
Contents
- What are antibiotics
- What are bacteria and viruses?
- Antibiotic resistance
- Do I need antibiotics for a common cold or the flu?
- When are antibiotics used?
- Principles of antibiotic prescribing
- How do antibiotics work
- Types of antibiotics
- Amoxicillin antibiotic
- Who can and can’t take amoxicillin
- How and when to take amoxicillin
- Amoxicillin side effects
- Will amoxicillin affect my contraception?
- Will amoxicillin affect my fertility?
- Will amoxicillin give me thrush?
- Does amoxicillin stain teeth?
- Is there any food or drink I need to avoid?
- Can I drive or ride a bike while taking amoxicillin?
- Sulfonamide antibiotics
- MRSA antibiotics
- Important things to consider before taking antibiotics
- Penicillin
- Cephalosporins
- Aminoglycosides
- Tetracyclines
- Macrolides
- Fluoroquinolones
- Is it safe to take antibiotics during pregnancy?
- Amoxicillin antibiotic
- The best way to take antibiotics
- Antibiotic Interactions
- Side effects of antibiotics
What are antibiotics
Antibiotics are powerful medicines used to treat a wide variety of infections or diseases caused by bacteria, such as respiratory tract infections (e.g., pneumonia and whooping cough), urinary tract infections, skin infections and infected wounds or prevent some types of bacterial infection. Used properly, antibiotics can save lives. Antibiotics only work on bacteria, not other infections like viruses that cause colds, flu, most sore throats, most coughs and bronchitis and runny noses. Antibiotics damage bacteria so your body’s immune system can fight them. Antibiotics have revolutionized medicine and saved millions of lives following their introduction in the 1940s because they provided a means of treating many infectious diseases and bacterial infections, including serious infections like meningitis and bacterial sepsis or septicemia. Antibiotics work by killing bacteria or preventing them from reproducing and spreading. But they don’t work against viruses. For example, antibiotics don’t work for viral infections such as common colds and flu, and most coughs and sore throats. And many mild bacterial infections also get better on their own without using antibiotics. Taking an antibiotic when it’s not needed will not make a significant difference to how you feel or how fast you recover. When you start to feel better it’s usually because your immune system is doing the work to treat your infection
Taking antibiotics when you don’t need them can put you and your family at risk of a longer and more severe illness.
Antibiotics are used to treat or prevent some types of bacterial infections. They aren’t effective against viral infections, such as the common cold or flu.
Other common viral infections that don’t benefit from antibiotic treatment include:
- Cold
- Flu (influenza)
- Bronchitis
- Most coughs
- Some ear infections
- Some sinus infections
- Stomach flu
Taking an antibiotic for a viral infection:
- Won’t cure the infection
- Won’t keep other people from getting sick
- Won’t help you or your child feel better
- May cause unnecessary and harmful side effects
- Promotes antibiotic resistance
If you take an antibiotic when you actually have a viral infection, the antibiotic attacks bacteria in your body — bacteria that are either beneficial or at least not causing disease. This misdirected treatment can then promote antibiotic-resistant properties in harmless bacteria that can be shared with other bacteria, or create an opportunity for potentially harmful bacteria to replace the harmless ones.
Taking antibiotics when you have a virus may do more harm than good 1:
- Taking antibiotics increases your risk of getting an antibiotic-resistant infection later.
- Antibiotics kill the healthy bacteria in the gut, allowing more harmful bacteria, such as C. difficile, to grow in its place.
- Although this infection is more commonly found in hospitals, it also occurs in clinics outside of the hospital. Read more about C. difficile.
- Antibiotics cause 1 out of 5 emergency department visits for adverse drug events.
- Antibiotics are the most common cause of emergency department visits for adverse drug events in children under 18 years of age.
It’s important to only take antibiotics for bacterial infections since they can put you or your child at risk for harmful side effects and antibiotic-resistant infections.
Antibiotics should only be prescribed to treat conditions:
- that aren’t especially serious but are unlikely to clear up without the use of antibiotics – such as moderately severe acne
- that aren’t especially serious but could spread to other people if not promptly treated – such as the skin infection impetigo or the sexually transmitted infection chlamydia
- where evidence suggests that antibiotics could significantly speed up recovery – such as a kidney infection
- that carry a risk of more serious complications – such as cellulitis or pneumonia
Table 1. Antibiotic Prescribing and Use in Doctor’s Offices
| Common Condition: What’s got you sick? | Common Cause Bacteria | Common Cause Bacteria or Virus | Common Cause Virus | Are antibiotics needed? |
|---|---|---|---|---|
| Strep throat | ✔ | Yes | ||
| Whooping cough | ✔ | Yes | ||
| Urinary tract infection | ✔ | Yes | ||
| Sinus infection | ✔ | Maybe | ||
| Middle ear infection | ✔ | Maybe | ||
| Bronchitis/chest cold (in otherwise healthy children and adults)* | ✔ | No | ||
| Common cold/runny nose | ✔ | No | ||
| Sore throat (except strep) | ✔ | No | ||
| Flu | ✔ | No |
Different antibiotics work against different bacteria. Sometimes, doctors choose an antibiotic based on what they believe will work. At other times, doctors will perform tests (e.g. culture and sensitivity) to work out which bacteria are causing the infection, and which antibiotics are likely to be effective against them.
Many antibiotics are less effective than they once were due to bacteria becoming resistive to their effects. This is called antibiotic resistance which may be prevented by only using antibiotics if they are needed to treat a bacterial infection.
How does a physician decide which antibiotic to prescribe?
Physicians examine patients and consider their symptoms in order to tell if they should prescribe an antibiotic and, if so, which one. Physicians can also take a culture to see if bacteria are causing a particular illness, such as a throat culture to determine the presence of “strep throat.” For hospital infections and some community-acquired infections, the doctor will obtain an “antimicrobial susceptibility report” that indicates which families of antibiotic drugs are useful for the particular bacteria recovered from the infection. If the cause of the infection is unclear, but suspected to be due to bacteria, the doctor may prescribe a broad-spectrum antibiotic that is useful for controlling a wide variety of bacterial types. The physician may choose either a generic or trade-name (non-generic) antibiotic depending on the individual circumstances.
What are bacteria and viruses?
Many human infections are caused by either bacteria or viruses. Bacteria are tiny single-celled organisms, thought by some researchers to be related to plants. They are among the most successful life forms on the planet, and range in habitat from ice slopes to deserts.
Bacteria can be beneficial – for instance, gut bacteria help you to digest food – but some are responsible for a range of infections. These disease-causing varieties are called pathogenic bacteria. Many bacterial infections can be treated successfully with appropriate antibiotics, although antibiotic-resistant strains are beginning to emerge. Vaccination is available to prevent many important bacterial diseases.
A virus is an even smaller micro-organism that can only reproduce inside a host’s living cell. It is very difficult to kill a virus. That’s why some of the most serious communicable diseases known to medical science are viral in origin.
To cause disease, pathogenic bacteria must gain access into the body. The range of access routes for bacteria includes:
- Cuts
- Contaminated food or water
- Close contact with an infected person
- Contact with the faces of an infected person
- Breathing in the exhaled droplets when an infected person coughs or sneezes
- Indirectly, by touching contaminated surfaces – such as taps, toilet handles, toys and nappies.
Viruses are spread from one person to another by:
- Coughs
- Sneezes
- Vomits
- Bites from infected animals or insects
- Exposure to infected bodily fluids through activities such as sexual intercourse or sharing hypodermic needles.
Forgetting to wash your hands after handling pets and animals is another way for germs to be taken in by mouth.
Characteristics of the bacterium
Most bacteria, apart from the cocci variety, move around with the aid of small lashing tails (flagella) or by whipping their bodies from side to side. Under the right conditions, a bacterium reproduces by dividing in two. Each ‘daughter’ cell then divides in two and so on, so that a single bacterium can bloom into a population of some 500,000 or more within just eight hours.
If the environmental conditions don’t suit the bacteria, some varieties morph into a dormant state. They develop a tough outer coating and await the appropriate change of conditions. These hibernating bacteria are called spores. Spores are harder to kill than active bacteria because of their outer coating.
Bacteria types
Bacteria that cause disease are broadly classified according to their shape.
