
What is atrial flutter
Atrial flutter is an abnormal heart rhythm (arrhythmia) that occurs in the atria of the heart, which can cause your heart to beat much faster than they should, around 300 beats per minute instead of the usual 60-90 beats per minute, but in a regular pattern. When atrial flutter first occurs, it is usually associated with a fast heart rate or tachycardia (beats over 100 per minute), and falls into the category of supra-ventricular tachycardias (SVTs). While this rhythm occurs most often in individuals with cardiovascular disease (e.g. hypertension, coronary artery disease, and cardiomyopathy) and diabetes mellitus, atrial flutter may occur spontaneously in people with otherwise normal hearts. Atrial flutter is typically not a stable rhythm, and frequently degenerates into atrial fibrillation (AF). Some people with atrial flutter also have atrial fibrillation and may experience periods of atrial flutter followed by periods of atrial fibrillation. However, atrial flutter does rarely persist for months to years.
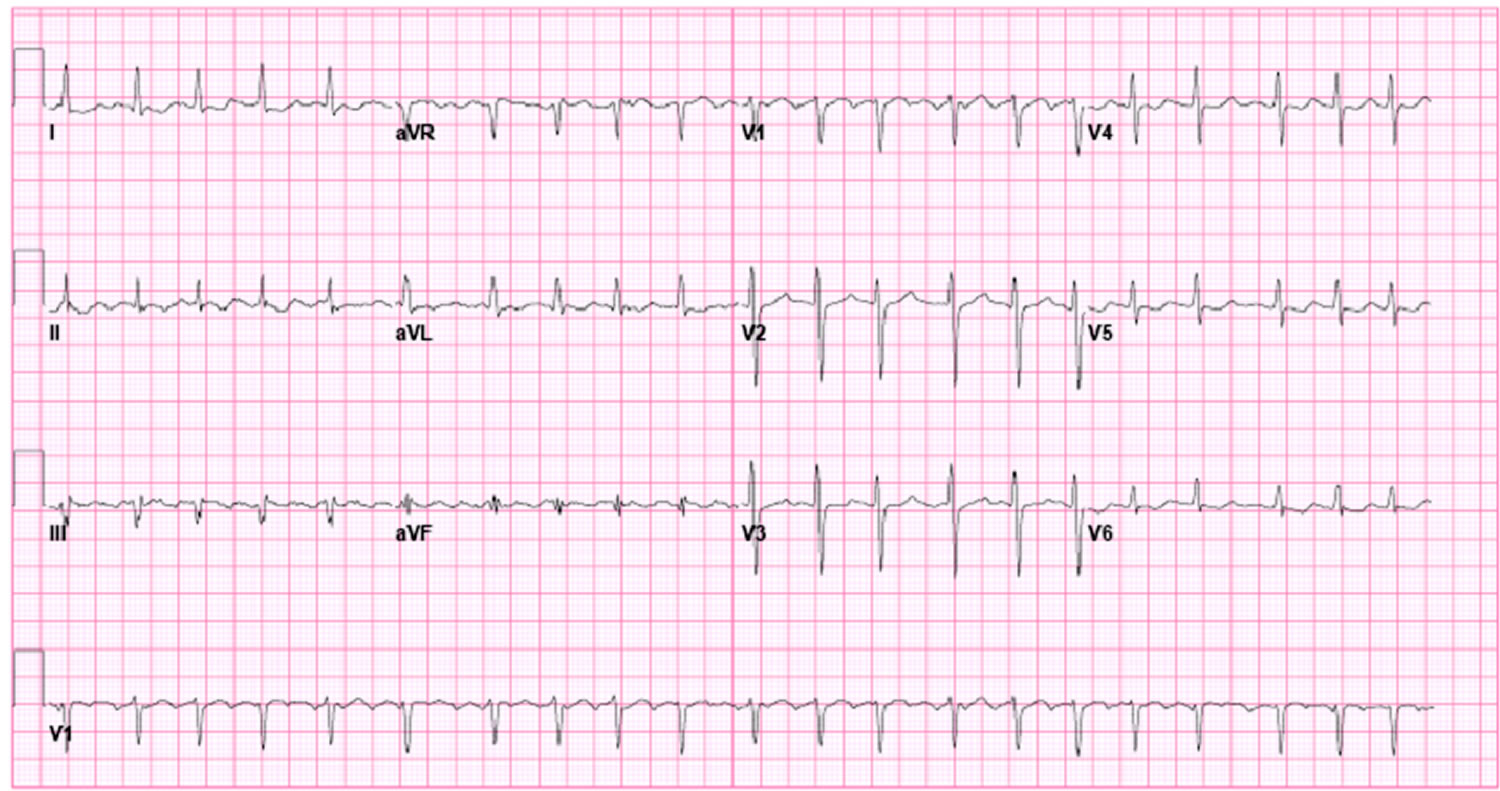
Atrial flutter is a heart rhythm disorder that is similar to the more common atrial fibrillation (AF). In atrial fibrillation (AF), the heart beats fast and in irregular pattern or rhythm. With atrial flutter, the heart beats abnormally fast, but in a regular pattern. The fast, but regular pattern of atrial flutter is what makes it special. Atrial flutter makes a very distinct “sawtooth” pattern on an electrocardiogram (ECG or EKG), a test used to diagnose abnormal heart rhythms (see Figure 4 below).
