
Contents
What is anorgasmia
Anorgasmia is the medical term for regular difficulty reaching orgasm after ample sexual stimulation, causing you personal distress. In males, anorgasmia is most closely associated with delayed ejaculation. Anorgasmia is far more common in females (4.7 percent) 1 than in males and is especially rare in younger men. The problem is greater in women who are post-menopause. Orgasm is defined an intense transient peak sensation of intense pleasure creating an altered state of consciousness associated with reported physical changes 2.
Primary anorgasmia
Primary anorgasmia is a condition where one has never experienced an orgasm. This is significantly more common in women, although it can occur in men who lack the gladipudendal (bulbocavernosus) reflex 3. Women with this condition can sometimes achieve a relatively low level of sexual excitement. Frustration, restlessness, and pelvic pain or a heavy pelvic sensation may occur because of vascular engorgement. On occasion, there may be no obvious reason why orgasm is unobtainable. In such cases, women report that they are unable to orgasm even if they have a caring, skilled partner, adequate time and privacy, and an absence of medical issues which would affect sexual satisfaction.
Secondary anorgasmia
Secondary anorgasmia is the loss of the ability to have orgasms (as opposed to primary anorgasmia which indicates a person who has never had an orgasm). Or loss of the ability to reach orgasm of past intensity. The cause may be alcoholism, depression, grief, pelvic surgery (such as total hysterectomy) or injuries, certain medications, illness, estrogen deprivation associated with menopause, or rape.
Secondary anorgasmia has been reported in 20% to 90% of men after undergoing prostatectomy 4. This is a serious adverse result because radical prostatectomy is considered the gold-standard treatment for localized prostate cancer according to most international clinical guidelines 5. Despite several technical advances, the achievement of good postoperative functional outcomes is still considered a troublesome issue for both patients and urologists; indeed, data reported in both open radical prostatectomy and robot-assisted radical prostatectomy series have consistently shown the postoperative incidence of erectile dysfunction (ED) and urinary incontinence (UI) to range from 6% to 68% and 4% to 31%, respectively 6. Both conditions have been thoroughly assessed in terms of risk factors, physiopathology, and postoperative management; similarly, patients are routinely counselled regarding the risk of erectile function (EF) and urinary continence (UC) impairment associated with radical prostatectomy. However, there is a series of other functional side effects that can occur after radical prostatectomy in addition to erectile dysfunction and urinary continence, which as a whole are referred to as neglected side effects 7. Indeed, data mainly from open radical prostatectomy series have shown impairments in sexual desire, orgasmic function and penile morphology after surgery 7. Among these conditions, orgasmic dysfunctions have been highlighted by several authors who have reported a non-negligible incidence of orgasm-associated incontinence (climacturia), orgasm-associated pain, and modifications of orgasmic sensations 8. Nevertheless, the awareness of these functional sequelae among both patients and physicians is still insufficient.
Unpreventable damage to the bladder neck, and eventually to the sympathetic fibres responsible for bladder neck contraction and external sphincter relaxation during the expulsion phase of ejaculation, has been proposed as a possible mechanism responsible for orgasm-associated urinary incontinence after radical prostatectomy (e.g., climacturia, which is defined as a leakage of urine occurring at orgasm) 7. Moreover, in a single study aiming to assess the pathophysiologic mechanisms of climacturia, Manassero et al 9 analysed video-urodynamic data coming from a series of patients with post-radical prostatectomy orgasm-associated urinary continence compared to a control group; they showed a significantly lower functional urethral length in patients with climacturia compared to controls, thus concluding that final urethral length may play a major role in determining this specific orgasmic alteration.
Finally, disruption of the ejaculatory mechanism, resulting in postoperative anejaculation, has been associated with altered orgasmic sensations, defined as the inability to achieve an orgasm (anorgasmia) or a markedly diminished intensity of orgasmic sensations 10. Numerous explanations for this have been proposed. From an organic standpoint, post-radical prostatectomy erectile difficulty could impair the stimulation of the dorsal penile nerve, thus reducing the afferent sensory stimuli responsible for orgasm/ejaculation 11; moreover, postoperative anejaculation could greatly affect patients’ psychological profile, creating a feeling of loss of masculinity, which in turn may affect orgasmic intensity 12. In this context, in a study assessing orgasmic function in a cohort of 63 patients after radical prostatectomy, Messaoudi et al 13 showed that among the most sexually motivated patients, 76.0% reported loss of masculine identity, 52% reported loss of self-esteem, and 36.0% reported performance anxiety. Similarly, the psychological distress related to surgery and cancer diagnoses may have a negative impact on the patient’s overall sexual health, including perceptions of orgasm 7.
Lastly, no data have been published yet regarding possible strategies to enhance the recovery of normal orgasmic function in the immediate postoperative setting. However, given the significant link between erectile function and orgasmic function, scientists speculate that all the factors that have been significantly associated with the risk of erectile dysfunction 14 (and urinary incontinence in the case of climacturia) may also play a major role in influencing orgasmic function outcomes after radical prostatectomy. This appears to be the case, although orgasmic function can still be normal after radical prostatectomy despite the absence of an erection 15.
Likewise, doctors are currently unable to offer proper treatment to patients complaining of orgasmic dysfunctions after radical prostatectomy surgery; indeed, although conservative strategies with potential good results could be suggested for climacturia and encouraging results have been published regarding the effect of urinary incontinence surgery on the improvement of orgasm-associated incontinence, doctors are still far from being able to suggest satisfactory treatments for either painful orgasm or postoperative anorgasmia 16.
Female anorgasmia
Orgasms vary in intensity, and women vary in the frequency of their orgasms and the amount of stimulation necessary to trigger an orgasm. In fact, most women don’t consistently have orgasms with vaginal penetration alone. Plus, orgasms often change with age, medical issues or medications you’re taking.
If you’re happy with the climax of your sexual activities, there’s no need for concern. However, if you’re bothered by lack of orgasm or the intensity of your orgasms, talk to your doctor about anorgasmia. Lifestyle changes and sex therapy may help.
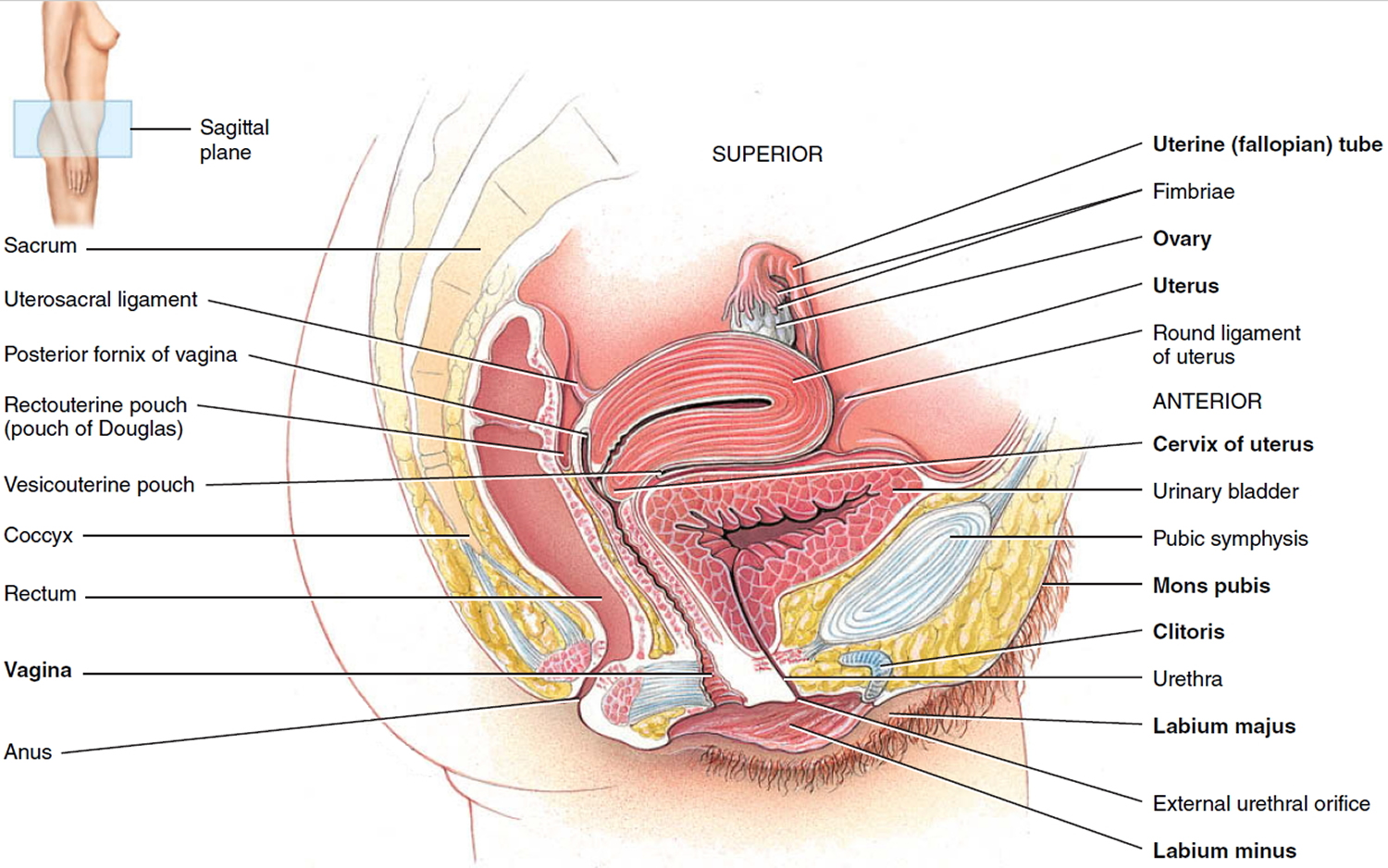
Figure 1. Female reproductive system
 Anorgasmia causes
Anorgasmia causes
About 10% to 15% of women have never had an orgasm. Surveys suggest that up to one half of women are not satisfied with how often they reach orgasm.
Sexual response involves the mind and body working together in a complex way. Both need to function well for an orgasm to happen.