The four main groups include:
- Bacilli – shaped like a rod with a length of around 0.03mm. Illnesses such as typhoid and cystitis are caused by bacilli strains.
- Cocci – shaped like a sphere with a diameter of around 0.001mm. Depending on the sort, cocci bacteria group themselves in a range of ways, such as in pairs, long lines or tight clusters. Examples include Staphylococci (which cause a host of infections including boils) and Gonococci (which cause the sexually transmissible infection gonorrhea).
- Spirochetes – as the name suggests, these bacteria are shaped like tiny spirals. Spirochetes bacteria are responsible for a range of diseases, including the sexually transmissible infection syphilis.
- Vibrio – shaped like a comma. The tropical disease cholera, characterized by severe diarrhea and dehydration, is caused by the vibrio bacteria.
Curing a bacterial infection
The body reacts to disease-causing bacteria by increasing local blood flow (inflammation) and sending in cells from the immune system to attack and destroy the bacteria. Antibodies produced by the immune system attach to the bacteria and help in their destruction. They may also inactivate toxins produced by particular pathogens, for example tetanus and diphtheria.
Serious infections can be treated with antibiotics, which work by disrupting the bacterium’s metabolic processes, although antibiotic-resistant strains are starting to emerge. Immunization is available to prevent many important bacterial diseases such as Hemophilus influenza Type b (Hib), tetanus and whooping cough.
Virus types
A virus is a miniscule pocket of protein that contains genetic material. If you placed a virus next to a bacterium, the virus would be dwarfed. For example, the polio virus is around 50 times smaller than a Streptococci bacterium, which itself is only 0.003mm long. Viruses can be described as either RNA or DNA viruses, according to which type of nucleic acid forms their core.
The four main types of virus include:
- Icosahedral – the outer shell (capsid) is made from 20 flat sides, which gives a spherical shape. Most viruses are icosahedral.
- Helical – the capsid is shaped like a rod.
- Enveloped – the capsid is encased in a baggy membrane, which can change shape but often appears spherical.
- Complex – the genetic material is coated, but without a capsid.
The body’s response to viral infection
Viruses pose a considerable challenge to the body’s immune system because they hide inside cells. This makes it difficult for antibodies to reach them. Some special immune system cells, called T-lymphocytes, can recognize and kill cells containing viruses, since the surface of infected cells is changed when the virus begins to multiply. Many viruses, when released from infected cells, will be effectively knocked out by antibodies that have been produced in response to infection or previous immunization.
Antibiotics are useless against viral infections. This is because viruses are so simple that they use their host cells to perform their activities for them. So antiviral drugs work differently to antibiotics, by interfering with the viral enzymes instead.
The treatment of viral infections can include:
- managing symptoms, such as honey for coughs and warm fluids like chicken soup for oral hydration
- paracetamol to relieve fever
- stopping viral reproduction using antiviral medicines, such as medicines for HIV/AIDS and cold sores
- preventing infection in the first place, such as vaccines for flu and hepatitis
Antiviral drugs are currently only effective against a few viral diseases, such as influenza, herpes, hepatitis B and C and HIV – but research is ongoing. A naturally occurring protein, called interferon (which the body produces to help fight viral infections), can now be produced in the laboratory and is used to treat hepatitis C infections.
Vaccination against viral infection is not always possible
It is possible to vaccinate against many serious viral infections such as measles, mumps, hepatitis A and hepatitis B. An aggressive worldwide vaccination campaign, headed by the World Health Organization (WHO), managed to wipe out smallpox. However, some viruses – such as those that cause the common cold – are capable of mutating from one person to the next. This is how an infection with essentially the same virus can keep dodging the immune system. Vaccination for these kinds of viruses is difficult, because the viruses have already changed their format by the time vaccines are developed.
Antibiotic resistance
Many bacterial infections are treated with antibiotics. Sometimes the bacteria change to protect themselves against the antibiotic. When this happens the antibiotic no longer works. This is called antibiotic resistance and is a serious global problem.
Bacteria become antibiotic resistant when their genes mutate after being in contact with an antibiotic. These changes allow the bacteria to survive or ‘resist’ the antibiotic, so that the antibiotic no longer works to kill the bacteria or stop them from multiplying.
As more antibiotics stop working against bacterial infections, doctors will have fewer antibiotics to use. Many common infections may eventually become untreatable with antibiotic medicines.
- The World Health Organization (WHO) has warned that antibiotic resistance is one of the greatest threats to global public health today.
- Approximately 2 million infections from antibiotic-resistant bacteria occur in the United States each year, resulting in 23,000 deaths.
- Other consequences of medication-resistant infections include:
- More-serious illness
- Longer recovery
- More-frequent or longer hospitalization
- More doctor visits
- More-expensive treatments
In the last 50 years only one antibiotic that works in a new way has been discovered and developed for use in humans.
In 2015, media reported the discovery of a new class of antibiotics, called teixobactin, as a “breakthrough” and a “game-changer”. However the new antibiotic has not yet even been tested in people. So far it has only been shown to be toxic to bacteria in mice. It will likely be years before it becomes a viable option in humans.
This new antibiotic only works on certain types of bacteria (gram-positive)—so it would help for some of the currently hard-to-treat infections, but not all.
For example, it is not effective against E coli (as that is gram-negative) which can be resistant to antibiotics.
The time it is taking for bacteria to become resistant to new antibiotics is getting shorter, so even if new antibiotics are discovered, this will likely become an issue again if we don’t change the way we use antibiotics.
Antibiotic resistance is already affecting individuals in the community.
Infection with antibiotic-resistant bacteria is associated with longer stays in hospital and a higher death rate. In America like other developed countries, the prevalence of multi-resistant bacteria (also known as ‘superbugs’) is increasing, and more patients are getting staph infections that are resistant to multiple antibiotics.
If you have an infection that is caused by bacteria which is resistant to antibiotics you are more likely to die from that infection.
Examples of bacteria in the community that have already developed resistance to a number of antibiotics include strains of Escherichia coli (E coli) that cause many urinary tract infections. ‘Golden staph’, a common cause of skin infections, is another example.
Failure of the last-resort antibiotic treatment for the sexually transmitted infection gonorrhea has occurred in the US.
How do bacteria develop antibiotic resistance?
Bacteria can change their genes after being exposed to an antibiotic. This allows them to survive antibiotic treatment. Then, when they multiply, they make more resistant bacteria. This is how antibiotic resistance develops.
Furthermore, bacteria can also develop antibiotic resistance through contact with other bacteria. Resistant bacteria can pass their genes to other bacteria, forming a new antibiotic-resistant ‘strain’ of the bacteria.
The more antibiotics are used, the more chances bacteria have to become resistant to them.
Why is antibiotic resistance a problem?
Antibiotic resistance happens when bacteria survive and continue causing infection despite treatment with an antibiotic – the bacteria are no longer sensitive to that antibiotic.
What does antibiotic resistance mean for me?
Using antibiotics when you don’t need them may mean that they won’t work for you when you do need them in the future.
If you or a member of your family develop an antibiotic-resistant infection:
- you will have the infection for longer
- you may be more likely to have complications of the infection
- you could remain infectious for longer, and pass your infection to other people, which increases the problem.
You could be passing it on
You could be passing on antibiotic-resistant bacteria to other people:
- if you take antibiotics for cold and flu viruses
- if you don’t take antibiotics as prescribed
- if you neglect good hygiene.
Antibiotic resistance can have personal consequences for you, your family and the community
Antibiotic-resistant bacteria can persist in your body for as long as 12 months and may be passed on to family members or others in the community.
Because the antibiotic no longer works against the resistant bacteria:
- infections take longer to heal
- infections can get worse and lead to more serious problems
- infections are more likely to spread to other people and because bacteria are resistant, the antibiotic may not work for other people, further spreading the problem
You might think it best to use another antibiotic to which bacteria aren’t resistant. However, it may not work as well, and it could have side effects. Also, bacteria may eventually become resistant to this antibiotic too.
For these reasons, antibiotic resistance is a major threat to human health. There is concern that in time, there will be bacterial infections that just can’t be treated with all the currently available antibiotics.
What causes antibiotic resistance?
The more bacteria are exposed to antibiotics, the more chances they have to change and become resistant. When you use antibiotics when not needed or don’t take antibiotics properly – such as missing doses or not completing the course – you give bacteria opportunities to become resistant.
