Contents
- Cyclosporine
- Cyclosporine special precautions
- Cyclosporine mechanism of action
- Cyclosporine uses
- Cyclosporine dosage
- Cyclosporine side effects
- Cyclosporine overdose
Cyclosporine
Cyclosporine also known as cyclosporin, ciclosporin A, cyclosporin A, Neoral, Gengraf or Sandimmune is a powerful immunosuppressant or a drug that weakens your body’s immune system in order to help keep it from “rejecting” a transplanted organ or bone marrow transplants 1. Organ rejection happens when your immune system treats the new organ as an invader and attacks it. Cyclosporine is currently used to prevent organ rejection after a kidney, heart, or liver transplantation. Cyclosporine is also used to treat severe, active rheumatoid arthritis in patients for whom classical slow-acting antirheumatic agents (including methotrexate) are inappropriate or ineffective. Cyclosporine is used to treat severe psoriasis in whom conventional therapy is ineffective or inappropriate and the disease has caused a significant interference with the quality of life. Cyclosporine is also sometimes used to treat Crohn’s disease (a condition in which the body attacks the lining of the digestive tract, causing pain, diarrhea, weight loss, and fever). Furthermore, cyclosporine is also used to treat severe atopic dermatitis when other treatment is ineffective or inappropriate. Careful monitoring of all cyclosporine-treated patients is mandatory. Cyclosporine should only be used by medical practitioners who are experienced in the use of immunosuppressive therapy (see “IMPORTANT WARNING”).
Cyclosporine was introduced into use in the United States in the early 1980s and rapidly became part of the primary treatment regimen of immunosuppression after allogenic, solid organ transplantation.
Cyclosporine and cyclosporine (modified) both come as capsules of 25 and 100 mg under the brand name of Sandimmune and a Cyclosporine (modified) solution with absorbed microemulsion formulation of 25 and 100 mg under the brand name of Neoral. Cyclosporine is also available in solution for intravenous use. Because of variable absorption, the usual maintenance dose of cyclosporine varies greatly and proper dosing requires monitoring for drug levels, which is also important because of its many dose dependent side effects and drug-drug interactions.
Cyclosporine is usually taken by mouth once a day. Cyclosporine (modified) is usually taken twice a day. It is important to take both types of cyclosporine on a regular schedule. Take cyclosporine or cyclosporine (modified) at the same time(s) each day, and allow the same amount of time between doses and meals every day. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take cyclosporine or cyclosporine (modified) exactly as directed. Do not take more or less of the medication or take it more often than prescribed by your doctor.
Your blood urea nitrogen (BUN), creatinine ratio, magnesium levels, and blood pressure require monitoring while on Cyclosporine therapy. Uric acid monitoring is debatable. Therapeutic monitoring of cyclosporine in transplant patients is a valuable tool in adjusting drug dosage to prevent acute rejection, nephrotoxicity, and predictable dose-dependent adverse reactions.
Your doctor will probably adjust your dose of cyclosporine or cyclosporine (modified) during your treatment. If you are taking either type of cyclosporine to prevent transplant rejection, your doctor will probably start you on a high dose of the medication and gradually decrease your dose. If you are taking cyclosporine (modified) to treat rheumatoid arthritis or psoriasis, your doctor will probably start you on a low dose of the medication and gradually increase your dose. Your doctor may also decrease your dose if you experience side effects of the medication. Tell your doctor how you are feeling during your treatment.
Cyclosporine (modified) helps control the symptoms of psoriasis and rheumatoid arthritis, but does not cure these conditions. If you are taking cyclosporine (modified) to treat psoriasis, it may take 2 weeks or longer for your symptoms to begin to improve, and 12 to 16 weeks for you to feel the full benefit of the medication. If you are taking cyclosporine (modified) to treat rheumatoid arthritis, it may take 4 to 8 weeks for your symptoms to improve. Continue to take cyclosporine (modified) even if you feel well. Do not stop taking cyclosporine (modified) without talking to your doctor. Your doctor may decrease your dose gradually.
You may notice an unusual smell when you open a blister card of cyclosporine capsules. This is normal and does not mean that the medication is damaged or unsafe to use.
Cyclosporine (modified) oral solution may gel or become lumpy if it is exposed to temperatures below 68 °F (20 °C). You can use the solution even if it has gelled, or you can turn the solution back to a liquid by allowing it to warm to room temperature (77 °F [25 °C]).
Cyclosporine and cyclosporine (modified) oral solution must be mixed with a liquid before use. Cyclosporine (modified) oral solution may be mixed with room temperature (77 °F [25 °C]) orange juice or apple juice but should not be mixed with milk. Cyclosporine oral solution may be mixed with milk, chocolate milk, or orange juice. You should choose one drink from the appropriate list and try to always mix your medication with that drink.
Cyclosporine common side effects of cyclosporine include headache, dizziness, paresthesias (pins and needles sensation), nerve damage (neuropathy), tremor, high blood pressure (hypertension), high blood cholesterol (hyperlipidemia), kidney damage (nephropathy), acne, hirsutism (unwanted excessive hair growth on a woman’s face, chest and back) and excessive growth of the gums (gum hyperplasia). Uncommon but potentially severe adverse events include kidney damage (nephrotoxicity), microangiopathic hemolytic anemia, neurotoxicity, serious and opportunistic infections, increase risk of cancer and anaphylactic reactions. Nephrotoxicity is one of the serious adverse effects that limit the therapeutic uses of cyclosporine A. Several reports have discussed the mechanisms by which cyclosporine A induces nephrotoxicity 2, 3.
Oral and parenteral cyclosporine should be prescribed only by physicians experienced in immunosuppressive therapy and management of its complications.
