
Contents
- What is anemia
- Red Blood Cells
- Types of anemia
- Complications of anemia
- Anemia causes
- Prevention of anemia
- Anemia signs and symptoms
- Anemia diagnosis
- Anemia treatment
- Anemia diet
- Iron
- How much iron do you need ?
- Folate
- Why do women need folic acid ?
- Do Women need to take Folic Acid every day even if you’re not planning to get pregnant ?
- What can happen if Women do Not get enough Folic Acid during Pregnancy ?
- How much Folic Acid do Women need ?
- How can you be sure you get enough folic acid ?
- Are some women at risk for not getting enough folic acid ?
- How a Woman can get enough Folic Acid
- How much folate do you need ?
- What foods provide folate ?
- Vitamin B12
- What foods provide vitamin B12 ?
What is anemia
Anemia is a lack of red blood cells (& hemoglobin). Red blood cells are important because they carry oxygen from the lungs around the body. Hemoglobin is contained within red blood cells and is necessary to transport and deliver oxygen from the lungs to the rest of the body. Without a sufficient supply of oxygen, many tissues and organs throughout the body can be adversely affected. People with anemia may experience fatigue and weakness and may lack energy.
Anemia is a fairly common condition, affecting both men and women of all ages, races, and ethnic groups. However, certain people have increased risk of developing anemia. These include people with diets poor in iron and vitamins, chronic diseases such as kidney disease, diabetes, cancer, inflammatory bowel disease, a family history of inherited anemia, chronic infections such as tuberculosis or HIV, and those who have had significant blood loss from injury or surgery. Anemia can be mild, moderate, or severe depending on how much the red blood cell (RBC) count and/or hemoglobin levels are decreased.
There are many forms of anemia, each with its own cause. Anemia can be temporary or long term, and it can range from mild to severe. See your doctor if you suspect you have anemia because it can be a warning sign of serious illness.
It’s important to find and treat the cause of the anemia as well as the anemia itself.
In general, the main causes of anemia include:
- Impaired or decreased production of red blood cells by the bone marrow due to nutritional deficiency (e.g., iron deficiency, B vitamin deficiencies), bone marrow failure (e.g., aplastic anemia, myelodysplastic syndrome), or diseases that involve the bone marrow (e.g., infection, lymphoma, solid tumor)
- Loss of red blood cells due to bleeding or to increased destruction of red blood cells as in hemolytic anemia
Anemia may be acute or chronic. Chronic anemia may develop slowly over a period of time with long-term illnesses such as diabetes, chronic kidney disease, or cancer. In these situations, the anemia-related symptoms may not be apparent because the underlying disease masks its symptoms and/or the body adapts to anemia when it develops over a period of time. The presence of anemia in chronic conditions may often go undetected for a period of time and sometimes may only be discovered during tests or examinations for other conditions.
Anemia may also occur in acute episodes such as with substantial blood loss (extensive injury or invasive surgery) or with certain anemias in which a significant number of red blood cells are destroyed known as hemolytic anemia. Signs and symptoms may become apparent very quickly, and the cause can be determined from a combination of physical examination, medical history, and testing.
Treatments for anemia range from taking supplements to undergoing medical procedures. You may be able to prevent some types of anemia by eating a healthy, varied diet.
Anemia in pregnancy
During pregnancy, some women become anemic, which means they have too few red blood cells in their body. This is usually managed without any harm to mother or baby.
Why do pregnant women become anemic?
The main reason is that the woman’s body changes during pregnancy to look after the growing child.
One change is that women make more blood when they become pregnant. The average woman will have about five litres of blood when not pregnant, but will have seven to eight litres of blood in her body as she gets near term.
Making the extra blood cells requires plenty of iron, vitamin B12 and folate to make all the extra haemoglobin needed. Unfortunately, iron is hard to absorb, which makes haemoglobin hard to make. So many women become anaemic during pregnancy unless they take iron supplements.
What are the tests for anemia during pregnancy?
You would usually have a blood count around the time you first see a doctor or midwife about your pregnancy. This blood count shows whether or not there is enough haemoglobin and enough blood cells. Any abnormality in these tests will guide your doctor towards other tests such as:
- iron levels
- vitamin B12 and folate levels
- genetic tests for inherited disorders such as thalassemia.
What are the risks if a pregnant woman is anemic?
If a woman becomes anemic while pregnant, it will make her even more tired than expected.
If the anemia is severe, there could be a reduced amount of amniotic fluid around baby. There is also an increased chance of miscarriage, the baby being delivered too early or having a low birth weight. Babies born from anemic mothers may also be anemic.
If a woman is anaemic throughout pregnancy and loses a lot of blood during the birth, she may need to have a blood transfusion around the time of the birth.
How can anemia in pregnancy be avoided?
There are three good ways to avoid becoming anaemic while pregnant. They are:
- start your pregnancy in good health
- eat well while pregnant
- take supplements.
Starting pregnancy in good health
If you are thinking about becoming pregnant, you should see your doctor and get a check-up. At this time, you will get advice about anaemia and other conditions, and particularly about taking folate supplements.
Women are advised to take a folic acid supplement for at least a month before becoming pregnant and continuing this for at least the first three months. This will help prevent anaemia, and will also decrease the risk of neural tube defects such as spina bifida. The standard dose is 0.5mg of folic acid per day, but the dose may be higher for women who have diabetes, epilepsy, are overweight or have had a child with a neural tube defect. This should be discussed with a doctor.
Eating well while pregnant
Eating a healthy diet protects against anaemia. Iron is found in meats, iron fortified breads and cereals, eggs, spinach and dried fruit. Vitamin B12 is found in meat, fish, shellfish, eggs and dairy products. High levels of folate are found in green leafy vegetables, beans, muesli, broccoli, beef, Brussels sprouts and asparagus Eating a diet rich in these foods will help prevent anaemia.
Women who are vegetarian can replace animal foods with lentils, beans, tofu, eggs and soy milk. Advice from a doctor or dietitian is suggested, and vitamin B12 supplements may be recommended.
Eating plenty of citrus fruit, and avoiding tea and coffee with or soon after meals, may help you absorb the iron in your food, and may help prevent anaemia.
Supplements
All women will be advised to take folate supplements, as well as eating foods rich in folate. Many women will be advised to take iron supplements. Vegetarians may be advised to take vitamin B12 supplements. If you are advised to take supplements, talk to your doctor about the best ways to take them, and how to avoid any possible side effects.
Red Blood Cells
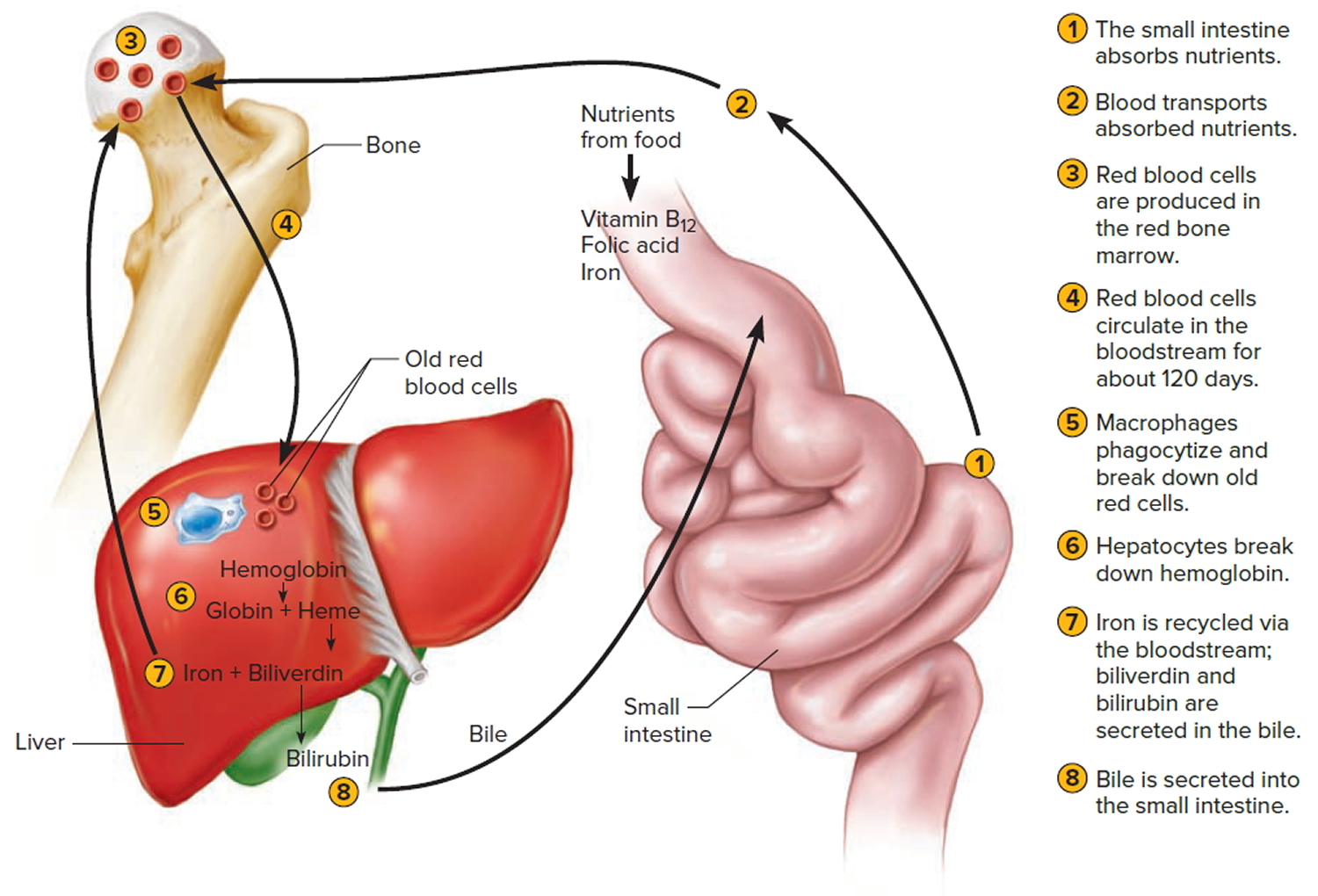
Red blood cell (also called erythrocyte) is biconcave disc without a nucleus. This biconcave shape is an adaptation for transporting the gases oxygen and carbon dioxide. It increases the surface area through which oxygen and carbon dioxide can diffuse into and out of the cell (Figure 4). The characteristic shape of a red blood cell also places the cell membrane closer to oxygen-carrying hemoglobin (Figure 6) molecules in the cell reducing the distance for diffusion.
The average life span of red blood cells is about four months (120 days) after which it breaks down. Red blood cells are elastic and flexible, and they readily bend as they pass through small blood vessels. As the cells near the end of their four-month life span, however, they become more fragile. The cells may sustain damage simply passing through capillaries, particularly those in active muscles that must withstand strong forces. Macrophages phagocytize and destroy damaged red blood cells, primarily in the liver and spleen. Macrophages are large, phagocytic, wandering cells. During phagocytosis, the iron from the hemoglobin is retained in the liver and spleen cells and is again used in the formation of red blood cells in the body. About 2-10 million red blood cells are formed and destroyed each second in a normal person.
