What is temporal arteritis
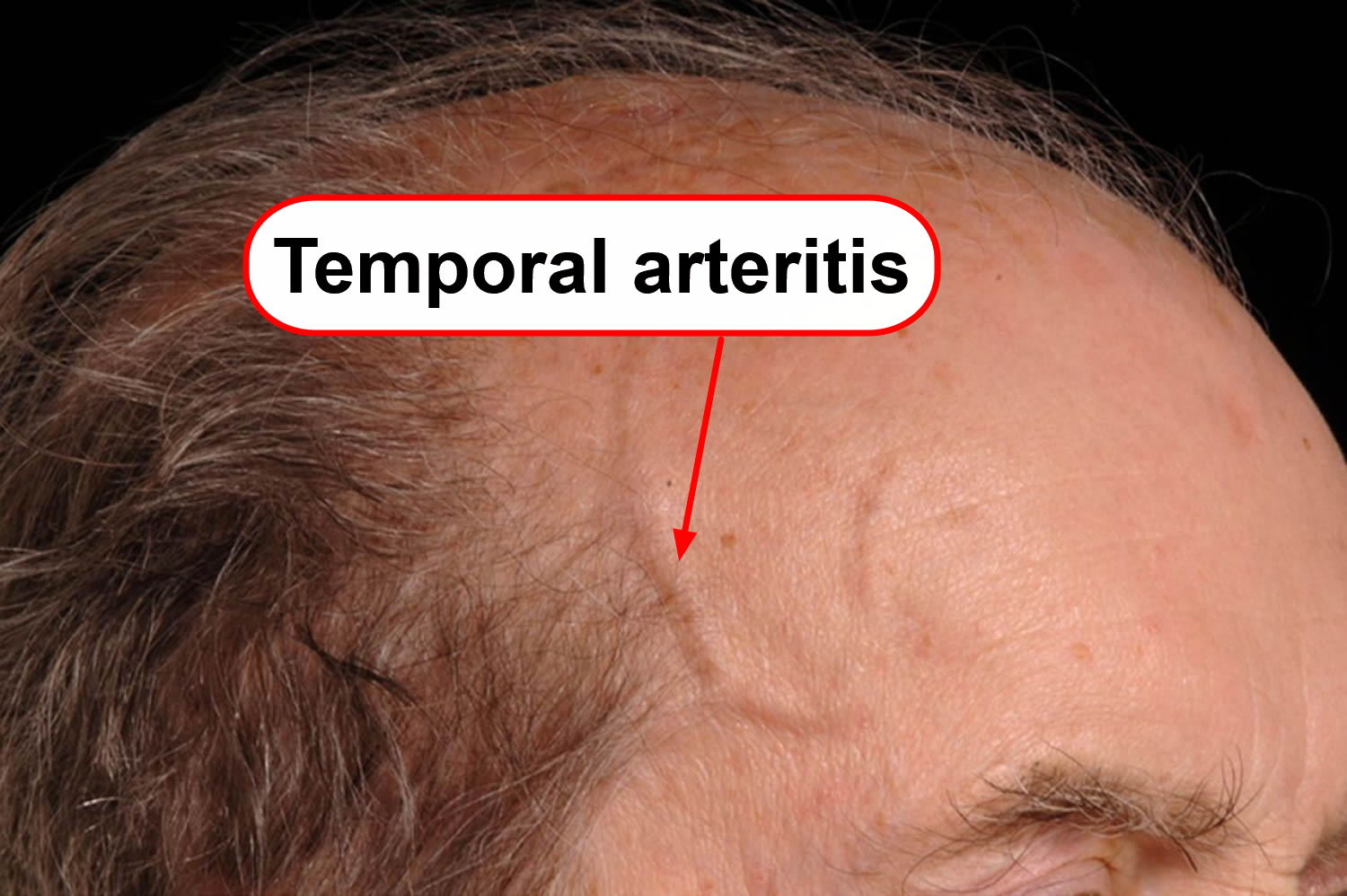
Temporal arteritis (giant cell arteritis) is where the arteries, particularly those at the side of your head (the temples), become inflamed. Temporal arteritis (giant cell arteritis) is a serious condition that requires urgent treatment.
- Temporal arteritis (giant cell arteritis) can lead to serious problems like stroke and blindness if not treated quickly.
Giant cell arteritis (temporal arteritis) is the most common form of vasculitis that occurs in adults. Almost all patients who develop temporal arteritis (giant cell arteritis) are over the age of 50. The average age at onset is 72, and almost all people with the disease are over the age of 50. Women are afflicted with temporal arteritis 2 to 3 times more commonly than men. Temporal arteritis (giant cell arteritis) can occur in every racial group but is most common in people of Scandinavian descent. Giant cell arteritis (temporal arteritis) commonly causes headaches, joint pain, facial pain, fever, and difficulties with vision, and sometimes permanent visual loss in one or both eyes. Because the disease is relatively uncommon and because the disease can cause so many different symptoms, the diagnosis of temporal arteritis (giant cell arteritis) can be difficult to make. With appropriate therapy, giant cell arteritis (temporal arteritis) is an eminently treatable, controllable, and often curable disease.