A normal heartbeat begins as a single electrical impulse that comes from the sinoatrial (SA) node, a small bundle of tissue located in the right atrium (see Figure 3). The impulse sends out an electrical pulse that causes the atria to contract (squeeze) and move blood into the lower ventricles. The electrical current passes through the atrioventricular (AV) node (the electrical bridge between the upper and lower chambers of the heart), causing the ventricles to squeeze and release in a steady, rhythmic sequence. As the chambers squeeze and release, they draw blood into the heart and push it back out to the rest of the body and lungs. This is what causes the pulse we feel on our wrist or neck.
If you have atrial flutter, the electrical impulses that tell your heart when to beat form a smaller circuit (it moves in an organized abnormal circular motion) in the top chambers of your heart (your atria), instead of traveling from your heart’s sinoatrial (SA) node to the AV (atrioventricular) node as they should. These impulses circulate very fast around your atria, causing your atria to beat much faster than they should, around 300 beats per minute instead of the usual 60-90 beats per minute. The bottom chambers of your heart (your ventricles) can’t pump this fast, so they will usually beat between 75 and 150 beats per minute. Your atria and ventricles will be beating at different speeds, putting your heart under strain. Atrial flutter can also cause blood to pool in your ventricles which can lead to a blood clot forming in your heart. If the clot breaks off, it could cause a stroke, so it’s important that you receive the right treatment for your atrial flutter.
Atrial flutter is much less common than atrial fibrillation. Of the patients admitted to US hospitals with a diagnosis of supraventricular tachycardia (SVT) between 1985 and 1990, 77% had atrial fibrillation and 10% had atrial flutter. On the basis of a study of patients referred to tertiary care centers, the incidence of atrial flutter in the United States is estimated to be approximately 200,000 new cases per year 1.
In a study of 100 patients with atrial flutter, 75% were men. In another study performed at a tertiary care study, atrial flutter was 2.5 times more common in men.
Patients with atrial flutter, as with atrial fibrillation, tend to be older adults. In one study, the average age was 64 years. The prevalence of atrial fibrillation increases with age, as follows:
- 25-35 years: 2-3 cases per 1000 population
- 55-64 years: 30-90 cases per 1000 population
- 65-90 years: 50-90 cases per 1000 population
Types of atrial flutter
There are two types of atrial flutter, the common type I and rarer type II. Most individuals with atrial flutter will manifest only one of these. Rarely someone may manifest both types; however, they can only manifest one type at a time.
Type I – Typical atrial flutter
Type I atrial flutter, also known as common atrial flutter or typical atrial flutter, has an atrial rate of 240 to 340 beats/minute. However, this rate may be slowed by antiarrhythmic agents.
- Counterclockwise atrial flutter (known as cephalad-directed atrial flutter) is more commonly seen. The flutter waves in this rhythm are inverted in ECG leads II, III, and aVF.
- The re-entry loop cycles in the opposite direction in clockwise atrial flutter, thus the flutter waves are upright in II, III, and aVF.
Type II – Paroxysmal atrial flutter
Type II flutter follows a significantly different re-entry pathway to type I flutter, and is typically faster, usually 340-440 beats/minute. Left atrial flutter is common after incomplete left atrial ablation procedures.
The heart’s electrical system
To understand the causes of heart rate or rhythm problems such as tachycardia, it helps to understand how the heart’s internal electrical system works.
Your heart is made up of four chambers — two upper chambers (atria) and two lower chambers (ventricles). The rhythm of your heart is normally controlled by a natural pacemaker called the sinus node, which is located in the right atrium. The sinus node produces electrical impulses that normally start each heartbeat.
From the sinus node, electrical impulses travel across the atria, causing the atrial muscles to contract and pump blood into the ventricles.
The electrical impulses then arrive at a cluster of cells called the atrioventricular (AV) node — usually the only pathway for signals to travel from the atria to the ventricles.
The AV node slows down the electrical signal before sending it to the ventricles. This slight delay allows the ventricles to fill with blood. When electrical impulses reach the muscles of the ventricles, they contract, causing them to pump blood either to the lungs or to the rest of the body.
When anything disrupts this complex system, it can cause the heart to beat too fast (tachycardia), too slow (bradycardia) or with an irregular rhythm.