Each red blood cell is about one-third hemoglobin by volume. This protein imparts the color of blood. When hemoglobin binds oxygen, the resulting oxyhemoglobin is bright red, and when oxygen is released, the resulting deoxyhemoglobin is darker.
Prolonged oxygen deficiency (hypoxia) causes cyanosis, in which the skin and mucous membranes appear bluish due to an abnormally high blood concentration of deoxyhemoglobin in the superficial blood vessels. Exposure to low temperature may also result in cyanosis by constricting superficial blood vessels. This response to environmental change slows skin blood flow. As a result, more oxygen than usual is removed from the blood flowing through the vessels, increasing the concentration of deoxyhemoglobin.
Note: Blood is a complex mixture of formed elements in a liquid extracellular matrix, called blood plasma. Note that water and proteins account for 99% of the blood plasma.
Figure 1. Blood composition


Note: Blood consists of a liquid portion called plasma and a solid portion (the formed elements) that includes red blood cells, white blood cells, and platelets. When blood components are separated by centrifugation, the white blood cells and platelets form a thin layer, called the “buffy coat,” between the plasma and the red blood cells, which accounts for about 1% of the total blood volume. Blood cells and platelets can be seen under a light microscope when a blood sample is smeared onto a glass slide.
Red Blood Cell Counts
The number of red blood cells in a microliter (μL or mcL or 1 mm3) of blood is called the red blood cell count (RBCC or RCC). This number varies from time to time even in healthy individuals. However, the typical range for adult males is 4,700,000 to 6,100,000 cells per microliter, and that for adult females is 4,200,000 to 5,400,000 cells per microliter.
The absolute numbers for red blood cell, white blood cell, and platelet counts can vary depending on how they are measured and the instruments used to measure them. For this reason, different sources may present different, but very similar, ranges of normal values.
An increase in the number of circulating red blood cells increases the blood’s oxygen-carrying capacity, much as a decrease in the number of circulating red blood cells decreases the blood’s oxygen-carrying capacity. Changes in this number may affect health. For this reason, red blood cell counts are routinely consulted to help diagnose and evaluate the courses of certain diseases.
Blood Cell Formation
The process of blood cell formation, called hematopoiesis, begins in the yolk sac, which lies outside the human embryo. Later in the fetal development, red blood cells are manufactured (erythropoiesis) in the liver and spleen, and still later they form in bone marrow. After birth, these cells are produced in the red bone marrow.
Bone marrow is a soft, netlike mass of connective tissue within the medullary cavities of long bones, in the irregular spaces of spongy bone, and in the larger central canals of compact bone tissue. It is of two kinds: red and yellow. Red bone marrow functions in the formation of red blood cells (erythrocytes), white blood cells (leukocytes), and blood platelets. The color comes from the oxygen-carrying pigment hemoglobin in the red blood cells.
In an infant, red marrow occupies the cavities of most bones. As a person ages, yellow bone marrow, which stores fat, replaces much of the red marrow. Yellow marrow is not active in blood cell production. In an adult, red marrow is primarily found in the spongy bone of the skull, ribs, breastbone (sternum), collarbones (clavicles), backbones (vertebrae), and hip bones. If the supply of blood cells is deficient, some yellow marrow may become red marrow, which then reverts to yellow marrow when the deficiency is corrected.
Figure 2 illustrates the stages in the formation of red blood cells from hematopoietic stem cells (blood-forming cells), which are also called hemocytoblasts.
Red blood cells have nuclei during their early stages of development but lose their nuclei as the cells mature. Losing the nuclei provides more space for hemoglobin. Because mature red blood cells do not have nuclei, they cannot divide. They use none of the oxygen they carry because they do not have mitochondria. Mature red blood cells produce ATP through glycolysis only.
The average life span of a red blood cell is 120 days. Many of these cells are removed from the circulation each day, and yet the number of cells in the circulating blood remains relatively stable. This observation suggests a homeostatic control of the rate of red blood cell production.
The hormone erythropoietin controls the rate of red blood cell formation through negative feedback. The kidneys, and to a lesser extent the liver, release erythropoietin in response to prolonged oxygen deficiency (Figure 5). At high altitudes, for example, where the amount of oxygen in the air is reduced, the blood oxygen level initially decreases. This drop in the blood oxygen level triggers the release of erythropoietin, which travels via the blood to the red bone marrow and stimulates red blood cell production.
After a few days of exposure to high altitudes, many newly formed red blood cells appear in the circulating blood. The increased rate of production continues until the number of erythrocytes in the circulation is sufficient to supply tissues with oxygen. When the availability of oxygen returns to normal, erythropoietin release decreases, and the rate of red blood cell production returns to normal as well. An excessive increase in red blood cells is called polycythemia. This condition increases blood viscosity, slowing blood flow and impairing circulation.
Figure 2. Bone marrow anatomy

Anatomy of the bone. The bone is made up of compact bone, spongy bone, and bone marrow. Compact bone makes up the outer layer of the bone. Spongy bone is found mostly at the ends of bones and contains red marrow. Bone marrow is found in the center of most bones and has many blood vessels. There are two types of bone marrow: red and yellow. Red marrow contains blood stem cells that can become red blood cells, white blood cells, or platelets. Yellow marrow is made mostly of fat.
Dietary Factors Affecting Red Blood Cell Production
Availability of B-complex vitamins—vitamin B12 and folic acid—significantly influences red blood cell production. Because these vitamins are required for DNA synthesis, they are necessary for the growth and division of cells. Cell division is frequent in blood-forming (hematopoietic) tissue, so this tissue is especially vulnerable to a deficiency of either of these vitamins.
Hemoglobin synthesis and normal red blood cell production also require iron. The small intestine absorbs iron slowly from food. The body reuses much of the iron released by the decomposition of hemoglobin from damaged red blood cells. Nonetheless, insufficient dietary iron can reduce hemoglobin synthesis.
A deficiency of red blood cells or a reduction in the amount of hemoglobin they contain results in a condition called anemia. This reduces the oxygen-carrying capacity of the blood, and the affected person may appear pale and lack energy. A pregnant woman may have a normal number of red blood cells, but she develops a relative anemia because her plasma volume increases due to fluid retention. This shows up as a decreased hematocrit.
In contrast to anemia, the inherited disorder called hemochromatosis results in the absorption of iron in the small intestine at ten times the normal rate. Iron builds up in organs, to toxic levels. Treatment is periodic blood removal, as often as every week.
Figure 3. Blood cell development. A blood stem cell goes through several steps to become a red blood cell, platelet, or white blood cell

Figure 4. Blood cells
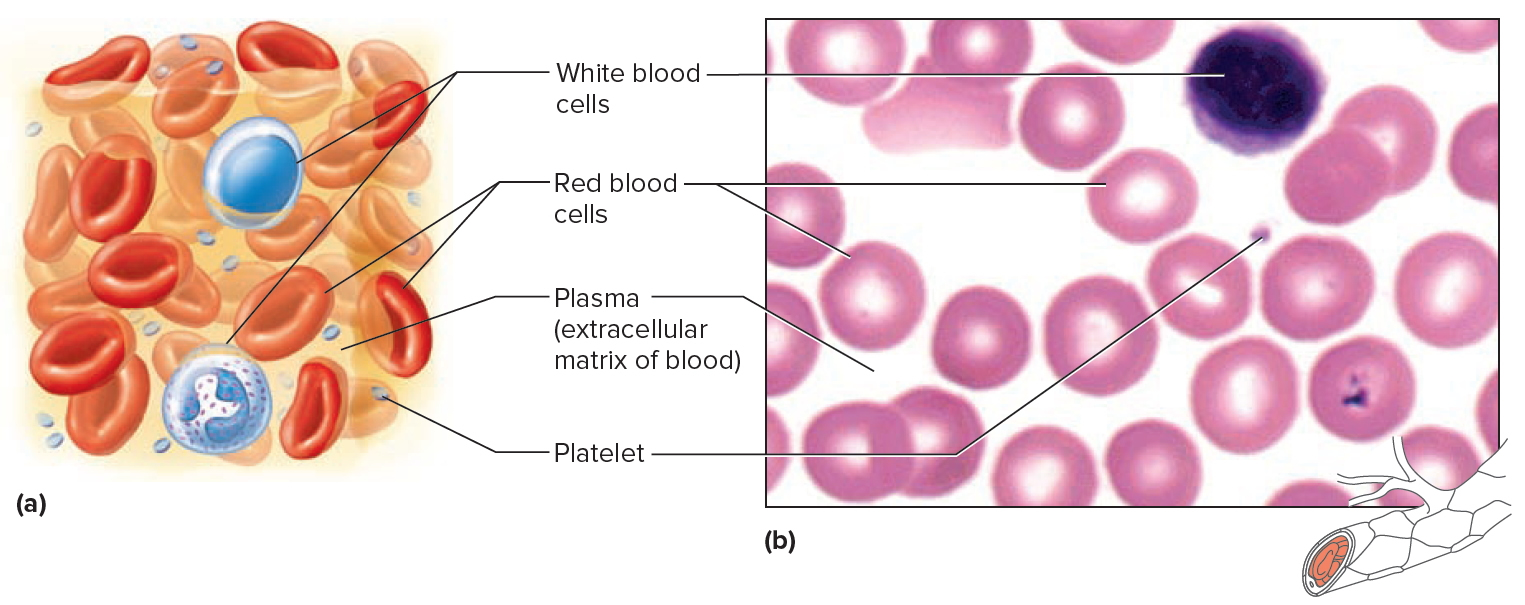
Note: Blood tissue consists of red blood cells, white blood cells, and platelets suspended in plasma. (a) Idealized representation of
a sample of blood. (b) Micrograph of a sample of blood (1,000x).
