
Contents
- What is acne
- What causes back acne
- Acne friendly skin care essential
- How to get rid of back acne
- Treatment of Acne Scars
What is acne
Acne, also known as pimples, zits, acne vulgaris (“common acne”) and blemishes, is the term used for plugged pores (blackheads and whiteheads) and even deeper lumps (cysts, known as cystic acne) that occur on the face, neck, chest, back, shoulders, and even the upper arms. Acne is a common chronic skin disorder affecting the hair follicle and sebaceous gland, in which there is expansion and blockage of the hair follicle and inflammation (see Figures 1 and 2). Acne is thought to be caused by multiple factors. Overproduction of a normal oil on the skin, called sebum, increases under the influence of hormones. This, coupled with insufficient shedding of exfoliating dead skin cells, plugs hair follicles. The plugged follicle can become inflamed and have increased growth of normal skin bacteria, Cutibacterium acnes (C. acnes, formally known as Propionibacterium acnes). Medications such as lithium, cortisone, hormones, iodides, some seizure medications, or isoniazid can also cause acne lesions. There is no cure for acne, but certain measures can help prevent more breakouts. Acne can result in scarring, so minimizing breakouts is important.
Acne is often confined to the face but it may involve neck, chest and back. Acne affects males and females of all races and ethnicities. Acne affects most teens to some extent. Close to 100% of people between the ages 12–17 have at least an occasional whitehead or blackhead. Acne tends to improve after the age of 25 years but may persist, especially in females. However, acne is not restricted to any age group; adults can also get acne too. In fact, one fifth of women between the ages 25–40 suffer from adult acne. Furthermore, some women who had very little to no acne before age 20 may develop acne in adulthood. The peak for women taking isotretinoin in one study was 24 years of age. While acne is not a life-threatening condition, it can be upsetting and disfiguring.
There are many variations of acne, one of which is a condition known as acne mechanica. This form of acne results from chronic physical pressure on the skin, such as from the straps of a backpack or sports equipment. Acne excoriée is a form of acne resulting from the picking, squeezing, and rubbing of lesions, which result in scratches (excoriations). This type of acne is seen more commonly in women and usually starts during the teen years. There is commonly a history of acne, and the scratches may involve the face, neck, chest, breasts, back, and upper arms. Unfortunately, this picking can lead to acne scars and discoloration. Additionally, acne excoriée can result from the presence of anxiety, depression, or emotional distress. Acne keloidalis, which affects the hair follicles of black individuals, is usually located on the nape of the neck and associated with acne that heal with hard, raised scars (keloids). Sometimes similar scars can also be left from acne lesions on the chest, back, or face.
Some lesions that appear to be acne are not acne at all. One skin condition that resembles acne is folliculitis (e.g., pityrosporum folliculitis), which is inflammation caused by infection of the hair follicles (see Figure 4).
Acne rosacea is a disorder affecting the middle portion of the face (mainly the forehead, chin, and lower half of the nose), which causes persistent redness. The tiny blood vessels in these areas enlarge and become more visible, appearing like tiny red lines (telangiectasias). The bumps of rosacea can resemble acne but, in fact, rosacea is different than acne. Unlike common acne, rosacea is not primarily a plague of teens but occurs most often in adults (ages 30–50), especially in those with fair skin. Additionally, unlike acne, there are no blackheads or whiteheads in rosacea.
Acne is characterized by:
- Open and closed uninflamed comedones (blackheads and whiteheads)
- Inflamed papules and pustules
- In severe acne, nodules and pseudocysts
- Post-inflammatory erythematous or pigmented macules and scars
- Adverse social and psychological effects
Severity is classified as mild, moderate or severe.
- Mild acne: total lesion count <30
- Moderate acne: total lesion count 30–125
- Severe acne: total lesion count >125
Figure 1. Skin structure

What is nodulocystic acne?
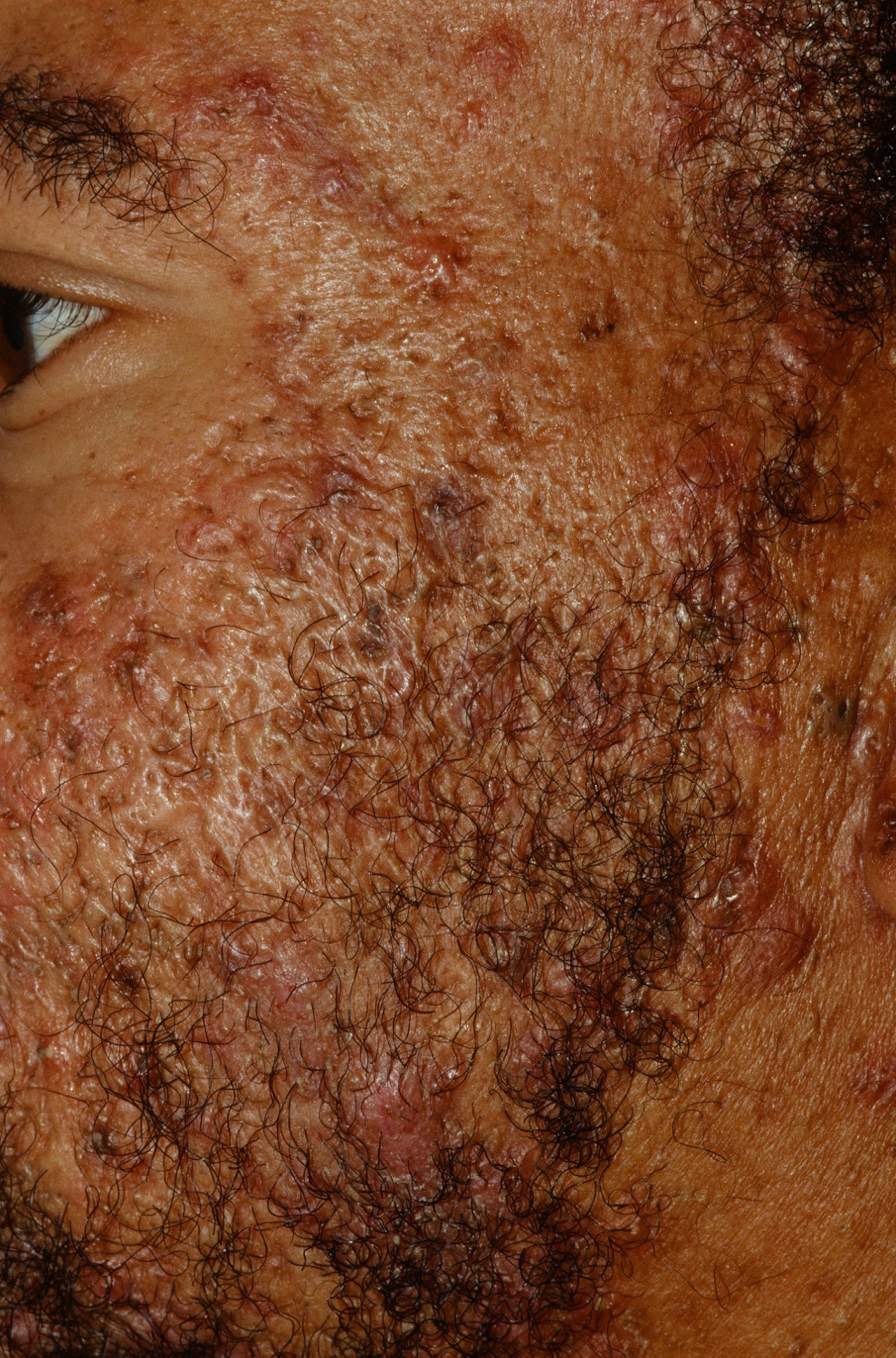
Nodulocystic acne is a severe form of acne affecting the face, chest and back. Nodulocystic acne is characterized by multiple inflamed and uninflamed nodules and frequently, scars. It is more common in males.
The name nodulocystic acne implies there are nodules (firm lumps) and cysts (fluid-filled cavities lined by epithelium). However, the fluctuant lesions are not true cysts as there is no lining. They are sometimes called pseudocysts.
Nodulocystic acne treatment
Treatment of nodulocystic acne can be challenging and may require a combination of medicines. Topical treatment is usually ineffective.
The recommended treatment for nodulocystic acne is isotretinoin, which should be commenced early to prevent scarring. The treatment is required for at least five months, and further courses are sometimes necessary.
Patients with acne conglobata often need additional treatments, such as:
- Oral antibiotics
- Intralesional steroids
- Systemic steroids
- Hormonal therapy in women
Figure 2. Back acne (Nodulocystic acne vulagris)

What is acne fulminans?
Acne fulminans is the explosive flare of crusted, inflammatory acne lesions in a patient with acne.
- Acne fulminans usually affects the young, tall male on the chest and back.
- Patients often experience fever, myalgias, and arthralgias.
- Occasionally, malaise, hepatosplenomegaly, leukocytosis, and an elevated erythrocyte sedimentation rate (ESR) are associated.
- May be precipitated by isotretinoin.
Patient with acne fulminans experiences the explosive onset of inflammatory nodules, crust, and ulcerative lesions on the upper trunk, especially the midchest and shoulders. There is often a history of mild acne. The most commonly affected patients are tall, white teenage boys. Acne fulminans may be precipitated by isotretinoin therapy, testosterone therapy, or it may develop without any obvious trigger factors. Pyogenic granuloma lesions may form in the crusts.