Giant cell arteritis used to be called “temporal arteritis” because the temporal arteries, which course along the sides of your head just in front of the ears (to the temples) can become inflamed. However, scientists and doctors also know that other blood vessels, namely the aorta and its branches, can also become inflamed. The term “giant cell arteritis” is often used because when you looks at biopsies of inflamed temporal arteries under a microscope, you often sees large or “giant” cells.
The diagnosis is made by doing a biopsy of the temporal artery. Using a local numbing medication (the same one used by a dentist), the doctor can remove a small part of the temporal artery from under the scalp and look at it under the microscope for evidence of inflammation. A temporal artery biopsy is almost always safe, causes very little pain, and often leaves little or no scar.
The mainstay of treatment is glucocorticoids (corticosteroids); temporal arteritis (giant cell arteritis) is now represent one of the most common reasons for medium-to-high dose, long-term corticosteroid treatment in primary care.
Figure 1. Temporal arteritis (giant cell arteritis)

Temporal arteritis / Giant cell arteritis symptoms
The symptoms of temporal arteritis (giant cell arteritis) depend on which arteries are affected. The onset of temporal arteritis (giant cell arteritis) can feel like the flu.
The most common symptoms of temporal arteritis (giant cell arteritis) are:
- frequent, severe headaches,
- pain and tenderness over the temples
- pain in the shoulders and hips (called polymyalgia rheumatica),
- pain in the jaw while eating or talking (called jaw claudication),
- fever,
- vision problems, such as double vision, blurred vision or a loss of vision in one or both eyes
Other symptoms can include tenderness of scalp (it hurts to comb the hair), cough, throat pain, tongue pain, weight loss, depression, stroke, or pain in the arms during exercise. Some patients have many of these symptoms; others have only a few. Blindness — the most feared complication — can develop if temporal arteritis (giant cell arteritis) is not treated in a timely fashion.
More general symptoms are also common – for example, flu-like symptoms, unintentional weight loss, depression and tiredness.
Around half of all people with temporal arteritis also develop polymyalgia rheumatica, which causes pain, stiffness and inflammation in the muscles around the shoulders, neck and hips.
Temporal arteritis causes (giant cell arteritis causes)
Just what causes these arteries to become inflamed isn’t known. Certain genes and gene variations may increase your susceptibility to the condition. Scientists do know that aging has something to do with the disease. And scientists know that the body’s immune system attacks and inflames the arteries. But scientists do not know why the immune system attack occurs when and where it does.
With temporal arteritis (giant cell arteritis), the lining of arteries becomes inflamed. This causes them to swell. This swelling narrows your blood vessels, reducing the amount of blood — and, therefore, oxygen and vital nutrients — that reaches your body’s tissues.
Almost any large or medium-sized artery can be affected, but swelling most often occurs in the arteries located in the temples. These are located just in front of your ears and continue up into your scalp. Sometimes the swelling affects just part of an artery with sections of normal vessel in between.
Risk factors for developing temporal arteritis (giant cell arteritis)
Several factors can increase your risk of developing giant cell arteritis, including:
- Age. Temporal arteritis (giant cell arteritis) affects adults only, and rarely those under 50. Most people with this condition first experience warning signs between the ages of 70 and 80.
- Sex. Women are about two times more likely to develop the condition.
- Race and geographic region. Temporal arteritis (giant cell arteritis) is most common among whites in northern European populations or of Scandinavian descent.
- Polymyalgia rheumatica. Having polymyalgia rheumatica puts you at increased risk of developing giant cell arteritis.
- Family history. Sometimes the condition runs in families.
Temporal arteritis (giant cell arteritis) complications
Temporal arteritis (giant cell arteritis) can cause the following complications:
- Blindness. Diminished blood flow to your eyes can cause sudden, painless vision loss in one or, rarely, both eyes. Loss of vision is usually permanent.
- Aortic aneurysm. An aneurysm is a bulge that forms in a weakened blood vessel, usually in the aorta, the large artery that runs down the center of your chest and abdomen. An aortic aneurysm may burst, causing life-threatening internal bleeding. Because this complication may occur even years after the initial diagnosis of giant cell arteritis, your doctor may monitor the health of your aorta with annual chest X-rays or other imaging tests, such as ultrasound and CT.
- Stroke. This is an uncommon complication of temporal arteritis (giant cell arteritis).
Temporal arteritis diagnosis (Giant cell arteritis diagnosis)
Temporal arteritis (giant cell arteritis) can be difficult to diagnose because its early symptoms resemble those of many common conditions. For this reason, your doctor will try to rule out other possible causes of your problem.
