Contents
- What is bladder cancer
- Types of bladder cancer
- Urothelial carcinoma (transitional cell carcinoma)
- Other cancers that start in the bladder
- Risk of bladder cancer
- Bladder Cancer Risk Factors
- Smoking
- Workplace exposures
- Certain medicines or herbal supplements
- Arsenic in drinking water
- Not drinking enough fluids
- Race and ethnicity
- Age
- Gender
- Chronic bladder irritation and infections
- Personal history of bladder or other urothelial cancer
- Bladder birth defects
- Genetics and family history
- Prior chemotherapy or radiation therapy
- What Causes Bladder Cancer ?
- Bladder Cancer Be Prevention
- Can Bladder Cancer Be Found Early ?
- Signs and Symptoms of Bladder Cancer
- How is bladder cancer diagnosed ?
- Bladder Cancer Stages
- Survival Rates for Bladder Cancer
- Bladder cancer treatment
- Bladder Cancer Surgery
- Intravesical Therapy for Bladder Cancer
- Chemotherapy for Bladder Cancer
- Radiation Therapy for Bladder Cancer
- Immunotherapy for Bladder Cancer
- Treatment of Bladder Cancer, by Stage
- Can you lower your risk of the cancer progressing or coming back ?
- About dietary supplements
- If the cancer comes back
- Could you get a second cancer after bladder cancer treatment ?
- Follow-up after bladder cancer treatment
- Can you lower your risk of getting a second cancer ?
- Types of bladder cancer
What is bladder cancer
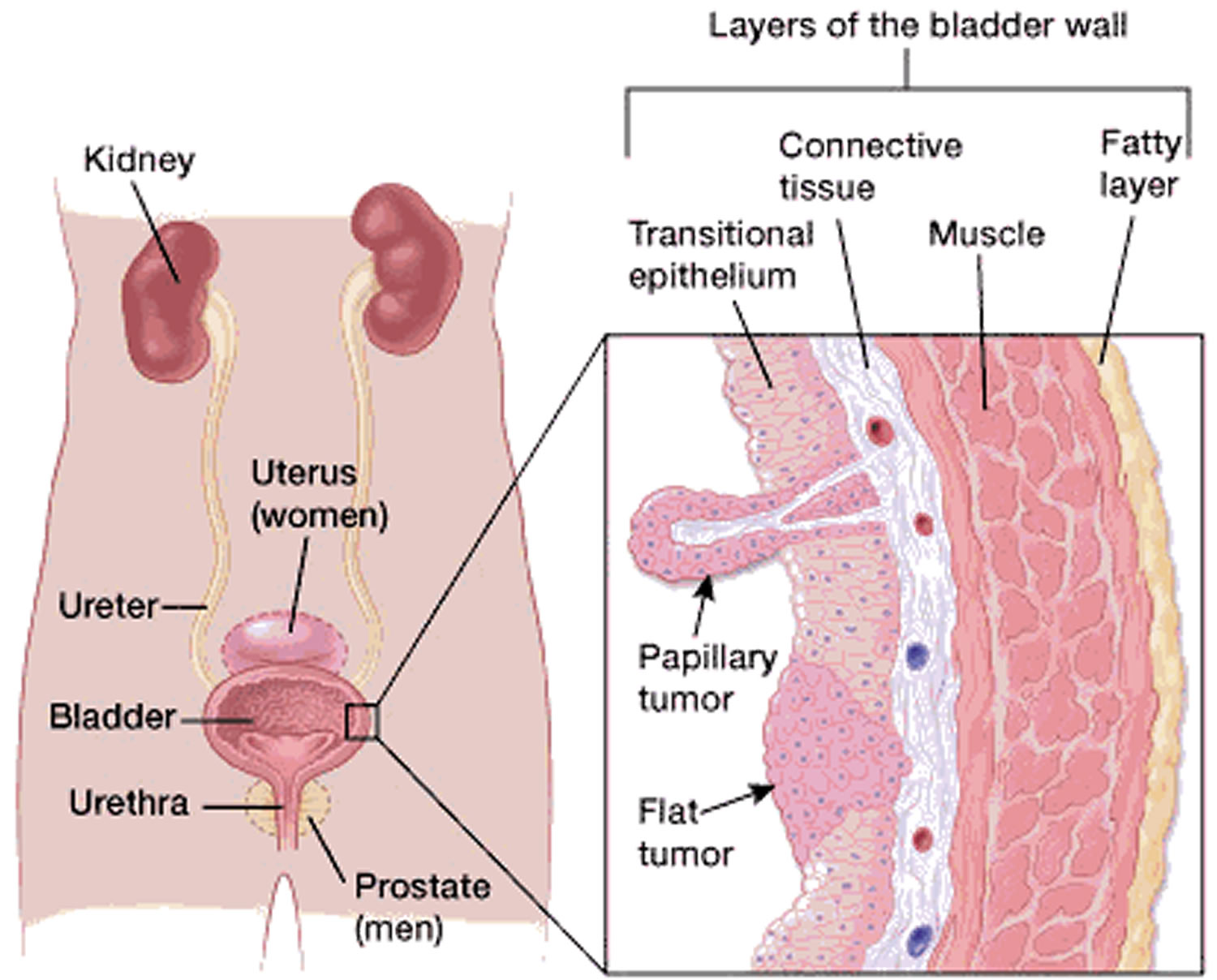
Bladder cancer begins when cells in the urinary bladder start to grow uncontrollably. As more cancer cells develop, they can form a tumor and spread to other areas of the body. The wall of the bladder has several layers, which are made up of different types of cells. Most bladder cancers start in the innermost lining of the bladder, which is called the urothelium or transitional epithelium. Although it’s most common in the bladder, this same type of cancer can occur in other parts of the urinary tract drainage system. As the cancer grows into or through the other layers in the bladder wall, it becomes more advanced and can be harder to treat.
Over time, the cancer might grow outside the bladder and into nearby structures. It might spread to nearby lymph nodes, or to other parts of the body. (If bladder cancer spreads, it often goes first to distant lymph nodes, the bones, the lungs, or the liver.)
Bladder cancer is one of the most common cancers.
The American Cancer Society’s estimates for bladder cancer in the United States for 2017 are:
- About 79,030 new cases of bladder cancer (about 60,490 in men and 18,540 in women)
- About 16,870 deaths from bladder cancer (about 12,240 in men and 4,630 in women)
The rates of new bladder cancers and of cancer deaths and have been dropping slightly in women in recent years. In men, incidence rates have been decreasing and death rates have been stable.
Bladder cancer accounts for about 5% of all new cancers in the US. It is the fourth most common cancer in men, but it is less common in women.
About seven out of every 10 bladder cancers diagnosed start out at an early stage — when bladder cancer is highly treatable. However, even early-stage bladder cancer may recur in the bladder. For this reason, people with bladder cancer typically need follow-up tests for years after treatment to look for bladder cancer that recurs or advances to a higher stage.
Figure 1. Urinary bladder location
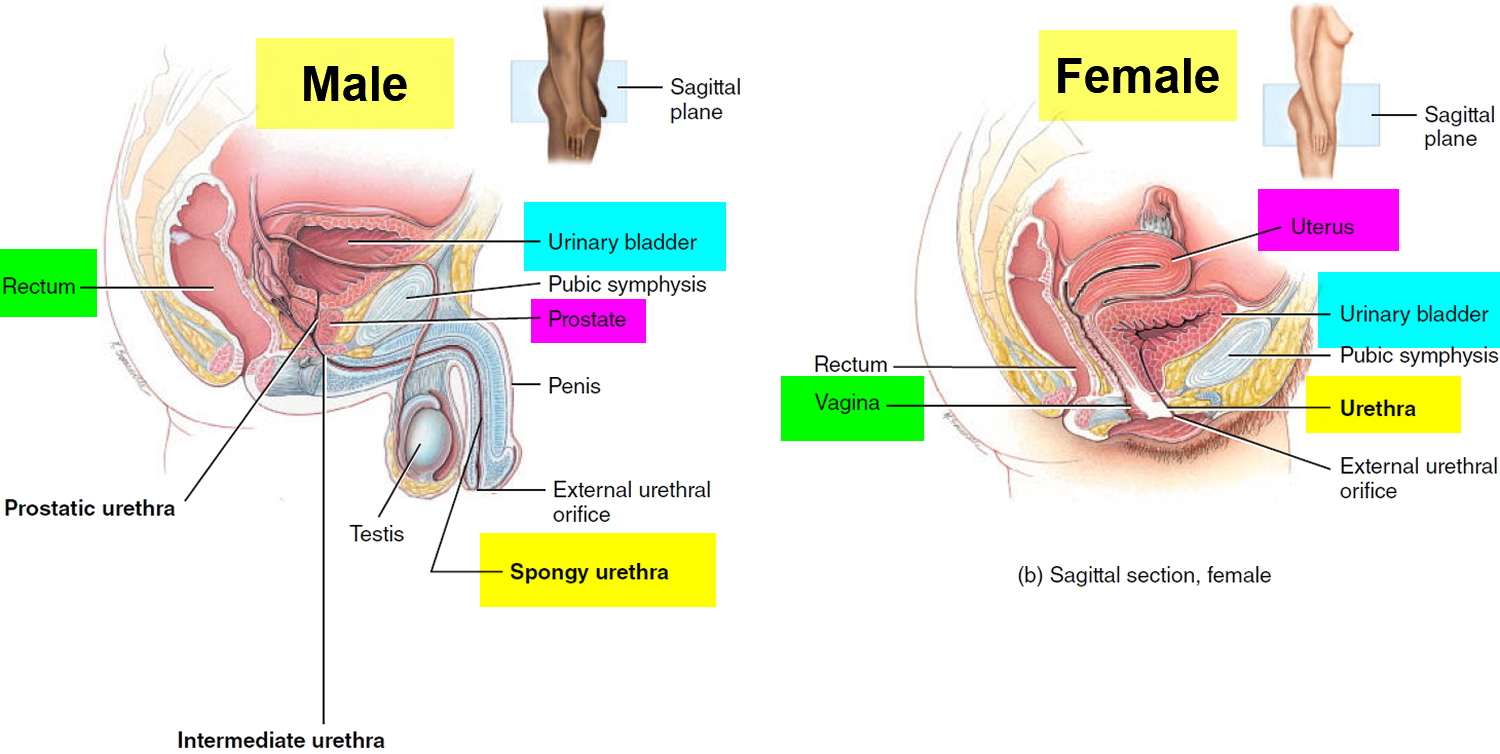
Figure 2. Urinary bladder anatomy
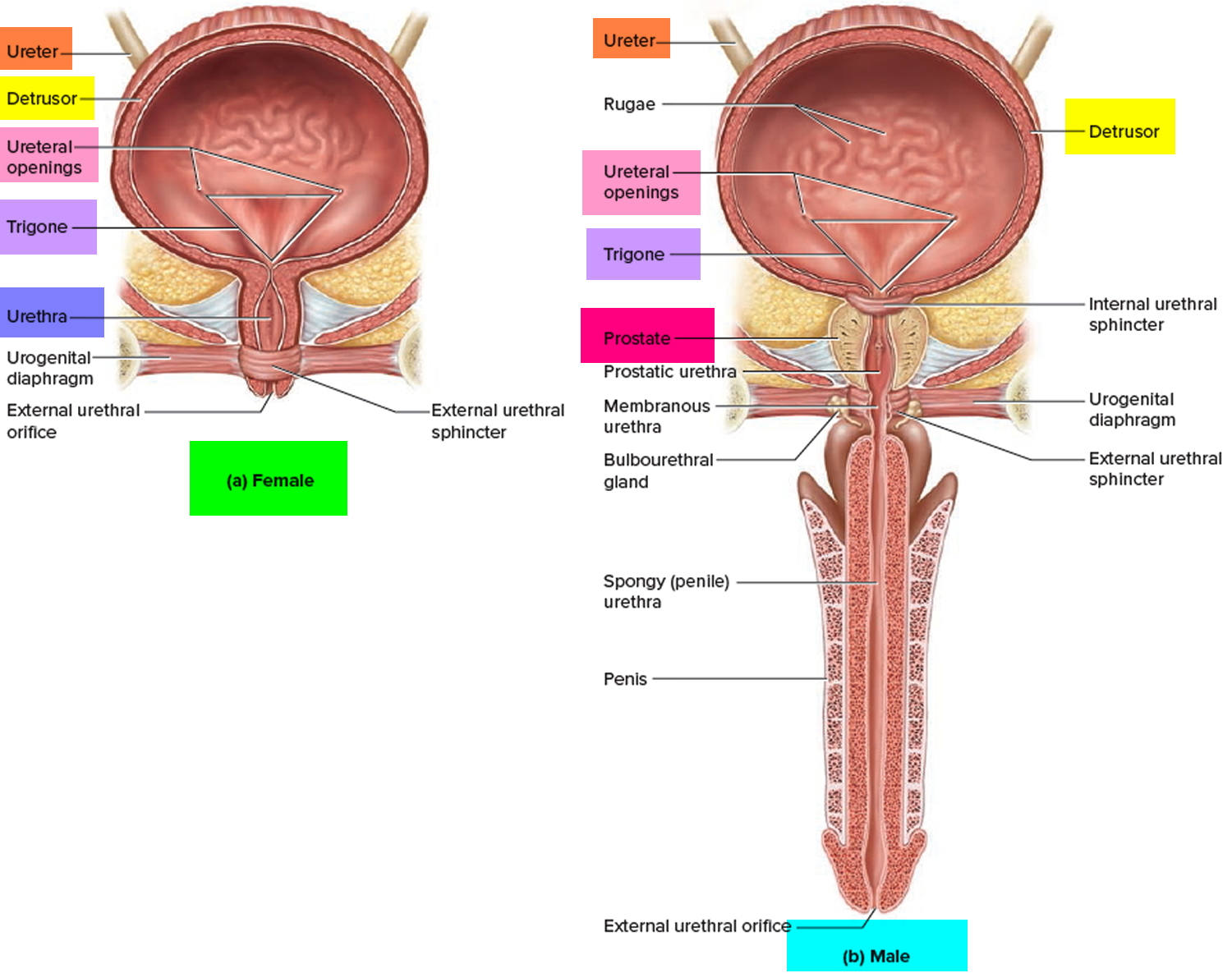
Figure 3. Bladder cancer

Figure 4. Bladder cancer type
Types of bladder cancer
Several types of cancer can start in the bladder.
Urothelial carcinoma (transitional cell carcinoma)
Urothelial carcinoma, also known as transitional cell carcinoma, is by far the most common type of bladder cancer 1. In fact, if you are told you have bladder cancer it is almost certain to be a urothelial carcinoma. These cancers start in the urothelial cells that line the inside of the bladder.
Urothelial cells also line other parts of the urinary tract, such as the part of the kidney that connects to the ureter (called the renal pelvis), the ureters, and the urethra. Patients with bladder cancer sometimes have other tumors in these places, so the entire urinary tract needs to be checked for tumors.
Invasive versus non-invasive bladder cancer
Bladder cancers are often described based on how far they have invaded into the wall of the bladder:
- Non-invasive cancers are still in the inner layer of cells (the transitional epithelium) but have not grown into the deeper layers.
- Invasive cancers have grown into deeper layers of the bladder wall. These cancers are more likely to spread and are harder to treat.
A bladder cancer can also be described as superficial or non-muscle invasive. These terms include both non-invasive tumors as well as any invasive tumors that have not grown into the main muscle layer of the bladder.
- About half of all bladder cancers are first found while the cancer is still confined to the inner layer of the bladder wall. These are called non-invasive or in situ cancers.
- About 1 in 3 bladder cancers have invaded into deeper layers but are still only in the bladder.
- In most of the remaining cases, the cancer has spread to nearby tissues or lymph nodes outside the bladder.
- Rarely (in about 4% of cases), it has spread to distant parts of the body. Black patients are slightly more likely to have more advanced disease when they are diagnosed, compared to whites.
Papillary versus flat cancer
Bladder cancers are also divided into 2 subtypes, papillary and flat, based on how they grow.
- Papillary carcinomas grow in slender, finger-like projections from the inner surface of the bladder toward the hollow center. Papillary tumors often grow toward the center of the bladder without growing into the deeper bladder layers. These tumors are called non-invasive papillary cancers. Very low-grade (slow growing), non-invasive papillary cancer is sometimes called papillary urothelial neoplasm of low-malignant potential and tends to have a very good outcome.