Acne fulminans treatment
- Prednisone and topical steroids initially
- Isotretinoin later (if the acne fulminans was not precipitated by isotretinoin)
Initial therapy often requires prednisone 0.5-1.0 mg/kg/day for 4-6 weeks until control is achieved followed by slow tapering. Any crusting or pyogenic granuloma-like lesions may be treated with a potent class one topical steroid (e.g., clobetasol ointment). Despite appropriate therapy, most patients scar badly.
If the acne fulminans was precipitated by isotretinoin, the isotretinoin should be stopped and prednisone given. In such cases, the patient may be tried on isotretinoin again at a future time (low dose initially, e.g. 0.1 mg/kg/day).
If isotretinoin was not the cause, then oral isotretinoin (e.g., 0.1-0.5 mg/kg/day) may be added after 2-4 weeks of prednisone. Starting the isotretinoin too soon or at too high a dose can flare the AF. The dose should be slowly increased to 1 mg/kg/day as the acne fulminans lesions clear. A standard course of isotretinoin (e.g., with a cumulative dose of 120 mg/kg) should be given–longer if needed. The prednisone should be tapered off over 2-4 months.
Cyclosporin is an alternative to prednisone. It was successfully employed in one case at a dose of 5 mg/kg/day 1.
Figure 3. Back acne fulminans

Pityrosporum folliculitis
Pityrosporum folliculitis is an infection of the hair follicle by the fungus Malassezia furfur, formerly known as Pityrosporum ovale.
- Think of pityrosporum folliculitis when the “acne” is not improving.
- Some have called it Malassezia folliculitis.
- Predisposing conditions include hot, humid environments, excessive sweating, immunosuppression, corticosteroid or antibiotic use, adolescence, male gender, and transplantation.
- Associated diseases include seborrheic dermatitis, steroid folliculitis, acne, and tinea versicolor.
Pityrosporum folliculitis commonly involves the face and is usually described as 1-2 mm monomorphous papules and pustules that may be keratosis pilaris-like. Teenagers and young adult woman are commonly affected. The upper portion of the forehead and hairline are preferred. Many patients are on oral antibiotic, benzoyl peroxide and/or a topical retinoid. Thus, you should think of pityrosporum folliculitis when the “acne” is not improving. Truncal pityrosporum folliculitis may occur, alone or in conjunction with facial pityrosporum folliculitis. Multiple follicular pustules and erythematous papules on the upper back and/or chest and shoulders are typical. Some women have noted a flare with their menstrual cycle. The lesions may be intensely itchy. In one review, less that 20% of patients had associated seborrheic dermatitis and/or tinea versicolor 2.
Differential Diagnosis
- Acne
- Bacterial Folliculitis
- Steroid Acne
Pityrosporum folliculitis may be misdiagnosed as acne and vice versa. Acne has comedones whereas pityrosporum folliculitis does not. Some patients have developed pityrosporum folliculitis after beginning a tetracycline for acne 3. Bacterial folliculitis will respond to oral antibiotics. Steroid acne/folliculitis probably represents pityrosporum folliculitis. In the case of pityrosporum folliculitis, Wood’s light may show a yellow-green fluorescence in 2/3 of cases. KOH (potassium hydroxide) may be employed, but caution exercised as Pityrosporum is part of the normal flora.
Of course a biopsy (punch) with PAS staining to visualize the Pityrosporum species may be needed in difficult cases. A trial of an oral antifungal agent, e.g., itraconazole, which if rapidly effective, may be the easiest way to establish the diagnosis.
Pityrosporum folliculitis treatment
- An oral antifungal agent, e.g., itraconazole, fluconazole.
- Topical antifungal shampoos or creams may help or prevent recurrences.
Ketoconazole 2% shampoo lathered on the scalp and trunk for 5-10 minutes once daily initially and then tapered is usually effective. Selenium sulfide 2.5% shampoo OTC (over-the-counter) is an alternative. One may have the patient use a soap containing 2% zinc pyrithione (ZNP bar). Zinc pyrithione has activity against Malassezia furfur. Topical clotrimazole cream has been employed.
Oral itraconazole and fluconazole (for 3 weeks) may be given if necessary although rapid relapse is common. Usually, this treatment is combined with ketoconazole 2% shampoo used as a wash in the shower and left on for 3-5 minutes several times a week to prevent recurrences. Itraconazole 200 mg/day x 7 days-1 month is typical. Fluconazole 100-200 mg daily x 1-3 weeks is a typical treatment regimen. Fluconazole 400 mg po once may be used. One patient of mine has done well with itraconazole 100 mg once daily for 7 days every 1-2 months.
Figure 4. Pityrosporum folliculitis

Acne conglobata
Acne conglobata is an uncommon and unpleasant form of nodulocystic acne that typically affects the cheeks, trunk and buttocks in which there are interconnecting abscesses and sinuses (channels under the skin). These result in unsightly hypertrophic (thick) and atrophic (thin) scars. There are groups of large macrocomedones and cysts that are filled with smelly pus. In contrast to typical acne, acne conglobata usually persists well into the adult years.
Acne conglobata is occasionally associated with:
- Other disorders associated with follicular occlusion, particularly hidradenitis suppurativa, a condition in which similar boil-like lesions and scars occur in the armpits, groins and under the breasts.
- Onset is usually in early adulthood.
- Much scarring of the cheeks and back is typical.
- Some patients with acne conglobata have been reported to have a peripheral oligoarthritis.
- Acne conglobata is often part of the follicular occlusion triad along with dissecting cellulitis of the scalp and hidradenitis superativa.
- Some patients with HIV have been reported to have AC and a generalized lichen spinulosis-like eruption.
- Nodulocystic acne may very rarely be a manifestation of a genetic disorder, PAPA syndrome.
Numerous comedones, papules, pustules, nodules, abscesses, and draining sinus tracts involving the cheeks, chest, back and buttocks are typical. The lesion characteristic of acne conglobata is the larger comedone with multiple openings (agminated comedone). The patient tends to develop much scarring over time. Although there is overlap with hidradenitis superativa, Hidradenitis superativa tends to involve the body folds (e.g., occluded areas of the breasts, axilla, and groin).
Acne conglobata treatment
Oral antibiotics such as tetracycline 500 mg, doxycycline 100 mg, or minocycline 100 mg all twice daily may be tried. A course of isotretinoin may help, but is not as effective as in acne vulgaris (common acne). Adalimumab has been very effective in a small number of case reports 4. Incision and drainage of acutely inflamed or fluctuant areas may be necessary. Chronically draining sinus tracts may need to be externalized.
Figure 5. Acne conglobata
What causes back acne
Acne is due to a combination of factors. The exact mechanisms are not fully understood.
- A combination of clogged pores and an infection of the follicles by the bacteria Cutibacterium acnes (C. acnes, formally known as Propionibacterium acnes)
- Comedones, then papules, pustules and nodules are present.
- Cutibacterium acnes resistance to antibiotics is widespread.
- Onset is earlier now. Acne may be the first sign of onset of puberty in children 7 to 11 years of age.
- Acne in an adult woman may be a manifestation of hyperandrogenism. See acne in a woman.
- Associations: insulin resistance in adult men with acne and low-fat/skim milk but not full-fat milk in teenagers with acne 5. Acne in late adolescence is associated with an increased risk of prostate cancer later in life 6.
- Familial tendency
- Acne bacteria
- Endogenous and exogenous androgenic hormones
- Innate immune activation with inflammatory mediators
- Distension and occlusion of the hair follicles
Flares of acne can be provoked by:
- Polycystic ovarian disease or Polycystic ovary syndrome (PCOS)
- Drugs: steroids, hormones, anticonvulsants, epidermal growth factor receptor inhibitors and others
- Application of occlusive cosmetics
- High environmental humidity
- Diet high in dairy products and high glycemic foods.
How do bacteria affect acne?
At puberty, the number of bacteria on the skin surface increases. These include:
- Cutibacterium acnes (C. acnes, formally known as Propionibacterium acnes)
- Corynebacterium granulosum (also known as Cutibacterium acnes and formally known as Propionibacterium granulosum)
- Staphylococcus epidermidis (coagulase-negative staphylococcus).
The number of malassezia yeasts probably also increases.
However, the severity of a person’s acne does not depend on the number of bacteria on the skin surface or in the sebaceous ducts (the passageway from the oil glands).
The number and activity of Cutibacterium acnes bacteria varies according to oxygen supply, nutrient supply and the pH level of the skin. Some acne lesion are colonized by Cutibacterium acnes and others are not.
The Cutibacterium acnes bacteria can produce active enzymes and innate inflammatory mediators and these may contribute to the activity of acne in some patients. Activation triggers expression of immune response genes. Inflammatory mediators detected in acne lesions colonized by Cutibacterium acnes include:
- Lipases (enzymes that break down fats)
- Proteases (enzymes that break down proteins)
- Hyaluronate lyase (enzyme that breaks down skin ground substance)
- Phosphatase (enzyme that breaks down phosphates)
- Smooth-muscle contracting substances
- Cytokines, such as IL-12 and IL-8, and defensins (these are chemical messengers).
The lipases can convert triglyceride in sebum to free fatty acids. The free fatty acids increase clumping of bacteria in sebaceous ducts and thus the colonisation of the ducts by more of them. The inflammatory mediators provoked by the bacteria penetrate surrounding skin and are a cause of inflammation.
What is the effect of treatment on acne bacteria?
Antimicrobials such as topical benzoyl peroxide and oral tetracyclines suppress Cutibacterium acnes in patients with acne. They also have non-antibiotic anti-inflammatory activity.