To help diagnose temporal arteritis (giant cell arteritis), you may have some or all of the following tests and procedures:
- Physical exam. In addition to asking about your symptoms and medical history, your doctor is likely to perform a thorough physical exam, paying particular attention to your temporal arteries. Often, one or both of these arteries are tender with a reduced pulse and a hard, cord-like feel and appearance.
- Blood tests. If your doctor thinks you might have temporal arteritis (giant cell arteritis), you’re likely to have a blood test that checks your erythrocyte sedimentation rate — commonly referred to as the sed rate. This test measures how quickly red blood cells fall to the bottom of a tube of blood. Red cells that drop rapidly may indicate inflammation in your body. You may also have a test that measures C-reactive protein (CRP), a substance your liver produces when inflammation is present. The same tests may be used to follow your progress during treatment.
- Temporal arteritis biopsy. The best way to confirm a diagnosis of temporal arteritis (giant cell arteritis) is by taking a small sample (biopsy) of the temporal artery. The procedure is performed on an outpatient basis during local anesthesia, usually with little discomfort or scarring. The sample is examined under a microscope in a laboratory. If you have temporal arteritis (giant cell arteritis), the artery will often show inflammation that includes abnormally large cells, called giant cells, which give the disease its name. It’s possible to have temporal arteritis (giant cell arteritis) and still have a negative biopsy result. If the results aren’t clear, your doctor may advise another temporal artery biopsy on the other side of your head.
Imaging tests may be used for diagnosing giant cell arteritis and for monitoring your response to treatment. Possible tests include:
- Magnetic resonance angiography (MRA). This test combines the use of magnetic resonance imaging (MRI) with the use of a contrast material that produces detailed images of your blood vessels. Let your doctor know ahead of time if you’re uncomfortable being confined in a small space because the test is conducted in a tube-shaped machine.
- Doppler ultrasound. This test uses sound waves to produce images of blood flowing through your blood vessels.
- Positron emission tomography (PET). Using an intravenous tracer solution that contains a tiny amount of radioactive material, a PET scan can produce detailed images of your blood vessels and highlight areas of inflammation.
Temporal arteritis / Giant cell arteritis treatment
Treatment for temporal arteritis (giant cell arteritis) consists of high doses of a corticosteroid drug such as prednisone. Typically, treatment begins with 40–60 mg of prednisone, taken by mouth each day. Most patients improve rapidly and dramatically on this dose, with improvement of most symptoms in 1–3 days. Unfortunately, if blindness has occurred as a symptom it is usually irreversible, which only emphasizes the importance of early detection and treatment.
Treatment will be started before temporal arteritis (giant cell arteritis) is confirmed because of the risk of vision loss if it isn’t dealt with quickly.
You’ll likely begin to feel better within just a few days of beginning treatment. Unless you have complete vision loss, your visual symptoms will likely clear up within three months.
You may need to continue taking medication for one to two years or longer. After the first month, your doctor may gradually begin to lower the dosage until you reach the lowest dose of corticosteroids needed to control inflammation.
Some symptoms, particularly headache, may return during this tapering period. This is also the point at which many people also develop symptoms of polymyalgia rheumatica. Such flares can usually be treated with slight increases in the corticosteroid dose. Your doctor may also suggest a drug called methotrexate, which may help reduce the side effects of corticosteroids.
Corticosteroids can lead to a number of serious side effects, such as osteoporosis, high blood pressure and muscle weakness. To counter these potential side effects, your doctor is likely to monitor your bone density and may prescribe calcium and vitamin D supplements or other medications to help prevent bone loss. Your doctor is also likely to monitor your blood pressure and may recommend an exercise program, diet changes and medication to keep blood pressure within a normal range. Most side effects go away when the corticosteroid treatment is tapered and stopped.
There are 2 stages of treatment:
- An initial high dose of steroids for a few weeks to help bring your symptoms under control.
- A lower steroid dose (after your symptoms have improved) given over a longer period of time, possibly several years.
You’ll have regular follow-ups to see how you’re doing and check for any side effects you may have. Almost all patients experience side effects from prednisone. After the patient improves, the doctor gradually reduces the prednisone dose. The rate of tapering prednisone depends on how the patient feels, what the doctor finds on exam, and the results of blood tests, including the sedimentation rate. Although virtually all patients are able to reduce their prednisone dose, most require some amount of prednisone for 1–2 years. Longer treatment periods are not uncommon. A small number of people may need to take steroids for the rest of their life.
About prednisone
Prednisone is a type of medicine known as a corticosteroid or steroid. Corticosteroids are NOT the same as anabolic steroids.
Prednisone is used to treat a wide range of health problems including allergies, blood disorders, skin diseases, infections, certain cancers and to prevent organ rejection after a transplant.