How can I help prevent antibiotic resistance?
Antibiotic resistance can’t be totally stopped, but it can be slowed down by sensibly using antibiotics. You can help by:
- not taking antibiotics for a cold or the flu, including cough and sore throat; viruses cause most colds, and antibiotics don’t work against viruses
- telling your doctor you only want antibiotics when necessary – such as for serious bacterial infections such as pneumonia
- taking your antibiotic as prescribed, and completing the full course
- never saving antibiotics for the next time you’re sick
- never taking antibiotics prescribed for someone else
- having good hygiene practices to avoid spreading infections
Sharing antibiotics and using leftovers can increase antibiotic resistance
When bacteria encounter an antibiotic, they adapt to protect themselves.
There are actions that you can take to reduce the chance of resistance developing.
- Take the prescribed dose and complete the whole course of treatment prescribed by your doctor. Even if you are feeling better, taking the whole course reduces the chance that some bacteria will survive and become resistant.
- Don’t share antibiotics with another person. This is important because the type of antibiotic may not be targeted to the bacteria causing their particular infection.
- Don’t keep leftovers. The dose and amount leftover may not be enough to destroy a new infection – creating more opportunity for resistant bacteria to develop and multiply.
What are ‘superbugs’?
‘Superbugs’ are bacteria that are difficult to treat because they are resistant to several different antibiotics, and especially antibiotics that treat other resistant bacteria.
Superbugs such as Methicillin-Resistant Staphylococcus aureus (MRSA), Clostridium difficile (also known as C. difficile or C. diff, is a bacterium that can infect the bowel and cause diarrhea often bloody diarrhea), the bacteria that cause tuberculosis (Mycobacterium tuberculosis) and multi-drug-resistant strains of Escherichia coli (E. coli) the bacteria that cause many urinary tract infections are becoming more common and are now very hard to treat because of antibiotic resistance and can be a real problem in hospitals.
These types of infections can be serious and challenging to treat, and are becoming an increasing cause of disability and death across the world.
The biggest worry is that new strains of bacteria may emerge that can’t be effectively treated by any existing antibiotics.
Do I need antibiotics for a common cold or the flu?
Good-quality, reliable clinical studies have shown that antibiotics do not improve the symptoms of a cold or the flu. This is because antibiotics work only on infections caused by bacteria – common colds and the flu are infections caused by viruses.
Antibiotics will not:
- help a cold or the flu get better faster
- stop a cold or the flu from getting worse or
- stop a cold or the flu from spreading to other people.
If you are usually healthy and well, your immune system will take care of most respiratory tract infections – both viral and some bacterial infections – by itself.
However, antibiotics are more likely to be needed for people who:
- have serious infections caused by bacteria (e.g., whooping cough)
- have an ongoing health condition (e.g., asthma, diabetes or lung disease)
- are older or in generally poor health, or have a weakened immune system (e.g., due to HIV infection)
- have a higher risk of complications with a respiratory tract infection (complications often include bacterial infections).
Using antibiotics when you don’t need them can contribute to the problem of antibiotic resistance. This might mean that if you have a serious infection, such as pneumonia, in the future, antibiotics may not work as well.
When are antibiotics used?
Antibiotics may be used to treat bacterial infections that:
- are unlikely to clear up without antibiotics
- could infect others unless treated
- could take too long to clear without treatment
- carry a risk of more serious complications
People at a high risk of infection may also be given antibiotics as a precaution, known as antibiotic prophylaxis.
People at risk of bacterial infections
Antibiotics may also be recommended for people who are more vulnerable to the harmful effects of infection. This may include:
- people aged over 75 years
- babies less than 72 hours old with a confirmed bacterial infection, or a higher than average risk of developing one
- people with heart failure
- people who have to take insulin to control their diabetes
- people with a weakened immune system – either because of an underlying health condition such as HIV infection or as a side effect of certain treatments, such as chemotherapy
Principles of antibiotic prescribing
Antibiotics are prescribed for three reasons 3:
- Prophylaxis – where administration of antibiotic is designed to prevent serious infection in a defined at-risk situation
- Empiric therapy – where a clinical syndrome that may be due to infection is managed before evidence confirming the presence of infection or its cause is available
- Directed therapy – where antibiotics are aimed at micro-organisms which have been confirmed as the cause of an infection.
For each type of therapy, there are principles that aim to minimize the use of antibiotics and also ameliorate the selection of antibiotic resistance.
Antibiotic prophylaxis
Antibiotics are sometimes given as a precaution to prevent, rather than treat, an infection. This is known as antibiotic prophylaxis. Prophylactic antibiotic is normally recommended if you’re having surgery on a certain part of the body which carries a high risk of infection or where infection could lead to devastating effects. For example, antibiotic prophylaxis is used for medical (for example, preventing relapses of rheumatic fever, infective endocarditis prevention for certain heart disease or the spread of meningococcal infection) and surgical purposes (prevention of wound infection).
For example, antibiotic prophylaxis may be used if you’re going to have:
- some types of eye surgery – such as cataract surgery or glaucoma surgery
- joint replacement surgery
- breast implant surgery
- pacemaker surgery
- surgery to remove the gall bladder
- surgery to remove the appendix
Your surgical team will be able to tell you if you require antibiotic prophylaxis.
Bites or wounds
Antibiotic prophylaxis may be recommended for a wound that has a high chance of becoming infected – this could be an animal or human bite, for example, or a wound that has come into contact with soil or feces.
Medical conditions
There are several medical conditions that make people particularly vulnerable to infection, making antibiotic prophylaxis necessary.
For example, the spleen plays an important role in filtering out harmful bacteria from the blood. People who have had their spleen removed, people having chemotherapy for cancer, or those with the blood disorder sickle cell anemia, where their spleen doesn’t work properly, should take antibiotics to prevent infection.
In some cases, antibiotic prophylaxis is prescribed for people who experience a recurring infection that’s causing distress or an increased risk of complications, such as:
- cellulitis
- a urinary tract infection
- genital herpes
- rheumatic fever
Recommendations to use antibiotic prophylaxis for a particular type of surgical operation are made after consideration of:
- the incidence of surgical wound infection
- the usual impact of this infection
- the demonstrated effectiveness of antibiotic prophylaxis in preventing these infections (randomized trial evidence).
Reducing bacterial resistance selection by antibiotic prophylaxis
Exposure to antibiotic surgical prophylaxis is often the initial selective pressure placed upon a patient’s bacterial flora on entry to hospital. The flora is modified in such a way as to facilitate colonization (and potential ensuing infection) with more resistant hospital bacteria. In order to minimize this adverse impact and to maximize effectiveness of antibiotic prophylaxis, narrow spectrum drugs should be used for the shortest time possible.
Empiric therapy
Patients often present with symptoms that may be caused by infection. A decision then has to be made about the likely cause of infection and whether it needs drug treatment. On occasions empiric antibiotic therapy is also used to prevent complications arising from a minor infection.
Are antibiotics indicated?
The decision to use antibiotics in a particular clinical situation is complex. It balances the natural history of the disease or syndrome, the potential seriousness of its outcomes, evidence that antibiotics affect these outcomes and the potential adverse effects of antibiotic therapy. Doctors now recognize that antibiotics are a precious resource, crucial to the management of many potentially fatal infections (such as meningitis). In order to actively safeguard future antibiotic effectiveness in these diseases doctors must reduce their reliance on antibiotics for mild or self-limiting conditions in hospitals and the community.
Hospital setting
Difficulties often arise in intensive care units (ICUs) where clinical features are frequently non-specific. For instance, although antibiotics are usually given for lung consolidation in severely ill patients, it is estimated that fewer than 50% of these patients actually have an infective cause for the consolidation 4.
Community setting
Most antibiotics are prescribed for patients with upper respiratory infection (acute otitis media, pharyngitis, sinusitis) and acute bronchitis. These conditions are most often caused by viruses and are of self-limited duration. Randomized trials show antibiotics have limited or no impact. The antibiotic guidelines published by Therapeutic Guidelines 3 place increasing emphasis on effective (non-antibiotic) symptom management, preventative measures such as immunization and where possible, evidence-based selection of subsets of patients that are most likely to benefit from antibiotic therapy. For example, in acute otitis media, children presenting with systemic symptoms such as high fever or vomiting are more likely, than children without these symptoms, to benefit from antibiotic therapy 5. The treatment of otitis media with antibiotics cannot be justified on the grounds of preventing mastoiditis as trial data show that this complication is rare in developed countries (1 per 1000 or less) 6.