Figure 1. The anatomy of the heart
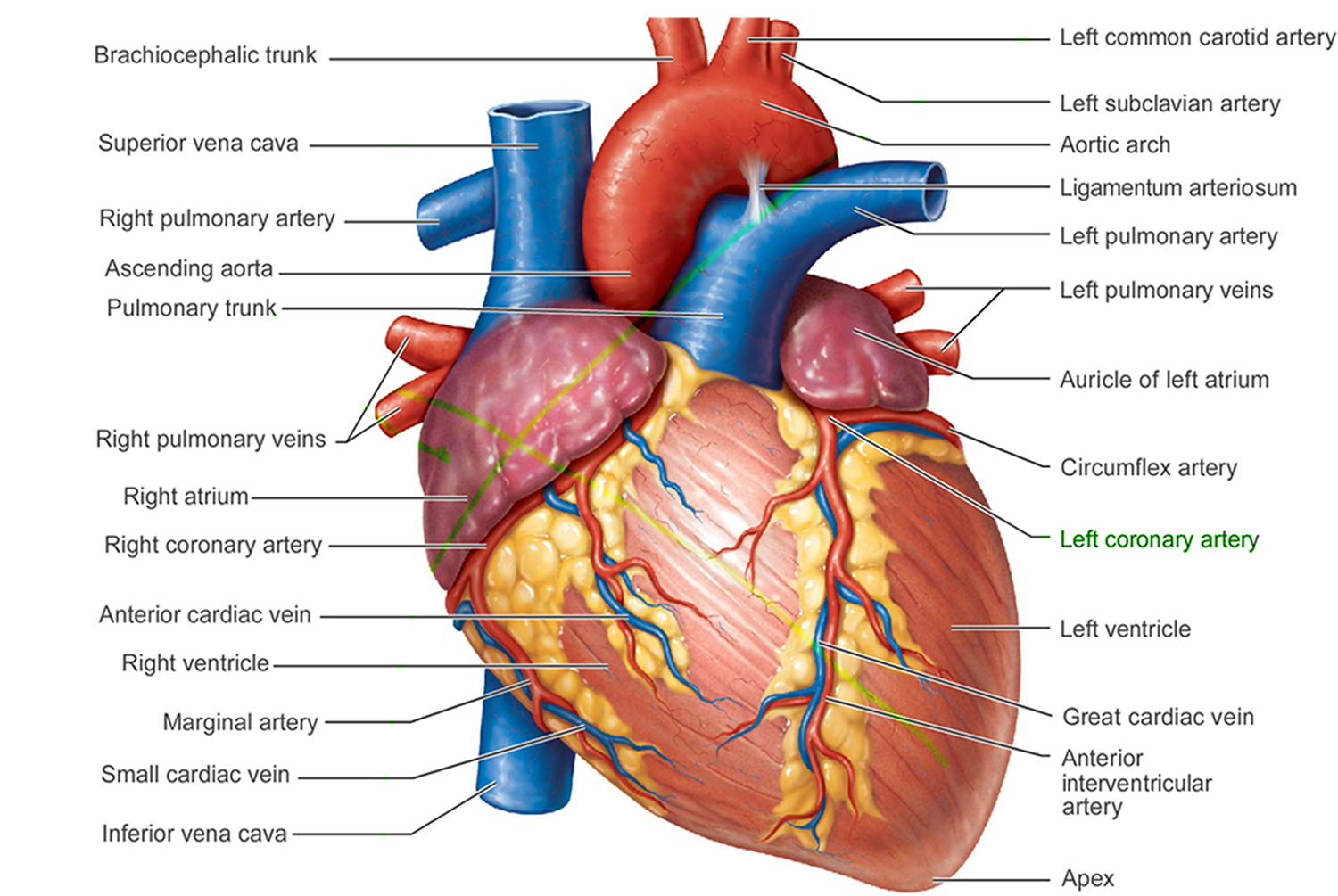
 Figure 3. The heart’s electrical system
Figure 3. The heart’s electrical system
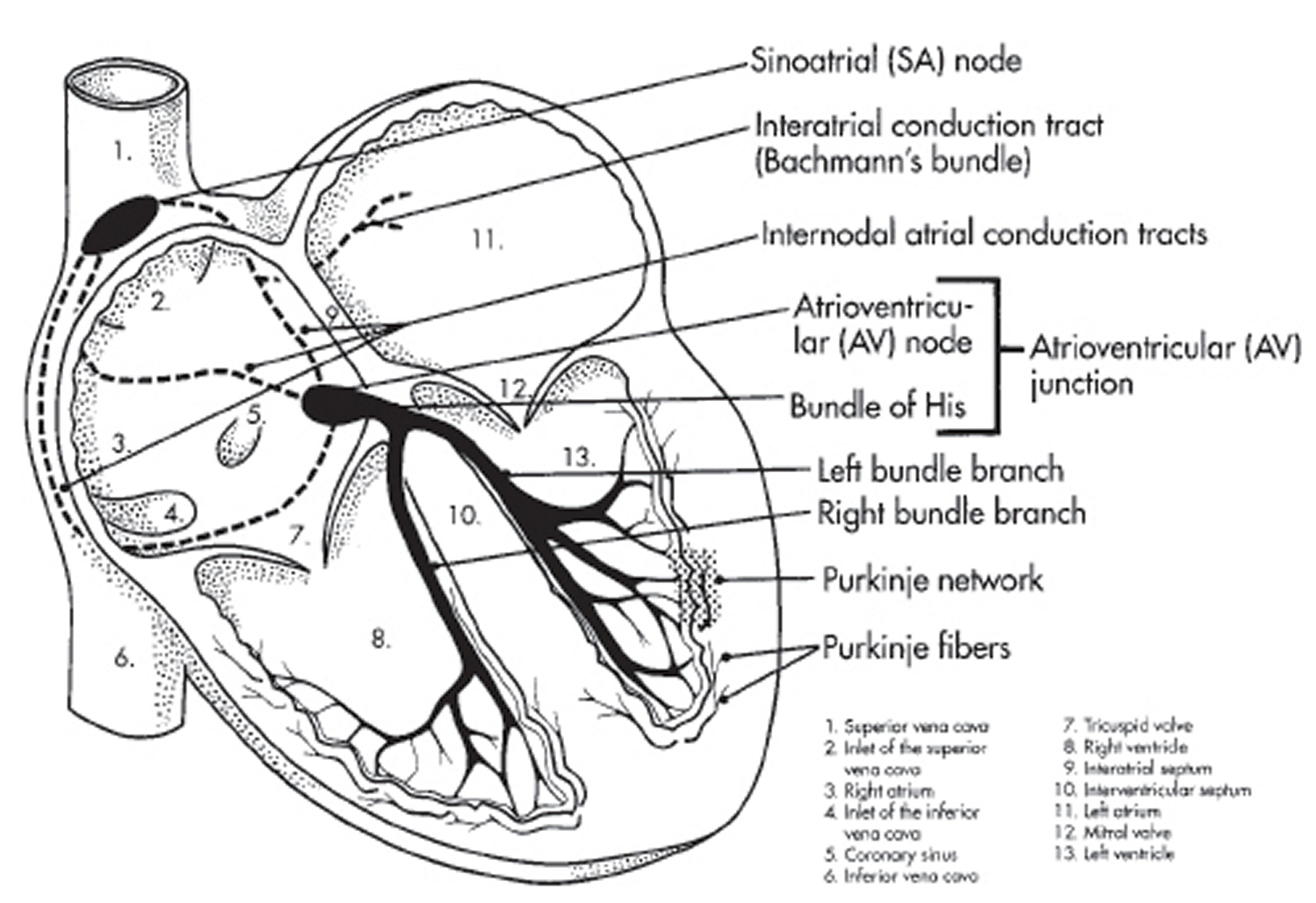
Figure 4. Atrial flutter ECG (atrial flutter EKG) – note the “sawtooth pattern”

Atrial flutter vs atrial fibrillation
Atrial flutter and atrial fibrillation are both abnormal heart rhythms (often called arrhythmias). They occur when there is an issue with the electrical signals and pathways in your heart, which usually help it beat in an organized, effective way.
Normally, the top chambers (atria) contract and push blood into the bottom chambers (ventricles). In atrial fibrillation (AF), impulses fire off from different places in the atria (the top heart chambers), causing chaotic electrical activity, the atria beat irregularly, but faster than usual and more often than the ventricles, so you may have four atrial beats to every one ventricular beat and you sometimes has fast, irregular pulse. The word fibrillation means an uncontrolled, uncoordinated twitching of individual muscle fibers.
In atrial flutter, the atria beat regularly.
Atrial flutter is less common, but has similar symptoms (feeling faint, tiredness, palpitations, shortness of breath or dizziness). Some people have mild symptoms, others have none at all. About a third of people with atrial flutter also have atrial fibrillation.
Both conditions carry increased risk of stroke, usually managed by drugs (such as warfarin or a newer anticoagulant). This is why, whether you have atrial fibrillation or atrial flutter, it is vital to be diagnosed early so you can get the right treatment and reduce your stroke risk. Either condition may require medications to prevent your heart rate becoming too rapid.
Catheter ablation is usually considered the best treatment for atrial flutter, whereas medication is often the first treatment for atrial fibrillation. Catheter ablation is a procedure that is done under local anesthetic, where radiofrequency energy is used to destroy the area inside your heart that’s causing the abnormal heart rhythm.
