Contents
- What is astrocytoma
- Pilocytic astrocytoma or juvenile pilocytic astrocytoma
- Diffuse astrocytoma
- Anaplastic astrocytoma
- Glioblastoma or Astrocytoma grade 4
- Subependymal giant cell astrocytomas
- Optic gliomas
- Astrocytoma prognosis
- Astrocytoma survival rates
- Astrocytoma causes
- Astrocytoma brain tumor symptoms
- Astrocytoma diagnosis
- Astrocytoma treatment
What is astrocytoma
An astrocytoma is a brain tumor that starts in cells called astrocytes, star-shaped cells that make up the “glue-like” or supportive tissue of the brain. Other supportive cells of the brain include oligodendrocytes and ependymal cells. Collectively, these cells are known as glial cells and the tissue they form is known as glial tissue. Tumors that arise from the glial tissue, including astrocytomas, are collectively referred to as gliomas. Astrocytomas can appear in various parts of the brain and nervous system, including the cerebellum, the cerebrum, the central areas of the brain, the brainstem, and the spinal cord. Astrocytoma tumors of the spinal cord are rare, occurring with an incidence of 0.8 to 2.5 cases per 100,000 per year. The average age at diagnosis is between 35 and 40 years.
The World Health Organization (WHO) classifies astrocytomas into four grades depending on how fast they are growing and the likelihood that they will spread (infiltrate) to nearby brain tissue. Non-infiltrating astrocytomas usually grow more slowly than the infiltrating forms. Infiltrating, or diffuse astrocytomas are more common than non-infiltrating astrocytomas. They are generally more common in men and are most common in the cerebral hemispheres of adult patients. In children they occur both in the cerebral hemispheres as well as the brain stem. Tumors from oligodendrocytes (oligodendrogliomas) are also in the category of infiltrating gliomas and can occasionally be difficult to distinguish from astrocytomas. Some infiltrating gliomas are categorized as mixed oligodendroglioma-astrocytoma (oligoastrocytoma).
- Astrocytoma grade 1 is usually a non-infiltrating tumor. The most common type of grade I astrocytoma is pilocytic astrocytoma which is also known as juvenile pilocytic astrocytoma or JPA. This tumor grows slowly but can become very large. Pilocytic astrocytoma occurs most often in the cerebellum, cerebrum, optic nerve pathway and brainstem. This tumor occurs most often in children and teens and accounts for 2% of all brain tumors.
- Astrocytoma grade 2 is also called low-grade astrocytoma or diffuse astrocytoma and is usually an infiltrating tumor. This tumor grows relatively slowly and usually does not have well-defined borders. It occurs most often in adults between the ages of 20 and 40.
- Astrocytoma grade 3 is also called anaplastic (malignant) astrocytoma because this tumor grows more quickly than a grade II astrocytoma. Anaplastic astrocytoma occurs most often in adults between the ages of 30 and 50, and accounts for 4% of all brain tumors.
- Astrocytoma grade 4 is also called glioblastoma or GBM (glioblastoma multiforme) and is the most aggressive type of nervous system tumor. It is also referred to as glioblastoma multiforme because of its wide variety of appearances under the microscope. Rarely, non-glial tissue elements can exist in a glioblastoma. The most common variant of glioblastoma multiforme showing these additional tissue elements is called a mixed glioblastoma-sarcoma, or gliosarcoma. Glioblastoma multiforme occurs most often in adults between the ages of 50 and 80, is more common in men, and accounts for 23% of all primary brain tumors.
Low-grade astrocytomas are usually localized and grow slowly. High-grade astrocytomas grow at a rapid pace and require a different course of treatment. Most astrocytoma tumors in children are low grade. In adults, the majority are high grade.
- Grade 1 astrocytoma (Pilocytic astrocytoma) occurs most often in children and teens and account for 2% of all brain tumors.
- Grade 2 astrocytoma (Diffuse astrocytoma) occurs most often in adults between the ages of 20 and 60.
- Grade 3 astrocytoma (Anaplastic astrocytoma) occurs most often in adults between the ages of 30 and 60, is more common in men and accounts for 4% of all brain tumors.
- Grade 4 astrocytoma (Glioblastoma) occurs most often in adults between the ages of 50 and 80, is more common in men and accounts for 23% of all primary brain tumors.
Most astrocytomas can spread widely throughout the brain and blend with the normal brain tissue, which can make them very hard to remove by surgery. Sometimes astrocytomas spread along the cerebrospinal fluid (CSF) pathways. It is very rare for them to spread outside of the brain or spinal cord.
Recently several markers have been identified in diffuse gliomas. Astrocytomas grades 2 (diffuse astrocytoma) and 3 (anaplastic astrocytoma) often have acquired mutations in a gene called IDH1. These mutations are acquired by the tumor and are not generally present in the normal cells of the patient. The presence of an IDH1 mutation in an astrocytoma is generally associated with an improved prognosis compared to an astrocytoma of similar grade that does not have an IDH1 mutation. A second marker, relevant to glioblastoma multiforme (GBM), is MGMT methylation. When present, MGMT methylation may be associated with better response to chemotherapy (usually temozolomide) compared to glioblastoma multiformes without MGMT methylation.
