Contents
- Bartonellosis
- Bartonellosis cause
- Cat scratch disease (Bartonella henselae infection)
- How cats and people become infected with bartonella henselae?
- My cat is completely healthy. How can it carry an infection?
- Should I get my pet tested and treated for Bartonella, just to be safe?
- My daughter got scratched by the neighbor’s kitten and now my husband is worried about “cat scratch disease.” How worried should we be?
- I have a medical condition that affects my immune system. Should I give my cat away?
- Trench fever (Bartonella quintana infection)
- Carrión’s disease (Bartonella bacilliformis infection)
- I have been suffering from fatigue and memory problems for the past year. Should I be tested for Bartonella infection?
- I heard that there are newer testing methods from laboratories that specialize in Bartonella testing. Are these new tests accurate?
- I got a tick bite. My friend said I should get tested for Lyme disease and Bartonella. Is that true?
- Cat scratch disease (Bartonella henselae infection)
- Bartonella Life Cycle and Infection Strategy
- Bartonellosis prevention
- Bartonellosis signs and symptoms
- Bartonellosis diagnosis
- Bartonellosis Differential Diagnosis
- Bartonellosis treatment
- Bartonellosis prognosis
- Bartonellosis cause
Bartonellosis
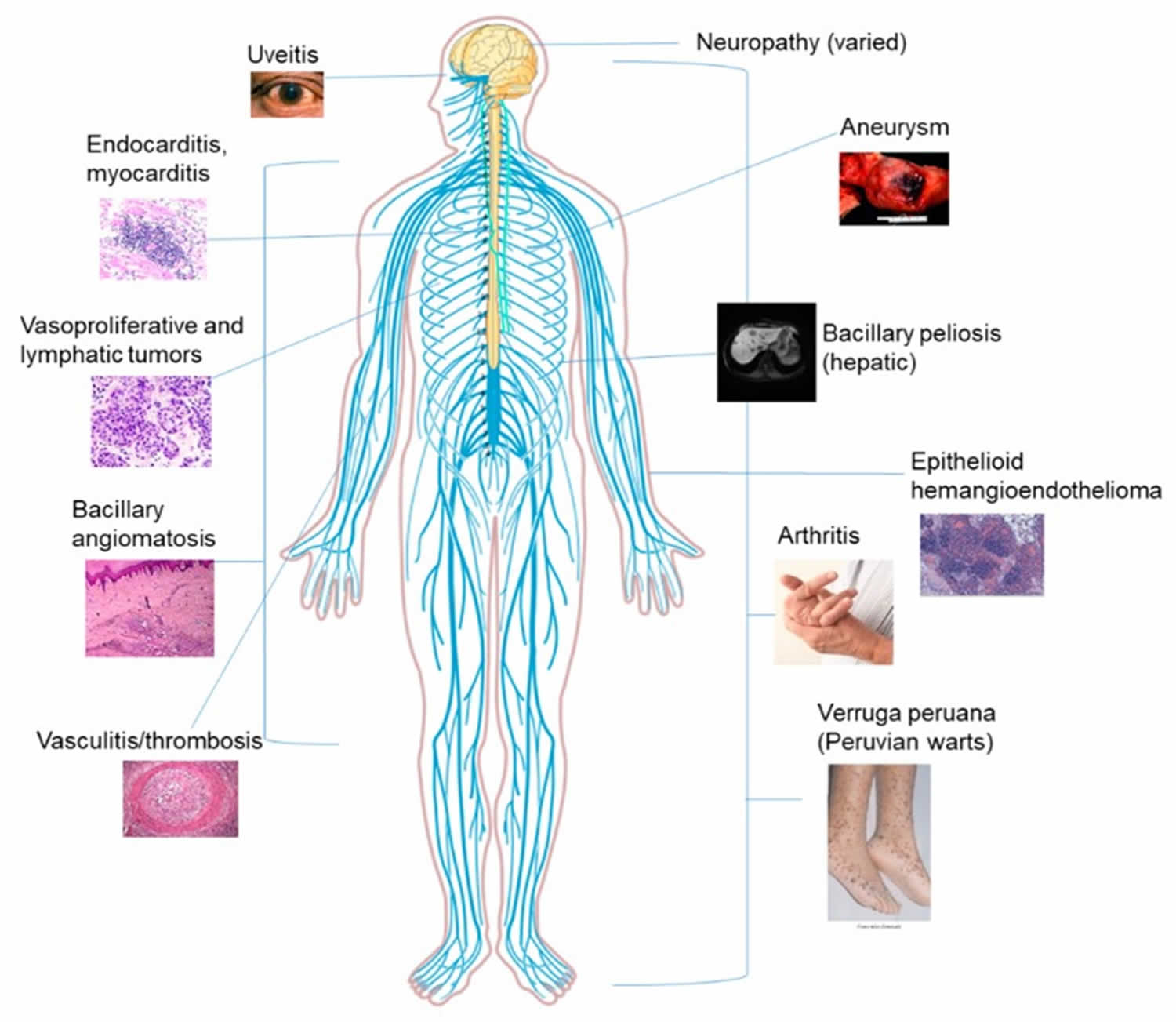
Bartonellosis is a group of infectious diseases in both animals and humans caused by Bartonella bacteria with Bartonella henselae (cat scratch disease), Bartonella bacilliformis (Carrion’s disease), and Bartonella quintana (trench fever) being the most common human pathogens 1, 2, 3, 4, 5. Bartonellosis diseases can be transmitted to humans through various vectors, including fleas, lice, and sandflies, and from animals like cats 6, 7, 1. Bartonella henselae (cat scratch disease) is transmitted by the scratch or bite of domestic or feral cats. Cats can have fleas that carry the Bartonella henselae bacteria. Bartonella quintana (trench fever) is transmitted by the human body louse. Bartonella bacilliformis (Carrion’s disease) is transmitted by bites from infected sand flies. Bartonellosis common signs and symptoms include cat scratch disease, Carrion’s disease, and trench fever. Chronic Bartonella infection can be associated with relapsing low-grade fever. Chronic eye problems include blurred vision, photophobia, and eye irritation 2. Bartonella commonly infects bone marrow with resulting bone pain, most commonly the shin bone 2. Another classic Bartonella symptom is a pain in the soles of feet upon waking in the morning. This is associated with trauma to blood vessels in the soles of the feet with walking. Anemia can occur from Bartonella scavenging nutrients from red blood cells. Neurological symptoms include poor balance, decreased cognition, memory impairment, insomnia, and restlessness 2. Another presentation of Bartonella infection includes negative culture endocarditis or Bartonella endocarditis. Even though several species have been implicated in causing endocarditis, Bartonella henselae and Bartonella quintana account for about 95% of endocarditis caused by Bartonella 8. Severe, progressive, disseminated Bartonella disease may occur in immunocompromised patients, especially those with HIV infection and organ transplants. Without therapy, the infection spreads systemically and can involve virtually any organ, and the outcome is sometimes fatal.
The incidence of cat-scratch disease was reported to be 6.4 cases per 100,000 population in adults and 9.4 cases per 100,000 population in children aged 5-9 years globally. The highest incidence is reported in the southeastern United States with a peak in January, late summer, and fall 9. Epidemic and sporadic outbreaks of trench fever have been reported since the early 20 century in several countries across the globe with the largest epidemics reported during world war 1 and world war 2. The homeless population is more frequently exposed to the pathogen and has the highest risk of contracting trench fever 10. Infections caused by Bartonella bacilliformis are endemic to Peru, Columbia, and Ecuador while sporadic cases have been reported in Chile, Guatemala, and Bolivia 11.
Bartonella bacteria are fastidious Gram-negative intracellular bacilli, well adapted to a variety of animal reservoirs, particularly mammals 2, 3. Bartonella bacteria are capable of infecting and surviving inside red blood cells (erythrocytes) 2, 3. After the Bartonella bacteria entered into the red blood cells, it prevents the cell from self-destructing and also creates a vacuole a protective cyst around itself, resulting in a prolonged and recurrent infection 2, 12. Bartonella bacteria can also infect endothelial cells 13.
An endotoxin called lipid A which is commonly found in the outer membrane of Gram-negative bacteria is the primary virulence factor for Bartonella 2. The ability of Bartonella bacteria to invade red blood cells (erythrocytes) and endothelial cells plays a major role in the pathogenesis of the disease process. The Bartonella bacteria alter the immune system in such a way that makes the host susceptible to infections by other bacterial pathogens. After this acute phase, the Bartonella bacteria invades the endovascular, lymphatic, and other organ systems of the body contributing to multiple presentations of the disease.
The main route of transmission of Bartonella bacteria is from infected humans or animals to new hosts through blood-sucking arthropod vectors 2, 3. Transmission through animal scratches has been reported but it is not certain, since fleas are needed for transmission among cats 1, 14. Recent studies reinforce the hypothesis that Bartonella bacteria can be transmitted through blood transfusion, which is a concern for people all over the world since currently there is no preventive action against this possibility 7, 15, 16, 17. In addition, asymptomatic infection by Bartonella bacteria has already been detected in blood donors 7, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26.
Figure 1. Bartonellosis in humans
Bartonellosis diagnosis
- Cat scratch disease (Bartonella henselae) may be diagnosed presumptively in patients with typical signs and symptoms and a compatible exposure history. Serology can confirm the diagnosis, although cross-reactivity may limit interpretation in some circumstances. In general, lymph node aspiration is not recommended except to relieve severe pain and swelling or in cases where the diagnosis is unclear.