Twenty years ago, Cutibacterium acnes was readily killed by erythromycin, clindamycin and the tetracyclines. Unfortunately, after decades of use, widespread antibiotic resistance by Cutibacterium acnes has emerged. These drugs are much less effective. Thus, acne therapy has shifted to emphasizing the use of benzoyl peroxide, the topical retinoids, and oral isotretinoin.
Acne friendly skin care essential
To get the results you expect from treatment, you’ll also need acne friendly skin care. Without it, your acne can flare, even when you’re treating it.
To help their patients with back acne get the best results, dermatologists recommend the following 7:
1)Develop these habits when working out or getting sweaty:
- Wear loose-fitting workout clothes made of cotton or sweat-wicking fabric.
- Wash workout clothes after each use.
- Shower and change clothes ASAP after working out (or doing anything that causes you to sweat).
If you cannot shower immediately, use an oil-free cleansing wipe to gently wipe off your sweaty skin. You’ll also want to change out of sweaty clothes.
2) Cleanse your skin gently. Scrubbing skin with acne may seem best, but this actually worsens acne. When washing your back and applying acne treatment, you want to be gentle.
3) Stop irritating your skin with harsh skin care products. Antibacterial soaps, astringents, and abrasive scrubs can worsen acne. Ditto for loofahs, back brushes, and buff puffs. For best results, you’ll want to use gentle, fragrance-free skin care products.
4) Use oil-free skin care products and cosmetics. The packaging may read “non-comedogenic,” “non-acnegenic,” “won’t clog pores,” or “oil-free.
5) Avoid using anything that rubs against your back, such as a backpack. Anything that rubs against your back can irritate your skin, causing back acne to flare. Swap a backpack for a handheld bag. If you carry a purse on your shoulder, place the strap on your arm.
6) Resist the temptation to pick and pop acne, even on your back. This will only worsen acne.
7) Protect your skin from the sun. People often believe that the sun’s rays will help clear acne, but the sun can actually worsen acne. The sun’s rays tend to darken acne and cause it to last longer.
When shopping for sunscreen, choose one that says the following on the packaging:
- Non-comedogenic (or oil-free)
- SPF 30 (or higher)
- Broad-spectrum protection (UVA/UVB protection)
- Water resistance
You can help clear acne by always wearing oil-free sunscreen when outdoors. You’ll want to apply sunscreen to all skin that clothes won’t cover.
8) Change your sheets and pillowcases weekly. Clean sheets and pillowcases are essential for clearing back acne. You may want to change pillowcases twice a week. By the end of a week, sheets and pillowcases are swarming with dead skin cells and bacteria.
When washing sheets and pillowcases, be sure to use fragrance-free detergent. If you like fabric softener, it, too, should be fragrance-free.
How to get rid of back acne
Treatment of acne depends on its severity – mild, moderate or severe.
General principles of back acne treatment
- Acne can be effectively treated, although response may sometimes be slow.
- Where possible, avoid excessively humid conditions such as a sauna, working in an unventilated kitchen or tropical vacations.
- Consider a low-glycemic, low-protein and low-dairy diet (note that the evidence that this helps is weak). Avoid protein or amino acid supplements, particularly if they contain leucine. Eat plenty of fresh fruit and vegetables.
- If you smoke, stop. Nicotine increases sebum retention and increased scale within the follicles, forming comedones (blackheads and whiteheads).
- Minimize the application of oils and cosmetics to the affected skin.
- Abrasive skin treatments can aggravate both comedones and inflammatory lesions.
- Try not to scratch or pick the spots.
- Exposure to sunlight filtered through window glass can help – see information about lasers, lights and acne. To avoid sunburn, protect your skin outdoors using a sunscreen and protective clothing.
Management of mild acne
Most patients with mild acne can be treated with topical treatment (gels, solutions and lotions) that can be obtained over-the-counter without prescription. Most people just use topical agents for facial skin as they can be difficult to apply to one’s back. Extra vitamins and minerals have not been proved to help.
- Wash affected areas twice daily with a mild cleanser and water or an antiseptic wash.
- Acne products should be applied to all areas affected by acne, rather than just put on individual spots.
- A thin smear should only be applied to dry clean skin at nighttime.
- Acne products may work better if applied in the morning as well.
- They often cause dryness particularly in the first 2–4 weeks of use. This is partly how they work. The skin usually adjusts to this.
- Apply an oil-free moisturizer only if the affected skin is obviously peeling.
- Avoid applying oily cosmetics such as foundation or sunscreen.
- It may take several weeks or even months to see convincing improvement.
- Discontinue using product if severe irritation results. See your doctor for advice.
Acne Cleansers
Acne cleansers help to remove excess oil from the skin, as well as make-up, sweat, and dirt, which can all accumulate on the surface of the skin. Cleansing is important for general skin hygiene too, as it is easy for all of these substances to build up on the skin.
General Tips:
- Do not over-cleanse as it will worsen, and not improve your acne
- Choose appropriate products for your skin type
- Be patient—topical medication takes time to work, and often worsen acne when first used until the skin becomes used to it
- Look for non-comedogenic cleansers cosmetics as they are less likely to aggravate your acne
It is important not to over-cleanse the skin. Acne cleansers can help to reduce oil and dirt, and contains ingredients that help reduce acne. They are an important part of acne treatment and maintenance. It is important to note, however, that more is not better when it comes to acne treatment. For most cleansers, one wash at night should be sufficient, and the skin should be patted dry gently.
Suitable topical agents for mild acne that can be obtained without prescription include:
- Antiseptic washes with triclosan or benoyl peroxide (Acnederm wash™, Benzac™ AC Wash, Dalacin™ T Prewash, Oxy™ Daily Skin Wash)
- Mild salicylic acid preparations to exfoliate and unplug the follicles (Neutrogena® Oil-free Acne Wash and many others)
- Benzoyl peroxide cream/lotion/gel (PanOxyl™ Acne Gel, Brevoxyl™ Cream, Oxy-10™, Clearasil™ Ultra Acne Cream, Benzac AC Gel)
- Azelaic acid (Skinoren™ cream, Acnederm™ medicated lotion, Azclear™ Action Lotion)
- Hydrogen peroxide in stabilised cream (Crystacide®, Crystaderm™)
- Immune defence proteins (Epiology®)
- Tea tree oil, bee venom, polyphenols and other products for which evidence of efficacy is limited.
How to apply medicine to your back
- For treatment to work, you must get it on your back. Investing in a lotion applicator for the back can help you apply the medicine where you want it.
- If you’re not sure where to find one of these, just search online for a “lotion applicator for the back.”
Benzoyl peroxide (emollient foam wash) + Retinoid (adapalene 0.1% gel)
Benzoyl Peroxide (emollient foam wash): This helps to kill the bacteria that cause acne. Used daily, it can help control back acne and reduce flares.
Benzoyl peroxide is an excellent antimicrobial agent in the treatment of acne. It kills Cutibacterium acnes in such a fundamental way that resistance cannot occur. It is over-the-counter (OTC) and usually should be purchased by price as most consumers are happy with the cheaper brands. As with all topical acne treatments, spot treating is not recommended. Apply all over acne-prone skin daily to prevent lesions. You should be aware that benzoyl peroxide bleaches carpet, clothing, and towels–but not skin or hair. The lower doses are preferred, e.g., 2.5-5%. The benzoyl peroxide washes reduce Cutibacterium acnes counts less than the leave-on benzoyl peroxide formulations, but they are more patient-friendly. The longer the contact time (at least 20 seconds) the better. They seem to work best on the face, but not so much on the trunk.
Unfortunately, one study showed that most patient do NOT follow the recommendation to buy and use OTC benzoyl peroxide. In that study of 84 patients told to buy and use a benzoyl peroxide-containing product, only 64% bought an OTC product, and of those products only 32% had benzoyl peroxide as the active ingredient. Thus, only 20% of patient told to buy an OTC benzoyl peroxide-containing product actually did so 8. Implications for therapy include better education of the patient, follow up calls to reinforce, specific recommendations for products to purchase and to give benzoyl peroxide as a prescription, e.g. benzoyl peroxide with erythromycin, benzoyl peroxide with adapalene (adapalene 0.1% gel).
Studies show that the key to getting results from a benzoyl peroxide wash is to leave it on your back for 2 to 5 minutes before rinsing it off.
Letting the benzoyl peroxide sit on your skin for a few minutes has two advantages:
- This approach helps the medicine penetrate your skin. Skin is thicker on the back than on the face.
- Rinsing it off prevents bleached clothes, sheets, and towels. Benzoyl peroxide is known to bleach fabrics.
You’ll find over-the-counter (OTC) benzoyl peroxide foaming washes in different strengths. Using a product that contains 5.3% benzoyl peroxide is less likely to cause irritated skin, dryness, or peeling.
If you feel that you need stronger medicine, you can start with a foaming wash that contains 10% benzoyl peroxide. That’s the strongest concentration of benzoyl peroxide that you can buy without a prescription.
Retinoid (adapalene 0.1% gel): Using this along with benzoyl peroxide can improve your results. This OTC retinoid can help unclog pores, which will help the benzoyl peroxide work better.
Topical Retinoids
Tretinoin, adapalene, and tazarotene are all excellent topical agents for reducing the blackheads and whiteheads of acne. They are applied once a day, usually at night (with benzoyl peroxide in the morning). Peeling and redness are the main side effects. Tazarotene is the strongest, but also the most irritating. Adapalene may be the least irritating. A combination product of benzoyl peroxide and adapalene (Epiduo in the US) is available and is a nice product. Combining a topical retinoid with a salicylic acid-containing cleanser often causes too much irritation and should be avoided.
Irritation with the use of topical retinoids is common. Strategies to combat this include:
- Starting therapy every other night.