- Flat carcinomas do not grow toward the hollow part of the bladder at all. If a flat tumor is only in the inner layer of bladder cells, it is known as a non-invasive flat carcinoma or a flat carcinoma in situ (CIS).
If either a papillary or flat tumor grows into deeper layers of the bladder, it is called an invasive urothelial (or transitional cell) carcinoma.
Other cancers that start in the bladder
Several other types of cancer can start in the bladder, but these are all much less common than urothelial (transitional cell) cancer.
Squamous cell carcinoma: In the United States, only about 1% to 2% of bladder cancers are squamous cell carcinomas. Under a microscope, the cells look much like the flat cells that are found on the surface of the skin. Nearly all squamous cell carcinomas are invasive.
Adenocarcinoma: Only about 1% of bladder cancers are adenocarcinomas. The cancer cells have a lot in common with gland-forming cells of colon cancers. Nearly all adenocarcinomas of the bladder are invasive.
Small cell carcinoma: Less than 1% of bladder cancers are small-cell carcinomas, which start in nerve-like cells called neuroendocrine cells. These cancers often grow quickly and typically need to be treated with chemotherapy like that used for small cell carcinoma of the lung.
Sarcoma: Sarcomas start in the muscle cells of the bladder, but they are rare. More information can be found in Soft Tissue Sarcoma and Rhabdomyosarcoma.
These less common types of bladder cancer (other than sarcoma) are treated similar to transitional cell carcinomas, especially for early stage tumors, but if chemotherapy is needed, different drugs might be used.
Risk of bladder cancer
Bladder cancer occurs mainly in older people. About 9 out of 10 people with this cancer are over the age of 55. The average age at the time of diagnosis is 73.
Men are about 3 to 4 times more likely to get bladder cancer during their lifetime than women. Overall, the chance men will develop this cancer during their life is about 1 in 26. For women, the chance is about 1 in 88. But each person’s chances of getting bladder cancer can be affected by certain risk factors.
Whites are diagnosed with bladder cancer about twice as often as African Americans or Hispanic Americans.
Bladder Cancer Risk Factors
A risk factor is anything that changes your chance of getting a disease such as cancer. Different cancers have different risk factors. Some risk factors, like smoking, can be changed. Others, like a person’s age or family history, can’t be changed.
But having a risk factor, or even several, does not mean that you will get the disease. Many people with risk factors never get bladder cancer, while others with this disease may have few or no known risk factors.
Still, it’s important to know about the risk factors for bladder cancer because there may be things you can do that might lower your risk of getting it. If you are at higher risk because of certain factors, you might be helped by tests that could find it early, when treatment is most likely to be effective.
Several risk factors make a person more likely to develop bladder cancer.
Risk factors you can change
Smoking
Smoking is the most important risk factor for bladder cancer. Smokers are at least 3 times as likely to get bladder cancer as nonsmokers. Smoking causes about half of all bladder cancers in both men and women.
Workplace exposures
Certain industrial chemicals have been linked with bladder cancer. Chemicals called aromatic amines, such as benzidine and beta-naphthylamine, which are sometimes used in the dye industry, can cause bladder cancer.
Workers in other industries that use certain organic chemicals also may have a higher risk of bladder cancer. Industries carrying higher risks include makers of rubber, leather, textiles, and paint products as well as printing companies. Other workers with an increased risk of developing bladder cancer include painters, machinists, printers, hairdressers (probably because of heavy exposure to hair dyes), and truck drivers (likely because of exposure to diesel fumes).
Cigarette smoking and workplace exposures can act together to cause bladder cancer. Smokers who also work with cancer-causing chemicals have an especially high risk of bladder cancer.
Certain medicines or herbal supplements
According to the US Food and Drug Administration (FDA), use of the diabetes medicine pioglitazone (Actos) for more than one year may be linked with an increased risk of bladder cancer. This possible link is still an area of active research.
Dietary supplements containing aristolochic acid (mainly in herbs from the Aristolochia family) have been linked with an increased risk of urothelial cancers, including bladder cancer.
Arsenic in drinking water
Arsenic in drinking water has been linked with a higher risk of bladder cancer in some parts of the world. The chance of being exposed to arsenic depends on where you live and whether you get your water from a well or from a public water system that meets the standards for low arsenic content. For most Americans, drinking water is not a major source of arsenic.
Not drinking enough fluids
People who drink a lot of fluids, especially water, each day tend to have lower rates of bladder cancer. This might be because they empty their bladders more often, which could keep chemicals from lingering in their bladder.
Risk factors you cannot change
Race and ethnicity
Whites are about twice as likely to develop bladder cancer as African Americans and Hispanics. Asian Americans and American Indians have slightly lower rates of bladder cancer. The reasons for these differences are not well understood.
Age
The risk of bladder cancer increases with age. About 9 out of 10 people with bladder cancer are older than 55.
Gender
Bladder cancer is much more common in men than in women.
Chronic bladder irritation and infections
Urinary infections, kidney and bladder stones, bladder catheters left in place a long time, and other causes of chronic bladder irritation have been linked with bladder cancer (especially squamous cell carcinoma of the bladder), but it’s not clear if they actually cause bladder cancer.
