled cavities. However, a case has been reported in which repeated biopsies were required to diagnose peliosis hepatis 19.
Ultrasound findings
Conventional gray-scale sonography appearances are non-specific, usually demonstrating an irregular hypoechoic region/mass 27
Doppler studies can show evidence of both perinodular and intranodular vascularity 26. Recently, the use of a sonographic contrast agent (Levovist [Schering], a galactose and palmitic acid compound) has been shown to provide a “fast surge” central-echo enhancement in peliotic lesions 32.
CT findings
Peliosis lesions appearance on pre-contrast CT (unenhanced CT) is variable, depending on liver density, but is usually of multiple hypoattenuating lesions of variable size 28. Central hemorrhage may lead to areas of hyperattenuation and even dystrophic calcification 26. CT findings vary with the size of lesions, presence or absence of thrombus within the cavities, and presence of hemorrhage. In particular, peliosis lesions may be spontaneously hyperattenuating to liver parenchyma in certain patients (probably related to intralesional hemorrhage). In addition, if peliotic cavities are smaller than 1 cm in diameter, CT findings may be normal 12. Calcifications within peliosis lesions have also been described.
On contrast-enhanced CT, peliosis lesions typically show early globular enhancement and multiple small, central accumulations of contrast material during the arterial phase, with a centrifugal progression of enhancement during the portal venous phase 26. In addition, some lesions can also show areas of increased attenuation. Notably, larger cavities communicating with sinusoids display the same attenuation of blood vessels, whereas thrombosed cavities have the same appearance as nonenhancing nodules 12. More often, during the arterial phase of contrast enhancement, peliosis lesions typically show early globular enhancement (vessel-like enhancement) and multiple small accumulations of contrast material in the center of the lesions the so-called target sign 28. During the portal venous phase, a centrifugal progression of enhancement without a mass effect on hepatic vessels is usually observed 28; however, a centripetal progression of enhancement can also be seen 33. On the delayed phase, late diffuse homogeneous hyperattenuation can also be seen in the phlebectatic type of peliosis hepatis because of the lack of hemorrhagic parenchymal necrosis 28. This accumulation of contrast material in the delayed phase can be useful in the differential diagnosis with other focal hepatic lesions that do not show blood pooling. In some instances, small (< 2 cm) peliotic lesions may also show hyperattenuation on both arterial and portal venous phase images.
MRI findings
On MRI, the signal intensities of peliosis lesions largely depend on the stage and the status of the blood components 26. On T1-weighted images, lesions are hypointense or heterogeneously hypointense if complicated by hemorrhage. On T2-weighted images, they are usually hyperintense compared to the liver parenchyma. Hemorrhagic parenchymal necrosis and thrombosed cavities manifest as non-enhancing areas. The differential diagnosis of peliosis hepatis may differ according to the actual imaging findings. On T2-weighted images, high signal together with early lesion enhancement can mimic hepatocellular carcinoma or hypervascular metastasis 33, while a bright T2-weighted signal and persistent delayed-phase CT or MRI may help distinguish peliosis hepatis.
Angiographic findings
On angiography, peliosis lesions appear as multiple vascular nodules (i.e., accumulations of contrast material) during the late arterial phase. The enhancement of peliotic lesions typically is more distinct during the parenchymal phase and persists during the portal venous phase 34.
Biopsy findings
A percutaneous needle biopsy can be used to obtain a specimen to further elucidate imaging findings and confirm the diagnosis. However, a percutaneous liver biopsy carries a risk of bleeding and hepatic hemangioma formation 1. Some authors claim that, due to the high risk of bleeding, an open biopsy is essential in order to realize the differential diagnosis under intraoperative ultrasound supervision 35, 36, 37, 38, 39, 40.
The gross pathologic appearance of peliosis hepatis is that of multiple, irregularly shaped blood-filled hepatic cavities 6. The lesions typically involve the entire liver, but focal peliosis hepatis has been described. At microscopic examination, cystic dilated sinusoids filled with red blood cells and bound by cords of liver cells can be seen (see Figure 1).
Macroscopic examinations show that peliotic lesions in the cutting section present hemorrhagic cyst cavities of various sizes (from < 1 mm to several centimeters) with features of “Swiss cheese”41, 42. From the histopathologic point of view, the differential diagnosis is used in order to diversify the sinusoids’ dilatation from Budd-Chiari syndrome, which determines a venous congestion of the liver due to a vascular occlusion 41, 17, 43.