Choice of antibiotic
If an antibiotic is indicated, a drug should be chosen that will limit the development of bacterial resistance (Table 2). The choice of drug is influenced by the likely pathogens and local resistance patterns.
Duration of empiric therapy
In hospital, the patient should be reassessed after 24–48 hours of empiric antibiotic therapy to decide whether infection is unlikely (cease therapy) or whether a firm diagnosis can be made (modify therapy as appropriate (see also Table 2). In community practice, as a general rule, the minimum duration of treatment recommended in Therapeutic Guidelines: Antibiotic 3 should be prescribed.
Table 2. Reducing bacterial resistance selection in empiric treatment with antibiotics
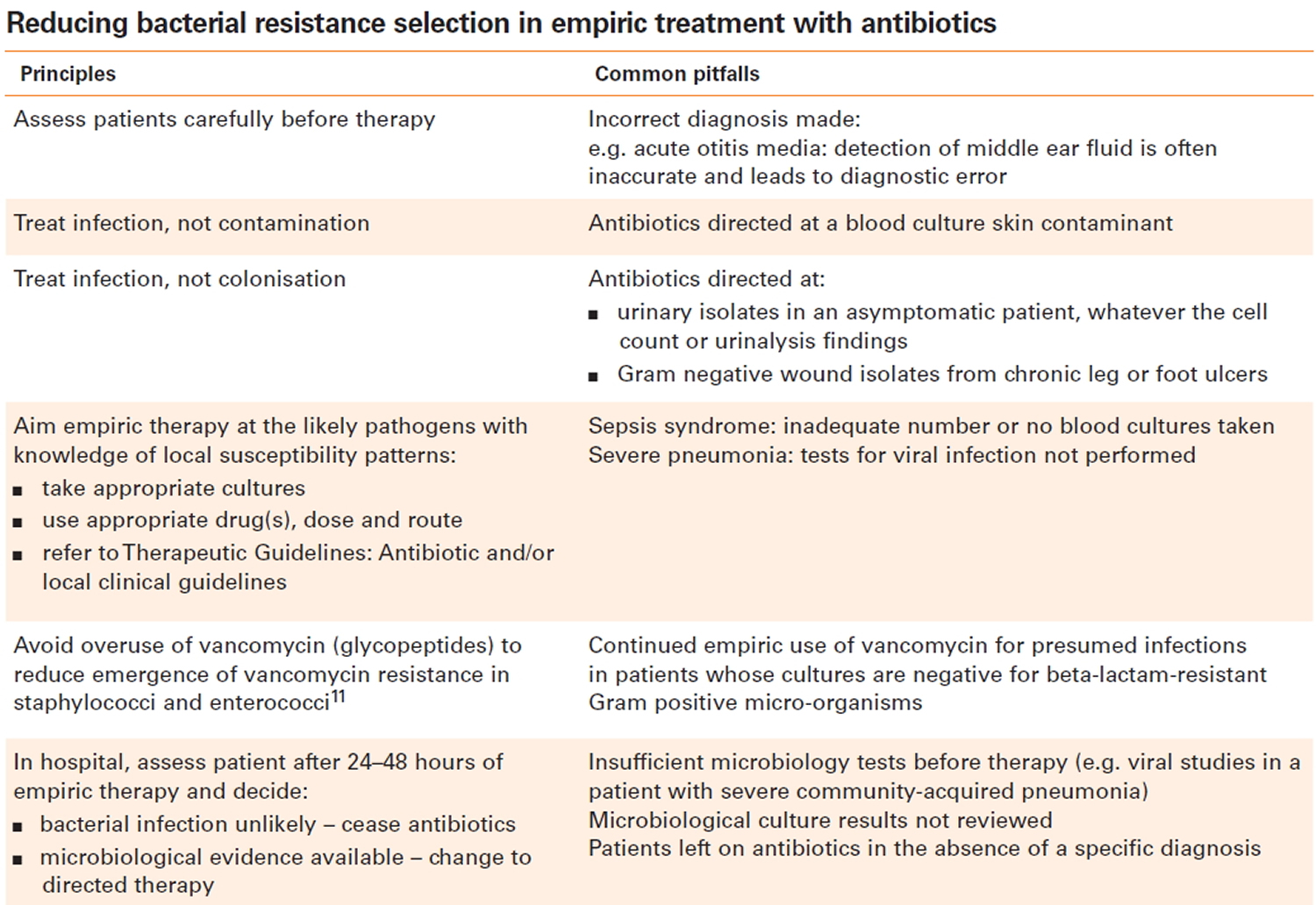
Directed therapy
When the cause of an infection is confirmed, antibiotic therapy is aimed at those micro-organisms. The confirmation may come from clinical or pathological information. Microbiological confirmation is preferred as it gives the greatest assurance that the correct antibiotic drug has been chosen. The involvement of a specific pathogen may be implied by evidence from microscopy, culture or direct detection through nucleic acid amplification (for example, polymerase chain reaction testing for meningococci in blood or cerebrospinal fluid).
Therapeutic Guidelines: Antibiotic 3 provides evidence-based recommendations for directed therapy for common infections. Correct selection of the antibiotic drug, its dosage and route are crucial to minimizing the emergence of resistance during therapy. For instance, the common practice of prescribing prolonged (more than 10 days) monotherapy with oral ciprofloxacin for Pseudomonas aeruginosa respiratory infection usually leads to stable high level ciprofloxacin resistance in this organism. Another common pitfall is the use of oral monotherapy with rifampicin, fusidic acid or ciprofloxacin for infections due to Methicillin-Resistant Staphylococcus aureus (MRSA), as resistance usually emerges during treatment. In both these circumstances, more resistant bacteria are created that frequently cause therapeutic difficulty in the patient or indeed another person who acquires the resistant strain from the treated patient.
Duration of treatment
Appropriate minimum durations of antibiotic therapy have only been investigated for a few infectious diseases. These include bacterial endocarditis, bone and joint disease and meningitis. Unfortunately, duration of therapy for some common sites of infection such as the lung is not well studied. In these situations, the decision to cease therapy is usually based on clinical criteria. Where possible, minimizing the duration of therapy is a key way to reduce emergence of resistance.
How do antibiotics work
Antibiotics work by blocking vital processes in bacteria, killing the bacteria or stopping them from multiplying. This helps the body’s natural immune system to fight the bacterial infection. Different antibiotics work against different types of bacteria.
- Antibiotics that affect a wide range of bacteria are called broad spectrum antibiotics (e.g., amoxicillin and gentamicin).
- Antibiotics that affect only a few types of bacteria are called narrow spectrum antibiotics (e.g., penicillin).
Different types of antibiotics work in different ways. For example, penicillin destroys bacterial cell walls, while other antibiotics can affect the way the bacterial cell works.
Doctors choose an antibiotic according to the bacteria that usually cause a particular infection. Sometimes your doctor will do a test to identify the exact type of bacteria causing your infection and its sensitivity to particular antibiotics.
Antibiotic medicines may contain one or more active ingredients and be available under different brand names. The active ingredient is the chemical in a medicine that makes it work. The medicine label should tell you the active ingredient and the brand name.
Types of antibiotics
There are hundreds of different types of antibiotics, but most of them can be broadly classified into six groups. These are outlined below.
- Penicillins (such as penicillin and amoxicillin) – widely used to treat a variety of infections, including skin infections, chest infections and urinary tract infections
- Cephalosporins (such as cephalexin) – used to treat a wide range of infections, but some are also effective for treating more serious infections, such as septicaemia and meningitis
- Aminoglycosides (such as gentamicin and tobramycin) – tend to only be used in hospital to treat very serious illnesses such as septicaemia, as they can cause serious side effects, including hearing loss and kidney damage; they’re usually given by injection, but may be given as drops for some ear or eye infections
- Tetracyclines (such as tetracycline and doxycycline) – can be used to treat a wide range of infections, but are commonly used to treat moderate to severe acne and rosacea
- Macrolides (such as erythromycin and clarithromycin) – can be particularly useful for treating lung and chest infections, or an alternative for people with a penicillin allergy, or to treat penicillin-resistant strains of bacteria
- Fluoroquinolones (such as ciprofloxacin and levofloxacin) – broad-spectrum antibiotics that can be used to treat a wide range of infections.