Many factors can lead to problems reaching orgasm. They include:
Psychological causes
Many psychological factors play a role in your ability to orgasm, including:
- Mental health problems, such as anxiety or depression
- Poor body image
- Stress and financial pressures
- Fatigue and stress or depression
- Lack of knowledge about sexual function
- Cultural and religious beliefs
- Fear of pregnancy or sexually transmitted infections
- Embarrassment
- Guilt about enjoying sexual experiences
- Past sexual or emotional abuse
- A history of sexual abuse or rape
- Negative feelings about sex (often learned in childhood or teen years)
- Shyness or embarrassment about asking for the type of touching off that works best.
Relationship issues
Many couples who have problems outside of the bedroom also experience problems in the bedroom.Overarching issues may include:
- Lack of connection with your partner
- Unresolved conflicts or fights
- Poor communication of sexual needs and preferences
- Infidelity or breach of trust
- Intimate partner violence
- Boredom in sexual activity or a relationship
Health problems that can cause problems reaching orgasm include:
- Certain drugs that are prescribed. The most common drugs used to treat depression may cause this problem. These include fluoxetine (Prozac), paroxetine (Paxil), and sertraline (Zoloft)
- Hormonal disorders or changes, such as menopause
- Chronic illnesses that affect health and sexual interest
- Chronic pelvic pain, such as from endometriosis
- Damage to the nerves that supply the pelvis due to conditions such as multiple sclerosis, diabetic nerve damage, and spinal cord injury
- Spasm of the muscles surrounding the vagina that occurs against your will
- Vaginal dryness
- Gynecologic issues. Orgasm may be affected by gynecologic surgeries, such as hysterectomy or cancer surgeries. In addition, lack of orgasm often goes hand in hand with other sexual concerns, such as uncomfortable or painful intercourse.
- The aging process. As you age, normal changes in your anatomy, hormones, neurological system and circulatory system can affect your sexuality. A tapering of estrogen levels during the transition to menopause can decrease blood flow to the vagina and clitoris, which can delay or stop orgasm entirely.
- Alcohol and smoking. Too much alcohol can cramp your ability to climax; the same is true of smoking, which can limit blood flow.
Anorgasmia Outlook (Prognosis)
Women do better when treatment involves learning sexual techniques or a method called desensitization. This treatment gradually works to decrease the response that causes lack of orgasms. Desensitization is helpful for women with significant sexual anxiety.
Anorgasmia symptoms
An orgasm is a feeling of intense physical pleasure and release of tension, accompanied by involuntary, rhythmic contractions of your pelvic floor muscles. But it doesn’t always look — or sound — like it does in the movies. The way an orgasm feels varies from woman to woman, and in an individual woman, it may even differ from orgasm to orgasm.
By definition, the major symptoms of anorgasmia are inability to experience orgasm or long delays in reaching orgasm. But there are different types of anorgasmia:
- Lifelong anorgasmia. This means you’ve never experienced an orgasm.
- Acquired anorgasmia. This means you used to have orgasms, but now experience difficulty reaching climax.
- Situational anorgasmia. This means you are able to orgasm only during certain circumstances, such as during oral sex or with a certain partner. Most women can’t reach orgasm through vaginal penetration alone.
- Generalized anorgasmia. This means you aren’t able to orgasm in any situation or with any partner.
The symptoms of orgasmic dysfunction include:
- Being unable to reach orgasm
- Taking longer than you want to reach orgasm
- Having only unsatisfying orgasms
Anorgasmia diagnosis
A complete medical history and physical exam needs to be done, but results are almost always normal. If the problem began after starting a medicine, tell the health care provider who prescribed the drug. A qualified specialist in sex therapy may be helpful.
A medical evaluation for anorgasmia usually consists of:
- A thorough medical history. Your doctor may ask about your sexual history, surgical history and current relationship. Don’t let embarrassment stop you from giving candid answers. These questions provide clues to the cause of your problem.
- A physical exam. Your doctor will probably conduct a general physical exam to look for physical causes of anorgasmia, such as an underlying medical condition. Your doctor may also examine your genital area to see if there’s some obvious physical or anatomical reason for lack of orgasm.
Anorgasmia treatment
Anorgasmia can be difficult to treat. Your treatment plan will depend on the underlying cause of your symptoms, but your doctor may recommend a combination of lifestyle changes, therapy and medication.
Important goals when treating problems with orgasms are:
- A healthy attitude toward sex, and education about sexual stimulation and response
- Learning to clearly communicate sexual needs and desires, verbally or non-verbally.
Lifestyle changes and therapy
For most women, a key part of treatment includes addressing relationship issues and everyday stressors. Understanding your body and trying different types of sexual stimulation also can help.
- Understand your body better. Understanding your own anatomy and how you like to be touched can lead to better sexual satisfaction. If you need a refresher course on your genital anatomy, ask your doctor for a diagram or get out a mirror and look. Then take some time to explore your own body. Self-stimulation or using a vibrator can help you discover what type of touch feels best to you, and then you can share that information with your partner. If you’re uncomfortable with self-exploration, try exploring your body with your partner.
- Increase sexual stimulation. Women who’ve never had an orgasm may not be getting enough effective sexual stimulation. Most women need direct or indirect stimulation of the clitoris in order to orgasm, but not all women realize this. Switching sexual positions can produce more clitoral stimulation during vaginal penetration; some positions also allow for you or your partner to gently touch your clitoris during sex. Using a vibrator during sex also can help trigger an orgasm. Mental imagery or fantasizing during sex also may help. For some women, a device called a clitoral vacuum may improve blood flow and increase stimulation. This device is battery operated and hand-held, with a cup that fits over the clitoris.
- Seek couples counseling. Conflicts and disagreements in your relationship can affect your ability to orgasm. A counselor can help you work through disagreements and tensions and get your sex life back on track.
- Cognitive behavioral therapy. This type of therapy attempts to change the negative thoughts you may have about sex. You may be given directed masturbation exercises to do at home to learn how to achieve orgasm on your own.
- Try sex therapy. Sex therapists are therapists who specialize in treating sexual concerns. You may be embarrassed or nervous about seeing a sex therapist, but sex therapists can be very helpful in treating anorgasmia. Therapy often includes sex education, help with communication skills, and behavioral exercises that you and your partner try at home. For example, you and your partner may be asked to practice “sensate focus” exercises, a specific set of body-touching exercises that teach you how to touch and pleasure your partner without focusing on orgasm. Or you and your partner may learn how to combine a situation in which you reach orgasm — such as clitoral stimulation — with a situation in which you desire to reach orgasm, such as vaginal penetration. By using these techniques and others, you may learn to view orgasm as one pleasurable part of sexual intimacy, not the whole goal of every sexual encounter.
How to make sex better:
- Get plenty of rest and eat well. Limit alcohol, drugs, and smoking. Feel your best. This helps with feeling better about sex.
- Do Kegel exercises. Tighten and relax the pelvic muscles.
- Focus on other sexual activities, not just intercourse.
- Use birth control that works for both you and your partner. Discuss this ahead of time so you aren’t worried about an unwanted pregnancy.
- If other sexual problems, such as lack of interest and pain during intercourse, are happening at the same time, these need to be addressed as part of the treatment plan.
Discuss the following with your health provider:
- Medical problems, such as diabetes or multiple sclerosis
- New medicines
- Menopausal symptoms
The role of taking female hormone supplements in treating orgasmic dysfunction is unproven and the long-term risks remain unclear.
Treatment can involve education and learning to reach orgasm by focusing on pleasurable stimulation, and directed masturbation.
- Most women require clitoral stimulation to reach an orgasm. Including clitoral stimulation in sexual activity may be all that is necessary.
- If this does not solve the problem, then teaching the woman to masturbate may help her understand what she needs to become sexually excited.
Treatment may include sexual counseling to learn series of couples’ exercises to:
- Learn and practice communication
- Learn more effective stimulation and playfulness.
Medical treatments
Hormone therapies aren’t a guaranteed fix for anorgasmia. But they can help. So can treating underlying medical conditions.
- Treating underlying conditions. If a medical condition is hindering your ability to orgasm, treating the underlying cause may resolve your problem. Changing or modifying medications known to inhibit orgasm also may eliminate your symptoms.
- Estrogen therapy for postmenopausal women. Systemic estrogen therapy — by pill, patch or gel — can have a positive effect on brain function and mood factors that affect sexual response. Local estrogen therapy — in the form of a vaginal cream or a slow-releasing suppository or ring that you place in your vagina — can increase blood flow to the vagina and help improve sexual arousal. In some cases, your doctor may prescribe a combination of estrogen and progesterone.
- Testosterone therapy. Testosterone plays an important role in female sexual function, though in much lower amounts. As a result, testosterone may help increase sexual arousal. However, replacing testosterone in women is controversial and it’s not approved by the Food and Drug Administration for sexual dysfunction in women. Additionally, it can cause negative side effects, including acne, excess body hair (hirsutism) and male-pattern baldness. Testosterone seems most effective for women with low testosterone levels as a result of surgical removal of the ovaries (oophorectomy). If you choose to use this therapy, your doctor will closely monitor your symptoms to make sure you’re not experiencing negative side effects.
Alternative medicine
Natural products, such as those made with L-arginine, are marketed as helpful for improving a woman’s sex life. But these supplements haven’t been well-studied for this use, and they’re not regulated by the Food and Drug Administration.
Talk with your doctor before trying any natural therapies. These products can cause side effects and may interact with other medications. Your doctor can help determine if they are safe for you.
Coping and support
If you’re experiencing difficulty reaching orgasm, it can be frustrating for you and your partner. Plus, concentrating on climax can make the problem worse.
Most couples aren’t experiencing the headboard-banging, earth-shaking sex that appears on TV and in the movies. So try to reframe your expectations. Focus on mutual pleasure, instead of orgasm. You may find that a sustained pleasure plateau is just as satisfying as orgasm.
Anorgasmia in men
Anorgasmia defined as the persistent or recurrent difficulty, delay in, or absence of attaining orgasm after sufficient sexual stimulation, which causes personal distress 2. One of the major concerns with delayed orgasm and in particular anorgasmia, young males or men with reproductive interest, is the failure to inseminate and therefore male infertility. Men with anorgasmia may develop anxiety and frustration, which may lead to other sexual problems such as erectile dysfunction (impotence) and loss of sex drive. It is critically important to understand that orgasm is an entirely separate process from ejaculation, although they are designed to occur simultaneously.
Orgasm and ejaculation are two separate physiological processes that are sometimes difficult to distinguish. In the clinical setting, most men with failure to ejaculate (retrograde ejaculation and failure of emission) experience orgasm (although a man with failure to ejaculate for medical reasons may also have delayed orgasm or anorgasmia). However, men with anorgasmia will not ejaculate.