Schistosomiasis (also known as bilharziasis), an infection with a parasitic worm that can get into the bladder, is also a risk factor for bladder cancer. In countries where this parasite is common (mainly in Africa and the Middle East), squamous cell cancers of the bladder are seen much more often. This is an extremely rare cause of bladder cancer in the United States.
Personal history of bladder or other urothelial cancer
Urothelial carcinomas can sometimes form in different areas in the bladder, as well as in the lining of the kidney, the ureters, and urethra. Having a cancer in the lining of any part of the urinary tract puts you at higher risk of having another cancer, either in the same area as before, or in another part of the urinary tract. This is true even when the first tumor is removed completely. For this reason, people who have had bladder cancer need careful follow-up to look for new cancers.
Bladder birth defects
Before birth, there is a connection between the belly button and the bladder. This is called the urachus. If part of this connection remains after birth, it could become cancerous. Cancers that start in the urachus are usually adenocarcinomas, which are made up of cancerous gland cells. About one-third of the adenocarcinomas of the bladder start here. However, this is still rare, accounting for less than half of 1% of all bladder cancers.
Another rare birth defect called exstrophy greatly increases a person’s risk of bladder cancer. In bladder exstrophy, both the bladder and the abdominal wall in front of the bladder don’t close completely during fetal development and are fused together. This leaves the inner lining of the bladder exposed outside the body. Surgery soon after birth can close the bladder and abdominal wall (and repair other related defects), but people who have this still have a higher risk for urinary infections and bladder cancer.
Genetics and family history
People who have family members with bladder cancer have a higher risk of getting it themselves. Sometimes this may be because the family members are exposed to the same cancer-causing chemicals (such as those in tobacco smoke). They may also share changes in some genes (like GST and NAT) that make it hard for their bodies to break down certain toxins, which can make them more likely to get bladder cancer.
A small number of people inherit a gene syndrome that increases their risk for bladder cancer. For example:
- A mutation of the retinoblastoma (RB1) gene can cause cancer of the eye in infants, and also increases the risk of bladder cancer.
- Cowden disease, caused by mutations in the PTEN gene, is linked mainly to cancers of the breast and thyroid. People with this disease also have a higher risk of bladder cancer.
- Lynch syndrome (also known as hereditary non-polyposis colorectal cancer, or HNPCC) is linked mainly to colon and endometrial cancer. People with this syndrome might also have an increased risk of bladder cancer (as well as other cancers of the urinary tract).
Prior chemotherapy or radiation therapy
Taking the chemotherapy drug cyclophosphamide (Cytoxan) for a long time can irritate the bladder and increase the risk of bladder cancer. People taking this drug are often told to drink plenty of fluids to help protect the bladder from irritation.
People who are treated with radiation to the pelvis are more likely to develop bladder cancer.
What Causes Bladder Cancer ?
Researchers do not know exactly what causes most bladder cancers. But they have found some risk factors (see What are the risk factors for bladder cancer?) and are starting to understand how they cause cells in the bladder to become cancer.
Certain changes in the DNA inside normal bladder cells can make them grow abnormally and form cancers. DNA is the chemical in each of our cells that makes up our genes, which control how our cells function. We usually look like our parents because they are the source of our DNA, but DNA affects more than just how we look.
Some genes control when cells grow, divide into new cells, and die:
- Genes that help cells grow, divide, and stay alive are called oncogenes.
- Genes that normally help control cell division, repair mistakes in DNA, or cause cells to die at the right time are called tumor suppressor genes.
Cancers can be caused by DNA changes (gene mutations) that turn on oncogenes or turn off tumor suppressor genes. Several different gene changes are usually needed for a cell to become cancer.
Acquired gene mutations
Most gene mutations related to bladder cancer develop during a person’s life rather than having been inherited before birth. Some of these acquired gene mutations result from exposure to cancer-causing chemicals or radiation. For example, chemicals in tobacco smoke can be absorbed into the blood, filtered by the kidneys, and end up in urine, where they can affect bladder cells. Other chemicals may reach the bladder the same way. But sometimes, gene changes may just be random events that sometimes happen inside a cell, without having an outside cause.
The gene changes that lead to bladder cancer are not the same in all people. Acquired changes in certain genes, such as the TP53 or RB1 tumor suppressor genes and the FGFR and RAS oncogenes, are thought to be important in the development of some bladder cancers. Changes in these and similar genes may also make some bladder cancers more likely to grow and invade the bladder wall than others. Research in this field is aimed at developing tests that can find bladder cancers at an early stage by finding their DNA changes.
Inherited gene mutations
Some people inherit gene changes from their parents that increase their risk of bladder cancer. But bladder cancer does not often run in families, and inherited gene mutations are not thought to be a major cause of this disease.
Some people seem to inherit a reduced ability to detoxify (break down) and get rid of certain types of cancer-causing chemicals. These people are more sensitive to the cancer-causing effects of tobacco smoke and certain industrial chemicals. Researchers have developed tests to identify such people, but these tests are not routinely done. It’s not certain how helpful the results of such tests might be, since doctors already recommend that all people avoid tobacco smoke and hazardous industrial chemicals.
Bladder Cancer Be Prevention
There is no sure way to prevent bladder cancer. Some risk factors such as age, gender, race, and family history can’t be controlled. But there may be things you can do that could lower your risk.
Don’t smoke
Smoking is thought to cause about half of all bladder cancers.
Limit exposure to certain chemicals in the workplace
Workers in industries that use certain organic chemicals may have a higher risk of bladder cancer. Workplaces where these chemicals are commonly used include the rubber, leather, printing materials, textiles, and paint industries. If you work in a place where you might be exposed to such chemicals, be sure to follow good work safety practices.
Some chemicals found in certain hair dyes might also increase risk, so it’s important for hairdressers and barbers who are exposed to these products regularly to use them safely. Most studies have not found that personal use of hair dyes increases bladder cancer risk.
Some research has suggested that people exposed to diesel fumes in the workplace might also have a higher risk of bladder cancer (as well as some other cancers), so limiting this exposure might be helpful.
Drink plenty of liquids
There is some evidence that drinking a lot of fluids – mainly water – might lower a person’s risk of bladder cancer.
Eat lots of fruits and vegetables
Some studies have suggested that a diet high in fruits and vegetables might help protect against bladder cancer, but other studies have not found this. Still, eating a healthy diet has been shown to have many benefits, including lowering the risk of some other types of cancer.
Can Bladder Cancer Be Found Early ?
Bladder cancer can sometimes be found early. Finding it early improves your chances that it can be treated successfully.
Screening for bladder cancer
Screening is the use of tests or exams to look for a disease in people who have no symptoms. At this time, no major professional organizations recommend routine screening of the general public for bladder cancer. This is because no screening test has been shown to lower the risk of dying from bladder cancer in people who are at average risk.
Some doctors may recommend bladder cancer tests for people at very high risk, such as:
- People who had bladder cancer before
- People who had certain birth defects of the bladder
- People exposed to certain chemicals at work
Tests that might be used to look for bladder cancer
Tests for bladder cancer look for different substances or cancer cells in the urine.
Urinalysis: One way to test for bladder cancer is to check for blood in the urine (called hematuria). This can be done during a urinalysis, which is a simple test to check for blood and other substances in a sample of urine. This test is sometimes done during a general health checkup.
Blood in the urine is usually caused by benign (non-cancerous) conditions such as infections, but it also can be the first sign of bladder cancer. Large amounts of blood in urine can be seen if the urine turns pink or red, but a urinalysis is needed to find small amounts.
Urinalysis can help find some bladder cancers early, but it has not been shown to be useful as a routine screening test.
Urine cytology: In this test, the doctor uses a microscope to look for cancer cells in urine. Urine cytology does find some cancers, but it is not reliable enough to make a good screening test.
Urine tests for tumor markers: Several newer tests look for substances in the urine that might indicate bladder cancer. These include:
- UroVysion™: This test looks for chromosome changes that are often seen in bladder cancer cells.
- BTA tests: These tests look for a substance called bladder tumor-associated antigen (BTA), also known as CFHrp, in the urine.
- Immunocyt™: This test looks at cells in the urine for the presence of substances such as mucin and carcinoembryonic antigen (CEA), which are often found on cancer cells.
- NMP22 BladderChek®: This test looks for a protein called NMP22 in the urine, which is often found at higher levels in people who have bladder cancer.
These tests might find some bladder cancers early, but they can miss some as well. In other cases, the test result might be abnormal even in some people who do not have cancer. At this time the tests are used mainly to look for bladder cancer in people who already have signs or symptoms of cancer, or in people who have had a bladder cancer removed to check for cancer recurrence. Further research is needed before these or other newer tests are proven useful as screening tests.
Watching for possible symptoms of bladder cancer
While no screening tests are recommended for people at average risk, bladder cancer can often be found early because it causes blood in the urine or other urinary symptoms (see Signs and symptoms of bladder cancer). Many of these symptoms often have less serious causes, but it’s important to have them checked by a doctor right away so the cause can be found and treated, if needed. If the symptoms are from bladder cancer, finding it early offers the best chance for successful treatment.
Signs and Symptoms of Bladder Cancer
Bladder cancer can often be found early because it causes blood in the urine or other urinary symptoms.
Blood in the urine
In most cases, blood in the urine (called hematuria) is the first sign of bladder cancer. Sometimes, there is enough blood to change the color of the urine to orange, pink, or, less often, darker red. Sometimes, the color of the urine is normal but small amounts of blood are found when a urine test (urinalysis) is done because of other symptoms or as part of a general medical checkup.
Blood may be present one day and absent the next, with the urine remaining clear for weeks or months. If a person has bladder cancer, blood eventually reappears.
Usually, the early stages of bladder cancer cause bleeding but little or no pain or other symptoms.
Blood in the urine does not always mean you have bladder cancer. More often it is caused by other things like an infection, benign (non-cancerous) tumors, stones in the kidney or bladder, or other benign kidney diseases. But it’s important to have it checked by a doctor so the cause can be found.
Changes in bladder habits or symptoms of irritation
Bladder cancer can sometimes cause changes in urination, such as:
- Having to urinate more often than usual
- Pain or burning during urination
- Feeling as if you need to go right away, even when the bladder is not full
- Having trouble urinating or having a weak urine stream
These symptoms are also more likely to be caused by a urinary tract infection (UTI), bladder stones, an overactive bladder, or an enlarged prostate (in men). Still, it’s important to have them checked by a doctor so that the cause can be found and treated, if needed.
Symptoms of advanced bladder cancer
Bladder cancers that have grown large enough or have spread to other parts of the body can sometimes cause other symptoms, such as:
- Being unable to urinate
- Lower back pain on one side
- Loss of appetite and weight loss
- Feeling tired or weak
- Swelling in the feet
- Bone pain
Again, many of these symptoms are more likely to be caused by something other than bladder cancer, but it’s important to have them checked so that the cause can be found and treated, if needed.