Amoxicillin antibiotic
Amoxicillin is an antibiotic that is commonly used to treat bacterial infections, such as chest infections (including pneumonia), dental abscesses and urinary tract infections (UTIs). Amoxicillin is a similar antibiotic to penicillin. It works by killing the bacteria that cause the infection.
Amoxicillin is used in children, often to treat ear infections and chest infections.
Amoxicillin antibiotic is only available on prescription. Amoxicillin comes as capsules or as a liquid that you drink. Amoxicillin is also given by injection, but this is usually only done in hospital.
- For most infections, you’ll start to feel better in a few days. Tell your doctor if you don’t start feeling better after taking amoxicillin for 3 days. Also tell them if, at any time, you start to feel worse.
- Carry on taking this medicine until you’ve completed the course, even if you feel better. If you stop your treatment early, the infection could come back.
- The most common side effects of amoxicillin are feeling sick and diarrhea.
- Liquid amoxicillin can stain your teeth. This doesn’t last and is removed by brushing.
- You can drink alcohol while taking amoxicillin.
Who can and can’t take amoxicillin
Amoxicillin can be taken by adults, including pregnant and breastfeeding women.
Amoxicillin can be taken by children.
Amoxicillin isn’t suitable for some people. To make sure amoxicillin is safe for you, tell your doctor if you:
- have had an allergic reaction to amoxicillin or penicillin or any other medicines in the past
- have liver or kidney problems
- have recently had, or are about to have, any vaccinations
How and when to take amoxicillin
The usual dose of amoxicillin is 250mg to 500mg taken 3 times a day. The dose may be lower for children.
Try to space the doses evenly throughout the day. If you take it 3 times a day, this could be first thing in the morning, mid-afternoon, and at bedtime.
You can take amoxicillin before or after food.
How to take amoxicillin
Swallow amoxicillin capsules whole with a drink of water. Don’t chew or break them.
Amoxicillin is available as a liquid for children and people who find it difficult to swallow tablets.
If you or your child are taking amoxicillin as a liquid, it will usually be made up for you by your pharmacist. The medicine will come with a plastic syringe or spoon to help you measure out the right dose. If you don’t have one, ask your pharmacist for one.
What if I forget to take it?
If you forget to take a dose, take it as soon as you remember, unless it’s nearly time for your next dose. In this case, just leave out the missed dose and take your next dose as normal.
Never take 2 doses at the same time. Never take an extra dose to make up for a forgotten one.
If you forget doses often, it may help to set an alarm to remind you. You could also ask your pharmacist for advice on other ways to remember your medicines.
What if I take too much?
Accidentally taking an extra dose of amoxicillin is unlikely to harm you or your child.
Speak to your pharmacist or doctor if you’re worried or you take more than 1 extra dose.
Amoxicillin side effects
Like all medicines, amoxicillin can cause side effects, although not everyone gets them.
Common side effects
These common side effects happen in around 1 in 10 people. Keep taking the medicine, but talk to your doctor or pharmacist if these side effects bother you or don’t go away:
- feeling sick
- diarrhea
How to cope with side effects
What to do about:
- feeling sick – stick to simple meals and don’t eat rich or spicy food. It might help to take your amoxicillin after a meal or snack.
- diarrhea – drink plenty of water or other fluids if you have diarrhea. It may also help to take oral rehydration solutions, which you can buy from a pharmacy, to prevent dehydration. Don’t take any other medicines to treat diarrhea without speaking to a pharmacist or doctor.
Serious side effects
Serious side effects are rare and happen in less than 1 in 1,000 people.
Tell a doctor straight away if you get:
- severe, bloody diarrhea
- yellowing of the whites of the eyes and skin [jaundice] (warning signs of liver or gallbladder problems)
- a bad skin rash that may include flushing, fever, blisters or ulcers, or skin that looks like it’s been burnt
- bruising or skin discoloration
- joint or muscle pain that comes on after 2 days of taking the medicine
- a skin rash with circular red patches
- dark pee
Some of these serious side effects can happen up to 2 months after finishing the amoxicillin.
Serious allergic reaction
Around 1 in 15 people have an allergic reaction to amoxicillin.
- A serious allergic reaction is an emergency. Call your local emergency number straight away if you think you or someone around you is having a serious allergic reaction.
In most cases, the allergic reaction is mild and can take the form of:
- a raised, itchy skin rash
- coughing
- wheezing
Mild allergic reactions can usually be successfully treated by taking antihistamines.
In rare cases, amoxicillin can cause a serious allergic reaction.
The warning signs of a serious allergic reaction are:
- getting a skin rash that may include itchy, red, swollen, blistered or peeling skin
- wheezing
- tightness in the chest or throat
- having trouble breathing or talking
- swelling of the mouth, face, lips, tongue, or throat
These are not all the side effects of amoxicillin. For a full list see the leaflet inside your medicines packet.
Cautions with other medicines
There are some medicines that don’t mix well with amoxicillin.
Tell your doctor if you’re taking these medicines before you start taking amoxicillin:
- methotrexate
- a blood thinner called warfarin
- gout medicines called probenecid and allopurinol
- other antibiotics
Mixing amoxicillin with herbal remedies and supplements
There are no known problems with taking herbal remedies and supplements alongside amoxicillin.
Will amoxicillin affect my contraception?
Amoxicillin doesn’t stop contraceptive pills working.
However, if amoxicillin makes you vomit or have severe diarrhea (6 to 8 watery poos in 24 hours) for more than 24 hours, your contraceptive pills may not protect you from pregnancy. Look on the pill packet to find out what to do.
Will amoxicillin affect my fertility?
Amoxicillin won’t affect your fertility. However, speak to a pharmacist or your doctor before taking it if you’re trying to get pregnant.
Will amoxicillin give me thrush?
Some people get a fungal infection called thrush after taking a course of antibiotics like amoxicillin. It happens because antibiotics kill the normal harmless bacteria that help to protect you against thrush.
Ask your doctor or pharmacist for advice if this happens to you.
Does amoxicillin stain teeth?
If you or your child take amoxicillin as a liquid medicine, it can stain your teeth. This doesn’t last and should go after brushing your teeth well.
Amoxicillin capsules don’t stain teeth.
Is there any food or drink I need to avoid?
You can eat and drink normally while taking amoxicillin.
Can I drive or ride a bike while taking amoxicillin?
Yes, amoxicillin shouldn’t affect you being able to drive or cycle.
Sulfonamide antibiotics
Sulfonamide antibiotics available on prescription in America include:
- Sulfamethoxazole used in combination with trimethoprim, available as Bactrim, Resprim or Septrin.
- Less commonly used sulfonamide antibiotics include sulfadiazine (tablets, injection or cream), sulfadoxine (for malaria), and sulfacetamide antibiotic eye drops.
- Sulfasalazine (Salazopyrin, Pyralin), used in inflammatory bowel disease or arthritis, is a combination sulfapyridine (a sulfonamide antibiotic) and a salicylate.
If you have had an allergic reaction to Bactrim, Resprim or Septrin, there is no way of knowing whether the allergy was to sulfamethoxazole or to trimethoprim, therefore you should avoid trimethoprim (Alprim, Triprim) as well as sulfonamide antibiotics.
Sometimes those who have had an allergic reaction to a sulfonamide antibiotic are labelled as “sulfur allergic” or allergic to sulfur, sulphur or sulfa. This wording should not be used since it is ambiguous and can cause confusion. Some people wrongly assume that they will be allergic to non-antibiotic sulfonamides or to other sulfur containing medicines or sulfite preservatives.
It is important to know that sulfur is an element which occurs throughout our body as a building block of life, and it is not possible to be allergic to sulfur itself.
Allergic reactions to sulfonamide antibiotics do not increase the likelihood of allergy to sulfur powder, sulfite preservatives, sulfates (in medicines, or soaps and shampoos) or non-antibiotic sulfonamide medicines like some pain killers or fluid tablets or other things that are yellow.
Other types of sulfur containing substances
Elemental sulfur powder
- This is commonly used in gardening, and while irritation may occur from skin contact or inhalation, allergy has not been described.