Pilocytic astrocytoma or juvenile pilocytic astrocytoma
Pilocytic astrocytomas (astrocytoma grade 1 or juvenile pilocytic astrocytoma) are slow growing and rarely infiltrate nearby tissues. Pilocytic astrocytomas generally form sacs of fluid (cysts), or may be enclosed within a cyst. Although they are usually slow-growing, these tumors can become very large. They most commonly occur in the cerebellum but can also begin in the optic nerve, hypothalamus, brain stem, or other areas. They account for nearly 1 out of 5 brain tumors in children. Juvenile pilocytic astrocytomas are typically seen in children and young adults. Most juvenile pilocytic astrocytomas develop within the first two decades of life. Juvenile pilocytic astrocytomas affect males and females in equal numbers.
Juvenile pilocytic astrocytomas are the most common cerebellar tumor in children. Astrocytomas as a whole are the most common brain tumor of childhood accounting for more than half of all primary childhood tumors of the central nervous system. The incidence rate is estimated at 14 new cases per million in children younger than 15 years of age. Most astrocytomas (approximately 80 percent) in children are low grade.
The symptoms associated with juvenile pilocytic astrocytomas vary depending upon the size and location of the tumor. A juvenile pilocytic astrocytoma can develop anywhere with the central nervous system (i.e., brain and spinal cord). Most cases arise in the lower area of brain near the back of the neck that controls movement and balance (cerebellum), the brainstem, the hypothalamic region or the optic nerve pathways.
The most common finding associated with a juvenile pilocytic astrocytoma is increased pressure within the brain, which may be caused by the tumor itself or by blockage of the fluid-filled spaces in the brain called ventricles, which results in the abnormal accumulation of cerebrospinal fluid (CSF) in the brain. Symptoms commonly associated with increased pressure on the brain include headaches, lethargy or drowsiness, vomiting, and changes in personality or mental status. In some cases, a juvenile pilocytic astrocytoma may also be associated with seizures, vision problems such as blurred vision or double vision (diplopia), gradual changes in behavior or mood, and weakness of the arms and legs resulting in coordination difficulties.
A juvenile pilocytic astrocytoma in the brainstem may be associated with nausea, vomiting, an impaired ability to coordinate voluntary movements (ataxia), and wryneck (torticollis). Ocular symptoms including swelling of the optic disc (papilledema) and involuntary rapid eye movements (nystagmus) may also occur. In some cases, paralysis (palsy) of the sixth and seventh cranial nerves may develop.
A juvenile pilocytic astrocytoma in the optic nerve pathways may be associated with loss of vision, degeneration (atrophy) of the optic nerve, papilledema, nystagmus, and protrusion of the eyeball (proptosis).
A juvenile pilocytic astrocytoma in the hypothalamic region may be associated with weight gain or loss, premature puberty or diencephalic syndrome, which is characterized by failure to thrive, abnormal thinness, irritability, and eye abnormalities.
Diffuse astrocytoma
Low-grade astrocytomas (astrocytoma grade 2 or diffuse astrocytoma): are also slow-growing tumors but with the important characteristic of growing into nearby tissues, which makes them hard to remove with surgery. Diffuse Astrocytomas tend to contain microcysts and mucous-like fluid. They are grouped by the appearance and behavior of the cells for which they are named. Diffuse astrocytomas are the most common type in children. Some special types, known as non-infiltrating astrocytomas, tend to grow very slowly and do not grow into (infiltrate) nearby tissues, so they often have a good prognosis. Though these tumors are thought of as low grade, they tend to become more aggressive and fast growing over time.
Anaplastic astrocytoma
Anaplastic astrocytoma is a grade 3 astrocytoma tumor. Anaplastic astrocytomas tend to have tentacle-like projections that grow into surrounding tissue, making them difficult to completely remove during surgery. These rare anaplastic astrocytomas require more aggressive treatment than more benign pilocytic astrocytoma. Anaplastic astrocytomas tend to grow quickly and spread into the surrounding normal brain tissue.
Anaplastic astrocytomas affect males slightly more often than females. The exact incidence of these tumors is unknown. Anaplastic astrocytoma and glioblastoma multiforme (astrocytoma grade 4) are estimated to affect 5-8 people per 100,000 in the general population. Anaplastic astrocytomas are more common in adults than children. In adults, anaplastic astrocytomas usually develop between 30 and 50 years of age. Astrocytomas and a related tumor (oligodendroglioma) are the most common primary brain tumors in adults.
In children, anaplastic astrocytomas usually develop between 5 and 9 years of age. Malignant astrocytomas (i.e., anaplastic astrocytoma and glioblastoma multiforme) account for approximately 10 percent of childhood central nervous stem tumors. Astrocytomas as a whole account for more than half of all primary childhood tumors of the central nervous system.