The International Consultation on Sexual Medicine defines anorgasmia as the perceived absence of orgasm, independent of the presence of ejaculation. The Diagnostic and Statistical Manual of Mental Disorders, Fifth edition 17 defines delayed orgasm as a marked delay in ejaculation or a marked infrequency or absence of ejaculation on almost all or all occasions (75–100%) of partnered sexual activity without the individual desiring delay, persisting for at least 6 months and causing significant distress to the individual. The sexual dysfunction is not explained by another non-sexual disorder, medication or significant relation/life distress/stressors.
Diagnostic and Statistical Manual of Mental Disorders, Fifth edition (DSM-5) 17 states that only 25% of males routinely achieve orgasm in all sexual encounters. According to the DSM-5, the prevalence remains constant up until age 50 and then the rate steadily increases with men in their 80s complaining twice as much as men under age 59 17. The increase with age is likely multifactorial and may be related to a combination of:
- changes in penile sensitivity,
- increased prevalence of testosterone deficiency,
- increased use of offending medications,
- decreased exercise tolerance and
- reduced partner tolerance for prolonged sexual intercourse.
In one study, the prevalence of primary delayed orgasm was found to be 1.5 in 1000 and secondary delayed orgasm in men under age 65 was 3–4% 18. Masters and Johnson only reported on 17 cases 19, Apfelbaum reported 34 cases 20, and Kaplan reported <50 cases 21. Because this is such an uncommon complaint, the true prevalence is probably underestimated. In a study by Carani et al, they assessed 48 adult men, 14 with hypothyroidism and 34 with hyperthyroidism, and delayed orgasm was identified in 64% of the hypothyroid patients and 3% of the hyperthyroid patients 22.
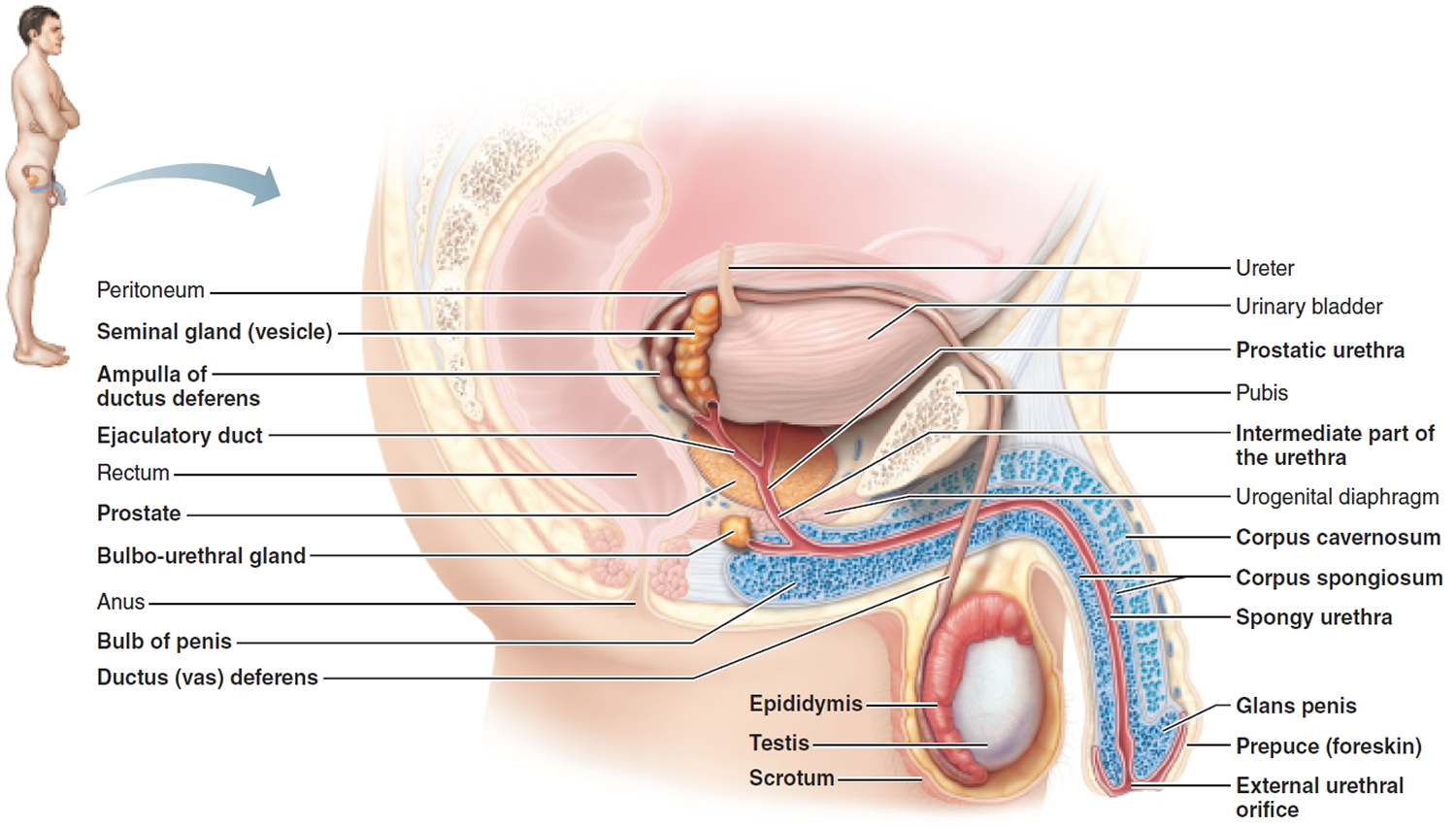
Figure 2. Male reproductive system
 Physiology of orgasm
Physiology of orgasm
Orgasm is a complex neurobiological process that comes as a result of sexual activity (physical sensation) and/or arousal (cognitive awareness). An International Conference on Sexual Medicine Committee has stated that the experience of orgasm is a distinct cortical (central nervous system) event, associated with the perception of striated muscle contractions and resulting in semen expelled during ejaculation, mediated through sensory neurons in the pelvic region 23. Although it is considered to be a distinct physiological process, male orgasm is strictly related to the process of ejaculation (Figure 2) 2. Ejaculation and orgasm are based on a complex interplay between the central nervous system and the peripheral nervous system, with the involvement of several neurotransmitters, including dopamine, norepinephrine, serotonin, acetylcholine, gamma-aminobutyric acid, and nitric oxide 24; moreover, hormonal pathways may influence the process of ejaculation, with active roles played by oxytocin, prolactin, thyroid hormone, glucocorticoids, and sex hormones 24.
Studies assessing brain function during ejaculation and orgasm using positron emission tomography 25 have shown that certain areas become hyperactivated during these processes. The parvicellular part of the subparafascicular thalamus, the posterodorsal preoptic nucleus, and the posterodorsal medial amygdaloid nucleus are all involved, and have connections with the medial preoptic area (MPOA) of the hypothalamus, which has been found to play an extensive role in controlling sexual behaviour 2. Moreover, the medial preoptic area (MPOA) showed further connections to the paraventricular thalamic nucleus (PVN), the periaqueductal grey, and the paragigantocellularis nucleus (nPGI) 2. The paraventricular thalamic nucleus (PVN) is known to have projections to the pudendal motor neurons in the L5~L6 spinal segment and to autonomic neurons located into the lumbosacral spinal cord; overall, the medial preoptic area (MPOA) has been shown to be involved in the stimulation of the ejaculatory response through interactions with the paragigantocellularis nucleus (nPGI) at the paraventricular thalamic nucleus (PVN) 26.
Figure 3. Physiology of orgasm and ejaculation
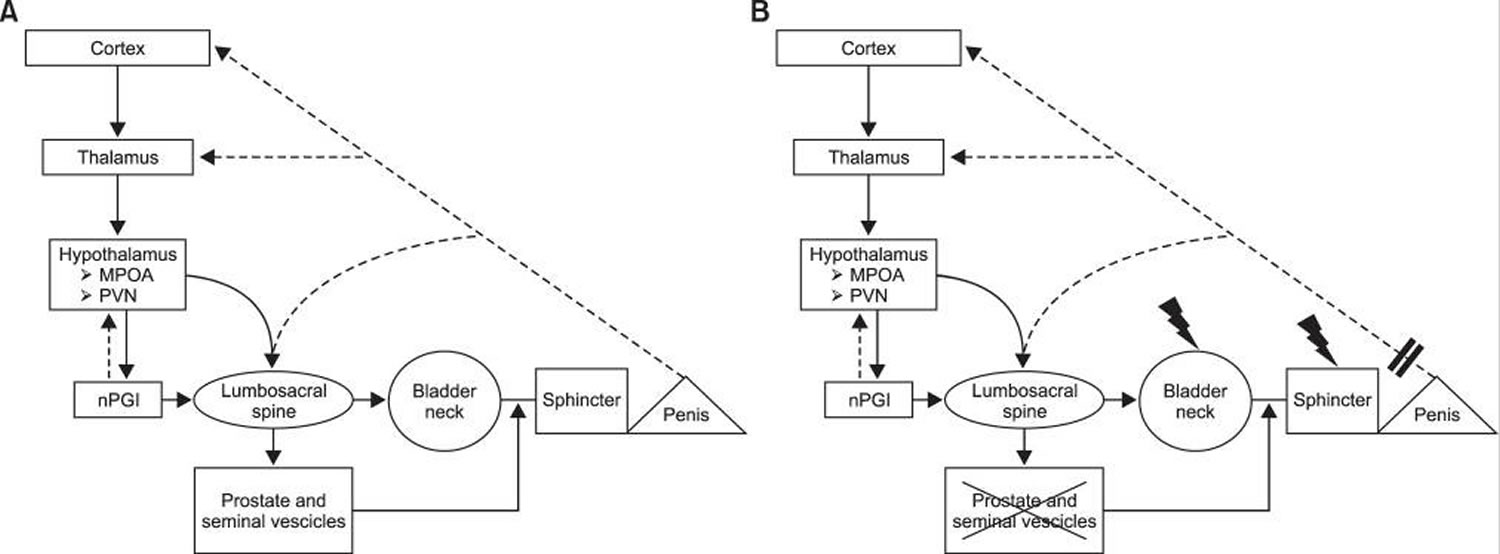
Note: (A) Physiology of orgasm and ejaculation. (B) Orgasmic alterations after radical prostatectomy. MPOA: medial preoptic area, PVN: paraventricular thalamic nucleus, nPGI: paragigantocellularis nucleus.