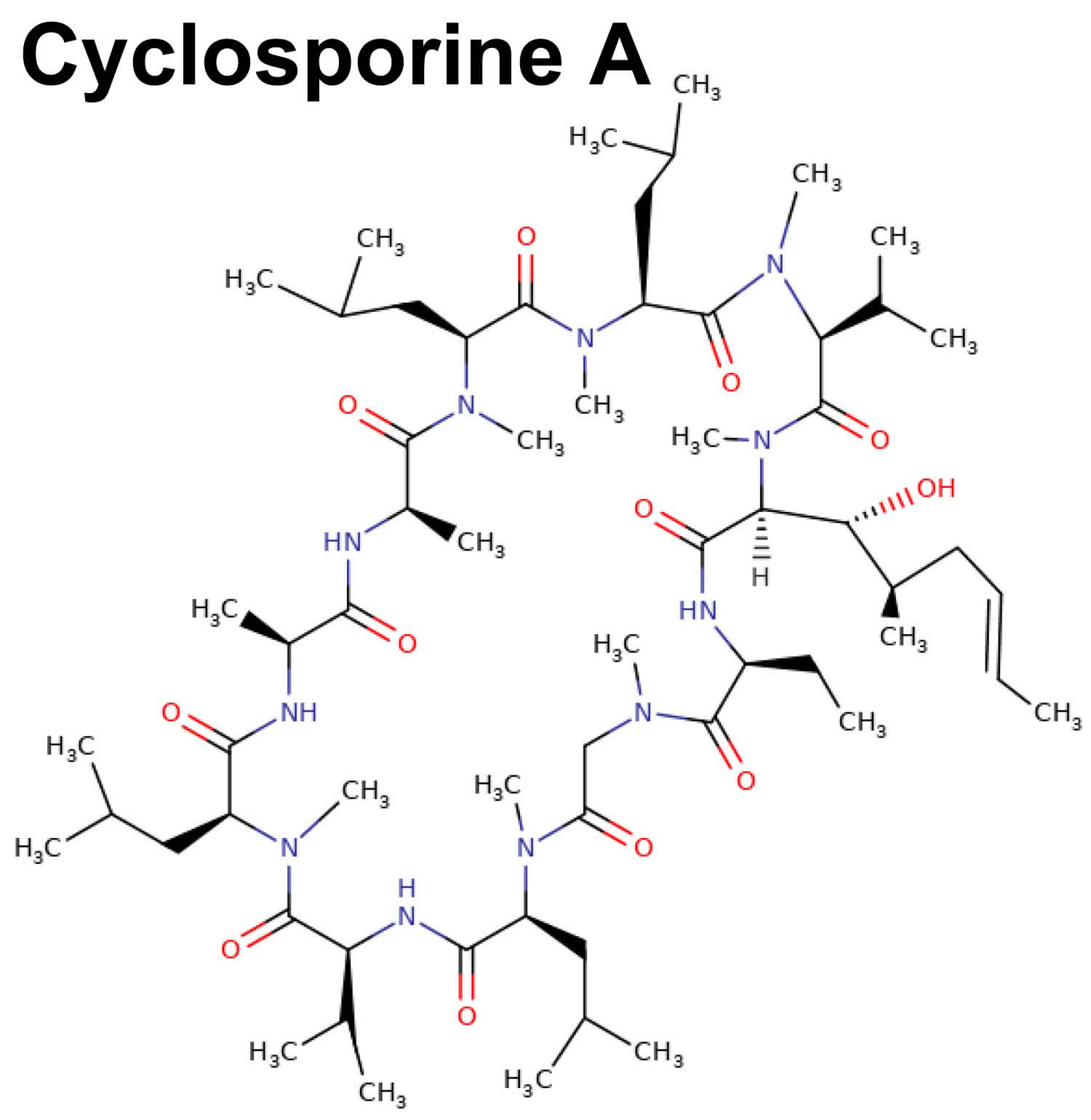
Figure 1. Cyclosporine A chemical structure
Cyclosporine is available in its original form and as another product that has been modified (changed) so that the medication can be better absorbed in the body. Original cyclosporine and cyclosporine (modified) are absorbed by the body in different amounts, so they cannot be substituted for one another. Take only the type of cyclosporine that was prescribed by your doctor. When your doctor gives you a written prescription, check to be sure that he or she has specified the type of cyclosporine you should receive. Each time you have your prescription filled, look at the brand name printed on your prescription label to be sure that you have received the same type of cyclosporine. Talk to your pharmacist if the brand name is unfamiliar or you are not sure you have received the right type of cyclosporine.
Taking cyclosporine or cyclosporine (modified) may increase the risk that you will develop an infection or cancer, especially lymphoma (cancer of a part of the immune system) or skin cancer. This risk may be higher if you take cyclosporine or cyclosporine (modified) with other medications that decrease the functioning of the immune system. Tell your doctor if you are taking any medications that decrease the functioning of the immune system and if you have or have ever had any type of cancer. To reduce your risk of skin cancer, plan to avoid unnecessary or prolonged exposure to sunlight and to wear protective clothing, sunglasses, and sunscreen during your treatment. If you experience any of the following symptoms, call your doctor immediately: sore throat, fever, chills, and other signs of infection; flu-like symptoms; coughing; difficulty urinating; pain when urinating; a red, raised, or swollen area on the skin; new sores or discoloration on the skin; lumps or masses anywhere in your body; night sweats; swollen glands in the neck, armpits, or groin; trouble breathing; weakness or tiredness that does not go away; or weight loss.
Cyclosporine and cyclosporine (modified) may cause high blood pressure and kidney damage. Tell your doctor if you have or have ever had high blood pressure or kidney disease. If you experience any of the following symptoms, call your doctor immediately: dizziness; swelling of the arms, hands, feet, ankles, or lower legs; fast, shallow breathing; nausea; or irregular heartbeat.
If you have psoriasis, tell your doctor about all the psoriasis treatments and medications you are using or have used in the past. The risk that you will develop skin cancer is greater if you have ever been treated with PUVA (psoralen and UVA; treatment for psoriasis that combines an oral or topical medication with exposure to ultraviolet A light); methotrexate (Rheumatrex) or other medications that suppress the immune system; UVB (exposure to ultraviolet B light to treat psoriasis); coal tar; or radiation therapy. You should not be treated with PUVA, UVB, or medications that suppress the immune system while you are taking cyclosporine (modified) to treat psoriasis.