If there is a reason to suspect you might have bladder cancer, the doctor will use one or more exams or tests to find out if it is cancer or something else.
How is bladder cancer diagnosed ?
Bladder cancer is often found because of signs or symptoms a person is having, or it might be found because of lab tests a person gets for another reason. If bladder cancer is suspected, exams and tests will be needed to confirm the diagnosis. If cancer is found, further tests will be done to help determine the extent ( stage) of the cancer.
Medical history and physical exam
Your doctor will want to get your medical history to learn more about your symptoms. The doctor might also ask about possible risk factors, including your family history.
A physical exam can provide other information about possible signs of bladder cancer and other health problems. The doctor might do a digital rectal exam, during which a gloved, lubricated finger is put into your rectum. If you are a woman, the doctor might do a pelvic exam as well. During these exams, the doctor can sometimes feel a bladder tumor, determine its size, and feel if and how far it has spread.
If the results of the exam are abnormal, your doctor will probably do lab tests and might refer you to a urologist (a doctor specializing in diseases of the urinary system and male reproductive system) for further tests and treatment.
Urine lab tests
Urinalysis
This is a simple test to check for blood and other substances in a sample of urine.
Urine cytology
For this test, a sample of urine is looked at with a microscope to see if it has any cancer or pre-cancer cells. Cytology is also done on any bladder washings taken during a cystoscopy. Cytology can help find some cancers, but this test is not perfect. Not finding cancer on this test doesn’t always mean you are cancer free.
Urine culture
If you are having urinary symptoms, this test may be done to see if an infection (rather than cancer) is the cause. Urinary tract infections and bladder cancers can have similar symptoms. For a urine culture, a sample of urine is put into a dish in the lab to allow any bacteria that are present to grow. It can take time for the bacteria to grow, so it may take a few days to get the results of this test.
Urine tumor marker tests
Different urine tests look for specific substances released by bladder cancer cells. One or more of these tests may be used along with urine cytology to help determine if you have bladder cancer. These include the tests for NMP22 (BladderChek) and BTA (BTA stat), the Immunocyt test, and the UroVysion test.
Some doctors find these urine tests useful in looking for bladder cancers, but they may not help in all cases. Most doctors feel that cystoscopy is still the best way to find bladder cancer. Some of these tests are more helpful when looking for a possible recurrence of bladder cancer in someone who has already had it, rather than finding it in the first place.
Cystoscopy
If bladder cancer is suspected, doctors will recommend a cystoscopy. For this exam, a urologist places a cystoscope – a thin tube with a light and a lens or a small video camera on the end – through the opening of the urethra and advances it into the bladder. Sterile salt water is then injected through the scope to expand the bladder and allow the doctor to look at its inner lining.
Cystoscopy can be done in a doctor’s office or in an operating room. Usually the first cystoscopy will be done in the doctor’s office using a small, flexible fiber-optic device. Some sort of local anesthesia may be used to numb the urethra and bladder for the procedure. If the cystoscopy is done using general anesthesia (where you are asleep) or spinal anesthesia (where the lower part of your body is numbed), the procedure is done in the operating room.
Fluorescence cystoscopy (also known as blue light cystoscopy) may be done along with routine cystoscopy. For this exam, a light-activated drug is put into the bladder during cystoscopy. It is taken up by cancer cells. When the doctor then shines a blue light through the cystoscope, any cells containing the drug will glow (fluoresce). This can help the doctor see abnormal areas that might have been missed by the white light normally used.
Transurethral resection of bladder tumor
If an abnormal area (or areas) is seen during a cystoscopy, it will be biopsied to see if it is cancer. A biopsy is the removal of small samples of body tissue to see if it is cancer. If bladder cancer is suspected, a biopsy is needed to confirm the diagnosis.
The procedure used to biopsy an abnormal area is a transurethral resection of bladder tumor (TURBT), also known as just a transurethral resection (TUR). During this procedure, the doctor removes the tumor and some of the bladder muscle near the tumor. The removed samples are then sent to a lab to look for cancer. If cancer is found, this can also show if it has invaded into the muscle layer of the bladder wall.
Bladder cancer can sometimes develop in more than one area of the bladder (or in other parts of the urinary tract). Because of this, the doctor may take samples from several different areas of the bladder, especially if cancer is strongly suspected but no tumor can be seen. Salt water washings of the inside the bladder may also be collected to look for cancer cells.
Biopsy results
The biopsy samples are sent to a lab, where they are looked at by a pathologist, a doctor who specializes in diagnosing diseases with lab tests. If bladder cancer is found, two important features are its invasiveness and grade.
Invasiveness: The biopsy can show how deeply the cancer has invaded (grown into) the bladder wall which is very important in deciding treatment.
- If the cancer stays in the inner layer of cells without growing into the deeper layers, it is called non-invasive.
- If the cancer grows into the deeper layers of the bladder, it is called invasive.
Invasive cancers are more likely to spread and are harder to treat.
You may also see a bladder cancer described as superficial or non-muscle invasive. These terms include both non-invasive tumors as well as any invasive tumors that have not grown into the main muscle layer of the bladder.
Grade: Bladder cancers are also assigned a grade, based on how they look under the microscope.
- Low-grade cancers look more like normal bladder tissue. They are also called well-differentiated cancers. Patients with these cancers usually have a good prognosis (outlook).
- High-grade cancers look less like normal tissue. These cancers may also be called poorly differentiated or undifferentiated. High-grade cancers are more likely to grow into the bladder wall and to spread outside the bladder. These cancers can be harder to treat.
Imaging tests
Imaging tests use x-rays, magnetic fields, sound waves, or radioactive substances to create pictures of the inside of your body.
If you have bladder cancer, your doctor may order some of these tests to see if the cancer has spread to structures near the bladder, to nearby lymph nodes, or to distant organs. If an imaging test shows enlarged lymph nodes or other possible signs of cancer spread, some type of biopsy might be needed to confirm the findings.
Intravenous pyelogram (IVP)
An intravenous pyelogram (IVP), also called an intravenous urogram (IVU), is an x-ray of the urinary system taken after injecting a special dye into a vein. This dye is removed from the bloodstream by the kidneys and then passes into the ureters and bladder. The dye outlines these organs on x-rays and helps show urinary tract tumors.
It’s important to tell your doctor if you have any allergies or have ever had a reaction to x-ray dyes, or if you have any type of kidney problems. If so, your doctor might choose to do another test instead.
Retrograde pyelogram
For this test, a catheter (thin tube) is placed through the urethra and up into the bladder or into a ureter. Then a dye is injected through the catheter to make the lining of the bladder, ureters, and kidneys easier to see on x-rays.
This test isn’t used as often as IVP, but it may be done (along with ultrasound of the kidneys) to look for tumors in the urinary tract in people who can’t have an IVP.
Computed tomography (CT) scan
A CT scan uses x-rays to make detailed cross-sectional images of your body. A CT scan of the kidney, ureters, and bladder is known as a CT urogram. It can provide detailed information about the size, shape, and position of any tumors in the urinary tract, including the bladder. It can also help show enlarged lymph nodes that might contain cancer, as well as other organs in the abdomen and pelvis.
CT-guided needle biopsy: CT scans can also be used to guide a biopsy needle into a suspected tumor. This is not used to biopsy tumors in the bladder, but it can be used to take samples from areas where the cancer may have spread. For this procedure, you lie on the CT scanning table while the doctor advances a biopsy needle through the skin and into the tumor.
Magnetic resonance imaging (MRI) scan
Like CT scans , MRI scans show detailed images of soft tissues in the body. But MRI scans use radio waves and strong magnets instead of x-rays.
MRI images are particularly useful in showing if the cancer has spread outside of the bladder into nearby tissues or lymph nodes. A special MRI of the kidneys, ureters, and bladder, known as an MRI urogram, can be used instead of an IVP to look at the upper part of the urinary system.
Ultrasound
Ultrasound uses sound waves to create pictures of internal organs. It can be useful in determining the size of a bladder cancer and whether it has spread beyond the bladder to nearby organs or tissues. It can also be used to look at the kidneys.
This is usually an easy test to have, and it uses no radiation.
Ultrasound-guided needle biopsy: Ultrasound can also be used to guide a biopsy needle into a suspected area of cancer spread in the abdomen or pelvis.
Chest x-ray
A chest x-ray may be done to see if the bladder cancer has spread to the lungs. This test is not needed if a CT scan of the chest has been done.
Bone scan
A bone scan can help look for cancer that has spread to bones. Doctors don’t usually order this test unless you have symptoms such as bone pain, or if blood tests show the cancer might have spread to your bones.
For this test, you get an injection of a small amount of low-level radioactive material, which settles in areas of damaged bone throughout the body. A special camera detects the radioactivity and creates a picture of your skeleton.
A bone scan may suggest cancer in the bone, but to be sure, other imaging tests such as plain x-rays, MRI scans, or even a bone biopsy might be needed.
Biopsies to look for cancer spread
If imaging tests suggest the cancer might have spread outside of the bladder, a biopsy might be needed to be sure.
In some cases, biopsy samples of suspicious areas are obtained during surgery to remove the bladder cancer.
Another way to get a biopsy sample is to use a thin, hollow needle to take a small piece of tissue from the abnormal area. This is known as a needle biopsy, and by using it the doctor can take samples without an operation. Needle biopsies are sometimes done using a CT scan or ultrasound to help guide the biopsy needle into the abnormal area.
Bladder Cancer Stages
What is the stage of a cancer ?
The stage of a bladder cancer describes how far it has spread. It’s one of the most important factors in choosing treatment options and predicting a person’s prognosis (outlook). If you have bladder cancer, ask your cancer care team to explain its stage. This can help you make informed choices about your treatment.
There are actually 2 types of stages for bladder cancer.
- The clinical stage is the doctor’s best estimate of the extent of the cancer, based on the results of physical exams, cystoscopy, biopsies, and any imaging tests that are done (such as CT scans). These exams and tests are described in Tests for bladder cancer.
- If surgery is done to treat the cancer, the pathologic stage can be determined using the same factors as the clinical stage, plus what is found during surgery.
The clinical stage is used to help plan treatment. Sometimes, though, the cancer has spread farther than the clinical stage estimates. Pathologic staging is likely to be more accurate, because it gives your doctor a firsthand impression of the extent of your cancer.
Understanding your bladder cancer stage
A staging system is a standard way for the cancer care team to describe how far a cancer has spread. The staging system most often used for bladder cancer is the American Joint Committee on Cancer TNM system, which is based on 3 key pieces of information:
- T describes how far the main (primary) tumor has grown through the bladder wall and whether it has grown into nearby tissues.
- N indicates any cancer spread to lymph nodes near the bladder. Lymph nodes are bean-sized collections of immune system cells, to which cancers often spread first.