- Bartonella test
- Bartonella henselae DNA may be detected by polymerase chain reaction (PCR) or culture of lymph node aspirates or blood, though sensitivity of these methods is not optimal for blood samples.
- Since Bartonella henselae is a fastidious, slow-growing bacterium, cultures should be held for a minimum of 21 days.
- Trench fever can be diagnosed by isolation of Bartonella quintana from blood cultured on blood or chocolate agar under 5% CO2. Microcolonies can be seen after 21 days of incubation at 37°C.
- Trench fever can also be diagnosed by serology.
- Carrión’s disease is typically diagnosed via blood culture or direct observation of the bacilli in peripheral blood smears during the acute phase of infection (Oroya fever).
- Endocarditis due to Bartonella species can be diagnosed by serology and by polymerase chain reaction (PCR) or culture of excised heart valve tissue.
The culture of Bartonella bacteria gives a definitive diagnosis, but it is a very time-consuming and expensive process with incubation periods as long as 21 days 2. Bartonella bacteria are very slow-growing, fastidious, and primary isolation is difficult, with the detection of colonies only after 1 to 4 weeks of incubation on blood agar plates 2. As Bartonella bacteria are difficult to culture, culture is not routinely recommended 2. Serology is the best initial test and can be performed by indirect fluorescent assay (IFA) or enzyme-linked immunosorbent assay (ELISA) 2.
Serological testing such as indirect fluorescence assay (IFA) for Bartonella henselae antibodies was the first microbiological test available but has a variable positive predictive value 2. It is an indirect diagnostic method that can be negative in the early stage of the disease. In some studies, the positive predictive value of the indirect immunofluorescence assay (IFA) for Bartonella henselae was reported to be high (91.4%) 2. Conversely, some studies found a lack of sensitivity of the serological test among patients with cat scratch disease. While there is variability in multiple studies of Bartonella henselae IgG and IgM indirect fluorescent antibody and ELISA serology, typical sensitivity values are approximately 50% to 80%, whereas specificity is 90% to 100% 27. Sensitivity increases when there is a higher clinical index of suspicion for cat scratch disease. An IgM titer of 1:16 or higher shows acute disease, with a 3-month duration of detection in 50% of patients 2. An IgG titer higher than 1:256 is considered evidence of current or past Bartonella infection 2. Unlike culture and PCR (polymerase chain reaction) of blood, serology does not rely on Bartonella being present in the blood 2. Serological testing can be used to evaluate response to therapy.
Histopathological examination of the tissue infected by Bartonella species usually shows neutrophils, lymphocytes, and debris scattered throughout the lesions 2. Warthin-Starry silver staining will show small dark staining bacteria and electron microscopic findings include pleomorphic bacilli with a trilaminar wall 2. Histopathological examination for Bartonella bacilliformis is performed using Giemsa stain, and it shows cytoplasmic inclusions known as Rocha-Lima inclusions 28.
Advanced diagnostic techniques such as PCR (polymerase chain reaction) on lymph nodes or other material have been applied to the detection of Bartonella 2. PCR provides the advantages of high specificity and rapid identification, however lacking in sensitivity, ranging from 43% to 76% 2. The sensitivity of PCR with samples of lymph node tissue or aspirates is 30-60% for cat scratch disease. A polymerase chain reaction (PCR) can detect different Bartonella species; specificity is high, but the sensitivity is lower than with serology 2.
Bartonellosis treatment depends on the underlying Bartonella infection. Trench fever, Carrión’s disease, and endocarditis due to Bartonella spp. are serious infections that require antibiotic treatment. Doctors should consult with an expert in infectious diseases regarding treatment options. Management of cat scratch disease depends on the clinical presentation of the disease. Because cat-scratch disease is not serious and self-limiting condition, with most cases of regional lymphadenopathy resolving spontaneously in two to four months, medical treatment may not be needed 29. However, studies have shown that the use of a single antibiotic regimen will reduce the duration of cat scratch disease symptoms significantly. The antimicrobial agents commonly used for cat scratch disease are azithromycin, ciprofloxacin, gentamicin, trimethoprim-sulfamethoxazole, and rifampin 2. For patients with extensive lymphadenopathy, oral azithromycin at 500 mg on the first day and 250 mg on days 2 to 5 2. For retinitis, oral Doxycycline 100 mg twice daily for 4 to 6 weeks and oral rifampin 300 mg twice daily for 4 to 6 weeks 2.
Trench fever or chronic bacteremia with Bartonella quintana can be treated with oral Doxycycline at 200 mg once daily for 4 weeks and intravenous gentamicin 3 mg/kg for 2 weeks 30.
Bacillary angiomatosis and Peliosis Hepatis treated with oral erythromycin 500 mg four times daily for 3 to 4 months 2.
Documented Bartonella culture-positive endocarditis should be treated with oral Doxycycline 100 mg for 6 weeks and intravenous gentamicin at 3 mg/kg/day for 14 days 2.
Recommended treatment for neuroretinitis and for central nervous system (brain and spinal cord) involvement is a combination of oral doxycycline 100 mg twice daily and rifampin 300mg twice daily 31. There are no controlled clinical trials comparing a nontreatment group with those given antibiotics. However, retrospective case series consistently associated antibiotics with hastened visual recovery and improved visual outcomes. Corticosteroid use in cat scratch disease with eye involvement has had mixed results 2.
The management of Oroya fever (Bartonella bacilliformis infection) includes the use of ciprofloxacin as the primary choice with chloramphenicol, ceftriaxone being alternative choice that are very effective. Verruga peruana (Peruvian wart) is managed with azithromycin primarily with rifampin, ciprofloxacin, and chloramphenicol being the preferred alternatives 2.
Bartonellosis cause
Bartonella bacteria are fastidious Gram-negative intracellular bacilli, well adapted to a variety of animal reservoirs, particularly mammals 2, 3. Bartonella bacteria are capable of infecting and surviving inside red blood cells (erythrocytes) 2, 3. The intraerythrocytic phase allows for Bartonella bacteria protection, resulting in a prolonged and recurrent infection 12. Bartonella bacteria can also infect endothelial cells 13.
Bartonella henselae (cat scratch disease) is transmitted by the scratch or bite of domestic or feral cats. Cats can have fleas that carry the Bartonella henselae bacteria. Bartonella quintana (trench fever) is transmitted by the human body louse. Bartonella bacilliformis (Carrion’s disease) is transmitted by bites from infected sand flies.
Once inside the body, Bartonella targets CD34+ cells which are specialized white blood cells that act as precursors for endothelial cells which are cells that line blood vessels and other tissues 2. After the Bartonella bacteria entered into the red blood cells, it prevents the cell from self-destructing and also creates a vacuole a protective cyst around itself, resulting in a prolonged and recurrent infection 2, 12. Bartonella bacteria can also infect endothelial cells 13.
An endotoxin called lipid A which is commonly found in the outer membrane of Gram-negative bacteria is the primary virulence factor for Bartonella 2. The ability of Bartonella bacteria to invade red blood cells (erythrocytes) and endothelial cells plays a major role in the pathogenesis of the disease process. The Bartonella bacteria alter the immune system in such a way that makes the host susceptible to infections by other bacterial pathogens. After this acute phase, the Bartonella bacteria invades the endovascular, lymphatic, and other organ systems of the body contributing to multiple presentations of the disease.
Cat scratch disease (Bartonella henselae infection)
People become infected with Bartonella henselae bacteria from the scratch or bite of domestic or feral cats, particularly kittens 32. Cats (especially kittens) can have fleas that carry Bartonella henselae bacteria 33, 34, 35. Cats can have a blood infection from the Bartonella henselae bacteria without symptoms for months. The Bartonella henselae bacteria can be transmitted from a cat to a person during a scratch that is contaminated with flea feces (poop). Infected cats that lick a person’s open wound or bite can also spread the Bartonella henselae bacteria. Some evidence suggests that the Bartonella henselae bacteria may also spread directly to people by the bite of infected cat fleas, but this has not been proven. Stray cats are more likely than pets to be infected with Bartonella henselae.
Besides cats, other pets have also been described as Bartonella henselae reservoirs include guinea pigs, rabbits, and dogs 36.
How cats and people become infected with bartonella henselae?
Cats can get infected with Bartonella henselae from flea bites and flea dirt (droppings) getting into their wounds. By scratching and biting at the fleas, cats pick up the infected flea dirt under their nails and between their teeth. Cats can also become infected by fighting with other cats that are infected. The germ spreads to people when infected cats bite or scratch a person hard enough to break their skin. The germ can also spread when infected cats lick at wounds or scabs that you may have.
Cat scratch disease is caused by a bacterium called Bartonella henselae. About 40% of cats carry Bartonella henselae at some time in their lives, although most cats with this infection show NO signs of illness. Kittens younger than 1 year are more likely to have Bartonella henselae infection and to spread the germ to people. Kittens are also more likely to scratch and bite while they play and learn how to attack prey.
My cat is completely healthy. How can it carry an infection?
Cats most commonly become infected with Bartonella henselae bacteria that cause cat scratch disease through flea bites. They can less commonly become infected during fights with other infected cats or through feline blood transfusions. While some cats become ill, most simply have the Bartonella henselae bacteria in their blood without getting sick. Some studies have found the Bartonella bacteria in the blood of up to 1 in 3 healthy cats, particularly kittens.
Should I get my pet tested and treated for Bartonella, just to be safe?
Testing and treatment is not recommended unless your pet is sick. For cats that do become sick, the illness usually consists of fever for 2 to 3 days. Symptoms requiring veterinary care include fever lasting more than 3 days, vomiting, lethargy, red eyes, swollen lymph nodes, or decreased appetite. Treating pets for Bartonella henselae with antibiotics can take a long time and it’s considered safer and more practical to let the pet handle the infection naturally. For cats that do become sick, the illness usually consists of fever for 2-3 days, with the cat recovering on its own.