Figure 5. Red blood cells
Figure 6. Red blood cell formation
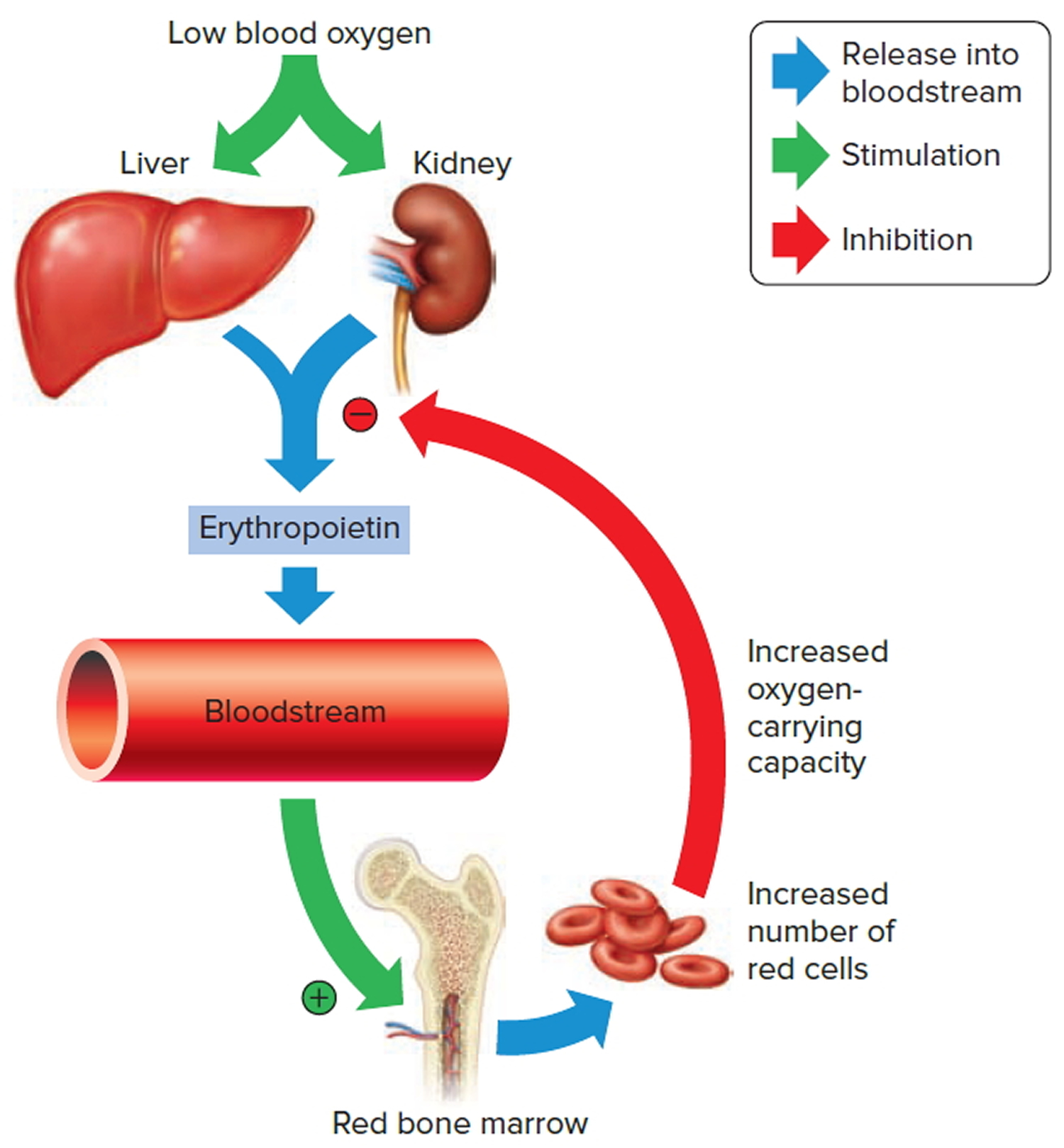
Note: Low blood oxygen causes the kidneys and to a lesser degree, the liver to release erythropoietin. Erythropoietin stimulates target cells in the red bone marrow to increase the production of red blood cells, which carry oxygen to tissues.
Figure 7. Red blood cell hemoglobin
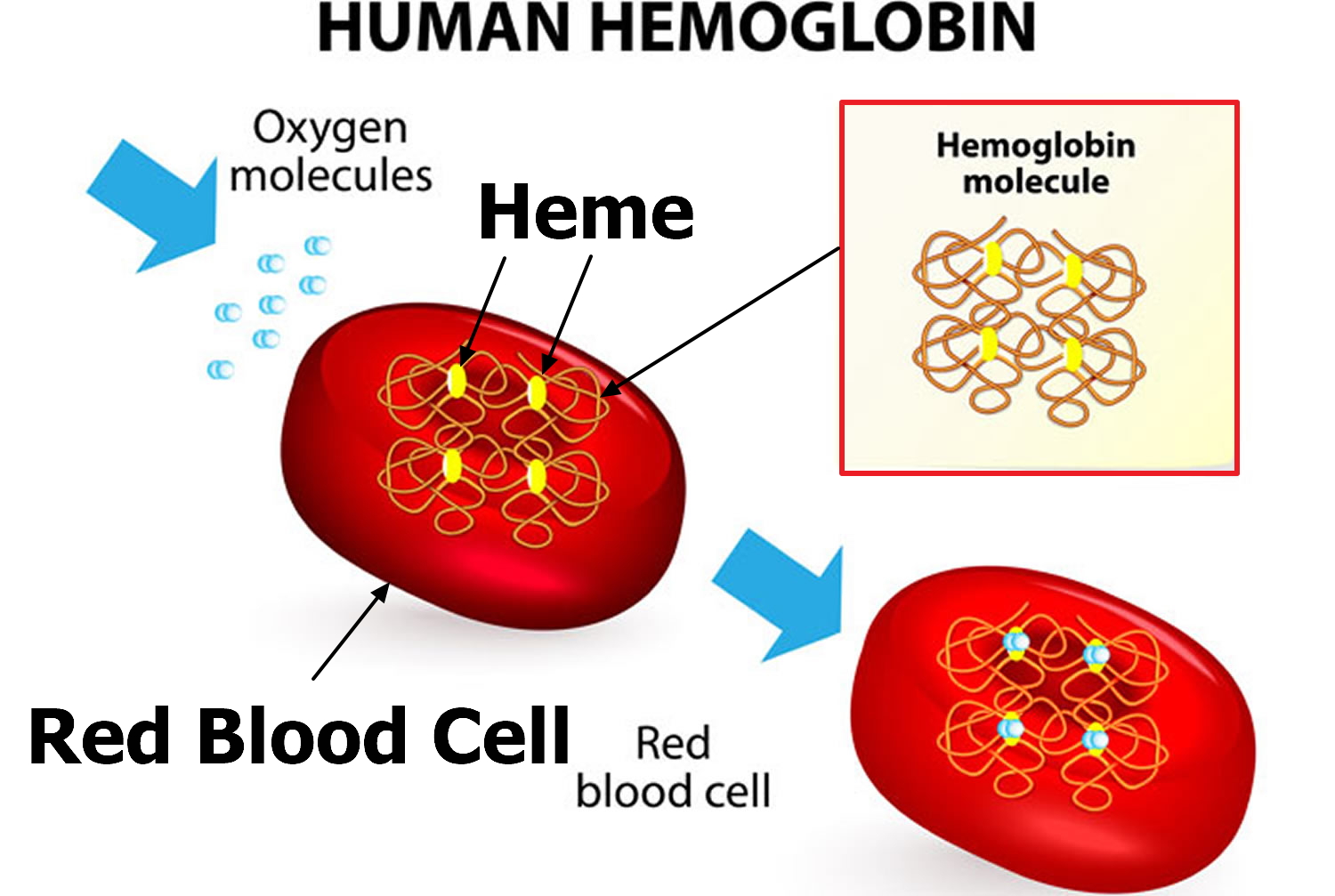
Figure 8. Lifecycle of a red blood cell
 Types of anemia
Types of anemia
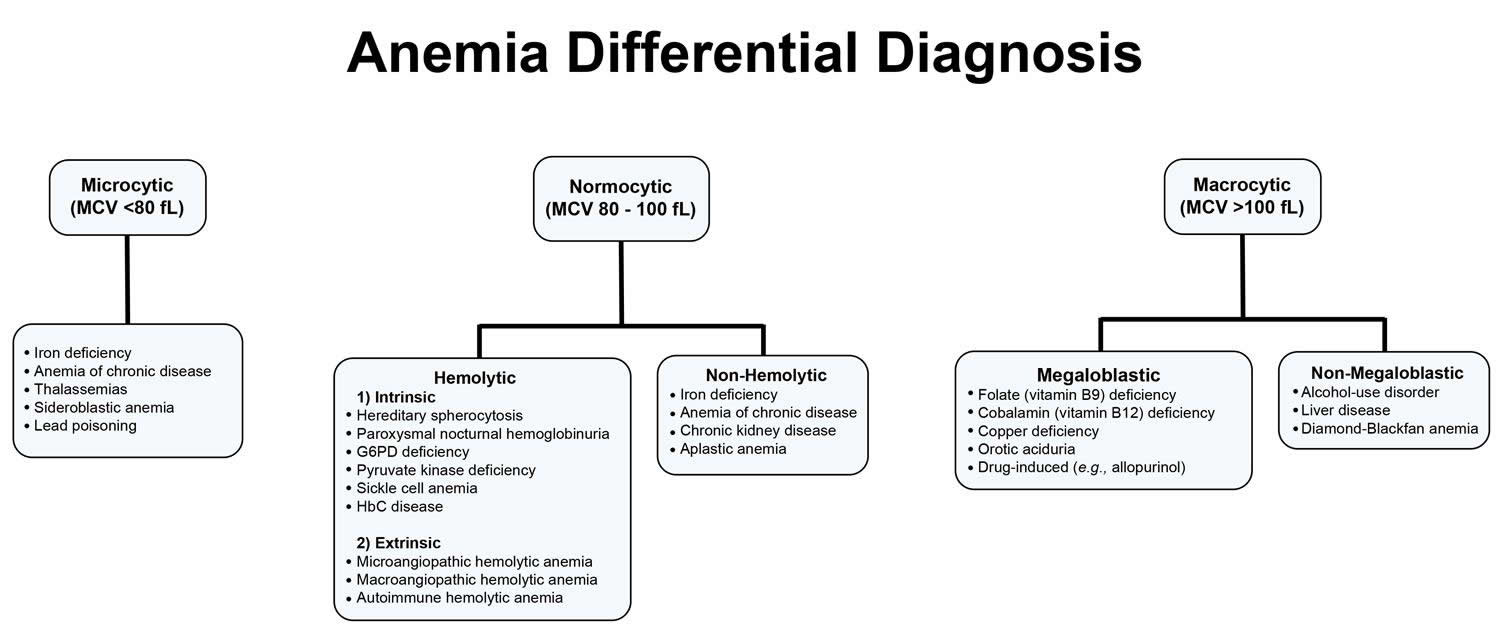
Anemias can also be described based on the red blood cell size and concentration of hemoglobin in them. If cell size is much smaller than normal, it is known as microcytic anemia. If it is much bigger than normal, then it is macrocytic anemia. Likewise, if the concentration of hemoglobin is much lower than normal, it is hypochromic anemia; if the concentration is much higher than normal, the red blood cells are called hyperchromic.
Within the two broad categories of general causes of anemia, there are several types with different specific causes. Some of the most common types are summarized below.
Figure 9. Anemia differential diagnosis
Different types of anemia and their causes include:
Iron deficiency anemia
This is the most common type of anemia worldwide. Iron deficiency anemia is caused by a shortage of iron in your body. Your bone marrow needs iron to make hemoglobin. Without adequate iron, your body can’t produce enough hemoglobin for red blood cells. Low levels of hemoglobin in turn leads to production of smaller and hypochromic red blood cells.
Examples of causes of iron deficiency anemia: Blood loss; diet low in iron; poor absorption of iron
Without iron supplementation, this type of anemia occurs in many pregnant women. It is also caused by blood loss, such as from heavy menstrual bleeding, an ulcer, cancer and regular use of some over-the-counter pain relievers, especially aspirin.