- Delaying the application of the retinoid after washing the face (e.g. 20 min-1 hour).
- Using a mild cleanser instead of soap.
- Using a non-comedogenic moisturizer 2/day.
- Applying a topical steroid (e.g. triamcinolone 0.025% cream) to the face after applying the retinoid.
One split-face study found the addition of triamcinolone 0.025% to the first 4 weeks of 0.05% tretinoin treatment greatly decreased dryness and peeling, increased compliance, and decreased acne severity 9. No atrophy was observed.
Dermatologists recommend applying adapalene after you shower or before going to bed. Again, you want to apply it daily.
Topical agents for mild acne which require prescription include:
- Antibiotics, such as clindamycin solution (Topicil™, ClindaTech™) or erythromycin solution (Stiemycin™) and gel (Eryacne™), which are best used with benzoyl peroxide or azelaic acid to reduce the chance of antibiotic resistance
- Retinoids i.e. tretinoin (ReTrieve™, Retin-A™), isotretinoin (Isotrex™), adapalene (Differin™); in some countries, adapalene is available without prescription.
Combination prescription topicals include clindamycin / benzoyl peroxide (Duac™) and adapalene/benzoyl peroxide gel (Epiduo™).
Topical clindamycin and erythromycin have been used for years in the treatment of acne. Unfortunately, that prolonged use has lead to widespread Cutibacterium acnes resistance and their efficacy is now much less.
Lights and lasers including blue light have been found to be safe and helpful for mild to moderate acne when oral medications are unhelpful or unsuitable.
See your doctor or dermatologist for advice if your pimples fail to clear up within six weeks or you have severe acne.
Management of moderately severe acne
Treatment for moderately severe acne usually includes the topical agents described above. In addition, oral medication may be prescribed, usually for at least 3–6 months.
Suitable oral medications include:
- Antibiotics such as tetracycline, minocycline, doxycycline or trimethoprim
- The combined oral contraceptive pill, in females
- Oral antiandrogens, such as low-dose cyproterone (in combination with oestrogen), and/or spironolactone, particularly if there are signs of hyperandrogenism
- Short-term use of nonsteroidal anti-inflammatory agents such as ibuprofen or naproxen
- Oral isotretinoin for resistant or persistent acne.
When oral antibiotics are discontinued, control should be maintained long term by continuing topical therapy.
Doxycycline
Doxycycline is widely used at 100 mg oral twice daily. Stomach upset is a common problem as is photosensitivity (look for red skin on the nose and dorsal hands). It should be taken with food and the patient should use sunscreen. In July 2014, the FDA approved Acticlate (doxycycline hyclate 75 mg and 150 mg tablets) for a number of infections including adjunctive therapy in severe acne.
Submicrobial dosing of doxycycline (20 mg oral twice daily) for acne has been evaluated in a few studies and only one that we can find that was placebo controlled. In that the mean change (reduction) in total inflammatory lesions from baseline to the end of treatment (6 months) was 50% in the doxycycline 20 mg oral twice daily group and 30% in the placebo group 10. Another study has been published, but it was not placebo controlled 11. So there is benefit, but it does not seem robust.
Minocycline
Minocycline is widely used at 100 mg oral twice daily. It can cause nausea and dizziness initially, especially in women. There is less photosensitivity than doxycycline, but a higher rate of side effects, e.g., allergic rash, dizziness, blue discoloration of skin, nails, or teeth over the long term, bruises that don’t go away, and hyperpigmentation of the lips or tongue.
Septra DS
Septra DS (double strength) is an excellent antibiotic for acne if the tetracyclines fail and the patient prefers to avoid isotretinoin. It contains 160 mg trimethoprim and 800 mg sulfamethoxazole and is given orally twice daily with topical benzoyl peroxide morning and a retinoid nightly. Unfortunately, it has several major drawbacks. First, there is a 4% risk of allergic rash in women and 2% in men. For this reason, patients may take only one pill a day for the first 10 days. If no rash, then they can go on to taking it twice daily. Second, widespread use of this agent may lead to antibiotic resistance, making it less useful for other more serious infections.
Azithromycin
Various reports have suggested benefit with azithromycin in acne.
- Pulsed oral azithromycin (500 mg/day over three consecutive days every 2 weeks) was used in conjunction with low-dose isotretinoin in one study.
- In Egypt, one study showed resistance of Cutibacterium acnes lowest to azithromycin (compared with doxycycline, clindamycin, and erythromycin)
- In another study, the following was used: three monthly pulses of azithromycin 500 mg for 3 consecutive days.
- Azithromycin, 500 mg orally thrice weekly for 8 weeks
Risk of Long-Term Antibiotics for Acne
Long-term use of oral antibiotics greatly increases the risk of antibiotic resistance. But does the long-term use of an oral antibiotic for acne in some way adversely affect the health of the patient? In one small study, the odds of reporting pharyngitis was 3 times more likely in patients receiving oral antibiotics for acne than in controls.
Moderate acne treatment
- Oral tetracycline class antibiotic plus benzoyl peroxide and topical retinoid.
- Don’t give an oral antibiotic alone–without topical therapy–as you always want to transition off oral antibiotics.
- For females, consider hormonal therapy.
- Topical clindamycin or erythromycin should not be given as monotherapy (as it runs the risk of resistance to Cutibacterium acnes)
- If scarring is present or the acne is resistant to the above, give isotretinoin.
- Try to limit any course of an oral antibiotic to 3 months.
The following may also be prescribed:
- High dose oral antibiotics for six months or longer
- In females, especially those with polycystic ovary syndrome, oral antiandrogens such as oestrogen/cyproterone or spironolactone may be suitable long-term
- Systemic corticosteroids are sometimes used
For moderate disease, e.g., acne with deeper, cystic papulonodules, the use of an oral antibiotic is needed. The tetracyclines are the mainstays of therapy, but again, after decades of use, Cutibacterium acnes resistance has developed and these agents are not nearly as effective as 20 years ago.
- Tetracycline 500 mg oral twice daily (Cutibacterium acnes resistance has made this agent much less effective)
- Doxycycline 100 mg oral twice daily
- Minocycline 100 mg oral twice daily
The typical antibiotics, listed above, are given for 3 months in combination with topical benzoyl peroxide every morning and a retinoid nightly. After 3 months, if control is achieved, stopping the oral antibiotic is recommended. If one agent is not effective, then the patient may be switched to another. In general, if one tetracycline does not work, it would be more advantageous to switch to either Septra or azithromycin than a different tetracycline. If two sequential oral antibiotics along with topical therapy is not sufficient to provide good control of the acne (and prevent scarring), then a course of isotretinoin is recommended. Anyone who gives isotretinoin must be trained in its use as it is highly teratogenic and has many potential side effects. For adult women, alternative therapies exist.
Acne treatment for adult women
The adult woman with acne tends to primarily have inflammatory lesions (few visible comedones). The distribution of these lesions is typically along the jawline and chin (as opposed to the teenage pattern of acne uniformly distributed on the face). Flaring premenstrually is common. Rosacea should be excluded. Inquiry should be made about menstrual disturbances, impaired fertility, and hirsutism (see also polycystic ovary syndrome).
In one study from Brazil of 835 women with acne, workup showed that 54.56% of the patients had hyperandrogenism and the levels of DHEAS (Dehydroepiandrosterone) were most frequently elevated 12. One drawback to this study, however, is that the exact criteria of “altered” or abnormal blood tests were not provided.
Causes of Hyperandrogenism in Women
- Polycystic ovary syndrome [PCOS] (80% of all hyperandrogenism in women)
- Androgen-secreting neoplasm (adrenal or ovary)
- Nonclassical congenital adrenal hyperplasia
- HAIR-AN (Hyperandrogenism, insulin resistance, acanthosis nigricans
- Hyperandrogenism and hirsutism
- Exogenous steroid administration
Workup
Blood work for androgens optimally should be obtained during the follicular phase (from menses to ovulation–classically days 1-14), optimally between the fourth and the seventh day of the cycle (day 1 is the first day of the period, day 14 is ovulation), and oral contraceptives should be discontinued for at least two months prior to this testing. The blood draw should be in the morning (highest level of testosterone), preferably before 8:30 AM and fasting.
Full hormonal workup can include DHEAS, free testosterone, sex-hormone binding globulin, prolactin, 24-hour urine cortisol, 17-OH progesterone, thyroid-stimulating hormone (TSH), pregnancy test, follicle-stimulating hormone (FSH) and luteinizing hormone (LH), and pelvic ultrasound.
Treatment for adult woman acne
- The usual conventional approaches: benzoyl peroxide, a topical retinoid, oral antibiotics, and isotretinoin.
- Dospirenone-containing birth control pills (e.g., Yasmin, Yasminelle, Yaz, Beyaz, Ocella, Zarah, Daylette, and Angeliq) are FDA-approved for the treatment of acne.
- Spironolactone 50-100 mg/day (do not give along with trimethoprim-sulfamethoxazole due to risk of hyperkalemia.)
- Cyproterone acetate-containing birth control pills are not FDA-approved in the US, but show benefit for both acne and hirsutism.
Women with acne often do well using conventional approaches to acne therapy (e.g., topical retinoids, benzoyl peroxide, minocycline, etc.) If these fail, isotretinoin is usually given. In those women who relapse after a course of isotretinoin, hormonal workup and therapy is most helpful.
Drospirenone
Drospirenone-containing birth control pills are effective for both acne and hirsutism. Drospirenone is a derivative of spironolactone and at usual doses, is equivalent to 25 mg of spironolactone. Because drospirenone can cause hyperkalemia, caution should be taken when patients are on other medications that may increase the potassium.