It helps by reducing inflammation. It also damps down your immune system, which can help in autoimmune illnesses, like temporal arteritis (giant cell arteritis) and rheumatoid arthritis, where your immune system mistakenly attacks its own tissues.
Prednisolone is available only on prescription as tablets and as a liquid to drink. It can also be given by injection but this is usually only done in hospital.
- It’s important to take prednisolone as your doctor has advised.
- Take prednisolone once a day in the morning so it doesn’t keep you awake.
- Taking prednisolone can make you more likely to get infections. Tell your doctor if you’re exposed to infectious illnesses like chickenpox or shingles.
- The most common side effects of prednisolone are weight gain, indigestion, insomnia and sweating a lot.
- Prednisolone can cause withdrawal problems if you stop taking it suddenly. Do not stop the medicine suddenly if you’ve been on it for more than 3 weeks or have taken high doses (more than 40mg) for more than 1 week.
Side effects
The higher the dose of prednisolone that you take, the greater the chance of side effects. You are less likely to get side effects if you take a relatively low dose of less than 20mg prednisolone daily.
Some side effects, such as stomach upset or mood changes, can happen straight away. Others, such as getting a rounder face, happen after weeks or months.
Common side effects
Common side effects happen in more than 1 in 100 people. Keep taking the medicine, but tell your doctor if they bother you or don’t go away:
- weight gain
- indigestion
- not able to sleep
- restlessness
- sweating a lot
Serious side effects
You are more likely to have a serious side effect if you take a higher dose (more than 20mg daily) of prednisolone or if you have been taking it for more than a few weeks.
Tell a doctor straight away if you get:
- fever, chills, a very sore throat, ear or sinus pain, a cough, more saliva or a change in colour of saliva, pain with passing urine, mouth sores or a wound that will not heal – these can be signs of an infection
- sleepy or confused, feeling very thirsty or hungry, passing urine more often, flushing, breathing quickly or breath that smells like fruit – these can be signs of high blood sugar
- weight gain in the upper back or belly, moon face, very bad headaches and slow wound healing – these can be signs of Cushing’s syndrome
- a very upset stomach or vomiting, very bad dizziness or passing out, muscle weakness, feeling very tired, mood changes, loss of appetite and weight loss – these can be signs of adrenal gland problems
- muscle pain or weakness, muscle cramps, or a heartbeat that does not feel normal – these can be signs of low potassium levels
- severe stomach pain, severe back pain, severe upset stomach or vomiting – these can be signs of pancreas problems
You should also tell a doctor straight away if you get:
- breathless
- swelling in your arms or legs
- changes in your eyesight
- any bruising or bleeding that isn’t normal
- black poo
- black or dark brown vomit or vomiting blood
Serious allergic reaction
In rare cases, it’s possible to have a serious allergic reaction to prednisolone.
Other treatments
Other types of medication you may need if you have temporal arteritis (giant cell arteritis) include:
- low-dose aspirin – to reduce the risk of stroke or a heart attack, which can occur if the arteries to your heart are affected
- proton pump inhibitors (PPIs) – to lower your risk of getting a stomach problem like indigestion or a stomach ulcer, which can be a side effect of taking prednisolone
- bisphosphonate therapy – to reduce the risk of osteoporosis when taking prednisolone
- immunosuppressants – to allow steroid medication to be reduced and help prevent temporal arteritis coming back
Home remedies
When temporal arteritis (giant cell arteritis) is diagnosed and treated early, the prognosis is usually excellent. Your symptoms will likely improve quickly after beginning corticosteroid treatment, and your vision isn’t likely to be affected. Your greatest challenge in this case may be coping with any side effects of your medication.
The following suggestions may help:
- Eat a healthy diet. Eating well can help prevent potential problems, such as thinning bones, high blood pressure and diabetes. Emphasize fresh fruits and vegetables, whole grains, and lean meats and fish, while limiting salt, sugar and alcohol. Be sure to get adequate amounts of calcium and vitamin D. Experts recommend 1,200 milligrams of calcium and 800 international units (IU) of vitamin D a day for women over 50 and men over 70. Check with your doctor to see what dose is right for you.
- Exercise regularly. Regular aerobic exercise, such as walking, can help prevent bone loss, high blood pressure and diabetes. It also benefits your heart and lungs. In addition, many people find that exercise improves their mood and overall sense of well-being. If you’re not used to exercising, start out slowly and build up gradually. Your doctor can help you plan an exercise program that’s right for you.
- Get regular checkups. See your doctor to check for side effects of treatment and development of any complications.
- Ask about aspirin. Ask your doctor about taking between 75 and 150 milligrams of aspirin daily. Taken daily, low-dose aspirin may reduce the risk of blindness and stroke.