Pathologists originally classified peliotic lesions by the presence or absence of endothelium (inner cellular lining of the blood vessels) 4. However, even though the blood-filled cavities do not always have endothelial lining , it has been observed that reendothelialization occurs rapidly 44, 45, 6. Therefore, the continuity or rupture of the endothelial lining of hepatic sinusoids is not a reliable criterion to define peliosis hepatis 12. To distinguish peliosis hepatis from hepatic sinusoidal dilatation, lesions should show evidence of rupture of the reticulin fibers that support the hepatocytes and sinusoids 4. This rupture may follow the intrinsic weakness of the fibers of the endothelial wall (peliosis hepatis of the phlebectatic type) or may be associated with focal hepatocyte necrosis (peliosis hepatis of the parenchymal type) 4.
Yanoff et al 46 described microscopically two different types of peliosis hepatis:
- “parenchymal peliosis,” which consists of irregular cavities that are surrounded neither by the sinusoidal cells nor by fibrous tissue, and
- “peliosis flebectasica” which is characterized by spherical regular cavities coated by endothelium and/or fibrosis 42, 44, 47
Peliotic lesions in bacillary peliosis contain clumps of organisms (i.e., Bartonella henselae and Bartonella quintana) that stain with the Warthin-Starry technique 4. Patients with bacillary peliosis often have peliosis of the spleen and lymph nodes and cutaneous angiomatous lesions 6.
Peliosis hepatis differential diagnosis
Peliosis hepatis differential diagnosis may include:
- Hepatic adenoma: Similar to peliosis, hepatic adenoma might also be associated with the long-term use of estrogens. In the case of diffuse peliosis hepatis, the differential diagnosis is relatively easy. In addition, the presence of fat in some adenomas is a useful sign to make a differential diagnosis. In certain instances, however, focal peliosis can be difficult to differentiate from adenomas. In these patients, biopsy is often required to reach a definitive diagnosis.
- Cavernous hemangioma: The typical enhancement pattern of hemangiomas (i.e., globular discontinuous contrast enhancement tends to be centripetal (periphery first) rather than centrifugal (center first)) is opposite of peliosis hepatis, and therefore differential diagnosis can be achieved in most patients. In addition, hemangiomas may be rather large lesions with a mass effect on the hepatic vessels, whereas peliotic lesions usually show no mass effect on hepatic vessels.
- Hepatocellular carcinoma (liver cancer): Hepatocellular carcinoma is usually hyperattenuating in the arterial phase with rapid washout in the portal venous phase and iso- or hypoattenuation in the delayed phase. Although rare, the possibility that peliosis hepatis may mimic the presence of hypervascular hepatocellular carcinoma has been reported in the literature. In these patients, biopsy is often necessary to reach a definitive diagnosis.
- Hepatic abscess (liver abscess): The differential diagnosis between peliosis hepatis and hepatic abscess is extremely important to avoid the percutaneous drainage of peliotic lesions, which can be dangerous and even fatal 48. With regard to imaging criteria, a hepatic abscess usually presents as a mass with a multiseptated or cluster-of-grapes appearance with nonenhancing contents.
- Focal nodular hyperplasia (benign tumor that forms in the liver): Focal nodular hyperplasias are typically homogeneously hyperattenuating masses on the arterial phase and isoattenuating on the portal venous and delayed phases. These lesions often have a central scar with low attenuation on the arterial and portal venous phases and enhancement on the delayed phase images. When such typical imaging characteristics of focal nodular hyperplasia are present, the differential diagnosis with peliosis hepatis can be achieved easily. Atypical forms of focal nodular hyperplasia may not show the characteristic enhancement patterns and the central scar just described, however, and thus pose some problems in the differential diagnosis with peliosis hepatis.
- Hepatic adenoma (an uncommon solid, benign liver lesion that develops in an otherwise normal-appearing liver) may contain fat
- Hypervascular metastases: Although some hypervascular metastases with fibrotic change can show mild hyperattenuation in the delayed phase, hypervascular metastases are usually totally hypoattenuating or isoattenuating in the delayed phase of contrast enhancement because of the rapid washout of contrast material. Thus, in general, peliotic lesions are rarely confused with hypervascular metastases.
- Hepatic sinusoidal dilation: usually the enhancement pattern is different on CT/MRI 49
Peliosis hepatis treatment
Peliosis hepatis treatment depends on the cause. When a causative drug or toxin is suspected, withdrawal of that agent may result in resolution. If peliosis hepatis seen in the setting of HIV/AIDS, antibiotic treatment may be effective in eradicating B. henselae. If focal and hemorrhagic, surgical resection may also be beneficial 26.