[Source 2]Erection
Erection occurs due to nervous impulses as a result of sexual arousal. The erectile tissue becomes engorged with blood, elongating and stiffening the penis. The nervous input also causes glands to secrete mucus, lubricating the penis in preparation for sexual intercourse.
Ejaculation
Ejaculation is controlled by separate nerve impulses to the penis. Nerve impulses cause the vas deferens to contract. The prostate gland and seminal vesicles both then contract, releasing their fluids into the propelling sperm. The release of fluid results in a full feeling in the genital organs. The sensory signals caused by this feeling results in contraction muscles compressing the base of the penile erectile tissue. This propels the sperm through the urethra and out of the body. At the same time, the contraction of muscles in the pelvis and body trunk causes pelvic thrusting movements.
The full process is referred to as the male orgasm.
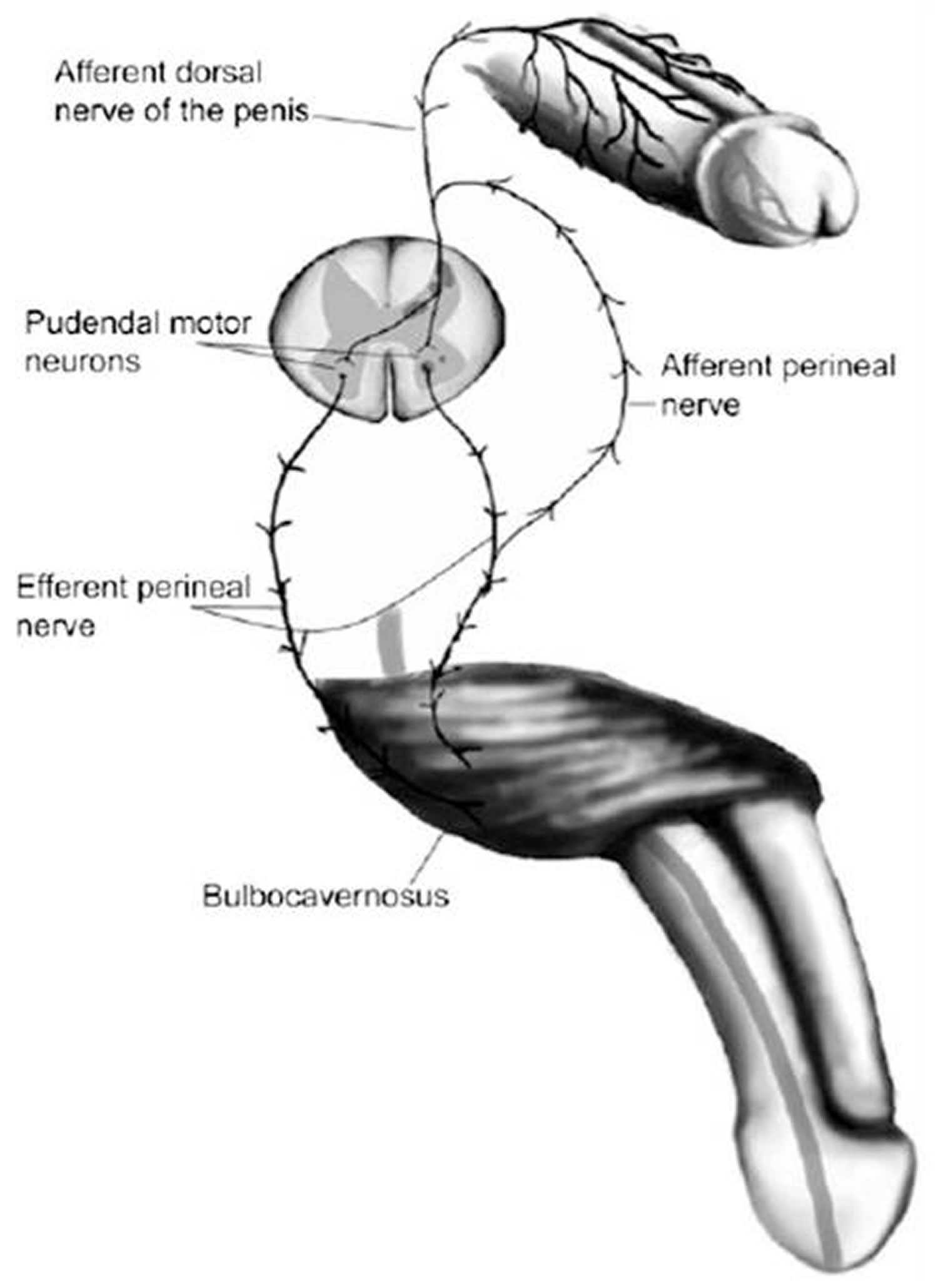
At the peripheral level, the main sensory input comes from the dorsal nerve of the penis transmitting sensation from the genital area to the spinal cord 27 (see Figure 4 below); this stimulation is potentiated by other areas at the level of the perineum and the testes.
The first step of the ejaculation process is the emission phase, characterized by closure of the bladder neck, preventing retrograde ejaculation, followed by the ejection of prostatic secretions and spermatozoa from the vas deferens into the prostatic urethra. Both the pelvic and the hypogastric plexus play a major role in the emission phase, involving mainly the sympathetic neurons; moreover, cerebral control over the spinal and peripheral neuronal elements is exerted in response to physical or visual stimulation 28. Subsequently, the ejection of semen through the urethral meatus is known as the expulsion phase, and is characterized by contractions of the pelvic striated muscles, the bulbospongiosus and ischiocavernosus muscles 29. Moreover, the bladder neck remains closed and the external urinary sphincter relaxes, and the pudendal nerve sensory stimuli resulting from the increased pressure in the posterior urethra and the contraction of the urethral bulb and other accessory sexual organs are processed at the level of the brain, thus inducing the sensation of orgasm 24.
When ejaculation occurs, the brain processes the sensation of the pressure buildup within the posterior urethra (bladder neck and external urinary sphincter are closed contemporaneously) leading up to seminal fluid emission and the contraction of the peri-urethral musculature. This processing leads to the triggering of an orgasm.
Figure 4. Reflex circuit needed to establish ejaculation
 Causes of anorgasmia and delayed orgasm in men
Causes of anorgasmia and delayed orgasm in men
Endocrinopathies
The role of prolactin in men is not fully understood. However, it is well understood that prolactin levels above normal, hyperprolactinemia, may result in an inhibitory effect on sexual desire 30. Mild forms of hyperprolactinemia (defined as >420 mU/L or 20 ng/mL) generally do not have an impact on sexual function; however, severe hyperprolactinemia (defined as >735 mU/L or 35 ng/mL) can have significant effects on sexual function, including erectile dysfunction and testosterone production suppression 31. Prolactin secretion is positively influenced by prolactin-releasing factors: thyroid-releasing hormone, oxytocin, vasopressin, and vasoactive intestinal peptide 32. Serotonin is implicated in the control of prolactin secretion via serotoninergic inputs from the dorsal raphe nucleus stimulating prolactin-releasing factors (thyroid-releasing hormone, oxytocin, vasopressin, and vasoactive intestinal peptide) in the paraventricular nucleus 33. Selective serotonin reuptake inhibitors are therefore capable of causing hyperprolactinemia and lead to delayed orgasm/anorgasmia 34. Corona et al 35 identified relationships between ejaculation and prolactin, thyroid stimulating hormone (TSH), and testosterone levels. Knowing that delayed orgasm and premature ejaculation represent two ends of a linear spectrum, it has been shown that prolactin and TSH levels progressively increased from patients with premature ejaculation to those with delayed orgasm, and the opposite was true for testosterone.
Hyperstimulation
Some men obtain greater pleasure from masturbation than they do with sexual intercourse and may continue deep-rooted habits such as frequent masturbation or using idiosyncratic masturbation techniques. Studies have shown a correlation between delayed orgasm and men with idiosyncratic masturbation practices 36. Also, with increasing frequency of masturbation the sensitivity of the penis can decline and lead to a vicious cycle where the man increases masturbation force to counteract the declining sensitivity, therefore leading to worsening delayed orgasm. Vaginal intercourse or orogenital stimulation may not be able to replicate the stimulation achieved through idiosyncratic masturbation and this may result in reduced penile stimulation leading to difficulty achieving an orgasm 36.
Patients with delayed orgasm have been shown to have higher masturbatory activity, decreased night-time emissions, lower orgasm and intercourse satisfaction scores on the International Index of Erectile Function (IIEF), as well as higher anxiety and depression scores when compared to controls 37. In a study by Xia et al 38, they compared 24 patients with primary delayed orgasm and 24 age-matched controls who had no sexual dysfunction complaints. They showed that patients with primary delayed orgasm had significantly longer intravaginal ejaculatory latency time (20 vs 5.5 minutes), higher frequency of masturbation, lower nocturnal emissions, and higher rates of anxiety and depression. They also found that although delayed orgasm patients had normal glans sensation, they reported penile shaft hyposensitivity and hypoexcitability. The patients with delayed orgasm were also found to more commonly use idiosyncratic masturbation methods.
Penile Sensation Loss
Penile sensation loss has been shown to increase with age 39. In a literature review (13 studies) by Rowland et al 40, they plotted penile sensory thresholds as a function of age as well as sexual functional status. They found penile sensation loss was more commonly present in those men with increased age and those with sexual dysfunctions.
Psychosexual Causes
Lifelong delayed orgasm has been associated with multiple psychological conditions. Some of these conditions include fear, anxiety, hostility, and relationship difficulties 41. Fear and anxiety during sexual relations have been examined, and the most common triggers included: hurting the female, impregnating the female, childhood sexual abuse, sexual trauma, repressive sexual education/religion, sexual anxiety, general anxiety, “spilling of seed,” and conflict in men in their first sexual relationship after becoming widowed or divorced 42.
The man may also suffer from a lack in sexual arousal, thus inhibiting his ability to reach orgasm. The man may achieve an erection without reaching adequate arousal to proceed with intercourse, such as men who achieve an erection with the assistance of erectogenic medications. With the assistance of medication, men are more likely to get an erection without significant psychoemotional arousal or the necessary mental/physical stimulation needed to reach orgasm 43.