Coping and support
Learning everything you can about temporal arteritis (giant cell arteritis) and its treatment can help you feel more in control of your condition. Your health care team can answer your questions, and online support groups may also be of help. Know the possible side effects of any medication you take, and report any changes in your health to your doctor.
Takayasu arteritis
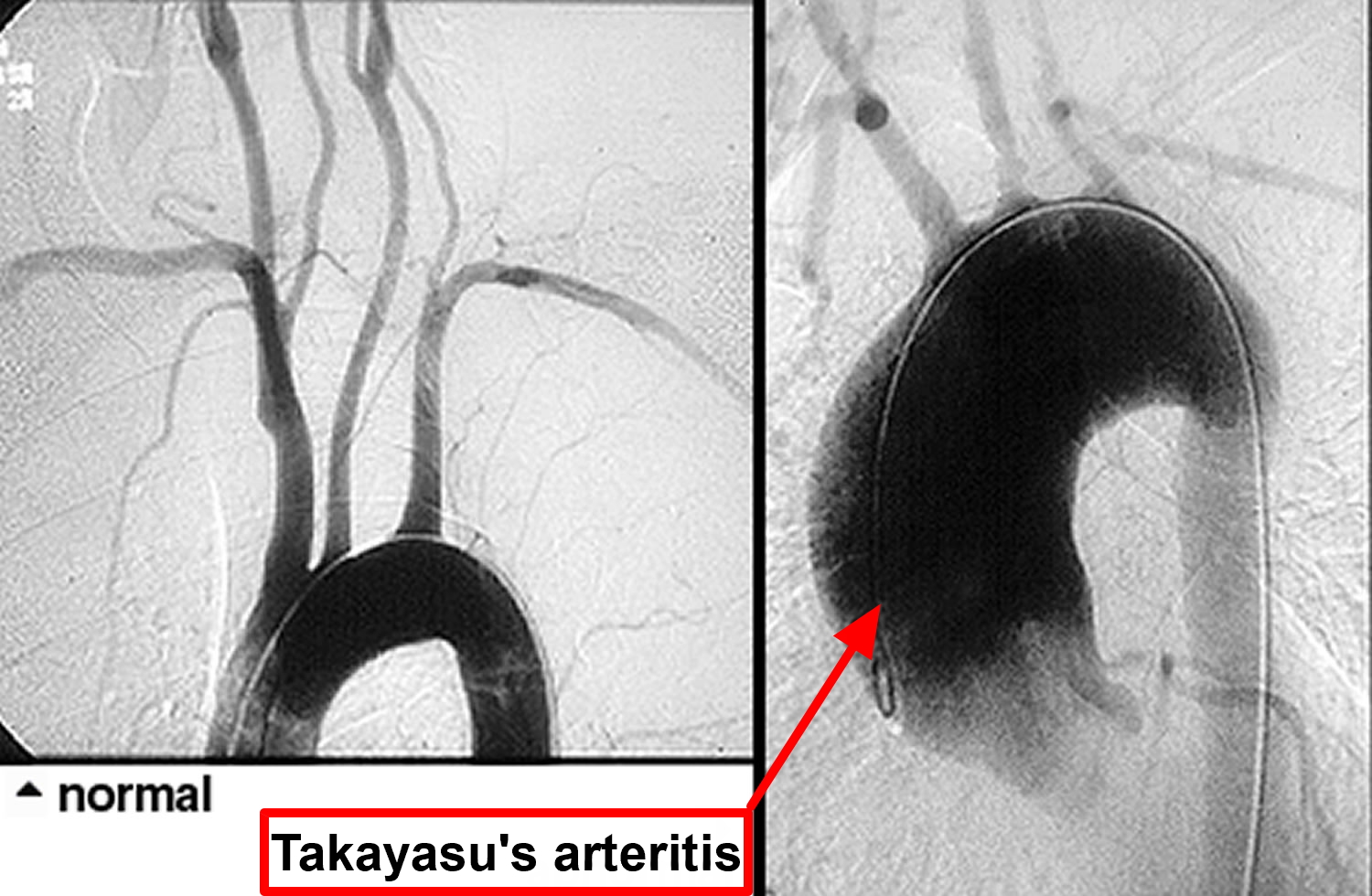
Takayasu’s arteritis is a rare type of vasculitis, a group of disorders that cause blood vessel inflammation. In Takayasu’s arteritis, the inflammation damages the aorta — the large artery that carries blood from your heart to the rest of your body and its main branches. Takayasu’s arteritis is occasionally called “pulseless disease”, because of the difficulty in detecting peripheral pulses that sometimes occurs as a result of the vascular narrowings.
The first case of Takayasu’s arteritis was described in 1908 by Dr. Mikito Takayasu at the Annual Meeting of the Japan Ophthalmology Society. Dr. Takayasu described a peculiar “wreathlike” appearance of blood vessels in the back of the eye (retina). It is now known that the blood vessel malformations that occur in the retina are a response (new blood vessel growth) to arterial narrowings in the neck, and that the absence of pulses noted in some patients occur because of narrowings of blood vessels to the arms.