The absolute risk of venous thromboembolism in events/100,000 woman-years is 13:
- 6-92 for traditional levonorgestrel-containing birth control pills
- 23-137 for drospirenone-containing birth control pills
- 200 for pregnancy
Spironolactone
- 50-100 mg/day for acne.
- Side effects include menstrual irregularities and rarely hyperkalemia.
- Do not give along with trimethoprim-sulfamethoxazole–increases risk hyperkalemia.
- In pregnancy, can feminize the male fetus.
- Spironolacone is okay for lactating women.
- Typically given with drospirenone-containing (or traditional) birth control pills.
Spironolactone is relatively safe and may be given to the woman already on a drospirenone-containing (or traditional) birth control pill. One study of 200 person-years of exposure to spironolactone and 506 person-years of followup over 8 years found no serious illnesses thought to be attributed to spironolactone 14. With respect to breast, uterus, ovarian, and cervical cancer, there does not seem to be evidence of increased risk with spironolactone 15. One study found the combination of spironolactone 100 mg/day and drospirenone/ethinyl estradiol 30 ug efficacious, safe, and well-tolerated 16. Do not, however, give spironolactone along with trimethoprim-sulfamethoxazole. That combination in one study was more than 12 times likelier than spironolactone/amoxicillin to cause hyperkalemia. In the elderly, giving trimethoprim-sulfamethoxazole to a patient on spironolactone puts them at risk for sudden death.
Prior to starting spironolactone, the potassium, pregnancy test, DHEAS, and free testosterone may be checked. Note that even though these women are thought to have a hormonal connection to their acne, the hormone levels are usually normal. Spironolactone (e.g., 50-100 mg/day) may be started. Side effects the patient should be made aware of include headache, lethargy, menstrual irregularities (usually not a problem if the patient is on a birth control pill), hyperkalemia, breast tenderness, and decreased sex drive. These side effects are less common at 100 mg/day or less. Women who wish to become pregnant, who are on antihypertensives, cardiac drugs, or diuretics should not take spironolactone. The patient needs to wait at least 3 months to see the full effect. Some women will note decreased facial oiliness. Women with baseline low blood pressure may have trouble with lightheadedness and even syncope. The blood pressure should be monitored at followup visits.
A national acne expert recommends spironolactone for all females with acne (as young as 11 years of age) who fail to respond to 3 months of a topical benzoyl peroxide and a retinoid. He may give it alone or in combination with birth control pills. If this is not sufficient to control the acne after 3 months, he moves on to isotretinoin.
One Expert’s Acne Algorithm for Females of any Age.
- Topical benzoyl peroxide and a retinoid for 3 months.
- Add spironolactone x 3 months
- Add birth control pill x 3 months
- If the above fails, monotherapy with isotretinoin.
Not that this totally eliminates the use of antibiotics for acne.
Physical treatments for acne
- Sunlight is anti-inflammatory and can help briefly. However, exposure to ultraviolet radiation results in ageing skin and can eventually lead to skin cancer.
- Lasers and other light systems using visible light wavengths, appear safe and helpful for acne. Treatment is often delivered twice weekly for four weeks. The effect may be enhanced by use of a photosensitising agent (photodynamic therapy).
- Cryotherapy (freezing treatment) may be useful to control new nodules.
- Intralesional steroid injections can be used to shrink older nodules and pseudocysts.
- Comedones can be expressed or removed by cautery or diathermy (electrosurgery).
- Microdermabrasion can help mild acne.
- Note: X-ray treatment is no longer recommended for acne, as it may cause skin cancer.
Management of severe acne
Treatment for severe acne requires oral treatment. Patients should be under the care of a dermatologist.
Many patients will be treated with oral isotretinoin. Isotretinoin is the treatment of choice.
Isotretinoin
Isotretinoin (13-cis retinoic acid) is a vitamin-A derivative (retinoid). The liver naturally makes small quantities of isotretinoin from vitamin-A, but the drug dermatologists prescribe is made synthetically.
Isotretinoin was developed in the 1950s, but only started being used in the mid 1970s. The original brand names were Accutane® and Roaccutane®, but there are now many generic versions on the market, of varying potency.
In acne, isotretinoin:
- Reduces sebum production
- Shrinks the sebaceous glands
- Reduces follicular occlusion
- Inhibits growth of bacteria
- Has anti-inflammatory properties.
Other uses for isotretinoin
Isotretinoin is a very effective medication for the treatment of acne. Originally licensed for use in severe disease, it is increasingly prescribed for all grades of acne.
Isotretinoin is also useful for other follicular conditions, such as:
- Rosacea
- Seborrhoea
- Hidradenitis suppurativa
- Scalp folliculitis.
Isotretinoin is also prescribed for many other skin diseases. Examples include:
- Discoid lupus erythematosus
- Granuloma annulare
- Grover disease
- Sarcoidosis
- Extensive actinic keratoses
- Prevention of cutaneous squamous cell carcinoma.
Isotretinoin has also been used as an adjuvant in neuroblastoma.
What is the usual dose of isotretinoin?
The range of doses used each day for acne is less than 0.1 to over 1 mg/kg body weight. Some patients may only need a small dose once or twice a week. A course of treatment may be completed in a few months or continue for several years.
It is common to start at a lower dose initially, e.g. 0.5 mg/kg/day, for a month to get the patient used to the medication, and prevent flaring. If there are no symptomatic or laboratory issues and no crusted acne flaring at one month, the patient may be advanced to 1 mg/kg/day and stay at that for the rest of the course, till the face is clear. For acne, some prescribers have targeted a total cumulative dose of 120–140 mg/kg, in the hope of reducing relapse, but the evidence for this remains controversial. The general trend has been to use lower dosages, unrelated to body weight (eg 10 mg/day).
If there is significant inflammation and crusting at the outset, an even lower dose, e.g. 0.1 mg/kg/day is recommended. As the inflammation clears, the dose may be advanced.
Blasiak et al published a study of 180 patients at a single institution 17. At one year follow up, those who had received 220 mg/kg total dose were less likely to have relapsed than those that received less than 220 mg/kg. However, these patients had higher side effects persistent at 1 year e.g. decreased hearing and muscle pains. Also, to get this level of total dose, you either have to give high daily doses, e.g. 120 mg/day as in this study or go for 7-8 months at 1 mg/kg/day.
In one study 18, the treatment regimen consisted of isotretinoin, fixed 20 mg daily, and duration of treatment-based on the weight of patient, until total cumulative dose of 120 mg/kg was achieved. This lead to a treatment duration from 10-22 months. The relapse (five year follow up) was only 8%. One significant drawback to this approach is the longer exposure to a highly teratogenic drug for female patients of child-bearing potential.
What predicts patients with acne more likely to relapse?
- Early onset (e.g. if a 12-year-old needs isotretinoin, a second course of isotretinoin will probably be needed before age 16.)
- Severe acne, male, truncal acne
- Women with hyperandrogenism
The key determinant of relapse of acne after a course of isotretinoin is age.
| Age at Treatment | Need for 2nd course |
|---|---|
| 10-11 years | 35-40% |
| 12-14 years of age | 20% |
| 15 and older | 10-15% |
The individual dose prescribed by the dermatologist for acne depends on:
- Prescriber preference
- Patient body weight
- The specific condition being treated
- Severity of the skin condition
- Response to treatment
- Other treatment used at the same time
- Side effects experienced.
All forms of isotretinoin except Absorica should be taken with a fatty meal or milk after food to help with its absorption. Taking isotretinoin with food doubles absorption 19. Absorica (isotretinoin-lidose) is isotretinoin combined with a material that improves absorption. Thus, Absorica can be taken with or without food. Isotretinoin may be taken on an empty stomach, but absorption may be halved. There is no particular advantage in splitting the dose over the day.
For how long is isotretinoin taken?
Most patients should be treated until their skin condition clears and then for a further few months. However, courses have often been restricted to 16–30 weeks (4–7 months) to minimise risk of teratogenicity (risk of congenital abnormalities), and to comply with local regulatory authorities. Isotretinoin may be prescribed for years, usually in low dose or intermittently.
Does acne ever fail to clear on isotretinoin?
Although isotretinoin is usually very effective for acne, occasionally it responds unexpectedly slowly and incompletely. Poor response is associated with:
- Macrocomedones (large whiteheads)
- Nodules (large, deep inflammatory lesions)
- Secondary infection
- Smoking
- Polycystic ovarian syndrome
- Younger age (< 14 years).
Options available to slow responders include:
- Electrocautery of comedones
- Prolonged course of isotretinoin
- Additional treatment with oral antibiotics and oral steroids.
Can isotretinoin be used again if acne recurs?
At least fifty per cent of patients with acne have a long lasting response after a single adequate course of isotretinoin. In others, acne may recur a few months to a few years after the medication has been discontinued. Relapse is more common in females than in males, and in patients > 25 years of age. These patients may receive one or more further courses of isotretinoin.
Long-term treatment (> 1 year) is often used for patients with:
- Persistent acne
- Seborrhoea
- Rosacea
- Scalp folliculitis
- Skin cancer.
Contraindications to isotretinoin
- Isotretinoin must not be taken in pregnancy, or if there is a significant risk of pregnancy.
- Blood donation by males and females on isotretinoin is not allowed in case the blood is used for a pregnant woman.
Precautions when taking isotretinoin
- Isotretinoin should be used with caution during breastfeeding.
- Commercial pilots may be subject to flying restrictions if they take isotretinoin.
- High dose isotretinoin in very young children has been associated with premature epiphyseal closure, leading to shorter stature (this is not seen in low dose used for the treatment of acne).