My daughter got scratched by the neighbor’s kitten and now my husband is worried about “cat scratch disease.” How worried should we be?
Most cat scratches do not result in cat scratch disease, and short of cleaning the wound with soap and water, there is no particular action to take. If your child develops a fever; enlarged, tender lymph nodes that develop 1 to 3 weeks after being scratched; or a pustule at the scratch site, please take her to your doctor. Treatment with antibiotics is usually not necessary but may help reduce lymph node swelling.
I have a medical condition that affects my immune system. Should I give my cat away?
If you’re human immunodeficiency virus (HIV)-positive, are being treated for cancer, or have any other condition that might disrupt your immune system, you can keep your cat. You do not need to test or treat a healthy cat for Bartonella. Just keep the following points in mind:
- Keep your cat indoors.
- Avoid rough play with cats and situations in which scratches are likely. Declawing is not recommended.
- Promptly wash any cat scratches or bites with soap and water.
- Avoid contact with fleas.
- Treat the cat with a flea control product recommended by your veterinarian.
- It’s not necessary to test or treat a healthy cat for Bartonella.
- If you are getting a cat, make sure it’s at least a year old, in good health, and free of fleas. Avoid stray cats and cats with flea infestations.
Trench fever (Bartonella quintana infection)
Bartonella quintana infection signs and symptoms may include:
- Fever (may occur once or repeatedly).
- Bone pain (mainly in the shins, neck, and back).
- Skin lesions called “bacillary angiomatosis”. Bacillary angiomatosis is an abnormal or excessive growth of blood vessels disorder caused by the Bartonella bacteria, primarily Bartonella henselae and Bartonella quintana. Bacillary angiomatosis can present as vascular lesions in the skin, under the skin, in bone, or in other organs. Bacillary angiomatosis typically affects people with weakened immune systems such as those with advanced human immunodeficiency virus (HIV) infection, presenting with skin lesions that can resemble Kaposi’s sarcoma or pyogenic granuloma. While most commonly seen in the skin, bacillary angiomatosis can also involve internal organs like the liver, spleen, and lymph nodes.
As with many Bartonella species, Bartonella quintana bacteria can sometimes cause infection of the heart valves (endocarditis). In many cases, blood cultures might be negative (culture-negative endocarditis), which can make the diagnosis more challenging.
Carrión’s disease (Bartonella bacilliformis infection)
Carrión’s disease previously known as as South American bartonellosis, is transmitted by bites from sand flies genus Lutzomyia that are infected with the Bartonella bacilliformis bacteria. Carrión’s disease has limited geographic distribution to some regions of South America; transmission occurs in the Andes Mountains at 3,000 to 10,000 ft in elevation in western South America, including Peru, Colombia, and Ecuador. Most cases are reported in Peru. Much is still unknown about which animals may be a part of the natural cycle of this disease.
Bartonella bacilliformis infection or Carrion’s disease has 2 distinct phases, Oroya fever and Veruga perruana (“Peruvian warts”):
- Oroya fever: During this phase, patients may present with fever, headache, muscle aches, abdominal pain, and severe anemia. Complications may occur in up to 70 percent of patients with Oroya fever, including secondary infections and cardiopulmonary complications such as heart failure, pericardial effusion, pulmonary edema, and cardiogenic shock.
- Verruga peruana also called Peruvian warts: During this later phase, lesions appear under the skin as nodular growths, then emerge from the skin as red-to-purple vascular lesions that are prone to ulceration and bleeding.
A few cases of Oroya fever and verruga peruana (Peruvian warts) have been reported in travelers who returned from the Andean highlands in South America, but the risk is low. In 2007, a newly recognized species of Bartonella (Bartonella rochalimae) was identified in an ill traveler returning from Peru. Much is still unknown regarding the existence of other competent arthropod vectors and the identification of a natural, nonhuman, vertebrate reservoir.
The classical course of infections with Bartonella bacilliformis is known as Carrion’s disease and consists of Oroya fever as the acute phase with hemolytic anemia and a subsequent chronic phase hallmarked by multiple vasoproliferative lesions on the skin (verruga peruana for “Peruvian wart”) 37. The devastating hemolytic anemia during Oroya fever is a critical difference between the pathologies of Bartonella bacilliformis and the other bartonellae, since severe morbidity and hemolytic anemia are usually not observed during infections with the modern species. A recent compilation of various studies concluded that the mortality during Oroya fever ranges from close to zero in the case of hospitalized patients receiving antibiotic treatment to up to 88% in untreated cases 38. Approximately 70% of patients suffering from Oroya fever develop complications of the disease, of which approximately half are of an infectious and half of a noninfectious nature. Noninfectious complications such as fever, anorexia or an altered mental status have been suggested to be primarily a consequence of systemic infection 39. The impairment of immunity during Oroya fever favors secondary infections that contribute prominently to morbidity and mortality by provoking septicemia, most often with Salmonella 39. During Carrion’s disease, the abrogation of hemolytic anemia is characteristically followed by massive pathological angiogenesis as hallmark of the chronic tissue phase called verruga peruana. It is crucial to note that the nodules observed over the course of this phase are “clinically and histologically indistinguishable” from the tumors arising during bacillary angiomatosis with the modern Bartonella species 40. Like these, the pathological angiogenesis during the verruga peruana phase usually occurs in the skin, but atypical cases involving other organs such as the spleen 41 have been reported. In striking contrast to the acute phase of Carrion’s disease, verruga peruana is associated with only negligible mortality 38. Notably, the name of this biphasic infection and the discovery of the link between its two phases derive from Daniel Alcides Carrion, who died from Oroya fever after he inoculated himself with blood from a verruga peruana nodule 42. However, it is known today that this classical course of Carrion’s disease is not the only possible outcome of a B. bacilliformis infection, since natives in the areas of endemicity exhibit a significant baseline of asymptomatic bacteremia (see above) and suffer from Oroya fever relatively rarely 43 but frequently develop verruga peruana without prior hemolytic anemia 44.
I have been suffering from fatigue and memory problems for the past year. Should I be tested for Bartonella infection?
There are many reasons why people might experience fatigue and memory problems. It’s unlikely that Bartonella is the cause of these issues. Work with your primary care physician to determine if a specialist is needed.
I heard that there are newer testing methods from laboratories that specialize in Bartonella testing. Are these new tests accurate?
Although Centers for Disease Control and Prevention (CDC) typically recommends FDA-cleared tests, there are not currently any Bartonella tests on the market that meet this standard. There are some things that you should keep in mind when evaluating the accuracy of a lab test.
- First, any laboratory that performs Bartonella serologic testing should provide you with information regarding the accuracy of the test.
- Second, be aware that while some labs may report that their tests find 100% of infected patients, this is unrealistic—the potential for false positives (and false negatives) almost always exists.
- Finally, it is important for all abnormal test results to be interpreted with your doctor in the context of your medical history.
I got a tick bite. My friend said I should get tested for Lyme disease and Bartonella. Is that true?
The Centers for Disease Control and Prevention (CDC) don’t recommend it. To date, no study in the United States has shown that Bartonella can be transmitted to humans by ticks. Transmission studies with ticks have only used mice and artificial feeding systems. A single study showed that one species of tick in Europe could transmit a specific species of Bartonella to mice in a laboratory setting.
Other studies have identified Bartonella in ticks, probably from ticks feeding on animals that carry Bartonella. This doesn’t mean that the bacteria can be transmitted from the tick to a person or that the bacteria can survive in the tick for any length of time.
Unfortunately there is a great deal of misinformation regarding multiple tickborne infections (called coinfections) on the internet. The possibility of having several tickborne infections at once or having pathogens such as Bartonella that have not been shown to be tickborne, is extremely unlikely.
Bartonella Life Cycle and Infection Strategy
The infection cycle of Bartonella is initiated with the inoculation of a mammal reservoir host, characteristically following transmission via bloodsucking arthropods. Upon inoculation, the bartonellae are not capable of directly colonizing erythrocytes. Instead, a preceding period of residence in a primary niche is apparently necessary to make the bacteria and/or the host competent for this step. From the primary niche, the bartonellae are seeded into the bloodstream and infect erythrocytes in a sequence of steps ranging from adhesion to eventually invasion and intracellular persistence that enables continuous vector transmission (Figure 2).
During the whole course of infection, the lack of an effective host immune response and a globally moderated inflammatory profile are highly beneficial for Bartonella and are promoted by the pathogen via both passive immune evasion and active immunomodulation. The infection cycle of Bartonella has been extensively studied and reviewed elsewhere 45. Importantly, although it is obvious that certain differences from species to species do exist and probably arose due to specific paths of pathogen-host adaptation, it is generally believed that the overall concept of this infection cycle is conserved among members of the genus Bartonella.