- M indicates whether or not the cancer has spread (metastasized) to distant sites, such as other organs or lymph nodes that are not near the bladder.
Numbers or letters appear after T, N, and M to provide more details about each of these factors. Higher numbers mean the cancer is more advanced.
T categories for bladder cancer
The T category describes how far the main tumor has grown into the wall of the bladder (or beyond).
The wall of the bladder has 4 main layers.
- The innermost lining is called the urothelium or transitional epithelium.
- Beneath the urothelium is a thin layer of connective tissue, blood vessels, and nerves.
- Next is a thick layer of muscle.
- Outside of this muscle, a layer of fatty connective tissue separates the bladder from other nearby organs.
Nearly all bladder cancers start in the urothelium. As the cancer grows into or through the other layers in the bladder, it becomes more advanced.
TX: Main tumor cannot be assessed due to lack of information
T0: No evidence of a primary tumor
Ta: Non-invasive papillary carcinoma
Tis: Non-invasive flat carcinoma (flat carcinoma in situ, or CIS)
T1: The tumor has grown from the layer of cells lining the bladder into the connective tissue below. It has not grown into the muscle layer of the bladder.
T2: The tumor has grown into the muscle layer.
T2a: The tumor has grown only into the inner half of the muscle layer.
T2b: The tumor has grown into the outer half of the muscle layer.
T3: The tumor has grown through the muscle layer of the bladder and into the fatty tissue layer that surrounds it.
T3a: The spread to fatty tissue can only be seen by using a microscope.
T3b: The spread to fatty tissue is large enough to be seen on imaging tests or to be seen or felt by the surgeon.
T4: The tumor has spread beyond the fatty tissue and into nearby organs or structures. It may be growing into any of the following: the stroma (main tissue) of the prostate, the seminal vesicles, uterus, vagina, pelvic wall, or abdominal wall.
T4a: The tumor has spread to the stroma of the prostate (in men), or to the uterus and/or vagina (in women).
T4b: The tumor has spread to the pelvic wall or the abdominal wall.
Bladder cancer can sometimes affect many areas of the bladder at the same time. If more than one tumor is found, the letter m is added to the appropriate T category.
N categories for bladder cancer
The N category describes spread only to the lymph nodes near the bladder (in the true pelvis) and those along the blood vessel called the common iliac artery. These lymph nodes are called regional lymph nodes. Any other lymph nodes are considered distant lymph nodes. Spread to distant nodes is considered metastasis (described in the M category). Surgery is usually needed to find cancer spread to lymph nodes, since it is not often seen on imaging tests.
NX: Regional lymph nodes cannot be assessed due to lack of information.
N0: There is no regional lymph node spread.
N1: The cancer has spread to a single lymph node in the true pelvis.
N2: The cancer has spread to 2 or more lymph nodes in the true pelvis.
N3: The cancer has spread to lymph nodes along the common iliac artery.
M categories for bladder cancer
M0: There are no signs of distant spread.
M1: The cancer has spread to distant parts of the body. (The most common sites are distant lymph nodes, the bones, the lungs, and the liver.)
Stages of bladder cancer
Once the T, N, and M categories have been determined, this information is combined to find the overall cancer stage. Bladder cancer stages are defined using 0 and the Roman numerals I to IV (1 to 4). Stage 0 is the earliest stage, while stage IV is the most advanced.
Stage 0a (Ta, N0, M0)
The cancer is a non-invasive papillary carcinoma (Ta). It has grown toward the hollow center of the bladder but has not grown into the connective tissue or muscle of the bladder wall. It has not spread to nearby lymph nodes (N0) or distant sites (M0).
Stage 0is (Tis, N0, M0)
The cancer is a flat, non-invasive carcinoma (Tis), also known as flat carcinoma in situ (CIS). The cancer is growing in the inner lining layer of the bladder only. It has not grown inward toward the hollow part of the bladder, nor has it invaded the connective tissue or muscle of the bladder wall. It has not spread to nearby lymph nodes (N0) or distant sites (M0).
Stage I (T1, N0, M0)
The cancer has grown into the layer of connective tissue under the lining layer of the bladder but has not reached the layer of muscle in the bladder wall (T1). The cancer has not spread to nearby lymph nodes (N0) or to distant sites (M0).
Stage II (T2a or T2b, N0, M0)
The cancer has grown into the thick muscle layer of the bladder wall, but it has not passed completely through the muscle to reach the layer of fatty tissue that surrounds the bladder (T2). The cancer has not spread to nearby lymph nodes (N0) or to distant sites (M0).
Stage III (T3a, T3b, or T4a, N0, M0)
The cancer has grown into the layer of fatty tissue that surrounds the bladder (T3a or T3b). It might have spread into the prostate, uterus, or vagina, but it is not growing into the pelvic or abdominal wall (T4a). The cancer has not spread to nearby lymph nodes (N0) or to distant sites (M0).
Stage IV
One of the following applies:
T4b, N0, M0: The cancer has grown through the bladder wall and into the pelvic or abdominal wall (T4b). The cancer has not spread to nearby lymph nodes (N0) or to distant sites (M0).
OR
Any T, N1 to N3, M0: The cancer has spread to nearby lymph nodes (N1-N3) but not to distant sites (M0).
OR
Any T, any N, M1: The cancer has spread to distant lymph nodes or to sites such as the bones, liver, or lungs (M1).
Survival Rates for Bladder Cancer
Survival rates tell you what portion of people with the same type and stage of cancer are still alive a certain amount of time (usually 5 years) after they were diagnosed. They can’t tell you how long you will live, but they may help give you a better understanding about how likely it is that your treatment will be successful. Some people will want to know the survival rates for their cancer, and some people won’t.
Cancer survival rates don’t tell the whole story
Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they can’t predict what will happen in any particular person’s case. There are a number of limitations to remember:
- The numbers below are among the most current available. But to get 5-year survival rates, doctors have to look at people who were treated at least 5 years ago. As treatments are improving over time, people who are now being diagnosed with bladder cancer may have a better outlook than these statistics show.
- These statistics are based on the stage of the cancer when it was first diagnosed. They do not apply to cancers that later come back or spread, for example.
- The outlook for people with bladder cancer varies by the stage (extent) of the cancer – in general, the survival rates are higher for people with earlier stage cancers. But many other factors can affect a person’s outlook, such as age and overall health, and how well the cancer responds to treatment. The outlook for each person is specific to their circumstances.
Your doctor can tell you how these numbers may apply to you, as he or she is familiar with your particular situation.
Survival rates for bladder cancer
According to the most recent data, when including all stages of bladder cancer:
- The 5-year relative survival rate is about 77%
- The 10-year relative survival rate is about 70%
- The 15-year relative survival rate is about 65%
Keep in mind that just as 5-year survival rates are based on people diagnosed and first treated more than 5 years ago, 10-year survival rates are based on people diagnosed more than 10 years ago (and 15-year survival rates are based on people diagnosed at least 15 years ago).
Survival rates, by stage
The numbers below are based on thousands of people diagnosed with bladder cancer from 1988 to 2001. These numbers come from the National Cancer Institute’s SEER database.
- The 5-year relative survival rate for people with stage 0 bladder cancer is about 98%.
- The 5-year relative survival rate for people with stage I bladder cancer is about 88%.
- For stage II bladder cancer, the 5-year relative survival rate is about 63%.
- The 5-year relative survival rate for stage III bladder cancer is about 46%.
- Bladder cancer that has spread to other parts of the body is often hard to treat. Stage IV bladder cancer has a relative 5-year survival rate of about 15%. Still, there are often treatment options available for people with this stage of cancer.
Remember, these survival rates are only estimates – they can’t predict what will happen to any individual person. We understand that these statistics can be confusing and may lead you to have more questions. Talk to your doctor to better understand your specific situation.
Bladder cancer treatment
Depending on the stage of the cancer and other factors, treatment options for people with bladder cancer can include:
- Surgery
- Intravesical therapy
- Chemotherapy
- Radiation therapy
- Immunotherapy
Sometimes, the best option might include more than one of type of treatment. Surgery, alone or with other treatments, is part of the treatment for most bladder cancers. Surgery can often remove early-stage bladder tumors. But a major concern in people with early-stage bladder cancer is that new cancers often form in other parts of the bladder over time. Removing the entire bladder (known as a radical cystectomy) is one way to avoid this, but it can have major side effects. If the entire bladder is not removed, other treatments may be given to try to reduce the risk of new cancers. Whether or not other treatments are given, close follow-up is needed to look for signs of new cancers in the bladder.
Which doctors treat bladder cancer ?
Depending on your options, you can have different types of doctors on your treatment team. The types of doctors who treat bladder cancers include:
- Urologists: surgeons who specialize in treating diseases of the urinary system and male reproductive system
- Radiation oncologists: doctors who treat cancer with radiation therapy
- Medical oncologists: doctors who treat cancer with medicines such as chemotherapy and immunotherapy
You might have many other specialists on your treatment team as well, including physician assistants (PAs), nurse practitioners (NPs), nurses, psychologists, social workers, nutrition specialists, rehabilitation specialists, and other health professionals. See Health Professionals Associated With Cancer Care for more on this.
Making treatment decisions
It’s important to discuss all of your treatment options, including their goals and possible side effects, with your doctors to help make the decision that best fits your needs. Some important things to consider include:
- Your age and expected life span
- Any other serious health conditions you have
- The stage and grade of your cancer
- The likelihood that treatment will cure your cancer (or help in some other way)
- Your feelings about the possible side effects from treatment
You may feel that you must make a decision quickly, but it’s important to give yourself time to absorb the information you have just learned. It’s also very important to ask questions if there is anything you’re not sure about.
Getting a second opinion
You may also want to get a second opinion. This can give you more information and help you feel more certain about the treatment plan you choose. If you aren’t sure where to go for a second opinion, ask your doctor for help.
Thinking about taking part in a clinical trial
Clinical trials are carefully controlled research studies that are done to get a closer look at promising new treatments or procedures. Clinical trials are one way to get state-of-the art cancer treatment. In some cases, they may be the only way to get access to newer treatments. They are also the best way for doctors to learn better methods to treat cancer. Still, they are not right for everyone.
If you would like to learn more about clinical trials that might be right for you, start by asking your doctor if your clinic or hospital conducts clinical trials.
Bladder Cancer Surgery
Surgery is part of the treatment for most bladder cancers. The type of surgery done depends on the stage (extent) of the cancer.
Transurethral resection of bladder tumor (TURBT)
A transurethral resection of bladder tumor (TURBT), also known as just a transurethral resection (TUR), is often used to determine if someone has bladder cancer and, if so, whether the cancer has invaded the muscle layer of the bladder wall.
This is also the most common treatment for early-stage or superficial (non-muscle invasive) bladder cancers. Most patients have superficial cancer when they are first diagnosed, so this is usually their first treatment. Some people might also get a second, more extensive TURBT as part of their treatment.