Keep all appointments with your doctor and the laboratory. Your doctor will order certain lab tests to check your body’s response to cyclosporine.
Cyclosporine special precautions
Before taking cyclosporine:
- tell your doctor and pharmacist if you are allergic to cyclosporine, cyclosporine (modified), any other medications, or any of the inactive ingredients in cyclosporine or cyclosporine (modified) capsules or solution. Ask your pharmacist for a list of the inactive ingredients.
- tell your doctor and pharmacist what prescription and nonprescription medications, vitamins, and nutritional supplements you are taking, or plan to take. Your doctor may need to change the doses of your medications or monitor you more carefully for side effects.
- if you are taking sirolimus (Rapamune), take it 4 hours after you take cyclosporine or cyclosporine (modified).
- The following nonprescription or herbal products may interact with cyclosporine: nonsteroidal anti-inflammatory medications (NSAIDs) such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn), and St. John’s wort. Be sure to let your doctor and pharmacist know that you are taking these medications before you start taking cyclosporine. Do not start any of these medications while taking cyclosporine without talking to your healthcare provider.
- Avoid drinking grapefruit juice or eating grapefruit while taking cyclosporine or cyclosporine (modified).
- tell your doctor if you have or have ever had any of the conditions mentioned in the IMPORTANT WARNING section or any of the following: low cholesterol, low levels of magnesium in your blood, high levels of potassium or uric acid in your blood, any condition that makes it difficult for your body to absorb nutrients, or liver disease.
- tell your doctor if you are pregnant or plan to become pregnant. If you become pregnant while taking either type of cyclosporine, call your doctor. Both types of cyclosporine may increase the risk that your baby will be born too early.
- tell your doctor if you are breast-feeding or planning to breast-feed.
- you should know that cyclosporine may make you drowsy, dizzy, or confused. Do not drive a car or operate machinery until you know how this medication affects you.
- you should know that cyclosporine capsules and oral solution contain alcohol. Ask your doctor about the safe use of alcoholic beverages while you are taking cyclosporine.
- do not have vaccinations without talking to your doctor.
Drugs that can decrease cyclosporin A levels include rifampicin, rifabutin, isoniazid, barbiturates, phenytoin, carbamazepine, intravenous trimethoprim, intravenous sulfadimidine, imipenem, cephalosporins, terbinafine, ciprofloxacin, ticlopidine, octreotide, and nefazodone. Conversely, drugs that can increase cyclosporine A levels include verapamil, diltiazem, amlodipine, nicardipine, ketoconazole, fluconazole, itraconazole, erythromycin, clarithromycin, azithromycin, saquinavir, indinavir, nelfinavir, ritonavir, methylprednisolone.
Your doctor may tell you to limit the amount of potassium in your diet. Follow these instructions carefully. Talk to your doctor about the amount of potassium-rich foods such as bananas, prunes, raisins, and orange juice you may have in your diet. Many salt substitutes contain potassium, so talk to your doctor about using them during your treatment.
Non-MODIFIED and MODIFIED formulations
- The non-modified formulation should be administered with corticosteroids but not with other immunosuppressive agents. Increased susceptibility to infection and the possible development of lymphoma may result from immunosuppression.
- The non-modified formulation has decreased bioavailability in comparison to the modified formulation.
- The absorption of cyclosporine during chronic administration of the non-modified formulation is erratic. Patients taking this formulation over a prolonged time should be monitored at intervals for cyclosporine blood concentrations and dose adjustments should be made to avoid toxicity due to high concentrations and possible organ rejection due to low absorption of the drug. This is especially important in liver transplants.
- The non-modified formulation and the modified formulation are not bioequivalent and cannot be used interchangeably without physician supervision.
- The modified formulation has increased bioavailability in comparison to the non-modified formulation. For a given trough concentration, cyclosporine exposure will be greater with the modified formulation than with the non-modified formulation. If a patient who is receiving exceptionally high doses of the non-modified formulation is converted to the modified formulation, caution should be exercised. Cyclosporine blood concentrations should be monitored in transplant and rheumatoid arthritis patients taking the modified formulation to avoid toxicity due to high concentrations. Dose adjustments should be made in transplant patients to minimize possible organ rejection due to low concentrations.
Cyclosporine mechanism of action
Cyclosporine is a cyclic polypeptide of 11 amino acids produced by a fungal species called Tolypocladium inflatum, which has profound immunosuppressive properties, particularly affecting T cells (T lymphocytes), cell-mediated immune response and humoral immunity 4, 5, 6. Cyclosporine works to suppress cell-mediated immune reactions.
The mechanism of action of cyclosporine is as calcineurin inhibitor, a cytochrome P450 3A4 inhibitor, and a P-glycoprotein inhibitor 7. Cyclosporine A acts by blocking T cell infiltration, activation, and the subsequent release of inflammatory cytokines as illustrated in Figure 2 8, 9, 10. In addition, cyclosporine A has an antiapoptotic and protective action on human conjunctival epithelial cells, unlike corticosteroids 11, 9.
Cyclosporine is in an inactive form (prodrug) at first 4. Because cyclosporine is a lipophilic peptide, it can easily pass through the cell membrane where cyclosporine gets combined with cyclophilin, which is a cytosolic protein. The cyclosporine/cyclophilin complexes inhibit the production of interleukins (IL), including interlukin-2 (IL-2), which is essential for the self-activation of T lymphocytes (T cells) and their differentiation via calcineurin inhibition. Calcineurin is accepted to be the target molecule that cyclosporine/cyclophilin complexes attach. What affects the signal production that calcineurin T cells trigger is an enzyme which is in bond with calmodulin and calcium and has serine/threonine phosphatase quality. Dephosphorylation, kinase activity, phosphatase activity, and protein expression can be included among the calcineurin activities. Dephosphorylation occurs in the target molecules within the cell as a result of cyclosporine/cyclophilin bonding with calcineurin, and as a result, inhibition of the IL-2 gene and other cytokine genes occur. Therefore, IL-2 production is blocked, and proliferation signals
of T cells disappear 12, 13.