Vitamin deficiency anemia
Also called Pernicious Anemia and B Vitamin Deficiency anemia.
In addition to iron, your body needs folate and vitamin B-12 to produce enough healthy red blood cells. A diet lacking in these and other key nutrients can cause decreased red blood cell production.
Examples of causes of vitamin deficiency anemia: Lack of intrinsic factor (needed for B12 absorption); diet low in B vitamins; decreased absorption of B vitamins
Additionally, some people may consume enough B-12, but their bodies aren’t able to process the vitamin. This can lead to vitamin deficiency anemia, also known as pernicious anemia.
Anemia of Chronic Disease
Certain diseases — such as cancer, HIV/AIDS, diabetes, tuberculosis, rheumatoid arthritis, kidney disease, Crohn’s disease, cancer and other chronic inflammatory diseases — can interfere with the production of red blood cells.
Aplastic anemia
This rare, life-threatening anemia occurs when your body doesn’t produce enough red blood cells. Causes of aplastic anemia include infections, certain medicines, autoimmune diseases, viral infections and exposure to toxic chemicals.
Anemias associated with bone marrow disease
A variety of diseases, such as leukemia and myelofibrosis, can cause anemia by affecting blood production in your bone marrow. The effects of these types of cancer and cancer-like disorders vary from mild to life-threatening.
Hemolytic anemias
This group of anemias develops when red blood cells are destroyed faster than bone marrow can replace them. Certain blood diseases increase red blood cell destruction. You can inherit a hemolytic anemia, or you can develop it later in life.
Sickle cell anemia
This inherited and sometimes serious condition is an inherited hemolytic anemia. It’s caused by a defective form of hemoglobin that forces red blood cells to assume an abnormal crescent (sickle) shape. These irregular blood cells die prematurely, resulting in a chronic shortage of red blood cells.
Other anemias
There are many other conditions that can, for various reasons, result in some level of anemia, such as:
- Bleeding—significant bleeding resulting from, for example, trauma or surgery (acute) or from gastrointestinal bleeding (ulcers) occurring over time (chronic)
- Leukemia (acute or chronic)
- Lymphoma
- Myelodysplastic syndrome
- Multiple myeloma
- Myeloproliferative neoplasms (e.g., myelofibrosis)
- Infections (e.g., HIV)
- Thalassemia
- Malarial anemia
Complications of anemia
Left untreated, anemia can cause many health problems, such as:
- Severe fatigue. When anemia is severe enough, you may be so tired that you can’t complete everyday tasks.
- Pregnancy complications. Pregnant women with folate deficiency anemia may be more likely to experience complications, such as premature birth.
- Heart problems. Anemia can lead to a rapid or irregular heartbeat (arrhythmia). When you’re anemic your heart must pump more blood to compensate for the lack of oxygen in the blood. This can lead to an enlarged heart or heart failure.
- Death. Some inherited anemias, such as sickle cell anemia, can be serious and lead to life-threatening complications. Losing a lot of blood quickly results in acute, severe anemia and can be fatal.
Anemia causes
Anemia occurs when your blood doesn’t have enough red blood cells. This can happen if:
- Your body doesn’t make enough healthy red blood cells in your bone marrow – this can be due to an inherited disease, a lack of iron or vitamins in the diet, or bone marrow disease
- Bleeding causes you to lose red blood cells more quickly than they can be replaced, whether that be heavy periods, a fast bleed or one so slow you didn’t even notice it
- You have a disease that destroys red blood cells.
Risk factors for anemia
These factors place you at increased risk of anemia:
- A diet lacking in certain vitamins. Having a diet that is consistently low in iron, vitamin B-12 and folate increases your risk of anemia.
- Intestinal disorders. Having an intestinal disorder that affects the absorption of nutrients in your small intestine — such as Crohn’s disease and celiac disease — puts you at risk of anemia.
- Menstruation. In general, women who haven’t experienced menopause have a greater risk of iron deficiency anemia than do men and postmenopausal women. That’s because menstruation causes the loss of red blood cells.
- Pregnancy. If you’re pregnant and aren’t taking a multivitamin with folic acid, you’re at an increased risk of anemia.
- Chronic conditions. If you have cancer, kidney failure or another chronic condition, you may be at risk of anemia of chronic disease. These conditions can lead to a shortage of red blood cells. Slow, chronic blood loss from an ulcer or other source within your body can deplete your body’s store of iron, leading to iron deficiency anemia.
- Family history. If your family has a history of an inherited anemia, such as sickle cell anemia, you also may be at increased risk of the condition.
- Other factors. A history of certain infections, blood diseases and autoimmune disorders, alcoholism, exposure to toxic chemicals, and the use of some medications can affect red blood cell production and lead to anemia.
- Age. People over age 65 are at increased risk of anemia.
Prevention of anemia
You can reduce your chances of getting anemia by:
- having a healthy diet
- seeing your doctor if you are feeling unusually tired.
Eat a vitamin-rich diet
Many types of anemia can’t be prevented. But iron deficiency anemia and vitamin deficiency anemias can be avoided by having a diet that includes a variety of vitamins and nutrients, including:
- Iron. Iron-rich foods include beef and other meats, beans, lentils, iron-fortified cereals, dark green leafy vegetables, and dried fruit.
- Folate. This nutrient, and its synthetic form folic acid, can be found in fruits and fruit juices, dark green leafy vegetables, green peas, kidney beans, peanuts, and enriched grain products, such as bread, cereal, pasta and rice.
- Vitamin B-12. Foods rich in vitamin B-12 include meat, dairy products, and fortified cereal and soy products.
- Vitamin C. Foods rich in vitamin C include citrus fruits and juices, peppers, broccoli, tomatoes, melons and strawberries. These items help increase iron absorption.
Consider a multivitamin
If you’re concerned about getting enough vitamins from the food you eat, ask your doctor whether a multivitamin may be right for you.
Consider genetic counseling
If you have a family history of an inherited anemia, such as sickle cell anemia or thalassemia, talk to your doctor and possibly a genetic counselor about your risk and what risks you may pass on to your children.
Prevent malaria
Anemia can be a complication of malaria. If you plan on traveling to a place where malaria is common, talk with your doctor beforehand about taking preventive drugs. In areas where malaria is common, prevention involves reducing exposure to mosquitoes, for example, by using bed nets treated with insecticide.
Anemia signs and symptoms
If you have anemia, you will feel tired and short of breath, even when doing things you could usually do easily.
You may also have a fast or irregular heartbeat, look pale, have cold feet or hands, feel dizzy or have problems thinking.
It’s important to see your doctor if you have any of these symptoms.
Signs and symptoms of anemia
- Fatigue
- Weakness
- Pale or yellowish skin
- Irregular heartbeats
- Shortness of breath
- Dizziness or lightheadedness
- Chest pain
- Cold hands and feet
- Headache
At first anemia can be so mild that it goes unnoticed. But symptoms worsen as anemia worsens.
Anemia diagnosis
If you have anemia, your doctor will talk to you and examine you to work out how severe the anaemia is, and what the cause could be. You might be asked to have more tests, depending on what your doctor has learned from talking to you and examining you.
To diagnose anemia, your doctor may ask you about your medical and family history, perform a physical exam, and run the following tests
Anemia tests
Several routine laboratory tests may be used to help diagnose anemia as well as help to determine the underlying cause. These are listed below. Depending on the results of these, the medical history of the person, and signs and symptoms, other tests may be done as follow up to help diagnose the cause of anemia and to help guide treatment. (Click on the links for the different types of anemia at the top of this page to read about these specific tests.)
Complete Blood Count (CBC)
Anemia may first be detected when a routine test that counts the number and relative proportion of each of the different types of cells in the blood stream, called a complete blood count (CBC), is done during a health exam or as part of testing for other conditions. A CBC is often ordered as part of a yearly physical exam and helps to evaluate overall health and to screen for a wide variety of disorders.
A complete blood count (CBC) is used to count the number of blood cells in a sample of your blood. For anemia your doctor will be interested in the levels of the red blood cells contained in the blood (hematocrit) and the hemoglobin in your blood.
- Normal adult hematocrit values vary from one medical practice to another but are generally between 40 and 52 percent for men and 35 and 47 percent for women. Normal adult hemoglobin values are generally 14 to 18 grams per deciliter for men and 12 to 16 grams per deciliter for women.
- A test to determine the size and shape of your red blood cells. Some of your red blood cells may also be examined for unusual size, shape and color.
With anemia, some of the components of the CBC that may show abnormal results include:
- RBC count—typically low
- Hemoglobin—low
- Hematocrit—low
- RBC indices—these include mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC). They give a healthcare practitioner information about the size of the red blood cells and the amount and concentration of hemoglobin in RBCs present in someone’s blood at that moment. For example, the size and hemoglobin concentration of RBCs can help with diagnosing anemia because those characteristics can vary for different kinds of anemia.
Blood Smear and Differential
If results of the CBC indicate anemia, it may be followed up with an examination of a blood smear or a differential, which counts white blood cells. The smear review can provide additional information, such as the shape of red blood cells and the presence of abnormal cells, which can help diagnose and classify anemia.
Reticulocyte Count
This test provides information on the number of relatively immature red blood cells in a person’s blood sample. When someone has anemia (low RBC count, hemoglobin, and hematocrit), the results of this test can help determine the cause and/or help classify the type of anemia. For example, for a person with anemia, an inappropriately low reticulocyte count often indicates decrease in red blood cell production in the bone marrow.
Results from these tests may give clues as to the cause. Several other tests may be run to help determine the cause of the anemia and to guide treatment. See the individual discussions of the different types of anemia for more on these.
Additional diagnostic tests
If you receive a diagnosis of anemia, your doctor may order additional tests to determine the underlying cause. For example, iron deficiency anemia can result from chronic bleeding of ulcers, benign polyps in the colon, colon cancer, tumors or kidney problems.
Occasionally, it may be necessary to study a sample of your bone marrow to diagnose anemia.
Anemia treatment
The treatment depends on the cause. But there are usually two parts:
- treating the anemia itself
- treating the cause of the anemia.
How to treat anemia
- Iron deficiency anemia. Treatment for this form of anemia usually involves taking iron supplements and making changes to your diet.
If the underlying cause of iron deficiency is loss of blood — other than from menstruation — the source of the bleeding must be located and stopped. This may involve surgery.
- Vitamin deficiency anemias. Treatment for folic acid and B-12 deficiency involves dietary supplements and increasing these nutrients in your diet.
If your digestive system has trouble absorbing vitamin B-12 from the food you eat, you may need vitamin B-12 shots. At first, you may receive the shots every other day. Eventually, you’ll need shots just once a month, which may continue for life, depending on your situation.
- Anemia of chronic disease. There’s no specific treatment for this type of anemia. Doctors focus on treating the underlying disease. If symptoms become severe, a blood transfusion or injections of synthetic erythropoietin, a hormone normally produced by your kidneys, may help stimulate red blood cell production and ease fatigue.
- Aplastic anemia. Treatment for this anemia may include blood transfusions to boost levels of red blood cells. You may need a bone marrow transplant if your bone marrow is diseased and can’t make healthy blood cells.