Special precautions for pilots considering isotretinoin
Good night vision is important for airline pilots and those flying after dark. Night vision may be affected by isotretinoin. True decreased night vision may occur, but is rare. When it does occur, it usually does so within several weeks of starting the isotretinoin. Pilots taking isotretinoin or considering a course of isotretinoin must report to their national aviation authority to discuss how this treatment affects their flying privileges.
Monitoring isotretinoin
- Pregnancy must be excluded before and during treatment with isotretinoin
In an otherwise healthy individual, blood tests are generally not needed. However, consider the following if using high dose (1 mg/kg/day), prolonged courses (> 12 months), or if patients have specific risk factors (eg, family history of dyslipidaemia, higher risk of viral hepatitis, etc):
- Pregnancy test baseline and monthly for females of childbearing potential.
- Cholesterol and triglyceride levels: Baseline, and 8 weeks.
- Liver function tests: Baseline and 8 weeks.
- Blood count.
- Additional tests should be done if any are abnormal.
Isotretinoin may cause hypertriglyceridemia, and patients with baseline elevated triglyceride are at particular risk. Hypertriglyceridemia for 4-5 months is not thought to convey significant cardiac risk. However levels above 800-1000 can trigger pancreatitis, although this is rare. Patients have been known to tolerate triglyceride levels in the 4000’s mg/dl without experiencing pancreatitis. In fact, pancreatitis during isotretinoin therapy is more likely idiosyncratic and unassociated with hypertriglyceridemia. In a meta-analysis covering the last 46 years 20, 25 cases of pancreatitis in patients on isotretinoin were found but only four had hypertriglyceridemia associated.
Therefore, baseline fasting triglyceride levels should be measured. If elevated, retesting 4 weeks into isotretinoin therapy is in order. It has been argued that patients with normal baseline triglyceride and no other risks for hypertriglyceridemia do not need further monitoring 20. In fact, that paper goes further and states that “baseline triglyceride monitoring is unnecessary for typical teenagers if they have no other risk factors for elevated triglycerides.” However, the current consensus for all patients on isotretinoin is to measure fasting triglycerides at baseline and if normal, to retest at 2 months. For any patients with significant hypertriglyceridemia, dose reduction, diet modification and rarely, additional medications are in order. For example, gemfibrozil is very effective in treating retinoid induced hyperlipidemia 21. A typical gemfibrozil dose would be 600 mg twice daily (30 minutes before the morning and evening meals).
Gamma-Glutamyl Transferase (GGT) may be a more useful test for the liver. Creatine kinase (CK) elevations (from muscle, e.g., young athletic men) are relatively common. It may make sense to monitor creatine kinase (CK) in athletically active patients 22.
Oral isotretinoin may cause an elevation of liver enzymes, however any changes are typically asymptomatic and transient and can resolve even with continuing therapy. Clinically apparent liver injury due to isotretinoin is exceedingly rare. Elevations in liver function tests during isotretinoin therapy may be unrelated and alcohol consumption, the taking of supplements (e.g., protein, creatine, or herbal extracts) or intercurrent illness should be excluded 23. The isotretinoin should be stopped if liver function test levels are greater than 2-3x normal and any abnormalities should be followed until they normalize.
A reversible myopathy has been seen 24. In one study of 89 patients with acne treated with isotretinoin 25, elevated creatine kinase (CK) levels were found in five patients. Maximum serum creatine kinase (CK) values ranged between 292 and 569 IU/l. Only one patient out of five had myalgia and four patients were completely asymptomatic. Males that exercise vigorously are at highest risk of elevated creatine kinase (CK) levels. For any values over 1000, the patient may be told hold the isotretinoin until levels improve, cut back on exercising and drink plenty of fluids.
Should isotretinoin be stopped before surgery?
Although there is concern that isotretinoin could interfere with wound healing, the overall the risk described in the larger and better reported studies is relatively small or absent 26 and 27.
Contraception in females considering isotretinoin
Isotretinoin must NOT be taken in pregnancy because of a very high risk of serious congenital abnormalities in the baby. Caution needs to be used during breast-feeding as it enters the breast milk and might affect the baby.
All females who could biologically have a child should take the following precautions during treatment with isotretinoin and for four weeks after the medication has been discontinued:
- Abstinence. The most reliable method of avoiding pregnancy is not to have sex. No method of contraception is completely reliable. “Natural” family planning is particularly risky.
- 19% of those who chose abstinence do not.
- 34% of those sexually active did not comply with 2 forms of birth control.
- Abstinence” accounts for 12%-14% of pregnancies in iPledge 28.
- If sexually active, two reliable methods of contraception should be used. Discuss contraception with your doctor (general practitioner, family planning specialist, gynaecologist or dermatologist). The combined oral contraceptive, IUD (intrauterine device), progesterone implant, or medroxyprogesterone injections may be suitable.
- The low-dose progesterone mini-pill on its own is not recommended.
A prescription for emergency contraception may be available from a medical practitioner (your family doctor or family planning clinic) or accredited pharmacy. It prevents 85% of pregnancies if taken within 72 hours of unprotected sexual intercourse.
If contraception fails, termination of pregnancy (an abortion) may be advised if pregnancy arises during treatment with isotretinoin or within a month of discontinuing it.
What happens if a pregnant woman takes isotretinoin?
Isotretinoin has a very high chance of resulting in a spontaneous miscarriage or a severe birth deformity if a fetus is exposed to it during the first half of pregnancy. The deformities affect the growth of tissues developing at the time of exposure to the drug:
- Cranium (skull and brain)
- Cardiac (heart)
- Eye, ear
- Limbs.
No contraceptive precautions are necessary for men
Isotretinoin has no effect on sperm or male fertility and has not been shown to cause birth defects in children fathered by men taking it.
What are the side effects and risks of isotretinoin?
The side effects of isotretinoin are dose dependent; at 1 mg/kg/day, nearly all patients will have some side effects, whereas at 0.1 mg/kg/day, most patients will not. The range and severity of the side effects also depends on personal factors and the disease being treated.
Patients with significant liver or kidney disease, high blood fats, diabetes and depression may be advised not to take isotretinoin or to be on a lower dose than usual and to have regular follow-up visits.
Cutaneous and mucocutaneous side effects
Most of the side effects due to isotretinoin are cutaneous or mucocutaneous and relate to the mode of action of the drug. The most common are listed here. When side effects are troublesome, isotretinoin may need to be withheld or the dose reduced.
- Acne flare-up (particularly if starting dose is > 0.5 mg/kg/day)
- Dry lips, cheilitis (sore, cracked or scaly lips) (100% of patients on 1 mg/kg/day)
- Dry skin, fragile skin, eczema/dermatitis (itchy, red patches of skin). Note: atopic eczema may improve.
- Increased sweating
- Dry nostrils, epistaxis (nose bleeds)
- Dry, watery or irritable eyes (especially in contact lens wearers), conjunctivitis, keratitis
- Dry anal mucosa, bleeding at the time of a bowel motion
- Dry genitals, dyspareunia (discomfort during intercourse)
- Facial erythema
- Sunburn on exposure to the sun
- Temporary hair loss
- Brittle nails
- Skin infections: impetigo, acute paronychia, pyogenic granuloma
Treatment of mucocutaneous side effects
- Reduce the dosage (eg, to 5–10 mg/day)
- Emollients, lip balm, petroleum jelly, sunscreen, eye drops and lubricants should be applied frequently and liberally when needed
- Dermatitis can be treated with topical steroids
- Take short, cool showers without using soap
- Use mild or diluted shampoo
- Do not start wearing contact lenses for the first time
- Do not have elective eye surgery while on isotretinoin or for 6 months afterwards.
- Do not have mechanical dermabrasion or ablative laser treatments (eg, CO2 resurfacing) while on isotretinoin or for 6 months afterwards. Other laser and
- light treatments may be performed with care
- Shave rather than wax
- Topical and/or oral antibiotics may be prescribed for impetigo
Other common dose-related side effects of isotretinoin
- Headache
- Myalgia (muscle aches) and arthralgia (joint aches), especially after exercise
- Acute arthritis precipitated by isotretinoin may occur 29. In reported cases, onset has been between the 2nd and 10th weeks of therapy and the knees are the most commonly affected joints. This condition is more severe that the usual aches and pains of isotretinoin. In this case, severe disability may result (e.g. difficulty walking). NSAIDs should be given and the isotretinoin stopped.
- Tiredness (lethargy and drowsiness)
- Disturbed night vision and slow adaptation to the dark. Drivers may experience increased glare from car headlights at night
- Hypertriglyceridaemia (high levels of triglyceride in the blood), usually of no clinical relevance
- Irregular or heavy menstrual periods
Rare side effects of isotretinoin
Causality of the listed side effects may not have been confirmed.
- Severe headache with blurred vision due to raised intracranial pressure (Pseudotumor Cerebri).
- If the patient develops a severe and sustained headache, visual disturbances (e.g. blurry or double vision), and/or ringing in the ears, pseudotumor cerebri should be considered. An urgent evaluation including eye exam looking for papilledema by a qualified physician (usually not the dermatologist!) is in order. Can isotretinoin be considered in patients with a history of pseudotumor cerebri from e.g. minocycline. Three patients with recalcitrant acne and a history of pseudotumor cerebri were successfully treated with isotretinoin 30. Thus, in patients whose acne truly warrants isotretinoin treatment, a history of pseudotumor cerebri (unrelated to isotretion) may not absolutely preclude its use. Baseline and subsequent ophthalmology or neurology evaluation is key.