Delayed orgasm based on a situational aspect (i.e. difficulties with a specific partner and not another) is more likely to be due to a psychologic etiology 44. One study looked at stress and anxiety related to timed intercourse demands for fertility treatments and found delayed orgasm developed in 6% of patients related to elevated anxiety levels 45. A novel study by Kirby et al used a rat model to show how stress can suppress the hypothalamic-pituitary-gonadal axis which is important in healthy normal sexual function 46. They showed that acute and chronic immobilization stress led to an increase in adrenal glucocorticoids causing an increase in gonadotropin inhibitory hormone which suppresses the hypothalamic-pituitary-gonadal axis via inhibition of gonadotropin releasing hormone (GnRH).
Selective serotonin reuptake inhibitors/Medications
There are numerous medications that have been implicated in the genesis of delayed orgasm including antidepressants (especially SSRIs), antipsychotics, and opioids 17. In a study by Corona et al 47, approximately 2000 male patients were evaluated for the sexual effects of anti-depressant therapy. A seven-fold risk for delayed orgasm was observed in SSRI patients, and they had a two-fold risk of low libido. In a study by Clayton et al, the effects on sexual functioning and antidepressant efficacy of bupropion extended release was compared with escitalopram 48. The incidence of orgasm dysfunction and worsened sexual function at week 8 was statistically significantly higher in the escitalopram (30%) vs bupropion (15%) and escitalopram (30%) vs placebo (9%) groups but not statistically significant in the bupropion (15%) vs placebo (9%) groups.
Many men have sexual problems. They become more common as men age. Problems can include:
- Erectile dysfunction
- Reduced or lost interest in sex
- Problems with ejaculation
- Low testosterone
Stress, illness, medicines, or emotional problems may also be factors. Occasional problems with sexual function are common. If problems last more than a few months or cause distress for you or your partner, you should see your health care provider.
In a study by Teloken et al 49, they performed an analysis of data on 206 patients who presented with secondary delayed orgasm. The cause for their condition were divided into selective serotonin reuptake inhibitor (SSRI) use (42%), low testosterone (21%; mean total testosterone 268±111 ng/dL), abnormal penile sensation (7%), chronic/idiosyncratic penile (hyper)stimulation (2%) and psychogenic (28%). Age-related hormonal declines (lower testosterone levels) and age-related loss of peripheral nerve conduction may account for the increased onset over age 50 years 17. It has also been suggested that hormonal aberrations such as hypothyroidism and testosterone deficiency may also play a role in delayed orgasm 35.
Table 1. Causes of anorgasmia and delayed orgasm in men
| Endocrine |
|
| Medication |
|
| Psychosexual Causes | |
| Hyperstimulation | |
| Penile sensation loss |
The surgical removal of the prostate along with the seminal vesicles and part of the vas deferens that occurs during radical prostatectomy has been associated with specific alterations of orgasmic function resulting from a disruption of the physiological process of orgasm/ejaculation at different levels (Figure 3).
Unpreventable damage to the bladder neck, and eventually to the sympathetic fibers responsible for bladder neck contraction and external sphincter relaxation during the expulsion phase of ejaculation, has been proposed as a possible mechanism responsible for orgasm-associated urinary incontinence after radical prostatectomy (e.g., climacturia, which is defined as a leakage of urine occurring at orgasm) 7. Moreover, in a single study aiming to assess the pathophysiologic mechanisms of climacturia, Manassero et al 9 analysed video-urodynamic data coming from a series of patients with post-radical prostatectomy orgasm-associated urinary incontinence compared to a control group; they showed a significantly lower functional urethral length in patients with climacturia compared to controls, thus concluding that final urethral length may play a major role in determining this specific orgasmic alteration.
Erectile dysfunction (Impotence)
Erectile dysfunction is the inability to develop or maintain an erection that is rigid enough to allow penetration of the vagina, and therefore functional sexual intercourse. Generally, the term erectile dysfunction is applied if this occurs frequently (75% of the time) over a significant period if time (several weeks to months). If this is the case, the term impotence may also be used.
Erectile dysfunction is estimated to effect 150 million men worldwide.
Erectile dysfunction may present in different ways. Some men are completely unable to develop an erection. Some may develop an erection that does not remain rigid enough to allow satisfactory intercourse.
There are several causes of erectile dysfunction, including certain drugs (prescription and non prescription), psychological causes, and problems with the hormones, nerves or blood vessels that supply the penis.
Erectile dysfunction is extremely common, particularly for men with heart disease, diabetes or who have been treated for prostate cancer.
Other problems with male sexual function include a lack of sexual drive or desire (libido), problems with ejaculation (ejaculatory dysfunction), and lack of pleasurable sensation (orgasm) during sex. These problems will not be discussed in detail.
Erectile dysfunction is a common problem as it affects as many as 40% of men. It is important that men who experience erectile dysfunction discuss it with their doctor, because the condition can have a negative impact on your relationships and self esteem; serious underlying causes need to be excluded; and effective treatment is available.
You should seek quality medical advice. Don’t seek help from unknown people on the internet. Go to a urologist with an interest in erectile dysfunction via a referral from your doctor. No reputable treatment for erectile dysfunction costs more than $100 for a first prescription, so beware if you are “signed up” for any long term agreements, as your requirements may change as time progresses. Despite what you may have heard, there are treatments that won’t break the bank. Talk to your doctor or urologist about available treatment options. Simple, safe and effective treatment is available. It is also an opportunity to review lifestyle issues and cardiovascular health. Treatment options include pills, penile injection therapy and the best means of long term normalization of erectile function, penile prosthetic surgery. This is a fixable problem.
Risk Factors for Male Sexual Dysfunction (Erectile Dysfunction, Impotence)
The predisposing factors for erectile dysfunction are as follows:
- Age
- Medical conditions such as diabetes mellitus and cardiovascular disease
- Neurological conditions including or arising from dementia, multiple sclerosis, stroke, or spinal cord or back injury
- Pelvic trauma, prostate surgery, previous priapism, prolonged bike riding (> 4 hours/week, depending on seat and posture)
- Depression and stress
- High blood pressure
- Obesity
- Increased cholesterol
- Smoking
- Certain drugs (some antidepressants, particularly SSRIs; diuretics; and others)
- Alcohol and recreational drugs such as cocaine and heroin may initially stimulate sexual arousal, however long term use has been shown to lead to erectile dysfunction.
If a man has the risk factors for cardiovascular disease during middle age (smoking, obesity, high cholesterol), he is at an increased risk of developing erectile dysfunction.
Exercise has been shown to have a protective effect.
Progression of Male Sexual Dysfunction (Erectile Dysfunction, Impotence)
Around one third of men who experience erectile dysfunction find that, without treatment, it becomes worse over time. Around a third of men find that erectile dysfunction improves without treatment.
Around half of men with severe erectile dysfunction remain impotent in the long term without treatment.
These figures vary depending on the cause of the erectile dysfunction. Even if men choose not to pursue treatment for erectile dysfunction, it is important that they be investigated by a doctor, as erectile dysfunction may indicate an increased risk of cardiovascular disease.
Prognosis of Male Sexual Dysfunction (Erectile Dysfunction, Impotence)
For the great majority of men, erectile dysfunction can be effectively treated.
It is essential that if you experience erectile dysfunction, you discuss it with your doctor. Serious underlying causes need to be excluded. Many treatment options are available, and your doctor can help you decide which one is most appropriate for you.
Some causes of erectile dysfunction such as hormonal problems or anxiety may be cured completely with treatment and/or therapy. Even if the underlying cause cannot be cured, medication may still allow a satisfactory erection. Ignoring the problem tends not to make it better, and can have a significant impact on relationships and self-esteem.
Symptoms of Male Sexual Dysfunction (Erectile Dysfunction, Impotence)
Temporary failure of erection is very common and is likely to resolve. If ongoing erectile dysfunction develops, the impact on relationships and self-esteem can be devastating. Men who suffer from erectile dysfunction are known to experience significant psychological distress. It is believed that sexual self-consciousness leads to:
- increased appearance related anxieties;
- interferes with attention, focus and concentration;
- impairs physical performance; and
- reduces awareness of our physiological arousals leading to sexual dysfunction.
This improves when erectile dysfunction is successfully treated.
While studies are limited, it has been shown that male sexual dysfunction can also negatively impact the sexual function of female partners. A study comparing the sexual function of women with partners with erectile dysfunction to those without showed that sexual arousal, lubrication, orgasm, satisfaction, pain and total score were significantly lower in those who had partners with erectile dysfunction. Later in that study, a large proportion of the men with erectile dysfunction underwent treatment. Following treatment, sexual arousal, lubrication, orgasm, satisfaction and pain were all significantly increased. It was concluded that female sexual function is impacted by male erection status, which may improve following treatment of male sexual dysfunction.
It is essential to discuss erectile dysfunction with your doctor, so any serious underlying causes can be excluded and treatment options can be discussed. Many men are embarrassed discussing this issue with their doctor, or even their partner. Open communication with your doctor, and in your relationship, is important for effectively managing this common problem.
Effective treatment for erectile dysfunction is available, and for most men will allow the return to a fulfilling sex life. The side effects of the treatment for erectile dysfunction vary depending on the treatment that is used. Some may interrupt the spontaneity of sexual activity. For example, phosphodiesterase 5 (PDE-5) inhibitors (e.g. Levitra, Viagra, Cialis, Revatio) typically need to be taken one hour before sex. Side effects may include headaches, indigestion, vasodilation, diarrhea and blue tinge to vision. Other treatments such as penile injections may cause pain at the injection site, or an erection that will not go down. Treatment options need to be carefully discussed with your doctor to determine which one is best suited to you.
How is Male Sexual Dysfunction (Erectile Dysfunction, Impotence) Diagnosed?
Clinical Examination of Male Sexual Dysfunction (Erectile Dysfunction, Impotence)
Following a detailed discussion about the history of erectile dysfunction and its risk factors, your doctor will examine the testicles and penis to help determine the cause of erectile dysfunction. Your doctor will check reflexes and pulses in the area to see if problems with blood vessels or nerves are contributing to the erectile dysfunction. If necessary, your doctor will order tests to help diagnose erectile dysfunction.
Diagnosis is based on information provided to the doctor regarding the history of erectile dysfunction (how quickly it came on, how often it occurs, etc), the assessment of risk factors, and whether erections still occur overnight while a man is asleep. It is normal for a man to have 3-5 full erections overnight during REM sleep.