- Anemias associated with bone marrow disease. Treatment of these various diseases can include medication, chemotherapy or bone marrow transplantation.
- Hemolytic anemias. Managing hemolytic anemias includes avoiding suspect medications, treating related infections and taking drugs that suppress your immune system, which may be attacking your red blood cells.
Depending on the severity of your anemia, a blood transfusion or plasmapheresis may be necessary. Plasmapheresis is a type of blood-filtering procedure. In certain cases, removal of the spleen can be helpful.
- Sickle cell anemia. Treatment for this anemia may include the administration of oxygen, pain-relieving drugs, and oral and intravenous fluids to reduce pain and prevent complications. Doctors also may recommend blood transfusions, folic acid supplements and antibiotics.
A bone marrow transplant may be an effective treatment in some circumstances. A cancer drug called hydroxyurea (Droxia, Hydrea) also is used to treat sickle cell anemia.
- Thalassemia. This anemia may be treated with blood transfusions, folic acid supplements, medication, removal of the spleen (splenectomy), or a blood and bone marrow stem cell transplant.
Anemia diet
Iron
Iron is a mineral that our bodies need for many functions. In the human body, iron is present in all cells and has several vital functions — as a carrier of oxygen to the tissues from the lungs in the form of hemoglobin (Hb), as a facilitator of oxygen use and storage in the muscles as myoglobin, as a transport medium for electrons within the cells in the form of cytochromes, and as an integral part of enzyme reactions in various tissues. Too little iron can interfere with these vital functions and lead to morbidity and mortality 1, 2.
Dietary iron has two main forms: heme and nonheme 3. Plants and iron-fortified foods contain nonheme iron only, whereas meat, seafood, and poultry contain both heme and nonheme iron 4. Heme iron, which is formed when iron combines with protoporphyrin IX, contributes about 10% to 15% of total iron intakes in western populations 5.
In adults, the recommended dietary allowance of iron is 8 to 11 mg per day for men and 8 to 18 mg for women in whom higher levels are recommended during pregnancy (27 mg per day) 6. Iron is poorly absorbed and body and tissue iron stores are controlled largely by modifying rates of absorption. Adequate amounts of iron are found in most Western diets, with highest levels found in red meats and moderate levels in fish, poultry, green vegetables, cereals and grains (some of which are fortified with iron).
How much iron do you need ?
The amount of iron you need each day depends on your age, your sex, and whether you consume a mostly plant-based diet. Average daily recommended amounts are listed below in milligrams (mg). Vegetarians who do not eat meat, poultry, or seafood need almost twice as much iron as listed in the table because the body doesn’t absorb nonheme iron in plant foods as well as heme iron in animal foods.
Table 1. Iron recommended intake
| Life Stage | Recommended Amount |
|---|---|
| Birth to 6 months | 0.27 mg |
| Infants 7–12 months | 11 mg |
| Children 1–3 years | 7 mg |
| Children 4–8 years | 10 mg |
| Children 9–13 years | 8 mg |
| Teens boys 14–18 years | 11 mg |
| Teens girls 14–18 years | 15 mg |
| Adult men 19–50 years | 8 mg |
| Adult women 19–50 years | 18 mg |
| Adults 51 years and older | 8 mg |
| Pregnant teens | 27 mg |
| Pregnant women | 27 mg |
| Breastfeeding teens | 10 mg |
| Breastfeeding women | 9 mg |
What foods provide iron ?
Iron is found naturally in many foods and is added to some fortified food products. You can get recommended amounts of iron by eating a variety of foods, including the following:
- Lean meat, seafood, and poultry.
- Iron-fortified breakfast cereals and breads.
- White beans, lentils, spinach, kidney beans, and peas.
- Nuts and some dried fruits, such as raisins.
Iron in food comes in two forms: heme iron and nonheme iron. Nonheme iron is found in plant foods and iron-fortified food products. Meat, seafood, and poultry have both heme and nonheme iron.
Heme iron has higher bioavailability than nonheme iron, and other dietary components have less effect on the bioavailability of heme than nonheme iron 5. The bioavailability of iron is approximately 14% to 18% from mixed diets that include substantial amounts of meat, seafood, and vitamin C (ascorbic acid, which enhances the bioavailability of nonheme iron) and 5% to 12% from vegetarian diets 4. In addition to ascorbic acid, meat, poultry, and seafood can enhance nonheme iron absorption, whereas phytate (present in grains and beans) and certain polyphenols in some non-animal foods (such as cereals and legumes) have the opposite effect 7. Unlike other inhibitors of iron absorption, calcium might reduce the bioavailability of both nonheme and heme iron. However, the effects of enhancers and inhibitors of iron absorption are attenuated by a typical mixed western diet, so they have little effect on most people’s iron status.
Several food sources of iron are listed in Table 2. Some plant-based foods that are good sources of iron, such as spinach, have low iron bioavailability because they contain iron-absorption inhibitors, such as polyphenols 8.
Your body absorbs iron from plant sources better when you eat it with meat, poultry, seafood, and foods that contain vitamin C, like citrus fruits, strawberries, sweet peppers, tomatoes, and broccoli.
Table 2: Selected Food Sources of Iron
| Food | Milligrams per serving | Percent DV* |
|---|---|---|
| Breakfast cereals, fortified with 100% of the DV for iron, 1 serving | 18 | 100 |
| Oysters, eastern, cooked with moist heat, 3 ounces | 8 | 44 |
| White beans, canned, 1 cup | 8 | 44 |
| Chocolate, dark, 45%–69% cacao solids, 3 ounces | 7 | 39 |
| Beef liver, pan fried, 3 ounces | 5 | 28 |
| Lentils, boiled and drained, ½ cup | 3 | 17 |
| Spinach, boiled and drained, ½ cup | 3 | 17 |
| Tofu, firm, ½ cup | 3 | 17 |
| Kidney beans, canned, ½ cup | 2 | 11 |
| Sardines, Atlantic, canned in oil, drained solids with bone, 3 ounces | 2 | 11 |
| Chickpeas, boiled and drained, ½ cup | 2 | 11 |
| Tomatoes, canned, stewed, ½ cup | 2 | 11 |
| Beef, braised bottom round, trimmed to 1/8” fat, 3 ounces | 2 | 11 |
| Potato, baked, flesh and skin, 1 medium potato | 2 | 11 |
| Cashew nuts, oil roasted, 1 ounce (18 nuts) | 2 | 11 |
| Green peas, boiled, ½ cup | 1 | 6 |
| Chicken, roasted, meat and skin, 3 ounces | 1 | 6 |
| Rice, white, long grain, enriched, parboiled, drained, ½ cup | 1 | 6 |
| Bread, whole wheat, 1 slice | 1 | 6 |
| Bread, white, 1 slice | 1 | 6 |
| Raisins, seedless, ¼ cup | 1 | 6 |
| Spaghetti, whole wheat, cooked, 1 cup | 1 | 6 |
| Tuna, light, canned in water, 3 ounces | 1 | 6 |
| Turkey, roasted, breast meat and skin, 3 ounces | 1 | 6 |
| Nuts, pistachio, dry roasted, 1 ounce (49 nuts) | 1 | 6 |
| Broccoli, boiled and drained, ½ cup | 1 | 6 |
| Egg, hard boiled, 1 large | 1 | 6 |
| Rice, brown, long or medium grain, cooked, 1 cup | 1 | 6 |
| Cheese, cheddar, 1.5 ounces | 0 | 0 |
| Cantaloupe, diced, ½ cup | 0 | 0 |
| Mushrooms, white, sliced and stir-fried, ½ cup | 0 | 0 |
| Cheese, cottage, 2% milk fat, ½ cup | 0 | 0 |
| Milk, 1 cup | 0 | 0 |
* DV = Daily Value. DVs were developed by the U.S. Food and Drug Administration (FDA) to help consumers compare the nutrient contents of products within the context of a total diet. The DV for iron is 18 mg for adults and children age 4 and older. Foods providing 20% or more of the DV are considered to be high sources of a nutrient.
[Source 9]Folate
Folate is also known vitamin B9 (Folacin, Folic Acid, Pteroylglutamic acid) that is naturally present in many foods.
Folic Acid is a form of folate that is manufactured and used in dietary supplements and fortified foods 10.
Your body need folate to make DNA and other genetic material. Folate is also needed for the body’s cells to divide.
In women and pregnant mothers, folic acid is very important because it can help prevent some major birth defects of the baby’s brain and spine (anencephaly and spina bifida). (Source 11).
Every woman needs folic acid every day, whether she’s planning to get pregnant or not, for the healthy new cells the body makes daily. Think about the skin, hair, and nails. These – and other parts of the body – make new cells each day.
Centers for Disease Control and Prevention urges women to take 400 mcg of folic acid every day, starting at least one month before getting pregnant and while she is pregnant, to help prevent major birth defects of the baby’s brain and spine.
Folic acid and folate also help your body make healthy new red blood cells. Red blood cells carry oxygen to all the parts of your body. If your body does not make enough red blood cells, you can develop anemia. Anemia happens when your blood cannot carry enough oxygen to your body, which makes you pale, tired, or weak. Also, if you do not get enough folic acid, you could develop a type of anemia called folate-deficiency anemia 12.
Folate functions as a coenzyme or cosubstrate in single-carbon transfers in the synthesis of nucleic acids (DNA and RNA) and metabolism of amino acids 13. One of the most important folate-dependent reactions is the conversion of homocysteine to methionine in the synthesis of S-adenosyl-methionine, an important methyl donor 13. Another folate-dependent reaction, the methylation of deoxyuridylate to thymidylate in the formation of DNA, is required for proper cell division. An impairment of this reaction initiates a process that can lead to megaloblastic anemia, one of the hallmarks of folate deficiency 14.
When consumed, food folates are hydrolyzed to the monoglutamate form in the gut prior to absorption by active transport across the intestinal mucosa 15. Passive diffusion also occurs when pharmacological doses of folic acid are consumed 15. Before entering the bloodstream, the monoglutamate form is reduced to tetrahydrofolate (THF) and converted to either methyl or formyl forms. The main form of folate in plasma is 5-methyl-THF. Folic acid can also be found in the blood unaltered (known as unmetabolized folic acid), but whether this form has any biological activity or can be used as a biomarker of status is not known 16.
The total body content of folate is estimated to be 10 to 30 mg; about half of this amount is stored in the liver and the remainder in blood and body tissues. A serum folate concentration is commonly used to assess folate status, with a value above 3 nanograms (ng)/mL indicating adequacy 14. This indicator, however, is sensitive to recent dietary intake, so it might not reflect long-term status. Erythrocyte folate concentration provides a longer-term measure of folate intakes, so when day-to-day folate intakes are variable—such as in people who are ill and whose folate intake has recently declined—it might be a better indicator of tissue folate stores than serum folate concentration 15. An erythrocyte folate concentration above 140 ng/mL indicates adequate folate status 15, although some researchers have suggested that higher values are optimal for preventing neural tube defects 17.
Why do women need folic acid ?