- Mood changes and depression. Note: depression is more often related to the skin condition being treated or other health or psychosocial problems.
- Antidepressant medications may be helpful
- Corneal opacities and cataracts
- High-tone deafness
- Accelerated diffuse interstitial skeletal hyperostosis (bony change)
- Abnormal liver function tests or symptomatic hepatitis
- Diarrhoea or bleeding from the bowel
- Pancreatitis
- Allergy to isotretinoin causing liver disease and a febrile illness
- Inflammatory Bowel Disease. There has been much controversy as to whether isotretinoin predisposes to inflammatory bowel disease (IBD). One study did not show any increased risk. In fact, the risk seemed to be decreased 31. Several other recent population studies support no increased risk. There may be some association between acne itself and inflammatory bowel disease.
- Asthma has been reported exacerbated by isotretinoin 32. Indeed, isotretinoin may reduce forced expiratory flow. It is postulated that the drug’s drying effect may lead to irritability of the tracheobronchial tree.
- The development of diffuse idiopathic skeletal hyperostosis (DISH) has been associated with chronic (e.g. multi-year) administration of oral retinoids. However, no increased incidence of DISH has been found with one or a few standard courses of isotretinoin. One study showed that the bone is not demineralized with a 20 week course of isotretinoin 33. Another study however showed that mean bone density was reduced an average of 4.4% after 6 months of isotretinoin 1 mg/kg 34. In order to evaluate for DISH in a patient exposed to retinoids for a prolonged period of time (longer that the standard course of isotretinoin, e.g. > 2 years) a lateral of the cervical and lumbar spine may be obtained. Back and/or neck pain and stiffness are symptoms of DISH.
Treatment of systemic side effects
- Drink minimal alcohol
- Take paracetamol for headache and for mild aches and pains
- Seek medical attention early, if unwell
Drug interactions with isotretinoin
Care should be taken with the following medications:
- Vitamin-A (retinoic acid): side effects are cumulative and could be severe. Beta-carotene (provitamin-A) is permitted.
- Tetracyclines (including doxycycline, minocycline): these could increase the risk of headaches and blurred vision due to raised intracranial pressure.
- Warfarin: monitor INR carefully.
Treatment of Acne Scars
The term “scarring” refers to a fibrous process in which new collagen is laid down to heal a full-thickness injury. It affects 30% of those with moderate or severe acne vulgaris. It is particularly common in nodulocystic acne, acne conglobata and acne fulminans. It may also be a long-term consequence of infantile acne.
To reduce the chance of scarring, seek treatment for your acne early. Severe acne can often be cured.
Acne scarring is common but surprisingly difficult to treat. In general, treatment of acne scars is a multistep procedure. First, examination of the patient is necessary to classify the subtypes of scarring that are present. Then, the patient’s primary concerns are elicited, and the patient is offered a menu of procedures that may address the various components of the scarring process. It is important to emphasize to the patient that acne scarring can be improved but never entirely reversed.
Acne Scar Treatment Facts:
- Ideally, acne should be quiescent or controlled before treating scars
- Treatments for scars depend on the specific scar type
- Treatment also depends on your skin type.
- Embarrassment from is most often due to facial scars – effective treatment can lead to an improvement in self-image and confidence
- Scars on the chest and back will also respond to treatment
What are the features of acne scarring ?
Unfortunately, true acne scars never completely disappear, although their appearance usually improves with time. They can be disguised with make-up (cosmetic camouflage).
The following types of scar occur in acne:
- Ice-pick scars – these are deep, narrow, pitted scars
- Rolling scars – broad depressions with sloping edge
- Boxcar scars – broad depressions with with sharply defined edges
- Atrophic scars – flat, thin scars or depressed scars (anetoderma)
- Hypertrophic or keloid scars – thick lumpy scars
How skin doctors treat acne scars ?
It is crucial to communicate the fact that acne scars are seldom completely or almost completely removed, and that several procedures may be required to collectively provide the optimal correction. The patient’s willingness to incur downtime must also be clarified since some procedures, like ablative resurfacing, may require post-treatment resting at home for up to 2 weeks. Patients with active acne should not be treated for acne scarring. Many acne scarring treatments, like resurfacing, excision, and subcision, can exacerbate acne, even stimulating the production of nodulocystic lesions. Those with active acne should be reassured that the physician is not abandoning them, and remains interested in treating their acne scarring. First, however, they must undergo treatment for their acne, which should be quiescent for at least 6 months to 1 year before therapy for the scarring is begun.
Finally, darker-skinned patients with Fitzpatrick skin types IV-VI are at risk for procedure-related hyperpigmentation. Asian, Mediterranean, and African-American patients can have diffuse, widespread hyperpigmentation lasting a year or more after laser resurfacing. Excision procedures can induce a similar problem. In susceptible patients, nonablative resurfacing, fillers, and subcision may be preferred, unless the patient is otherwise a candidate for ablative resurfacing, and also indicates a willingness to endure protracted hyperpigmentation.
Non-surgical Treatment For Acne Scars
There are several non-surgical treatment options that may be appropriate for your acne scars:
Skin Camouflage/Cover-up:
For patients with active acne, acne staining, and scars – effective camouflage foundation can improve the appearance of the skin rapidly. Choose products that are non-comedogenic and non-acnegenic and have your tones matched by a skin-care expert to achieve that matte, flawless appearance.
Topical Creams: (Tretinoin):
Can improve your acne, reduce staining and improve fine scars by causing gentle exfoliation and by encouraging collagen production.
Chemical Peels (AHA peels):
Can improve overall skin tone and luster, but do little for scars, it works best if you get a series of at least six peels, having one every 1-2 weeks.
Skin Fillers/injectables:
Materials are injected into the depressed area of the scar to elevate it to the level of the normal surrounding skin. This treatment is best for scars with smooth shoulders such as thumbprint or rolling scars. Evaluating whether individual scars will respond to fillers is easily done by placing slight tension at the scar edge – if this improves the appearance of the scars, fillers will help. There are temporary and permanent fillers – examples are: Artecoll®, Zyplast®, Restylane®, and HylaForm®.
Non-ablative collagenosis:
New laser and radiofrequency devices are being evaluated for enhancing collagen formation in deeper skin layers without damaging the skin surface. It is possible that these treatments may also prove useful in acne scarring.
Surgical Treatment Options For Acne Scars
1. Microdermabrasion:
It uses very fine aluminum crystals to achieve light exfoliation of the skin. This is helpful for staining and very fine scars. It also works best if you get a series of at least 6, having one every 1-2 weeks.
2. Photorejuvenation:
Using laser or broadband visible light, 5-6 treatments that are performed every 3-4 weeks. This treatment improves mild acne scarring by causing new collagen formation.
3. Scar Revision:
Surgical removal (excision) of acne scars is especially effective for ice pick and boxcar scars. The excision may be in the form of a punch that is closed with sutures that are removed about 7 days later. The end result is replacement of a circular scar with a linear suture scar.
Another technique called subcision uses a sharp instrument to undercut the tethered bases of scars. In this case, the overlying skin is not cut so there is no need for sutures. Further improvement can then be achieved by injecting filler substances into the subcised regions.
4. Resurfacing:
a) Ablative Laser Treatments: – Laser resurfacing (CO2 laser, Erbium Yag laser): These resurfacing lasers remove the surface layer of skin and cause a zone of heat injury. The healing process allows for reformation with younger less scarred skin and deeper layer of new collagen formation.
b) Dermabrasion: – This is a mechanical procedure in which a rapidly rotating wire or brush is used to strip off the surface irregularities of skin. Felt by most experts to be the most effective primary treatment for extensive scarring, it can be used in conjunction with fillers and excision.
Treatment options according to acne scar type
Ice pick and boxcar scars
- Dermabrasion
- Laser resurfacing
- Punch grafting for deep scars
- TCA CROSS (Chemical Reconstruction Of Skin Scarring) uses precisely placed 50–100% trichloracetic acid
- Subcision®: a surgical technique in which the fibrous band under the scar is divided, allowing the skin to return to its normal position
- Larger scars can be excised (cut out) and the defect closed to form a scar in a thin line
Atrophic and rolling scars
- Soft tissue augmentation techniques such as hyaluronic acid, collagen, gelatin matrix and fat implants
- Dermabrasion
- Skin needling
- Laser resurfacing (Er:YAG and ablative fractional lasers)
Hypertrophic scars
- Potent topical steroids applied under occlusion to the scar for a few weeks
- Intralesional steroid injections into the body of the scar
- Silicone gel dressings applied for 24 hours a day continously for some months
- Skin needling
- Cryotherapy (freezing)
- Surgical revision
Unfortunately, hypertrophic or keloid scars are particularly prone to recur even after apparently successful treatment.
Treatment Modalities for Acne Scars
Among the therapeutic tools for treatment of acne scarring are resurfacing methods, fillers, and other dermal remodeling techniques. These methods can be adapted to treat specific acne scar types.