The symptoms of anaplastic astrocytoma vary depending upon the exact location and size of the tumor. Most symptoms result from increased pressure within the brain. An anaplastic astrocytoma usually develops slowly over time, but may develop rapidly.
Increased pressure within the brain may be caused by the tumor itself or by blockage of the fluid-filled spaces in the brain called ventricles, which results in the abnormal accumulation of cerebrospinal fluid (CSF) in the brain. Symptoms commonly associated with anaplastic astrocytomas include headaches, lethargy or drowsiness, vomiting, and changes in personality or mental status. In some cases, seizures, vision problems, weakness of the arms and legs resulting in coordination difficulties may also occur.
More specific symptoms relate to the area of brain where the tumor is located. Anaplastic astrocytomas may develop in any area of the central nervous system, although there is a strong preference for the large rounded portion of the brain (cerebrum) that occupies most of the skull. The cerebrum is divided into two halves known as the cerebral hemispheres. Anaplastic astrocytomas may develop in the frontal, temporal, parietal and occipital lobes of the cerebrum.
A tumor in the frontal lobe may cause memory problems, changes in personality and mood, and paralysis (hemiplegia) on the side of the body opposite of the tumor. Tumors in the temporal lobe may cause seizures, memory problems, and problems with coordination and speech. Tumors in the parietal lobe may cause difficulties with communication through writing (agraphia), problems with fine motor skills, or sensory abnormalities such as tingling or burning sensations (paresthesias). Tumors in the occipital lobe can cause visual loss.
Other common sites for anaplastic astrocytomas include the part of the brain that contains the thalamus and hypothalamus (diencephalon), the lower area of brain near the back of the neck that controls movement and balance (cerebellum), and the spinal cord. Tumors in the diencephalon region may cause headaches, fatigue, weakness of the arms and legs, vision problems, and hormonal imbalances. Tumors in the cerebellum may cause headaches, changes in personality or behavior, and balance problems. Tumors of spinal cord may cause back pain, sensory abnormalities such as tingling or burning sensations (paresthesias), weakness, and gait disturbances.
Glioblastoma or Astrocytoma grade 4
Astrocytoma grade 4 (also called Glioblastoma, previously named “Glioblastoma Multiforme,” “Grade IV Glioblastoma,” and “GBM”) is the fastest growing astrocytoma. Astrocytoma grade 4 (glioblastoma) is the most common malignant primary brain tumor accounting for approximately 50 percent of cases of primary brain tumors (i.e. excluding diseases that metastasize to the brain from other sites in the body). There are two types of astrocytoma grade 4—primary, or de novo, and secondary. Primary tumors are very aggressive and the most common form of astrocytoma grade 4. The secondary tumors are those which originate as a lower-grade astrocytoma tumor and evolve into a grade 4 tumor.
Astrocytomas grade 4 (glioblastomas) are often aggressive and infiltrate surrounding brain tissue. Astrocytomas grade 4 (glioblastomas) arise from glial cells, which are cells that form the tissue that surrounds and protects other nerve cells found within the brain and spinal cord.
Astrocytoma grade 4 (glioblastoma) affects males slightly more often than females and adults more often than children. Most cases develop in individuals between 40 and 60 years of age. Astrocytoma grade 4 (glioblastoma) accounts for approximately 3-4 percent of primary childhood brain tumors. The incidence is estimated to be 2-3 people per every 100,000 in the United States and most European countries.
The symptoms of astrocytoma grade 4 (glioblastoma) vary depending upon the exact location and size of the tumor. Most symptoms result from increased pressure within the brain.
Increased pressure within the brain may be caused by the tumor itself or by blockage of the fluid-filled spaces in the brain called ventricles, which results in the abnormal accumulation of cerebrospinal fluid (CSF) in the brain. Symptoms associated with increased pressure within the brain include headaches, lethargy or drowsiness, nausea, vomiting, and changes in personality or mental status. In some cases, seizures, vision problems, loss of previously acquired speech and language skills (aphasia), and weakness of the arms and legs resulting in coordination difficulties may also occur.
Astrocytomas grade 4 (glioblastomas) may grow rapidly and infiltrate nearby normal brain tissue, eventually causing life-threatening complications. Astrocytomas grade 4 (glioblastomas) usually do not spread outside of the central nervous system, although it can happen in extremely rare cases.
Subependymal giant cell astrocytomas
Subependymal giant cell astrocytomas (SEGAs) occur in the ventricles. They are also slow growing and rarely infiltrate nearby tissues. These tumors are almost always linked with an inherited condition called tuberous sclerosis.
Optic gliomas
Optic gliomas are low-grade astrocytomas that start in the optic nerves (the nerves leading from the eyes to the brain). They are often linked with an inherited condition called neurofibromatosis type 1. These tumors are rarely fatal, but they may cause vision loss and injury to nearby brain tissue.