Everyone needs folic acid to be healthy. But it is especially important for women:
- Before and during pregnancy. Folic acid protects unborn children against serious birth defects called neural tube defects. These birth defects happen in the first few weeks of pregnancy, often before a woman knows she is pregnant. Folic acid might also help prevent other types of birth defects and early pregnancy loss (miscarriage). Since about half of all pregnancies in the United States are unplanned 18, experts recommend all women get enough folic acid even if you are not trying to get pregnant.
- To keep the blood healthy by helping red blood cells form and grow. Not getting enough folic acid can lead to a type of anemia called folate-deficiency anemia. Folate-deficiency anemia is more common in women of childbearing age than in men.
Do Women need to take Folic Acid every day even if you’re not planning to get pregnant ?
Yes. All women who can get pregnant need to take 400 to 800 micrograms of folic acid every day, even if you’re not planning to get pregnant 19. There are several reasons why:
- Your birth control may not work or you may not use birth control correctly every time you have sex. In a survey by the Centers for Disease Control and Prevention, almost 40% of women with unplanned pregnancies were using birth control 20.
- Birth defects of the brain and spine can happen in the first few weeks of pregnancy, often before you know you are pregnant. By the time you find out you are pregnant, it might be too late to prevent the birth defects.
- You need to take folic acid every day because it is a water soluble B-vitamin. Water soluble means that it does not stay in the body for a long time. Your body metabolizes (uses) folic acid quickly, so your body needs folic acid each day to work properly.
What can happen if Women do Not get enough Folic Acid during Pregnancy ?
If you do not get enough folic acid before and during pregnancy, your baby is at higher risk for neural tube defects.
Neural tube defects are serious birth defects that affect the spine, spinal cord, or brain and may cause death. These include:
- Spina bifida 21. This condition happens when an unborn baby’s spinal column does not fully close during development in the womb, leaving the spinal cord exposed. As a result, the nerves that control the legs and other organs do not work. Children with spina bifida often have lifelong disabilities. They may also need many surgeries.
- Anencephaly 22. This means that most or all of the brain and skull does not develop in the womb. Almost all babies with this condition die before or soon after birth.
How much Folic Acid do Women need ?
All women need 400 micrograms of folic acid every day. Women who can get pregnant should get 400 to 800 micrograms of folic acid from a vitamin or from food that has added folic acid, such as breakfast cereal 23. This is in addition to the folate you get naturally from food.
Some women may need more folic acid each day. See the chart to find out how much folic acid you need.
| If you: | Amount of folic acid you may need daily 23 |
|---|---|
| Could get pregnant or are pregnant | 400–800 micrograms.23 Your doctor may prescribe a prenatal vitamin with more. |
| Had a baby with a neural tube defect (such as spina bifida) and want to get pregnant again | 4,000 micrograms. Your doctor may prescribe this amount. Research shows taking this amount may lower the risk of having another baby with spina bifida. 24 |
| Have a family member with spina bifida and could get pregnant | 4,000 micrograms. Your doctor may prescribe this amount. |
| Have spina bifida and want to get pregnant | 4,000 micrograms. Your doctor may prescribe this amount. Women with spina bifida have a higher risk of having children with the condition. |
| Take medicines to treat epilepsy, type 2 diabetes, rheumatoid arthritis, or lupus | Talk to your doctor or nurse. Folic acid supplements can interact with these medicines. |
| Are on dialysis for kidney disease | Talk to your doctor or nurse. |
| Have a health condition, such as inflammatory bowel disease or celiac disease, that affects how your body absorbs folic acid | Talk to your doctor or nurse. |
How can you be sure you get enough folic acid ?
You can get enough folic acid from food alone. Many breakfast cereals have 100% of your recommended daily value (400 micrograms) of folic acid.
If you are at risk for not getting enough folic acid, your doctor may recommend that you take a vitamin with folic acid every day. Most U.S. multivitamins have at least 400 micrograms of folic acid. Check the label on the bottle to be sure. You can also take a pill that contains only folic acid.
If swallowing pills is hard for you, try a chewable or liquid product with folic acid.
Are some women at risk for not getting enough folic acid ?
Yes, certain groups of women do not get enough folic acid each day 25.
- Women who can get pregnant need more folic acid (400 to 800 micrograms). 24
- Nearly one in three African-American women does not get enough folic acid each day.
- Spanish-speaking Mexican-American women often do not get enough folic acid. However, Mexican-Americans who speak English usually get enough folic acid. 26
Not getting enough folic acid can cause health problems, including folate-deficiency anemia, and problems during pregnancy for you and your unborn baby.
How a Woman can get enough Folic Acid
There are two easy ways to be sure to get enough folic acid each day:
- Take a vitamin that has folic acid in it every day. Most multivitamins sold in the United States have the amount of folic acid women need each day. Women can also choose to take a small pill (supplement) that has only folic acid in it each day.
- Multivitamins and folic acid pills can be found at most local pharmacy, grocery, or discount stores.
- Check the label to be sure it contains 100% of the daily value (DV) of folic acid, which is 400 micrograms (mcg).
- Eat a bowl of breakfast cereal that has 100% of the daily value of folic acid every day.
Not every cereal has this amount. Make sure you check the label on the side of the box, and look for one that has “100%” next to folic acid or 400 micrograms (mcg).
How much folate do you need ?
The amount of folate you need depends on your age. Average daily recommended amounts are listed below in micrograms (mcg) of dietary folate equivalents (DFEs).
All women and teen girls who could become pregnant should consume 400 mcg of folic acid daily from supplements, fortified foods, or both in addition to the folate they get naturally from foods.
Table 3: Recommended Dietary Allowances (RDAs) for Folate
| Life Stage | Recommended Amount |
|---|---|
| Birth to 6 months* | 65 mcg DFE* |
| Infants 7–12 months* | 80 mcg DFE* |
| Children 1–3 years | 150 mcg DFE |
| Children 4–8 years | 200 mcg DFE |
| Children 9–13 years | 300 mcg DFE |
| Teens 14–18 years | 400 mcg DFE |
| Adults 19–50 years | 400 mcg DFE |
| Adults 51–70 years | 400 mcg DFE |
| Adults 71+ years | 400 mcg DFE |
| Pregnant teens and women | 600 mcg DFE |
| Breastfeeding teens and women | 500 mcg DFE |
* Adequate Intake (AI)
[Source 15]Do you need folic acid after menopause ?
Yes. Women who have gone through menopause still need 400 micrograms of folic acid every day for good health. Talk to your doctor or nurse about how much folic acid you need.
What foods provide folate ?
Folate is naturally present in many foods and food companies add folic acid to other foods, including bread, cereal, and pasta. You can get recommended amounts by eating a variety of foods, including the following:
- Leafy Green Vegetables (especially asparagus, Brussels sprouts, and dark green leafy vegetables such as spinach and mustard greens).
- Fruits and fruit juices (especially oranges and orange juice).
- Nuts, beans, and peas (such as peanuts, black-eyed peas, and kidney beans).
- Grains (including whole grains; fortified cold cereals; enriched flour products such as bread, bagels, cornmeal, and pasta; and rice).
- Folic acid is added to many grain-based products, enriched breads, cereals and corn masa flour (used to make corn tortillas and tamales, for example). To find out whether folic acid has been added to a food, check the product label.
Beef liver is high in folate but is also high in cholesterol, so limit the amount you eat. Only small amounts of folate are found in other animal foods like meats, poultry, seafood, eggs, and dairy products.
In January 1998, the U.S. Food and Drug Administration (FDA) began requiring manufacturers to add folic acid to enriched breads, cereals, flours, cornmeals, pastas, rice, and other grain products 27. Because cereals and grains are widely consumed in the United States, these products have become very important contributors of folic acid to the American diet. The fortification program was projected to increase folic acid intakes by approximately 100 mcg/day 28, but the program actually increased mean folic acid intakes in the United States by about 190 mcg/day 29. In April 2016, FDA approved the voluntary addition of folic acid to corn masa flour at levels consistent with other enriched grain products 30.
The Canadian government has also required the addition of folic acid to many grains, including white flour, enriched pasta, and cornmeal, since November 1, 1998 31. Other countries, including Costa Rica, Chile, and South Africa, have also established mandatory folic acid fortification programs 32.
Table 4. Selected Food Sources of Folate and Folic Acid
| Food | mcg DFE per serving | Percent DV* |
|---|---|---|
| Beef liver, braised, 3 ounces | 215 | 54 |
| Spinach, boiled, ½ cup | 131 | 33 |
| Black-eyed peas (cowpeas), boiled, ½ cup | 105 | 26 |
| Breakfast cereals, fortified with 25% of the DV† | 100 | 25 |
| Rice, white, medium-grain, cooked, ½ cup† | 90 | 23 |
| Asparagus, boiled, 4 spears | 89 | 22 |
| Spaghetti, cooked, enriched, ½ cup† | 83 | 21 |
| Brussels sprouts, frozen, boiled, ½ cup | 78 | 20 |
| Lettuce, romaine, shredded, 1 cup | 64 | 16 |
| Avocado, raw, sliced, ½ cup | 59 | 15 |
| Spinach, raw, 1 cup | 58 | 15 |
| Broccoli, chopped, frozen, cooked, ½ cup | 52 | 13 |
| Mustard greens, chopped, frozen, boiled, ½ cup | 52 | 13 |
| Green peas, frozen, boiled, ½ cup | 47 | 12 |
| Kidney beans, canned, ½ cup | 46 | 12 |
| Bread, white, 1 slice† | 43 | 11 |
| Peanuts, dry roasted, 1 ounce | 41 | 10 |
| Wheat germ, 2 tablespoons | 40 | 10 |
| Tomato juice, canned, ¾ cup | 36 | 9 |
| Crab, Dungeness, 3 ounces | 36 | 9 |
| Orange juice, ¾ cup | 35 | 9 |
| Turnip greens, frozen, boiled, ½ cup | 32 | 8 |
| Orange, fresh, 1 small | 29 | 7 |
| Papaya, raw, cubed, ½ cup | 27 | 7 |
| Banana, 1 medium | 24 | 6 |
| Yeast, baker’s, ¼ teaspoon | 23 | 6 |
| Egg, whole, hard-boiled, 1 large | 22 | 6 |
| Vegetarian baked beans, canned, ½ cup | 15 | 4 |
| Cantaloupe, raw, 1 wedge | 14 | 4 |
| Fish, halibut, cooked, 3 ounces | 12 | 3 |
| Milk, 1% fat, 1 cup | 12 | 3 |
| Ground beef, 85% lean, cooked, 3 ounces | 7 | 2 |
| Chicken breast, roasted, ½ breast | 3 | 1 |
* DV = Daily Value. The FDA developed DVs to help consumers compare the nutrient contents of products within the context of a total diet. The DV for folate is 400 mcg for adults and children aged 4 and older. However, the FDA does not require food labels to list folate content unless a food has been fortified with this nutrient. Foods providing 20% or more of the DV are considered to be high sources of a nutrient.
† Fortified with folic acid as part of the folate fortification program.