Figure 2. Bartonella life cycle and infection strategy
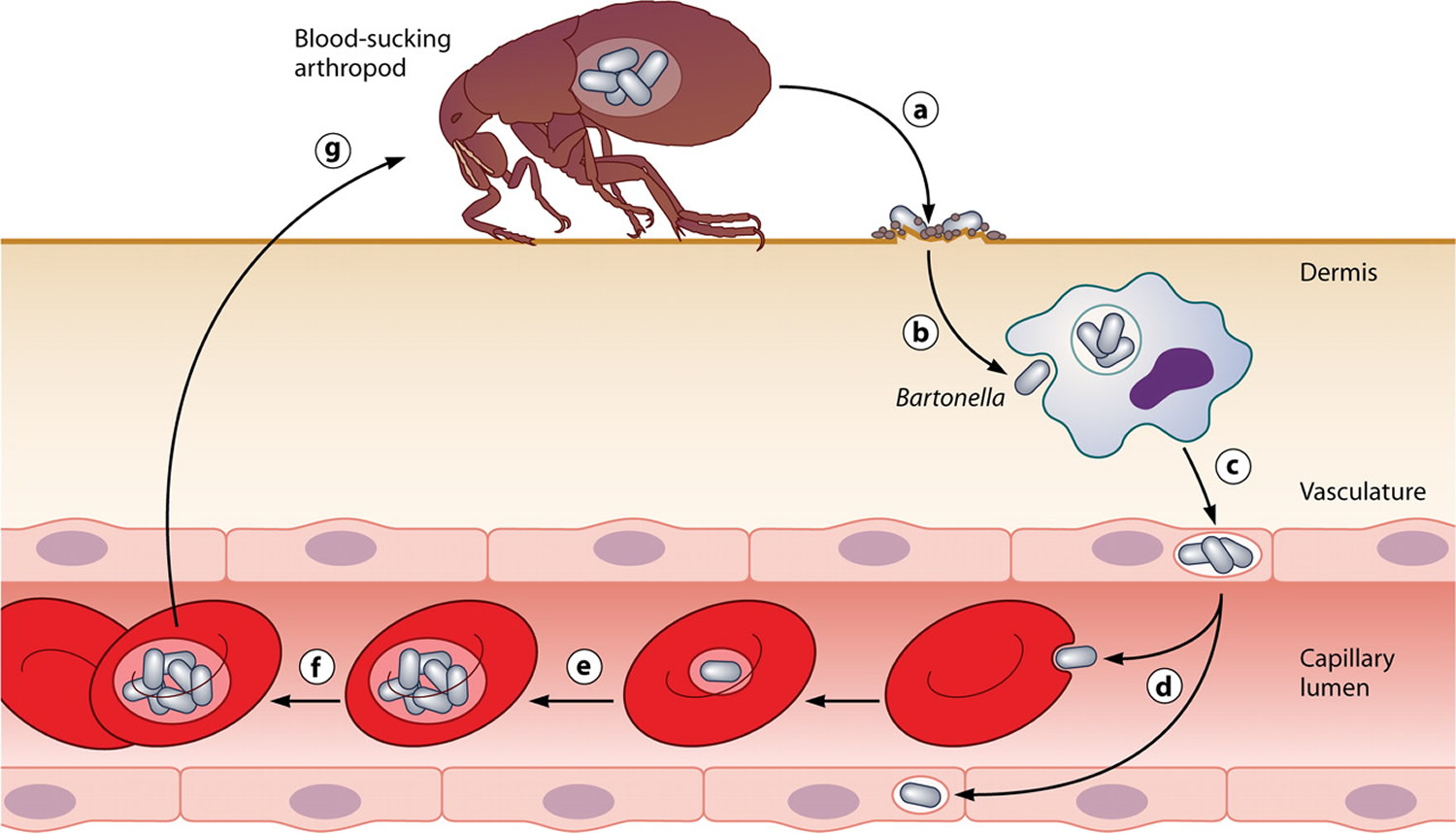
Footnotes: Common infection strategy of the bartonellae. The drawing illustrates the general concept of reservoir host infections with Bartonella. Following transmission by an arthropod vector (a), the bartonellae colonize the primary niche, which probably involves entry into migratory cells (b) and transport to the vascular endothelium (c), where the bacteria persist intracellularly. From the primary niche, the bacteria are seeded into the bloodstream (d), where they invade erythrocytes and reinfect the primary niche. After limited replication inside the red blood cell (e), they persist in the intraerythrocytic niche (f) competent for transmission by a bloodsucking arthropod (g).
Bartonellosis prevention
Cat scratch disease (Bartonella henselae) prevention
- Avoid rough play with cats, particularly strays and kittens, to prevent scratches and bites. This is especially important for people with weakened immune systems. Wash your hands thoroughly with soap and water after playing with your cat. Wash any bites or scratches thoroughly.
- Don’t allow a cat to lick your skin, eyes, mouth, or open wounds or scratches.
- Treat cats for fleas using fipronil and other spot-on treatments. Check with your veterinarian. Permethrin should not be used on cats.
- Use a flea collar or similar topical preventive on dogs (fipronil, methoprene, imidocloprid, or permethrin), especially if you have both cats and dogs in your household.
- Keep cats indoors and away from stray cats.
- Immunocompromised individuals should avoid owning cats less than one year of age.
- Wash cat bites and scratches well with soap and running water. Do not allow cats to lick your wounds. Contact your doctor if you develop any symptoms of cat-scratch disease or infection.
Trench fever (Bartonella quintana) prevention
- Avoid exposure to human body lice. Body lice are typically associated with crowded living conditions and limited access to bathing and clean clothes.
- Access to regular showers and laundry services is critical to prevent Bartonella quintana infection among people living in congregate shelters or who lack access to housing.
- Do not share clothing, beds, bedding, and towels used by a person who might have body lice.
Body lice are spread most commonly by direct contact with an infested person or an infested person’s clothing or bedding. Body lice usually infest persons who do not launder and change their clothes regularly.
The following are steps that can be taken to help prevent and control the spread of body lice:
- Bathe regularly and change into properly laundered clothes at least once a week; launder infested clothing at least once a week.
- Machine wash and dry infested clothing and bedding using the hot water (at least 130°F or 55 degrees Celsius) laundry cycle and dry on high heat to kill lice and their eggs. Clothing and items that are not washable can be dry-cleaned OR sealed in a plastic bag and stored for 2 weeks.
- Do not share clothing, beds, bedding, and towels used by an infested person.
- Fumigation or dusting with chemical insecticides sometimes is necessary to control and prevent the spread of body lice for certain diseases.
Carrión’s disease (Bartonella bacilliformis) prevention
Use insect repellents and protective clothing to avoid sand fly bites in areas where Carrión’s disease (Bartonella bacilliformis) is common (South America). If possible, limit your outdoor activities at dawn and dusk, when sand flies are most active.
Find the insect repellent that is Right for You here: https://www.epa.gov/insect-repellents/find-repellent-right-you
For the safe and effective use of pesticide products, always read the product label before using the product.
Bartonellosis signs and symptoms
Bartonella bacteria are responsible for a broad spctrum of clinical diseases, from asymptomatic bacteremia to potentially fatal presentations. Among the 16 species of Bartonella that are pathogenic to humans, 3 are responsible for the majority of clinical symptoms: Bartonella bacilliformis, Bartonella quintana, and Bartonella henselae 13, 47. Bartonellosis common signs and symptoms in humans include cat scratch disease (Bartonella henselae infection), Carrion’s disease (Bartonella bacilliformis infection), and trench fever (Bartonella quintana infection). Another presentation of Bartonella infection includes negative culture endocarditis or Bartonella endocarditis. Even though several species have been implicated in causing endocarditis, Bartonella henselae and Bartonella quintana account for about 95% of endocarditis caused by Bartonella 8.
The severity of Bartonella infection is often correlated with the immune status of the patient, although other factors such as the species infecting the host, virulence factors, and bacterial load should be considered as components in disease severity 4. Severe, progressive, disseminated disease may occur in immunocompromised patients, especially those with HIV infection and organ transplants 2. Without therapy, the infection spreads systemically and can involve virtually any organ, and the outcome is sometimes fatal 2.
Peliosis hepatis is defined as a vascular proliferation of sinusoidal hepatic capillaries resulting in blood-filled spaces in the liver. Peliosis hepatis was first described in patients with tuberculosis and advanced cancers and correlated with the use of drugs such as anabolic steroids. Bartonella henselae is now recognized as an infectious cause of peliosis hepatis in HIV-infected patients. Peliosis hepatis has also been reported in organ transplant recipients. Peliosis hepatis can occur simultaneously with peliosis of the spleen, and bacillary angiomatosis of the skin, in HIV-infected patients 2.
Chronic Bartonella infection can be associated with relapsing low-grade fever. Chronic eye problems include blurred vision, photophobia, and eye irritation 2. Bartonella commonly infects bone marrow with resulting bone pain, most commonly the shin bone 2. Another classic Bartonella symptom is a pain in the soles of feet upon waking in the morning. This is associated with trauma to blood vessels in the soles of the feet with walking. Anemia can occur from Bartonella scavenging nutrients from red blood cells. Neurological symptoms include poor balance, decreased cognition, memory impairment, insomnia, and restlessness 2.
Cat scratch disease (Bartonella henselae infection) signs and symptoms
Cat scratch disease or Bartonella henselae infection occurs most often in children under the age of 15 49. Cat-scratch disease is spread through contact with an infected cat (a bite or scratch) or exposure to cat fleas 33, 34, 35. It also can be spread through contact with cat saliva on broken skin or mucosal surfaces like those in the nose, mouth, and eyes. Though more common in the southeast, cat scratch disease occurs throughout the United States. In the United States, most cases of cat scratch disease occur in the fall and winter.
Cat scratch disease signs and symptoms may include:
- Low-grade fever
- Swollen, painful lymph nodes (lymphadenopathy) that develop 1 to 3 weeks after exposure to a cat
- A papule (small raised, tender bump under your skin) or pustule (a small blister on the skin containing pus) at the site of the scratch. The bumps can look like a rash or more like nodules, and they’re usually near your wound.