Figure 1. Human brain
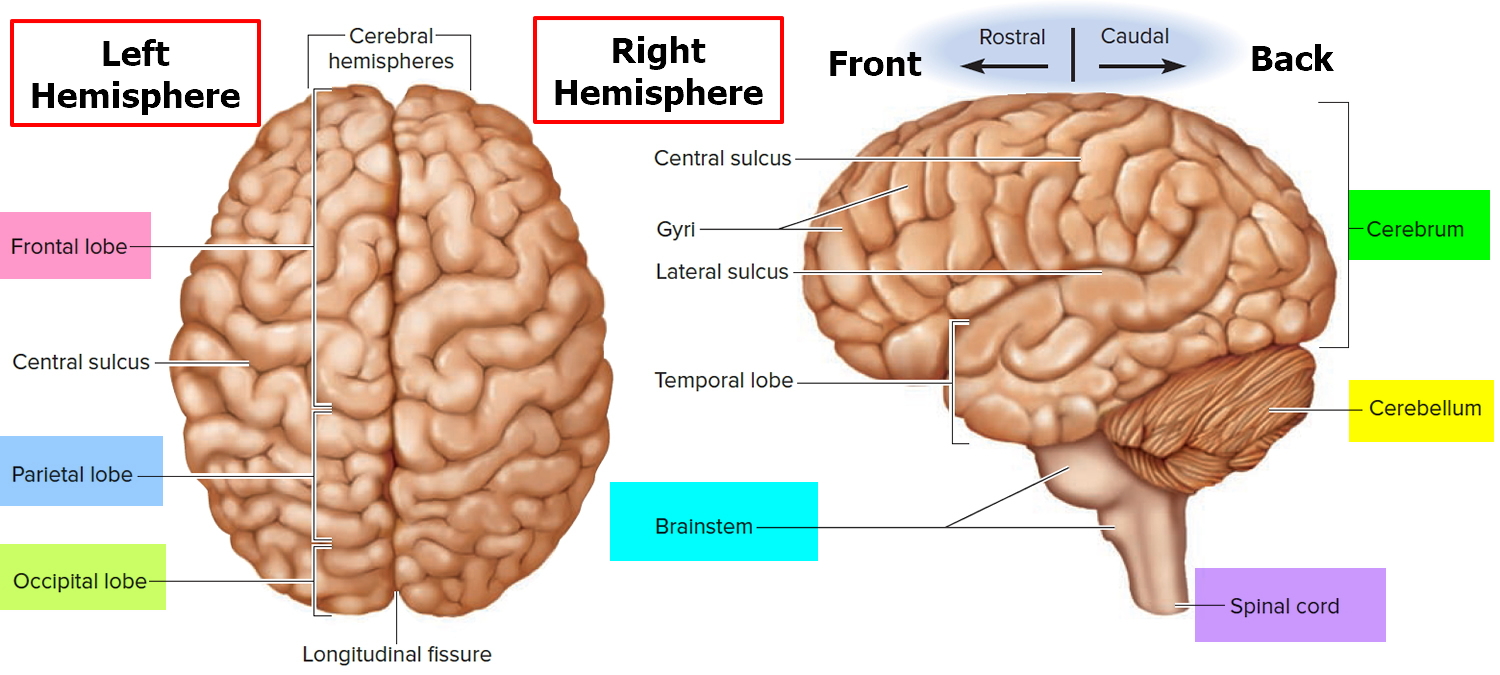
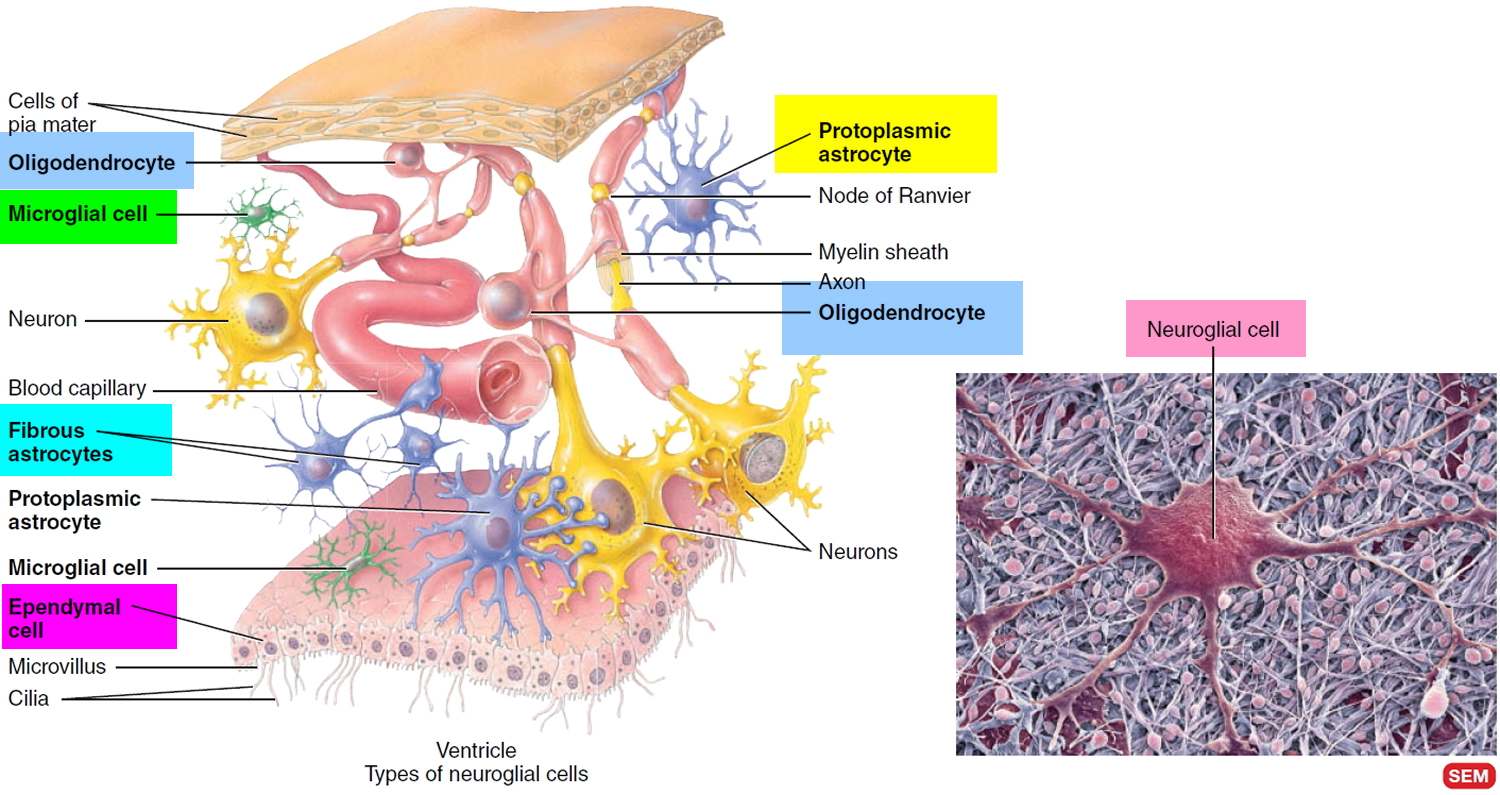
Figure 2. Glia cells (Neuroglia) of the brain and spinal cord (CNS)
Astrocytoma prognosis
A number of factors will influence outlook. These include the grade of the astrocytoma brain tumor (1 to 4), and its location within the brain.
The outlook for low grade astrocytoma brain tumors is generally good with 60-95% rate at 10 years. High grade astrocytomas tend to have a poorer outlook, with survival at 10 years being less than 30%; brain tumor patients who survive are often afflicted by some degree of motor, cognitive or endocrine dysfunction.
Brain tumors involving certain areas tend to carry a worse prognosis; for instance involvement of the visual pathways has a poorer 10 year survival rate, as well as an increased incidence of sustained visual deficits.
The overall 5-year survival rate for patients with spinal cord astrocytomas is about 50%. 5-year survival is approximately 70-90% for patients with low-grade astrocytomas, and 30% for those with high-grade astrocytomas.
Astrocytoma survival rates
The 5-year survival rate refers to the percentage of children who live at least 5 years after their cancer is diagnosed. Of course, many children live much longer than 5 years (and many are cured).
The numbers below come from the Central Brain Tumor Registry of the United States (CBTRUS) and are based on children aged 19 or younger who were treated between 1995 and 2010. There are some important points to note about these numbers:
- These numbers are for some of the more common types of tumors. Numbers are not readily available for all types of tumors that occur in children, often because they are rare or are hard to classify.
Table 1. Astrocytoma survival rates
| Type of Tumor | 5-Year Survival Rate |
| Pilocytic astrocytoma (Astrocytoma grade 1) | About 95% |
| Fibrillary (diffuse) astrocytoma (Astrocytoma grade 2) | About 80% to 85% |
| Anaplastic astrocytoma (Astrocytoma grade 3) | About 30% |
| Glioblastoma (Astrocytoma grade 4) | About 20% |
Note: Survival rates are often based on previous outcomes of large numbers of children who had the disease, but they can’t predict what will happen in any particular child’s case. Knowing the type of a child’s brain tumor is important in estimating their outlook. But many other factors can also affect a child’s outlook, such as the location and extent of the tumor and how well it responds to treatment. Even taking these other factors into account, survival rates are at best rough estimates. Your child’s doctor knows your child’s situation and is your best source of information on this topic.