Atrial fibrillation (AF) is the most common type of irregular heart rhythm and is a major cause of stroke. The chances of having atrial fibrillation increase substantially as you get older, and about seven in every 100 people over the age of 65 have it. An ageing population means that atrial fibrillation is becoming more common. High blood pressure and obesity also make it more likely, as they put extra strain on the heart, which can trigger impulses to fire off erratically. Coronary heart disease, heart valve disease or an overactive thyroid can also cause atrial fibrillation.
Atrial fibrillation increases the risk of a blood clot developing, which can lead to a stroke. Even if you don’t have symptoms, atrial fibrillation can increase the risk of stroke by five times. The disorganized electrical activity also means that the heart doesn’t pump as efficiently as it should. This can increase the risk of heart failure further down the line. The good news for people with atrial fibrillation is that with the right treatment these risks can be dramatically reduced.
Atrial fibrillation signs and symptoms
Palpitation (being aware of your heart beat) is a common symptom. People describe it as if their heart is jumping all over the place. It’s also common to feel breathless and tired, although some people don’t have any symptoms at all. An irregular pulse is a sign that you might have atrial fibrillation, so it’s important to know how to check yours. If your pulse doesn’t follow a steady pattern, tell your doctor.
What can people with atrial fibrillation do to prevent an episode?
Alcohol can irritate the cells in the heart that can trigger an attack. So if you drink any kind of alcohol, it’s important to do so in moderation. Contrary to popular belief, cutting back on caffeine doesn’t usually make much of a difference for most people with atrial fibrillation, and there is little evidence that suggests avoiding stressful situations can help prevent it. However, preventing atrial fibrillation from developing in the first place is key. Although doctors can’t stop your bodies from ageing (yet), you can try to keep your weight and blood pressure under control by making sure that you have a healthy lifestyle.
Atrial fibrillation treatment
Controlling your heart rate and rhythm helps to improve symptoms and reduce the risk of heart failure. Amiodarone, sotalol and flecainide are some of the medicines that are used to try to get people’s hearts back to their normal rhythm. The earlier someone is diagnosed and treated, the higher the chances of success. If someone has had continuous atrial fibrillation for a long time, it can be hard to control their rhythm, so it may be that they are given medicines such as digoxin or beta blockers to slow down their heart rate.
Taking warfarin, a medicine that makes blood clots less likely to form, substantially reduces the risk of stroke. Levels of warfarin in the bloodstream can vary, so people need to go for regular blood tests to make sure they are on the right dose. However, medicines that don’t require frequent monitoring are becoming available for people with atrial fibrillation. These are alternative options for people who struggle with their warfarin control or for those who find it difficult to get to a clinic.
A treatment called ablation is used to try to get people’s heart rhythms back to normal. It involves using radio frequency energy to heat up and destroy an area of tissue. The most common form of ablation is pulmonary vein isolation. Pulmonary veins are the tubes that drain blood from the lungs into the heart. atrial fibrillation is usually triggered by rapid impulses within the pulmonary veins, so isolation electrically disconnects the veins to stop these impulses entering the heart. This treatment has a success rate of about 80 to 90 per cent for people with paroxysmal atrial fibrillation.
If you’ve had continuous atrial fibrillation for a long time, you might need more than one ablation or a treatment called a catheter maze. This involves having more widespread ablation to stop the atrial fibrillation from spreading further. Another procedure called cardioversion involves using a machine called a defibrillator to give a controlled electrical shock in order to make the heartbeat return to a normal rhythm. It can restore a normal rhythm for a short while, but because it doesn’t sort the underlying problem out, the atrial fibrillation often returns.
Living with atrial fibrillation
Because atrial fibrillation can be unpredictable, and therefore you don’t know when an attack might happen, some people worry about going out or being active, but most find that they are able to carry on as normal with the help of medicines. Getting your warfarin levels checked can be inconvenient, but most people realize how important it is in helping to protect them from a stroke.
Atrial flutter complications
Atrial flutter itself is not life threatening. If left untreated, the side effects of atrial flutter can be potentially life threatening. atrial flutter makes it harder for the heart to pump blood effectively. With the blood moving more slowly, it is more likely to form clots. If the clot is pumped out of the heart, it could travel to the brain and lead to a stroke or heart attack.
Without treatment, atrial flutter can also cause a fast pulse rate for long periods of time. This means that the ventricles are beating too fast. When the ventricles beat too fast for long periods of time, the heart muscle can become weak and tired. This condition is called cardiomyopathy. This can lead to heart failure and long-term disability.
Without treatment, atrial flutter can also cause another type of arrhythmia called atrial fibrillation. Atrial fibrillation (AF) is the most common type of abnormal heart rhythm.
Atrial flutter prognosis
The prognosis for atrial flutter depends on the patient’s underlying medical condition. Any prolonged atrial arrhythmia can cause a tachycardia-induced cardiomyopathy. Intervening to control the ventricular response rate or to return the patient to sinus rhythm is important. Thrombus formation in the left atrium has been described in patients with atrial flutter (0-21%). Thromboembolic complications have also been described 2.