- Muscle, bone or joint aches.
- Headache
- Overall discomfort (malaise)
- Fatigue.
About three to 14 days after the skin is broken, a mild infection can occur at the site of the scratch or bite. A small red raised spot develops at the site of contact with an infected cat’s saliva. This changes into a fluid-filled blister or pus that later forms a crusty sore. This usually heals without scarring in several days or months. It is often mistaken for an insect bite. Most are found on the hands, arms, face or neck as people often hold kittens close to their chest and face.
A person with cat scratch disease may also have a fever, headache, poor appetite, and exhaustion. Later, the person’s lymph nodes closest to the original scratch or bite can become swollen, tender, or painful.
The nearest lymph glands then become swollen and tender, most often those on the head, neck and armpit. This is known as regional lymphadenopathy. The lymph glands may swell to 10-12 cm in the first two weeks of the disease. On questioning, patients often recall being licked, bitten or scratched by a cat in the previous one to eight weeks.
About 50% of patients will experience additional signs and symptoms including:
- fever
- malaise/fatigue
- headache
- nausea and vomiting
- sore throat
- rash
- stomach pains
- conjunctivitis
Less common problems occur in about 10% of patients. These include:
- Parinaud’s oculoglandular syndrome, characterized by an inflamed lump in the eye and swollen lymph glands in front of the nearby ear
- Bacillary angiomatosis (infection of the blood vessels)
- Bacillary hepatitis and splenitis (infection of the liver and spleen)
- Erythema nodosum (red lumps on the shins)
- Sepsis (infection disseminated through the blood stream)
- Encephalopathy (brain infection)
- Bacterial endocarditis (heart valve infection). As with many Bartonella species, Bartonella henselae can sometimes cause infection of the heart valves, called endocarditis. In many cases, blood cultures might be negative (culture-negative endocarditis), which can make the diagnosis more challenging.
Rarely, Bartonella henselae infections of the eye, liver, spleen, brain, bones, or heart valves (endocarditis) can occur. Some of these infections occur primarily in people with weakened immune systems, such as those with advanced human immunodeficiency virus (HIV) infection. The abrupt symptoms of fever, seizures and coma can be frightening. With hospitalization and high doses of antibiotics most patients recover completely.
Figure 3. Cat scratch disease papulopustular lesions

Figure 4. Cat scratch disease neck abscess that developed over 3 weeks on a 2.5-year-old boy who acquired cat scratch disease 10 months before

Figure 5. Bartonella henselae infection with skin annular granuloma

Footnotes: Annular granuloma presented by a 52-year-old woman. Bartonella henselae DNA was amplified in a fragment of the mediastinal lymph node and in the patient’s blood.
[Source 3 ]Figure 6. Bartonella henselae with sclerosing panniculitis

Footnotes: Sclerosing panniculitis with recurrent anemia. Sclerosing panniculitis in the right leg of a 32-year-old woman with a history of recurrent anemia of unknown origin. The patient subsequently tested for positive Bartonella henselae DNA in blood samples.
[Source 3 ]Figure 7. Bartonella henselae with cutaneous vasculitis on the leg

Footnotes: Cutaneous vasculitis on the leg of a 42-year-old man with a history of cat scratches and fever, with a diagnosis of Bartonella henselae endocarditis confirmed by polymerase chain reaction, serology, and culture.
[Source 3 ]Carrion’s disease (Bartonella bacilliformis infection)
Bartonella bacilliformis infection or Carrion’s disease has 2 distinct phases, Oroya fever and Veruga perruana (“Peruvian warts”):
- Oroya fever: During this phase, patients may present with fever, headache, muscle aches, abdominal pain, and severe anemia. Complications may occur in up to 70 percent of patients with Oroya fever, including secondary infections and cardiopulmonary complications such as heart failure, pericardial effusion, pulmonary edema, and cardiogenic shock.
- Verruga peruana also called Peruvian warts: During this later phase, lesions appear under the skin as nodular growths, then emerge from the skin as red-to-purple vascular lesions that are prone to ulceration and bleeding.
The acute phase of Carrion’s disease lasts from one to four weeks and severity can range from mild to fatal 3. Absence of antibiotic treatment can lead to a mortality rate of up to 88% 3. This is caused by the massive invasion of red blood cells and initially leads to non-specific symptoms such as malaise, drowsiness, headache, chills, fever, anorexia and myalgia, which make the patient increasingly more jaundiced and confused 3. As Carrion’s disease progresses, a severe hemolytic condition, accompanied by lymphadenopathy and hepatosplenomegaly, is established. Carrion’s disease worsening can lead to acute respiratory distress, pericardial effusion, myocarditis, endocarditis, delirium, seizures, coma and multiple organ failure 1, 17, 50.
After an average of two months in the acute febrile phase (which may not occur, particularly in natives of the endemic region) the Peruvian wart (Verruga peruana) appears, an eruptive cutaneous manifestation formed by angiomatous lesions, which is often clinically and histologically similar to lesions of bacillary angiomatosis 3. Peruvian wart (Verruga peruana) lesions may present as angiomatous lesions, papules, papule-tumors, or nodules. They appear in patches, predominantly on the face and extremities, and measure 0.2–4 cm in diameter. They may persist for months or even years, and can be accompanied by fever, bone, and/or joint pains. The severity of the eruption is variable and it appears not to be related to previous antibiotic treatment. This is the tissue phase of Carrion’s disease and is self-limiting 49. Although not fatal, if left untreated, these lesions persist as pathogen reservoirs and a source of contagion through the vector. Bartonella bacilliformis infection is usually treated with rifampicin, although streptomycin is also effective and was the drug of choice before 1975. Peruvian wart does not respond to treatment with chloramphenicol or penicillin 3. Treatment alternatives include ciprofloxacin and azithromycin associated with deflazacort 51. It does not lead to scarring, except when there is secondary infection 52, 53.
As with many Bartonella species, Bartonella bacilliformis can sometimes cause infection of the heart valves (endocarditis). In many cases, blood cultures might be negative (culture-negative endocarditis), which can make the diagnosis more challenging.
Figure 8. Verruga peruana (Peruvian warts)

Footnotes: Patients with Verruga peruana (Peruvian warts) caused by Bartonella bacilliformis. (Left) 9‑year‑old girl with numerous bleeding verrugas on her legs. (Right) 17‑year‑old girl (facing left) showing multiple verrugas (Peruvian warts) close to her left elbow; a single verruga has broken the overlying epidermis, and
may later bleed
Trench fever (Bartonella quintana infection)
Bartonella quintana bacteria are spread to people by human body lice. Body lice spread from person to person by close physical contact or through shared clothing or bedding. Bartonella quintana infection is most commonly associated with body louse infestations in areas of high population density and poor sanitation. During the first World War, infection with Bartonella quintana was referred to as “trench fever” due to the many cases among soldiers who lived in crowded trenches under poor hygienic conditions. People experiencing homelessness are at increased risk of developing Bartonella quintana infection because of limited access to shower and laundry facilities. Bartonella quintana infections are currently being reported in hikers, alcoholics, and AIDS patients in the United States and Europe 3. Bartonella quintana disease has been considered as re-emergent and is the bacteria implicated in cases of chronic bacteremia, endocarditis, and bacillary angiomatosis.
Humans are the only known reservoirs and the transmission from person to person is through body lice, the reason why Bartonella quintana bacteria is strongly associated to unsanitary conditions and poor personal hygiene 55. Bartonella quintana disease is also known as quintana fever or five-day fever, and it has an incubation period of 15–25 days. Trench fever can be asymptomatic or severe. Approximately half of those affected experience a sudden onset of flu-like symptoms with no respiratory symptoms and short duration. High and prolonged fever can occur over several weeks. Symptoms remit for many days and after an asymptomatic period there can be paroxysmal clinical exacerbation three to five times or more within a year 3. Eighty to 90% of patients present with reddish, maculopapular lesions of up to 1 cm on the trunk 56. Furred tongue, conjunctival congestion, and musculoskeletal pain are frequently associated symptoms 57.
Bartonella quintana infection signs and symptoms may include:
- Fever (may occur once or repeatedly).
- Bone pain (mainly in the shins, neck, and back).
- Skin lesions called “bacillary angiomatosis”. Bacillary angiomatosis is an abnormal or excessive growth of blood vessels disorder caused by the Bartonella bacteria, primarily Bartonella henselae and Bartonella quintana. Bacillary angiomatosis can present as vascular lesions in the skin, under the skin, in bone, or in other organs. Bacillary angiomatosis typically affects people with weakened immune systems such as those with advanced HIV infection, presenting with skin lesions that can resemble Kaposi’s sarcoma or pyogenic granuloma. While most commonly seen in the skin, bacillary angiomatosis can also involve internal organs like the liver, spleen, and lymph nodes.
As with many Bartonella species, Bartonella quintana bacteria can sometimes cause infection of the heart valves (endocarditis). In many cases, blood cultures might be negative (culture-negative endocarditis), which can make the diagnosis more challenging.
Figure 9. Bacillary angiomatosis

Bartonellosis diagnosis
There is no standard laboratory diagnosis for infections caused by Bartonella bacteria.
- Cat scratch disease (Bartonella henselae) may be diagnosed presumptively in patients with typical signs and symptoms and a compatible exposure history. Serology can confirm the diagnosis, although cross-reactivity may limit interpretation in some circumstances. In general, lymph node aspiration is not recommended except to relieve severe pain and swelling or in cases where the diagnosis is unclear.
- Bartonella test
- Bartonella henselae DNA may be detected by polymerase chain reaction (PCR) or culture of lymph node aspirates or blood, though sensitivity of these methods is not optimal for blood samples.