Takayasu’s arteritis can lead to blockages or narrowed arteries (stenosis) or abnormally dilated arteries (aneurysms). Takayasu’s arteritis can also lead to arm or chest pain and high blood pressure and eventually to heart failure or stroke.
The “typical” patient with Takayasu’s arteritis is a woman under the age of 40. There is a 9:1 female predominance in this disease. Although the disease has a worldwide distribution, it appears to occur more often in Asian women.
Takayasu’s arteritis is a rare disease. The best estimates of the disease frequency suggest that 2 or 3 cases occur each year per million people in a population.
If you don’t have symptoms, you may not need treatment. Or you may need medications to control the inflammation in the arteries and prevent complications. But even with treatment, relapses are common.
Figure 2. Takayasu’s arteritis
Takayasu’s arteritis symptoms
Takayasu’s arteritis is a chronic inflammatory condition that affects the largest blood vessel in the body (the aorta) and its branches. Thus, the complications of Takayasu’s arise directly or indirectly from damage to these blood vessels. The vasculitides are classified according to the size of blood vessel involved. Takayasu’s is the classic “large vessel” vasculitis.
Clinicians divide Takayasu’s arteritis into two phases: 1) a systemic phase; and 2) an occlusive phase. Although these two phases are not always distinct (i.e., patients may have features of both phases at the same time), this division is a useful way of thinking about the disease.
Stage 1 Systemic phase Takayasu’s arteritis
In the systemic phase, patients have symptoms and signs of an active inflammatory illness. These may include “constitutional symptoms” (fever, fatigue, weight loss), arthritis, and non-specific aches and pains. There may be tenderness overlying affected arteries. Most patients have elevations of the erythrocyte sedimentation rate during the systemic phase.
The systemic phase is succeeded by the occlusive phase, during which patients begin to develop symptoms caused by the narrowing of affected arteries.
In the first stage, you’re likely to feel unwell with:
- Fatigue
- Unintended weight loss
- General aches and pains
- Mild fever
Not everyone has these early signs and symptoms. It’s possible for inflammation to damage arteries for years before you realize something is wrong.
Stage 2 Occlusive phase Takayasu’s arteritis
During the second stage, inflammation is causing arteries to narrow so less blood, oxygen and nutrients reach your organs and tissues. Stage 2 signs and symptoms may include:
- Weakness or pain in your limbs with use
- Lightheadedness, dizziness or fainting
- Headaches
- Memory problems
- Trouble thinking
- Shortness of breath
- Visual changes
- High blood pressure
- Difference in blood pressure between your arms
- Decreased pulse
- Too few red blood cells (anemia)
- Chest pain
- Noises heard over the arteries (bruits) when listening with a stethoscope
The narrowing of affected arteries may cause pain in your limbs that occurs during repetitive activities (“claudication”), such as pain in the arm that occurs while using a handsaw or pain in the calves brought on by walking. The symptoms also include dizziness upon standing up, headaches, and visual problems. During the occlusive phase, affected blood vessels may be narrowed to such an extent that the normal arterial pulsations (“pulses”) in the neck, elbow, wrist, or lower extremities cannot be felt. Using a stethoscope, one may also hear “bruits”, a harsh, “whooshing” sounds made by the flow of blood through abnormally narrowed vessels. High blood pressure is common, but blood pressures taken in the arms may be read as falsely low if there is a narrowing of an artery high up in the arm. With some patients, it is not possible to get accurate blood pressure readings in the arms. Using an ophthalmoscope, a physician may observe characteristic malformations of blood vessels that occur in advanced cases of Takayasu’s arteritis.
Although the lung involvement in Takayasu’s is frequently overshadowed by involvement of systemic large blood vessels, the pulmonary arteries may also be affected in this disorder.
Takayasu’s arteritis causes
No one knows exactly what causes the initial inflammation in Takayasu’s arteritis. Some evidence suggests that an infection of some kind — viral, bacterial, or other — occurring in a person with other predisposing factors (such as the correct genes), may lead to this disease. This is an attractive hypothesis, but definitive evidence for it is lacking. It’s likely that the condition is an autoimmune disease in which your immune system attacks your own arteries by mistake. The disease may be triggered by a virus or other infection.
With Takayasu’s arteritis, the aorta and other major arteries, including those leading to your head and kidneys, become inflamed. Over time the inflammation causes changes in these arteries, including thickening, narrowing and scarring.
Risk factors for Takayasu’s arteritis
Takayasu’s arteritis primarily affects girls and women between the ages of 10 and 40. The disorder occurs worldwide, but it’s most common in Asia. Sometimes the condition runs in families.