Resurfacing
Resurfacing options include:
- Ablative resurfacing with carbon dioxide or erbium: yttrium aluminum garnet (Er:YAG) laser, medium- depth to deep chemical peel, dermabrasion, or plasma
- Nonablative and partially ablative resurfacing with fractional laser, infrared laser (1,320nm neodymium:YAG (Nd:YAG), 1,450nm diode, or 1,540nm erbium:Glass)
Ablative Resurfacing
Ablative resurfacing entails removal of the epidermis and partial thickness dermis, and is considered by most as the gold standard for pitted scars and some box-car scars. While ablative resurfacing is most effective if it is deep, thereby removing as much as possible of the depressed scar, it cannot be so deep as to destroy the base of the hair follicles; such destruction could impede skin regrowth, and induce scar formation at the treated site. Carbon dioxide resurfacing is the most effective but also most operator-dependent method for deep ablative resurfacing 35. Dermabrasion is possibly even more effective, but this is another procedure that is very technique dependent. Deep phenol (Baker-Gordon) peels, also highly effective, have fallen out of favor because of the associated cardiac risk and the frequency of porcelain-white postinflammatory hypopigmentation. Definitive ablative resurfacing results in 2 weeks of patient downtime, during which period re-epithelialization occurs 36. More superficial resurfacing with the Er:YAG laser or plasma can provide recovery within 1 week, but deeper acne scars may be less improved.
Nonablative Resurfacing
Nonablative resurfacing with laser and lights warms the dermis and can provide modest improvement of acne scarring by stimulating collagen remodeling. All subtypes of acne scars can be improved by nonablative therapy. Among the lasers used for this indication are devices originally developed for other uses, such as pulsed-dye lasers, intense pulsed light devices, and Q-switched Nd:YAG lasers. However, more recently nonablative devices have been optimized to specifically target textural irregularities. For example, a series of treatments with infrared lasers can significantly improve uneven contour associated with acne scarring 37. These treatments are typically uncomfortable and may require oral and/or topical analgesics.
Similarly, fractional resurfacing is quite effective in the treatment of acne scarring. Fractional resurfacing is a minimally ablative technique that creates microscopic zones of dermal injury in a grid-like pattern 38. Because only a small proportion of the skin surface is treated at one time, and since the stratum corneum is not perforated, recovery is quick. However, a series of treatments is needed.
Fillers
During the past 5 years, many new injectable prepackaged soft-tissue augmentation materials have become available in the US. Among these are the so-called linear fillers, which permit fine correction of individual lines and depressions: human collagen, hyaluronic acid derivatives, calcium hydroxylapatite (off-label use), and silicone (off-label use).
Injectable linear fillers can enable short-, medium-, or long-term correction of acne scars. Large-particle fillers such as calcium hydroxylapatite have a longer persistence in vivo and are appropriate for larger areas of rolling scars; thicker fillers must be injected no higher than the dermal subcutaneous junction. Collagen or hyaluronic acid products can be injected directly beneath individual pitted or box-car scars, or be used to buttress areas of rolling scars. Patients should be advised that the duration of action varies, with collagen lasting 2-3 months, hyaluronic acid products, 4-6 months, and calcium hydroxylapatite, 1 year. Volumetric fillers, such as poly-L-lactic acid, may not be appropriate for acne scars, except for rolling scars. By definition, volumetric fillers are designed to correct skin and subcutaneous wasting over wide areas rather than individual fine textural abnormalities.
Injectable silicone is a controversial product gaining new acceptance as a filler for correction of acne scars, especially pitted and box-car scars 39. Now approved by the US FDA for intraocular tamponade, medical-grade silicone is used off-label for permanent correction of acne scars. To avoid delayed hypersensitivity and immune reactivity, very small aliquots of 0.01ml, known as “microdroplets”, are used, and placement is sparse. Repeat treatments with small quantities enable gradual complete correction. The inconvenience of numerous treatments, as well as the theoretical risks of adverse events are mitigated by the promise of permanence.
Excision and Subcision
Ice-pick and box-car scars may also be removed by surgical excision. This technique may entail punch excision of a given small acne scar with a punch biopsy instrument of equal or slightly greater diameter. Then one or two 5.0 or 6.0 simple interrupted sutures are used to close the resulting defect, with the attendant transformation of a round, indented scar into a flat slit-like scar. Larger linear box-car scars can be excised by elliptical excision and repaired by bilayered closure. Sufficient eversion is necessary to avoid recurrence of an indented groove.
Alternatively, after punch excision of a small scar, the defect may be filled by a punch graft. Harvested from another area, commonly the postauricular sulcus, a punch graft is pressed into the created defect and either sutured or glued in place. Punch grafting creates a secondary defect and risks poor color and texture match between donor and recipient sites. However, by filling the deadspace at the excision site, punch grafting may reduce the likelihood that scar excision and closure will fail because of excessive tension in the closure.
Subcision treats rolling scars by separating the fibrous bands securing them to the deep dermis 40. A sharp device, often an 18-gauge Nokor® needle with a spear-like tip, is inserted at an angle into the dermis at a distance of 1–2cm from the scar. The needle tip is aimed upward, tenting but not puncturing the skin, and is advanced to a point under the scar. Backward and forward rasping of the underside of the dermis beneath the scar is used to sever fibrous bands while initiating a reactive fibrosis that gradually, over several weeks, propels the depressed scar upwards. Bruising following subcision can last 1–2 weeks, but the procedure is well-tolerated with local infiltration of anesthetic. A benefit of subcision is the absence of any epidermal injury, except for minute needle insertion points.
Treatment Modalities for Color Change due to acne scars
Laser and light sources can be used to improve acne-associated color change, especially erythema. Difficult-to-correct textural abnormalities associated with acne scarring can be camouflaged by reducing the ring of redness around such scars. The redness accentuates the depth of the scar and focuses the observer’s attention, but removal of the redness can make the scar seem less deep and noticeable, even if the depth and size are objectively unchanged. Pulsed-dye laser 41, KTP laser, and intense pulsed light devices can be used for treatment of peripheral redness around acne scars. Usually, 3–4 or more treatments are required, at approximately 1 month intervals.
Brown discoloration around acne scars tends to occur in darker-skinned patients and is usually postinflammatory. As with all postinflammatory hyperpigmentation, the treatment of choice is the passage of time. Managing any residual active acne is also crucial, as further acne lesions will give rise to additional pigmentation. In some cases, a topical bleaching agent, such as 4% hydroquinone, may be appropriate adjuvant therapy.
- JAAD Feb 2014[↩]
- JAAD 20018;78;511[↩]
- zeit fur Haut 1997;72;928[↩]
- JAMA Derm 2013:149;1306[↩]
- JAAD 2016;75;318[↩]
- Int J Cancer ahead of print Feb 2018[↩]
- Back acne: How to see clearer skin. https://www.aad.org/public/diseases/acne-and-rosacea/back-acne-how-to-see-clearer-skin[↩]
- JAAD 2017;77;763[↩]
- Br J Dermatol 2017;177;567[↩]
- Effects of Subantimicrobial-Dose Doxycycline in the Treatment of Moderate Acne. Arch Dermatol. 2003 Apr;139(4):459-6 https://jamanetwork.com/journals/jamadermatology/fullarticle/479281[↩]
- Subantimicrobial-dose doxycycline in the treatment of moderate facial acne. J Drugs Dermatol. 2008 Dec;7(12):1149-52 https://www.ncbi.nlm.nih.gov/pubmed/19137768[↩]
- Dermatology 2013;226:167–171[↩]
- JAAD 2014;71:864 and Ann Intern Med. 2005;143:697-706[↩]
- J Cutan Med Surg 2002;6:541-5[↩]
- Cancer Epidemiol 2013;37:870-5[↩]
- JAAD 2008;58:60-2[↩]
- JAMA Derm Dec 2015;149;1392[↩]
- Adv Biomed Res. 2014; 3: 103[↩]
- J Clin Pharmacol. 1983 Nov-Dec;23(11-12):534-9[↩]
- BJD 2017;177;960[↩][↩]
- ADV 1995;75;377[↩]
- Dermatology Online Journal 2017;5[↩]
- Pediatrics. 2017 Oct;140;4[↩]
- BMJ 1986;293;425[↩]
- Int J Dermatol. 2008;47:398[↩]
- British Journal of Dermatology (2014) 170, 239–244[↩]
- JAAD 2017;77;159[↩]
- JAAD 2014;70:55-9[↩]
- Dermatology 1999;199;406[↩]
- JAMA Derm 2016;152;582[↩]
- JAMA Derm 2014;150;1322[↩]
- BJD 2000;142;370[↩]
- AD 1996;132;769[↩]
- AD 1999;135;961[↩]
- Batra RS, Jacob CI, Hobbs L, Arndt KA, Dover JS. A prospective survey of patient experiences after laser skin surfacing: results from 2½ years of follow-up. Arch Dermatol 139(10):1295-9 (2003 Oct).[↩]
- Alam M, Pantanowitz, Harton AM, Arndt KA, Dover JS. A prospective trial of fungal colonization after laser resurfacing of the face: correlation between culture positivity and symptoms of pruritus. Dermatol Surg 29(3):255-60 (2003 Mar).[↩]
- Bhatia AC, Dover JS, Arndt KA, Steward B, Alam M. Patient satisfaction and reported long-term therapeutic efficacy associated with 1,320nm Nd:YAG laser treatment of acne scarring and photoaging. Dermatol Surg 32(3):346-52 (2006 Mar).[↩]
- Geronemus RG. Fractional photothermolysis: current and future applications. Lasers Surg Med 38(3):169-76 (2006 Mar).[↩]
- Barnett JG, Barnet CR. Treatment of acne scars with liquid silicone injections: 30-year perspective. Dermatol Surg 31(11 Pt 2):1542-9 (2005 Nov).[↩]
- Alam M, Omura N, Kaminer MS. Subcision for acne scarring: technique and outcomes in 40 patients. Dermatol Surg 31(3):310-7 (2005 Mar).[↩]
- Alster TS, McMeekin TO. Improvement of facial acne scars by the 585nm flashlamp-pumped pulsed-dye laser. J Am Acad Dermatol 35(1):79-81 (1996 Jul).[↩]





{kind=link}