How Transurethral resection of bladder tumor (TURBT) is done
This surgery is done using an instrument put up the urethra, so it doesn’t require cutting into the abdomen. You will get either general anesthesia (where you are asleep) or regional anesthesia (where the lower part of your body is numbed).
For this operation, a type of rigid cystoscope called a resectoscope is placed into the bladder through the urethra. The resectoscope has a wire loop at its end to remove any abnormal tissues or tumors. The removed tissue is sent to a lab to be looked at by a pathologist.
After the tumor is removed, more steps may be taken to try to ensure that it has been destroyed completely. Any remaining cancer may be treated by fulguration (burning the base of the tumor) while looking at it with the cystoscope. Cancer can also be destroyed using a high-energy laser through the cystoscope.
Possible side effects
The side effects of TURBT are generally mild and do not usually last long. You might have some bleeding and pain when you urinate after surgery. You can usually return home the same day or the next day and can resume your usual activities within a week or two.
Even if the TURBT removes the tumor completely, bladder cancer often comes back (recurs) in other parts of the bladder. This might be treated with another TURBT. But if TURBT needs to be repeated many times, the bladder can become scarred and lose its capacity to hold much urine. Some people may have side effects such as frequent urination, or even incontinence (loss of control of urination).
In patients with a long history of recurrent, non-invasive low-grade tumors, the surgeon may sometimes just use fulguration to burn small tumors that are seen during cystoscopy (rather than removing them). This can often be done using local anesthesia (numbing medicine) in the doctor’s office. It is safe but can be mildly uncomfortable.
Cystectomy
When bladder cancer is invasive, all or part of the bladder may need to be removed. This operation is called a cystectomy.
Partial cystectomy: If the cancer has invaded the muscle layer of the bladder wall but is not very large and only in one place, it can sometimes be removed along with part of the bladder wall without taking out the whole bladder. The hole in the bladder wall is then closed. Nearby lymph nodes are also removed and examined for cancer spread. Only a small portion of people with cancer that has invaded the muscle can have this surgery.
The main advantage of this surgery is that the person keeps their bladder and doesn’t need reconstructive surgery (see below). But the remaining bladder may not hold as much urine, which means they will have to urinate more often. The main concern with this type of surgery is that bladder cancer can still recur in another part of the bladder wall.
Radical cystectomy: If the cancer is larger or is in more than one part of the bladder, a radical cystectomy will be needed. This operation removes the entire bladder and nearby lymph nodes. In men, the prostate and seminal vesicles are also removed. In women, the ovaries, fallopian tubes (tubes that connect the ovaries and uterus), the uterus (womb), cervix, and a small portion of the vagina are often removed along with the bladder.
General anesthesia (where you are in a deep sleep) is used for either type of cystectomy.
Typically, these procedures are done through a cut (incision) in the abdomen. You will need to stay in the hospital for about a week after the surgery. You can usually go back to your normal activities after several weeks.
In some cases, the surgeon may operate through several smaller incisions using special long, thin instruments, one of which has a tiny video camera on the end to see inside the pelvis. This is known as laparoscopic, or “keyhole” surgery. The surgeon may either hold the instruments directly or may sit at a control panel in the operating room and maneuver robotic arms to do the surgery (sometimes known as a robotic cystectomy). This type of surgery may result in less pain and quicker recovery because of the smaller incisions. But it hasn’t been around as long as the standard type of surgery, so it’s not yet clear if it is equally as effective.
It is important that any type of cystectomy be done by a surgeon with experience in treating bladder cancer. If the surgery is not done well, the cancer is more likely to come back.
Reconstructive surgery after radical cystectomy
If your whole bladder is removed, you will need another way to store urine and and remove it. Several types of reconstructive surgery can be done depending on your medical situation and personal preferences.
Incontinent diversion: One option may be to remove a short piece of your intestine and connect it to the ureters. This creates a passageway, known as an ileal conduit, for urine to pass from the kidneys to the outside of the body. Urine flows from the kidneys through the ureters into the ileal conduit. One end of the conduit is connected to the skin on the front of the abdomen by an opening called a stoma (also known as a urostomy).
After this procedure, a small bag is placed over the stoma to collect the urine, which comes out continuously in small amounts. The bag then needs to be emptied once it is full. This approach is sometimes called an incontinent diversion, because you no longer control the flow of urine out of the body.
Continent diversion: Another way for urine to drain is called a continent diversion. In this approach, a pouch is made from the piece of intestine that is attached to the ureters. One end of the pouch is connected to an opening (stoma) in the skin on the front of the abdomen. A valve is created in the pouch to allow urine to be stored there. You then empty the pouch several times a day by putting a drainage tube (catheter) into the stoma through the valve. Some people prefer this method because there is no bag on the outside.
Neobladder: A newer method routes the urine back into the urethra, restoring urination. To do this, the surgeon creates a neobladder – basically a new bladder made of a piece of intestine. As with the incontinent and continent diversions, the ureters are connected to the neobladder. The difference is that the neobladder is also sewn to the urethra. This lets the patient urinate normally. Over several months, most people regain the ability to urinate normally during the day, although many people might still have some incontinence at night.
If the cancer has spread or can’t be removed with surgery, a diversion may be made without removing the bladder. In this case, the purpose of the surgery is to prevent or relieve blockage of urine flow, rather than try to cure the cancer.
Risks and side effects of cystectomy
The risks with any type of cystectomy are much like those with any major surgery. Problems during or shortly after the operation can include:
- Reactions to anesthesia
- Bleeding from the surgery
- Blood clots in the legs or lungs
- Damage to nearby organs
- Infections at the surgery site
Most people will have at least some pain after the operation, which is usually helped with pain medicines, if needed.
Effects on urination: Bladder surgery can affect how you urinate. If you have had a partial cystectomy, this might be limited to having to go more often (because your bladder can’t hold as much urine).
If you have a radical cystectomy, you will need reconstructive surgery (described above) to create a new way for urine to leave your body. Depending on the type of reconstruction, you might need to learn how to empty your urostomy bag or to put a catheter into your stoma. Aside from these changes, urinary diversion and urostomy can also lead to:
- Infections
- Urine leaks
- Pouch stones
- Blockage of urine flow
The physical changes that come from removing the bladder and having a urostomy can affect your quality of life as well. Discuss your feelings and concerns with your health care team.
Sexual effects of radical cystectomy in men: Radical cystectomy removes the prostate gland and seminal vesicles. Since these glands make most of the seminal fluid, removing them means that a man will no longer make semen. He can still have an orgasm, but it will be “dry.”
After surgery, many men have nerve damage that affects their ability to have erections. In some men this may improve over time. Generally, the younger a man is, the more likely he is to regain the ability to have full erections. If this issue is important to you, discuss it with your doctor before surgery. Newer surgical techniques may lower the chance of erection problems.
Sexual effects of radical cystectomy in women: This surgery often removes the front part of the vagina. This can make sex less comfortable for some women, although most of the time intercourse is still possible. One option is to have the vagina rebuilt, which is known as vaginal reconstruction. There is more than one way to do this, so talk with your surgeon about the pros and cons of each. Whether or not you have reconstruction, there are many ways to make sex more comfortable.
Radical cystectomy can also affect a woman’s ability to have an orgasm if the nerve bundles that run along each side of the vagina are damaged. Talk with your doctor about whether these nerves can be left in place during surgery.
If the surgeon takes out the end of the urethra where it opens outside the body, the clitoris can lose some of its blood supply, which might affect sexual arousal. Talk with your surgeon about whether the end of the urethra can be spared.
Sexual effects of urostomy: It’s normal for both men and women to be concerned about having a sex life with a urostomy. Having your ostomy pouch fit correctly and emptying it before sex reduces the chances of a major leak. A pouch cover or small ostomy pouch can be worn with a sash to keep the pouch out of the way. Wearing a snug fitting shirt may be even more comfortable. Choose sexual positions that keep your partner’s weight from rubbing against the pouch.
Intravesical Therapy for Bladder Cancer
With intravesical therapy, the doctor puts a liquid drug directly into the bladder (through a catheter) rather than giving it by mouth or injecting it into a vein. The drug can affect the cells lining the bladder without having major effects in other parts of the body
When might intravesical therapy be used ?
Intravesical therapy is used after transurethral resection of bladder tumor (TURBT) for non-invasive (stage 0) or minimally invasive (stage I) bladder cancers to help keep the cancer from coming back.
It is used only for these early-stage cancers because medicines given this way mainly affect the cells lining the inside of the bladder, with little to no effect on cells elsewhere. This means that any cancer cells outside of the bladder lining, including those that have grown deeply into the bladder wall, are not treated. Drugs put into the bladder also can’t reach cancer cells in the kidneys, ureters, and urethra, or those that have spread to other organs.
Types of intravesical therapy
There are two types of intravesical therapy:
- Immunotherapy
- Chemotherapy
Intravesical immunotherapy
Immunotherapy causes the body’s own immune system to attack the cancer cells.
Bacillus Calmette-Guerin therapy: Bacillus Calmette-Guerin (BCG) is the main intravesical immunotherapy for treating early-stage bladder cancer. BCG is a germ that is related to the one that causes tuberculosis (TB), but it doesn’t usually cause serious disease. BCG is put directly into the bladder through a catheter. The body’s immune system cells are attracted to the bladder and activated by BCG, which in turn affects the bladder cancer cells. Treatment is usually started a few weeks after a TURBT and is given once a week for 6 weeks. Sometimes long-term maintenance BCG therapy is given.
Treatment with BCG can cause symptoms that feel like having the flu, such as fever, chills, and fatigue. It can also cause a burning feeling in the bladder. Rarely, BCG can spread through the body, leading to a serious infection. One sign of this can be a high fever that isn’t helped by aspirin or similar medicines. If this happens, call your doctor right away.
Intravesical chemotherapy
For this treatment, chemotherapy (chemo) drugs are put directly into the bladder through a catheter. These drugs kill actively growing cancer cells. Many of these same drugs can also be given systemically (usually into a vein) to treat more advanced stages of bladder cancer.
Mitomycin is the drug used most often for intravesical chemotherapy. Other drugs that can be used include valrubicin, docetaxel, thiotepa, and gemcitabine. Delivery of mitomycin into the bladder along with heating the inside of the bladder, a treatment called electromotive mitomycin therapy, may work even better than giving intravesical mitomycin the usual way.
A major advantage of giving chemo directly into the bladder instead of injecting it into the bloodstream is that the drugs usually do not reach other parts of the body. This helps people avoid many of the side effects that can occur with chemo..
The main side effects of intravesical chemo are irritation and a burning feeling in the bladder.