[Source 9]Vitamin B12
Vitamin B12 is also known as Cyanocobalamin is a nutrient that helps keep the body’s nerve and blood cells healthy and helps make DNA, the genetic material in all cells. Vitamin B12 also helps prevent a type of anemia called megaloblastic anemia that makes people tired and weak.
Vitamin B12 is a water-soluble vitamin that is naturally present in some foods, added to others, and available as a dietary supplement and a prescription medication. Vitamin B12 exists in several forms and contains the mineral cobalt 33, 34, 35, 36, so compounds with vitamin B12 activity are collectively called “cobalamins”. Methylcobalamin and 5-deoxyadenosylcobalamin are the forms of vitamin B12 that are active in human metabolism 37.
Two steps are required for the body to absorb vitamin B12 from food.
- First, food-bound vitamin B12 is released in the stomach’s acid environment (hydrochloric acid and and gastric protease in the stomach separate vitamin B12 from the protein to which vitamin B12 is attached in food) and is bound to R protein (haptocorrin) 37. When synthetic vitamin B12 is added to fortified foods and dietary supplements, it is already in free form and thus, does not require this separation step.
- Second, pancreatic enzymes cleave this B12 complex (B12-R protein) in the small intestine. After cleavage, intrinsic factor (a protein made by the stomach), secreted by parietal cells in the gastric mucosa, binds with the free vitamin B12. Intrinsic factor is required for absorption of vitamin B12, which takes place in the terminal ileum 37, 38. Approximately 56% of a 1 mcg oral dose of vitamin B12 is absorbed, but absorption decreases drastically when the capacity of intrinsic factor is exceeded (at 1–2 mcg of vitamin B12) 39. Some people have pernicious anemia, a condition where they cannot make intrinsic factor. As a result, they have trouble absorbing vitamin B12 from all foods and dietary supplements.
Pernicious anemia is an autoimmune disease that affects the gastric mucosa and results in gastric atrophy. This leads to the destruction of parietal cells, achlorhydria, and failure to produce intrinsic factor, resulting in vitamin B12 malabsorption 35, 37, 40, 41, 42. If pernicious anemia is left untreated, it causes vitamin B12 deficiency, leading to megaloblastic anemia and neurological disorders, even in the presence of adequate dietary intake of vitamin B12. For more details see below – Groups at Risk of Vitamin B12 Deficiency.
In the blood plasma, vitamin B12 is bound to transcobalamins I and II. Transcobalamin II is responsible for delivering vitamin B12 to tissues. The liver stores large amounts of vitamin B12. Enterohepatic reabsorption helps retain vitamin B12. Liver vitamin B12 stores can normally sustain physiologic needs for 3 to 5 yr if B12 intake stops (eg, in people who become vegans) and for months to 1 yr if enterohepatic reabsorption capacity is absent.
Vitamin B12 is required for proper red blood cell formation, neurological function, and DNA synthesis 33, 34, 35, 36, 37. Vitamin B12 functions as a cofactor for methionine synthase and L-methylmalonyl-CoA mutase. Methionine synthase catalyzes the conversion of homocysteine to methionine 37, 43. Methionine is required for the formation of S-adenosylmethionine, a universal methyl donor for almost 100 different substrates, including DNA, RNA, hormones, proteins, and lipids. L-methylmalonyl-CoA mutase converts L-methylmalonyl-CoA to succinyl-CoA in the degradation of propionate 35, 37, 43, an essential biochemical reaction in fat and protein metabolism. Succinyl-CoA is also required for hemoglobin synthesis.
Large amounts of vitamin B12 seem to be nontoxic but are not recommended for regular use (ie, as a general tonic).
How much vitamin B12 do you need ?
The amount of vitamin B12 you need each day depends on your age. Average daily recommended amounts for different ages are listed below in micrograms (mcg):
Table 1 lists the current RDAs for vitamin B12 in micrograms (mcg). For infants aged 0 to 12 months, the Food and Nutrition Board established an adequate intake (AI) for vitamin B12 that is equivalent to the mean intake of vitamin B12 in healthy, breastfed infants.
Recommended Dietary Allowance (RDA): average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%–98%) healthy individuals.
Adequate Intake (AI): established when evidence is insufficient to develop an RDA and is set at a level assumed to ensure nutritional adequacy.
| Life Stage | Recommended Amount |
|---|---|
| Birth to 6 months | 0.4 mcg |
| Infants 7–12 months | 0.5 mcg |
| Children 1–3 years | 0.9 mcg |
| Children 4–8 years | 1.2 mcg |
| Children 9–13 years | 1.8 mcg |
| Teens 14–18 years | 2.4 mcg |
| Adults | 2.4 mcg |
| Pregnant teens and women | 2.6 mcg |
| Breastfeeding teens and women | 2.8 mcg |
(Source 44).
What foods provide vitamin B12 ?
Vitamin B12 is naturally found in animal products, including fish, meat, poultry, eggs, milk, and milk products. Vitamin B12 is generally not present in plant foods, but fortified breakfast cereals are a readily available source of vitamin B12 with high bioavailability for vegetarians 37, 45, 46, 47. Some nutritional yeast products also contain vitamin B12. Fortified foods vary in formulation, so it is important to read product labels to determine which added nutrients they contain.
The U.S. Department of Agriculture’s (USDA’s) Nutrient Database Web site 45 lists the nutrient content of many foods and provides a comprehensive list of foods containing vitamin B12 arranged by nutrient content 48 and by food name 49.
Dietary vitamin B12 deficiency usually results from inadequate absorption, but deficiency can develop in vegans who do not take vitamin supplements. Infants of vegan mothers should receive supplemental vitamin B12 from birth. Deficiency causes megaloblastic anemia, damage to the white matter of the spinal cord and brain, and peripheral neuropathy. Diagnosis is usually made by measuring serum vitamin B12 levels. The Schilling test helps determine etiology 50.
Vitamin B12 is found naturally in a wide variety of animal foods and is added to some fortified foods. Plant foods have no vitamin B12 unless they are fortified. You can get recommended amounts of vitamin B12 by eating a variety of foods including the following:
- Beef liver and clams, which are the best sources of vitamin B12.
- Fish, meat, poultry, eggs, milk, and other dairy products, which also contain vitamin B12.
- Some breakfast cereals, nutritional yeasts and other food products that are fortified with vitamin B12. To find out if vitamin B12 has been added to a food product, check the product labels.
Several food sources of vitamin B12 are listed in Table 2.
Table 5: Selected Food Sources of Vitamin B12
| Food | Micrograms (mcg) per serving | Percent DV* |
|---|---|---|
| Clams, cooked, 3 ounces | 84.1 | 1,402 |
| Liver, beef, cooked, 3 ounces | 70.7 | 1,178 |
| Breakfast cereals, fortified with 100% of the DV for vitamin B12, 1 serving | 6.0 | 100 |
| Trout, rainbow, wild, cooked, 3 ounces | 5.4 | 90 |
| Salmon, sockeye, cooked, 3 ounces | 4.8 | 80 |
| Trout, rainbow, farmed, cooked, 3 ounces | 3.5 | 58 |
| Tuna fish, light, canned in water, 3 ounces | 2.5 | 42 |
| Cheeseburger, double patty and bun, 1 sandwich | 2.1 | 35 |
| Haddock, cooked, 3 ounces | 1.8 | 30 |
| Breakfast cereals, fortified with 25% of the DV for vitamin B12, 1 serving | 1.5 | 25 |
| Beef, top sirloin, broiled, 3 ounces | 1.4 | 23 |
| Milk, low-fat, 1 cup | 1.2 | 18 |
| Yogurt, fruit, low-fat, 8 ounces | 1.1 | 18 |
| Cheese, Swiss, 1 ounce | 0.9 | 15 |
| Beef taco, 1 soft taco | 0.9 | 15 |
| Ham, cured, roasted, 3 ounces | 0.6 | 10 |
| Egg, whole, hard boiled, 1 large | 0.6 | 10 |
| Chicken, breast meat, roasted, 3 ounces | 0.3 | 5 |
*DV = Daily Value. DVs were developed by the U.S. Food and Drug Administration (FDA) to help consumers determine the level of various nutrients in a standard serving of food in relation to their approximate requirement for it. The DV for vitamin B12 is 6.0 mcg. However, the FDA does not require food labels to list vitamin B12 content unless a food has been fortified with this nutrient. Foods providing 20% or more of the DV are considered to be high sources of a nutrient, but foods providing lower percentages of the DV also contribute to a healthful diet.
[Source 9]Vitamin B12 Supplements
In dietary supplements, vitamin B12 is usually present as cyanocobalamin 37, a form that the body readily converts to the active forms methylcobalamin and 5-deoxyadenosylcobalamin. Dietary supplements can also contain methylcobalamin and other forms of vitamin B12.
Existing evidence does not suggest any differences among forms with respect to absorption or bioavailability. However the body’s ability to absorb vitamin B12 from dietary supplements is largely limited by the capacity of intrinsic factor. For example, only about 10 mcg of a 500 mcg oral supplement is actually absorbed in healthy people 39.
In addition to oral dietary supplements, vitamin B12 is available in sublingual preparations as tablets or lozenges. These preparations are frequently marketed as having superior bioavailability, although evidence suggests no difference in efficacy between oral and sublingual forms 51, 52.
Vitamin B12 Prescription Medications
Vitamin B12, in the form of cyanocobalamin and occasionally hydroxocobalamin, can be administered parenterally as a prescription medication, usually by intramuscular injection 53. Parenteral administration is typically used to treat vitamin B12 deficiency caused by pernicious anemia and other conditions that result in vitamin B12 malabsorption and severe vitamin B12 deficiency 53.
Vitamin B12 is also available as a prescription medication in a gel formulation applied intranasally, a product marketed as an alternative to vitamin B12 injections that some patients might prefer 54. This formulation appears to be effective in raising vitamin B12 blood levels 55, although it has not been thoroughly studied in clinical settings.