Cyclosporin A is effective due to specific and reversible inhibition of immunocompetent lymphocytes in the G0 and G1-phase of the cell cycle 7. The T-helper cell is the primary target, although it may also suppress T-suppressor cells. The B-lymphocyte (B cell) co-operation is essential for activation of B-lymphocyte; the latter also gets inhibited. In addition, research has demonstrated that Cyclosporin had an inhibiting effect on CD4+ CD25+ Tregs, which might block the host immune tolerance potentiality.
Cyclosporine metabolism is via liver CYP450 3A 4/5 and is metabolized into a pair of hydroxylated derivatives (AM1 and AM9) and one N-methylated derivative (AM4N) 14.
Figure 2. Cyclosporine A mechanism of action
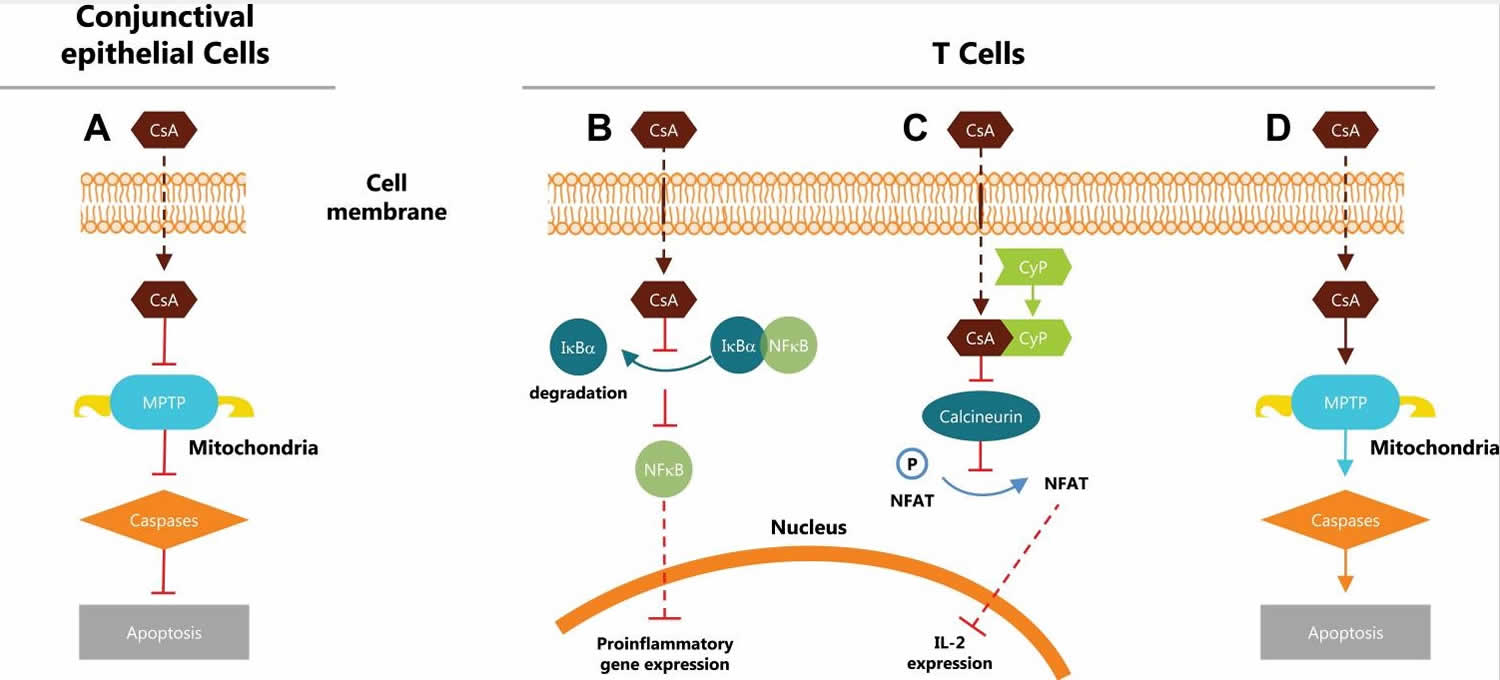
Footnotes: (A) Inhibits intrinsic mitochondrial pathway and caspase activation with an antiapoptotic and protective action on human conjunctival epithelial cells 11, 9 (B) Inhibits nuclear factor κB (NFκB) activation and the subsequent release of proinflammatory cytokines through modulating proteasome activity 10, 15 (C) Binds with cyclophilin to form a calcineurin complex and inhibits dephosphorylation of nuclear factor of activated T cells and the subsequent release of interleukin 2 (IL-2) 8 (D) Induces T cell apoptosis by regulating Fas/Fas ligand expression, caspase activation, and mitochondrial permeability transition pore (MPTP) opening.
Abbreviations: CsA = cyclosporine A; CyP = cyclophilin; Iĸßα = nuclear factor of ĸ light polypeptide gene enhancer in ß-cell inhibitor alpha; IL-2 = interleukin 2; MPTP = mitochondrial permeability transition pore; NFAT = nuclear factor of activated T cells; NFkB = nuclear factor of kB; P = phosphorylated.
[Source 16 ]Cyclosporine uses
Cyclosporine is a potent immunosuppressive agent used to treat organ rejection post-transplant. Cyclosporine also has uses in certain other autoimmune diseases 17, 18, 19, 20, 21.
U.S. Food and Drug Administration (FDA) approved indications 7:
- Solid organ transplantation,Cyclosporine is used to treat organ rejection in kidney, liver, and heart allogeneic transplants.
- In patients with rheumatoid arthritis, Cyclosporine is indicated when the disease has not adequately responded to methotrexate.
- For psoriasis, indications include the treatment of adult, nonimmunocompromised patients with severe, recalcitrant, plaque psoriasis who have not responded to at least one systemic therapy.