Takayasu’s arteritis complications
With Takayasu’s arteritis, extended or recurring cycles of inflammation and healing in the arteries might lead to one or more of the following complications:
- Hardening and narrowing of blood vessels, which can cause reduced blood flow to organs and tissues
- High blood pressure, usually as a result of decreased blood flow to your kidneys
- Inflammation of the heart, which may affect the heart muscle (myocarditis) or the heart valves
- Heart failure due to high blood pressure, myocarditis or aortic regurgitation — a condition in which a faulty aortic valve allows blood to leak back into your heart — or a combination of these
- Stroke, which occurs as a result of reduced or blocked blood flow in arteries leading to your brain
- Transient ischemic attack (TIA), is like a stroke, producing similar symptoms but causing no permanent damage
- Aneurysm in the aorta, which occurs when the walls of the blood vessel weaken and stretch out, forming a bulge that has the potential to rupture
- Heart attack, which may occur as a result of reduced blood flow to the heart
Takayasu’s arteritis and Pregnancy
A healthy pregnancy is possible for women with Takayasu’s arteritis. But the disease and drugs used to treat it can affect your fertility and pregnancy. If you have Takayasu’s arteritis and are planning on becoming pregnant, work with your doctor to develop a plan to limit complications of pregnancy before you conceive. And during your pregnancy see your doctor regularly for checkups.
Takayasu’s arteritis diagnosis
Making the diagnosis of Takayasu’s arteritis can be extremely difficult. Unfortunately it is very common for the disease to smoulder in the walls of large blood vessels for years, causing only non-specific symptoms associated with the systemic phase of the illness (or no symptoms), until a major complication results. These major complications may include dilation of the aorta with “stretching” of the aortic valve in the heart; critically reduced blood flow to an arm or leg; a stroke caused by high blood pressure in vessels of the brain, and many others.
Your doctor will ask you about your signs and symptoms, conduct a physical exam, and take your medical history. He or she may also have you undergo some of the following tests and procedures to help rule out other conditions that resemble Takayasu’s arteritis and to confirm the diagnosis. Some of these tests may also be used to check on your progress during treatment.
- Blood tests. These tests can be used to look for signs of inflammation, such as a high level of C-reactive protein or a high erythrocyte sedimentation rate — commonly referred to as a sed rate. Your doctor may also check for anemia.
- X-rays of your blood vessels (angiography). During an angiogram, a flexible catheter is inserted into a large artery or vein. A special dye (contrast medium) is then injected into the catheter, and X-rays are taken as the dye fills your arteries or veins. The resulting images allow your doctor to see if blood is flowing normally or if it’s being slowed or interrupted due to narrowing (stenosis) of a blood vessel. A person with Takayasu’s arteritis generally has several areas of stenosis.
- Magnetic resonance angiography (MRA). This less invasive form of angiography produces detailed images of your blood vessels without the use of catheters or X-rays, although an intravenous contrast medium generally is used. MRA works by using radio waves in a strong magnetic field to produce data that a computer turns into detailed images of tissue slices.
- Computerized tomography (CT) angiography. This is another noninvasive form of angiography combining computerized analysis of X-ray images with the use of intravenous contrast dye to allow your doctor to check the structure of your aorta and its nearby branches and to monitor blood flow.
- Ultrasonography. Doppler ultrasound, a more sophisticated version of the common ultrasound, has the ability to produce very high-resolution images of the walls of certain arteries, such as those in the neck (carotid arteries) and those in the shoulder (subclavian arteries). It may be able to detect subtle changes in these arteries before other imaging techniques can.
- Positron emission tomography (PET). This imaging is able to measure the intensity of inflammation in blood vessels. Before the scan, you are given a radioactive drug (tracer).
Unlike other types of vasculitis, Takayasu’s arteritis is not usually diagnosed by the removal and analysis of tissue (biopsy).
Once the diagnosis is suspected, it is usually confirmed by a radiographic procedure such as an angiogram or a magnetic resonance imaging study demonstrating significant large artery disease consistent with Takayasu’s arteritis. In some cases in which blood vessel damage is so severe as to necessitate surgery to repair the aortic valve, the aorta, or some other large blood vessel, physicians are able to make unequivocal diagnoses by looking at tissue from the involved blood vessels under the microscope. Takayasu’s arteritis is pathologically indistinguishable from giant cell arteritis/temporal arteritis. In both, destruction of the blood vessel wall and giant cells are frequently present.
Takayasu’s arteritis treatment
Treatment of Takayasu’s arteritis focuses on controlling the inflammation with medications and preventing further damage to your blood vessels. The disease can sometimes be difficult to treat because even if you appear to be in remission the disease might still be active. In addition, by the time some people are diagnosed, it’s possible that irreversible damage has already occurred.