[Source 1]Astrocytoma causes
The cause of most astrocytomas is not known. Researchers speculate that genetic and immunologic abnormalities, environmental factors (e.g., exposure to ultraviolet rays, certain chemicals, ionizing radiation), diet, stress, and/or other factors may play contributing roles in causing specific types of cancer. Investigators are conducting ongoing basic research to learn more about the many factors that may result in cancer. Researchers believe that some individuals may have a genetic predisposition to developing an astrocytoma. A person who is genetically predisposed to a disorder carries a gene (or genes) for the disease, but it may not be expressed unless it is triggered or “activated” under certain circumstances, such as due to particular environmental factors.
Astrocytomas occur with greater frequency with certain genetic disorders including Turcot syndrome, neurofibromatosis type-I tuberous sclerosis, Ollier’s disease and Li-Fraumeni syndrome.
In general, this brain tumour occur with equal frequency in males and females. There does not appear to be significant variation between ethnic groups. The majority of cases occur in children under the age of 10 years.
Research has not identified significant links between parental and environmental exposures and the risk of future development of this type of brain tumor.
Astrocytoma brain tumor symptoms
Headaches, seizures, memory loss, and changes in behavior are the most common early symptoms of astrocytoma. Other symptoms may occur depending on the size and location of the tumor.
Symptoms of grade 1 and grade 2 astrocytomas are subtle because the brain is able to temporarily adapt to the presence of a slow-growing tumor. Symptoms of grade 3 and grade 4 astrocytomas may be sudden and debilitating. Symptoms can result from increased pressure within the brain and may include headaches, vision changes and nausea or vomiting. Symptoms may also occur based on the location of the tumor due to interference with normal brain function and include focal seizures, difficulty with speaking, loss of balance and weakness, paralysis or loss of sensation of one side of the body. Fatigue and depression are common in individuals with an astrocytoma.
Symptoms commonly associated with anaplastic astrocytomas include headaches, lethargy or drowsiness, vomiting, and changes in personality or mental status. In some cases, seizures, vision problems, weakness of the arms and legs resulting in coordination difficulties may also occur.
Desmoplastic infantile astrocytoma is a very rare grade 1 astrocytoma. This tumor tends to occur the cerebral hemispheres and is usually diagnosed in children less than two years of age. Symptoms may include an increased head size, bulging soft spots (fontanelles) in the skull, eyes that focus downward and seizures. A related tumor, desmoplastic infantile ganglioglioma, is a mixed astrocytic and neuronal tumor, but is otherwise similar to desmoplastic infantile astrocytoma.
Subependymal giant cell astrocytoma occurs in the ventricles of the brain and is almost always associated with a genetic condition called tuberous sclerosis. Other rare neuroepithelial tumors include pleomorphic xanthoastrocytoma and ganglioglioma (a mixed glial-neuronal tumor).
Astrocytoma diagnosis
Tests and procedures used to diagnose astrocytoma include:
- Neurological exam. During a neurological exam, your doctor will ask you about your signs and symptoms. He or she may check your vision, hearing, balance, coordination, strength and reflexes. Problems in one or more of these areas may provide clues about the part of your brain that could be affected by a brain tumor.
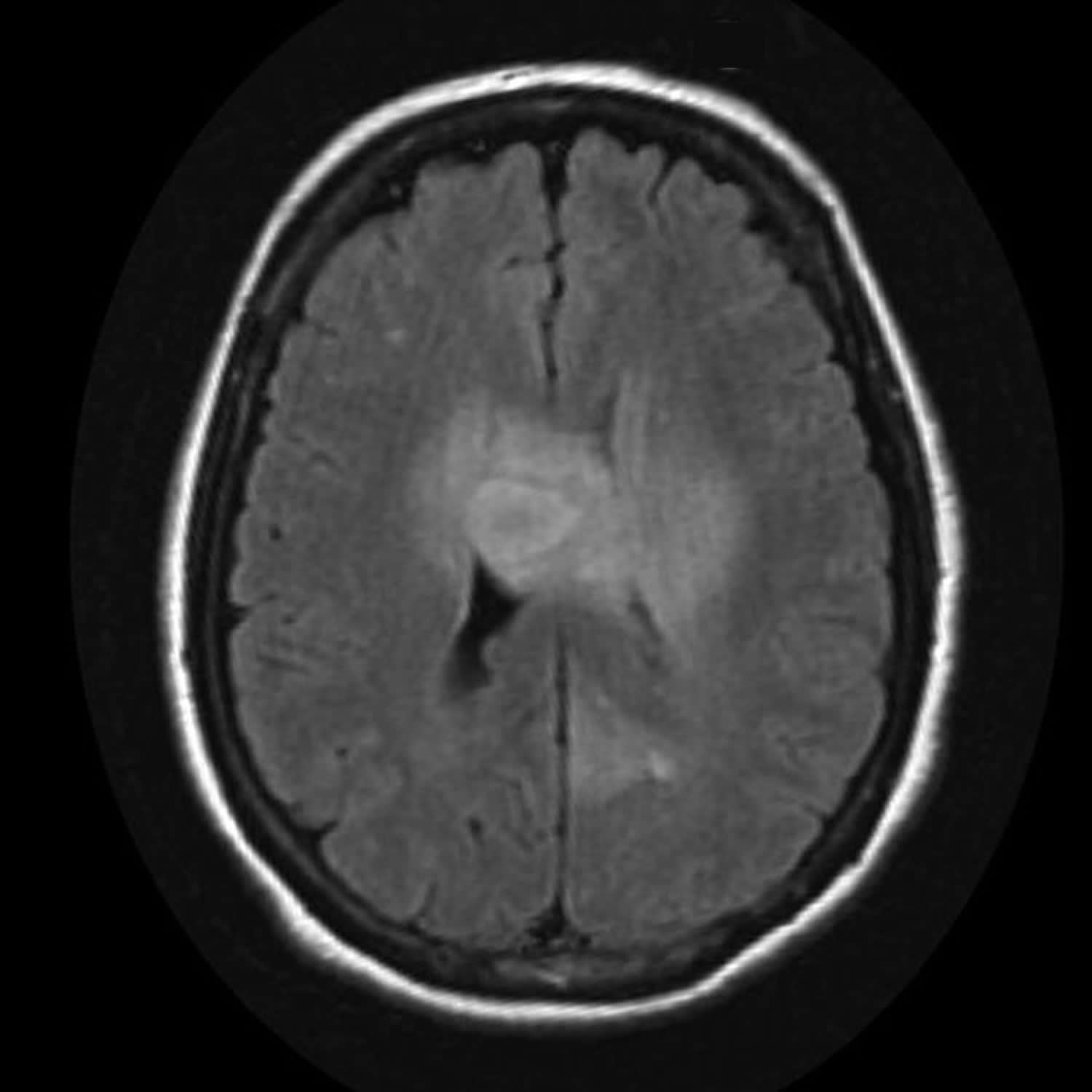