- In patients with amyotrophic lateral sclerosis (ALS or Lou Gehrig disease), cyclosporin is approved to treat amyotrophic lateral sclerosis (ALS) and its variants.
- In nephrotic syndrome, Cyclosporin is indicated to treat focal segmental glomerulosclerosis not responding to corticosteroids.
- In individuals with graft vs. host disease (GVHD), Cyclosporin prevents and treats the disease.
- In the case of uveitis, cyclosporin is indicated for refractory posterior uveitis and Behcet disease.
Non-FDA approved indications 7:
- Allergic conjunctivitis, keratoconjunctivitis, Langerhans cells histiocytosis, ocular graft vs. host disease, autoimmune hepatitis, Duchenne muscular dystrophy, ulcerative colitis, pure red cell aplasia, and Henoch Schönlein purpura nephritis.
To take oral cyclosporine, follow these steps:
- Fill a glass (not plastic) cup with the drink you have chosen.
- Remove the protective cover from the top of the dosing syringe that came with your medication.
- Place the tip of the syringe into the bottle of solution and pull back on the plunger to fill the syringe with the amount of solution your doctor has prescribed.
- Hold the syringe over the liquid in your glass and press down on the plunger to place the medication in the glass.
- Stir the mixture well.
- Drink all of the liquid in the glass right away.
- Pour a little more of the drink you have chosen into the glass, swirl the glass around to rinse, and drink the liquid.
- Dry the outside of the syringe with a clean towel and replace the protective cover. Do not wash the syringe with water. If you do need to wash the syringe, be sure that it is completely dry before you use it to measure another dose.
Cyclosporine dosage
Adult Dosing for Organ Transplant
- Oral cyclosporine
- Four to 12 hours pre-transplant: 14 to 18 mg/kg by mouth for one dose.
- One to two weeks post-transplant: 5 to 15 mg/kg per day by mouth divided twice a day.
- Reduce the dose by 5% per week until 5 to 10 mg/kg per day by mouth divided twice per day.
- Intravenous (IV) cyclosporine (maximum concentration 2.5 mg/dL)
- Four to 12 hours pre-transplant IV: 5 to 6 mg/kg IV for one dose over 2 to 6 hours.
- Post-transplant until the patient can tolerate oral therapy: 2 to 10 mg/kg IV once per day.
- Adjust dosage according to trough levels.
Cyclosporine dosage for focal segmental glomerulosclerosis
- Oral 3 mg/kg/day every 12 hours.
Cyclosporine dosage for Rheumatoid arthritis
- Oral (modified), initially: 2.5 mg/kg per day every 12 hrs, increase 0.5 to 0.75 mg/kg per day after eight weeks if the response has not been effective. Maximum dose: 4 mg/kg per day.
Cyclosporine dosage for Psoriasis
- Oral (modified), initially: 2.5 mg/kg per day every 12 hours, increase 0.5 mg/kg per day after four weeks if the response has not been effective. Maximum dose: 4 mg/kg per day.
The ideal therapeutic range of cyclosporine in whole blood is as follows 7:
- Kidney transplant: 200 to 400 ng/ml in the first week after transplantation; 125 to 275 ng/ml in the second week to the sixth-month post-transplantation; 100 to 150 ng/ml in the seventh to the twelfth-month post-transplantation; and 75 to 160 ng/ml one year after transplantation (residual concentration predose).
- Heart transplant: 250 to 350 ng/mL in the first six months; 100 to 200 ng/mL six months to one year after transplantation (residual concentration predose).
- Liver transplant: 250 to 350 ng/mL for the first six months; 100 to 200 ng/mL six months to one year after transplantation (residual concentration predose).
The range between effective cyclosporine concentrations and the concentrations associated with serious toxicity is fairly narrow. Sub-optimal doses or concentrations can lead to therapeutic failure or severe toxicity. Cyclosporine is subject to therapeutic monitoring based on pharmacokinetics measures. The medication has low-to-moderate within-subject variability.
Adult dose for Organ Transplant
Uses: For the prevention of organ rejection in kidney, liver, and heart allogeneic transplants with corticosteroids and in the treatment of chronic rejection in patients previously treated with other immunosuppressive agents. Modified and non-modified cyclosporine formulations are not bioequivalent and cannot be used interchangeably without physician supervision.
Oral cyclosporine (modified with absorbed microemulsion formulation)
- Note: The dose is dependent upon type of transplant and formulation; refer to local protocol for specific dosing.
- Initial dose: Give 4 to 12 hours prior to transplantation or postoperatively; the initial dose varies depending on the organ and concomitant immunosuppressives.
Newly transplanted patients:
- Kidney transplantation: 9 mg/kg/day (plus or minus 3 mg/kg/day) orally in 2 divided doses
- Liver transplantation: 8 mg/kg/day (plus or minus 4 mg/kg/day) orally in 2 divided doses
- Heart transplantation: 7 mg/kg/day (plus or minus 3 mg/kg/day) orally in 2 divided doses
Comment:
- The initial dose of cyclosporin A varies depending on the transplanted organ and the other immunosuppressive agents included in the protocol.
- In newly transplanted patients, the initial oral dose is the same as the initial oral dose of the non-modified formulation.
- Titrate the dose based on rejection and tolerability.
- Lower doses of the modified formulation may be sufficient as maintenance therapy.
- Adjunct therapy with corticosteroids is recommended initially. Consult local protocol and/or manufacturer product information.
Oral cyclosporine
Note: The dosing presented here is to be used as a guideline only. Local protocol should be consulted for specific dosing. Dosing in clinical practice may be very different than the manufacturer labeling. Non-modified formulations have decreased bioavailability in comparison to modified absorbed microemulsion formulations. Modified and non-modified formulations are not bioequivalent and cannot be used interchangeably without physician supervision.