- Since Bartonella henselae is a fastidious, slow-growing bacterium, cultures should be held for a minimum of 21 days.
- Trench fever can be diagnosed by isolation of Bartonella quintana from blood cultured on blood or chocolate agar under 5% CO2. Microcolonies can be seen after 21 days of incubation at 37°C.
- Trench fever can also be diagnosed by serology.
- Carrión’s disease is typically diagnosed via blood culture or direct observation of the bacilli in peripheral blood smears during the acute phase of infection (Oroya fever).
- Endocarditis due to Bartonella species can be diagnosed by serology and by polymerase chain reaction (PCR) or culture of excised heart valve tissue.
- Histologically, Verruga peruana (Peruvian warts) lesions show a proliferation of endothelial cells of the terminal vasculature in the dermis and subcutis. The acute and chronic inflammatory infiltrate that accompanies the presence of Bartonella bacilliformis in the interstice and inside the endothelial cells is an important finding, even in non-ulcerated lesions. The lesions can have more differentiated and ectatic vessels that are clinically and histologically similar to pyogenic granuloma. Cellular atypia can be seen, particularly in more solid lesions, with imperceptible lumens and spindle cells that resemble Kaposi sarcoma 3.
The culture of Bartonella bacteria gives a definitive diagnosis, but it is a very time-consuming and expensive process with incubation periods as long as 21 days 2. Bartonella bacteria are very slow-growing, fastidious, and primary isolation is difficult, with the detection of colonies only after 1 to 4 weeks of incubation on blood agar plates 2. As Bartonella bacteria are difficult to culture, culture is not routinely recommended 2. Serology is the best initial test and can be performed by indirect fluorescent assay (IFA) or enzyme-linked immunosorbent assay (ELISA) 2.
Serological testing such as indirect fluorescence assay (IFA) for Bartonella henselae antibodies was the first microbiological test available but has a variable positive predictive value 2. It is an indirect diagnostic method that can be negative in the early stage of the disease. In some studies, the positive predictive value of the indirect immunofluorescence assay (IFA) for Bartonella henselae was reported to be high (91.4%) 2. Conversely, some studies found a lack of sensitivity of the serological test among patients with cat scratch disease. While there is variability in multiple studies of Bartonella henselae IgG and IgM indirect fluorescent antibody and ELISA serology, typical sensitivity values are approximately 50% to 80%, whereas specificity is 90% to 100% 27. Sensitivity increases when there is a higher clinical index of suspicion for cat scratch disease. An IgM titer of 1:16 or higher shows acute disease, with a 3-month duration of detection in 50% of patients 2. An IgG titer higher than 1:256 is considered evidence of current or past Bartonella infection 2. Unlike culture and PCR (polymerase chain reaction) of blood, serology does not rely on Bartonella being present in the blood 2. Serological testing can be used to evaluate response to therapy.
Histopathological examination of the tissue infected by Bartonella species usually shows neutrophils, lymphocytes, and debris scattered throughout the lesions 2. Warthin-Starry silver staining will show small dark staining bacteria and electron microscopic findings include pleomorphic bacilli with a trilaminar wall 2. Histopathological examination for Bartonella bacilliformis is performed using Giemsa stain, and it shows cytoplasmic inclusions known as Rocha-Lima inclusions 28.
Advanced diagnostic techniques such as PCR (polymerase chain reaction) on lymph nodes or other material have been applied to the detection of Bartonella 2. PCR provides the advantages of high specificity and rapid identification, however lacking in sensitivity, ranging from 43% to 76% 2. The sensitivity of PCR with samples of lymph node tissue or aspirates is 30-60% for cat scratch disease. A polymerase chain reaction (PCR) can detect different Bartonella species; specificity is high, but the sensitivity is lower than with serology 2.
Cat scratch disease diagnosis
If you have swollen lymph nodes and a scratch or bite from a cat, your doctor may suspect cat-scratch disease.
To diagnose cat scratch disease, your doctor will perform a physical exam where he/she will:
- Look at your scratch or wound (if you have one).
- Look at your skin for a rash or bumps.
- Feel your lymph nodes. Sometimes, an infected lymph node may form a tunnel (fistula) through the skin and drain (leak fluid).
- A physical exam may also reveal an enlarged spleen.
Sometimes cat scratch disease is diagnosed with physical exam alone. However, cat scratch disease is hard to diagnose, in part because it is rare.
Your doctor may also:
- Take a sample of your blood to test for Bartonella henselae bacteria. The Bartonella henselae immunofluorescence assay (IFA) blood test can detect the infection caused by these bacteria. The results of this test will be considered along with other information from your medical history, lab tests, or biopsy.
- In rare cases, a lymph node biopsy may also be done to test for Bartonella henselae bacteria or for other causes of swollen glands.
Trench fever (Bartonella quintana infection) diagnosis
People can get Bartonella quintana infection from the human body louse. You can diagnose body lice infestation by finding eggs and crawling lice in the seams of clothing. Sometimes you can see a body louse crawling or feeding on the skin. Although body lice and nits can be large enough to see with the naked eye, a magnifying lens may help to find crawling lice or eggs.
Bartonella quintana infection symptoms include fever (may occur once or repeatedly), bone pain (mainly in the shins, neck, and back), and bacillary angiomatosis. People experiencing homelessness are at increased risk of developing infection with Bartonella quintana bacteria because of limited access to shower and laundry facilities.
- Bartonella quintana is a fastidious, slow-growing bacterium. Cultures should be held for a minimum of 21 days. It is often helpful for providers to alert the microbiology laboratory that Bartonella quintana is suspected to optimize conditions for growth.
- Serology can aid the diagnosis of Bartonella quintana, although cross-reactivity with other Bartonella species may limit interpretation. Doctors should be aware that serological tests do not reliably differentiate among Bartonella species and positive results may persist for years even after effective treatment.
- Molecular detection including PCR (Polymerase Chain Reaction) can be particularly useful in cases of culture-negative endocarditis. Patients with infectious endocarditis sometimes have damaged heart valves that need to be surgically replaced. Molecular detection of Bartonella spp. should be performed on excised heart valve tissue if a patient with endocarditis requires surgical valvular replacement. For patients with suspected Bartonella quintana bacteremia, PCR testing can also be performed on blood.
Bartonella bacilliformis infection diagnosis
Bartonella bacilliformis is typically diagnosed by blood culture or direct observation of the bacteria in peripheral blood smears during the acute phase of infection (Oroya fever).
Bartonellosis Differential Diagnosis
Bartonellosis differential diagnosis may include:
- Atypical mycobacterial diseases
- Coccidioidomycosis and valley fever
- Leishmaniasis
- Lyme disease
- Lymphogranuloma venereum (LGV)
- Nocardiosis
- Sarcoidosis
- Sporotrichosis
- Syphilis
- Toxoplasmosis
Bartonellosis treatment
Bartonellosis treatment depends on the underlying Bartonella infection. Trench fever, Carrión’s disease, and endocarditis due to Bartonella bacteria are serious infections that require antibiotic treatment. Doctors should consult with an expert in infectious diseases regarding treatment options. Management of cat scratch disease depends on the clinical presentation of the disease. Because cat-scratch disease is not serious and self-limiting condition, with most cases of regional lymphadenopathy resolving spontaneously in two to four months, medical treatment may not be needed 29. However, studies have shown that the use of a single antibiotic regimen will reduce the duration of cat scratch disease symptoms significantly. The antimicrobial agents commonly used for cat scratch disease are azithromycin, ciprofloxacin, gentamicin, trimethoprim-sulfamethoxazole, and rifampin 2. For patients with extensive lymphadenopathy, oral azithromycin at 500 mg on the first day and 250 mg on days 2 to 5 2. For retinitis, oral Doxycycline 100 mg twice daily for 4 to 6 weeks and oral rifampin 300 mg twice daily for 4 to 6 weeks 2.
Trench fever or chronic bacteremia with Bartonella quintana can be treated with oral Doxycycline at 200 mg once daily for 4 weeks and intravenous gentamicin 3 mg/kg for 2 weeks 30. Gentamicin associated with doxycycline is considered the best treatment for endocarditis and trench fever, and rifampicin or streptomycin can also be used to treat Peruvian warts 13.
Bacillary angiomatosis and peliosis hepatis are treated with oral erythromycin 500 mg four times daily for 3 to 4 months 1, 2.
Documented Bartonella culture-positive endocarditis should be treated with oral Doxycycline 100 mg for 6 weeks and intravenous gentamicin at 3 mg/kg/day for 14 days 2.
Recommended treatment for neuroretinitis and for central nervous system (brain and spinal cord) involvement is a combination of oral doxycycline 100 mg twice daily and rifampin 300mg twice daily 31. There are no controlled clinical trials comparing a nontreatment group with those given antibiotics. However, retrospective case series consistently associated antibiotics with hastened visual recovery and improved visual outcomes. Corticosteroid use in cat scratch disease with eye involvement has had mixed results 2.
The management of Oroya fever (Bartonella bacilliformis infection) includes the use of ciprofloxacin as the primary choice with chloramphenicol, ceftriaxone being alternative choice that are very effective. Verruga peruana (Peruvian wart) is managed with azithromycin primarily with rifampin, ciprofloxacin, and chloramphenicol being the preferred alternatives 2.