- Imaging tests. Imaging tests can help your doctor determine the location and size of your brain tumor. MRI is often used to diagnose brain tumors, and it may be used along with specialized MRI imaging, such as functional MRI, perfusion MRI and magnetic resonance spectroscopy. Other imaging tests may include CT and positron emission tomography (PET).
- Removing a sample of tissue for testing (biopsy). A biopsy can be done with a needle before surgery or during surgery to remove your astrocytoma, depending on your particular situation and the location of your tumor. The sample of suspicious tissue is analyzed in a laboratory to determine the types of cells and their level of aggressiveness. Specialized tests of the tumor cells can tell your doctor the types of mutations the cells have acquired. This gives your doctor clues about your prognosis and may guide your treatment options.
Astrocytoma treatment
Treatment options depend on the type, size, and location of the tumor, if and how far it has spread, previous treatment received, and the patient’s overall health. Treatment methods for the various types of astrocytomas are briefly explained below.
Astrocytoma treatments include:
- Surgery to remove the astrocytoma. Your brain surgeon (neursurgeon) will work to remove as much of the astrocytoma as possible. The goal is to remove all of the cancer, but sometimes the astrocytoma is located near sensitive brain tissue that makes that too risky. Even removing some of the cancer may reduce your signs and symptoms. For some people, surgery may be the only treatment needed. For others, additional treatments may be recommended to kill any cancer cells that might remain and reduce the risk that the cancer will return.
- Radiation therapy. Radiation therapy uses high-energy beams, such as X-rays or protons, to kill cancer cells. During radiation therapy, you lie on a table while a machine moves around you, directing beams to precise points in your brain. Radiation therapy might be recommended after surgery if your cancer wasn’t removed completely or if there’s an increased risk your cancer will return. Radiation is often combined with chemotherapy for aggressive cancers. For people who can’t undergo surgery, radiation therapy and chemotherapy may be used as a primary treatment.
- Chemotherapy. Chemotherapy uses drugs to kill cancer cells. Chemotherapy drugs can be taken in pill form or through a vein in your arm. In certain situations, a circular wafer of chemotherapy medicine can be placed in your brain after surgery where it slowly dissolves and releases the medication. Chemotherapy is often used after surgery to kill any cancer cells that might remain. It can be combined with radiation therapy for aggressive cancers.
- Clinical trials. Clinical trials are studies of new treatments. These studies give you a chance to try the latest treatment options, but the risk of side effects may not be known. Ask your doctor whether you might be eligible to participate in a clinical trial.
- Supportive (palliative) care. Palliative care is specialized medical care that focuses on providing relief from pain and other symptoms of a serious illness. Palliative care specialists work with you, your family and your other doctors to provide an extra layer of support that complements your ongoing care. Palliative care can be used while undergoing other aggressive treatments, such as surgery, chemotherapy or radiation therapy.
Pilocytic Astrocytoma
These tumors are often removed by surgery alone.
Surgery is the standard treatment. Total surgical removal of accessible astrocytomas is often possible and successful. Accessible tumors are those that can be operated on without causing unacceptably severe damage to other parts of the brain. If surgery is performed, the surgeon will attempt to remove all identifiable parts of the astrocytoma when possible. When the astrocytoma involves a crucial part of the brain, partial removal of the growth usually reduces pressure, relieves symptoms and helps control seizures.