It is important not to drain peliosis, having mistaken it for a hepatic abscess, as bleeding can be life threatening 48.
Peliosis hepatis prognosis
The progression of peliosis hepatis is still largely uncertain 23. Researchers have not observed any apparent patterns of peliosis hepatis disease progression. The natural course of peliosis hepatis is regression after drug withdrawal, cessation of steroid therapy, or resolution of an associated infectious disease 6. However, peliosis hepatis can become worse asymptomatically and present as an accidental finding that occurs during investigations of other diseases or on the autopsy table 35, 47. A pseudotumoral and hemorrhagic evolution has also been described 47, 50.
Some authors claim that peliosis hepatis could be associated to liver failure with clinical features of hepatomegaly, portal hypertension, cholestasis, liver rupture leading to intraperitoneal hemorrhage (internal bleeding in which blood gathers in your peritoneal cavity) or shock and, more rarely, in cirrhotic patients positive for hepatitis C virus 47, 36, 51 or in cases of rupture of peliosis hepatis lesions with hemoperitoneum and hemodynamic decompensation with lethargy and abdominal pain 35, 47, 42, 36. In general, if untreated, ruptured peliosis hepatis may be rapidly fatal 51.
In other cases, especially when peliosis hepatis occurs at very young age, the disease shows important effects of compression with stenosis of the vena cava 52.
In still other cases, after the interruption of the steroid therapy or the resolution of the subsequent infections, a total regression was noticed 44, 36, 47. Peliosis hepatis regression can also occur without any connection with the past medical history, especially in those cases (20% to 50%) that do not allow association of peliosis hepatis to any kind of etiology 27.
Even though some authors support possible transplantation in acute liver failure cases or to use hepatectomy for the diagnosis and treatment of peliosis hepatis, surgery is more and more often used in urgent cases as treatment for the bleeding that may occur. At the same time, for the same issue, some authors proposed embolization that may be performed by an interventional radiologist or during the operation or the laparoscopic biopsy 53, 54.
- Crocetti D, Palmieri A, Pedullà G, Pasta V, D’Orazi V, Grazi GL. Peliosis hepatis: Personal experience and literature review. World J Gastroenterol. 2015 Dec 14;21(46):13188-94. doi: 10.3748/wjg.v21.i46.13188[↩][↩]
- Dong Y, Wang WP, Lim A, Lee WJ, Clevert DA, Höpfner M, Tannapfel A, Dietrich CF. Ultrasound findings in peliosis hepatis. Ultrasonography. 2021 Oct;40(4):546-554. doi: 10.14366/usg.20162[↩]
- Iwata T, Adachi K, Takahashi M. Peliosis Hepatis Mimicking Malignant Hypervascular Tumors. J Gastrointest Surg. 2017 Jun;21(6):1095-1098. doi: 10.1007/s11605-016-3298-5[↩][↩]
- Wanless IR. Vascular disorders. In: MacSween RNM, Burt AD, Portmann BC, Ishak KG, Scheuer PJ, Anthony PP, eds. Pathology of the liver, 4th ed. Glasgow, UK: Churchill Living stone,2002 : 553-555[↩][↩][↩][↩][↩][↩]
- Zak FG. Peliosis hepatis. Am J Pathol. 1950 Jan;26(1):1-15, incl 2 pl. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1942842/pdf/amjpathol00591-0007.pdf[↩]