On the other hand, if you don’t have a lot of signs and symptoms or serious complications, you may not need treatment at all.
One of the biggest problems confronting Takayasu’s patients and the physicians who care for them is determining how active the disease is. This can be an exceptionally challenging problem. The erythrocyte sedimentation rate (ESR) probably remains the most reliable marker of disease activity, but even this test is not helpful in a sizeable number of patients who have active arterial inflammation but normal ESRs. Because the treatments for Takayasu’s arteritis may be associated with substantial side–effects, scientists and doctors need more accurate means of gauging Takayasu’s arteritis disease activity.
Medications
Talk with your doctor about the drug or drug combinations that are options for you and what the possible side effects are. Your doctor may prescribe:
- Corticosteroids to control inflammation. The first line of treatment is usually with a corticosteroid, such as prednisone. The great majority of patients with Takayasu’s arteritis respond to prednisone. The usual starting dose is approximately 1 milligram per kilogram of body weight per day (for most people, this is approximately 60 milligrams a day). Because of the significant side–effects of long-term high–dose prednisone use, the starting dose is tapered over several weeks to a dose that the physician feels is tolerable for the patient. Even if you soon start feeling better, you may need to continue taking the drug long term. After the first month, your doctor may gradually begin to lower the dose until you reach the lowest dose you need to control inflammation. Some of your symptoms may return during this tapering period. Possible side effects of corticosteroids include weight gain, increased risk of infections, bone thinning (osteoporosis) and menstrual irregularities.
For long–term treatment in addition to prednisone (as “steroid sparing agents”), methotrexate, azathioprine, and even cyclophosphamide are sometimes used. There have been few studies of the use of these medications in this disease.
- Other drugs that suppress the immune system. If your condition doesn’t respond well to corticosteroids or you have trouble tapering off the medication, your doctor may prescribe immunosuppressant drugs. Examples are methotrexate (Trexall) and azathioprine (Azasan, Imuran). Some people respond well to medications that were developed for people receiving organ transplants. These drugs, including mycophenolate mofetil (CellCept), work by suppressing the immune system, and there is some evidence that they may be helpful with corticosteroids in effectively reducing blood vessel inflammation in people with Takayasu’s arteritis. The most common side effect is an increased risk of infection.
- Medications to regulate the immune system. If you don’t respond to standard treatments, your doctor may suggest drugs that correct abnormalities in the immune system (biologics). Examples are etanercept (Enbrel) and infliximab (Remicade). Small studies have found these medications effective at controlling signs and symptoms, as well as at reducing the need for corticosteroid treatments. In addition, tocilizumab (Actemra) has been reported to be beneficial in treating Takayasu’s arteritis. More research is needed. The most common side effect with these drugs an increased risk of infection.
Surgery
If your arteries become severely narrowed or blocked, you may need surgery to open or bypass these arteries to allow an uninterrupted flow of blood. Often this helps to improve certain symptoms, such as high blood pressure and chest pain. In some cases, though, narrowing or blockage may recur, requiring a second procedure. Also, if you develop large aneurysms, surgery may be needed to prevent them from rupturing. Your doctor may suggest holding off surgery until your condition is in remission.
Surgical options, which are best performed when inflammation of the arteries has been reduced, include:
- Bypass surgery. In this procedure, an artery or a vein is removed from a different part of your body and attached to the blocked artery, providing a bypass for blood to flow through.
- Blood vessel widening (percutaneous angioplasty). During this procedure, a tiny balloon is threaded through a blood vessel and into the affected artery. Once in place, the balloon is expanded to widen the blocked area, then it’s deflated and removed.
- Aortic valve surgery. Surgical repair or replacement of the aortic valve may be needed if the valve is leaking significantly (aortic valve regurgitation).
Living with Takayasu’s arteritis
One of the greatest challenges of living with Takayasu’s arteritis may be coping with side effects of your medication. The following suggestions may help:
- Understand your condition. Learn everything you can about Takayasu’s arteritis and its treatment. Know the possible side effects of the drugs you take, and tell your doctor about any changes in your health. Ask your doctor about the benefit of taking low-dose aspirin regularly.
- Eat a healthy diet. Eating well can help prevent potential problems that can result from your condition and medications, such as high blood pressure, thinning bones and diabetes. Emphasize fresh fruits and vegetables, whole grains, and lean meats and fish, while limiting salt, sugar and alcohol. If you’re taking a corticosteroid drug, ask your doctor if you need to take a vitamin D or calcium supplement.
- Exercise regularly. Regular aerobic exercise, such as walking, can help prevent bone loss, high blood pressure and diabetes. It also benefits your heart and lungs. In addition, many people find that exercise improves their mood and overall sense of well-being.
- Avoid all tobacco products. It’s important to stop using all forms of tobacco to reduce the risk of injuring your blood vessels and tissues even more.





{kind=link}