Manufacturer recommendation:
- Initial dose: 15 mg/kg orally 4 to 12 hours prior to transplantation; although a single dose of 14 to 18 mg/kg was used in most clinical trials, most clinicians favor the lower end of the scale; lower initial doses are usually used for renal transplantation in the ranges of 10 to 14 mg/kg/day
- Maintenance dose: The initial single daily dose is continued postoperatively for 1 to 2 weeks and then tapered by 5% per week to a maintenance dose of 5 to 10 mg/kg/day; some clinicians prefer to reduce the maintenance dose to 3 mg/kg/day in some renal transplant patients without an apparent rise in rejection rate
Cyclosporine Parenteral formulation
Note: Local protocol should be consulted for dosing recommendations.
Manufacturer suggested dosing:
- Initial dose: 5 to 6 mg/kg/day IV (or one-third of the oral dose) as a single dose infused over 2 to 6 hours given 4 to 12 hours prior to transplantation
- Maintenance dose: 5 to 6 mg/kg/day IV continued postoperatively until the patient can tolerate capsules or oral solution
Comments:
- Due to the risk of anaphylaxis, the IV formulation should be reserved for patients who are unable to take the oral formulation.
- Adjunct steroid therapy should be used with cyclosporine.
Adult dose for Rheumatoid Arthritis
Use: For severe active, rheumatoid arthritis where the disease has not adequately responded to methotrexate; ciclosporin A can be used in combination with methotrexate in rheumatoid arthritis patients who do not respond adequately to methotrexate alone.
Oral cyclosporine (modified with absorbed microemulsion formulation)
- Initial dose: 1.25 mg/kg orally 2 times a day; onset of action usually occurs between 4 and 8 weeks
- Titration: If insufficient benefit is seen and tolerability is good at the initial dose (including serum creatinine less than 30% above baseline), the dose may be increased by 0.5 to 0.75 mg/kg/day after 8 weeks and again after 12 weeks
- Maximum dose: 4 mg/kg/day orally in 2 divided doses; if no benefit is seen by 16 weeks, therapy should be discontinued
Comments:
- Salicylates, nonsteroidal anti-inflammatory agents, and oral corticosteroids may be continued concomitantly with cyclosporine.
- Dose decreases by 25% to 50% should be made at any time to control adverse events (e.g., hypertension, elevations in serum creatinine 30% above pretreatment level), or significant laboratory abnormalities.
- Most patients can be treated with the modified formulation at doses of 3 mg/kg/day or below when combined with methotrexate doses of up to 15 mg/week.
Adult dose for Psoriasis
Use: For nonimmunocompromised patients with severe (i.e., extensive and/or disabling), recalcitrant, plaque psoriasis who have failed to respond to at least one systemic therapy (e.g., PUVA, retinoids, or methotrexate) or in patients for whom other systemic therapies are contraindicated, or cannot be tolerated.
Oral cyclosporine (modified with absorbed microemulsion formulation)
- Initial dose: 1.25 mg/kg orally 2 times a day for at least 4 weeks
- Titration: If insufficient benefit is seen at 4 weeks and tolerability is good at the initial dose, the dose may be increased by 0.5 mg/kg/day at 2-week intervals based on patient response.
- Maximum dose: 4 mg/kg/day in 2 divided doses
- Note: Doses below 2.5 mg/kg/day may also be effective.
Comments:
- Dose decreases by 25% to 50% should be made at any time for adverse events (e.g., hypertension, elevations in serum creatinine greater than or equal to 25% above pretreatment level), or significant laboratory abnormalities. Discontinue therapy if dose reduction is not effective.
- Improvement is usually seen in 2 weeks; stabilization may take 12 to 16 weeks.
- Discontinue therapy if a satisfactory response cannot be achieved after 6 weeks at 4 mg/kg/day or the maximum tolerated dose.
- When a patient appears stable the dose should be lowered, and the patient treated with the lowest dose that maintains an adequate response (not necessarily a complete response).
- Doses at the lower end of the recommended range are effective in maintaining a satisfactory response in 60% of the patients. Doses below 2.5 mg/kg/day may also be effective.
- Most patients will experience relapse of their psoriasis upon cessation of therapy.
- Long term experience in psoriasis patients is limited; therefore, therapy beyond one year is not recommended. Alternating with other forms of therapy should be considered in the long-term management of psoriasis.
Children dose for Organ Transplant
Uses: For the prevention of organ rejection in kidney, liver, and heart allogeneic transplants with corticosteroids and in the treatment of chronic rejection in patients previously treated with other immunosuppressive agents. Modified and non-modified cyclosporine formulations are not bioequivalent and cannot be used interchangeably without physician supervision.
The same dose and dosing regimen may be used in children as in adults although in several studies, children have required and tolerated higher doses than adults. Consult the manufacturer product information/and or local protocol.
Oral cyclosporine (modified with absorbed microemulsion formulation)
1 year and older:
- Note: The dose is dependent upon type of transplant and formulation; refer to local protocol for specific dosing.
- Initial dose: Give 4 to 12 hours prior to transplantation or postoperatively; the initial dose varies depending on the organ and concomitant immunosuppressives.
Newly transplanted patients:
- Kidney transplantation: 9 mg/kg/day (plus or minus 3 mg/kg/day) orally in 2 divided doses
- Liver transplantation: 8 mg/kg/day (plus or minus 4 mg/kg/day) orally in 2 divided doses
- Heart transplantation: 7 mg/kg/day (plus or minus 3 mg/kg/day) orally in 2 divided doses
Comments:
- The initial dose of cyclosporine varies depending on the transplanted organ and the other immunosuppressive agents included in the protocol.
- In newly transplanted patients, the initial oral dose is the same as the initial oral dose of the non-modified formulation.
- Titrate the dose based on rejection and tolerability.
- Lower doses of the modified formulation may be sufficient as maintenance therapy.
- Adjunct therapy with adrenal corticosteroids is recommended initially. Consult local protocol and/or manufacturer product information.
Oral cyclosporine
Uses: For the prevention of organ rejection in kidney, liver, and heart allogeneic transplants concomitantly with corticosteroids and in the treatment of chronic rejection in patients previously treated with other immunosuppressive agents
6 months and older: The dosing presented here is to be used as a guideline only. Local protocol should be consulted for specific dosing. Dosing in clinical practice may be very different than the manufacturer labeling. Non-modified formulations have decreased bioavailability in comparison to modified formulations. Modified and non-modified formulations are not bioequivalent and cannot be used interchangeably without physician supervision.