Sulfates
- Some injectable drugs are sulfate compounds, for example heparin sulfate, dextran sulfate, morphine sulfate. The sulfates in soaps (such as sodium lauryl sulfate) are strong detergents and can irritate the skin or eyes, however sulfate itself does not cause allergic reactions. It is usually safe to use a sulfate when a person has a sulfonamide allergy or a sulfite intolerance.
Sulfite preservatives
- Commonly known as sulfur dioxide and metabisulfites, preservative numbers 220-228, sulfites are a group of compounds used to preserve flavor and color within food, inhibit bacterial growth, reduce spoilage, stop fresh food from spotting and turning brown and help preserve medication and increase shelf life. Sulfites are found most often found in wine, dried fruit, dried vegetables and sometimes sausages and salads. They can also occur naturally in low concentrations. Sulfites can cause adverse reactions which are similar to allergy but do not involve the immune system and are therefore called intolerance. The most common reactions are asthma symptoms (in those with underlying asthma) and rhinitis (hay fever-like) reactions. Occasionally urticaria (hives) may occur, and very rarely, anaphylaxis (allergic shock). There is no relationship between sulfite sensitivity and sulfonamide antibiotic allergy.
Non-antibiotic sulfonamide medicines
- Other medications such as some fluid medicines, diabetes medicines and arthritis medicines contain sulfonamide components but these are not sufficiently similar to sulfonamide antibiotics to pose an allergy risk. These medicines do not need to be avoided by people who are allergic to sulfonamide antibiotics because the allergy rarely if ever cross-reacts.
Those who have had an allergic reaction to one sulfonamide antibiotic are usually advised to avoid all sulfonamide antibiotics. Since these antibiotics are not normally used in an emergency, wearing a MedicAlert bracelet is not routinely recommended although it may be advisable in those who have had life-threatening allergic reactions. Allergy is not always lifelong and cross-reaction does not always occur, therefore challenge with the same or a different sulfonamide antibiotic may be attempted (with caution, under specialist supervision) in those who have a strong indication for a sulfonamide antibiotic, if the allergic reaction was mild/moderate and in the distant past. Desensitisation, to switch off antibiotic allergy temporarily, is available should a sulfonamide antibiotic be the only suitable drug to use, but this is not always possible.
MRSA antibiotics
Evidence-based guidelines for the management of patients with methicillin-resistant Staphylococcus aureus (MRSA) infections were prepared by an Expert Panel of the Infectious Diseases Society of America (IDSA) 7. The guidelines are intended for use by health care providers who care for adult and pediatric patients with MRSA infections 8.
Management of skin and soft-tissue infections
For a cutaneous abscess, incision and drainage is the primary treatment. For simple abscesses or boils, incision and drainage alone is likely to be adequate, but additional data are needed to further define the role of antibiotics, if any, in this setting.
Antibiotic therapy is recommended for abscesses associated with the following conditions: severe or extensive disease (e.g., involving multiple sites of infection) or rapid progression in presence of associated cellulitis, signs and symptoms of systemic illness, associated comorbidities or immunosuppression, extremes of age, abscess in an area difficult to drain (e.g., face, hand, and genitalia), associated septic phlebitis, and lack of response to incision and drainage alone.
For outpatients with purulent cellulitis (e.g., cellulitis associated with purulent drainage or exudate in the absence of a drainable abscess), empirical therapy for community-associated-MRSA is recommended pending culture results. Empirical therapy for infection due to β-hemolytic streptococci is likely to be unnecessary. Five to 10 days of therapy is recommended but should be individualized on the basis of the patient’s clinical response.
For outpatients with nonpurulent cellulitis (eg, cellulitis with no purulent drainage or exudate and no associated abscess), empirical therapy for infection due to β-hemolytic streptococci is recommended. The role of community-associated-MRSA is unknown. Empirical coverage for community-associated-MRSA is recommended in patients who do not respond to β-lactam therapy and may be considered in those with systemic toxicity. Five to 10 days of therapy is recommended but should be individualized on the basis of the patient’s clinical response.
For empirical coverage of community-associated-MRSA in outpatients with skin and soft-tissue infection, oral antibiotic options include the following:
- clindamycin,
- trimethoprim-sulfamethoxazole (bactrim),
- a tetracycline (doxycycline or minocycline) and linezolid.
If coverage for both β-hemolytic streptococci and community-associated-MRSA is desired, options include the following: clindamycin alone or trimethoprim-sulfamethoxazole (bactrim) or a tetracycline in combination with a β-lactam (e.g., amoxicillin) or linezolid alone.
The use of rifampin as a single agent or as adjunctive therapy for the treatment of skin and soft-tissue infection is not recommended.
For hospitalized patients with complicated skin and soft-tissue infection (defined as patients with deeper soft-tissue infections, surgical/traumatic wound infection, major abscesses, cellulitis, and infected ulcers and burns), in addition to surgical debridement and broad-spectrum antibiotics, empirical therapy for MRSA should be considered pending culture data. Options include the following:
- intravenous (IV) vancomycin (A-I), oral (PO) or IV linezolid 600 mg twice daily,
- daptomycin 4 mg/kg/dose IV once daily,
- telavancin 10 mg/kg/dose IV once daily and clindamycin 600 mg IV or PO 3 times a day.
- A β-lactam antibiotic (e.g., cefazolin) may be considered in hospitalized patients with nonpurulent cellulitis with modification to MRSA-active therapy if there is no clinical response. Seven to 14 days of therapy is recommended but should be individualized on the basis of the patient’s clinical response.
Cultures from abscesses and other purulent skin and soft-tissue infections are recommended in patients treated with antibiotic therapy, patients with severe local infection or signs of systemic illness, patients who have not responded adequately to initial treatment, and if there is concern for a cluster or outbreak.
Pediatric considerations
- For children with minor skin infections (such as impetigo) and secondarily infected skin lesions (such as eczema, ulcers, or lacerations), mupirocin 2% topical ointment can be used.
- Tetracyclines should not be used in children <8 years of age.
- In hospitalized children with complicated skin and soft-tissue infection, vancomycin is recommended. If the patient is stable without ongoing bacteremia or intravascular infection, empirical therapy with clindamycin 10–13 mg/kg/dose IV every 6–8 h (to administer 40 mg/kg/day) is an option if the clindamycin resistance rate is low (eg, <10%) with transition to oral therapy if the strain is susceptible. Linezolid 600 mg PO/IV twice daily for children ≥12 years of age and 10 mg/kg/dose PO/IV every 8 h for children <12 years of age is an alternative.
Important things to consider before taking antibiotics
There are some important things to consider before taking antibiotics.
Penicillin
Don’t take one of the penicillin-based antibiotics if you’ve had an allergic reaction to them in the past. People who are allergic to one type of penicillin will be allergic to all of them.
People with a history of allergies, such as asthma, eczema or hay fever, are at higher risk of developing a serious allergic reaction (anaphylaxis) to penicillins, although cases are rare.
Penicillins may need to be used at lower doses and with extra caution if you have:
- severe kidney disease
- liver disease
Pregnancy and breastfeeding
Most penicillins can be used during pregnancy and breastfeeding in the usual doses.
Tell your healthcare professional if you’re pregnant or breastfeeding, so they can prescribe the most suitable antibiotic for you.
Cephalosporins
If you previously had an allergic reaction to penicillin, there’s a chance that you may also be allergic to cephalosporins.
Cephalosporins may not be suitable if you have kidney disease, but if you need one you will probably be given a lower than usual dose.
If you’re pregnant or breastfeeding, or have acute porphyria, check with your doctor, midwife or pharmacist before taking cephalosporins.
Aminoglycosides
Aminoglycosides are normally only used in hospital to treat life-threatening conditions such as septicemia, as they can cause kidney damage in people with pre-existing kidney disease.
They’re only used during pregnancy if your doctor believes they’re essential.
Tetracyclines
The use of tetracyclines isn’t usually recommended unless absolutely necessary in the following groups:
- people with kidney disease – except doxycycline, which can be used
- people with liver disease
- people with the autoimmune condition lupus – which can cause skin problems, joint pain and swelling, and fatigue (feeling tired all the time)
- children under the age of 12
- pregnant or breastfeeding women
Macrolides
You shouldn’t take macrolides if you have porphyria – a rare inherited blood disorder.