In order to establish whether normal erections are occurring overnight (nocturnal erections), the doctor may organize nocturnal penile tumescence (NPT) testing. This involves wearing a monitor overnight in your own home. The data from this monitor is then assessed to analyse how often erections occurred, how long they lasted, and how rigid and large the penis was during the erections. If nocturnal penile tumescence (NPT) testing is normal, the cause of erectile dysfunction is usually psychological. If not, further testing of the blood flow in the genital area may be required to see if there is blockage or leakage. The doctor may also organize a blood test of levels of hormones such as testosterone, prolactin and thyroid stimulating hormone to see if these are contributing to the erectile dysfunction.
How is Male Sexual Dysfunction (Erectile Dysfunction, Impotence) Treated?
Before starting treatment for erectile dysfunction, a doctor needs to check there is no underlying cardiovascular disease, and do other checks to determine the cause of the erectile dysfunction.
The most common treatment for erectile dysfunction is drugs known as phosphodiesterase-5 (PDE-5) inhibitors. These include tadalafil (Cialis), vardenafil (Levitra), and sildenafil citrate (Viagra or Revatio). These are effective for about 75% of men with erectile dysfunction. They are tablets that are taken around an hour before sex, and last between 4 and 36 hours. Sexual stimulation is required before an erection will occur. The PDE-5 inhibitors cause dilation of blood vessels in the penis to allow erection to occur, and help it to stay rigid. Men using nitrate medication (e.g. GTN spray or sublingual tablets for angina) should not use PDE-5 inhibitors.
If testosterone levels are found to be low, erectile dysfunction should initially be treated with testosterone replacement therapy.
If PDE-5 inhibitors are not suitable or don’t work, other therapies include injections into the base of the penis, which cause flow of blood into the penis and a fairly immediate erection that lasts around an hour. The drugs injected are alprostadil (Caverject and Erectile dysfunctionex) and Invicorp (VIP and phentolamine). Alprostadil may also be inserted as a gel into the opening of the penis. This is not suitable if your partner is pregnant.
Vacuum erection devices use a pump mechanism to create negative pressure around the penis, encouraging it to become erect. An elastic device is then placed around the base of the penis to help maintain the erection.
As a last resort, penile prostheses may be considered. Malleable rods and inflatable versions are available. This option involves surgery to insert the device, and so has more risks than the other treatments.
Surgery to correct blocked or leaking blood vessels used to be popular, but is not very effective for long term erectile function unless it is being done to correct traumatic vascular damage in young men.
Erectile dysfunction experienced by obese men has been shown to improve considerably with weight loss and exercise.Other lifestyle changes that improve erectile dysfunction include reducing the use of alcohol, recreational drugs and cigarettes.
If erectile dysfunction is found to be caused by anxiety or depression, psychotherapy may be an effective treatment on its own or in combination with certain drugs (e.g. antidepressants). Sexual therapy counselors specialize in this field.
If men are found to be taking a medication that is known to cause erectile dysfunction, their doctor may prescribe an alternative, equally effective therapy.
Anorgasmia in men diagnosis
History and Physical Exam
Management should begin with a good medical/psychosexual history, social/religious history, medication list, and physical exam. Focusing on the major etiologic factors (as listed above) is a useful starting point. Medication history should focus on selective serotonin reuptake inhibitor (SSRI) agents and other psychotropic agents, and define the onset of the use of the medication as it pertains to the timing of onset of delayed orgasm. Asking about penile sensitivity is a useful question, especially in men at risk for penile sensation loss such as diabetics. Symptoms and signs of endelayed orgasmcrinopathies such as testosterone deficiency, hypothyroidism and hyperprolactinemia should be sought. Masturbatory style is another useful line of inquiry as frequent masturbation or idiosyncratic masturbatory styles may lead to delayed orgasm. Defining relationship status, satisfaction and the role external stressors may be playing in the delayed orgasm genesis is also important.
Furthermore, identifying the onset of the delayed orgasm is critical, whether lifelong or acquired. Next, understanding whether the condition is generalized or situational is also critical to understanding the pathophysiology. Asking patients to describe a typical sexual encounter is often a useful ploy to unearth potential contributing factors. Defining the consistency of the problem, that is: “does it happen all the time or only some of the time? with sexual intercourse and sexual outercourse with a partner? and how this differs between partner-based relations and masturbation?” For example, men who achieve orgasm with masturbation but have difficulty with partner-based relations often have one of two factors as causes – loss of penile sensitivity (overcome by vigorous masturbation) or psychological issues (interpersonal conflict, fear, anxiety, or hostility). Inquiring about how long a man attempts relations before stopping may also provide valuable insight into the problem. Some older men, due to inadequate exercise reserve of upper body strength, cease sexual relations sooner than they did when they were younger and thus interpret this as delayed orgasm. Finally, asking about strategies or medications that have been tried previously for this problem will aid in plotting a course of treatment.
Additional Testing
The role of laboratory testing, such a testosterone and TSH levels, is optional and is applied depending upon patient symptoms. If laboratory values are abnormal, endelayed orgasmcrine function should be corrected. As shown by Carani et al 22, with correction of thyroid hormone levels, patients had significant improvements in delayed orgasm. After thyroid hormone treatment and normalization of lab values, half of the hypothyroid patients reported their delayed orgasm improved, and intravaginal ejaculatory latency time improved from 22 to 7 minutes.
In patients complaining of loss of penile sensitivity, biothesiometry and/or pudendal somatosensory evoked potentials might be warranted 36. Biothesiometry examines the sensory threshold of vibratory tactile stimulation. Pudendal somatosensory evoked potentials evaluates the afferent activity from the dorsal nerve of the penis towards the brain. Sympathetic skin testing is another test that allows the evaluation of sympathetic efferent flow to the skin of the genitals. Lastly, sacral reflex arc testing examines the motor and sensory branches of the pudendal nerve and nerve roots S2, S3, and S4 51.
Anorgasmia in men treatment
Lifestyle changes and therapy
Various lifestyle changes include: steps to improve intimacy, reduce masturbation frequency, change of masturbation style and decreasing alcohol consumption, 52.
Figure 5. Anorgasmia Management Plan (for Men)
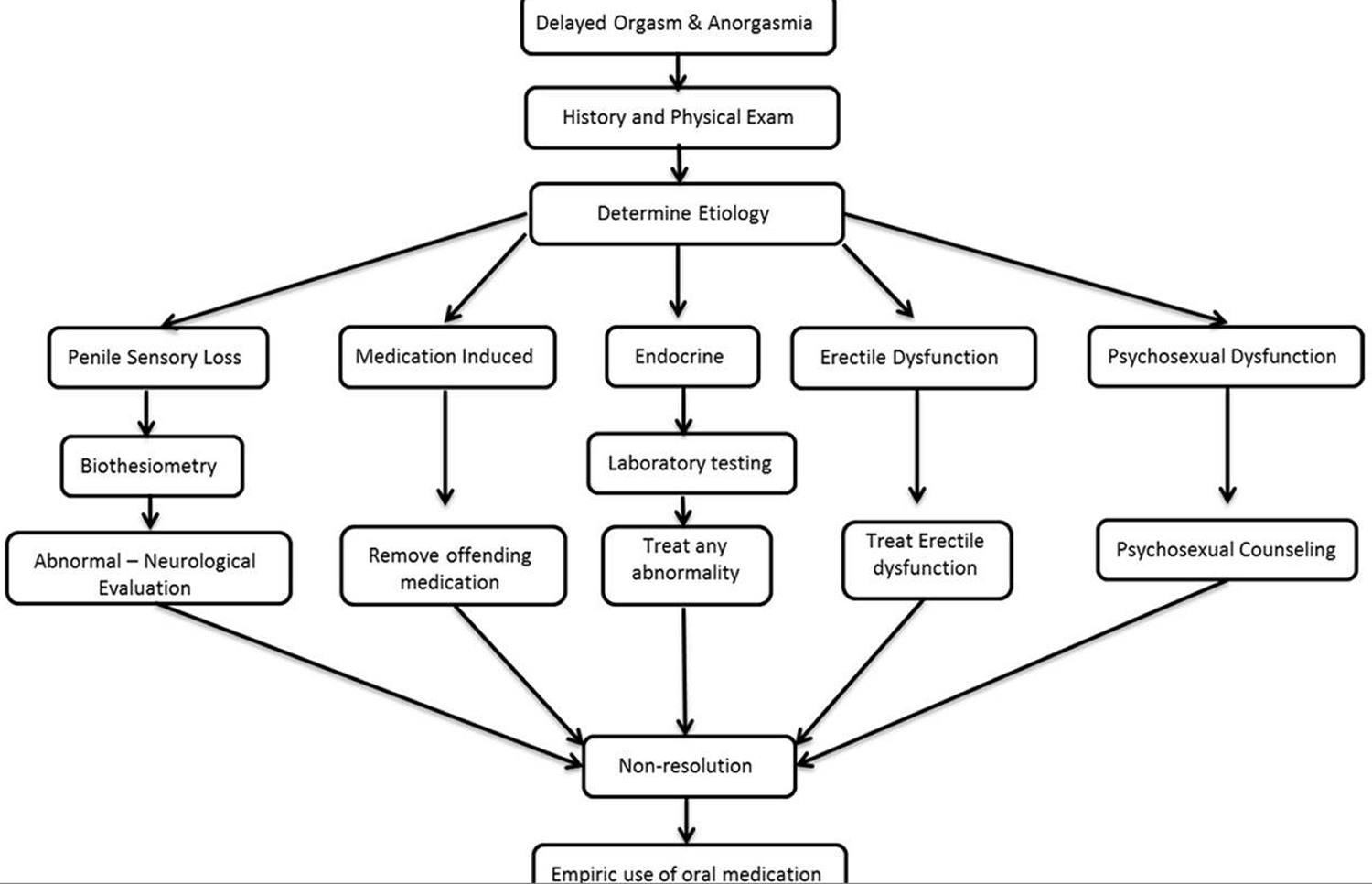
Psychosexual Counseling
Once the organic causes are ruled out and in some cases contemporaneously, the patient may benefit from a thorough psychosexual evaluation (along with his partner). There are numerous types of psychotherapy techniques that have been used with delayed orgasm including: masturbation retraining/desensitization, adjustments of sexual fantasies, changes in arousal methods, sexual education, sexual anxiety reduction, increased genital stimulation, and role playing an exaggerated orgasm alone and/or with his partner 53. There are numerous strategies that utilize combinations of approaches. Success rates are difficult to determine from literature, and few have had significant testing of their results.