Manufacturer recommendation:
- Initial dose: 15 mg/kg orally 4 to 12 hours prior to transplantation; although a single dose of 14 to 18 mg/kg was used in most clinical trials, most clinicians favor the lower end of the scale; lower initial doses are usually used for renal transplantation in the ranges of 10 to 14 mg/kg/day
- Maintenance dose: The initial single daily dose is continued postoperatively for 1 to 2 weeks and then tapered by 5% per week to a maintenance dose of 5 to 10 mg/kg/day; some clinicians prefer to reduce the maintenance dose to 3 mg/kg/day in some renal transplant patients without an apparent rise in rejection rate
Cyclosporine Parenteral formulation
6 months and older: Local protocol should be consulted for dosing recommendations.
Manufacturer suggested dosing:
- Initial dose: 5 to 6 mg/kg/day IV (or one-third of the oral dose) as a single dose infused over 2 to 6 hours given 4 to 12 hours prior to transplantation
- Maintenance dose: 5 to 6 mg/kg/day IV continued postoperatively until the patient can tolerate capsules or oral solution
Comments:
- Due to the risk of anaphylaxis, the IV formulation should be reserved for patients who are unable to take the oral formulation.
- Adjunct steroid therapy should be used with cyclosporin A.
Kidney disease dose adjustments
- Rheumatoid arthritis or psoriasis patients with abnormal kidney function: Cyclosporin A is Contraindicated
- Careful monitoring of blood or plasma concentrations of cyclosporine A is necessary to avoid exacerbation of kidney impairment.
Liver disease dose adjustments
- Dose reduction may be necessary in patients with severe liver impairment to maintain blood concentrations within the recommended target range
- Due to decreased plasma clearance of Cyclosporin A in patients with liver disease, plasma or blood concentrations should be monitored closely and dose adjustments made as necessary.
What should I do if I forget a dose?
If you forget to take a dose, take the missed dose as soon as you remember it. However, if it is almost time for the next dose, skip the missed dose and continue your regular dosing schedule. Do not take a double dose to make up for a missed one.
Cyclosporine side effects
Cyclosporine may cause side effects. Tell your doctor if any of these symptoms are severe or do not go away:
- headache
- diarrhea
- heartburn
- gas
- increased hair growth on the face, arms, or back
- growth of extra tissue on the gums
- acne
- flushing
- uncontrollable shaking of a part of your body
- burning or tingling in the hands, arms, feet, or legs
- muscle or joint pain
- cramps
- pain or pressure in the face
- ear problems
- breast enlargement in men
- depression
- difficulty falling asleep or staying asleep
Some side effects can be serious. If you experience any of the following symptoms, or those listed in the IMPORTANT WARNING section, see your doctor immediately:
- unusual bleeding or bruising
- pale skin
- yellowing of the skin or eyes (jaundice), nausea, vomiting, loss of appetite, extreme tiredness, flu-like symptoms, pain in the upper right part of the stomach, dark urine, or light-colored bowel movements
- seizures
- loss of consciousness
- changes in behavior or mood
- difficulty controlling body movements
- loss of balance or coordination, or unsteadiness
- weakness or the inability to move on one side of the body
- changes in vision
- confusion
- purple blotches on the skin
- rash, itching, or hives
- Kidney damage: Decreases glomerular filtration rate (GFR) due to an increased tone of the glomerular afferent arterioles. Serum creatinine concentration rises and decreases creatinine clearance. The undesirable effects correlate with the duration of treatment and dose of Cyclosporine A.
- Neurotoxicity: There have been reports of convulsions, especially in combination with high dose methylprednisolone, encephalopathy, anxiety, headache, and fever.
- Cancer. There is an increased risk of developing skin and lymphoproliferative cancers in cyclosporine-treated psoriasis patients. Increase in the occurrence of malignant lymphomas.
- Increase the level of inflammatory cytokines such as TNF-alfa.
- Increase the risk of infection risk 22, 23, 4.
Cyclosporine may cause other side effects. Talk to your doctor if you experience unusual problems while taking cyclosporine.
Cyclosporine overdose
Cyclosporine overdose symptoms may include:
- vomiting
- drowsiness
- headache
- fast heart beat
- yellowing of the skin or eyes
- swelling of the arms, hands, feet, ankles, or lower legs.
In the event of Cyclosporin overdose, establishing a patent airway is a priority. There is a need to watch for signs of respiratory insufficiency and provide ventilation assistance if needed. Also, the healthcare provider needs to monitor for shock and treat if necessary. They should anticipate seizures and treat if necessary, and initiate supportive and symptomatic treatment. When overdosage occurs in patients prescribed cyclosporine A therapy, the healthcare provider may withhold the drug for a few days or initiate alternate-day therapy until the patient stabilizes 24.
Hemodialysis only eliminates 1% of the Cyclosporin dose. Monitoring serum Cyclosporin A levels is mandatory, and patients may need multiple dose adjustments during the treatment period. The central venous catheter (CVC) line is not used to infuse cyclosporine A and can be safely used to collect blood samples for serum cyclosporin A levels. The procedure can be performed immediately after interrupting the infusion if using the appropriate technique for discarding 5 mL of blood.