Chemotherapy for Bladder Cancer
Chemotherapy (chemo) is the use of drugs to treat cancer. Chemo for bladder cancer can be given in 2 different ways:
- Intravesical chemotherapy: For this treatment, the chemo drug is put directly into the bladder. This type of chemo is used only for very early-stage bladder cancers. It is described in Intravesical therapy for bladder cancer.
- Systemic chemotherapy: When chemo drugs are given in pill form or injected into a vein (IV) or muscle (IM), the drugs enter the bloodstream and travel throughout the body. This is called systemic chemotherapy. Systemic chemo can affect cancer cells far away from the main tumor.
When might chemotherapy be used ?
Systemic chemo can be used :
- Before surgery to try to shrink a large tumor so that it can be removed more easily and to lower the chance the cancer will come back. Giving chemo before surgery is known as neoadjuvant therapy.
- After surgery (or sometimes after radiation therapy). This is called adjuvant therapy. The goal of adjuvant therapy is to kill any cancer cells that remain after other treatments but are too small to be seen. This can lower the chance that the cancer will come back later.
- In people getting radiation therapy, to help the radiation work better.
- As the main treatment for advanced bladder cancers, such as those that have spread to distant parts of the body.
Which chemo drugs are used to treat bladder cancer ?
Chemo drugs may be used alone or in combination, depending on what they’re being used for, a person’s overall health, and other factors.
When chemo is given with radiation, the most common drugs used include:
- Cisplatin
- Cisplatin plus fluorouracil (5-FU)
- Mitomycin with 5-FU
When chemo is used without radiation, the most common combinations include:
- Gemcitabine and cisplatin
- Methotrexate, vinblastine, doxorubicin (Adriamycin), and cisplatin (called MVAC)
- Cisplatin, methotrexate, and vinblastine (called CMV)
- Carboplatin and either paclitaxel or docetaxel (for patients with poor kidney function)
For some people, the side effects of getting more than one chemo drug might be too much to handle. For those people, treatment with a single drug, such as gemcitabine or cisplatin, may be a good option. Other drugs sometimes used alone for bladder cancer include carboplatin, docetaxel, paclitaxel, doxorubicin, 5-FU, methotrexate, vinblastine, ifosfamide, and pemetrexed.
Doctors give chemo in cycles, with each period of treatment followed by a rest period to allow the body time to recover. Each cycle typically lasts for a few weeks.
Most bladder cancers are transitional cell (urothelial) cancers, but there are other types as well, including squamous cell carcinoma, adenocarcinoma, and small cell carcinoma. Chemo for these rare types of bladder cancer may use drugs different from those listed above.
Side effects of chemotherapy
Chemo drugs attack cells that are dividing quickly, which is why they work against cancer cells. But other cells in the body, such as those in the bone marrow (where new blood cells are made), the lining of the mouth and intestines, and the hair follicles, also divide quickly. These cells are also likely to be affected by chemo, which can lead to side effects.
The side effects of chemo depend on the type and dose of drugs given and how long they are taken. When chemo and radiation are given at the same time, side effects tend to be worse. Common side effects of chemo include:
- Nausea and vomiting
- Loss of appetite
- Hair loss
- Mouth sores
- Diarrhea or constipation
- Increased risk of infections (because of a shortage of white blood cells)
- Bleeding or bruising after minor cuts or injuries (due to a shortage of blood platelets)
- Fatigue (because of a shortage of red blood cells)
These side effects usually go away after treatment is finished. There are often ways to lessen these side effects. For example, drugs can be given to help prevent or reduce nausea and vomiting. Ask your health care team about the side effects your chemo drugs may cause.
Some chemo drugs can cause other, less common side effects. For example, drugs such as cisplatin, carboplatin, docetaxel, and paclitaxel can damage nerves. This can sometimes lead to symptoms (mainly in the hands and feet) such as pain, burning or tingling sensations, sensitivity to cold or heat, or weakness. This is called peripheral neuropathy. Some chemo drugs have been linked to an increased risk of leukemia later in life, but this is very rare.
Be sure to report any side effects to your medical team so that they can be treated promptly. In some cases, the doses of the chemo drugs may need to be reduced or treatment may need to be delayed or stopped to prevent the effects from getting worse.
Radiation Therapy for Bladder Cancer
Radiation therapy uses high-energy radiation to kill cancer cells.
When might radiation therapy be used ?
Radiation therapy can be used:
- As part of the treatment for some early stage bladder cancers, after surgery that doesn’t remove the whole bladder (such as TURBT)
- As the main treatment for people with earlier-stage cancers who can’t have surgery
- As part of the initial treatment for advanced bladder cancer
- To help prevent or treat symptoms caused by advanced bladder cancer
Radiation therapy is often combined with chemotherapy to make the radiation more effective. This is known as chemoradiation.
How is radiation therapy given ?
The type of radiation most often used to treat bladder cancer, known as external beam radiation therapy, focuses radiation from a source outside of the body on the cancer.
Before your treatments start, your radiation team will take careful measurements to find the correct angles for aiming the radiation beams and the proper dose of radiation. This planning session, called simulation, usually includes getting imaging tests such as CT or MRI scans.
The treatment is much like getting an x-ray, but the radiation is stronger. The procedure itself is painless. Each treatment lasts only a few minutes, but the setup time – getting you into place for treatment – usually takes longer. Most often, radiation treatments are given 5 days a week for several weeks.
Possible side effects of radiation therapy
Side effects of radiation depend on the dose given and the area being treated. They can include:
- Skin changes in areas getting radiation, ranging from redness to blistering and peeling
- Nausea and vomiting
- Bladder symptoms, like burning or pain when you urinate, feeling the need to go often, or blood in urine
- Diarrhea
- Fatigue
- Low blood counts, which can lead to fatigue, easy bruising or bleeding, or increased risk of infection
These effects usually go away after treatment, although some people can have longer-term problems. For example:
In some people radiation treatments can lead to incontinence (problems holding urine) later on.
Radiation can damage the lining of the bladder. This is known as radiation cystitis and can cause long-term problems such as blood in the urine or painful urination.
If you have side effects from radiation therapy, discuss them with your health care team. They can suggest ways to ease many of them.
Immunotherapy for Bladder Cancer
Immunotherapy is the use of medicines to help a person’s own immune system recognize and destroy cancer cells. Immunotherapy can sometimes be used to treat bladder cancer.
Intravesical Bacillus Calmette-Guerin (BCG) (for some early-stage cancers)
Bacillus Calmette-Guerin (BCG) is a type of bacteria related to the one that causes tuberculosis. While it doesn’t usually cause a person to get sick, it can help trigger an immune response. Bacillus Calmette-Guerin (BCG) can be put directly into the bladder (as a liquid) through a catheter. This activates immune system cells in the bladder, which in turn can attack bladder cancer cells.
For some early-stage cancers, BCG can be used after transurethral resection of bladder tumor (TURBT) to help keep the cancer from coming back. For more details on this treatment, see the section on intravesical therapy.
Immune checkpoint inhibitors (for advanced cancers)
An important part of the immune system is its ability to keep itself from attacking normal cells in the body. To do this, it uses “checkpoints” – molecules on immune cells that need to be turned on (or off) to start an immune response. Cancer cells sometimes use these checkpoints to avoid being attacked by the immune system. But newer drugs that target these checkpoints hold a lot of promise as cancer treatments.
Atezolizumab (Tecentriq), durvalumab (Imfinzi), and avelumab (Bavencio) are drugs that target PD-L1, a protein on cells (including some cancer cells) that helps keep the immune system from attacking them. By blocking PD-L1, these drugs boost the immune response against the cancer cells. This can shrink some tumors or slow their growth.
Nivolumab (Opdivo) and pembrolizumab (Keytruda) target PD-1, another protein that normally helps keep the immune system in check. Blocking PD-1 can help the immune system attack the cancer cells.
Any of these drugs can be used in people with advanced bladder that starts growing again after chemotherapy. Atezolizumab and pembrolizumab can also be used in people who can’t get the chemo drug cisplatin for some reason.
These drugs are given as intravenous (IV) infusions, typically every 2 or 3 weeks.
Possible side effects
Common side effects of these drugs include fatigue, nausea, loss of appetite, fever, urinary tract infections, rash, diarrhea, and constipation.
Less often, more serious side effects can occur. These drugs work by basically removing the brakes on the body’s immune system. Sometimes the immune system starts attacking other parts of the body, which can cause serious or even life-threatening problems in the lungs, intestines, liver, hormone-making glands, or other organs.
It’s very important to report any new side effects to your health care team promptly. If serious side effects do occur, treatment may need to be stopped and you may get high doses of corticosteroids to suppress your immune system.
Treatment of Bladder Cancer, by Stage
Most of the time, initial treatment of bladder cancer is based on the tumor’s clinical stage, which is how deep it is thought to have grown into the bladder wall and whether it has spread beyond the bladder. Other factors, such as the size and grade of the tumor and a person’s overall health, can also affect treatment options.
Treating stage 0 bladder cancer
Stage 0 bladder cancer includes non-invasive papillary carcinoma (Ta) and flat non-invasive carcinoma (Tis). In either case, the cancer has not invaded the bladder wall beyond the inner layer.
This early stage of bladder cancer is most often treated with transurethral resection (TURBT). This may be followed either by observation (close follow-up without further treatment) or by intravesical therapy to try to keep the cancer from coming back.
Of the intravesical treatments, immunotherapy with Bacille-Calmette Guerin (BCG) seems to be better than chemotherapy at both keeping cancers from coming back and from getting worse. But it also tends to have more side effects.
Stage 0 bladder cancers rarely need to be treated with more extensive surgery. Cystectomy (removal of the bladder) is considered only when there are many superficial cancers or when a superficial cancer continues to grow (or seems to be spreading) despite treatment.
Stage 0a
For low-grade non-invasive papillary (Ta) tumors, the options after TURBT include observation, a single dose of intravesical chemotherapy (usually with mitomycin) within a day of surgery, or weekly intravesical chemo, starting a few weeks after surgery. If the cancer comes back, the treatments can be repeated.
High-grade non-invasive papillary (Ta) tumors are more likely to come back after treatment, so intravesical Bacille-Calmette Guerin (BCG) is often recommended after surgery. Another option is intravesical chemotherapy with mitomycin. Either one is usually started several weeks after surgery and is given every week for several weeks. A third option is close observation without intravesical treatment.
Stage 0is
For flat non-invasive (Tis) tumors, BCG is the treatment of choice after surgery. Patients with these tumors often get 6 weekly treatments of intravesical BCG, starting a few weeks after TUR. Some doctors recommend repeating BCG treatment every 3 to 6 months.
Follow-up and outlook after treatment
After treatment for any stage 0 cancer, close follow-up is recommended, with cystoscopy about every 3 to 6 months for a least a couple of years to look for signs of the cancer coming back or for new bladder tumors.