If you’re pregnant or breastfeeding, the only type of macrolide you can take is erythromycin (Erymax, Erythrocin, Erythroped or Erythroped A) unless a different antibiotic is recommended by your doctor.
Erythromycin can be used at the usual doses throughout your pregnancy and while you’re breastfeeding.
Other macrolides shouldn’t be used during pregnancy, unless advised by a specialist.
Fluoroquinolones
Fluoroquinolones aren’t normally suitable for women who are pregnant or breastfeeding.
Is it safe to take antibiotics during pregnancy?
Antibiotics are commonly prescribed during pregnancy. The specific medication must be chosen carefully, however. Some antibiotics are OK to take during pregnancy, while others are not. Safety depends on various factors, including the type of antibiotic, when in your pregnancy you take the antibiotic, how much you take, what possible effects it might have on your pregnancy and for how long you’re on antibiotics.
Here’s a sampling of antibiotics generally considered safe during pregnancy:
- Penicillins, including amoxicillin, ampicillin
- Cephalosporins, including cefaclor, cephalexin
- Erythromycin
- Clindamycin
Certain other antibiotics are believed to pose risks during pregnancy. For example, tetracyclines can discolor a developing baby’s teeth. Tetracyclines aren’t recommended for use after the 15th week of pregnancy.
If an antibiotic is the best way to treat your condition, your health care provider will prescribe the safest antibiotic at the safest dosage. If you have questions or concerns about the use of an antibiotic during pregnancy, talk to your health care provider.
The best way to take antibiotics
If you are prescribed antibiotics, it is important that you follow your doctor’s advice on when, how and for how long to take them.
Be medicine wise with antibiotics
- Take your antibiotics at the right time, and for as long as directed on the packet or the patient information leaflet that comes with the medication, or as instructed by your doctor or pharmacist.
- Don’t take more than the dose your doctor has prescribed – sometimes the medicine box may contain more antibiotic pills than you will be instructed to take.
- Don’t keep unused antibiotics for another time – return leftover pills to your pharmacy for disposal.
- Don’t share antibiotics with others – they may have a different infection and this can lead to antibiotic resistance.
Doses of antibiotics can be provided in several ways:
- Oral antibiotics – tablets, capsules or a liquid that you drink, which can be used to treat most types of mild to moderate infections in the body
- Topical antibiotics – creams, lotions, sprays or drops, which are often used to treat skin infections
- Injections of antibiotics – these can be given as an injection or infusion through a drip directly into the blood or muscle, and are usually reserved for more serious infections
It’s essential to finish taking a prescribed course of antibiotics, even if you feel better, unless a healthcare professional tells you otherwise. If you stop taking an antibiotic part way through a course, the bacteria can become resistant to the antibiotic.
Missing a dose of antibiotics
If you forget to take a dose of your antibiotics, take that dose as soon as you remember and then continue to take your course of antibiotics as normal.
But if it’s almost time for the next dose, skip the missed dose and continue your regular dosing schedule. Don’t take a double dose to make up for a missed one.
There’s an increased risk of side effects if you take two doses closer together than recommended.
Accidentally taking an extra dose
Accidentally taking one extra dose of your antibiotic is unlikely to cause you any serious harm.
But it will increase your chances of experiencing side effects, such as pain in your stomach, diarrhea, and feeling or being sick.
Antibiotic Interactions
Some antibiotics aren’t suitable for people with certain medical conditions, or women who are pregnant or breastfeeding. You should only ever take antibiotics prescribed for you – never “borrow” them from a friend or family member.
Some antibiotics can also react unpredictably with other medications, such as the oral contraceptive pill and alcohol. It’s important to read the information leaflet that comes with your medication carefully and discuss any concerns with your pharmacist or doctor.
Antibiotics can sometimes interact with other medicines or substances. This means it can have an effect that is different to what you expected.
Some of the more common interactions are listed below, but this isn’t a complete list.
If you want to check that your medicines are safe to take with your antibiotics, ask your doctor or local pharmacist.
Some antibiotics need to be taken with food, while others need to be taken on an empty stomach. You should always read the patient information leaflet that comes with your medicine.
Antibiotics and alcohol
It’s sensible to avoid drinking alcohol when taking medication or feeling unwell. But it’s unlikely that drinking alcohol in moderation will cause problems if you’re taking most common antibiotics.
To reduce the health risks associated with drinking alcohol, drink alcohol in moderation, if at all. For healthy adults, moderate drinking means up to one drink a day for women and up to two drinks a day for men.
When to avoid drinking alcohol completely
Completely avoid drinking alcohol when taking:
- metronidazole – an antibiotic sometimes used to clear dental or vaginal infections, or to clear infected leg ulcers or pressure sores
- tinidazole – an antibiotic sometimes used to treat many of the same infections as metronidazole, as well as to help clear bacteria called Helicobacter pylori (H. pylori) from the gut
Alcohol can cause a serious reaction when combined with these medications. Symptoms of this reaction can include:
- feeling or being sick
- abdominal pain
- hot flushes
- a fast or irregular heartbeat
- headaches
- dizziness
- drowziness
Because of this risk, you should avoid alcohol while you’re taking these medications. You should continue to avoid alcohol for 48 hours after you stop taking metronidazole and 72 hours after you stop taking tinidazole.
Things like mouthwash and other medicines sometimes contain alcohol, so you should also avoid using these while you’re taking metronidazole or tinidazole.
Other antibiotics that can interact with alcohol
There are some antibiotics that can sometimes interact with alcohol, so you should be wary of drinking alcohol if you’re taking:
- linezolid – linezolid can interact with undistilled (fermented) alcoholic drinks, such as wine, beer, sherry and lager
- doxycycline – this is known to interact with alcohol, and the effectiveness of doxycycline may be reduced in people with a history of chronic alcohol consumption; it should not be taken by people with liver problems
Side effects
Some antibiotics have a variety of side effects, such as causing sickness and dizziness, which might be made worse by drinking alcohol.
It’s best to avoid drinking alcohol while feeling unwell anyway, as the alcohol itself can make you feel worse.
Both metronidazole and tinidazole can cause drowsiness. Check with your pharmacist whether your antibiotic could make you drowsy.
You should not drive or operate machinery if you’re taking an antibiotic that makes you drowsy.
Contraceptives and antibiotics
Rifampicin (Rifadin, Rimycin) and rifabutin (Mycobutin) are the only antibiotics that are thought to affect how well some hormonal contraceptives work. These antibiotics are usually only used to treat serious bacterial infections like tuberculosis and methicillin-resistant Staphylococcus aureus (MRSA), and for preventing meningitis (an infection around the brain or spinal cord).
Ask your health professional for advice as you may need to use extra contraceptive precautions while you are taking rifampicin or rifabutin (and after finishing the prescribed course).
Medications and antibiotics
Some of the medications you may need to avoid, or seek advice on, while taking a specific class of antibiotic are outlined below.
Penicillins
It’s usually recommended that you avoid taking penicillin at the same time as methotrexate, which is used to treat psoriasis, rheumatoid arthritis and some forms of cancer. This is because combining the two medications can cause a range of unpleasant and sometimes serious side effects.
However, some forms of penicillin, such as amoxicillin, can be used in combination with methotrexate.
You may experience a skin rash if you take penicillin and allopurinol, which is used to treat gout.
Cephalosporins
Cephalosporins may increase the chance of bleeding if you’re taking blood-thinning medications (anticoagulants) such as heparin and warfarin.
If you need treatment with cephalosporins, you may need to have your dose of anticoagulants changed or additional blood monitoring.
Aminoglycosides
The risk of damage to your kidneys and hearing is increased if you’re taking one or more of the following medications:
- antifungals – used to treat fungal infections
- cyclosporin – used to treat autoimmune conditions such as Crohn’s disease and given to people who have had an organ transplant
- diuretics – used to remove water from the body
- muscle relaxants
The risk of kidney and hearing damage has to be balanced against the benefits of using aminoglycosides to treat life-threatening conditions such as septicemia.
In hospital, blood levels are carefully monitored to ensure the antibiotic is only present in the blood in safe amounts. If aminoglycosides are used properly in topical preparations, such as ear drops, these side effects don’t occur.