Because of the conduction properties of the atrioventricular (AV) node, many people with atrial flutter will have a faster ventricular response than those with atrial fibrillation. The heart rate is often more difficult to control with atrial flutter than with atrial fibrillation, because of increased concealed conduction in those with atrial fibrillation.
For the most part, morbidity and mortality result from complications of rate (e.g, syncope and congestive heart failure). In patients with atrial flutter, the risk of embolic occurrences approaches that seen in atrial fibrillation. Patients with Wolff-Parkinson-White syndrome who develop atrial flutter can develop life-threatening ventricular responses and therefore should be considered for catheter ablation of their accessory bypass tract.
Data from the Framingham study suggest that patients with atrial fibrillation do not live as long as patients without atrial fibrillation (i.e, control subjects). No data are available on atrial flutter.
The prognosis for patients with typical atrial flutter who undergo catheter ablation is excellent, with a very low recurrence rate. The picture is not as clear for patients with both atrial flutter and atrial fibrillation. Some reports have documented fewer episodes of atrial fibrillation after successful flutter ablation; others have not. It is possible that atrial fibrillation may be more responsive to antiarrhythmic agents after atrial flutter has been eliminated.
Bohnen et al performed a prospective study to assess the incidence and predictors of major complications from contemporary catheter ablation procedures 3. Major complication rates ranged from 0.8% (supraventricular tachycardia) to 6% (ventricular tachycardia associated with structural heart disease), depending on the ablation procedure performed. Renal insufficiency was the only independent predictor of a major complication.
Numerous reports indicate that patients with atrial fibrillation who are given class IC antiarrhythmic agents may convert to atrial flutter with faster ventricular rates. Thus, patients receiving type IC agents (e.g, flecainide) should also receive an AV node−blocking drug such as a beta blocker or calcium channel blocker. In patients with atrial flutter in one study, the relative risk for development of stroke was 1.4 in comparison to control subjects 4.
A multicenter report by Stiell et al 5 that prospectively evaluated management and 30-day outcomes in 1091 emergency department patients with recent-onset atrial fibrillation (84.7%) or atrial flutter (15.3%) found that oral anticoagulants were underprescribed and that patients discharged from the emergency department in sinus rhythm had a smaller likelihood of experiencing an adverse event. More than 10% of all patients had adverse events within 30 days, including one case of stroke, but no deaths were reported. Potential risk factors for adverse events included longer duration from arrhythmia onset, radiographic evidence of pulmonary congestion, previous history of stroke/transient ischemic attack, and emergency department discharge without being in sinus rhythm 5.
Atrial flutter causes
What causes atrial flutter
Atrial flutter is associated with a variety of heart disorders. People who have atrial flutter usually have an underlying heart problem such as coronary heart disease (coronary artery disease), cardiomyopathy, heart valve disease, congenital heart disease, inflammation of the heart (such as myocarditis), high blood pressure, or another condition such as lung disease or thyroid problems. In most studies, approximately 30% of patients with atrial flutter have coronary artery disease, 30% have hypertensive heart disease, and 30% have no underlying cardiac disease. Rheumatic heart disease, congenital heart disease, pericarditis, and cardiomyopathy may also lead to atrial flutter. Rarely, mitral valve prolapse or acute myocardial infarction has been associated with atrial flutter.
In addition, the following conditions are also associated with atrial flutter:
- Hypoxia
- Chronic obstructive pulmonary disease
- Pulmonary embolism
- Hyperthyroidism
- Pheochromocytoma
- Diabetes
- Electrolyte imbalance
- Alcohol consumption
- Obesity
- Digitalis toxicity
- Myotonic dystrophy in childhood (rare) 6
Atrial Flutter is usually found in patients with:
- Heart failure
- Previous heart attack
- Valve abnormalities or congenital defects
- High blood pressure
- Recent surgery
- Thyroid dysfunction
- Alcoholism (especially binge drinking)
- Chronic lung disease
- Acute (serious) illness
- Diabetes
- After open-heart surgery (bypass surgery)
- Atrial flutter can be found concurrently in people with atrial fibrillation
Atrial flutter may be a sequela of open heart surgery. After cardiac surgery, atrial flutter may be reentrant as a result of natural barriers, atrial incisions, and scar. Some patients develop atypical left atrial flutter after pulmonary vein isolation for atrial fibrillation.
Although there are no clearly defined genetic conditions that cause atrial flutter, in many cases there is likely an underlying genetic susceptibility to acquiring it. Genome-wide association studies have identified genes associated with atrial flutter 7.
The PITX2 (paired-like homeodomain 2) gene on chromosome locus 4q25 is known to play a major role in left-right asymmetry of the heart and has been found to have a strong association with atrial fibrillation 8 and an even stronger association with typical atrial flutter 9. There are not yet any clinically available genetic tests that can identify persons at increased risk for atrial flutter.