- U.S. National Library of Medicine. Medline Plus. Iron. https://medlineplus.gov/iron.html#cat_51[↩]
- Centers for Disease Control and Prevention. Recommendations to Prevent and Control Iron Deficiency in the United States. https://www.cdc.gov/mmwr/preview/mmwrhtml/00051880.htm[↩]
- Wessling-Resnick M. Iron. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler RG, eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2014:176-88.[↩]
- Aggett PJ. Iron. In: Erdman JW, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. Washington, DC: Wiley-Blackwell; 2012:506-20.[↩][↩]
- Murray-Kolbe LE, Beard J. Iron. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements. 2nd ed. London and New York: Informa Healthcare; 2010:432-8.[↩][↩]
- U.S. National Library of Medicine. Iron. https://livertox.nlm.nih.gov/Iron.htm[↩]
- Hurrell R, Egli I. Iron bioavailability and dietary reference values. Am J Clin Nutr 2010;91:1461S-7S. http://ajcn.nutrition.org/content/91/5/1461S.long[↩]
- Rutzke CJ, Glahn RP, Rutzke MA, Welch RM, Langhans RW, Albright LD, et al. Bioavailability of iron from spinach using an in vitro/human Caco-2 cell bioassay model. Habitation 2004;10:7-14. https://www.ncbi.nlm.nih.gov/pubmed/15880905[↩]
- U.S. Department of Agriculture, Agricultural Research Service. USDA National Nutrient Database for Standard Reference, Release 27. Nutrient Data Laboratory home page, 2014. https://ndb.nal.usda.gov/ndb/[↩][↩][↩]
- U.S. National Library of Medicine, MedlinePlus – Folic Acid – https://medlineplus.gov/folicacid.html[↩]
- Centers for Disease Control and Prevention – Facts About Folic Acid – https://www.cdc.gov/ncbddd/folicacid/about.html[↩]
- Office on Women’s Health, U.S. Department of Health and Human Services – Folic acid – https://www.womenshealth.gov/a-z-topics/folic-acid[↩]
- Bailey LB, Gregory JFr (2006). Folate. Present Knowledge in Nutrition. B. Bowman and R. Russell. Washington, DC, International Life Sciences Institute. I: 278-301.[↩][↩]
- Carmel R (2005). Folic Acid. Modern Nutrition in Health and Disease. M. Shils, M. Shike, A. Ross, B. Caballero and R. Cousins. Baltimore, MD, Lippincott Williams & Wilkins: 470-481.[↩][↩]
- Institute of Medicine. Food and Nutrition Board (1998). Dietary Reference Intakes: Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. Washington, DC, National Academy Press. https://www.nap.edu/catalog/6015/dietary-reference-intakes-for-thiamin-riboflavin-niacin-vitamin-b6-folate-vitamin-b12-pantothenic-acid-biotin-and-choline[↩][↩][↩][↩][↩]
- Yetley EA, Pfeiffer CM, Phinney KW, Fazili Z, Lacher DA, Bailey RL, et al. (2011). Biomarkers of folate status in NHANES: a roundtable summary. Am J Clin Nutr 94(1): 303S-312S. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3127517/[↩]
- Colapinto CK, O’Connor DL, Dubois L, Tremblay MS (2012). Folic acid supplement use is the most significant predictor of folate concentrations in Canadian women of childbearing age. Appl Physiol Nutr Metab 37(2): 284-292. http://www.nrcresearchpress.com/doi/full/10.1139/h11-161[↩]
- Finer, L.B., Zolna, M.R. (2016). Declines in unintended pregnancy in the United States, 2008-2011. The New England Journal of Medicine; 374(9):843–52.[↩]
- U.S. Preventive Services Task Force. (2016). Final Recommendation Statement: Folic Acid for the Prevention of Neural Tube Defects: Preventive Medication – https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/folic-acid-for-the-prevention-of-neural-tube-defects-preventive-medication[↩]
- Mosher, W.D., Jones, J., Abma, J.C. (2012). Intended and Unintended Births in the United States: 1982–2010 (PDF, 404 KB). National Health Statistics Reports; no. 55.[↩]
- CDC. (2016). Spina Bifida. – https://www.cdc.gov/ncbddd/spinabifida/facts.html[↩]
- CDC. (2015). Facts about Anencephaly. – https://www.cdc.gov/ncbddd/birthdefects/anencephaly.html[↩]
- U.S. Preventive Services Task Force. (2016). Final Recommendation Statement: Folic Acid for the Prevention of Neural Tube Defects: Preventive Medication[↩][↩][↩]
- CDC. (2016). Folic Acid Recommendations.- https://www.cdc.gov/ncbddd/folicacid/recommendations.html[↩][↩]
- Bailey, R.L., Dodd, K.W., Gahche, J.J., Dwyer, J.T., McDowell, M.A., Yetley, E.A., et al. (2010). Total folate and folic acid intake from foods and dietary supplements in the United States: 2003–2006. American Journal of Clinical Nutrition; 91(1): 231–237.[↩]
- Hamner, H.C., Cogswell, M.E., Johnson, M.A. (2011). Acculturation factors are associated with folate intakes among Mexican American women. The Journal of Nutrition; 141(10): 1889–97.[↩]
- U.S. Food and Drug Administration (1996). Food standards: amendment of standards of identity for enriched grain products to require addition of folic acid. Federal Register 61(44). https://www.gpo.gov/fdsys/pkg/FR-1996-03-05/pdf/96-5014.pdf[↩]
- Whittaker P, Tufaro PR, Rader JI (2001). Iron and folate in fortified cereals. J Am Coll Nutr 20(3): 247-254. https://www.ncbi.nlm.nih.gov/pubmed/11444421[↩]
- Choumenkovitch SF, Selhub J, Wilson PW, Rader JI, Rosenberg IH Jacques PF (2002). Folic acid intake from fortification in United States exceeds predictions. J Nutr 132(9): 2792-2798. http://jn.nutrition.org/content/132/9/2792.long[↩]
- Food and Drug Administration. Final rule: food additives permitted for direct addition to food for human consumption; folic acid. Federal Register 81(73):22176-22183, April 15, 2016. https://www.federalregister.gov/documents/2016/04/15/2016-08792/food-additives-permitted-for-direct-addition-to-food-for-human-consumption-folic-acid[↩]
- Government of Canada (1998). Regulations Amending the Food and Drug Regulations (1066). Canada Gazette 132(24).[↩]
- Centers for Disease Control and Prevention (2010). CDC Grand Rounds: additional opportunities to prevent neural tube defects with folic acid fortification. MMWR Morb Mortal Wkly Rep 59(31): 980-984. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5931a2.htm[↩]
- Herbert V. Vitamin B12 in Present Knowledge in Nutrition. 17th ed. Washington, DC: International Life Sciences Institute Press, 1996.[↩][↩]
- Herbert V, Das K. Vitamin B12 in Modern Nutrition in Health and Disease. 8th ed. Baltimore, MD: Williams & Wilkins, 1994.[↩][↩]
- Combs G. Vitamin B12 in The Vitamins. New York: Academic Press, Inc., 1992.[↩][↩][↩][↩]
- Zittoun J, Zittoun R. Modern clinical testing strategies in cobalamin and folate deficiency. Sem Hematol 1999;36:35-46. https://www.ncbi.nlm.nih.gov/pubmed/9930567?dopt=Abstract[↩][↩]
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes: Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. Washington, DC: National Academy Press, 1998.[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Klee GG. Cobalamin and folate evaluation: measurement of methylmalonic acid and homocysteine vs vitamin B(12) and folate. Clin Chem 2000;46:1277-83. https://www.ncbi.nlm.nih.gov/pubmed/10926922?dopt=Abstract[↩]
- Carmel R. How I treat cobalamin (vitamin B12) deficiency. Blood.2008;112:2214-21. https://www.ncbi.nlm.nih.gov/pubmed/18606874?dopt=Abstract[↩][↩]
- Gueant JL, Safi A, Aimone-Gastin I, Rabesona H, Bronowicki J P, Plenat F, et al. Autoantibodies in pernicious anemia type I patients recognize sequence 251-256 in human intrinsic factor. Proc Assoc Am Physicians 1997;109:462-9. https://www.ncbi.nlm.nih.gov/pubmed/9285945?dopt=Abstract[↩]
- Kapadia CR. Vitamin B12 in health and disease: part I—inherited disorders of function, absorption, and transport. Gastroenterologist 1995;3:329-44. https://www.ncbi.nlm.nih.gov/pubmed/8775094?dopt=Abstract[↩]
- Johnson MA. If high folic acid aggravates vitamin B12 deficiency what should be done about it? Nutr Rev 2007;65:451-8. https://www.ncbi.nlm.nih.gov/pubmed/17972439?dopt=Abstract[↩]
- Clarke R. B-vitamins and prevention of dementia. Proc Nutr Soc 2008;67:75-81. https://www.ncbi.nlm.nih.gov/pubmed/18234134?dopt=Abstract[↩][↩]
- National Institute of Health. Vitamin B12. https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/[↩]
- U.S. Department of Agriculture, Agricultural Research Service. 2011. USDA National Nutrient Database for Standard Reference, Release 24. Nutrient Data Laboratory Home Page, https://www.ars.usda.gov/northeast-area/beltsville-md/beltsville-human-nutrition-research-center/nutrient-data-laboratory/[↩][↩]
- Subar AF, Krebs-Smith SM, Cook A, Kahle LL. Dietary sources of nutrients among US adults, 1989 to 1991. J Am Diet Assoc 1998;98:537-47. https://www.ncbi.nlm.nih.gov/pubmed/9597026?dopt=Abstract[↩]
- Tucker KL, Rich S, Rosenberg I, Jacques P, Dallal G, Wilson WF, et al. Plasma vitamin B12 concentrations relate to intake source in the Framingham Offspring Study. Am J Clin Nutr 2000;71:514-22. https://www.ncbi.nlm.nih.gov/pubmed/10648266?dopt=Abstract[↩]
- U.S. Department of Agriculture, Agricultural Research Service. 2011. USDA National Nutrient Database for Standard Reference, Release 24. Nutrient Data Laboratory Home Page, https://ods.od.nih.gov/pubs/usdandb/VitaminB12-Content.pdf[↩]
- U.S. Department of Agriculture, Agricultural Research Service. 2011. USDA National Nutrient Database for Standard Reference, Release 24. Nutrient Data Laboratory Home Page, https://ods.od.nih.gov/pubs/usdandb/VitaminB12-Food.pdf[↩]
- Merck Sharp & Dohme Corp., Merck Manual. Vitamin B 12. https://www.merckmanuals.com/professional/nutritional-disorders/vitamin-deficiency,-dependency,-and-toxicity/vitamin-b-12[↩]
- Yazaki Y, Chow G, Mattie M. A single-center, double-blinded, randomized controlled study to evaluate the relative efficacy of sublingual and oral vitamin B-complex administration in reducing total serum homocysteine levels. J Altern Complement Med 2006;12:881-5. https://www.ncbi.nlm.nih.gov/pubmed/17109579?dopt=Abstract[↩]
- Sharabi A, Cohen E, Sulkes J, Garty M. Replacement therapy for vitamin B12 deficiency: comparison between the sublingual and oral route. Br J Clin Pharmacol 2003;56:635-8. https://www.ncbi.nlm.nih.gov/pubmed/14616423?dopt=Abstract[↩]
- Andrès E, Federici L, Affenberger S, Vidal-Alaball J, Loukili NH, Zimmer J, et al. B12 deficiency: a look beyond pernicious anemia. J Fam Pract 2007;56:537-42. https://www.ncbi.nlm.nih.gov/pubmed/17605945?dopt=Abstract[↩][↩]
- Suzuki DM, Alagiakrishnan K, Masaki KH, Okada A, Carethers M. Patient acceptance of intranasal cobalamin gel for vitamin B12 replacement therapy. Hawaii Med J 2006;65:311-4. https://www.ncbi.nlm.nih.gov/pubmed/17265990?dopt=Abstract[↩]
- Slot WB, Merkus FW, Van Deventer SJ, Tytgat GN. Normalization of plasma vitamin B12 concentration by intranasal hydroxocobalamin in vitamin B12-deficient patients. Gastroenterology.1997;113:430-3. https://www.ncbi.nlm.nih.gov/pubmed/9247460?dopt=Abstract[↩]





{kind=link}