Bartonella henselae treatment
Treatment of uncomplicated cat scratch disease remains controversial. Because cat-scratch disease is not serious and self-limiting condition, with most cases of regional lymphadenopathy resolving spontaneously in two to four months, medical treatment may not be needed. The use of antibiotics to shorten the course of disease is debated. Most cases of cat scratch disease resolve without treatment, although some patients may develop complications from disseminated disease. Azithromycin has been shown to decrease lymph node volume more rapidly compared to no treatment. The recommended dose of azithromycin for cat scratch disease is:
- For adults and children > 45.5 kg: Azithromycin 500 mg on day 1, followed by 250 mg for 4 days
- For children ≤ 45.5 kg: Azithromycin 10 mg/kg on day 1, followed by 5 mg/kg for 4 days
A number of other antibiotics are effective against Bartonella infections, including penicillins, tetracyclines, clarithromycin, cephalosporins, ciprofloxacin, trimethoprim-sulfamethoxazole and aminoglycosides. Since aminoglycosides are bactericidal, they are typically used as first-line treatment for Bartonella infections other than cat scratch disease. Often, with serious infections, more than one antibiotic is used. In people with HIV/AIDS and others, who have a weak immune system, cat-scratch disease can be more serious. Treatment with antibiotics may be needed.
Some studies suggest that certain antibiotics including doxycycline, erythromycin, gentamicin, rifampicin, trimethoprim + sulphamethoxazole and ciprofloxacin may significantly shorten the duration of lymphadenopathy. Antibiotics are warranted in patients with severe or persistent symptoms of cat scratch disease.
In rare cases, large pus-filled lymph nodes may persist for one to three years. The pus may need to be repeatedly drained through a needle. Pain and fever can be managed by increasing fluid intake and paracetamol. Warm moist compresses to affected lymph glands may decrease swelling and tenderness.
Bartonella quintana treatment
Infection with Bartonella quintana requires antibiotic treatment. A number of antibiotics are effective against Bartonella infections, including tetracyclines, aminoglycosides, and macrolides. More than one antibiotic is often used. Consult with an expert in infectious diseases regarding treatment options.
Trench fever or chronic bacteremia with Bartonella quintana can be treated with oral Doxycycline at 200 mg once daily for 4 weeks and intravenous gentamicin 3 mg/kg for 2 weeks 30.
Bartonella bacilliformis treatment
Infection with Bartonella bacilliformis bacteria requires antibiotic treatment. A number of antibiotics are effective against Bartonella infections, including tetracyclines, aminoglycosides, and macrolides. More than one antibiotic is often used. Consult with an expert in infectious diseases regarding treatment options.
The management of Oroya fever (Bartonella bacilliformis infection) includes the use of ciprofloxacin as the primary choice with chloramphenicol, ceftriaxone being alternative choice that are very effective. Verruga peruana (Peruvian wart) is managed with azithromycin primarily with rifampin, ciprofloxacin, and chloramphenicol being the preferred alternatives 2. Treatment alternatives include ciprofloxacin and azithromycin associated with deflazacort 51. Verruga peruana (Peruvian wart) does not lead to scarring, except when there is secondary infection 52, 53.
Bartonellosis prognosis
People who have a healthy immune system should recover fully without treatment. People with weak immune systems especially those with HIV infection and organ transplants may develop more serious problems and need antibiotic treatment to recover. Without therapy, the infection spreads systemically and can involve virtually any organ, and the outcome is sometimes fatal.
People with weak immune systems may develop complications such as:
- Encephalopathy (loss of brain function)
- Neuroretinitis (inflammation of the retina and optic nerve of the eye)
- Osteomyelitis (bone infection)
- Parinaud syndrome (red, irritated, and painful eye).
- Maguina C., Guerra H., Ventosilla P. Bartonellosis. Clin Dermatol. 2009;27:271–280. doi: 10.1016/j.clindermatol.2008.10.006[↩][↩][↩][↩][↩]
- Mada PK, Zulfiqar H, Joel Chandranesan AS. Bartonellosis. [Updated 2023 Jun 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430874[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Lins KA, Drummond MR, Velho PENF. Cutaneous manifestations of bartonellosis. An Bras Dermatol. 2019 Sep-Oct;94(5):594-602. doi: 10.1016/j.abd.2019.09.024[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Cheslock MA, Embers ME. Human Bartonellosis: An Underappreciated Public Health Problem? Trop Med Infect Dis. 2019 Apr 19;4(2):69. doi: 10.3390/tropicalmed4020069[↩][↩]
- Breitschwerdt EB, Bradley JM, Maggi RG, Lashnits E, Reicherter P. Bartonella Associated Cutaneous Lesions (BACL) in People with Neuropsychiatric Symptoms. Pathogens. 2020 Dec 4;9(12):1023. doi: 10.3390/pathogens9121023[↩]
- Dujardin J.C., Herrera S., do Rosario V., Arevalo J., Boelaert M., Carrasco H.J. Research priorities for neglected infectious diseases in Latin America and the Caribbean region. PLoS Negl Trop Dis. 2010;4:e780. doi: 10.1371/journal.pntd.0000780[↩]
- Pitassi L.H.U., Diniz P., Scorpio D.G., Drummond M.R., Lania B.G., Barjas-Castro M.L. Bartonella spp. bacteremia in blood donors from Campinas, Brazil. PLoS Negl Trop Dis. 2015;9:12. doi: 10.1371/journal.pntd.0003467[↩][↩][↩]
- Raoult D, Fournier PE, Drancourt M, Marrie TJ, Etienne J, Cosserat J, Cacoub P, Poinsignon Y, Leclercq P, Sefton AM. Diagnosis of 22 new cases of Bartonella endocarditis. Ann Intern Med. 1996 Oct 15;125(8):646-52. doi: 10.7326/0003-4819-125-8-199610150-00004. Erratum in: Ann Intern Med 1997 Aug 1;127(3):249.[↩][↩]
- Nelson CA, Moore AR, Perea AE, Mead PS. Cat scratch disease: U.S. clinicians’ experience and knowledge. Zoonoses Public Health. 2018 Feb;65(1):67-73. doi: 10.1111/zph.12368[↩]
- Brouqui P, Stein A, Dupont HT, Gallian P, Badiaga S, Rolain JM, Mege JL, La Scola B, Berbis P, Raoult D. Ectoparasitism and vector-borne diseases in 930 homeless people from Marseilles. Medicine (Baltimore). 2005 Jan;84(1):61-68. doi: 10.1097/01.md.0000152373.07500.6e[↩]
- Sanchez Clemente N, Ugarte-Gil CA, Solórzano N, Maguiña C, Pachas P, Blazes D, Bailey R, Mabey D, Moore D. Bartonella bacilliformis: a systematic review of the literature to guide the research agenda for elimination. PLoS Negl Trop Dis. 2012;6(10):e1819. doi: 10.1371/journal.pntd.0001819[↩]
- Pulliainen A.T., Dehio C. Persistence of Bartonella spp. stealth pathogens: from subclinical infections to vasoproliferative tumor formation. FEMS Microbiol Rev. 2012;36:563–599. doi: 10.1111/j.1574-6976.2012.00324.x[↩][↩][↩]
- Angelakis E., Raoult D. Pathogenicity and treatment of Bartonella infections. Int J Antimicrob Agents. 2014;44:16–25. doi: 10.1016/j.ijantimicag.2014.04.006[↩][↩][↩][↩][↩]
- Chomel B.B., Kasten R.W., Floyd-Hawkins K., Chi B., Yamamoto K., Roberts-Wilson J. Experimental transmission of Bartonella henselae by the cat flea. J Clin Microbiol. 1996;34:1952–1956. doi: 10.1128/jcm.34.8.1952-1956.1996[↩]
- Silva M.N., Vieira-Damiani G., Ericson M.E., Gupta K., Gilioli R., Almeida A.R. Bartonella henselae transmission by blood transfusion in mice. Transfusion. 2016;56:1556–1559. doi: 10.1111/trf.13545[↩]
- Correa F.G., Pontes C.L.S., Verzola R.M.M., Mateos J.C.P., Velho P., Schijman A.G. Association of Bartonella spp. bacteremia with Chagas cardiomyopathy, endocarditis and arrhythmias in patients from South America. Braz J Med Biol Res. 2012;45:644–651. doi: 10.1590/S0100-879X2012007500082[↩][↩]
- Pons M.J., Lovato P., Silva J., Urteaga N., Mendoza J.D., Ruiz J. Carrion’s disease after blood transfusion. Blood Transfus. 2016;14:527–530. doi: 10.2450/2015.0036-15[↩][↩][↩]
- Ellis D.I., Dunn W.B., Griffin J.L., Allwood J.W., Goodacre R. Metabolic fingerprinting as a diagnostic tool. Pharmacogenomics. 2007;8:1243–1266. doi: 10.2217/14622416.8.9.1243[↩]