Full or partial removal of the astrocytoma is sometimes followed by radiation therapy to destroy any remaining tumor cells. With the use of CT (computed tomography) and MRI (magnetic resonance imaging), radiation sometimes may be deferred for several months or years while the patient is scanned at regular intervals. Radiation as primary therapy is occasionally used on grade 1 astrocytomas.
Chemotherapy may be administered after radiation in an attempt to destroy any cells that remain or may also be given during the course of radiation treatment. Chemotherapy may be used instead of radiation in very young children to avoid damage to the developing brain. The type of chemotherapeutic drug therapy selected is determined by a neuro-oncologist who examines the grade of tumor, previous treatment and current health status of the affected individual.
Grade 1 astrocytoma can sometimes progress to a higher grade so follow-up scans at regular intervals are necessary to check for re-growth.
Diffuse Astrocytoma
Treatment depends on the size and location of the tumor. Surgery may be used to remove accessible tumors. As with all infiltrating astrocytomas (grades 2 to 4) it cannot be completely removed with surgery because the tentacle-like projections of the tumor grow into the surrounding tissue. Radiation may be used if the tumor is not accessible or in addition to surgery. Grade 2 astrocytoma can also progress to a higher grade so follow-up is necessary to check for re-growth. A recurrent tumor may be treated with surgery, radiation or chemotherapy. The role of chemotherapy in treating these tumors is being investigated.
Anaplastic Astrocytoma
Treatment depends on the size and location of the tumor, what it looks like under the microscope and how far it has spread. The standard first step in treatment of anaplastic astrocytoma is surgery. Radiation is then used to treat the remaining tumor. Chemotherapy may be recommended immediately after radiation or when and if the tumor recurs. If surgery is not possible, radiation and chemotherapy may be recommended. Several different types of radiation therapy are available including conventional external beam radiation, focused radiation, stereotactic radiosurgery implanted radiation or conformal radiation. A radiation oncologist determines the most appropriate form of radiation for a particular tumor. Chemotherapeutic agents that are commonly used to treat grade 3 astrocytoma include carmustine (BCNU), lomustine (CCNU), procarbazine, cisplatin and temozolomide. Biodegradable wafers (called Gliadel Wafers) containing BCNU is sometimes inserted in the cavity that remains after a tumor is removed. Grade 3 astrocytoma tend to recur and treatment depends on the grade of tumor that recurs.
The Food and Drug Administration (FDA) has approved temozolomide (Temodar) for the treatment of adults with anaplastic astrocytoma that has not responded to other forms of therapy (refractory anaplastic astrocytoma) 2.
Astrocytoma Grade 4 (Glioblastoma)
The first treatment step is surgery to remove as much tumor as possible. Surgery is almost always followed by radiation. Chemotherapy is often given at the same time as radiation and may be used to delay radiation in young children.
The initial treatment in most cases is surgical excision and removal of as much as the tumor as possible (resection). Often, only a portion of the tumor can be safely removed because malignant cells may have spread to surrounding brain tissue. Because surgery cannot completely remove a tumor, radiation therapy and chemotherapy are used following surgery to continue treatment.
The FDA has approved temozolomide (Temodar) for the treatment of adults with glioblastoma multiforme. Temozolomide is used concurrently with radiation therapy, and also for a period of time after completion of radiotherapy 2.
Gliadel Wafers have been approved by the FDA for the treatment of individuals with newly-diagnosed glioblastoma multiforme as an adjunct to surgery and radiation 3. It has also been approved for individuals with recurrent glioblastoma multiforme. Several of the wafers are placed in the cavity created by the surgical removal of a glioblastoma multiforme. The wafers release the drugs into the surrounding tissue over a period of two or three weeks.
On May 8th, 2009 the U.S. Food and Drug Administration recently approved Avastin (bevacizumab) to treat patients with glioblastoma multiforme (GBM) when this form of brain cancer continues to progress following standard therapy 4.
Avastin is a laboratory-produced molecule known as a monoclonal antibody that mimics the antibodies produced by the body’s immune system to defend against harmful substances. The medication inhibits the action of vascular endothelial growth factor that helps form new blood vessels. These vessels can feed a tumor, helping it to grow and can also provide a pathway for cancer cells to circulate in the body.
The drug was first approved in 2004 to treat metastatic cancer of the colon or rectum and has since been approved for treatment of non-squamous, non-small cell lung cancer and metastatic breast cancer.
- Survival Rates for Selected Childhood Brain and Spinal Cord Tumors. https://www.cancer.org/cancer/brain-spinal-cord-tumors-children/detection-diagnosis-staging/survival-rates.html[↩]
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/021029s031lbl.pdf[↩][↩]
- https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&applno=020637[↩]
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/125085s319lbl.pdf[↩]





{kind=link}