- Iannaccone R, Federle MP, Brancatelli G, Matsui O, Fishman EK, Narra VR, Grazioli L, McCarthy SM, Piacentini F, Maruzzelli L, Passariello R, Vilgrain V. Peliosis hepatis: spectrum of imaging findings. AJR Am J Roentgenol. 2006 Jul;187(1):W43-52. https://doi.org/10.2214/AJR.05.0167[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Yanoff M, Rawson AJ. Peliosis hepatis. an anatomic study with demonstration of two varieties. Arch Pathol 1964;77:159-165.[↩]
- Torabi M, Hosseinzadeh K, Federle MP. CT of nonneoplastic hepatic vascular and perfusion disorders. Radiographics. 2008 Nov-Dec;28(7):1967-82. doi: 10.1148/rg.287085067[↩]
- Levin D, Hod N, Anconina R, Ezroh Kazap D, Shaco-Levy R, Lantsberg S. Peliosis Hepatis Simulating Metastatic Liver Disease on FDG PET/CT. Clin Nucl Med. 2018 Jul;43(7):e234-e236. doi: 10.1097/RLU.0000000000002114[↩]
- Maves CK, Caron KH, Bisset GS 3rd, Agarwal R. Splenic and hepatic peliosis: MR findings. AJR Am J Roentgenol. 1992 Jan;158(1):75-6. doi: 10.2214/ajr.158.1.1727362[↩]
- Tsuda K, Nakamura H, Murakami T, Kozuka T, Yoshii M, Isozaki K, Tsukahara Y, Takami M, Hanada M. Peliosis of the spleen with intraperitoneal hemorrhage. Abdom Imaging. 1993;18(3):283-5. doi: 10.1007/BF00198124[↩]
- Radin DR, Kanel GC. Peliosis hepatis in a patient with human immunodeficiency virus infection. AJR Am J Roentgenol. 1991 Jan;156(1):91-2. doi: 10.2214/ajr.156.1.1845436[↩][↩][↩][↩][↩]
- Ahsan N, Holman MJ, Riley TR, Abendroth CS, Langhoff EG, Yang HC. Peloisis hepatis due to Bartonella henselae in transplantation: a hemato-hepato-renal syndrome. Transplantation. 1998 Apr 15;65(7):1000-3. doi: 10.1097/00007890-199804150-00024[↩][↩]
- Bagheri SA, Boyer JL. Peliosis hepatis associated with androgenic-anabolic steroid therapy. A severe form of hepatic injury. Ann Intern Med. 1974 Nov;81(5):610-8. doi: 10.7326/0003-4819-81-5-610[↩][↩][↩]
- van Erpecum KJ, Janssens AR, Kreuning J, Ruiter DJ, Kroon HM, Grond AJ. Generalized peliosis hepatis and cirrhosis after long-term use of oral contraceptives. Am J Gastroenterol. 1988 May;83(5):572-5.[↩][↩]
- Clin Mol Hepatol. 2015;21 (4): 387-392. Publication Date (Web): 2015 December 24 (Case Report) https://doi.org/10.3350/cmh.2015.21.4.387[↩][↩][↩]
- Tsokos M, Erbersdobler A. Pathology of peliosis. Forensic Sci Int. 2005 Apr 20;149(1):25-33. doi: 10.1016/j.forsciint.2004.05.010[↩][↩][↩]
- Dai YN, Ren ZZ, Song WY, Huang HJ, Yang DH, Wang MS, Huang YC, Chen MJ, Zhang JJ, Tong YX, Pan HY. Peliosis hepatis: 2 case reports of a rare liver disorder and its differential diagnosis. Medicine (Baltimore). 2017 Mar;96(13):e6471. doi: 10.1097/MD.0000000000006471[↩][↩]
- Grønlykke L, Tarp B, Dutoit SH, Wilkens R. Peliosis hepatis: a complicating finding in a case of biliary colic. BMJ Case Rep. 2013 Sep 26;2013:bcr2013200539. doi: 10.1136/bcr-2013-200539[↩][↩]
- Elsing C, Placke J, Herrmann T. Alcohol binging causes peliosis hepatis during azathioprine therapy in Crohn’s disease. World J Gastroenterol. 2007 Sep 14;13(34):4646-8. doi: 10.3748/wjg.v13.i34.4646[↩]
- Sanz-Canalejas L, Gómez-Mampaso E, Cantón-Moreno R, Varona-Crespo C, Fortún J, Dronda F. Peliosis hepatis due to disseminated tuberculosis in a patient with AIDS. Infection. 2014 Feb;42(1):185-9. doi: 10.1007/s15010-013-0490-3[↩]
- Hepatic peliosis. https://radiopaedia.org/articles/hepatic-peliosis?lang=us[↩]
- Siddiqi I, Gupta N. Peliosis Hepatis. [Updated 2023 Jun 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554470[↩][↩][↩][↩][↩][↩]