- Minadakis G., Chochlakis D., Kokkini S., Gikas A., Tselentis Y., Psaroulaki A. Seroprevalence of Bartonella henselae antibodies in blood donors in Crete. Scand J Infect Dis. 2008;40:846–847. doi: 10.1080/00365540802120000[↩]
- Lamas C.C., Mares-Guia M.A., Rozental T., Moreira N., Favacho A.R.M., Barreira J. Bartonella spp. infection in HIV positive individuals, their pets and ectoparasites in Rio de Janeiro, Brazil: serological and molecular study. Acta Trop. 2010;115:137–141. doi: 10.1016/j.actatropica.2010.02.015[↩]
- Sun J.M., Fu G.M., Lin J.F., Song X.P., Lu L.A., Liu Q.Y. Seroprevalence of Bartonella in Eastern China and analysis of risk factors. BMC Infect Dis. 2010;10:4. doi: 10.1186/1471-2334-10-121[↩]
- Mansueto P., Pepe I., Cillari E., Arcoleo F., Micalizzi A., Bonura F. Prevalence of antibodies anti-Bartonella henselae in western Sicily: children, blood donors, and cats. J Immunoassay Immunochem. 2012;33:18–25. doi: 10.1080/15321819.2011.591476[↩]
- Noden B.H., Tshavuka F.I., van der Colf B.E., Chipare I., Wilkinson R. Exposure and risk factors to Coxiella burnetii, spotted fever group and typhus group rickettsiae, and Bartonella henselae among volunteer blood donors in Namibia. PLOS ONE. 2014;9 doi: 10.1371/journal.pone.0108674[↩]
- Muller A., Reiter M., Schotta A.M., Stockinger H., Stanek G. Detection of Bartonella spp. in Ixodes ricinus ticks and Bartonella seroprevalence in human populations. Ticks Tick-Borne Dis. 2016;7:763–767. doi: 10.1016/j.ttbdis.2016.03.009[↩]
- Yilmaz C, Ergin C, Kaleli I. Pamukkale Universitesi Kan Merkezine başvuran donörlerde Bartonella henselae seroprevalansinin araştirilmasi ve risk faktörlerinin irdelenmesi [Investigation of Bartonella henselae seroprevalence and related risk factors in blood donors admitted to Pamukkale University Blood Center]. Mikrobiyol Bul. 2009 Jul;43(3):391-401.[↩]
- Aydin N, Bülbül R, Tellı M, Gültekın B. Aydın ili kan donörlerinde Bartonella henselae ve Bartonella quintana seroprevalansı [Seroprevalence of Bartonella henselae and Bartonella quintana in blood donors in Aydin province, Turkey]. Mikrobiyol Bul. 2014 Jul;48(3):477-83. Turkish.[↩]
- Sander A, Posselt M, Oberle K, Bredt W. Seroprevalence of antibodies to Bartonella henselae in patients with cat scratch disease and in healthy controls: evaluation and comparison of two commercial serological tests. Clin Diagn Lab Immunol. 1998 Jul;5(4):486-90. doi: 10.1128/CDLI.5.4.486-490.1998[↩][↩]
- Arias-Stella J, Lieberman PH, Erlandson RA, Arias-Stella J Jr. Histology, immunohistochemistry, and ultrastructure of the verruga in Carrion’s disease. Am J Surg Pathol. 1986 Sep;10(9):595-610. doi: 10.1097/00000478-198609000-00002[↩][↩]
- Bass JW, Freitas BC, Freitas AD, Sisler CL, Chan DS, Vincent JM, Person DA, Claybaugh JR, Wittler RR, Weisse ME, Regnery RL, Slater LN. Prospective randomized double blind placebo-controlled evaluation of azithromycin for treatment of cat-scratch disease. Pediatr Infect Dis J. 1998 Jun;17(6):447-52. doi: 10.1097/00006454-199806000-00002[↩][↩]
- Foucault C, Raoult D, Brouqui P. Randomized open trial of gentamicin and doxycycline for eradication of Bartonella quintana from blood in patients with chronic bacteremia. Antimicrob Agents Chemother. 2003 Jul;47(7):2204-7. doi: 10.1128/AAC.47.7.2204-2207.2003[↩][↩][↩]
- Tunkel AR, Glaser CA, Bloch KC, Sejvar JJ, Marra CM, Roos KL, Hartman BJ, Kaplan SL, Scheld WM, Whitley RJ; Infectious Diseases Society of America. The management of encephalitis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2008 Aug 1;47(3):303-27. doi: 10.1086/589747[↩][↩]
- Chomel BB, Kasten RW, Floyd-Hawkins K, Chi B, Yamamoto K, Roberts-Wilson J, Gurfield AN, Abbott RC, Pedersen NC, Koehler JE. Experimental transmission of Bartonella henselae by the cat flea. J Clin Microbiol. 1996 Aug;34(8):1952-6. doi: 10.1128/jcm.34.8.1952-1956.1996[↩]
- Regier Y., Rourke F.O., Kempf V.A. Bartonella spp.—A chance to establish one health concepts in veterinary and human medicine. Parasit Vectors. 2016;9:261. doi: 10.1186/s13071-016-1546-x[↩][↩]
- Cheslock M.A., Embers M.E. Human bartonellosis: An underappreciated public health problem? Trop. Med. Infect. Dis. 2019;19:2. doi: 10.3390/tropicalmed4020069[↩][↩]
- Landau M., Kletter Y., Avidor B., Ephrat G., Ephros M., Brenner S., Giladi M. Unusual eruption as a presenting symptom of cat scratch disease. J. Am. Acad. Dermatol. 1999;41:833–836. doi: 10.1016/S0190-9622(99)70337-3[↩][↩]
- Mazur-Melewska K., Mania A., Kemnitz P., Figlerowicz M., Sluzewski W. Cat-scratch disease: a wide spectrum of clinical pictures. Postepy Dermatol Alergol. 2015;32:216–220. doi: 10.5114/pdia.2014.44014[↩]
- Maguina C, Guerra H, Ventosilla P. 2009. Bartonellosis. Clin. Dermatol. 27:271–280.[↩]
- Pachas P. 2000. Epidemiología de la Bartonelosis en el Peru. Oficina General de Epidemiología, Lima, Peru.[↩][↩]
- Maguina C, Garcia PJ, Gotuzzo E, Cordero L, Spach DH. 2001. Bartonellosis (Carrion’s disease) in the modern era. Clin. Infect. Dis. 33:772–779.[↩][↩]
- Caceres-Rios H, et al. 1995. Verruga peruana: an infectious endemic angiomatosis. Crit. Rev. Oncog. 6:47–56.[↩]
- Lydy SL, et al. 2008. Isolation and characterization of Bartonella bacilliformis from an expatriate Ecuadorian. J. Clin. Microbiol. 46:627–637.[↩]
- Schultz MG. 2010. Daniel Alcides Carrión [photo quiz]. Emerg. Infect. Dis. vol 16:1025–1027.[↩]
- Ricketts WE. 1948. Bartonella bacilliformis anemia (Oroya fever); a study of 30 cases. Blood 3:1025–1049.[↩]
- Garcia FU, Wojta J, Broadley KN, Davidson JM, Hoover RL. 1990. Bartonella bacilliformis stimulates endothelial cells in vitro and is angiogenic in vivo . Am. J. Pathol. 136:1125–1135.[↩]
- Chomel BB, et al. 2009. Ecological fitness and strategies of adaptation of Bartonella species to their hosts and vectors. Vet. Res. 40:29.[↩]
- Intruders below the Radar: Molecular Pathogenesis of Bartonella spp. Alexander Harms, Christoph Dehio. Clinical Microbiology Reviews Jan 2012, 25 (1) 42-78; DOI: 10.1128/CMR.05009-11 https://cmr.asm.org/content/25/1/42[↩]
- Harms A., Dehio C. Intruders below the radar: molecular pathogenesis of Bartonella spp. Clin Microbiol Rev. 2012;25:42–78. doi: 10.1128/CMR.05009-11[↩]
- Koehler JE, Sanchez MA, Garrido CS, Whitfeld MJ, Chen FM, Berger TG, Rodriguez-Barradas MC, LeBoit PE, Tappero JW. Molecular epidemiology of bartonella infections in patients with bacillary angiomatosis-peliosis. N Engl J Med. 1997 Dec 25;337(26):1876-83. doi: 10.1056/NEJM199712253372603[↩]
- Chian C.A., Arrese J.E., Pierard G.E. Skin manifestations of Bartonella infections. Int J Dermatol. 2002;41:461–466. doi: 10.1046/j.1365-4362.2002.01489.x[↩][↩]
- Dehio C. Molecular and cellular basis of Bartonella pathogenesis. Annu Rev Microbiol. 2004;58:365–390. doi: 10.1146/annurev.micro.58.030603.123700[↩]
- Minnick M.F., Anderson B.E., Lima A., Battisti J.M., Lawyer P.G., Birtles R.J. Oroya fever and verruga peruana: bartonelloses unique to South America. PLoS Negl Trop Dis. 2014;8 doi: 10.1371/journal.pntd.0002919. e2919[↩][↩]
- Alexander B. A review of bartonellosis in Ecuador and Colombia. Am J Trop Med Hyg. 1995;52:354–359. doi: 10.4269/ajtmh.1995.52.354[↩][↩]
- Garcia-Caceres U, Garcia FU. Bartonellosis. An immunodepressive disease and the life of Daniel Alcides Carrión. Am J Clin Pathol. 1991 Apr;95(4 Suppl 1):S58-66.[↩][↩]
- García-Quintanilla, Meritxell & Dichter, Alexander & Guerra, Humberto & Kempf, Volkhard. (2019). Carrion’s disease: More than a neglected disease. Parasites & Vectors. 12. 141. 10.1186/s13071-019-3390-2[↩]
- Foucault C., Brouqui P., Raoult D. Bartonella quintana characteristics and clinical management. Emerg Infect Dis. 2006;12:217–223. doi: 10.3201/eid1202.050874[↩]
- Pierard-Franchimont C., Quatresooz P., Pierard G.E. Skin diseases associated with Bartonella infection: facts and controversies. Clin Dermatol. 2010;28:483–488. doi: 10.1016/j.clindermatol.2010.03.003[↩]
- Maurin M., Raoult D. Bartonella (Rochalimaea) quintana infections. Clin Microbiol Rev. 1996;9:273. doi: 10.1128/cmr.9.3.273[↩]




{kind=link}