- Ibrahim SRM, Abdallah HM, El-Halawany AM, Mohamed GA, Alhaddad AA, Samman WA, Alqarni AA, Rizq AT, Ghazawi KF, El-Dine RS. Natural Reno-Protective Agents against Cyclosporine A-Induced Nephrotoxicity: An Overview. Molecules. 2022 Nov 11;27(22):7771. doi: 10.3390/molecules27227771[↩]
- Wu Q., Wang X., Nepovimova E., Wang Y., Yang H., Kuca K. Mechanism of cyclosporine A nephrotoxicity: Oxidative stress, autophagy, and signalings. Food Chem. Toxicol. 2018;118:889–907. doi: 10.1016/j.fct.2018.06.054[↩]
- Tedesco D., Haragsim L. Cyclosporine: A Review. J. Transplant. 2012;2012:230386. doi: 10.1155/2012/230386[↩]
- Arslansoyu Camlar S, Soylu A, Kavukçu S. Cyclosporine in Pediatric Nephrology. Iran J Kidney Dis. 2018 Nov;12(6):319-330. http://www.ijkd.org/index.php/ijkd/article/view/3815/1033[↩][↩][↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Cyclosporine. [Updated 2020 Feb 17]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548753[↩]
- Neoral® (Cyclosporine capsules and oral solution, USP) MODIFIED. Full prescribing information. Novartis; East Hanover, NJ: 2009.[↩]
- Tapia C, Nessel TA, Zito PM. Cyclosporine. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482450[↩][↩][↩][↩][↩]
- Ambroziak AM, Szaflik J, Szaflik JP, Ambroziak M, Witkiewicz J, Skopinski P. Immunomodulation on the ocular surface: a review. Cent Eur J Immunol. 2016;41(2):195–208. doi: 10.5114/ceji.2016.60995[↩][↩]
- Gao J, Sana R, Calder V, et al. Mitochondrial permeability transition pore in inflammatory apoptosis of human conjunctival epithelial cells and T cells: effect of cyclosporin A. Invest Ophthalmol Vis Sci. 2013;54(7):4717–4733. doi: 10.1167/iovs.13-11681[↩][↩][↩]
- Meyer S, Kohler NG, Joly A. Cyclosporine A is an uncompetitive inhibitor of proteasome activity and prevents NF-kappaB activation. FEBS Lett. 1997;413(2):354–358. doi: 10.1016/S0014-5793(97)00930-7[↩][↩]
- Jones L, Downie LE, Korb D, et al. TFOS DEWS II Management and Therapy Report. Ocul Surf. 2017;15(3):575–628. doi: 10.1016/j.jtos.2017.05.006[↩][↩]
- Taylor AL, Watson CJ, Bradley JA. Immunosuppressive agents in solid organ transplantation: Mechanisms of action and therapeutic efficacy. Crit Rev Oncol Hematol. 2005 Oct;56(1):23-46. doi: 10.1016/j.critrevonc.2005.03.012[↩]
- Faulds D, Goa KL, Benfield P. Cyclosporin. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic use in immunoregulatory disorders. Drugs. 1993 Jun;45(6):953-1040. doi: 10.2165/00003495-199345060-00007. Erratum in: Drugs 1993 Sep;46(3):377. Erratum in: Drugs. 1993 Sep;46(3):377.[↩]
- Colombo M.D., Perego R., Bellia G. Drug interaction and potential side effects of cyclosporine. Adv. Exp. Med. Biol. 2013;74:1–24.[↩]
- Du S, Hiramatsu N, Hayakawa K, et al. Suppression of NF-kappaB by cyclosporin a and tacrolimus (FK506) via induction of the C/EBP family: implication for unfolded protein response. J Immunol. 2009;182(11):7201–7211. doi: 10.4049/jimmunol.0801772[↩]
- Jerkins GW, Pattar GR, Kannarr SR. A Review of Topical Cyclosporine A Formulations-A Disease-Modifying Agent for Keratoconjunctivitis Sicca. Clin Ophthalmol. 2020 Feb 20;14:481-489. doi: 10.2147/OPTH.S228070[↩]
- Pradier A, Papaserafeim M, Li N, Rietveld A, Kaestel C, Gruaz L, Vonarburg C, Spirig R, Puga Yung GL, Seebach JD. Small-Molecule Immunosuppressive Drugs and Therapeutic Immunoglobulins Differentially Inhibit NK Cell Effector Functions in vitro. Front Immunol. 2019 Mar 27;10:556. doi: 10.3389/fimmu.2019.00556[↩]
- Pharmacoeconomic Review Report: Ixekizumab (Taltz): (Eli Lilly Canada Inc.): Indication: Treatment of adult patients with active psoriatic arthritis who have responded inadequately to, or are intolerant to one or more disease-modifying antirheumatic drugs (DMARD). Taltz can be used alone or in combination with a conventional DMARD (e.g., methotrexate) [Internet]. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2018 Aug. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539537[↩]
- Ponticelli C, Glassock RJ. Prevention of complications from use of conventional immunosuppressants: a critical review. J Nephrol. 2019 Dec;32(6):851-870. doi: 10.1007/s40620-019-00602-5[↩]
- Xin GLL, Khee YP, Ying TY, Chellian J, Gupta G, Kunnath AP, Nammi S, Collet T, Hansbro PM, Dua K, Chellappan DK. Current Status on Immunological Therapies for Type 1 Diabetes Mellitus. Curr Diab Rep. 2019 Mar 23;19(5):22. doi: 10.1007/s11892-019-1144-3[↩]
- Sun SL, Liu JJ, Zhong B, Wang JK, Jin X, Xu H, Yin FY, Liu TN, Chen QM, Zeng X. Topical calcineurin inhibitors in the treatment of oral lichen planus: a systematic review and meta-analysis. Br J Dermatol. 2019 Dec;181(6):1166-1176. doi: 10.1111/bjd.17898[↩]
- Pal P, Giri PP, Sinha R. Cyclosporine in Resistant Systemic Arthritis – A Cheaper Alternative to Biologics. Indian J Pediatr. 2019 Jul;86(7):590-594. doi: 10.1007/s12098-019-02912-9[↩]
- Shin HS, Grgic I, Chandraker A. Novel Targets of Immunosuppression in Transplantation. Clin Lab Med. 2019 Mar;39(1):157-169. doi: 10.1016/j.cll.2018.10.008[↩]
- Patocka J, Nepovimova E, Kuca K, Wu W. Cyclosporine A: Chemistry and Toxicity – A Review. Curr Med Chem. 2021;28(20):3925-3934. doi: 10.2174/0929867327666201006153202[↩]




{kind=link}