- Kaplowitz N. The importance and regulation of hepatic glutathione. Yale J Biol Med. 1981 Nov-Dec;54(6):497-502. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2596047/pdf/yjbm00117-0089.pdf[↩]
- Bedair TM, ElNaggar MA, Joung YK, Han DK. Recent advances to accelerate re-endothelialization for vascular stents. J Tissue Eng. 2017 Sep 28;8:2041731417731546. doi: 10.1177/2041731417731546[↩]
- Iannaccone R, Federle MP, Brancatelli G, Matsui O, Fishman EK, Narra VR, Grazioli L, McCarthy SM, Piacentini F, Maruzzelli L, Passariello R, Vilgrain V. Peliosis hepatis: spectrum of imaging findings. AJR Am J Roentgenol. 2006 Jul;187(1):W43-52. doi: 10.2214/AJR.05.0167[↩][↩][↩][↩][↩][↩]
- Savastano S, San Bortolo O, Velo E, Rettore C, Altavilla G. Pseudotumoral appearance of peliosis hepatis. AJR Am J Roentgenol. 2005 Aug;185(2):558-9. doi: 10.2214/ajr.185.2.01850558[↩][↩][↩]
- Gouya H, Vignaux O, Legmann P, de Pigneux G, Bonnin A. Peliosis hepatis: triphasic helical CT and dynamic MRI findings. Abdom Imaging. 2001 Sep-Oct;26(5):507-9. doi: 10.1007/s00261-001-0023-x[↩][↩][↩][↩][↩]
- Orandi M, Pirozynski WJ. Peliosis hepatis. Can Med Assoc J. 1967 Apr 29;96(17):1219-20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1922866/pdf/canmedaj01213-0036.pdf[↩]
- Charatcharoenwitthaya P, Tanwandee T. Education and Imaging: hepatobiliary and pancreatic: spontaneous intrahepatic hemorrhage from peliosis hepatis-an uncommon complication of a rare liver disorder. J Gastroenterol Hepatol. 2014 Oct;29(10):1754. doi: 10.1111/jgh.12636[↩]
- Kim SH, Lee JM, Kim WH, Han JK, Lee JY, Choi BI. Focal peliosis hepatis as a mimicker of hepatic tumors: radiological-pathological correlation. J Comput Assist Tomogr. 2007 Jan-Feb;31(1):79-85. doi: 10.1097/01.rct.0000232919.22287.20[↩]
- Kleinig P, Davies RP, Maddern G, Kew J. Peliosis hepatis: central “fast surge” ultrasound enhancement and multislice CT appearances. Clin Radiol. 2003 Dec;58(12):995-8. doi: 10.1016/s0009-9260(03)00141-7[↩]
- Steinke K, Terraciano L, Wiesner W. Unusual cross-sectional imaging findings in hepatic peliosis. Eur Radiol. 2003 Aug;13(8):1916-9. doi: 10.1007/s00330-002-1675-9[↩][↩]
- Tsukamoto Y, Nakata H, Kimoto T, Noda T, Kuroda Y, Haratake J. CT and angiography of peliosis hepatis. AJR Am J Roentgenol. 1984 Mar;142(3):539-40. doi: 10.2214/ajr.142.3.539[↩]
- Choi SK, Jin JS, Cho SG, Choi SJ, Kim CS, Choe YM, Lee KY. Spontaneous liver rupture in a patient with peliosis hepatis: a case report. World J Gastroenterol. 2009 Nov 21;15(43):5493-7. doi: 10.3748/wjg.15.5493[↩][↩][↩]
- Samyn M, Hadzic N, Davenport M, Verma A, Karani J, Portmann B, Mieli-Vergani G. Peliosis hepatis in childhood: case report and review of the literature. J Pediatr Gastroenterol Nutr. 2004 Oct;39(4):431-4. doi: 10.1097/00005176-200410000-00024[↩][↩][↩][↩]
- Kleger A, Bommer M, Kunze M, Klaus J, Leithaeuser F, Wegener M, Adler G, Dikopoulos N. First reported case of disease: peliosis hepatis as cardinal symptom of Hodgkin’s lymphoma. Oncologist. 2009 Nov;14(11):1088-94. doi: 10.1634/theoncologist.2009-0215[↩]
- Tallón García M, Cobelas Cobelas MC, Fernández Sanmartín M, Bao Corral A, Granja Martínez MC. Peliosis hepática secundaria a tratamiento hormonal [Peliosis hepatitis secondary to hormone treatment]. An Pediatr (Barc). 2011 Oct;75(4):286-8. Spanish. doi: 10.1016/j.anpedi.2011.05.012[↩]