The outlook for people with stage 0a (non-invasive papillary) bladder cancer is excellent. These cancers are nearly always cured with treatment. During long-term follow-up care, more superficial cancers are often found in the bladder or elsewhere in the urinary system. Although these new cancers do need to be treated, they rarely are deeply invasive or life threatening.
The long-term outlook for stage 0is (flat non-invasive) bladder cancer is not quite as good as for stage 0a cancers. These cancers have a higher risk of coming back, and may return as a more serious cancer that is growing into deeper layers of the bladder or has spread to other tissues.
Treating stage I bladder cancer
Stage I bladder cancers have grown into the connective tissue layer of the bladder wall but have not reached the muscle layer.
Transurethral resection (TURBT) is typically the first treatment for these cancers, but it is done to help determine the extent of the cancer rather than to try to cure it. If no other treatment is given, many patients will later get a new bladder cancer, which will often be more advanced. This is more likely to happen if the first cancer is high grade.
Even if the cancer is found to be low grade, a second TURBT is often recommended several weeks later. If the doctor then feels that all of the cancer has been removed, intravesical BCG or mitomycin is usually given. (Less often, close follow-up alone might be an option.) If not all of the cancer was removed, options include either intravesical BCG or cystectomy (removal of part or all of the bladder).
If the cancer is high grade, if many tumors are present, or if the tumor is very large when it is first found, radical cystectomy may be recommended.
For people who aren’t healthy enough for a cystectomy, radiation therapy (often along with chemo) might be an option for treatment, although the chances for cure might not be as good.
Treating stage II bladder cancer
These cancers have invaded the muscle layer of the bladder wall. Transurethral resection (TURBT) is typically the first treatment for these cancers, but it is done to help determine the extent of the cancer rather than to try to cure it.
When the cancer has invaded the muscle, radical cystectomy (removal of the bladder) is the standard treatment. Lymph nodes near the bladder are often removed as well. If cancer is in only one part of the bladder, some patients can be treated with a partial cystectomy instead. Only a small number of patients are good candidates for this.
Although at this stage the cancer has not been detected outside the bladder, in some cases there may already be tiny deposits of cancer growing elsewhere in the body. For this reason, chemotherapy is often given either before surgery (neoadjuvant chemo) or after surgery (adjuvant chemo) to lower the chance the cancer will come back.
Many doctors prefer to give chemo before surgery because it has been shown to help patients live longer than surgery alone. When chemo is given first, surgery is delayed. This is not a problem if the chemo shrinks the bladder cancer, but it might be harmful if the tumor continues to grow during chemo.
Another option for some patients may be a second (and more extensive) transurethral resection (TURBT), followed by radiation and chemotherapy. Some people may prefer this because it lets them keep their bladder, but it’s not clear if the outcomes are as good as they are after cystectomy, so not all doctors agree with this approach. If this treatment is used you will need frequent and careful follow-up exams. Some experts recommend a repeat cystoscopy and biopsy during treatment with chemo and radiation. If cancer is found in the biopsy sample, a cystectomy will likely be needed.
For patients who can’t have a major operation because of other serious health problems, TURBT, radiation, chemotherapy, or some combination of these may options.
Treating stage III bladder cancer
These cancers have reached the outside of the bladder and might have grown into nearby tissues or organs.
Transurethral resection (TURBT) is typically done first to help determine how far the cancer has grown. Radical cystectomy (removal of the bladder and nearby lymph nodes) is then the standard treatment. Partial cystectomy is seldom an option for stage III cancers.
Neoadjuvant chemotherapy (chemo) is often given before surgery. It can shrink the tumor, which may make surgery easier. This can be especially useful for T4a tumors, which have grown outside the bladder. The chemo may also kill any cancer cells that could already have spread to other areas of the body. This approach helps patients live longer than cystectomy alone. When chemo is given first, surgery to remove the bladder is delayed. The delay is not a problem if the chemo causes the bladder cancer to shrink, but it can be harmful if the tumor continues to grow during chemotherapy.
Some patients get chemo after surgery (adjuvant treatment) to kill any areas of cancer cells left after surgery that are too small to see. Chemo given after cystectomy may help patients stay cancer-free longer, but so far it’s not clear if it helps them live longer.
An option for some patients with single, small tumors might be treatment with a second (and more extensive) transurethral resection (TURBT) followed by a combination of chemotherapy and radiation. If this isn’t successful and cancer is found when cystoscopy is repeated, the patient might need cystectomy.
For patients who can’t have a major operation because of other serious health problems, treatment options might include TURBT, radiation, chemotherapy, immunotherapy, or some combination of these.
Treating stage IV bladder cancer
These cancers have reached the abdominal or pelvic wall (T4b tumors) or have spread to nearby lymph nodes or distant parts of the body. Stage IV cancers are very hard to get rid of completely.
In most cases surgery (even radical cystectomy) can’t remove all of the cancer, so treatment is usually aimed at slowing the cancer’s growth and spread to help you live longer and feel better. If you and your doctor discuss surgery as treatment option, be sure you understand the goal of the operation – whether it is to try to cure the cancer, to help you live longer, or to help prevent or relieve symptoms from the cancer – before deciding on treatment.
For stage IV bladder cancers that have not spread to distant sites, chemotherapy (with or without radiation) is usually the first treatment. If the cancer shrinks in response to treatment, a cystectomy might be an option. Patients who can’t tolerate chemo (because of other health problems) might be treated with radiation therapy or with an immunotherapy drug such as atezolizumab or pembrolizumab.
For stage IV bladder cancers that have spread to distant areas, chemo is usually the first treatment, sometimes along with radiation therapy. Patients who can’t tolerate chemo (because of other health problems) might be treated with radiation therapy or with an immunotherapy drug such as atezolizumab or pembrolizumab. Urinary diversion without cystectomy is sometimes done to prevent or relieve a blockage of urine that could otherwise cause severe kidney damage.
Because treatment is unlikely to cure these cancers, taking part in a clinical trial may offer you access to newer forms of treatment that might help you live longer or relieve symptoms.
Treating bladder cancer that progresses or recurs
If cancer continues to grow during treatment (progresses) or comes back (recurs), your treatment options will depend on where and how much the cancer has spread, what treatments you have already had, and on your health and desire for more treatment. It’s important that you understand the goal of any further treatment – if it’s to try to cure the cancer, to slow its growth, or to help relieve symptoms – as well as the likelihood of benefits and risks.
For example, non-invasive bladder cancer often comes back in the bladder. The new cancer may be found either in the same site as the original cancer or at other sites in the bladder. These tumors are often treated the same way as the first tumor. But if the tumor keeps coming back, the patient may need a cystectomy (removal of the bladder) at some point.
Cancers that recur in distant parts of the body can be harder to remove with surgery and might require other treatments, such as chemotherapy, immunotherapy, or radiation therapy. For more on dealing with a recurrence, see the website section Understanding Recurrence.
At some point, it may become clear that standard treatments are no longer controlling the cancer. If you want to continue getting treatment, you might think about taking part in a clinical trial of newer bladder cancer treatments. While these are not always the best option for every person, they may benefit you as well as future patients.
Can you lower your risk of the cancer progressing or coming back ?
If you have (or have had) bladder cancer, you probably want to know if there are things you can do that might lower your risk of the cancer growing or coming back, such as exercising, eating a certain type of diet, or taking nutritional supplements.
Unfortunately, it’s not yet clear if there are things you can do that will help. But because bladder cancer often comes back or new bladder cancers develop, this is an active area of study. Clinical trials are now looking to see if certain vitamins, minerals, dietary supplements, or medicines might lower the risk of bladder cancer returning.
Adopting healthy behaviors such as not smoking, eating well, being active, and staying at a healthy weight might help as well, but no one knows for sure. However, we do know that these types of changes can have positive effects on your health that can extend beyond your risk of cancer.
About dietary supplements
So far, no dietary supplements (including vitamins, minerals, and herbal products) have been shown to clearly help lower the risk of bladder cancer progressing or coming back. This doesn’t mean that no supplements will help, but it’s important to know that none have been proven to do so.
Dietary supplements are not regulated like medicines in the United States – they do not have to be proven effective (or even safe) before being sold, although there are limits on what they’re allowed to claim they can do. If you are thinking about taking any type of nutritional supplement, talk to your health care team. They can help you decide which ones you can use safely while avoiding those that might be harmful.
If the cancer comes back
If your cancer does come back at some point, your treatment options will depend on the location of the cancer and what treatments you’ve had before. Options might include surgery, intravesical therapy, radiation therapy, chemotherapy, immunotherapy, or some combination of these.
Could you get a second cancer after bladder cancer treatment ?
People who’ve had bladder cancer can still get other cancers. In fact, bladder cancer survivors are at higher risk for getting some other types of cancer.
Second Cancers After Bladder Cancer
Cancer survivors can be affected by a number of health problems, but often a major concern is facing cancer again. If a cancer comes back after treatment it is called a recurrence. But some cancer survivors may develop a new, unrelated cancer later. This is called a second cancer.
Unfortunately, being treated for bladder cancer doesn’t mean you can’t get another cancer. People who have had bladder cancer can still get the same types of cancers that other people get. In fact, they might be at higher risk for certain types of cancer.
Survivors of bladder cancer can get any type of second cancer, but they have an increased risk of certain cancers, including:
- A second bladder cancer (This is different from the first cancer coming back.)
- Cancer of the renal pelvis/ureter (the ureter is the tube connecting the kidney to the bladder; the part of the kidney where it attaches is called the renal pelvis)
- Cancer of the pancreas
- Cancer of the larynx (voice box)
- Lung cancer
- Vaginal cancer
- Prostate cancer
- Kidney cancer
- Acute myeloid leukemia (AML)
Many of these cancers are linked to smoking, which is a major risk factor for bladder cancer.
Follow-up after bladder cancer treatment
After completing treatment for bladder cancer, you should see your doctor regularly. Let them know about any new symptoms or problems, because they could be caused by the cancer coming back or by a new disease or second cancer.
Bladder cancer survivors should also follow the American Cancer Society guidelines for the early detection of cancer, such as those for colorectal and lung cancer. Most experts don’t recommend any other testing to look for second cancers unless you have symptoms.
Can you lower your risk of getting a second cancer ?
There are steps you can take to lower your risk and stay as healthy as possible. For example, it’s important to stay away from tobacco products. Smoking increases the risk of some of the second cancers seen after bladder cancer, as well as many other cancers.
To help maintain good health, bladder cancer survivors should also:
- Get to and stay at a healthy weight
- Stay physically active
- Eat a healthy diet, with an emphasis on plant foods
- Limit alcohol to no more than 1 drink per day for women or 2 per day for men
These steps may also lower the risk of some other health problems.
- What Is Bladder Cancer? American Cancer Society. https://www.cancer.org/cancer/bladder-cancer/about/what-is-bladder-cancer.html[↩]





{kind=link}