Risk Factors for atrial flutter
Some medical conditions increase the risk for developing atrial flutter. These medical conditions include:
- Heart failure
- Previous heart attack
- Acquired or congenital valve abnormalities
- High Blood Pressure
- Recent upper chamber surgery
- Thyroid dysfunction
- Alcoholism (especially binge drinking)
- Chronic lung disease
- Acute (serious) illness
- Diabetes.
Atrial flutter symptoms
The electrical signal that causes atrial flutter circulates in an organized, predictable pattern. This means that people with atrial flutter usually continue to have a steady heartbeat, even though it is faster than normal. It is possible that people with atrial flutter may feel no symptoms at all. Signs and symptoms in patients with atrial flutter typically reflect decreased cardiac output as a result of the rapid ventricular rate. Others do experience symptoms, which may include:
- Heart palpitations (feeling like your heart is racing, pounding, or fluttering)
- Fatigue or poor exercise tolerance
- Fast, steady pulse
- Shortness of breath (dyspnea)
- Trouble with everyday exercises or activities
- Pain, pressure, tightness, or discomfort in your chest
- Dizziness, lightheadedness, or fainting
Less common symptoms include angina, profound dyspnea, or syncope. Tachycardia may or may not be present, depending on the degree of AV block associated with the atrial flutter activity.
How to check your pulse
You can check to see if you might have atrial flutter or atrial fibrillation by feeling your pulse at your wrist. A normal pulse should follow a steady beat. If you have atrial fibrillation (AF), your pulse will feel irregular, erratic and possibly fast, and the strength will vary. If your pulse feels like this, or if you’re concerned, see your doctor.
Finding your pulse
The easiest places to find your pulse are:
Your wrist
- Put one of your hands out so you’re looking at your palm.
- Use the first finger (your index finger) and middle finger of your other hand and place the pads of these fingers on the inside of your wrist, at the base of your thumb.
- Press lightly and feel the pulse. If you can’t feel anything press slightly harder or move your fingers around until you feel your pulse.
How to check your pulse
Once you’ve found your pulse, continue to feel it for about 20-30 seconds. Feel your pulse and check if it’s regular or irregular. You can work out your heart rate in beats per minute (bpm) by:
- counting the number of beats in your pulse after 60 seconds, or
- counting the beats for 30 seconds and multiplying by two.
If your pulse feels irregular, you should check for a full 60 seconds.
What should you check?
Your heart rate:
- Most adults have a resting heart rate between 60 and 100 bpm
- Your heart rate may be lower if you do lots of exercise and are very fit. Some athletes have heart rates ranging from 40 to 60 bpm.
Your heart rhythm:
- Occasional irregularities such as missed beats are very common and usually nothing to worry about, but it is still best to check this with your doctor.
- An irregular pulse could also be a sign of an arrhythmia (an abnormal heart rhythm), such as Atrial Fibrillation (AF). This is more likely if you are 65 or older.
Listen to the example heart rhythms below to help you spot an irregular heart beat:
Regular pulse
Irregular pulse
Atrial flutter diagnosis
Your doctor might recommend that you have an electrocardiography (ECG) or echocardiogram test or an electrophysiological (EP) study to help diagnose atrial flutter. Electrocardiography (ECG) is essential in making the diagnosis.
The history and physical examination findings guide laboratory studies. Although hyperthyroidism is a rare cause of atrial flutter, asymptomatic hyperthyroidism, especially in elderly patients, can manifest as atrial fibrillation or flutter and should be excluded with thyroid function studies.
- Electrocardiography (ECG): This is an essential diagnostic modality for atrial flutter
- Vagal maneuvers: These can be helpful in determining the underlying atrial rhythm if flutter waves are not seen well
- Adenosine: This drug can be helpful in making the diagnosis of atrial flutter by transiently blocking the AV node
- Exercise testing: This can be utilized to identify exercise-induced atrial fibrillation and to evaluate the response of the ventricular rate to activity, as well as its interaction with symptoms including those of ischemic heart disease
- Holter monitor: This can be used to help identify arrhythmias in patients with nonspecific symptoms, to identify triggers, and to detect associated atrial arrhythmias
Transthoracic echocardiography (TTE) is the preferred initial imaging modality for evaluating atrial flutter. It can evaluate right and left atrial size, as well as the size and function of the right and left ventricles, and this information facilitates diagnosis of valvular heart disease, left ventricular hypertrophy (LVH), and pericardial disease.