- Dai W, Zhong D. Peliosis hepatis mimicking cancer: A case report. Oncol Lett. 2013 Oct;6(4):960-962. doi: 10.3892/ol.2013.1479[↩]
- Battal B, Kocaoglu M, Atay AA, Bulakbasi N. Multifocal peliosis hepatis: MR and diffusion-weighted MR-imaging findings of an atypical case. Ups J Med Sci. 2010 May;115(2):153-6. doi: 10.1080/03009730903262118[↩]
- Sommacale D, Palladino E, Tamby EL, Diebold MD, Kianmanesh AR. Spontaneous hepatic rupture in a patient with peliosis hepatis: A report of one case. Int J Surg Case Rep. 2013;4(5):508-10. doi: 10.1016/j.ijscr.2013.01.030[↩][↩]
- Caremani M, Tacconi D, Lapini L. Acute nontraumatic liver lesions. J Ultrasound. 2013 Nov 26;16(4):179-86. doi: 10.1007/s40477-013-0049-2[↩][↩][↩]
- Picardi N, Pasta V, Monti M. Possibilità di compenso emodinamico del sistema del Retzius e delle vene paravertebrali nella sindrome di Budd-Chiari [Possibility of hemodynamic compensation of the Retzius system and of the paravertebral veins in Budd-Chiari syndrome]. Ann Ital Chir. 1975-1976;49(1-6):163-77. Italian.[↩]
- Wang SY, Ruggles S, Vade A, Newman BM, Borge MA. Hepatic rupture caused by peliosis hepatis. J Pediatr Surg. 2001 Sep;36(9):1456-9. doi: 10.1053/jpsu.2001.26397[↩][↩][↩]
- Buelow B, Otjen J, Sabath AP, Harruff RC. Peliosis hepatis presenting as liver rupture in a vulnerable adult: a case report. Am J Forensic Med Pathol. 2012 Dec;33(4):307-10. doi: 10.1097/PAF.0b013e31823a8b38[↩]
- Yanoff M, Rawson AJ. Peliosis hepatis. An anatomic study with demonstration of two varieties. Arch Pathol. 1964;77:159–165.[↩]
- Ferrozzi F, Tognini G, Zuccoli G, Cademartiri F, Pavone P. Peliosis hepatis with pseudotumoral and hemorrhagic evolution: CT and MR findings. Abdom Imaging. 2001 Mar-Apr;26(2):197-9. doi: 10.1007/s002610000131[↩][↩][↩][↩][↩][↩]
- Cohen GS, Ball DS, Boyd-Kranis R, Gembala RB, Wurzel J. Peliosis hepatis mimicking hepatic abscess: fatal outcome following percutaneous drainage. J Vasc Interv Radiol. 1994 Jul-Aug;5(4):643-5. doi: 10.1016/s1051-0443(94)71572-4[↩][↩]
- Yang DM, Jung DH, Park CH, Kim JE, Choi SJ. Imaging findings of hepatic sinusoidal dilatation. AJR Am J Roentgenol. 2004 Oct;183(4):1075-7. doi: 10.2214/ajr.183.4.1831075[↩]
- Verswijvel G, Janssens F, Colla P, Mampaey S, Verhelst H, Van Eycken P, Erven W. Peliosis hepatis presenting as a multifocal hepatic pseudotumor: MR findings in two cases. Eur Radiol. 2003 Dec;13 Suppl 4:L40-4. doi: 10.1007/s00330-003-1852-5[↩]
- Hyodo M, Mogensen AM, Larsen PN, Wettergren A, Rasmussen A, Kirkegaard P, Yasuda Y, Nagai H. Idiopathic extensive peliosis hepatis treated with liver transplantation. J Hepatobiliary Pancreat Surg. 2004;11(5):371-4. doi: 10.1007/s00534-004-0908-5[↩][↩]
- Hiorns MP, Rossi UG, Roebuck DJ. Peliosis hepatis causing inferior vena cava compression in a 3-year-old child. Pediatr Radiol. 2005 Feb;35(2):209-11. doi: 10.1007/s00247-004-1311-8[↩]
- Suzuki S, Suzuki H, Mochida Y, Hirai H, Yoshida T, Ide M, Tani M, Shimura T, Morinaga N, Ishizaki M, Kuwano H. Liver hemorrhage due to idiopathic peliosis hepatis successfully treated with hepatic artery embolization. Int Surg. 2011 Oct-Dec;96(4):310-5. doi: 10.9738/cc43.1[↩]
- Omori H, Asahi H, Irinoda T, Takahashi M, Kato K, Saito K. Peliosis hepatis during postpartum period: successful embolization of hepatic artery. J Gastroenterol. 2004;39(2):168-71. doi: 10.1007/s00535-003-1268-7[↩]




{kind=link}