Medications
There are no FDA approved drugs for delayed orgasm, and those drugs that have been studied often have limited efficacy or significant side effect profiles. One could first consider withdrawing any offending medications if possible, such as SSRIs, although it is our clinical practice to liaise with the SSRI-prescribing clinician and have them coordinate the drug manipulation (drug holiday, substitution or cessation) and monitor the patient.
Some medications are used to counteract the side effects of other medications. Bupropion (open-label bupropion-SR 150 mg/day for 2 months) was trialed in an age-matched group of 19 males with reported lifelong delayed orgasm 37. There was a 25% decrease in mean intravaginal ejaculatory latency time, and the percentage rating control over ejaculation as “fair to good” increased from 0 to 21%. Also, orgasm and intercourse satisfaction domain scores on the intravaginal ejaculatory latency time improved significantly from baseline after treatment.
Cyproheptadine, an anti-histamine known to increase brain serotonin levels, has been studied to treat delayed orgasm related to SSRI use 54. However, there have been no large randomized controlled studies conducted with this agent to date. In a small study by Ashton et al 55, improvement was seen in 12/25 men treated with cyproheptadine for SSRI-induced delayed orgasm. Treatment was limited by sedation and reversal of the antidepressant’s effects.
Amantadine, an indirect stimulant of central and peripheral dopaminergic nerves, has been used by some investigators to stimulate sexual behavior in rats 51. In a human study, Ashton et al used amantadine to treat SSRI-induced delayed orgasm and found improvements in 8/19 men 55.
Ashton also used yohimbine and found improvements treating men with SSRI-induced delayed orgasm. Yohimbine is a product from the bark of the Pausinystalia johimbe tree and functions as an α-2 adrenergic receptor blocker. Yohimbine has been used as a traditional medicine in Africa as an aphrodisiac, and is being studied as a possible medication to treat erectile dysfunction. Several groups have studied yohimbine to treat other sexual dysfunctions 56. Adeniyi et al 56 performed a study using yohimbine in 29 patients with anorgasmia who presented to their clinic with complaints of infertility or orgasmic dysfunction. The patients achieved orgasm at a mean yohimbine dose of 38 mg. In all, 19 men achieved orgasm; however, 3 required the use of penile vibratory stimulation. Also, 7 out of 8 men with secondary anorgasmia were able to achieve orgasm.
Oxytocin is a nine amino acid peptide released by the posterior pituitary at higher levels during orgasm. Ishak et al 57 reported on one case of oxytocin used successfully for the treatment of anorgasmia. The patient was given a 20–24 IU dose of oxytocin intranasally when he was ready to orgasm, and a positive response was reported through at least 8 months of follow up.
A rat model (sexually sluggish male rats) has been used to study low dose endocannabinoid anandamide effects on the CB1 cannabinoid receptor to lower the ejaculatory threshold 58. Their results were encouraging and found that low dose anandamide did lower the ejaculatory threshold in their study group. The effects were temporary and the rats no longer displayed the behavior 7 days after the initial dosing. There were no effects observed on other sexual behaviors.
Endocrine Therapy
The dopamine agonist cabergoline has been shown to augment plasma prolactin levels and was studied for its utility in treating psychogenic erectile dysfunction (ED) 59. In one study, patients were treated with cabergoline 0.5 mg for 4 months in a randomized, double-blinded, placebo-controlled trial with 25 patients in the active arm and 25 in the placebo arm. Baseline hyperprolactinemia was found in 38 of the patients, in addition, after the treatment period ended both prolactin and testosterone levels normalized in most of the patients. Erectile function, orgasmic function, and sexual desire were all enhanced based on International Index of Erectile Function questionnaire scores.
Testosterone plays an important role in sexual response and motivation with effects at both the central and peripheral levels. Testosterone also plays a facilitative role in the orgasmic response mechanism 60. Hackett et al 61 performed a prospective, randomized, double-blind, placebo-controlled trial on 190 men with testosterone deficiency and type 2 diabetes using long acting testosterone injections over 30 weeks. They found patients had improvements in most sexual function areas, including orgasm (based on the orgasm domain of the International Index of Erectile Function questionnaire 5.7±4. vs 4±4,).
Corona et al 62 performed a meta-analysis examining studies about testosterone supplementation and sexual function. Data was available on the effect of testosterone supplementation on orgasmic function in 10 studies totaling 677 patients. They identified an inverse relationship between testosterone levels and the influence treatment caused on the orgasm domain of the International Index of Erectile Function. The mean difference in the International Index of Erectile Function orgasm function domain between the treatment groups and placebo was 1.62.
- Nolen-Hoeksema, Susan (2014). Abnormal Psychology Sixth Edition. New York, NY: McGraw-Hill Education. p. 368. ISBN 978-0-07-803538-8.[↩]
- Alwaal A, Breyer BN, Lue TF. Normal male sexual function: emphasis on orgasm and ejaculation. Fertility and sterility. 2015;104(5):1051-1060. doi:10.1016/j.fertnstert.2015.08.033. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4896089/[↩][↩][↩][↩][↩][↩]
- Brindley, G. S.; Gillan, P. (1982). “Men and women who do not have orgasms”. The British Journal of Psychiatry. 140 (4): 351. doi:10.1192/bjp.140.4.351. http://bjp.rcpsych.org/content/140/4/351[↩]
- Capogrosso P, Ventimiglia E, Cazzaniga W, Montorsi F, Salonia A. Orgasmic Dysfunction after Radical Prostatectomy. The World Journal of Men’s Health. 2017;35(1):1-13. doi:10.5534/wjmh.2017.35.1.1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5419114[↩]
- Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M, et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2017;71:618–629. https://www.ncbi.nlm.nih.gov/pubmed/27568654[↩]
- Ficarra V, Novara G, Ahlering TE, Costello A, Eastham JA, Graefen M, et al. Systematic review and meta-analysis of studies reporting potency rates after robot-assisted radical prostatectomy. Eur Urol. 2012;62:418–430. https://www.ncbi.nlm.nih.gov/pubmed/22749850[↩]
- Frey AU, Sønksen J, Fode M. Neglected side effects after radical prostatectomy: a systematic review. J Sex Med. 2014;11:374–385. https://www.ncbi.nlm.nih.gov/pubmed/24267516[↩][↩][↩][↩][↩]
- Salonia A, Burnett AL, Graefen M, Hatzimouratidis K, Montorsi F, Mulhall JP, et al. Prevention and management of postprostatectomy sexual dysfunctions part 2: recovery and preservation of erectile function, sexual desire, and orgasmic function. Eur Urol. 2012;62:273–286. https://www.ncbi.nlm.nih.gov/pubmed/22575910[↩]
- Manassero F, Di Paola G, Paperini D, Mogorovich A, Pistolesi D, Valent F, et al. Orgasm-associated incontinence (climacturia) after bladder neck-sparing radical prostatectomy: clinical and video-urodynamic evaluation. J Sex Med. 2012;9:2150–2156. https://www.ncbi.nlm.nih.gov/pubmed/22759835[↩][↩]
- Montorsi F, Adaikan G, Becher E, Giuliano F, Khoury S, Lue TF, et al. Summary of the recommendations on sexual dysfunctions in men. J Sex Med. 2010;7:3572–3588. https://www.ncbi.nlm.nih.gov/pubmed/21040491[↩]
- Georgiadis JR, Reinders AA, Paans AM, Renken R, Kortekaas R. Men versus women on sexual brain function: prominent differences during tactile genital stimulation, but not during orgasm. Hum Brain Mapp. 2009;30:3089–101. https://www.ncbi.nlm.nih.gov/pubmed/19219848[↩]
- Masters WH, Johnson VE. Human sexual inadequacy. London: Churchill; 1970. [↩]
- Messaoudi R, Menard J, Ripert T, Parquet H, Staerman F. Erectile dysfunction and sexual health after radical prostatectomy: impact of sexual motivation. Int J Impot Res. 2011;23:81–86. https://www.ncbi.nlm.nih.gov/pubmed/21471982[↩]
- Capogrosso P, Ventimiglia E, Serino A, Stabile A, Boeri L, Gandaglia G, et al. Orgasmic dysfunction after robot-assisted versus open radical prostatectomy. Eur Urol. 2016;70:223–226. https://www.ncbi.nlm.nih.gov/pubmed/26572706[↩]
- Dubbelman Y, Wildhagen M, Schröder F, Bangma C, Dohle G. Orgasmic dysfunction after open radical prostatectomy: clinical correlates and prognostic factors. J Sex Med. 2010;7:1216–1223. https://www.ncbi.nlm.nih.gov/pubmed/19912504[↩]
- Capogrosso P, Ventimiglia E, Cazzaniga W, Montorsi F, Salonia A. Orgasmic Dysfunction after Radical Prostatectomy. The World Journal of Men’s Health. 2017;35(1):1-13. doi:10.5534/wjmh.2017.35.1.1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5419114/[↩]
- American Psychiatric A, American Psychiatric A, Force DSMT. Diagnostic and statistical manual of mental disorders : DSM-5. 2013[↩][↩][↩][↩][↩]
- Retarded ejaculation in men: an overview of psychological and neurobiological insights. Waldinger MD, Schweitzer DH. World J Urol. 2005 Jun; 23(2):76-81. https://www.ncbi.nlm.nih.gov/pubmed/15937707/[↩]