Atrial flutter treatment
General treatment goals for symptomatic atrial flutter are similar to those for atrial fibrillation. They include the following:
- Control of ventricular rate: This can be achieved with drugs that block the AV node; intravenous (IV) calcium channel blockers (eg, verapamil and diltiazem) or beta blockers can be used, followed by initiation of oral agents
- Restoration of sinus rhythm: This can be achieved by means of electrical or pharmacologic cardioversion or radiofrequency ablation (RFA); successful ablation reduces or eliminates the need for long-term anticoagulation and antiarrhythmic medications
- Prevention of recurrent episodes or reduction in their frequency or duration: In general, the use of antiarrhythmic drugs in atrial flutter is similar to that in atrial fibrillation
- Prevention of thromboembolic complications: Adequate anticoagulation, as recommended by the American College of Chest Physicians, has been shown to decrease thromboembolic complications in patients with chronic atrial flutter and in patients undergoing cardioversion
- Minimization of adverse effects from therapy: Because atrial flutter is a nonfatal arrhythmia, carefully assess the risks and benefits of drug therapy, especially with antiarrhythmic agents
Once your atrial flutter has been confirmed, your doctor might recommend a cardioversion or ablation treatment, and /or medicines such as beta-blockers, calcium channel blockers and other anti-arrhythmic medicines. To reduce this risk of having a stroke, you may also need to take an anticoagulant medicine such as warfarin.
Atrial flutter ablation
Atrial flutter ablation is a procedure to create scar tissue within the right upper chamber of the heart in order to block the electrical signals that cause a fluttering heartbeat.
Atrial flutter occurs when your heart’s electrical signals tell the upper chambers of your heart (atria) to beat too quickly. The goal of atrial flutter ablation is to stop the incorrect electrical signals and restore a normal heart rhythm.
Doctors use atrial flutter ablation to control the signs and symptoms associated with atrial flutter. Atrial flutter ablation may restore a normal heart rhythm, which may improve your quality of life.
What you can expect
Atrial flutter ablation is performed in the hospital. You’ll receive a medication called a sedative that helps you relax.
Once the sedative takes effect, a small area near a vein in your groin or neck is numbed and catheters are inserted into the vein. Your doctor carefully guides the catheters through the vein and into your heart.
The catheters are equipped with electrodes that are used to record your heart’s electrical activity and to send electrical impulses. Your doctor uses this information to determine the best place to apply the treatment. For atrial flutter ablation, the treatment is applied to the right upper chamber of the heart.
Special catheters are used to transmit electrical energy (radiofrequency ablation) to the target area, damaging the tissue and causing scarring. In some cases, this will block the electrical signals that are contributing to your atrial flutter.
Atrial flutter ablation typically takes two to three hours. Afterward, you’ll be taken to a recovery area where your condition will be closely monitored. Depending on your condition, you may be allowed to go home the same day or you may spend a night in the hospital.
Your doctor will schedule follow-up examinations to monitor your heart. Most people experience an improvement in quality of life after atrial flutter ablation. But there’s a chance that atrial flutter may return. In these cases, the procedure may be repeated or you and your doctor might consider other treatments.
- Granada J, Uribe W, Chyou PH, et al. Incidence and predictors of atrial flutter in the general population. J Am Coll Cardiol. 2000 Dec. 36 (7):2242-6.[↩]
- Ghali WA, Wasil BI, Brant R, Exner DV, Cornuz J. Atrial flutter and the risk of thromboembolism: a systematic review and meta-analysis. Am J Med. 2005 Feb. 118 (2):101-7.[↩]
- Bohnen M, Stevenson WG, Tedrow UB, et al. Incidence and predictors of major complications from contemporary catheter ablation to treat cardiac arrhythmias. Heart Rhythm. 2011 Nov. 8 (11):1661-6.[↩]
- Biblo LA, Yuan Z, Quan KJ, Mackall JA, Rimm AA. Risk of stroke in patients with atrial flutter. Am J Cardiol. 2001 Feb 1. 87 (3):346-9, A9.[↩]
- Stiell IG, Clement CM, Rowe BH, et al. Outcomes for emergency department patients with recent-onset atrial fibrillation and flutter treated in Canadian hospitals. Ann Emerg Med. 2017 May. 69 (5):562-71.e2.[↩][↩]
- Suda K, Matsumura M, Hayashi Y. Myotonic dystrophy presenting as atrial flutter in childhood. Cardiol Young. 2004 Feb. 14 (1):89-92.[↩]
- Ioannidis JP. Prediction of cardiovascular disease outcomes and established cardiovascular risk factors by genome-wide association markers. Circ Cardiovasc Genet. 2009 Feb. 2 (1):7-15.[↩]
- Olesen MS, Holst AG, Jabbari J, et al. Genetic loci on chromosomes 4q25, 7p31, and 12p12 are associated with onset of lone atrial fibrillation before the age of 40 years. Can J Cardiol. 2012 Mar-Apr. 28 (2):191-5.[↩]
- Gudbjartsson DF, Arnar DO, Helgadottir A, et al. Variants conferring risk of atrial fibrillation on chromosome 4q25. Nature. 2007 Jul 19. 448 (7151):353-7.[↩]





{kind=link}