Tetracyclines
You should check with your doctor or pharmacist before taking a tetracycline if you’re currently taking any of the following:
- vitamin A supplements
- retinoids – such as acitretin, isotretinoin and tretinoin, which are used to treat severe acne
- blood-thinning medication
- diuretics
- kaolin-pectin and bismuth subsalicylate – used to treat diarrhea
- medicines to treat diabetes – such as insulin
- atovaquone – used to treat pneumonia
- antacids – used to treat indigestion and heartburn
- sucralfate – used to treat ulcers
- lithium – used to treat bipolar disorder and severe depression
- digoxin – used to treat heart rhythm disorders
- methotrexate
- strontium ranelate – used to treat osteoporosis
- colestipol or colestyramine – used to treat high cholesterol
- ergotamine and methysergide – used to treat migraines
Macrolides
It’s highly recommended that you don’t combine a macrolide with any of the following medications unless directly instructed to by your doctor, as the combination could cause heart problems:
- terfenadine, astemizole and mizolastine – these are all antihistamines used to treat allergic conditions such as hay fever
- amisulpride – used to treat episodes of psychosis
- tolterodine – used to treat urinary incontinence
- statins – used to treat high cholesterol
Fluoroquinolones
You should check with your doctor or pharmacist before taking a fluoroquinolone if you’re currently taking any of the following:
- theophylline – used to treat asthma; also found in some cough and cold medicines
- non-steroidal anti-inflammatory drug (NSAID) painkillers – such as ibuprofen
- ciclosporin
- probenecid – used to treat gout
- clozapine – used to treat schizophrenia
- ropinirole – used to treat Parkinson’s disease
- tizanadine – used to treat muscle spasms
- glibenclamide – used to treat diabetes
- cisapride – used to treat indigestion, heartburn, vomiting or nausea
- tricyclic antidepressants – such as amitriptyline
- steroid medications (corticosteroids)
Some fluoroquinolones can intensify the effects of caffeine (a stimulant found in coffee, tea and cola), which could make you feel irritable, restless and cause problems falling asleep (insomnia).
You may need to avoid taking medication that contains high levels of minerals or iron, as this can block the beneficial effects of fluoroquinolones. This includes:
- antacids
- zinc supplements
- some types of multivitamin supplements.
Side effects of antibiotics
Like all medicines, antibiotics have the potential to cause side effects. When antibiotics are necessary, the benefits far outweigh the risks, but when they are not needed, you are taking an unnecessary risk.
Up to 10% of people taking an antibiotic may experience these common side effects:
- stomach problems like diarrhea, nausea and vomiting
- bloating and indigestion
- abdominal pain
- loss of appetite
- being sick
- feeling sick
- thrush or yeast infections (Candida infection or candidiasis), which can affect the mouth (white patches will be visible) and in women can also occur in the vagina (causing itchiness, pain and discharge called vaginitis).
These side effects are usually mild and should pass once you finish your course of treatment.
Yeast infections affect different parts of the body in different ways:
- Thrush is a yeast infection that causes white patches in your mouth
- Candida esophagitis is thrush that spreads to your esophagus, the tube that takes food from your mouth to your stomach. It can make it hard or painful to swallow.
- Women can get vaginal yeast infections, causing vaginitis
- Yeast infections of the skin cause itching and rashes
- Yeast infections in your bloodstream can be life-threatening
Other less common side effects include:
- ongoing diarrhea caused by an intestinal infection, which may be serious and require further investigation and treatment
- allergic reactions, such as hives (large, red, raised areas on the skin), fever and breathing problems.
Ask your prescribing doctor about the possible side effects of your medicine. You should also ask if there are any medicines you should not take with your antibiotic.
Antibiotic allergic reactions
Around 1 in 15 people have an allergic reaction to antibiotics, especially penicillin and cephalosporins. In very rare cases, this can lead to a serious allergic reaction (anaphylaxis), which is a medical emergency.
In most cases, the allergic reaction is mild to moderate and can take the form of:
- a raised, itchy skin rash (urticaria, or hives)
- swelling of the face, lips and/or eyes
- coughing
- wheezing
- tightness of the throat, which can cause breathing difficulties
These mild to moderate allergic reactions can usually be successfully treated by taking antihistamines.
- But if you’re concerned, or your symptoms don’t respond to treatment, you should call your doctor for advice.
In rare cases, an antibiotic can cause a severe and potentially life-threatening allergic reaction known as anaphylaxis.
Initial symptoms of anaphylaxis are often the same as above and can lead to:
- a rapid heartbeat
- increasing difficulty breathing caused by swelling and tightening of the neck
- difficult/noisy breathing
- a sudden intense feeling of apprehension and fear
- a sharp and sudden drop in your blood pressure, which can make you feel light-headed and confused
- swelling of the tongue
- swelling/tightness of the throat
- difficulty talking/hoarse voice
- wheezing or coughing
- dizziness or collapse
- pale and floppy (especially young children)
- falling unconsciousness
Anaphylaxis is a medical emergency and can be life-threatening if prompt treatment isn’t given. Dial your local emergency number immediately and ask for an ambulance if you think you or someone around you is experiencing anaphylaxis.
The Society of Clinical Immunology and Allergy recommends that for a severe allergic reaction adrenaline is the initial treatment. If you are allergic to antibiotics you may be instructed by a doctor how to avoid triggers and if severe may instruct you how to use a self-administered adrenalin injection such as EpiPen®. The doctor will record the allergy and type of reaction in your notes and electronic health records and will give you an anaphylaxis action plan.
Most allergies are caused by penicillin or antibiotics closely related to penicillin, or by another type of antibiotic called sulfonamides.
Feeling nauseous and vomiting after taking antibiotics is usually a side-effect of the medicine, rather than an allergic reaction.
Your doctor can usually diagnose allergic reactions to antibiotics by talking to you. He or she may refer you to an allergy specialist, who may ask for skin allergy and blood tests.
If you have any other concerns about antibiotics, including possible side effects, contact your doctor.
Tetracyclines and sensitivity to light
Tetracyclines can make your skin sensitive to sunlight and artificial sources of light, such as sun lamps and sunbeds.
You should avoid prolonged exposure to bright light while taking these drugs.
Summary
Antibiotics are valuable therapeutic agents. Their widespread use has resulted in the emergence of many multi-resistant bacterial pathogens in hospitals and the community. In order to preserve the action of existing antibiotics, their use for prophylaxis, empiric or directed therapy should be reserved for situations where there is good evidence to support use and/or the consequences of infection are serious. It is increasingly important to avoid empiric antibiotic use for most patients with upper respiratory infections and pursue symptomatic treatment.
- https://www.cdc.gov/antibiotic-use/community/about/should-know.html[↩]
- Antibiotic Prescribing and Use in Doctor’s Offices. https://www.cdc.gov/antibiotic-use/community/about/should-know.html[↩]
- Writing group for Therapeutic Guidelines: Antibiotic. Therapeutic Guidelines: Antibiotic. 12th edition. Melbourne: Therapeutic Guidelines Ltd.; 2003.[↩][↩][↩][↩]
- Wunderink RG, Woldenberg LS, Zeiss J, Day CM, Ciemins J, Lacher DA. The radiologic diagnosis of autopsy-proven ventilator-associated pneumonia. Chest 1992;101:458-63.[↩]
- Little P, Gould C, Moore M, Warner G, Dunleavey J, Williamson I. Predictors of poor outcome and benefits from antibiotics in children with acute otitis media: pragmatic randomised trial. Br Med J 2002;325:22.[↩]
- Takata GS, Chan LS, Shekelle P, Morton SC, Mason W, Marcy SM. Evidence assessment of management of acute otitis media: I. The role of antibiotics in treatment of uncomplicated acute otitis media. Pediatrics 2001;108:239-47.[↩]
- Management of Patients with Infections Caused by Methicillin-Resistant Staphylococcus Aureus: Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA). http://www.idsociety.org/Guidelines/Patient_Care/IDSA_Practice_Guidelines/Infections_by_Organism/Bacteria/MRSA/[↩]
- Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin-Resistant Staphylococcus aureus Infections in Adults and Children. Clinical Infectious Diseases, Volume 52, Issue 3, 1 February 2011, Pages e18–e55 https://academic.oup.com/cid/article/52/3/e18/306145[↩]



{kind=link}