- Masters WH, Johnson VE. Human sexual inadequacy. London: Churchill; 1970.[↩]
- Leiblum SR, Rosen R. Principles and practice of sex therapy. 3. New York: Guilford Press; 2000.[↩]
- Perelman MA, Rowland DL. Retarded ejaculation. World journal of urology. 2006;24:645–52. https://www.ncbi.nlm.nih.gov/pubmed/17082938[↩]
- Carani C, Isidori AM, Granata A, Carosa E, Maggi M, Lenzi A, et al. Multicenter study on the prevalence of sexual symptoms in male hypo- and hyperthyroid patients. The Journal of clinical endocrinology and metabolism. 2005;90:6472–9. https://www.ncbi.nlm.nih.gov/pubmed/16204360[↩][↩]
- Rowland D, McMahon CG, Abdo C, Chen J, Jannini E, Waldinger MD, et al. Disorders of orgasm and ejaculation in men. J Sex Med. 2010;7:1668–1686. https://www.ncbi.nlm.nih.gov/pubmed/20388164[↩]
- Althof SE, McMahon CG. Contemporary management of disorders of male orgasm and ejaculation. Urology. 2016;93:9–21. https://www.ncbi.nlm.nih.gov/pubmed/26921646[↩][↩][↩]
- Holstege G, Georgiadis JR, Paans AM, Meiners LC, van der Graaf FH, Reinders AA. Brain activation during human male ejaculation. J Neurosci. 2003;23:9185–9193. http://www.jneurosci.org/content/23/27/9185.long[↩]
- Waldinger MD, Berendsen HH, Blok BF, Olivier B, Holstege G. Premature ejaculation and serotonergic antidepressants-induced delayed ejaculation: the involvement of the serotonergic system. Behav Brain Res. 1998;92:111–118. https://www.ncbi.nlm.nih.gov/pubmed/9638953[↩]
- Núñez R, Gross GH, Sachs BD. Origin and central projections of rat dorsal penile nerve: possible direct projection to autonomic and somatic neurons by primary afferents of nonmuscle origin. J Comp Neurol. 1986;247:417–429. https://www.ncbi.nlm.nih.gov/pubmed/3755143[↩]
- Comarr AE. Sexual function among patients with spinal cord injury. Urol Int. 1970;25:134–168. https://www.ncbi.nlm.nih.gov/pubmed/5422714[↩]
- Gerstenberg TC, Levin RJ, Wagner G. Erection and ejaculation in man. Assessment of the electromyographic activity of the bulbocavernosus and ischiocavernosus muscles. Br J Urol. 1990;65:395–402. https://www.ncbi.nlm.nih.gov/pubmed/2340374[↩]
- Corona G. Effect of hyperprolactinemia in male patients consulting for sexual dysfunction. J Sex Med. 2007;4:1485–93. https://www.ncbi.nlm.nih.gov/pubmed/17655655[↩]
- Balercia G. Sexual symptoms in endocrine diseases: psychosomatic perspectives. Psychother Psychosom. 2007;76:134–40. https://www.ncbi.nlm.nih.gov/pubmed/17426412[↩]
- Corona G, Jannini EA, Vignozzi L, Rastrelli G, Maggi M. The hormonal control of ejaculation. Nature reviews Urology. 2012;9:508–19. https://www.ncbi.nlm.nih.gov/pubmed/22869001[↩]
- Van de Kar LD, Bethea CL. Pharmacological evidence that serotonergic stimulation of prolactin secretion is mediated via the dorsal raphe nucleus. Neuroendocrinology. 1982;35:225–30. https://www.ncbi.nlm.nih.gov/pubmed/7145018[↩]
- Giuliano F. Neurophysiology of erection and ejaculation. J Sex Med. 2011;8:310–5. https://www.ncbi.nlm.nih.gov/pubmed/21967393[↩]
- Corona G, Jannini EA, Lotti F, Boddi V, De Vita G, Forti G, et al. Premature and delayed ejaculation: two ends of a single continuum influenced by hormonal milieu. International journal of andrology. 2011;34:41–8. https://www.ncbi.nlm.nih.gov/pubmed/20345874[↩][↩]
- McMahon CG, Jannini E, Waldinger M, Rowland D. Standard operating procedures in the disorders of orgasm and ejaculation. The journal of sexual medicine. 2013;10:204–29. https://www.ncbi.nlm.nih.gov/pubmed/22970767[↩][↩][↩]
- Abdel-Hamid IA, Saleh el S. Primary lifelong delayed ejaculation: characteristics and response to bupropion. The journal of sexual medicine. 2011;8:1772–9. https://www.ncbi.nlm.nih.gov/pubmed/21114770[↩][↩]
- Xia JD, Han YF, Pan F, Zhou LH, Chen Y, Dai YT. Clinical characteristics and penile afferent neuronal function in patients with primary delayed ejaculation. Andrology. 2013;1:787–92. https://www.ncbi.nlm.nih.gov/pubmed/23970455[↩]
- Johnson RD, Murray FT. Reduced sensitivity of penile mechanoreceptors in aging rats with sexual dysfunction. Brain Res Bull. 1992;28:61–4. https://www.ncbi.nlm.nih.gov/pubmed/1540846[↩]
- Rowland DL. Penile sensitivity in men: a composite of recent findings. Urology. 1998;52:1101–5. https://www.ncbi.nlm.nih.gov/pubmed/9836563[↩]
- Shull GR, Sprenkle DH. Retarded ejaculation reconceptualization and implications for treatment. J Sex Marital Ther. 1980;6:234–46. https://www.ncbi.nlm.nih.gov/pubmed/6152867[↩]
- Waldinger MD, Schweitzer DH. Retarded ejaculation in men: an overview of psychological and neurobiological insights. World journal of urology. 2005;23:76–81. https://www.ncbi.nlm.nih.gov/pubmed/15937707[↩]
- Perelman MA. Regarding ejaculation, delayed and otherwise. Journal of andrology. 2003;24:496. https://www.ncbi.nlm.nih.gov/pubmed/12826687[↩]
- Rowland DL. Psychophysiology of ejaculatory function and dysfunction. World journal of urology. 2005;23:82–8. https://www.ncbi.nlm.nih.gov/pubmed/15883812[↩]
- Byun JS, Lyu SW, Seok HH, Kim WJ, Shim SH, Bak CW. Sexual dysfunctions induced by stress of timed intercourse and medical treatment. BJU international. 2013;111:E227–34. https://www.ncbi.nlm.nih.gov/pubmed/23107357[↩]
- Kirby ED, Geraghty AC, Ubuka T, Bentley GE, Kaufer D. Stress increases putative gonadotropin inhibitory hormone and decreases luteinizing hormone in male rats. Proceedings of the National Academy of Sciences of the United States of America. 2009;106:11324–9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2698887/[↩]
- Corona G, Ricca V, Bandini E, Mannucci E, Lotti F, Boddi V, et al. Selective serotonin reuptake inhibitor-induced sexual dysfunction. The journal of sexual medicine. 2009;6:1259–69. https://www.ncbi.nlm.nih.gov/pubmed/19473282[↩]
- Clayton AH, Croft HA, Horrigan JP, Wightman DS, Krishen A, Richard NE, et al. Bupropion extended release compared with escitalopram: effects on sexual functioning and antidepressant efficacy in 2 randomized, double-blind, placebo-controlled studies. J Clin Psychiatry. 2006;67:736–46. https://www.ncbi.nlm.nih.gov/pubmed/16841623[↩]
- Teloken P, Nelson C, Mulhall J. 1384 SECONDARY DELAYED ORGASM: PATTERNS, CORRELATES AND PREDICTORS. The Journal of urology. 2012;187:e562.[↩]
- Jenkins LC, Mulhall JP. Delayed Orgasm and Anorgasmia. Fertility and sterility. 2015;104(5):1082-1088. doi:10.1016/j.fertnstert.2015.09.029. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4816679/[↩]
- SEXUAL MEDICINE Sexual Dysfunctions in Men and Women. 2010 ed: International Consultation on Urological Diseases. International Society for Sexual Medicine; 2010.[↩][↩]
- Standard operating procedures in the disorders of orgasm and ejaculation. McMahon CG, Jannini E, Waldinger M, Rowland D. J Sex Med. 2013 Jan; 10(1):204-29. https://www.ncbi.nlm.nih.gov/pubmed/22970767/[↩]
- Althof SE. Psychological interventions for delayed ejaculation/orgasm. International journal of impotence research. 2012;24:131–6. https://www.ncbi.nlm.nih.gov/pubmed/22378496[↩]
- McMahon CG, Jannini E, Waldinger M, Rowland D. Standard operating procedures in the disorders of orgasm and ejaculation. The journal of sexual medicine. 2013;10:204–29 https://www.ncbi.nlm.nih.gov/pubmed/22970767[↩]
- Ashton AK, Hamer R, Rosen RC. Serotonin reuptake inhibitor-induced sexual dysfunction and its treatment: a large-scale retrospective study of 596 psychiatric outpatients. J Sex Marital Ther. 1997;23:165–75. https://www.ncbi.nlm.nih.gov/pubmed/9292832[↩][↩]
- Adeniyi AA, Brindley GS, Pryor JP, Ralph DJ. Yohimbine in the treatment of orgasmic dysfunction. Asian journal of andrology. 2007;9:403–7. https://www.ncbi.nlm.nih.gov/pubmed/17486282[↩][↩]
- Ishak WW, Berman DS, Peters A. Male anorgasmia treated with oxytocin. The journal of sexual medicine. 2008;5:1022–4. https://www.ncbi.nlm.nih.gov/pubmed/18086171[↩]
- Rodriguez-Manzo G, Canseco-Alba A. Anandamide reduces the ejaculatory threshold of sexually sluggish male rats: possible relevance for human lifelong delayed ejaculation disorder. The journal of sexual medicine. 2015;12:1128–35. https://www.ncbi.nlm.nih.gov/pubmed/25808995[↩]
- Nickel M, Moleda D, Loew T, Rother W, Pedrosa Gil F. Cabergoline treatment in men with psychogenic erectile dysfunction: a randomized, double-blind, placebo-controlled study. International journal of impotence research. 2007;19:104–7 https://www.ncbi.nlm.nih.gov/pubmed/16728967[↩]
- Corona G. Different testosterone levels are associated with ejaculatory dysfunction. J Sex Med. 2008;5:1991–8. https://www.ncbi.nlm.nih.gov/pubmed/18399946[↩]
- Hackett G, Cole N, Bhartia M, Kennedy D, Raju J, Wilkinson P. Testosterone replacement therapy with long-acting testosterone undecanoate improves sexual function and quality-of-life parameters vs. placebo in a population of men with type 2 diabetes. The journal of sexual medicine. 2013;10:1612–27. https://www.ncbi.nlm.nih.gov/pubmed/23551886[↩]
- Corona G, Isidori AM, Buvat J, Aversa A, Rastrelli G, Hackett G, et al. Testosterone supplementation and sexual function: a meta-analysis study. The journal of sexual medicine. 2014;11:1577–92. https://www.ncbi.nlm.nih.gov/pubmed/24697970[↩]





{kind=link}